left ventricular ejection fraction and risk of stroke and...
TRANSCRIPT

1
In patients with heart failure (HF), a reduced left ventricu-lar (LV) systolic function is associated with an increase in
mortality and incidence of cardiovascular events. LV ejec-tion fraction (LVEF) is the most widely accepted indicator of LV systolic function and is associated with cardiovascular
outcomes. LVEF was shown to be inversely associated with cardiovascular mortality up to an LVEF of 45%, above which level the association is lost. In the Candesartan in Heart Failure Reduction in Mortality (CHARM) trial, all-cause mortality increased by 39% for every 10% reduction in
Background and Purpose—In heart failure (HF), left ventricular ejection fraction (LVEF) is inversely associated with mortality and cardiovascular outcomes. Its relationship with stroke is controversial, as is the effect of antithrombotic treatment. We studied the relationship of LVEF with stroke and cardiovascular events in patients with HF and the effect of different antithrombotic treatments.
Methods—In the Warfarin Versus Aspirin in Reduced Ejection Fraction (WARCEF) trial, 2305 patients with systolic HF (LVEF≤35%) and sinus rhythm were randomized to warfarin or aspirin and followed for 3.5±1.8 years. Although no differences between treatments were observed on primary outcome (death, stroke, or intracerebral hemorrhage), warfarin decreased the stroke risk. The present report compares the incidence of stroke and cardiovascular events across different LVEF and treatment subgroups.
Results—Baseline LVEF was inversely and linearly associated with primary outcome, mortality and its components (sudden and cardiovascular death), and HF hospitalization, but not myocardial infarction. A relationship with stroke was only observed for LVEF of <15% (incidence rates: 2.04 versus 0.95/100 patient-years; P=0.009), which more than doubled the adjusted stroke risk (adjusted hazard ratio, 2.125; 95% CI, 1.182–3.818; P=0.012). In warfarin-treated patients, each 5% LVEF decrement significantly increased the stroke risk (adjusted hazard ratio, 1.346; 95% CI, 1.044–1.737; P=0.022; P value for interaction=0.04).
Conclusions—In patients with systolic HF and sinus rhythm, LVEF is inversely associated with death and its components, whereas an association with stroke exists for very low LVEF values. An interaction with warfarin treatment on stroke risk may exist.
Clinical Trial Registration—URL: http://www.clinicaltrials.gov. Unique identifier: NCT00041938. (Stroke. 2016;47:00-00. DOI: 10.1161/STROKEAHA.116.013679.)
Key Words: aspirin ◼ echocardiography ◼ heart failure ◼ heart ventricles ◼ stroke ◼ warfarin
Left Ventricular Ejection Fraction and Risk of Stroke and Cardiac Events in Heart Failure
Data From the Warfarin Versus Aspirin in Reduced Ejection Fraction Trial
Marco R. Di Tullio, MD; Min Qian, PhD; John L.P. Thompson, PhD; Arthur J. Labovitz, MD; Douglas L. Mann, MD; Ralph L. Sacco, MD;
Patrick M. Pullicino, MD; Ronald S. Freudenberger, MD; John R. Teerlink, MD; Susan Graham, MD; Gregory Y.H. Lip, MD; Bruce Levin, PhD; J.P. Mohr, MD;
Richard Buchsbaum; Conrado J. Estol, MD; Dirk J. Lok, MD; Piotr Ponikowski, MD; Stefan D. Anker, MD; Shunichi Homma, MD; for the WARCEF Investigators
Received April 5, 2016; final revision received May 31, 2016; accepted May 31, 2016.From the Division of Cardiology, Department of Medicine (M.R.D.T., S.H.), Department of Biostatistics, Mailman School of Public Health (M.Q.,
J.L.P.T., B.L., R.B.), and Department of Neurology (J.P.M.), Columbia University Medical Center, New York; Department of Cardiovascular Medicine, University of South Florida, Tampa (A.J.L.); Cardiovascular Division, Department of Medicine, Washington University, St. Louis, MO (D.L.M.); Departments of Neurology, Epidemiology and Public Health, University of Miami, FL (R.L.S.); Kent Institute of Medicine and Health Science, Canterbury, United Kingdom (P.M.P.); Division of Cardiology, Department of Medicine, Lehigh Valley Hospital, Allentown, PA (R.S.F.); Section of Cardiology, San Francisco Veterans Affairs Medical Center, University of California San Francisco (J.R.T.); Division of Cardiology, Department of Medicine, SUNY Upstate Medical University, Buffalo, NY (S.G.); University of Birmingham Centre for Cardiovascular Sciences, City Hospital, United Kingdom (G.Y.H.L.); Centro Neurológico de Tratamiento y Rehabilitación, Buenos Aires, Argentina (C.J.E.); Department of Cardiology, Deventer Hospital, The Netherlands (D.J.L.); Department of Heart Diseases, Wroclaw Medical University, Military Hospital, Poland (P.P.); and Department of Innovative Clinical Trials, University Medicine Göttingen (UMG), Germany (S.D.A.).
The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA. 116.013679/-/DC1.
Correspondence to Marco R. Di Tullio, MD, Division of Cardiology, PH 3–342, 622 W, 168th St, New York, NY 10032. E-mail [email protected]© 2016 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.116.013679
Original Contribution
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

2 Stroke August 2016
LVEF <45%.1 Similar results were reported by the Digitalis Investigation Group (DIG).2
Some aspects of the relationship between LVEF and cardiovas-cular events in HF remain controversial. An association between decreased LVEF and thromboembolic events (stroke or periph-eral embolism) has been alternatively suggested3 or refuted.1,2 Although patients with HF are often treated with antithrom-botic agents (antiplatelet or systemic anticoagulation) to prevent thromboembolic complications and especially ischemic stroke, it is unclear whether lower LVEF may have a different impact on outcome depending on the antithrombotic treatment chosen.
In the Warfarin Versus Aspirin in Reduced Ejection Fraction (WARCEF) trial, 2305 patients with HF were randomized to aspirin or adjusted-dose warfarin and followed-up for an aver-age of 3.5 years. In the main results of the trial, patients on either treatment had similar rates of death and primary outcome (death, stroke, or intracerebral hemorrhage), although patients on warfarin had significantly reduced incidence of stroke.4,5 Here, we analyze the relationship of LVEF with mortality, stroke, and cardiovascular outcomes in WARCEF and possible interactions between LVEF and antithrombotic treatment.
Materials and Methods
Study PatientsDetails of the WARCEF trial enrollment were previously published.4 Briefly, from October 2002 through January 2010, a total of 2305 patients were enrolled in the trial (1119 in the United States and Canada and 1186 in Europe and Argentina) at 168 centers in 11 countries. Eligible patients were ≥18 years of age and had normal sinus rhythm, no contraindication to warfarin therapy, and an LVEF of ≤35% as assessed by quantitative echocardiography (or a wall-motion index of ≤1.2) or by radionuclide or contrast angiography within 3 months before randomization.
For details on eligibility criteria and study medications, please see the online-only Data Supplement. Patients were randomized to either adjusted-dose warfarin with target international normalized ratio of 2.75 (acceptable range: 2.0–3.5) or aspirin 325 mg daily in a double-blind, double-dummy design.
LVEF DeterminationLVEF assessment was performed by echocardiography at the individual sites. Mean time from echocardiogram performance to enrollment was 6.5 days. All echocardiograms were reinterpreted, blinded to treatment assignment, at a core echocardiography laboratory to confirm LVEF assessment. LVEF was determined by contrast angiography, radionu-clide scanning, or magnetic resonance imaging in 239 patients (10.4%).
Follow-Up and Outcome EventsFollow-up was performed monthly by telephone or in person. An in-person assessment was conducted quarterly for clinical evaluation.
Primary outcome of the trial was the time to first event in a com-posite end point of ischemic stroke, intracerebral hemorrhage, or death. Individual outcomes were also recorded. For definitions of outcome events, please see the online-only Data Supplement.
Statistical AnalysisBaseline demographics, clinical characteristics, and various outcome events by LVEF categories were compared using ANOVA F tests for continuous variables, χ2 tests for categorical variables, and log-rank tests for time-to-event outcomes. Univariable and multivariable Cox models were used to assess the effect of demographic and clinical variables on outcomes of interest.
To identify high-risk thresholds, we dichotomized LVEF at dif-ferent cutoff points and assessed the association between dichoto-mized LVEF and each outcome first with univariable Cox models and then with adjustment for covariates. Incidence rates of outcome events stratified by optimal LVEF cutoff points were compared using Poisson regression.
Cox models were used to evaluate separately the association between LVEF and outcomes in patients treated with warfarin or aspi-rin and assess any interaction between LVEF level and treatment type.
For warfarin treatment, time in therapeutic range (TTR) was compared in different stroke and LVEF subgroups using Wilcoxon signed-rank test.
ResultsMean LVEF in the study cohort was 24.7±7.5. Demographics and clinical characteristics of the cohort by LVEF category are shown in Table 1.
The mean follow-up time was 3.5±1.8 years, and the total follow-up time was 8225 patient-years. Survival status was known for 97.0% of the patients. A total of 34 patients (1.5%) withdrew consent, and 35 patients (1.5%) were lost to follow-up.
Overall, 622 of the 2305 patients (27.0%) had a primary outcome (531 deaths [85.4%], 84 ischemic stroke [13.5%], and 7 intracerebral hemorrhage [1.1%]), 356 patients (15.4%) had cardiovascular death, 195 patients (8.5%) had sudden death, 72 patients (3.1%) had a myocardial infarction (MI), and 451 patients (19.6%) experienced HF hospitalization.
LVEF and OutcomesTable 1 also summarizes the frequency of outcome events by LVEF category. Incidence of primary outcome, death (all-cause, cardiovascular death, and sudden death), and HF hos-pitalization increased progressively with decreasing LVEF; no such relationship was observed for stroke and MI.
Age, male sex, heart rate, diabetes mellitus, New York Heart Association class, ischemic cardiomyopathy, previous stroke/transient ischemic attack, and serum creatinine level were sig-nificantly associated with the primary outcome. LVEF, body mass index, systolic blood pressure, and the presence of an internal defibrillator were inversely associated with this out-come (Table I in the online-only Data Supplement).
Although most of these variables were also associated with all-cause death (Table II in the online-only Data Supplement) and also with cardiovascular or sudden death and HF hospi-talization, only LVEF of <15% and previous stroke/transient ischemic attack were associated with stroke (Table III in the online-only Data Supplement).
For the primary outcome and all-cause death, the LVEF cut-off point associated with the greatest increase in risk was 25%; for cardiovascular death, sudden death, and HF hospitalization it was 20% (Table IV in the online-only Data Supplement). For all 5 outcomes, all LVEF cutoff points were associated with increased risk, confirming the linearity of the association. LVEF of <15% was associated with a doubling of the risk of stroke; no other cutoff point was identified. No cutoff point of increased risk was identified for MI.
Table 2 shows the hazard ratios for each outcome after adjustment for pertinent covariates, using the cutoff points of greatest increase in risk.
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Di Tullio et al LVEF, Stroke, and Cardiovascular Events in Heart Failure 3
Table 1. Demographics and Clinical Characteristics of the Study Cohort by LVEF Categories*
Covariate LVEF<20% (n=603)LVEF 21%–25%
(n=559)LVEF 26%–29%
(n=533) LVEF≥30% (n=610) P Value
Location <0.001
Argentina 18/603 (3.0) 29/559 (5.2) 15/533 (2.8) 30/610 (4.9)
Europe 284/603 (47.1) 221/559 (39.5) 249/533 (46.7) 340/610 (55.7)
North America 301/603 (49.9) 309/559 (55.3) 269/533 (50.5) 240/610 (39.3)
Age, y 59.6±11.6 60.6±11.2 60.9±11.4 62.0±11.1 0.004
Male sex 486/603 (80.6) 438/556 (78.8) 419/531 (78.9) 497/610 (81.5) 0.598
Race or ethnic group 0.018
Non-Hispanic white 440/603 (73.0) 407/555 (73.3) 395/531 (74.4) 491/610 (80.5)
Non-Hispanic black 106/603 (17.6) 88/555 (15.9) 76/531 (14.3) 62/610 (10.2)
Hispanic 37/603 (6.1) 47/555 (8.5) 41/531 (7.7) 41/610 (6.7)
Other 20/603 (3.3) 13/555 (2.3) 19/531 (3.6) 16/610 (2.6)
Height, cm 171.6±9.2 171.8±9.4 171.4±9.1 171.8±9.4 0.841
Weight, kg 85.6±20.0 86.0±19.5 86.8±19.7 86.2±18.7 0.768
Body mass index, kg/m2 29.0±6.3 29.0±5.8 29.4±5.9 29.1±5.8 0.666
Heart rate, bpm 74.5±12.9 71.3±11.9 71.4±11.1 70.5±11.5 <0.001
Educational level 0.574
<High school 248/603 (41.1) 235/553 (42.5) 238/530 (44.9) 271/609 (44.5)
High-school graduate or some college 267/603 (44.3) 231/553 (41.8) 213/530 (40.2) 236/609 (38.8)
College graduate or postgraduate 88/603 (14.6) 87/553 (15.7) 79/530 (14.9) 102/609 (16.7)
Systolic blood pressure, mm Hg 120.5±18.2 122.3±18.3 125.5±18.5 127.6±19.5 <0.001
Diastolic blood pressure, mm Hg 74.2±11.3 73.5±11.5 74.2±11.6 74.9±11.4 0.203
NYHA classification 0.135
I 69/599 (11.5) 75/553 (13.6) 78/529 (14.7) 93/609 (15.3)
II 324/599 (54.1) 314/553 (56.8) 289/529 (54.6) 340/609 (55.8)
III 195/599 (32.6) 154/553 (27.8) 158/529 (29.9) 173/609 (28.4)
IV 11/599 (1.8) 10/553 (1.8) 4/529 (0.8) 3/609 (0.5)
Distance covered on 6-min walk, m 353.5±147.5 339.1±146.2 340.4±139.4 369.1±151.5 0.002
Pacemaker or defibrillator 141/603 (23.4) 142/551 (25.8) 132/531 (24.9) 109/610 (17.9) 0.006
Serum creatinine, mg/dL 1.2±0.3 1.2±0.3 1.1±0.3 1.2±0.3 0.677
eGFR, mL/min 69.0±19.9 67.6±20.0 69.5±22.0 67.7±20.6 0.310
Hemoglobin, g/dL 14.1±1.6 14.0±1.6 14.0±1.5 14.1±1.6 0.731
Serum sodium, mEq/L 139.2±6.4 139.4±3.3 139.7±3.3 140.0±3.4 0.015
Medical comorbidities
Diabetes mellitus 182/603 (30.2) 183/551 (33.2) 163/531 (30.7) 194/609 (31.9) 0.699
Hypertension 330/580 (56.9) 300/530 (56.6) 331/520 (63.7) 406/602 (67.4) <0.001
Ischemic cardiomyopathy 254/603 (42.1) 247/550 (44.9) 239/531 (45.0) 251/609 (41.2) 0.453
Myocardial infarction 263/602 (43.7) 276/551 (50.1) 273/531 (51.4) 300/610 (49.2) 0.045
Atrial fibrillation 18/603 (3.0) 25/551 (4.5) 20/531 (3.8) 23/610 (3.8) 0.588
Peripheral vascular disease 55/603 (9.1) 58/559 (10.4) 70/533 (13.1) 78/610 (12.8) 0.092
Previous stroke or TIA 67/603 (11.1) 68/551 (12.3) 73/531 (13.7) 86/610 (14.1) 0.393
Alcohol consumption <0.001
Current consumption, >2 oz/d 141/603 (23.4) 113/555 (20.4) 130/531 (24.5) 188/609 (30.9)
(Continued )
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

4 Stroke August 2016
The incidence of ischemic stroke, primary outcome, and death, also stratified by optimal cutoff point for each out-come, is reported in Figure 1, which also reports the rate ratio for each event. Corresponding information for other outcomes is provided in Figure I in the online-only Data Supplement.
Effect of Antithrombotic TreatmentFigure 2 shows the outcome incidence rates for ischemic stroke, primary outcome, and death by antithrombotic treat-ment (aspirin or warfarin), stratified by LVEF category (for other outcomes, please refer to Figure II in the online-only Data Supplement). Incidence rates were similar between aspirin- and warfarin-treated patients, as already known from the WARCEF main results.4 The deleterious effect of a lower LVEF tended to be stronger in warfarin-treated than in aspirin-treated patients for all 3 outcomes. A trend toward a significant interaction between treatment type and LVEF was noted for ischemic stroke and primary outcome. An
additional analysis by 5% LVEF decrements showed a sig-nificant interaction between LVEF and treatment for isch-emic stroke only, with the warfarin-treated group showing a significantly greater stroke risk per each 5% LVEF decre-ment (adjusted hazard ratio, 1.346; 95% CI, 1.044–1.737; P=0.022) than the aspirin-treated group (adjusted hazard ratio, 0.971; 95% CI, 0.805–1.171; P=0.757; P value for the interaction=0.04).
Because the interaction between LVEF and warfarin on stroke risk might be mediated by differences in TTR, this vari-able was examined in different stroke and LVEF subgroups. TTR was similar in patients with LVEF of <15% or ≥15% (56.5±28.6% versus 57.1±28.5%; P=0.793). TTR tended to be lower in patients who experienced a stroke during follow-up than in those who did not (45.9±27.9% versus 57.2±28.4%; P=0.064); this trend was stronger in patients with LVEF of <15% (36.1±24.1% versus 57.6±28.5%; P=0.074) than in patients with LVEF of ≥15% (49.0±29.0% versus 57.2±28.4%; P=0.249).
Previous consumption, >2 oz/d 148/603 (24.5) 141/555 (25.4) 105/531 (19.8) 112/609 (18.4)
Never consumed alcohol 314/603 (52.1) 301/555 (54.2) 296/531 (55.7) 309/609 (50.7)
Smoking status 0.449
Current smoker 122/602 (20.3) 90/555 (16.2) 93/531 (17.5) 103/608 (16.9)
Former smoker 307/602 (51.0) 295/555 (53.2) 275/531 (51.8) 303/608 (49.8)
Never smoked 173/602 (28.7) 170/555 (30.6) 163/531 (30.7) 202/608 (33.2)
Medications
ACE inhibitor or ARB 593/603 (98.3) 541/551 (98.2) 522/529 (98.7) 601/610 (98.5) 0.922
β-Blocker 538/603 (89.2) 489/551 (88.7) 490/530 (92.5) 545/610 (89.3) 0.163
Aldosterone blocker 231/355 (65.1) 220/333 (66.1) 175/296 (59.1) 187/361 (51.8) <0.001
Nitrate 143/603 (23.7) 122/551 (22.1) 141/530 (26.6) 137/609 (22.5) 0.296
Calcium-channel blocker 38/603 (6.3) 51/550 (9.3) 48/528 (9.1) 66/610 (10.8) 0.047
Diuretic 519/603 (86.1) 446/551 (80.9) 421/530 (79.4) 469/610 (76.9) 0.001
Statin 327/418 (78.2) 340/408 (83.3) 341/397 (85.9) 386/455 (84.8) 0.017
Warfarin 305/603 (50.6) 287/559 (51.3) 261/533 (49.0) 289/610 (47.4) 0.532
Event
Primary outcome 189 (41.7%) 161 (39.3%) 140 (35.1%) 132 (30.3%) 0.011
Ischemic stroke 26 (30.3%) 20 (5.0%) 14 (3.7%) 24 (6.0%) 0.387
Death 162 (37.9%) 139 (35.9%) 124 (32.3%) 106 (25.6%) 0.008
Cardiovascular death 120 (28.8%) 91 (24.5%) 79 (20.8%) 66 (15.9%) 0.001
Sudden death 69 (16.4%) 43 (11.2%) 46 (13.1%) 37 (8.2%) 0.010
Myocardial infarction 21(4.3%) 19 (7.1%) 14 (3.5%) 18 (3.8%) 0.792
Heart failure hospitalization 150 (34.3%) 112 (27.2%) 104 (26.7%) 85 (22.4%) <0.001
ACE indicates angiotensin-converting enzyme; ARB, angiotensin receptor blockers; eGFR, estimated glomerular filtration rate; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; and TIA, transient ischemic attack.
*For continuous variables, mean±SD were reported, and P values were calculated using ANOVA F-test. For categorical variables, no/total no (%) were reported, and P values were calculated using χ2 test. For time-to-event outcomes, no (Kaplan–Meier %) were reported, and P values were calculated using log-rank test.
Table 1. Continued
Covariate LVEF<20% (n=603)LVEF 21%–25%
(n=559)LVEF 26%–29%
(n=533) LVEF≥30% (n=610) P Value
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Di Tullio et al LVEF, Stroke, and Cardiovascular Events in Heart Failure 5
DiscussionThis study evaluates the effect of LVEF on ischemic stroke and other outcome events in HF patients with sinus rhythm and reduced LVEF treated with currently recommended HF medications and randomized to different antithrombotic treatments.
In patients with systolic HF, several hemodynamic vari-ables have been shown to be associated with outcome, some of which easily obtainable such as systolic blood pressure,6–8 pulse pressure,9 and resting heart rate.8,10 However, LVEF is the most widely used clinical indicator of LV systolic func-tion and related risk for cardiovascular events in patients with HF. The results of our study support the presence of a linear, inverse relationship between LVEF and the considered out-come events with the exception of stroke, for which a relation-ship was observed only for low LVEF (<15%) and of MI, for which no relationship was observed. An LVEF of <15% more than doubled the risk of stroke.
Comparison With Previous StudiesThe observation of an inverse relationship between LVEF and death is in agreement with those from previous obser-vational11,12 and more recent, large-scale studies.1,2,13 Among the latter, results from the CHARM trial showed LVEF to be inversely and linearly associated with all-cause mortality and with all components of cardiovascular death for LVEF val-ues <45% over a median follow-up of 38 months.1 The DIG trial also reported similar results.2 Our study provides similar results in a more recently enrolled cohort, but notable differ-ences exist. Our study only included patients with systolic HF, and an LVEF of <35% was an inclusion criterion. However, an LVEF cutoff of 35% was indeed the one associated with increased mortality at 180 days in the recent Acute Studies of Nesiritide in Decompensated Heart Failure (ASCEND-HF) trial, and a linear relationship between decreasing LVEF and risk of death was only observed below that level.13 Compared with the CHARM cohort, the WARCEF cohort had differences
Table 2. LVEF and Outcome Events (By Optimal Cutoff Point of Increased Risk)
Unadjusted Adjusted*
HR (95% CI) P Value HR (95% CI) P Value
LVEF <15% vs ≥15%
Ischemic stroke 2.105 (1.186–3.738) 0.011 2.125 (1.182–3.818) 0.012
LVEF <25% vs ≥25%
Primary outcome 1.266 (1.081–1.484) 0.004 1.250 (1.063–1.469) 0.007
Death 1.288 (1.085–1.529) 0.004 1.252 (1.050–1.492) 0.012
LVEF <20% vs ≥20%
Cardiovascular death 1.481 (1.189–1.845) <0.001 1.359 (1.085–1.702) 0.008
Sudden death 1.593 (1.187–2.136) 0.002 1.481 (1.097–1.999) 0.010
HF hospitalization 1.520 (1.249–1.849) <0.001 1.395 (1.142–1.706) 0.001
BMI indicates body mass index; BP, blood pressure; CI, confidence interval; HF, heart failure; HR, hazard ratio; ICD, intracardiac defibrillator; LVEF, left ventricular ejection fraction; and NYHA, New York Heart Association.
*Adjusted for age, sex, BMI, systolic BP, heart rate, smoking status, education, NYHA class (III, IV vs I, II), diabetes mellitus, hypertension, ischemic cardiomyopathy, previous stroke or TIA, ICD presence, serum creatinine and hemoglobin for primary outcome, death, cardiovascular death and sudden death; adjusted for age, sex, BMI, systolic BP, smoking status, NYHA class (III, IV vs I, II), diabetes mellitus, hypertension, ischemic cardiomyopathy, previous stroke or TIA, ICD presence, serum creatinine and hemoglobin for stroke; adjusted for age, sex, BMI, systolic BP, heart rate, smoking status, alcohol consumption, NYHA class (III, IV vs I, II), diabetes mellitus, hypertension, ischemic cardiomyopathy, previous stroke or TIA, ICD presence, serum creatinine, hemoglobin and sodium for HF hospitalization.
Figure 1. Outcome incidence rates for ischemic stroke, primary outcome, and death by left ventricular ejection fraction (LVEF; dichotomized at optimal cutoff points). CI indicates confidence interval.
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

6 Stroke August 2016
in the medical treatment that reflect the more recent conduct of the study. Patients in WARCEF were more often on β-blockers (>90% of patients versus ≈55%), aldosterone-blockers (60% versus ≈20%), and statins or other lipid-lowering medications (>80% versus ≈40%). The most important difference, how-ever, is that all patients in WARCEF received an antithrom-botic medication per-protocol, which may have affected the relationship between LVEF and thromboembolic events.
Unlike CHARM, which found no association between LVEF and incidence of stroke, we observed an increased stroke risk for extremely low LVEF values (<15%). This dif-ference may reflect the low incidence of stroke in CHARM (slightly >1% over a mean follow-up of ≈3 years). The stroke incidence in WARCEF (slightly >1% per year) is at the lower end of what traditionally reported in the HF literature (1.3%–3.5% per year),14–17 probably reflecting the updated back-ground medical treatment and the per-protocol antithrombotic agents. In the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT), the rate of stroke and other thromboembolic events was 1.7% per year, and lower LVEF was associated with an increased risk of thromboembolic events, with the highest risk observed in patients with LVEF of <20%.3 From this cumulative experience, it seems that LVEF may indeed be associated with stroke risk in patients with systolic HF, but predominantly at very low LVEF levels. The possibility exists that very low LVEF may be associated with more frequent occurrence of undetected episodes of paroxysmal atrial fibril-lation, an established stroke risk factor that might be involved in explaining this finding.
Although CHARM documented a slight but significant increase in risk of MI (adjusted hazard ratio, 1.14; 95% CI, 1.01–1.28 per 10% LVEF reduction <45%), no such increase was observed in WARCEF. Although the low frequency of MI (≈2% in CHARM and 3% in WARCEF in correspond-ing LVEF categories) prevents definitive conclusions, the antithrombotic treatments prescribed in WARCEF may have affected the relationship between LVEF and a predominantly thrombotic outcome such as MI.
Effect of Antithrombotic TreatmentIn the main results of WARCEF, patients on warfarin or aspirin treatment had similar rates of death and primary
outcome, although patients on warfarin treatment had significantly reduced incidence of ischemic stroke.4,5 In the present analysis, lower LVEF tended to have a more deleterious effect in patients treated with warfarin than in patients receiving aspirin with respect to primary outcome, death, and ischemic stroke (Figure 2). The only significant interaction between LVEF and treatment was observed for stroke, where each 5% decrease in LVEF was associ-ated with a 35.6% increase in the adjusted risk of stroke in patients treated with warfarin (P=0.02). Warfarin-treated patients with LVEF of <15% showed an increased stroke rate, whereas those with higher LVEF had low stroke inci-dence, actually lower than that of aspirin-treated patients. The hypothesis that patients with extremely low LVEF might have greater difficulty in maintaining an adequate TTR was not confirmed in our analysis because mean TTR was nearly identical in patients with LVEF of <15% or ≥15%; however, the mean TTR tended to be lower in patients with LVEF of <15% who experienced a stroke than in patients with LVEF of <15% who did not (P=0.074). Taken together, these results suggest that, although main-taining an adequate TTR may not necessarily be more dif-ficult in patients with extremely low LVEF, the stroke risk may increase in them when an adequate TTR is for any reason not achieved. Given the low number of incident strokes, these results should be regarded with a degree of caution; however, particular emphasis should be placed on international normalized ratio control in patients with very low LVEF and switching to another antithrombotic agent considered when international normalized ratio manage-ment proves difficult. The use of newer oral anticoagulants in patients with severely reduced LVEF and sinus rhythm, while an appealing possibility, requires appositely designed and powered clinical trials to assess safety and efficacy of these drugs in this specific clinical setting.
Our study has strengths and limitations. Strengths are the relatively large cohort of patients with HF in sinus rhythm, the central interpretation of echocardiograms and consequent standardization of LVEF measurement, and the ability to investigate the effect of 2 antithrombotic treatments. Among the limitations, the study only included patients with sys-tolic HF; therefore, the effect of LVEF on outcomes within
Figure 2. Outcome incidence rates for ischemic stroke, primary outcome, and death by antithrombotic treatment type, stratified by left ventricular ejection fraction (LVEF) category. BMI indicates body mass index; BP, blood pressure; CI, confidence interval; NYHA, New York Heart Association; and TIA, transient ischemic attack.
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Di Tullio et al LVEF, Stroke, and Cardiovascular Events in Heart Failure 7
a normal or mildly decreased LVEF could not be evaluated. The incidence of some outcomes was rather low; therefore, the related results for subgroup analyses should be considered exploratory.
SummaryIn patients with systolic HF in sinus rhythm treated with currently recommended HF regimen and antithrombotic medications, LVEF is inversely associated with death and its various components, ischemic stroke, and HF hospital-ization, but not MI; the association is linear for most out-comes, but an increased stroke risk is observed only for very low LVEF (<15%); an interaction between LVEF and warfarin treatment may exist on stroke risk, which deserves further investigation.
AcknowledgmentsWe thank Michelle Bierig, RDCS, and Rui Liu, MD, for their help with the echocardiographic measurements.
Sources of FundingThe study was funded by U01-NS-043975 (Dr Homma) and U01-NS-039143 (Dr Thompson) from the National Institute of Neurological Diseases and Stroke (NINDS).
DisclosuresDr Homma reports receiving payment from AGA Medical (now St. Jude Medical) for his work as a member of a data and safety monitoring board and consulting fees from Boehringer Ingelheim. Dr Levin reports receiving consulting fees from United Healthcare. Dr Teerlink reports receiving research grants or consulting fees from Amgen, Bayer, Cardio3 Bioscience, Cytokinetics, Mast Therapeutics, Medtronic, Novartis, St. Jude, and Trevena. Dr Labovitz reports receiving grant support from Boehringer Ingelheim and BMS Pfizer, lecture fees from Boehringer Ingelheim, and fees for the develop-ment of educational presentations from the American College of Cardiology. Dr Anker reports receiving consulting fees from Vifor, Bayer, Janssen, Novartis, Relypsa, ZS-Pharma, and Thermo Fisher; grant support from Vifor Pharma, and Abbott Vascular; and lecture fees from Vifor, Novartis, and Stealth Peptides. Dr Ponikowski reports receiving consulting fees from Bayer, Boehringer Ingelheim, Coridea, Corthera, Johnson & Johnson, Pfizer, Respicardia, and Vifor Pharma; grant support from Vifor Pharma on behalf of him-self and his institution; and lecture fees from Abbott, Boehringer Ingelheim, Merck Serono, Pfizer, Respicardia, Sanofi-Aventis, Servier, and Vifor Pharma. Dr Lip reports receiving consulting fees from Bayer/Janssen, Astellas, Merck, Sanofi, BMS/Pfizer, Biotronik, Medtronic, Portola, Boehringer Ingelheim, Microlife, and Daiichi-Sanky; speakers bureau fees from Bayer, BMS/Pfizer, Medtronic, Boehringer Ingelheim, Microlife, Roche, and Daiichi-Sankyo; and payment for the development of educational presentations from Bayer, Boehringer Ingelheim, and Merck. The other authors report no conflicts.
References 1. Solomon SD, Anavekar N, Skali H, McMurray JJ, Swedberg K,
Yusuf S, et al; Candesartan in Heart Failure Reduction in Mortality (CHARM) Investigators. Influence of ejection fraction on cardiovascu-lar outcomes in a broad spectrum of heart failure patients. Circulation. 2005;112:3738–3744. doi: 10.1161/CIRCULATIONAHA.105.561423.
2. Curtis JP, Sokol SI, Wang Y, Rathore SS, Ko DT, Jadbabaie F, et al. The association of left ventricular ejection fraction, mortality, and cause
of death in stable outpatients with heart failure. J Am Coll Cardiol. 2003;42:736–742.
3. Freudenberger RS, Hellkamp AS, Halperin JL, Poole J, Anderson J, Johnson G, et al; SCD-HeFT Investigators. Risk of thromboembolism in heart failure: an analysis from the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Circulation. 2007;115:2637–2641. doi: 10.1161/CIRCULATIONAHA.106.661397.
4. Homma S, Thompson JL, Pullicino PM, Levin B, Freudenberger RS, Teerlink JR, et al; WARCEF Investigators. Warfarin and aspirin in patients with heart failure and sinus rhythm. N Engl J Med. 2012;366:1859–1869. doi: 10.1056/NEJMoa1202299.
5. Homma S, Thompson JL, Sanford AR, Mann DL, Sacco RL, Levin B, et al; WARCEF Investigators. Benefit of warfarin compared with aspirin in patients with heart failure in sinus rhythm: a subgroup analysis of WARCEF, a randomized controlled trial. Circ Heart Fail. 2013;6:988–997. doi: 10.1161/CIRCHEARTFAILURE.113.000372.
6. Meredith PA, Ostergren J, Anand I, Puu M, Solomon SD, Michelson EL, et al. Clinical outcomes according to baseline blood pressure in patients with a low ejection fraction in the CHARM (Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity) Program. J Am Coll Cardiol. 2008;52:2000–2007. doi: 10.1016/j.jacc.2008.09.011.
7. Ambrosy AP, Vaduganathan M, Mentz RJ, Greene SJ, Subačius H, Konstam MA, et al. Clinical profile and prognostic value of low sys-tolic blood pressure in patients hospitalized for heart failure with reduced ejection fraction: insights from the Efficacy of Vasopressin Antagonism in Heart Failure: Outcome Study with Tolvaptan (EVEREST) trial. Am Heart J. 2013;165:216–225. doi: 10.1016/j.ahj.2012.11.004.
8. Maeder MT, Kaye DM. Differential impact of heart rate and blood pressure on outcome in patients with heart failure with reduced versus preserved left ventricular ejection fraction. Int J Cardiol. 2012;155:249–256. doi: 10.1016/j.ijcard.2010.10.007.
9. Regnault V, Lagrange J, Pizard A, Safar ME, Fay R, Pitt B, et al. Opposite predictive value of pulse pressure and aortic pulse wave velocity on heart failure with reduced left ventricular ejection fraction: insights from an Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) substudy. Hypertension. 2014;63:105–111. doi: 10.1161/HYPERTENSIONAHA.113.02046.
10. Castagno D, Skali H, Takeuchi M, Swedberg K, Yusuf S, Granger CB, et al; CHARM Investigators. Association of heart rate and outcomes in a broad spectrum of patients with chronic heart failure: results from the CHARM (Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity) program. J Am Coll Cardiol. 2012;59:1785–1795. doi: 10.1016/j.jacc.2011.12.044.
11. St John Sutton M, Pfeffer MA, Moye L, Plappert T, Rouleau JL, Lamas G, et al. Cardiovascular death and left ventricular remodeling two years after myocardial infarction: baseline predictors and impact of long-term use of captopril: information from the Survival and Ventricular Enlargement (SAVE) trial. Circulation. 1997;96:3294–3299.
12. McDermott MM, Feinglass J, Lee PI, Mehta S, Schmitt B, Lefevre F, et al. Systolic function, readmission rates, and survival among consecu-tively hospitalized patients with congestive heart failure. Am Heart J. 1997;134:728–736.
13. Toma M, Ezekowitz JA, Bakal JA, O’Connor CM, Hernandez AF, Sardar MR, et al. The relationship between left ventricular ejection frac-tion and mortality in patients with acute heart failure: insights from the ASCEND-HF Trial. Eur J Heart Fail. 2014;16:334–341. doi: 10.1002/ejhf.19.
14. Fuster V, Gersh BJ, Giuliani ER, Tajik AJ, Brandenburg RO, Frye RL. The natural history of idiopathic dilated cardiomyopathy. Am J Cardiol. 1981;47:525–531.
15. Dunkman WB, Johnson GR, Carson PE, Bhat G, Farrell L, Cohn JN. Incidence of thromboembolic events in congestive heart failure. The V-HeFT VA Cooperative Studies Group. Circulation. 1993;87(suppl 6):VI94–V101.
16. Katz SD, Marantz PR, Biasucci L, Jondeau G, Lee K, Brennan C, et al. Low incidence of stroke in ambulatory patients with heart failure: a prospective study. Am Heart J. 1993;126:141–146.
17. Dries DL, Rosenberg YD, Waclawiw MA, Domanski MJ. Ejection frac-tion and risk of thromboembolic events in patients with systolic dysfunc-tion and sinus rhythm: evidence for gender differences in the studies of left ventricular dysfunction trials. J Am Coll Cardiol. 1997;29:1074–1080.
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Dirk J. Lok, Piotr Ponikowski, Stefan D. Anker and Shunichi HommaGraham, Gregory Y.H. Lip, Bruce Levin, J.P. Mohr, Richard Buchsbaum, Conrado J. Estol,
Ralph L. Sacco, Patrick M. Pullicino, Ronald S. Freudenberger, John R. Teerlink, Susan Marco R. Di Tullio, Min Qian, John L.P. Thompson, Arthur J. Labovitz, Douglas L. Mann,Failure: Data From the Warfarin Versus Aspirin in Reduced Ejection Fraction TrialLeft Ventricular Ejection Fraction and Risk of Stroke and Cardiac Events in Heart
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2016 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke published online June 28, 2016;Stroke.
http://stroke.ahajournals.org/content/early/2016/06/28/STROKEAHA.116.013679World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2017/07/10/STROKEAHA.116.013679.DC2 http://stroke.ahajournals.org/content/suppl/2016/06/28/STROKEAHA.116.013679.DC1
Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 19, 2018http://stroke.ahajournals.org/
Dow
nloaded from

SUPPLEMENTAL MATERIAL
Left Ventricular Ejection Fraction and Risk of Stroke and Cardiovascular Events
in Heart Failure: Insights from the WARCEF trial

SUPPLEMENTAL METHODS
Eligibility criteria
Patients in any New York Heart Association (NYHA) functional classes were eligible, but patients
in NYHA class I could account for no more than 20% of the total number of patients undergoing
randomization. Patients who had a clear indication for warfarin or aspirin were not eligible. Patients
were also ineligible if they had a condition that conferred a high risk of cardiac embolism, such as atrial
fibrillation, a mechanical cardiac valve, endocarditis, or an intracardiac mobile or pedunculated
thrombus. Planned treatment with a beta-blocker, an angiotensin-converting–enzyme (ACE) inhibitor or
an angiotensin-receptor blocker (ARB), or hydralazine and nitrates, was also a reason for ineligibility,
whereas current treatment with those medications was allowed.
Study Medication
Patients were randomized to adjusted dose warfarin or aspirin in a double-blind, double-dummy
design in which patients who were assigned to active warfarin received warfarin and placebo aspirin,
and patients assigned to active aspirin received aspirin and placebo warfarin. The statistical analysis
center fabricated clinically plausible INR results for patients in the aspirin group and provided these
results to the sites, along with the actual INR results for the patients in the warfarin group, so that all the
patients were treated as if they were receiving active warfarin.
Definition of outcome events
Stroke was defined as a clinically relevant new lesion detected on computed tomography or MRI
or, in the absence of a new lesion, clinical findings that were consistent with the occurrence of clinical
stroke and that lasted for longer than 24 hours.
The diagnosis of MI based was based on two of the following: 1) Typical cardiac pain or its
equivalent; 2) ECG evidence of acute MI; 3) Cardiac biomarkers indicative of acute MI.
Sudden death was defined as: 1) death witnessed and noted to occur instantaneously or within
15 minutes of observed collapse or new cardiac symptoms, without preceding circulatory failure (shock,
pulmonary edema, refractory NYHA class IV CHF) or other modes of death, or 2) death unwitnessed, but
known to have occurred in the absence of pre-existing circulatory failure or other modes of death within
an observation period of 72 hours, or 3) patient resuscitated from cardiac arrest in the absence of pre-
existing circulatory failure or other modes of death and died within 24 hours or prior to discharge if
neurologic function was not restored.
Cardiovascular death included sudden death; documented ventricular tachycardia or fibrillation;
documented bradyarrhythmia; MI; and circulatory failure.
Hospitalizations for heart failure during the follow-up were defined as admissions with the
following features: typical symptoms; IV diuretics, vasodilator or inotropic therapy; at least 24-hour
hospital stay.

SUPPLEMENTAL TABLES
Supplemental Table I – Association of demographic and clinical variables with primary outcome (death, stroke
or intracerebral hemorrhage). Univariable and multivariable Cox models
covariate For an increase of
Univariable model Multivariable model
HR (95% CI) p-value HR (95% CI) p-value
Ejection fraction, % 1 0.982 (0.971,0.992) 0.001 0.984
(0.974, 0.995)
0.005
Age-yr 1 1.027 (1.020,1.035) <0.001 1.020
(1.011, 1.028)
<0.001
Male sex 1.348 (1.089,1.668) 0.006 1.394
(1.108, 1.754)
0.005
Body-mass index 1 0.966 (0.952,0.980) <0.001 0.972
(0.957, 0.988)
<0.001
Systolic blood
pressure, mmHg
1 0.994 (0.990,0.998) 0.006 0.995
(0.991, 1.000)
0.048
Heart rate -
beats/min
1 1.008 (1.001,1.014) 0.021 1.011
(1.005, 1.018)
0.001
Smoking status ref: Never smoked 0.043 0.441
. Current smoker 1.133 (0.889,1.445) . 1.130
(0.876, 1.459)
0.347
. Former smoker 1.266 (1.051,1.525) . 1.129
(0.931, 1.371)
0.218
educational level ref: < High school 0.027 0.147
. High-school
graduate or some
college
0.908 (0.766,1.075) . 0.948
(0.798, 1.126)
0.543
. College graduate or
postgraduate
0.716 (0.561,0.915) . 0.780
(0.609, 1.000)
0.050
NYHA class III or IV 1.554 (1.323,1.825) <0.001 1.421
(1.203, 1.678)
<0.001
Diabetes Mellitus 1.486 (1.265,1.745) <0.001 1.295
(1.088, 1.541)
0.004
Hypertension 0.991 (0.843,1.165) 0.912 0.917
(0.772, 1.091)
0.329
Ischemic
Cardiomyopathy
1.621 (1.385,1.898) <0.001 1.392
(1.180, 1.643)
<0.001

covariate For an increase of
Univariable model Multivariable model
HR (95% CI) p-value HR (95% CI) p-value
Prior stroke or TIA yes vs. no 1.402 (1.133,1.735) 0.002 1.298
(1.045, 1.613)
0.018
Pacemaker or
defibrillator
0.838 (0.685,1.024) 0.083 0.710
(0.578, 0.872)
0.001
creatinine - mg/dL 1 2.255 (1.830,2.778) <0.001 1.637
(1.297, 2.065)
<0.001
hemoglobin - g/dL 1 0.873 (0.827,0.921) <0.001 0.916
(0.864, 0.971)
0.003
HR = Hazard Ratio
CI = Confidence Interval

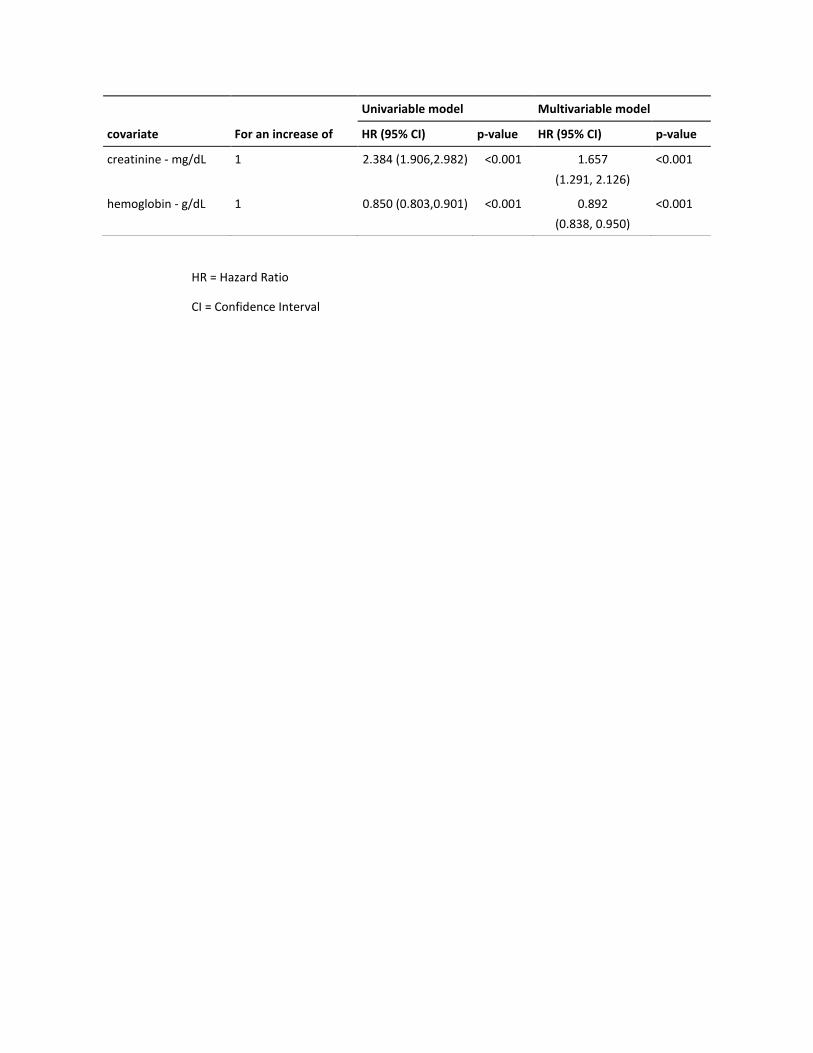
Supplemental Table II – Demographics and clinical variables associated with death from any cause in the study
cohort
covariate For an increase of
Univariable model Multivariable model
HR (95% CI) p-value HR (95% CI) p-value
Ejection fraction % 1 0.981 (0.969,0.992) 0.001 0.985
(0.973, 0.996)
0.011
Age-yr 1 1.030 (1.022,1.038) <0.001 1.023 (1.013, 1.032) <0.001
Male sex 1.413 (1.118,1.786) 0.004 1.495
(1.162, 1.922)
0.002
Body-mass index 1 0.964 (0.949,0.980) <0.001 0.971
(0.954, 0.988)
0.001
Systolic blood
pressure, mmHg
1 0.993 (0.988,0.998) 0.003 0.995
(0.989, 1.000)
0.040
pulse - beats/min 1 1.010 (1.003,1.017) 0.006 1.014
(1.007, 1.022)
<0.001
Smoking status ref: Never smoked 0.027 0.361
. Current smoker 1.181 (0.907,1.537) . 1.180
(0.894, 1.557)
0.242
. Former smoker 1.320 (1.077,1.618) . 1.153
(0.933, 1.424)
0.188
educational level ref: < High school 0.004 0.033
. High-school graduate
or some college
0.889 (0.741,1.066) . 0.935
(0.777, 1.125)
0.477
College graduate or
postgraduate
0.629 (0.478,0.828) . 0.691
(0.523, 0.913)
0.009
NYHA class III or IV 1.642 (1.380,1.952) <0.001 1.484
(1.240, 1.775)
<0.001
Diabetes Mellitus 1.508 (1.267,1.794) <0.001 1.292
(1.071, 1.559)
0.007
Hypertension 0.991 (0.832,1.180) 0.920 0.925
(0.767, 1.116)
0.416
Ischemic
Cardiomyopathy
1.681 (1.417,1.993) <0.001 1.419
(1.186, 1.698)
<0.001
Prior stroke or TIA 1.136 (0.886,1.456) 0.315 1.046
(0.813, 1.347)
0.725
Pacemaker or
defibrillator
0.875 (0.706,1.084) 0.223 0.723
(0.581, 0.901)
0.004
covariate For an increase of
Univariable model Multivariable model
HR (95% CI) p-value HR (95% CI) p-value
creatinine - mg/dL 1 2.384 (1.906,2.982) <0.001 1.657
(1.291, 2.126)
<0.001
hemoglobin - g/dL 1 0.850 (0.803,0.901) <0.001 0.892
(0.838, 0.950)
<0.001
HR = Hazard Ratio
CI = Confidence Interval

Supplemental Table III – Demographics and clinical variables associated with ischemic stroke in the study cohort
covariate
For an increase
of
Univariable model Multivariable model
HR (95% CI) p-value HR (95% CI) p-value
Ejection fraction <15% 2.105
(1.186,3.738)
0.011 2.125 (1.182,
3.818)
0.012
Age-yr 1 1.008
(0.988,1.027)
0.442 1.002 (0.981,
1.023)
0.876
Male sex 0.947
(0.562,1.594)
0.836 0.830 (0.466,
1.476)
0.525
Body-mass index 1 0.979
(0.943,1.017)
0.281 0.983 (0.943,
1.026)
0.436
Systolic blood pressure,
mmHg
1 1.000
(0.988,1.011)
0.968 0.999 (0.987,
1.011)
0.870
Smoking status ref: never
smoked
0.992 0.965
. Current smoker 0.975
(0.516,1.841)
. 0.924 (0.474,
1.800)
0.817
. Former smoker 0.970
(0.596,1.579)
. 1.001 (0.606,
1.655)
0.997
NYHA class III or IV 1.125
(0.712,1.778)
0.615 1.003 (0.626,
1.606)
0.990
Diabetes Mellitus 1.337
(0.858,2.082)
0.199 1.297 (0.801,
2.101)
0.290
Hypertension 1.006
(0.648,1.563)
0.978 0.883 (0.551,
1.418)
0.607
Ischemic Cardiomyopathy 1.157
(0.752,1.781)
0.507 1.140 (0.722,
1.800)
0.574
Prior stroke or TIA 3.381
(2.139,5.345)
<0.001 3.290 (2.056,
5.263)
<0.001
Pacemaker or
defibrillator
0.583
(0.316,1.075)
0.084 0.570 (0.307,
1.059)
0.075
creatinine - mg/dL 1 1.657
(0.908,3.026)
0.100 1.638 (0.863,
3.111)
0.132
hemoglobin - g/dL 1 1.037
(0.891,1.207)
0.638 1.098 (0.931,
1.295)
0.268

Supplemental Table IV – LVEF and outcomes: cutoff points of increased risk
Unadjusted Adjusted*
HR (95% CI) p-value HR (95% CI) p-value
Primary outcome
EF < 15% vs. EF≥15% 1.395 (1.090,1.787) 0.008 1.247 (0.969, 1.606) 0.087
EF < 20% vs. EF≥20% 1.274 (1.074,1.511) 0.006 1.242 (1.043, 1.480) 0.015
EF < 25% vs. EF≥25% 1.266 (1.081,1.484) 0.004 1.250 (1.063, 1.469) 0.007
EF < 30% vs. EF≥30% 1.269 (1.047,1.538) 0.015 1.231 (1.014, 1.496) 0.036
Death
EF < 15% vs. EF≥15% 1.284 (0.973,1.694) 0.077 1.113 (0.838, 1.477) 0.460
EF < 20% vs. EF≥20% 1.282 (1.066,1.543) 0.008 1.223 (1.012, 1.479) 0.037
EF < 25% vs. EF≥25% 1.288 (1.085,1.529) 0.004 1.252 (1.050, 1.492) 0.012
EF < 30% vs. EF≥30% 1.366 (1.104,1.690) 0.004 1.310 (1.056, 1.625) 0.014
CV death
EF < 15% vs. EF≥15% 1.324 (0.949,1.847) 0.098 1.102 (0.784, 1.547) 0.577
EF < 20% vs. EF≥20% 1.481 (1.189,1.845) <0.001 1.359 (1.085, 1.702) 0.008
EF < 25% vs. EF≥25% 1.432 (1.159,1.769) 0.001 1.337 (1.077, 1.660) 0.008
EF < 30% vs. EF≥30% 1.503 (1.151,1.964) 0.003 1.387 (1.058, 1.818) 0.018
Sudden death
EF < 15% vs. EF≥15% 1.420 (0.919,2.195) 0.114 1.257 (0.806, 1.960) 0.314
EF < 20% vs. EF≥20% 1.593 (1.187,2.136) 0.002 1.481 (1.097, 1.999) 0.010
EF < 25% vs. EF≥25% 1.328 (1.000,1.764) 0.050 1.273 (0.953, 1.700) 0.102
EF < 30% vs. EF≥30% 1.472 (1.029,2.106) 0.034 1.395 (0.972, 2.004) 0.071
Stroke
EF < 15% vs. EF≥15% 2.105 (1.186,3.738) 0.011 2.125 (1.182, 3.818) 0.012
EF < 20% vs. EF≥20% 1.302 (0.820,2.067) 0.264 1.388 (0.868, 2.220) 0.170
EF < 25% vs. EF≥25% 1.190 (0.775,1.829) 0.427 1.238 (0.800, 1.915) 0.337
EF < 30% vs. EF≥30% 0.868 (0.540,1.393) 0.556 0.879 (0.543, 1.422) 0.599
MI
EF < 15% vs. EF≥15% 0.766 (0.309,1.900) 0.565 0.753 (0.302, 1.879) 0.543
EF < 20% vs. EF≥20% 1.192 (0.717,1.981) 0.499 1.243 (0.743, 2.082) 0.407
EF < 25% vs. EF≥25% 1.232 (0.774,1.961) 0.380 1.305 (0.815, 2.092) 0.268
EF < 30% vs. EF≥30% 1.040 (0.610,1.772) 0.887 1.083 (0.630, 1.859) 0.773
HF hospitalization (1st
event)
EF < 15% vs. EF≥15% 1.337 (0.993,1.798) 0.055 1.139 (0.841, 1.544) 0.400
EF < 20% vs. EF≥20% 1.520 (1.249,1.849) <0.001 1.395 (1.142, 1.706) 0.001

Unadjusted Adjusted*
HR (95% CI) p-value HR (95% CI) p-value
EF < 25% vs. EF≥25% 1.413 (1.172,1.704) <0.001 1.277 (1.054, 1.546) 0.012
EF < 30% vs. EF≥30% 1.551 (1.225,1.964) <0.001 1.380 (1.086, 1.753) 0.008
* adjusted for age, gender, BMI, systolic BP, heart rate, smoking status, education, NYHA class (III, IV vs. I, II),
diabetes, hypertension, ischemic cardiomyopathy, prior stroke or TIA, device, creatinine and hemoglobin for
primary outcome, death, CV death and sudden death; adjusted for age, gender, BMI, systolic BP, smoking
status, NYHA class (III, IV vs. I, II), diabetes, hypertension, ischemic cardiomyopathy, prior stroke or TIA,
device, creatinine and hemoglobin for stroke, and MI; adjusted for age, gender, BMI, systolic BP, heart rate,
smoking status, alcohol consumption, NYHA class (III, IV vs. I, II), diabetes, hypertension, ischemic
cardiomyopathy, prior stroke or TIA, device, creatinine, hemoglobin and sodium for HF hospitalization.

SUPPLEMENTAL FIGURES
Supplemental Figure I
* From Poisson regression.
No LVEF cutoff of increased risk was identified for MI

Supplemental Figure II
* From Cox models, adjusted for age, gender, BMI, systolic BP, heart rate, smoking status, education, NYHA
class (III, IV vs. I, II), diabetes, hypertension, ischemic cardiomyopathy, prior stroke or TIA, ICD presence,
serum creatinine and hemoglobin for CV death and sudden death; adjusted for age, gender, BMI, systolic
BP, heart rate, smoking status, alcohol consumption, NYHA class (III, IV vs. I, II), diabetes, hypertension,
ischemic cardiomyopathy, prior stroke or TIA, ICD presence, serum creatinine, hemoglobin and sodium for
HF hospitalization.

iris
18 Stroke日本語版Vol. 11, No. 4
左室駆出率と心不全患者の脳卒中および心イベントのリスクWarfarin Versus Aspirin in Reduced Ejection Fraction (WARCEF) Trial データLeft Ventricular Ejection Fraction and Risk of Stroke and Cardiac Events in Heart FailureData From the Warfarin Versus Aspirin in Reduced Ejection Fraction Trial
Marco R. Di Tullio, MD1; Min Qian, PhD2; John L.P. Thompson, PhD2, et al.1 Division of Cardiology, Department of Medicine, 2 Department of Biostatistics, Mailman School of Public Health, Columbia University Medical Center, New York
Stroke. 2016; 47: 2031-2037. DOI: 10.1161/STROKEAHA.116.013679.
背景および目的:左室駆出率(LVEF)は心不全(HF)における死亡および心血管の転帰と逆相関する。抗血栓治療の影響と同様,LVEFと脳卒中との関連についても議論がある。本研究では,HF患者におけるLVEFと脳卒中および心血管イベントの関連性,および 2種類の抗血栓薬の影響を検討した。方法:WarfarinVersusAspirininReducedEjectionFraction(WARCEF)試験において収縮期HF(LVEF≦ 35%)で洞調律の患者2,305例をワルファリン投与群またはアスピリン投与群に無作為に割り付け,3.5±1.8年間追跡調査した。主要評価項目(死亡,脳卒中,脳内出血)に関して群間差は認めなかったが,ワルファリンは脳卒中リスクを低下させた。本報告では,LVEFおよび治療法の異なるサブグループ間における脳卒中および心血管イベントの発生率を比較する。結果:ベースラインのLVEFは,主要評価項目,死亡および死亡の内訳(突然死,心血管死),HFによる入院に
対して線形の逆相関を示したが,心筋梗塞との相関は示されなかった。脳卒中との関連はLVEF15%未満の場合にのみ認められ(発生率:2.04vs.0.95/100 患者年,P =0.009),調整済みの脳卒中リスクは 2倍を超えた[調整ハザード比 2.125,95%信頼区間(CI):1.182 ~ 3.818,P= 0.012]。ワルファリン投与患者ではLVEFが 5%低下するごとに脳卒中リスクが有意に増加した(調整ハザード比 1.346,95 % CI:1.044 ~ 1.737,P = 0.022,Pvalueforinteraction = 0.04)。結論:収縮期HFで洞調律の患者においてLVEFは死亡および死亡の内訳と逆相関するが,脳卒中との相関はLVEF値が著しく低い場合にのみ認められる。脳卒中リスクに対するワルファリン投与の交互作用は存在すると考えられる。臨床試験登録情報:URL:http://www.clinicaltrials.gov. 固有の識別番号:NCT00041938。
Abstract
図 2
左 室 駆 出 率(LVEF)によって層別化した抗血栓薬の種類別の虚血性脳卒中,主要評価項目,死亡の転帰 発 生 率。BMI:肥 満 指 数,BP:血圧,CI:信頼区間,NYHA:ニューヨ ー ク 心 臓 協 会
(New York Heart Association) ,TIA:一過性脳虚血発作。
虚血性脳卒中ワルファリンアスピリン
EF<15%8/110 (2.34)6/109 (1.74)
EF≥15%21/1032 (0.57)49/1054 (1.33)
ワルファリンアスピリン
死亡 EF<25%162/592 (7.72)139/570 (7.04)
EF≥25%106/550 (5.45)124/593 (6.02)
主要評価項目ワルファリンアスピリン
EF<25%183/592 (8.72)167/570 (8.46)
EF>25%119/550 (6.12)153/593 (7.43)
患者数/合計数(100患者年あたりの発生率) サブグループ内
0 1 2 3 4 5 6 7 8 9
0.0010.494
0.078
0.145
0.070
0.0050.421
0.0010.451
交互作用値* Pハザード比 (95%CI)
*Coxモデルより。脳卒中については年齢,性別,BMI,収縮期血圧,喫煙状況,NYHA分類 (III, IV vs. I,II),糖尿病,高血圧,脳卒中またはTIAの既往,ICD,クレアチニンおよびヘモグロビンで調整。主要評価項目および死亡については年齢,性別,BMI,収縮期血圧,心拍数,喫煙状況,教育,NYHA分類(III,IV vs. I, II),糖尿病,高血圧,虚血性心筋症,脳卒中またはTIAの既往,デバイス,クレアチニンおよびヘモグロビンで調整。