lisa marr, md section chief, palliative care department of internal medicine university of new...
TRANSCRIPT

LISA MARR, MDSection Chief, Palliative Care
Department of Internal MedicineUniversity of New [email protected]
Communication in End of Life Care: What’s New?
Disclosure
No conflicts of interest to disclose

RATIONING, DEATH PANELS, AND GRANNY-OH MY!
OUR STORY BEGINS IN JULY OF 2009…..
Health Care Debate 2009
Health Care Bill (HR 3200): 7/09
“Advance Care Planning Consultation”: A senior and a medical
practitioner (MD, PA, NP) discussing “advance care planning, if…the individual involved has not had such a consultation within the last 5 years.” Reimbursement by
Medicare Voluntary

“Advance Care Planning Consultation”, p. 425
Explanation by the practitioner of “…advance care planning, including key questions and
considerations, important steps, and suggested people to talk to”
“…advance directives, including living wills and durable powers of attorney, and their uses”
“…the role and responsibilities of a health care proxy”
“Advance Care Planning Consultation”, p. 425
Explanation by the practitioner of “…the continuum of end-of-life services and supports
available, including palliative care and hospice, and benefits for such services and supports that are available under this title”
“…orders regarding life sustaining treatment or similar orders.”
“Provide a list of national and State-specific resources to assist consumers and their families with advance care planning”
Euthanasia? 7/09
“This provision might start us down a treacherous path toward government-encouraged euthanasia if enacted into law.”
House Minority Leader John Boehner
Death Panels? 8/09
“And who will suffer the most when they ration care? The sick, the elderly, and the disabled, of course. The America I know and love is not one in which my parents or my baby with Down Syndrome will have to stand in front of Obama’s “death panel” so his bureaucrats can decide, based on a subjective judgment of their “level of productivity in society,” whether they are worthy of health care. Such a system is downright evil.”
Former Alaska Governor Sarah Palin

Rationing care? 8/09
“[I]t was President Obama himself who suggested that seniors who don’t have as long to live might want to consider just taking a pain pill instead of getting an expensive operation to cure them,” said Huckabee.
Under President Obama's health care plan, (Ted) Kennedy would have been told to go home to take pain pills and die" during his last year of life, rather than… freely d(oing) what most of us would do. He chose an expensive operation and painful follow up treatments.”
Former Arkansas Governor Mike Huckabee

Newsweek 9/09
2006 health care expenditures: >$2 trillion
Population > 65 yo: 2006: 37.3 million 2030: 71.5 million
30% of Medicare funds each year are spent on terminal care for 5% of the program's patients. Nearly all Medicare
beneficiaries spend some time in hospital in last year of life
78% of last-year-of-life expenses occur in the month before death (primarily secondary to life sustaining care)
Rationing- 1962 Dialysis “God Squads”; 2009: Insurance, Transplant Committees, No money/No Care, Non-citizens, Clinical Trials, Oregon Health Plan, etc.
“Americans want the best, they want the latest, and they want it now”
Questions:
Do end of life conversations help or harm patients? What is the evidence?
Example: Code status/DNR discussions Communication: What works? What doesn’t?
Review an 8 step process to discuss code status
WHY DISCUSS THE FUTURE?
Setting the Stage

Do patients want to discuss EOL care?
<50% patients who want to have EOL care discussions with physicians do so (cancer and non-cancer)
Advanced Cancer: 25% of patients with incurable cancer aren’t told that65% no time-based prognosis discussed 1/3 of patients receiving chemotherapy believe its intent is to cure
them20% of patients receive chemo in the last 3 weeks of life.
Providers less likely to have EOL discussions for patients with non-cancer illnesses
Matsuyama J Clin Oncol 2006. Hagerty Ann Oncol 2005. Ray A J Palliat Med 2006. Zhang ASCO 2008. Mitchell Supp Care Cancer 2007.

Do we do a good job of discussing the future?
As a profession – no. Why not? Perceived lack of training Stress Take away hope No time to address emotional needs Harm patients (they’ll give up and die sooner) Hurt our relationship with the patient What if we’re wrong? Uncertainty about prognosis It’s emotionally difficult for us Explicit requests by patient/family not to discuss
This is despite strong evidence patients benefit from this and consistent evidence they want to talk about it
Hancock Palliat Med 2007.

Elephant in the Room
Prognosis affects choices about CPR
People can make better medical decisions (better = more informed) when they know their prognosis 41% of elderly patients would want CPR for an in-
hospital cardiac arrest Decreases to 22% when told their probability of
survival to discharge was “10-17%” 11% with a chronic/terminal illness (life-expectancy
<1 year) would want CPR Decreases to 5% when told prognosis “0-5%”
probability of survival to discharge
Murphy et al. NEJM 1994
Prognosis affects choices about EOL care
Hospitalized cancer patients with prognosis <6 months Those who thought prognosis >6 months were
much more likely to… Want life-prolonging treatments Want ‘aggressive’ treatments (ICU, ventilators) Die on the vent
…Than those who thought prognosis was <6months.
Survival was the same in both groups
Weeks et al. JAMA 1998.
Coping With Cancer Study (CWCS)
Coping with Cancer Study: 332 patients with metastatic cancer and progression through
1st-line chemo and their caregivers (dyads) NCI/NIMH funded, multisite, prospective cohort
71.3% white; 14.8% Black; 11.9% Hispanic; 1.7% Asian and 51.1% male
Median survival: 4.4 months 123/332 (37.0%) reported EOL discussions with MD at
baseline Sicker patients: lower performance status, higher
symptom burden, shorter survival time No difference in age, sex, race, religion, education, cancer
type, marital status, race/ethnicity, health insurance status
Wright et al. JAMA 2008

Do EOL conversations cause emotional harm?
CWCS: Discussions about EOL were NOT associated with feeling: “Depressed”, “sad”, “terrified”, “worried” or meeting
DSM criteria for mental disorder
Wright et al. JAMA 2008

Care choices affected by EOL discussions
Patients who had discussions about EOL with physicians
More likely to: Accept diagnosis as terminal (59.2% vs. 28.7%) p<.001 Prefer medical treatment focused on relieving pain and
discomfort over life extending therapies (52.9% vs. 28.7%) p<.001
Complete a DNR order (63.0% vs. 28.5%) p<.001Less likely to:
Receive mechanical ventilation (1.6% vs. 11.0%) p=.02 Undergo resuscitation effort (0.8% vs. 6.7%) p=.02 Be admitted to an intensive care unit (65.5% vs. 44.5%) p=.03
Wright et al. JAMA 2008
QOL and aggressive care
Quality of Life In final week of life, QOL decreased with increasing
number of aggressive interventions (even after adjustment for severity of illness) (6.4 vs. 4.6, p=0.1)
In final weeks of life, QOL increased with hospice care Longer on hospice, higher reported QOL (6.9 vs. 5.6,
p=0.1)
Wright et al. JAMA 2008

Do conversations about EOL harm families?
No! If physicians discussed EOL options/the future with patients, bereaved families reported: Higher satisfaction with communication from
physician, comfort of patient Better understanding of “what to expect” as family
member died
Teno J et al. JAGS 2007. Engel SE et al. JAGS 2006.
CWCS: Caregiver Outcomes
Caregivers of patients who received aggressive care in last week of life were more likely to: Develop Major Depressive Disorder (OR 3.37) Experience regret (p=.01) Feel unprepared for patient’s death (p<.001) Have poorer overall QOL (p=.004) Have poorer self reported health (p=.04)
Wright et al. JAMA 2008

CWCS: Caregiver Outcomes
Better QOL in patients associated with Better overall QOL (p=.001) Self reported health (p=.004) Physical functioning (p=.02) Mental health (p=.04) Felling better prepared for the death (p=.002) Less regret (p<.001)
In caregivers at 6 month follow-up“Cascading benefits” for patients and
caregivers Wright et al. JAMA 2008
EOL discussions decrease health care costs
CWCS: 188/603 participants (31.2%) reported EOL discussions at baseline no difference in cancer type, recruitment site,
treatment preferences, illness acknowledgement, SESQuestion: Do end of life conversations
result in cost savings (aggregate costs)? Did not have discussion:
$2917 ($285/day) Had discussion:
$1876 ($177/day)
Zhang B et al. Arch Intern Med. 2009

EOL discussions decrease health care costs
EOL discussion reduced cost by 35.7% (less use intensive interventions) Higher medical costs associated with worse
physical distress (p=.003), worse overall QOL per caregiver (p=.006)
Survival was the same in both groups…..
Zhang B et al. Arch Intern Med. 2009
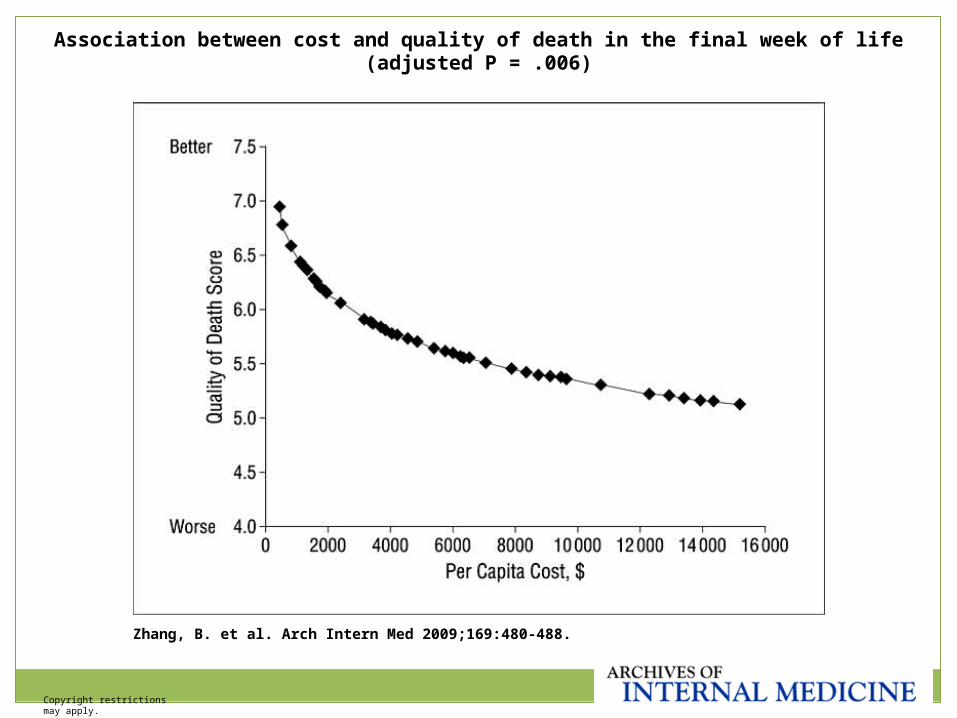
Copyright restrictions may apply.
Zhang, B. et al. Arch Intern Med 2009;169:480-488.
Association between cost and quality of death in the final week of life (adjusted P = .006)
Outcomes of EOL discussions
Patients who have EOL discussions with their doctors
More likely to: Have an advance directive Understand illness terminal Die at home Have EOL choices followed (i.e. DNR order in patients who
want to be DNR) Choose hospice
Improved QOL for EOL patients (sx relief, MD communication, emotional support, being tx with respect)
Decreased Major Depression in bereaved caregiversLess likely to:
Have a feeding tube
References 1-7
What do patients want to know?
Studied extensively in Western worldMostly cancer – although other diseases
representedPatients want
Realistic, truthful information What will happen is as important as time How they are told is as important as what they are
told Hope, optimism
How one is told
Loved ones presentAdequate timeAcknowledgment of emotional, spiritual,
existential impact of having a life-limiting disease
‘Attitude’ of the clinicianRespect for patient’s emotional state
Hagerty Ann Onc 2005. Clayton Supp Care CA 2005. Curtis J Palliat Med 2008.
Hope and Optimism
Qualitative research: Clayton Cancer 2005: Explored with advanced
cancer patients n=19 (& caregivers) how can clinicians can foster hope when they talk about future.
Major themes Emphasize what can be done Emotional support, care, dignity, listening, non-
abandonment Practical support (help in home)/Discuss day-to-day
living Truth-telling but ‘not blunt,’ leaving space for the
unanticipated

Hope & Optimism – What generates hope?
The top 4 hope-destroying actions by physicians Appeared nervous or uncomfortable “Gave my prognosis to my family, then gradually
told me” Used euphemisms “Avoided talking about the cancer and only
discussed treatment”Hagerty J Clin Oncol 2005

Hope & Optimism
“Hope” = a sense of receiving good care…“best” care – all the
right things are being done, non-abandonment, confidence and warmth with the physician, completeness of information, And NOT being told unambiguously “There is no
hope of recovery” These themes far out-shadow the way
preserving hope is often conceived: half-truths, concealing information, only positives

“Most patients…”
…means some patients Don’t want to talk about the future Don’t want straight-forward assessments of
prognosis Don’t want to talk about anything ‘negative’ Want us to promise them cure, recovery
…doesn’t necessary include the patient in front of us

What will happen…
…Is just as important as timeNear universal finding when looked at
Impact of illness & its treatment on their lives What to expect – treatment and functional courses True in cancer, CHF, COPD, dementia Near the end…
Places of death, impact of death on family, help they can get
Hagerty et al Ann Oncol 2005. Curtis et al. Eur Resp J 2004. Curtis et al. Chest 2002. Knauft et al. Chest 2005.

Can’t I just give him an Advance Directive?
Patient Self-Determination Act (PSDA) 1990 Requires that all Medicaid and Medicare
providers inform adult patients of right to: Participate in and direct their own HC decisions Accept or refuse treatment To prepare an Advance Directive (Living Will, POAHC) Be informed of healthcare facilities policies on these
rights
Can’t I just give him an Advance Directive?
Mixed results: Hospital LOS, place of death (home vs. hospital), costs of
hospital stay, medical treatments not affected by AD (ref. 19-27)
Teno JM et al. JAGS 2007 (retrospective) Less Life Sustaining Treatment, greater use hospice, less
likelihood of terminal hospitalization Families : fewer concerns about physician communication; more
aware of “what to expect” with the dying process BUT
¼ unmet pain needs ½ inadequate emotional support for dying person 1/3 inadequate family support
Advance directives should be the start of a conversation, not the end…..
“DO YOU WANT US TO DO EVERYTHING?”
Discussions About Code Status
Case 1: RF
A 68 yo man is newly diagnosed with metastatic hepatocellular cancer, alcohol related liver failure, and impending kidney failure.
Because of his poor functional status (ECOG 3-4) and organ failure, he is not a candidate for chemotherapy. The oncologist told him this.
Prognosis: days to a week or twoMedicine Team: “He seems to have unrealistic
expectations. I asked him “Do you want us to do everything? and he said “Yes”. So he’s a full code.”
CPR- How effective is it?
Inpatient setting: 40% survive the CPR effort 1/3 survive to leave the hospital (i.e. 14% of total) So 86% of patients who code in hospital die in the
hospital More successful if CPR is in OR, ICU, Cath lab
Depending on study, 7-26% survive a CPR effort
MH Ebell et al. J Gen Intern Med. 1998 (Meta-analysis); Tresch D et al. JAGS 1994; Warner SC and Sharma TK. Resuscitation 1994.
CPR-How effective is it?
Low likelihood of survival if: Sepsis
1/73; 0/42 survived CPR effort Metastatic cancer
0-14% survived CPR effort Renal failure Need for vasopressors or inotropes
2/55 survived CPR effort (both had reversible conditions, i.e. AMI, arrythmia)
Nursing home residents 0-1.7% survive CPR effort
Age alone not a RF References 30-38, 41

Outcome of CPR in the ICU Setting
114 MICU patients underwent CPRMean age 59
25% malignancy, 18% vascular disease, 7% chronic liver disease, 5% ESRD, 5% COPD: 34% sepsis, 20% PNA
33% had been housebound or bedridden prior to admission44% survived initial effort, but…Only 31% with CPR effort survived >24 hours,
and…. 1/29 malignancy; 1/39 sepsis survived effort
Only 5% survived to discharge. 6 patients survived to hospital D/C (5% patients)
4/6 died in one year; 2 had severe disabilities and were alive at 1 year
Patients with chronic medical conditions undergoing CPR even in an ICU setting seldom survive to discharge…FJ Landry et al. Arch Intern Med 1992
Problems that arise in DNR discussions
Expecting patients to make decisions without adequate information (i.e. un-informed consent) Diagnosis Treatment options Prognosis
CPR discussions MUST be framed in terms of the overall goals of care and care plan, not in isolation
Weigh benefit/burden of each treatment option Can we do it? Should we do it?

Communication
Common phrases: “What would you like us to do if your heart stops?” “Do you want us to restart your heart if it stops?” “Do you want us to do everything?” “You don’t want us to break your ribs, and shove a
tube down your throat, and hook you to a breathing machine, do you?”
Barriers to patients accepting DNR
DNR only refers to this medical interventionMany patients and families fear that
DNR=“No Care”Unfortunately, medical teams often reinforce
this fear: We can’t take him to the ICU if he’s DNR He can’t get antibiotics if he’s DNR We think the best thing is to “withdraw care”

Steps for Discussion of CPR
Quiet setting; clarify goals for the meetingDetermine decisionality- make sure right people
are at meeting (team/decision maker)Clarify in your mind beforehand what is best
medical careWho is this person? “Tell me about your Dad. I
have all the medical information, but want to know more about him as a person. Can you tell me a little about him, and how things were going before he came into the hospital?”
Steps for Discussion of CPR
Ask patient/family what they know about medical condition- make no assumptions!
Present medical information; clarify misunderstandings
“Have you ever thought about what your wishes would be if you were ever in this situation?” or “ Has your father ever talked about what would be most important to him if he was ever in this situation?”
Helpful Communication Phrases
Make recommendation in terms of overall plan of care “Given that your cancer is growing and not responding to
chemotherapy, I think the best plan would be that we don’t use any more chemotherapy.”
“Your father is very sick. His heart, liver and kidneys are failing, despite our best medical efforts. He is dying.”
Judge whether the time is right to talk about CPR, or whether this would best be left to another discussion
These discussions are often a process….
Helpful Communication Phrases if Team Believes DNR is Not Appropriate
I want to talk about something that’s hard to discuss.
When someone’s heart and breathing stop, in other words when they die, we have a lot of things we can do to attempt to try and reverse this. This is called cardiopulmonary resuscitation, or CPR.
In patients who are very sick as you are, CPR has a low likelihood of working. In other words, patients rarely survive the CPR effort, and if they do, it’s extremely rare to make it out of the hospital.
Helpful Communication Phrases
CPR may just prolong the dying process, cause suffering and not bridge you to getting better, because it doesn’t fix the cancer (or whatever underlying process is present).
I would recommend that we protect you from CPR, which will only harm you and not offer benefit, and not do this when that time comes. This is what’s called “Do Not Resuscitate.”
Helpful Communication Phrases
Instead, I would recommend that we make sure you are comfortable, as pain free as possible, and well cared for as you are dying.
What are your thoughts about this?

Communication
Remember it often takes several discussions; people are processing tough information; give people time (if possible) and space
Respond to affect with affect I can see this is hard for you to hear (reflect on emotion in
the room). Silence: Can you tell me what your thoughts are? Have you
thought about this before? Allow silence; let patient determine tempo of discussion
To patient, this is an out-of-control situation. Try and give back as much control as possible
Communication
If you take something “off the table”, put something back on: Symptom control Family support Hospice care Other
Reassure non-abandonment“Even though we can’t fix the illness, there is
a lot we can do to help you and your family in this time. I want to hear what is most important to you and your family”
Does the order make sense?
Don’t let the sun set on a code status order that makes no sense Only cardioversion (in a patient who will die a
respiratory death) Only one shock, then stop Only for 5 minutes, then stop Chest compressions without cardioversion “He wants intubation, but he doesn’t want to be on a
ventilator…”
Summary
EOL discussions can benefit patients and families in real ways; do not cause harm May take a series of discussions…
EOL counseling should optimally start before a crisis
EOL discussions can help ensure patient autonomy, not take it away
Communication skills training is needed to help clinicians Major education focus of Palliative Medicine team:
medicine residents; oncology, geriatric and pain fellows. Better communication skills=less anxiety for HCP’s?
References
1. Hofmann JC et al. Patient preferences for communication with physicians about end-of-life decisions. Ann Intern Med 1997;127(1):1-12.
2. Teno JM et al. Family perspectives on end of life care at the last place of care. JAMA 2004;291(1):88-93.
3. Reilly BM et al. Can we talk? Inpatient discussions about advance directives in a community hospital. Attending physicians' attitudes, their inpatients' wishes, and reported experience. Arch Intern Med. 1994;154:2299-308.
4. Haas JS et al. Discussion of preferences for life-sustaining care by persons with AIDS. Predictors of failure in patient-physician communication. Arch Intern Med. 1993;153:1241-8.
5. Shmerling RH et al. Discussing cardiopulmonary resuscitation: a study of elderly outpatients. J Gen Intern Med. 1988;3:317-21.
6. Frankl D, Oye RK, Bellamy PE. Attitudes of hospitalized patients toward life support: a survey of 200 medical inpatients. Am J Med. 1989;86(6 pt 1): 645-8.
7. Teno JM et al. Association between advance directives and quality of end-of-life care: a national study. JAGS 2007; 55:189-94.
8. Engel SE et al. Satisfaction with end-of-life care for nursing home residents with advanced dementia. JAGS 2006; 54:1567-72
References
9. Zhang B et al. Health Care Costs in the Last Week of Life: Associations With End-of-Life Conversations. Arch Intern Med. 2009;169(5):480-488.
10. Wright AA et al. Associations Between End-of-Life Discussions, Patient Mental Health, Medical Care Near Death, and Caregiver Bereavement Adjustment. JAMA 2009;8(300):1665-1673.
11. Weeks JC et al. Relationship Between Cancer Patients’ Predictions of Prognosis and Their Treatment Preferences. JAMA 1998;279(21):1709-1714.
12. Hanchate A et al. Racial and Ethnic Differences in End-of-Life Costs: Why Do Minorities Cost More Than Whites? Arch Intern Med 2009;169(30): 493-501
13. Phelps AC et al. Religious Coping and Use of Intensive Life-Prolonging Care Near Death in Patients With Advanced Cancer. JAMA 2009;301(11):1140-1147

References
14. Murphy DJ et al. The Influence of the Probability of Survival on Patients' Preferences Regarding Cardiopulmonary Resuscitation. NEJM 1994; 330:545-549.
15. Volandes AE et al. Using video images of dementia in advance care planning. Arch Int Med 2007; 167:828-833.
16. Volandes AE et al. Health literacy not race predicts EOL preferences. J Palliat Med. 2008; 11: 754-62.
17. Volandes AE et al. Overcoming educational barriers for advance care planning in Latinos with video images. J Palliat Med. 2008; 11: 700-6.
18. Prigerson HG. Socialization to Dying: Social Determinants of Death Acknowledgement and treatment Among Terminally Ill Geriatric Patients. J Health Soc Behavior 1992;33:378-395.
19. Schneiderman LJ et al. Effects of Offering Advance Directives on medical Treatments and Costs. Ann Intern Med 1992;117:599-606.
20. Kessler DP and McClellan MB. Advance directives and medical treatment at end of life. J Health Econ. 2004 Jan;23(1):111-27
21. Teno JM et al. Association between advance directives and quality of end-of-life care: a national study. J Am Geriatr Soc. 2007 Feb;55(2):189-94

References
22. Weeks WB, Kofoed LL, Wallace AE et al. Advance directives and the cost of terminal hospitalization. Arch Intern Med 1994;154:2077–2083.
23. Chambers CV, Diamond JJ, Perkel RL et al. Relationship of advance directives to hospital charges in a Medicare population. Arch Intern Med 1994;154:541–547.
24. Molloy DW, Guyatt GH, Russo R et al. Systematic implementation of anadvance directive program in nursing homes: A randomized controlled trial. JAMA 2000;283:1437–1444.
25. Degenholtz HB, Rhee Y, Arnold RM. Brief communication: The relationship between having a living will and dying in place. Ann Intern Med
2004;141:113–117.26. Teno JM, Lynn J, Phillips RS et al. Do formal advance directives affect
resuscitation decisions and the use of resources for seriously ill patients? SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments. J Clin Ethics 1994;5:23–30.
27. Teno JM, Lynn J, Connors AF Jr et al. The illusion of end-of-life resource savings with advance directives. SUPPORT Investigators. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment. J AmGeriatr Soc 1997;45:513–518.
28. Hancock K et al. Truth-telling in discussing prognosis in advanced life-limiting illnesses: a systematic review. Palliat Med. 2007; 21:507-517.
29. Mark H Ebell, Lorne A Becker, Henry C Barry, and Michael Hagen. Survival After In-House Cardiopulmonary Resuscitation: A Meta-Analysis. J Gen Intern Med. 1998 December; 13(12): 805–816.

References
30. Saklayen, M et al. In-Hospital Cardiopulmonary Resuscitation: Survival in 1 Hospital and Literature Review. Medicine 1995; Volume 74(4): 163-175.
31. Faber-Langendorf K. Resuscitation of patients with metastatic cancer: is transient benefit still futile? Arch Intern Med 1991;151:235-239.
32. Vitelli CE et al. Cardiopulmonary resuscitation and the patient with cancer. J Clin Oncol 1991;9:111-115.
33. Rosenberg M et al. Results of cardiopulmonary resuscitation: Failure to predict survival in two community hospitals. Arch Intern Med 1993;153:1370-1375
34. Bedell SE et al. Survival after cardiopulmonary resuscitation in the hospital. JAMA 1985;253:1370-1375
35. Murphy DJ et al. Outcomes of cardiopulmonary resuscitation in the elderly. Ann Intern Med 1989;111:199-205.
36. Appelbaum GE et al. The outcome of CPR initiated in nursing homes. J Am Geriatr Soc 1990;38:197-200
37. Awoke S, Mouton CP, Parrott M. Outcomes of skilled cardiopulmonary resuscitation in a long-term care facility. J Am Geriatr Soc 1992;40:593-595
38. Francis J. Landry; Joseph M. Parker; Yancy Y. Phillips. Outcome of Cardiopulmonary Resuscitation in the Intensive Care Setting. Arch Intern Med 1992;152:2305-2308.
References
39. Grigoriyan A et al. Outcomes of cardiopulmonary resuscitation for patients on vasopressors or inotropes: A pilot study. J Critical Care 2009;24:415-418.
40.Hwang J et al. Survival in cancer patients after out-of-hospital cardiac arrest. Support Care Cancer 2009;epub
41.Ehlenbach WJ et al. Epidemiologic Study of In-Hospital Cardiopulmonary Resuscitation in the Elderly. NEJM 2009;361(1):22-31
42.Tresch D et al. Cardiopulmonary resuscitation in elderly patients hospitalized in the 1990’s: a favorable outcome. J Am Geriatr Soc 1994;42:137-141.
43. Warner SC, Sharma TK. Outcome of cardiopulmonary resuscitation and predictors of resuscitation status in an urban community teaching hospital. Resuscitation 1994;27:13-21.

Thank you! Questions?