comparison of magnetic resonance angiography,...
TRANSCRIPT
341
Comparison of Magnetic ResonanceAngiography, Conventional Angiography,
and Duplex Scanning
Thomas S. Riles, MD; Elizabeth M. Eidelman, MD; Andrew W. Litt, MD;Richard S. Pinto, MD; Frances Oldford, RN; and G.W.S. Thoe Schwartzenberg, MD
Background and Purpose: To determine the accuracy of magnetic resonance angiography in assessingpatients with cerebrovascular disease, we performed a study comparing the results of conventionalcerebral angiography, duplex scanning, and magnetic resonance angiography.
Methods: From 42 patients, a total of 25 carotid arteries were evaluated by all three techniques. Thestudies were independently read and sorted into five categories according to the degree of stenosis: 0-15%,normal; 16-49%, mild; 50-79%, moderate; 80-99%, severe; and totally occluded.
Results: Magnetic resonance angiography correlated exactly with conventional angiography in 39arteries (52%); duplex scanning correlated with conventional angiography in 49 cases (65%). Comparedwith conventional angiography, both magnetic resonance angiography and duplex scanning tended tooverread the degree of stenosis. The most critical errors associated with magnetic resonance angiographywere three readings of total occlusion in vessels found to be patent on conventional angiograms.
Conclusions: Although magnetic resonance angiography offers great hope of providing high-qualityimaging of the carotid artery with no risk and at less cost, data from this study suggest that misreadingthe degree of stenosis, or misinterpreting a stenosis for an occlusion, could lead to errors in clinicaldecisions. Guidelines for use of magnetic resonance angiography in a clinical setting are offered. (S • >ke1992;23:341-346)
KEY WORDScomputed
angiography • carotid artery diseases • endarterectomy • tomography, x-ray
Magnetic resonance angiography is a relativelynew, noninvasive technique of imaging theextracranial carotid arteries. Its high-quality
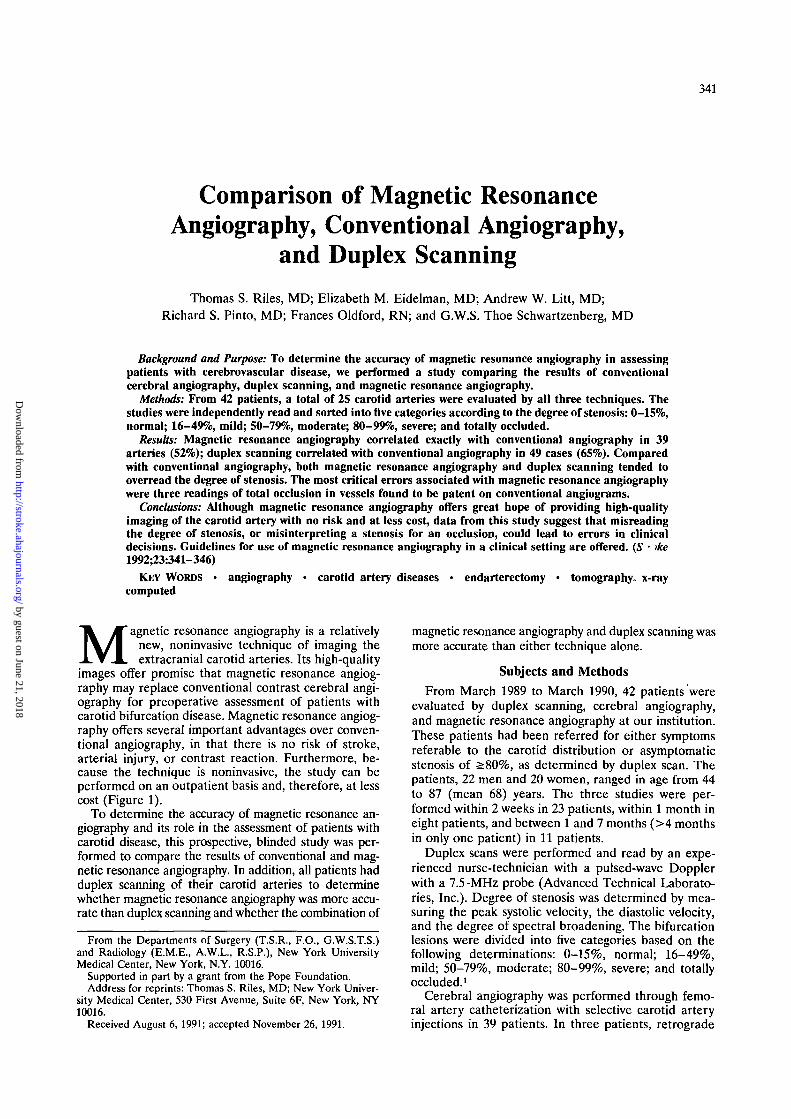
images offer promise that magnetic resonance angiog-raphy may replace conventional contrast cerebral angi-ography for preoperative assessment of patients withcarotid bifurcation disease. Magnetic resonance angiog-raphy offers several important advantages over conven-tional angiography, in that there is no risk of stroke,arterial injury, or contrast reaction. Furthermore, be-cause the technique is noninvasive, the study can beperformed on an outpatient basis and, therefore, at lesscost (Figure 1).
To determine the accuracy of magnetic resonance an-giography and its role in the assessment of patients withcarotid disease, this prospective, blinded study was per-formed to compare the results of conventional and mag-netic resonance angiography. In addition, all patients hadduplex scanning of their carotid arteries to determinewhether magnetic resonance angiography was more accu-rate than duplex scanning and whether the combination of
From the Departments of Surgery (T.S.R., F.O., G.W.S.T.S.)and Radiology (E.M.E., A.W.L., R.S.P.), N e w York UniversityMedical Center, New York, N.Y. 10016.
Supported in part by a grant from the Pope Foundation.Address for reprints: Thomas S. Riles, MD; New York Univer-
sity Medical Center, 530 First Avenue, Suite 6F, New York, NY10016.
Received August 6, 1991; accepted November 26, 1991.
magnetic resonance angiography and duplex scanning wasmore accurate than either technique alone.
Subjects and Methods
From March 1989 to March 1990, 42 patients wereevaluated by duplex scanning, cerebral angiography,and magnetic resonance angiography at our institution.These patients had been referred for either symptomsreferable to the carotid distribution or asymptomaticstenosis of >80%, as determined by duplex scan. Thepatients, 22 men and 20 women, ranged in age from 44to 87 (mean 68) years. The three studies were per-formed within 2 weeks in 23 patients, within 1 month ineight patients, and between 1 and 7 months (>4 monthsin only one patient) in 11 patients.
Duplex scans were performed and read by an expe-rienced nurse-technician with a pulsed-wave Dopplerwith a 7.5-MHz probe (Advanced Technical Laborato-ries, Inc.). Degree of stenosis was determined by mea-suring the peak systolic velocity, the diastolic velocity,and the degree of spectral broadening. The bifurcationlesions were divided into five categories based on thefollowing determinations: 0-15%, normal; 16-49%,mild; 50-79%, moderate; 80-99%, severe; and totallyoccluded.1
Cerebral angiography was performed through femo-ral artery catheterization with selective carotid arteryinjections in 39 patients. In three patients, retrograde
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from
342 Stroke Vol 23, No 3 March 1992
FIGURE 1. Comparison of images of the carotid bifurcation in a patient with severe (80-99%) stenosis. Left panel: Conventionalcerebral angiogram. Right panel: Resonance angiogram.
right brachial injections were performed, assessing onlythe right carotid and vertebral. Biplane views of thecarotids were obtained using either film-screen or digi-tal subtraction technique. The region of stenosis wasmeasured on the view that showed it to be most severe.The percent diameter reduction was calculated usingthe formula [1 —(diameter of vessel at lesion/diameterof outflow vessel)] x 100. After calculating the percentstenosis, we assigned vessels to one of the five categoriesidentical to those used for the duplex scans.
Magnetic resonance angiograms were performed on a1.5-T Philips Gyroscan S15 with 10 mT/m gradients anda standard head/neck coil. The images were obtainedusing a two-dimensional time-of-flight technique de-scribed by Keller et al.2 These images, seen in 16different views, were viewed on film as well as on acomputer console, permitting the viewer to see them ina three-dimensional fashion. The estimate of the sever-ity of stenosis was made by experienced neuroradiolo-gists using the same categories as those for duplex scansand contrast arteriograms. The three studies were ini-tially read independently by separate teams. A finalreview by the combined teams was required for severalproblem cases. At the final review, however, the observ-ers were focused on the specific study and were notaware of the results of the other two studies on the samepatient.
Thirty-four patients eventually underwent carotid sur-gery. Thirty-two patients had carotid endarterectomy, onehad a carotid-to-subclavian bypass for subclavian arterystenosis, and one had a common carotid aneurysmectomy.There were no major operative complications. There werethree complications attributable to angiography: twostrokes and one transient ischemic attack.
ResultsOf the 42 patients studied, three had retrograde right
brachial angiograms resulting in visualization of only theright carotid arteries. One conventional angiogramcould not be measured on either side for technicalreasons. In one patient, internal carotid artery occlusionoccurred before all three studies could be performed.Three patients had unilateral carotid endarterectomiesbefore magnetic resonance angiography was performed.In all, complete studies were available for both carotidarteries in 34 patients and only one carotid artery inseven patients, which left a total of 75 carotid arteriesavailable for review.
Based on the measurements of the conventionalcontrast angiograms, six bifurcations had 0-15% steno-sis, 19 had 16-49% stenosis, 25 had 50-79% stenosis, 20had 80-99% stenosis, and five were totally occluded.
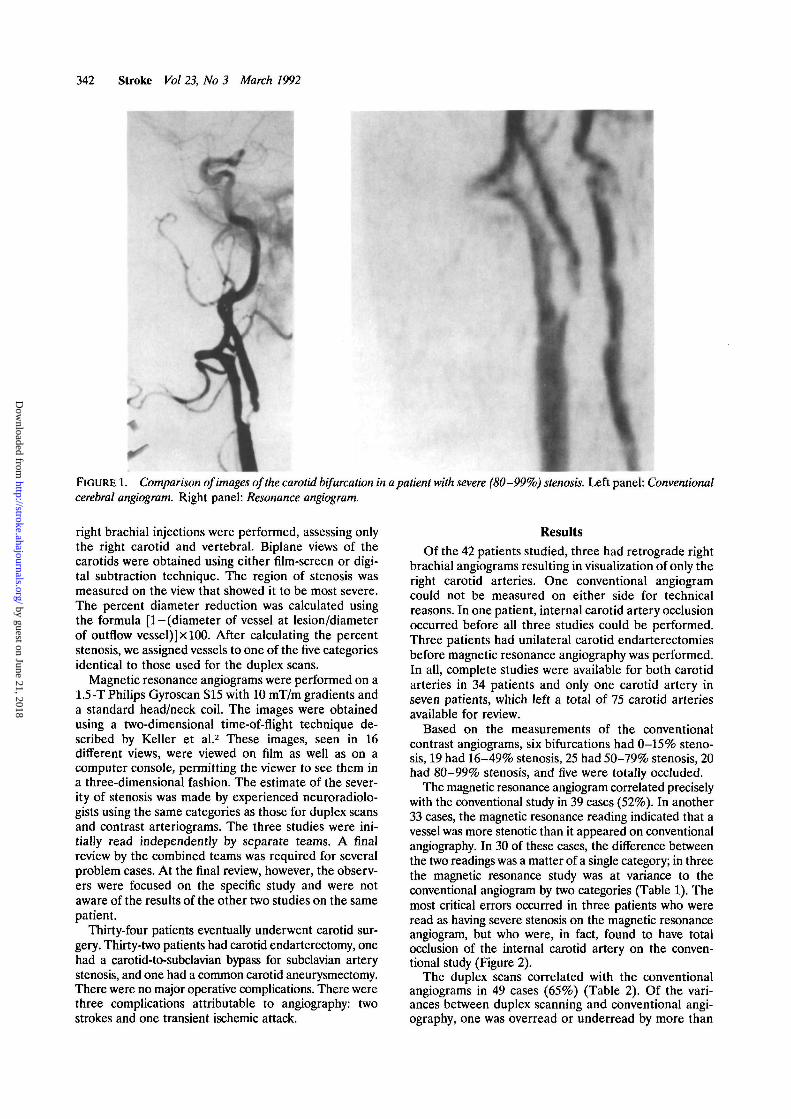
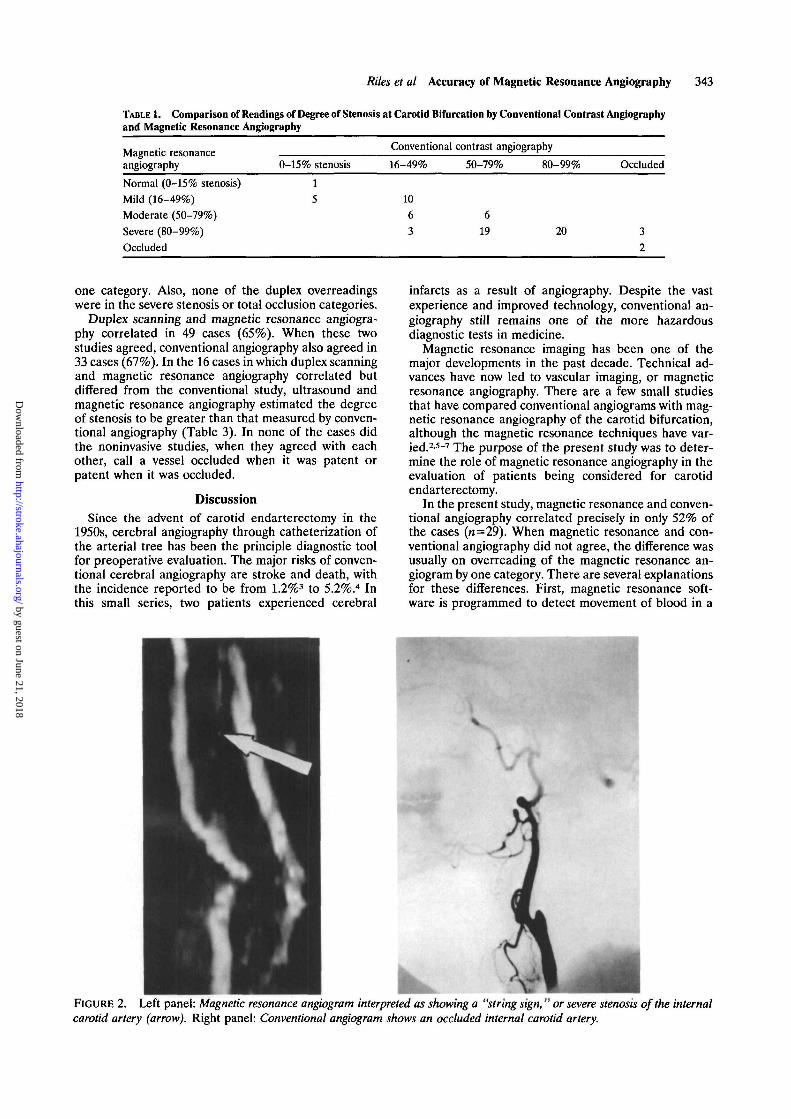
The magnetic resonance angiogram correlated preciselywith the conventional study in 39 cases (52%). In another33 cases, the magnetic resonance reading indicated that avessel was more stenotic than it appeared on conventionalangiography. In 30 of these cases, the difference betweenthe two readings was a matter of a single category; in threethe magnetic resonance study was at variance to theconventional angiogram by two categories (Table 1). Themost critical errors occurred in three patients who wereread as having severe stenosis on the magnetic resonanceangiogram, but who were, in fact, found to have totalocclusion of the internal carotid artery on the conven-tional study (Figure 2).
The duplex scans correlated with the conventionalangiograms in 49 cases (65%) (Table 2). Of the vari-ances between duplex scanning and conventional angi-ography, one was overread or underread by more than
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Riles et al Accuracy of Magnetic Resonance Angiography 343
TABLE 1. Comparison of Readings of Degree of Stenosis at Carotid Bifurcation by Conventional Contrast Angiographyand Magnetic Resonance Angiography
Magnetic resonanceangiography
Conventional contrast angiography
0-15% stenosis 16-49% 50-79% 80-99% Occluded
Normal (0-15% stenosis)Mild (16-49%)Moderate (50-79%)Severe (80-99%)Occluded
1
5 10
63
619
one category. Also, none of the duplex overreadingswere in the severe stenosis or total occlusion categories.
Duplex scanning and magnetic resonance angiogra-phy correlated in 49 cases (65%). When these twostudies agreed, conventional angiography also agreed in33 cases (67%). In the 16 cases in which duplex scanningand magnetic resonance angiography correlated butdiffered from the conventional study, ultrasound andmagnetic resonance angiography estimated the degreeof stenosis to be greater than that measured by conven-tional angiography (Table 3). In none of the cases didthe noninvasive studies, when they agreed with eachother, call a vessel occluded when it was patent orpatent when it was occluded.
DiscussionSince the advent of carotid endarterectomy in the
1950s, cerebral angiography through catheterization ofthe arterial tree has been the principle diagnostic toolfor preoperative evaluation. The major risks of conven-tional cerebral angiography are stroke and death, withthe incidence reported to be from 1.2%3 to 5.2%.4 Inthis small series, two patients experienced cerebral
infarcts as a result of angiography. Despite the vastexperience and improved technology, conventional an-giography still remains one of the more hazardousdiagnostic tests in medicine.
Magnetic resonance imaging has been one of themajor developments in the past decade. Technical ad-vances have now led to vascular imaging, or magneticresonance angiography. There are a few small studiesthat have compared conventional angiograms with mag-netic resonance angiography of the carotid bifurcation,although the magnetic resonance techniques have var-ied.2'5-7 The purpose of the present study was to deter-mine the role of magnetic resonance angiography in theevaluation of patients being considered for carotidendarterectomy.
In the present study, magnetic resonance and conven-tional angiography correlated precisely in only 52% ofthe cases (n=29). When magnetic resonance and con-ventional angiography did not agree, the difference wasusually on overreading of the magnetic resonance an-giogram by one category. There are several explanationsfor these differences. First, magnetic resonance soft-ware is programmed to detect movement of blood in a
FIGURE 2. Left panel: Magnetic resonance angiogram interpreted as showing a "string sign," or severe stenosis of the internalcarotid artery (arrow). Right panel: Conventional angiogram shows an occluded internal carotid artery.
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

344 Stroke Vol 23, No 3 March 1992
TABLE 2. Comparison of Readings of Degree of Stenosis at Carotid Bifurcation by Conventional Contrast Angiographyand Duplex Scan
Duplex scanning andmagnetic resonanceangiography agree
Conventional contrast angiography
0-15% stenosis 16-49% 50-79% 80-99% Occluded
Normal (0-15% stenosis)Mild (16-49%)Moderate (50-79%)Severe (80-99%)Occluded
611 17
specific direction and at a specific range in velocity. Asthe blood passes through an area of stenosis, there is achange in velocity and vector. As a result, some of theblood, particularly in regions of severe stenosis, is notimaged, giving the appearance of stenosis more severethan that which actually exists.
Another potential source of error is in the method ofmeasuring the degree of stenosis on the contrast angio-gram. We performed our measurements as recom-mended by Baker et al.8 Because the bulb is generallylarger than the more distal internal carotid artery,considerably more plaque is usually present than esti-mated when one measures only the residual lumen.Moreover, the categorization of stenosis on the mag-netic resonance angiograms were based on an estimateof the normal luminal diameter including the bulb, thusincreasing the amount of "stenosis" compared with thedistal vessel measured on the contrast study. Finally, asacknowledged by Baker et al,8 it is impossible to achieveexact correlations when comparing anatomic measure-ments to physiological measurements of stenosis. To acertain extent, the magnetic resonance images are de-rived from the physiology of the blood flow through thecarotid artery. The duplex scan measurements arebased entirely on physiology rather than on directanatomic measurement.
The most critical interpretation errors in this studyoccurred in three cases in which the magnetic resonanceangiogram led to the diagnosis of severe stenosis of theinternal carotid artery, although the conventional studyshowed total occlusion. Surgeons and neurologists gen-erally do not advise surgery if the internal carotid arteryis totally occluded. In the present study, had the deci-sion for surgery been based solely on magnetic reso-nance readings, the surgeon would have been expectingin these three cases to find a high-grade stenosis butinstead would have found a vessel unsuitable for recon-struction. Surgery was not performed on these patientsbecause of the conventional angiographic findings.
To a lesser degree, the magnetic resonance angiog-raphy-based diagnoses in 19 patients of 80-99% steno-sis, but which were found to be 50-79% stenosis bycontrast study, were misreadings that may have mis-guided our clinical decisions. If the patient has focalneurological symptoms of the ipsilateral hemisphere,the difference in interpretation is not of great conse-quence; surgery would be advised in either case. In ourpractice, if the patient is asymptomatic, accurate mea-surement of the degree of stenosis is of greater impor-tance in deciding whether surgery is worthwhile. Basedon the natural history studies of asymptomatic steno-sis,9-11 we have advised prophylactic carotid endarter-ectomy for patients with >80% reduction in the diam-eter of the internal carotid bifurcation. In this study,had magnetic resonance angiography rather than con-ventional contrast angiography been used as the onlydiagnostic test for patient selection, it is likely that moreasymptomatic patients would have undergone surgery.
Compared to the magnetic resonance angiograms,the duplex scans had a higher percentage of correlationswith the conventional angiograms than did the magneticresonance studies (65% versus 52%). Eleven patientsjudged to have 80-99% stenosis on duplex had, in fact,only moderate stenosis. Three patients with moderatestenosis on the duplex scan had severe stenosis on thecontrast angiogram. As previously discussed, these 14misreadings in the moderate-to-severe categories are ofimportance mainly in the selection of patients forsurgery if they are asymptomatic. There was no instancein which duplex scanning failed to distinguish between atotal occlusion and a severe stenosis.
The use of duplex scanning as the sole diagnostic testfor the selection of patients for carotid surgery has beenwidely discussed.12-15 Although it may be argued that nocritical errors would have occurred had decisions beenbased on duplex scanning alone, we continue to havereservations regarding this practice. Recent data fromthe Asymptomatic Carotid Artery Stenosis Study16 con-
TABLE 3. Comparison of Readings of Bifurcation Stenosis by Noninvasive Tests With Those of Conventional ContrastAngiography in Cases in Which Duplex Scan Agreed With Magnetic Resonance Angiogram
Duplex scanning
Normal (0-15% stenosis)Mild (16-49%)Moderate (50-79%)Severe (80-99%)Occluded
0-15% stenosis
1
3
Conventional contrast angiography
16-49%
1
13
7
50-79%
1
13
11
80-99%
3
17
Occluded
5
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Riles et al Accuracy of Magnetic Resonance Angiography 345
firm our impression that there is a wide variabilityamong vascular laboratories. Few of the laboratoriesthat perform duplex scans have made an effort tovalidate their results and, therefore, do not know theiraccuracy in diagnosing carotid stenosis. Finally, there isalways some unease in undertaking the risks of carotidsurgery solely on the basis of a technician-performedtest that does not provide a hard-copy image of thecarotid bifurcation.
Part of the purpose of this study was to determinewhether conventional angiography was necessary orhelpful if there was agreement between the reading ofthe magnetic resonance angiogram and the duplexscan. Of the 49 cases in which magnetic resonance andduplex did agree, the two agreed with the contraststudy in only 33 cases (67%). We reviewed the 16 casesin which duplex scanning and magnetic resonanceangiography correlated but conventional angiographydid not. In three instances the magnetic resonance andduplex scan read mild stenosis, but the contrast studywas interpreted as normal. In two cases the magneticresonance and duplex were interpreted as moderate,but the contrast study showed 16-49% stenosis. Ineach of these five cases, the patient was asymptomatic,and the variance in the readings was not of clinicalsignificance. In 11 cases, the magnetic resonance an-giogram and duplex scan determined a vessel to beseverely stenosed, whereas it measured 50-79% ste-nosis by conventional study. A review of these angio-grams showed that they were mostly on the moderate-to-severe borderline. Management of these patientswould have been altered had angiography not beenperformed only if the evaluation was for asymptomaticdisease. In fact, each of these vessels was associatedwith ipsilateral carotid territory symptoms and, there-fore, the differences in reading were not of clinicalsignificance.
To answer the question of whether information frommagnetic resonance angiography can be relied on whenit correlates with duplex scanning, the data from thisstudy suggest that both noninvasive studies tend tooverread the degree of stenosis. Judgment must be usedto determine whether an overreading would change theclinical decision for a given patient. In our practice,overreading would not change the decision if the patienthad appropriate neurological symptoms, but it might ifthe patient were asymptomatic. If one limits surgery to>80% stenosis for this group, the information needed isa precise measurement of the degree of stenosis at thebifurcation. Caution must be used when relying on themagnetic resonance angiography information in theasymptomatic patient, as overreadings will lead to someunnecessary operations.
At present we feel one must be selective in usingmagnetic resonance angiography as the sole diagnostictool before performing carotid endarterectomy. If thepatient has hemispheric symptoms and a duplex scanshows an ipsilateral carotid stenosis, magnetic reso-nance angiography may be performed to confirm theduplex finding before surgery and to assess the contra-lateral carotid. For patients with repetitive symptomsand minimal stenosis on the duplex scan and patientswith unusual neurological symptoms, a conventionalcontrast angiogram is the procedure of choice. In thesecases high-resolution films are needed to detect luminal
surface irregularities or intracranial lesions that may beresponsible for the symptoms.
Although rapid improvements in magnetic resonanceangiography are taking place, the technique has severalinherent drawbacks. Patients with pacemakers or othermetallic implant devices cannot be studied by magneticresonance angiography because of the effect of thestrong magnetic field on these objects. The images canbe significantly degraded by patient motion. Poor car-diac output may also contribute to poor quality ofimages. Finally, the high-velocity blood flow and turbu-lence at areas of severe stenosis can distort the imageand may lead to misreadings regarding the degree ofstenosis.
Magnetic resonance angiography is an exciting devel-opment that is already having an impact on the diagno-sis and treatment of vascular disease. As our experienceincreases and the technology advances, it is likely thatangiography by percutaneously placed arterial catheterswill become a relic of the past. At present, however,there are limitations to the technique, and we must becautious when relying on information from these studiesto make clinical decisions. To establish the role ofmagnetic resonance angiography in selecting patientsfor carotid surgery, more validation studies comparingmagnetic resonance angiography with conventional con-trast angiography are needed.
References1. Taylor DC, Strandness DE Jr: Carotid artery duplex scanning.
J Clin Ultrasound 1987;15:635-6442. Keller PJ, Drayer BP, Fram EK, Williams KD, Dumoulin CL,
Souza SP: Magnetic resonance angiography with two-dimensionalacquisition and three-dimensional display. Radiology 1989; 173:527-532
3. Hass WK, Fields WS, North RR, Kricheff II, Chase NE, BauerRB: Joint Study of extracranial arterial occlusion: II. Arteriogra-phy, techniques, sites and complications. JAMA 1968;203:961-968
4. Faught G, Trader SD, Hanna GR: Cerebral complications ofangiography for transient ischemia and stroke: Prediction of risk.Neurology 1979;29:4-15
5. Masaryk JT, Modic MR, Ruggieri PM, Ross JS, Laub G, LenzGW, Tkach JA, Haacke EM, Selman WR, Harik SL: Threedimensional (volume) gradient echo imaging of the carotid bifur-cation: Preliminary clinical experience. Radiology 1989;171:801-806
6. Pernicone JR, Siebert JE, Potchen EJ, Pera A, Dumoulin CL,Souza SP: Three-dimensional phase-contrast magnetic resonanceangiography in the head and neck: Preliminary report. AJNR1990;ll:457-466
7. Masaryk TJ, Ross JS, Modic MT, Lenz GW, Haacke EM: Carotidbifurcation: Magnetic resonance imaging. Radiology 1988;166:461-466
8. Baker JD, Rutherford RB, Bernstein EF, Courbier R, Ernst CB,Kempczinski RF, Riles TS, Zarins CK: Suggested standards forreports dealing with cardiovascular disease. J Vase Surg 1988;8:721-729
9. Roederer GO, Langlois YE, Jager KA: The natural history ofcarotid arterial disease in asymptomatic patients with cervicalbruits. Stroke 1984;15:605-613
10. Hertzer NR, Flanigan RA, O'Hara PJ, Beven EG: Surgical vs.nonoperative treatment of asymptomatic carotid stenosis. Ann Surg1986;204:163-171
11. Chambers BR, Norris JW: Outcome in patients with asymptomaticneck bruits. N Engl J Med 1986;315:860-865
12. Geuder JW, Lamparello PJ, Riles TS, Giangola G, Imparato AM:Is duplex scanning sufficient evaluation before carotid endarterec-tomy?/ Vase Surg 1989;9:193-201
13. Ricotta JJ, Holen J, Schenk E, Plassche W, Green RM, GramiakR, DeWeese JA: Is routine angiography necessary prior to carotidendarterectomy? / Vase Surg 1984;l:96-102
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

346 Stroke Vol 23, No 3 March 1992
14. Goodson SF, Flanigan P, Bishara RA, Schuler JJ, Kikta MJ, Meyer 16. Howard G, Jones AM, Chambless L: A multicenter validation ofJP: Can carotid duplex scanning supplant arteriography in patients Doppler ultrasound vs. angiogram: The Asymptomatic Carotidwith focal carotid territory symptoms? J Vase Surg 1987;5:551-557 Atherosclerosis Study experience. Presented at the 16th Interna-
15. Kenagy JW: Comparison of duplex scanning and contrast arteriogra- tional Joint Conference on Stroke and Cerebral Circulation, Sanphy: A community hospital experience. J Vase Surg 1985;2:591-593 Francisco, Calif, February 22, 1991
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from

T S Riles, E M Eidelman, A W Litt, R S Pinto, F Oldford and G W Schwartzenbergscanning.
Comparison of magnetic resonance angiography, conventional angiography, and duplex
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.23.3.341
1992;23:341-346Stroke.
http://stroke.ahajournals.org/content/23/3/341World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 21, 2018http://stroke.ahajournals.org/
Dow
nloaded from