left heart catheterization
TRANSCRIPT

LEFT HEART CATHETERIZATION
Dr. Nagula Praveen,Final yr PG
Introduction
Indications
Contraindications
Preparation of patient
Access – techniques
Catheters
Angiographic Views
Pressure wave forms
Interpretation
Complications
Case profile examples
Introduction Cardiac catheterization – “the insertion and passage of small plastic
catheters into arteries,veins,the heart,and other vascular structures.”
Standard medical procedure – guides treatment decision, we can
measure intracardiac pressures, cardiac output, oximetry data, have
radiographic images of coronaries, aorta and peripheral vessels for
anomalies, obstruction.
Presently more of therapuetic concern – eg; angioplasty, stenting and
closure of ASD,VSD.

IndicationsUsually an elective procedure.Diagnostic – discreprancy between the symptoms and clinical features
of patient. Valve area, cardiac output and resistance.Quantification of shunts Pressure gradients Therapeutic – useful for assessing the pressure gradients before and
after Mitral Stenosis – PBMV Aortic Stenosis – PBAV PDA device closure HOCM – alcohol septal ablation. Cooarctation of Aorta Aorto Pulmonary Window closure

Contraindications Absolute – patient not prepared either psychologically or physically.
Relative –
Fever
Anemia
Electrolyte abnormalities (Hypokalemia)
Systemic illness
Anticoagulation (INR >1.6)
Using medications (digitalis,phenothiazines)
Renal failure
Uncontrolled CHF
Pregnancy

Preparing the patient Informed consent – simple terms, steps of procedure, complications (usually
taken by operator).
All peripheral pulses to be felt.
For diabetic patients – dose of NPH insulin should be cut by 50% (overnight
fast with normal dosing of insulin – hypoglycemia).
To stop metformin – 48 hrs before procedure – lactic acidosis.(no evidence for
clinical benefit).
Adequate hydration. (urine output > 50ml/h)
Anxiolytic
Shaving of the both forearms and inguinal regions.
IE prophylaxis if valvular heart disease.

Access Femoral artery/vein
Modified Seldinger technique.
Fluoroscopy guidance – medial edge of the middle of the head of the
femur.
30 angle to the vessel.
A syringe may be attached to seldinger needle and gently aspirated
while advancing-in case of femoral vein access.
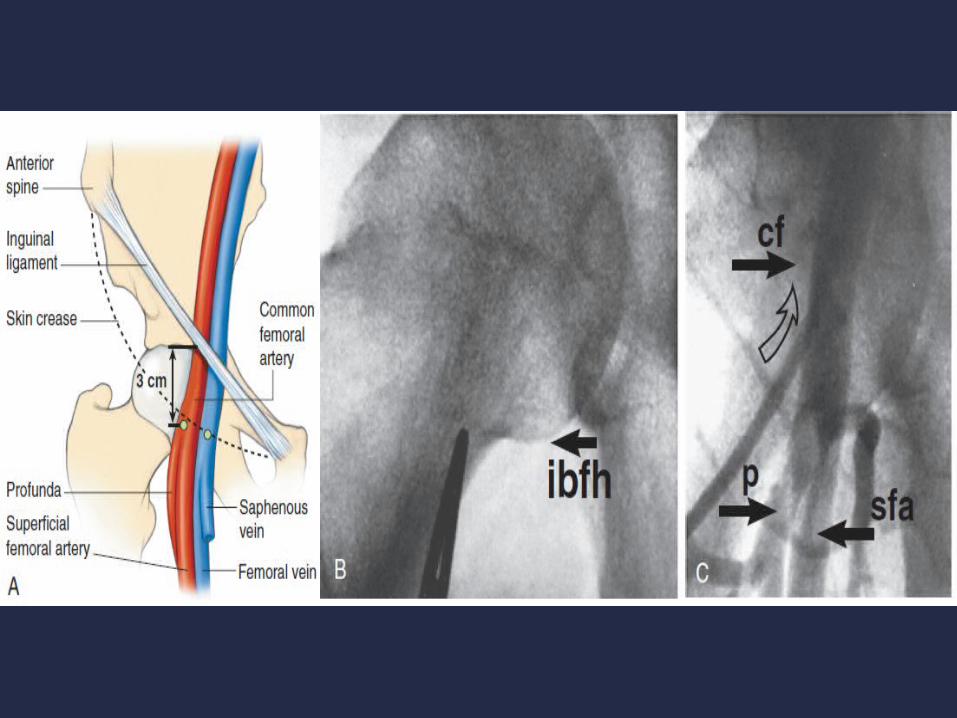

Modified Seldinger technique

Catheters Angiographic catheters Pigtail catheter
• 1.Quanticor - cardiomarker pigtail – radioopaque markers set 2cm apart.
• Exact LV distances, volumes and stroke volume can be calculated using these markers as a ruler.
• 2.Angiographic Pigtail - MC used• 3.Van Tassel angled pigtail – 145-155 angle ,dilated aorta.• 4.Groll man Pigtail – curve generally on reverse side
RV selective angiography,PA angiography.• 5.Elliptical or Oval - small aortic valves• 6.Tennis Racquet – reduced risk of vessel wall extravasation



Gensini catheter Woven dacron catheter with polyurethane coating.
Tapered tip.
Three pairs of laterally opposed oval side holes within 1.5 cm of
its open tip.
Right and left angiography studies.
Disadvantages
Straight tip – more arrhythmogenic.
Catheter recoil during high flow rates.
Risk of intramyocardial injection.

NIH catheter. – no end hole, six sideholes.
Multitrack catheter.
• end hole and side hole catheter.
• useful to record pressure while wire inside – pull back
gradient across valvular stenosis.
• Angiography while wire inside.

Techniques Retrograde Techniques
The Judkins technique - Femoral artery.
Percutaneous Radial technique.
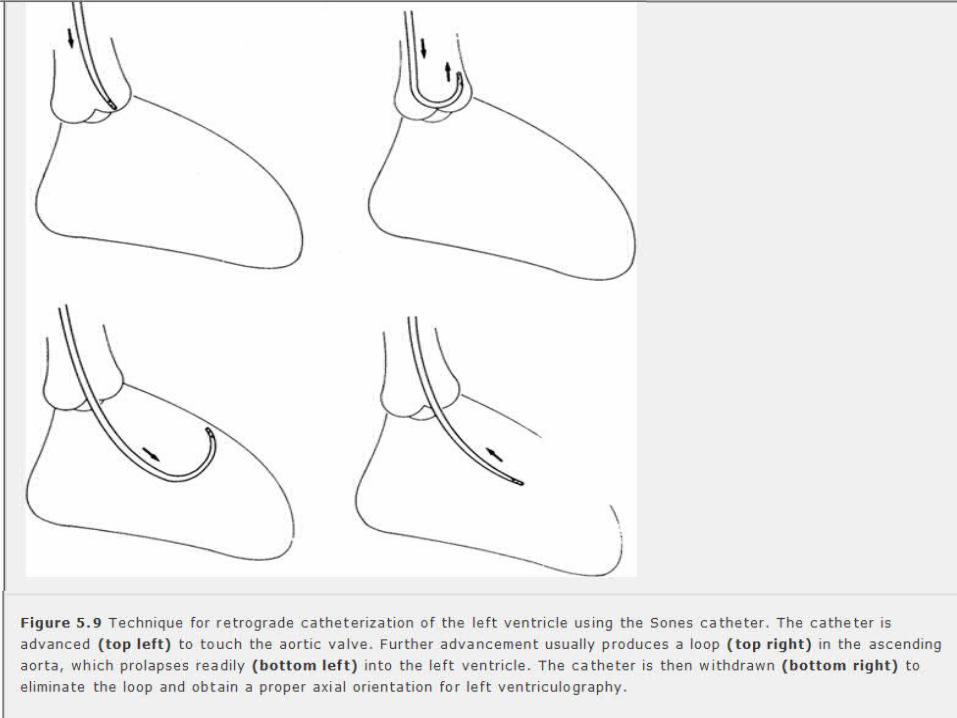
Percutaneous Brachial artery technique – Sones Technique.
Antegrade technique
Transeptal Catheterization.
Apical Approach
Direct Transthoracic Left ventricular puncture.

Judkins technique Relatively easy, speed, reliability,low complication rate.
MC method for left heart catheterization.
1% xylocaine infiltrated at the puncture site.
Artery to be punctured 3cms below the inguinal ligament, not the inguinal
crease.
Modified Seldinger technique is used(double wall puncture leads to
hematoma).
18 G thin walled needle is used.
0.035-0.038 J tip PTFE coated guidewire is advanced through the needle.(hot
knife passing through the butter).
A sheath atleast equal size of the catheter to be passed over the guide wire
after small nick by scalpel. Heparin - 2000 to 3000 units.

LV systolic and end diastolic pressures can be recorded by advancing
a pigtail into the LV.
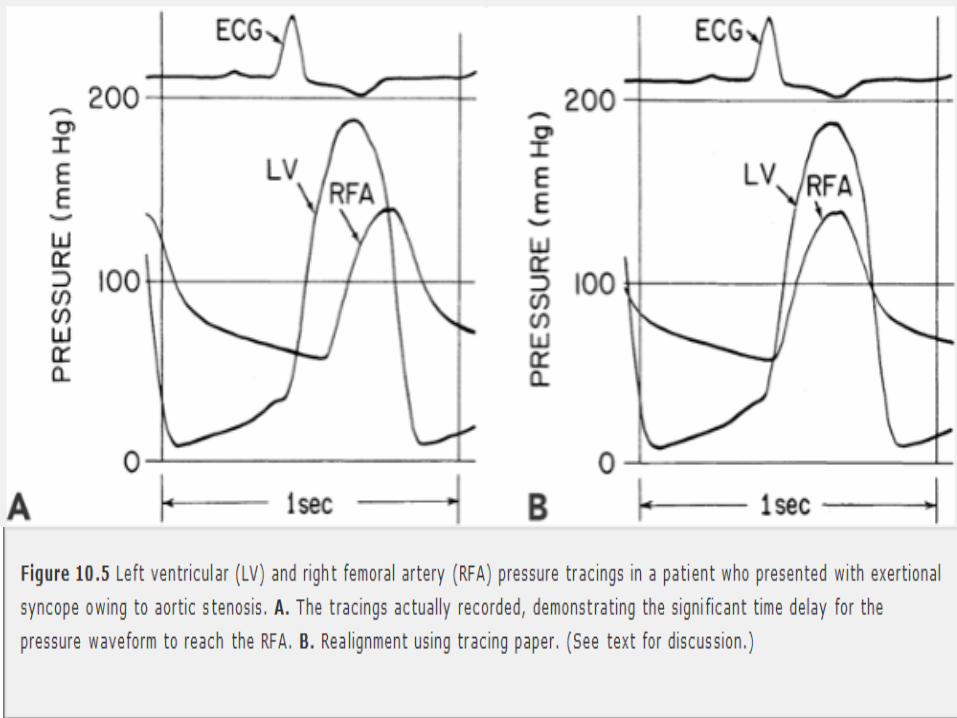
For assessing AS, LV and Aortic pressure should be recorded
simultaneously with two transducers.
Femoral artery pressure not to be taken – attenuation in pressure
can occur in older patients,with PAD.
Pigtails with both distal and proximal lumen to be used.
LV Aangiography - pigtail is used – to assess LV function.
Intraventricular gradients – multipurpose catheter to be used.


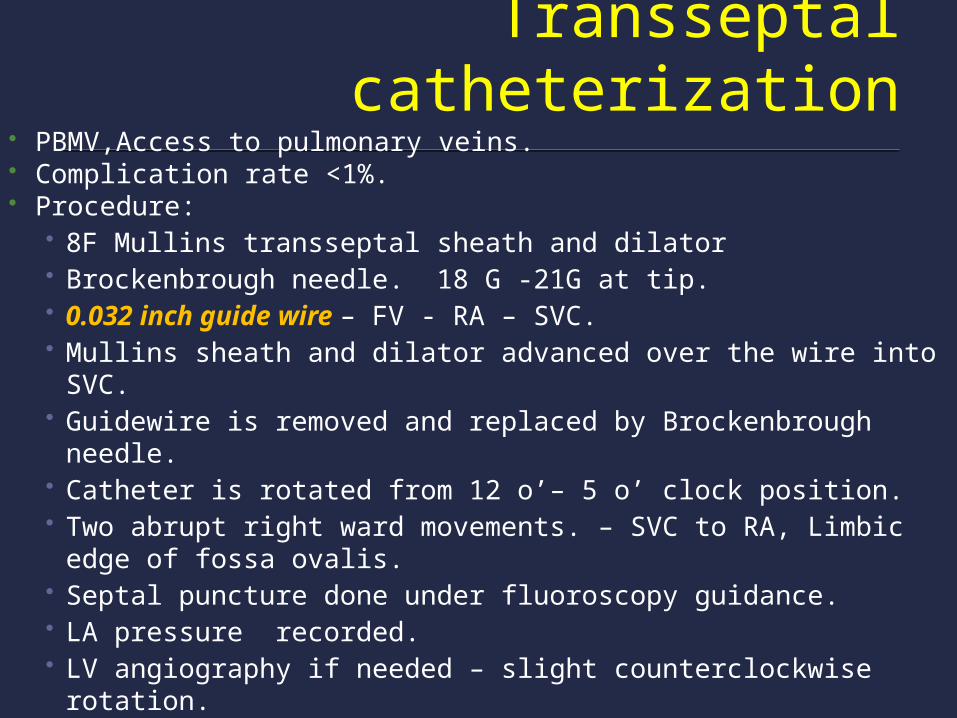
Transseptal catheterization PBMV,Access to pulmonary veins. Complication rate <1%. Procedure:
• 8F Mullins transseptal sheath and dilator• Brockenbrough needle. 18 G -21G at tip.• 0.032 inch guide wire – FV - RA – SVC.• Mullins sheath and dilator advanced over the wire into SVC.• Guidewire is removed and replaced by Brockenbrough needle.• Catheter is rotated from 12 o’– 5 o’ clock position.• Two abrupt right ward movements. – SVC to RA, Limbic edge of
fossa ovalis.• Septal puncture done under fluoroscopy guidance.• LA pressure recorded.• LV angiography if needed – slight counterclockwise rotation.




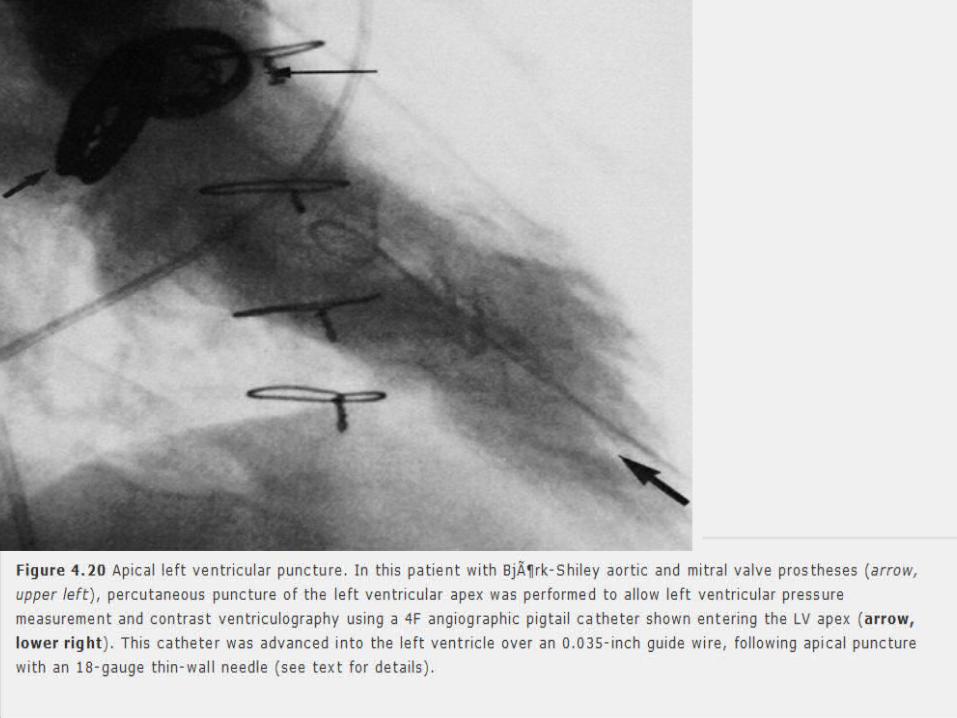
Direct Transthoracic LV puncture Measure LV pressure and perform ventriculography in patients with
mechanical prosthetic valves in both the mitral and aortic positions that prevent
both retrograde and transseptal catheterization.
Crossing of tilting disks to be avoided – catheter entrapment, occlusion of the
valve,possible dislodgement and embolization of the disc.
Localization of LV apex by palpation or by echocardiography.
18 G 6” inch Teflon catheter system is inserted at upper rib margin, directed
slightly posteriorly and toward the right second intercostal space.
Needle and sheath are advanced into the LV.
Stylet and the needle removed.
Sheath connected for pressure measurement.

Views Left ventriculography RAO 30 - Anterior ,apical and inferior walls.
LAO 60 and Cranial 20 - lateral and septal ventricular walls.
• Suspected VSD,MR.
Aortography LAO view – Ascending aorta, Aortic arch, innominate,carotids,left
subclavian arteries.
RAO view – lower thoracic aorta, assessing AR.
The descending aorta and ascending aorta are superimposed across the
arch in AP projection.

Power injection of 30-40ml of contrast medium into the left
ventricle at 12-15ml/sec is used to assess LV function and the
severity of MR.


Normal lv angiogram
RAO DIASTOLIC FRAME RAO SYSTOLIC FRAME
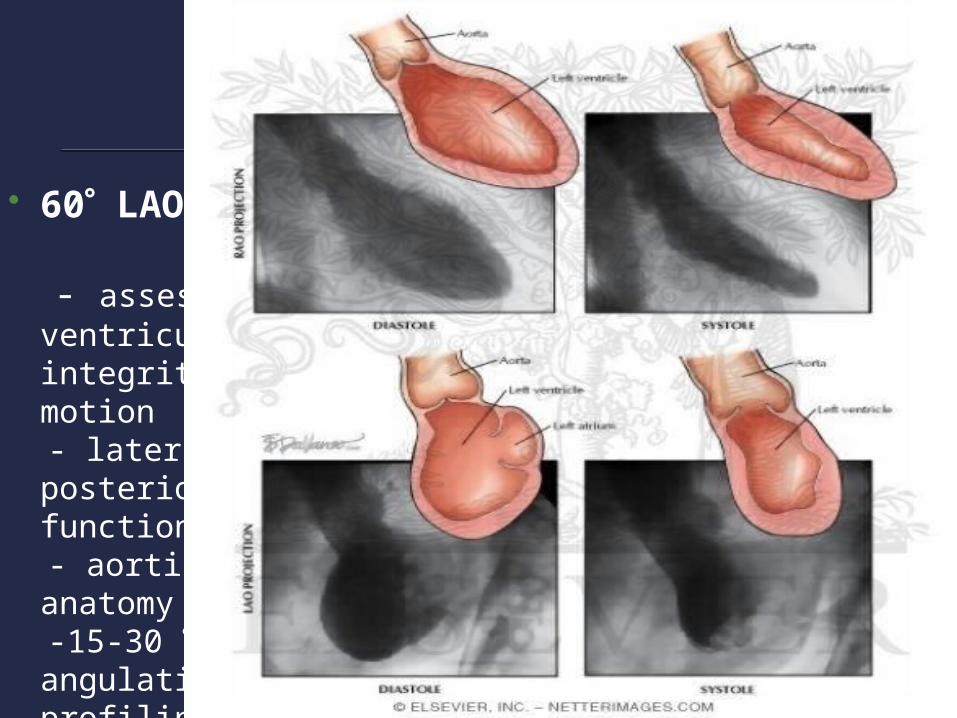
60 LAO
- assess ventricular septal integrity and motion
- lateral and posterior segmental function
- aortic valvular anatomy -15-30 cranial angulation for
profiling entire IVS

Views for only left heartPROJECTION DEGREES VESSEL/
CHAMBER IMAGED
LESIONS
Long axial oblique
70 LAO,30Cranial LV LVOT obstruction
Hepatoclavicular view
45 LAO ,45 Cranial
Four chambers LV –RA connection
Lateral view 90 Descending aorta Coarctation,PDA
LAO 60 -70 LAO Aorta Coarctation/Aortic valve disease
RAO 30- RAO with or without caudal angulation
LV Mitral valve disease

Catheter course
Judkins:
Pigtail catheter – FA – Abdominal aorta – Thoracic aorta – Aortic arch
–Ascending aorta – Aortic sinus – Aortic valve – LV.
Transseptal Technique
Femoral vein – IVC - SVC – RA – PFO/Puncture - LA – MV – LV .
Pull BACK
LV – LVOT – AV – Aortic sinus – Ascending aorta – arch –
descending aorta.

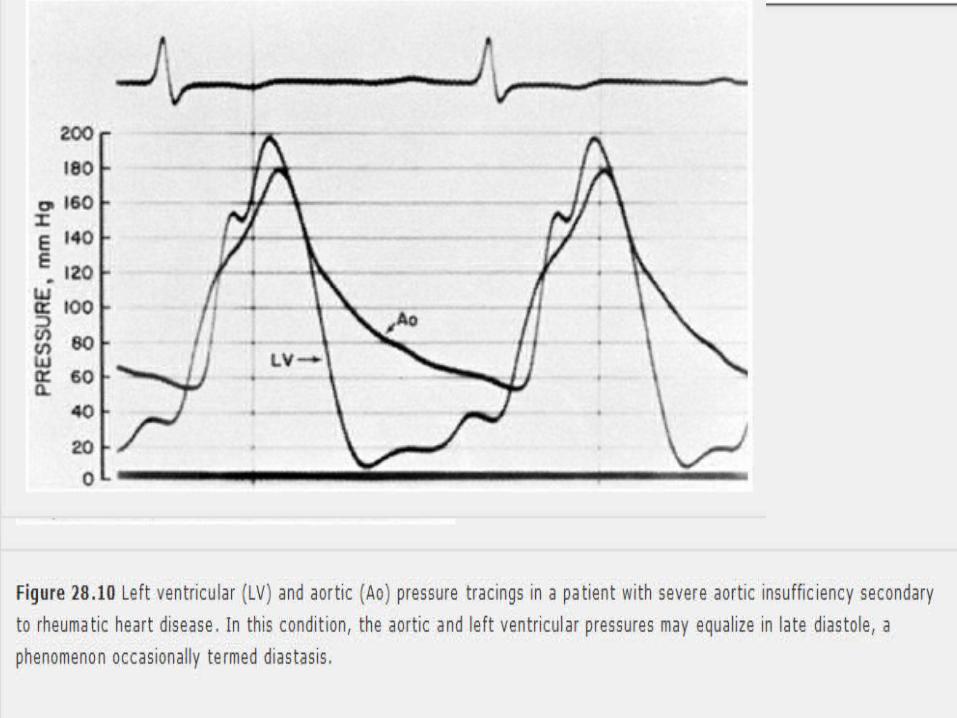
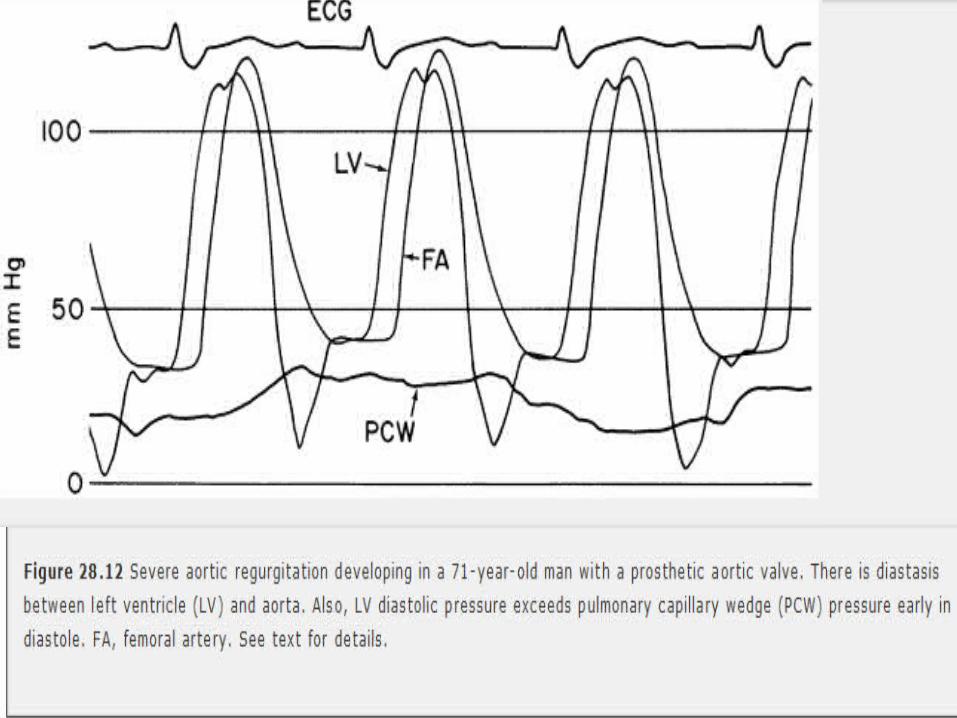
Sellers quantification


Aortic Regurgitation
+ small regurgitant jet only, LV ejects contrast each systole.
+ + regurgitant jet faintly opacifies LV cavity, not cleared with each
systole.
+++ persistent LV opacification = Aortic root density; LV
enlargement.
++++ Persistent LV opacification > Aortic root concentration, often
marked LV enlargement.

Hemodynamic data
Pressure measurements
Measurement of flow (eg: cardiac output,shunt flow,flow
across a stenotic orifice,regurgitant flow,and coronary blood
flow)
Determination of vascular resistance.

Left atrial wave form Normal left atrial pressure is higher than the right atrium.(high
pressure system of the left side of the heart).
The v wave is generally higher than the a wave.
Left atrium is constrained posteriorly by the pulmonary veins whereas
the right atrium can easily decompress through the SVC and IVC.
Height of the left atrial v wave –most accurately reflects the left
atrial compliance.
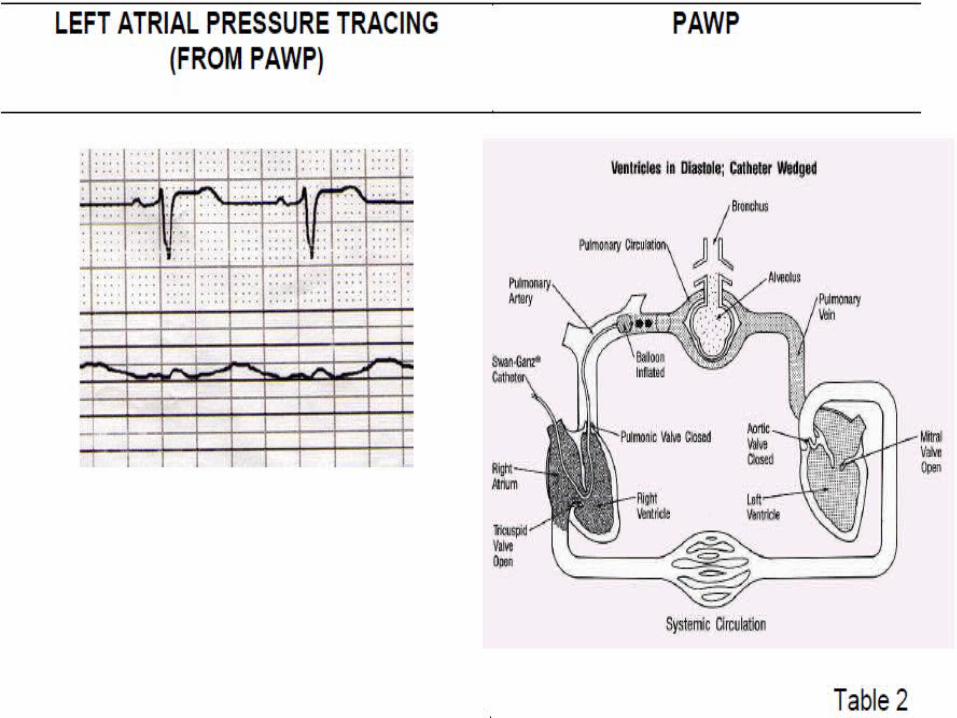

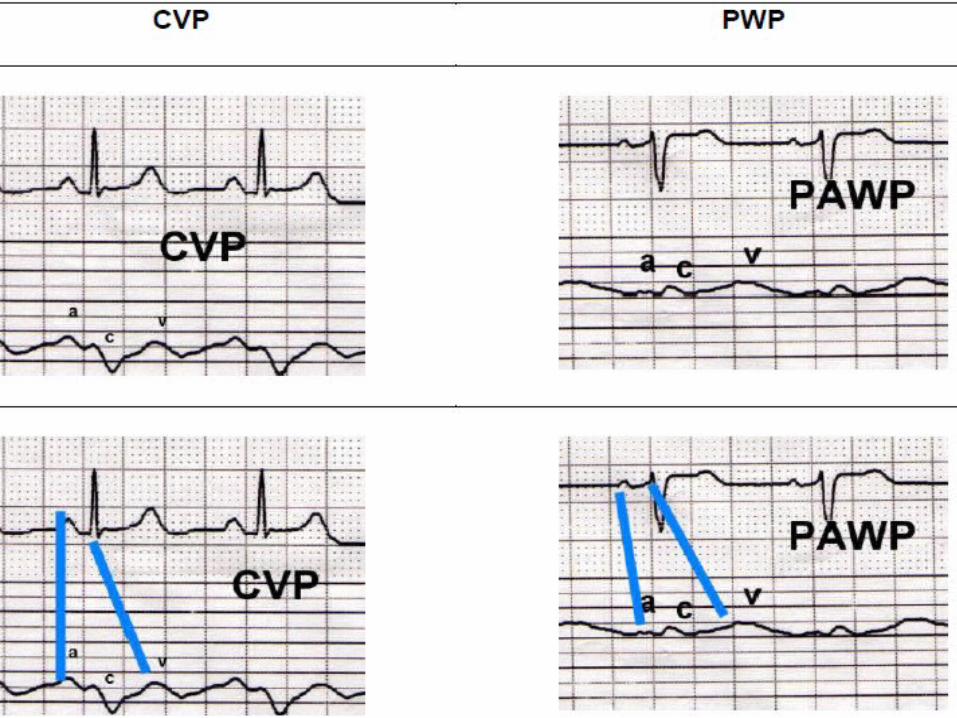
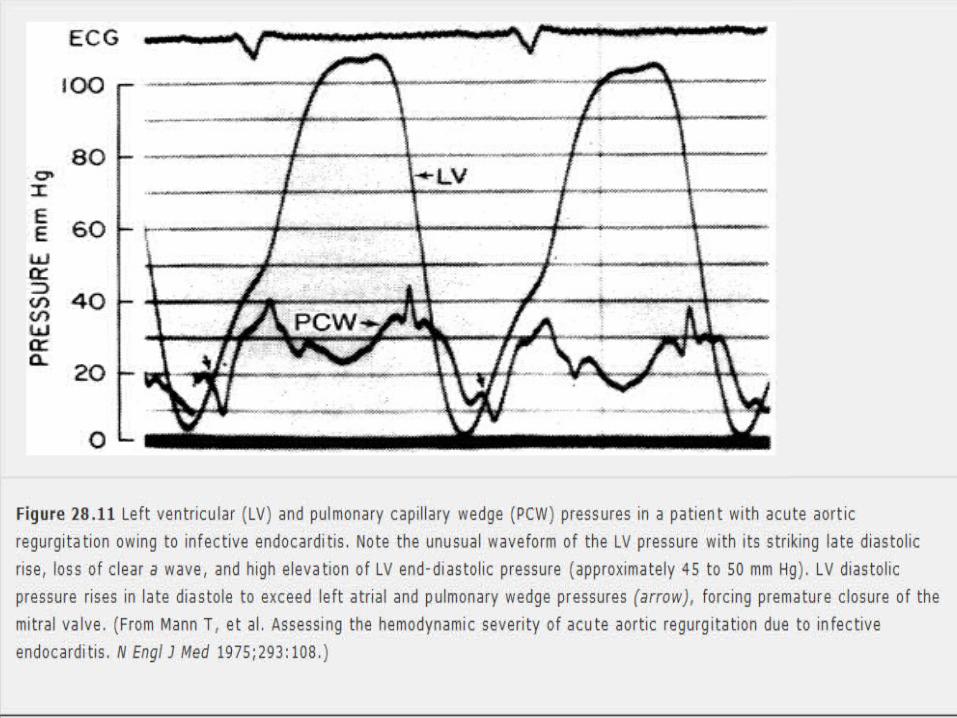
Pulmonary capillary wedge pressure
Similar to left atrial pressure
Slightly damped and delayed (transmission through the lungs).
c waves may not be seen.
PADP = mean PCWP - as pulmonary circulation has low resistance.
PCWP may overestimate true left atrial pressure - High PVR
• Hypoxemia
• Pulmonary embolism
• Chronic pulmoanry hypertension
• After mitral valve surgery(accurate gradients across MV – LA pressure needed)
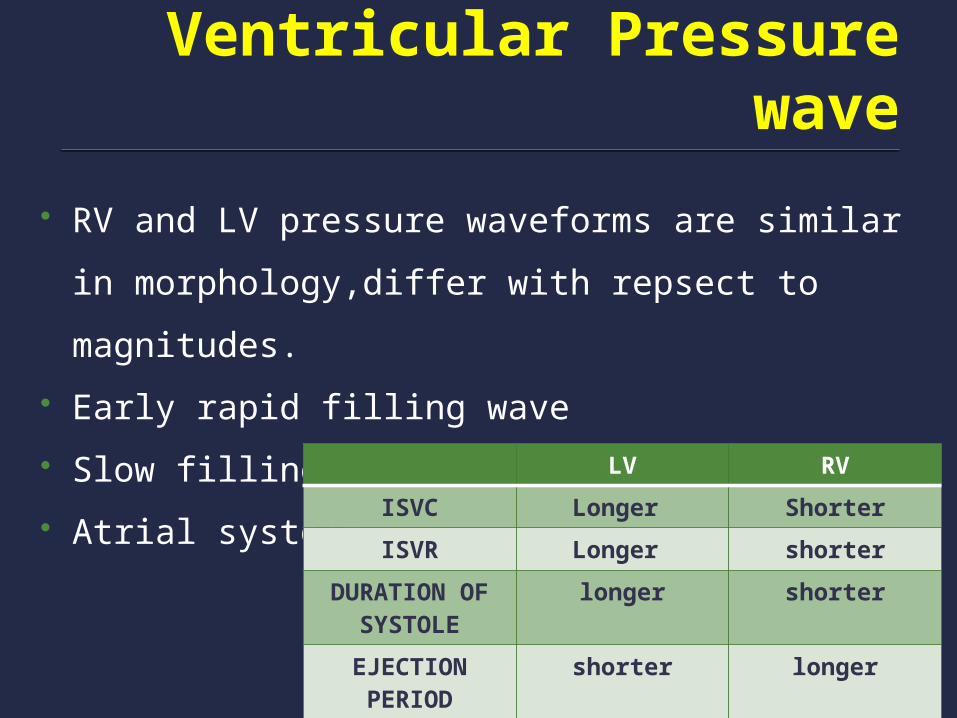
Ventricular Pressure wave
RV and LV pressure waveforms are similar in
morphology,differ with repsect to magnitudes.
Early rapid filling wave
Slow filling phase
Atrial systole. LV RV
ISVC Longer Shorter
ISVR Longer shorter
DURATION OF SYSTOLE
longer shorter
EJECTION PERIOD
shorter longer

Imp.points
End diastolic pressure is generally measured at the C point – rise in
ventricular pressure at the onset of isovolumic contraction.
When the C point is not well seen, a line drawn from the R wave on
the simultaneous ECG to the ventricular pressure waveform is used
as enddiastolic pressure.

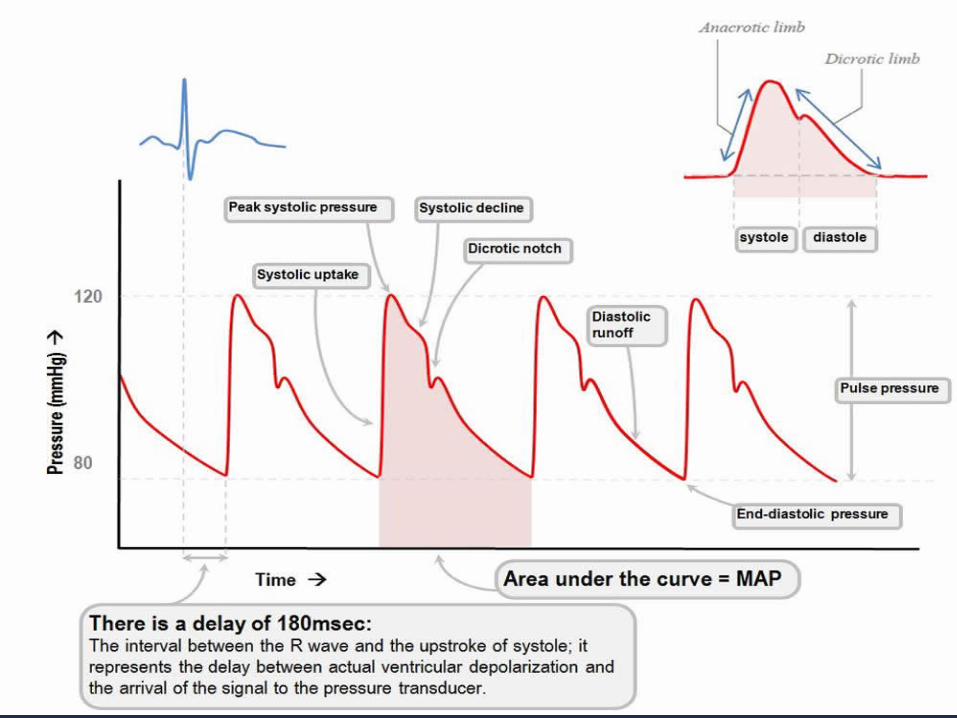
Great vessel pressure Systolic wave
The incisura (indicating the closure of the semilunar valves)
Gradual decline in pressure until the following systole.
Pulse pressure – reflects stroke volume and compliance of the
arterial system.
Mean aortic pressure – peripheral resistance(accurately).


At periphery artery
Systolic wave increases in amplitude – becomes more
triangular.
Diastolic wave decreases(until the midthoracic aorta),and
then increases.
Mean aortic pressure similar.
Mean peripheral arterial pressure is typically lower than mean
central aortic pressure by 5 mm Hg or less.





Difference between the central aorta and the
periphery(femoral,brachial,or radial arteries) is greatest in younger
patients – increased vascular compliance.
Imp. in patients with stenotic lesions.
When a transvalvualr gradient is present, the most accurate measure of
aortic pressure is obtained at the level of the coronary arteries(to avoid
the pressure recovery).
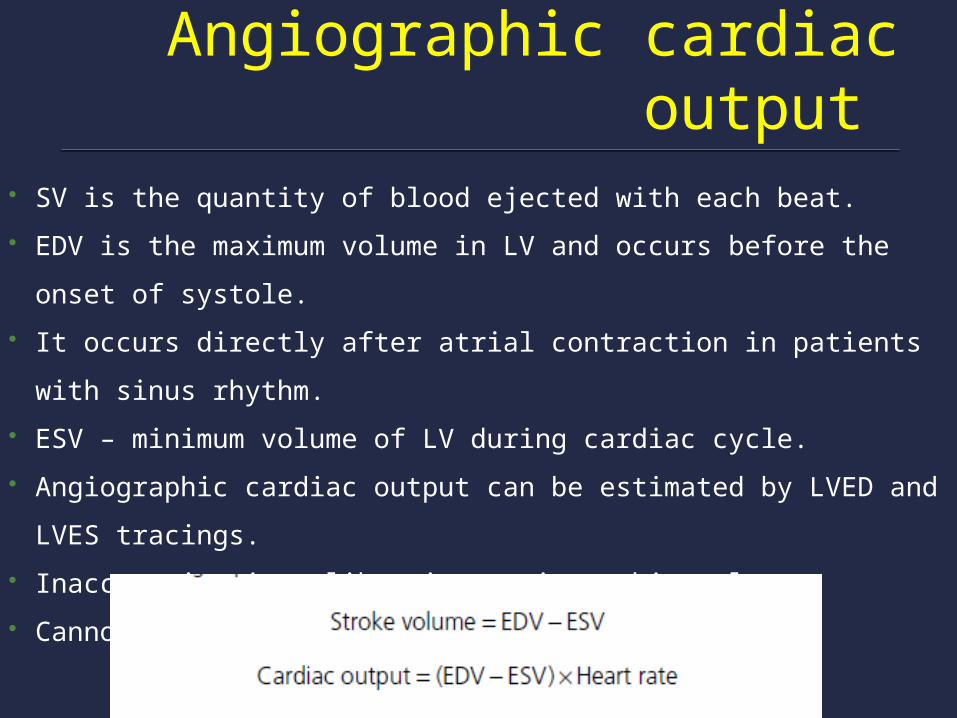
Angiographic cardiac output SV is the quantity of blood ejected with each beat.
EDV is the maximum volume in LV and occurs before the onset of
systole.
It occurs directly after atrial contraction in patients with sinus rhythm.
ESV – minimum volume of LV during cardiac cycle.
Angiographic cardiac output can be estimated by LVED and LVES
tracings.
Inaccuracies in calibrating angiographic volumes.
Cannot be used in AF, regurgitant lesions.

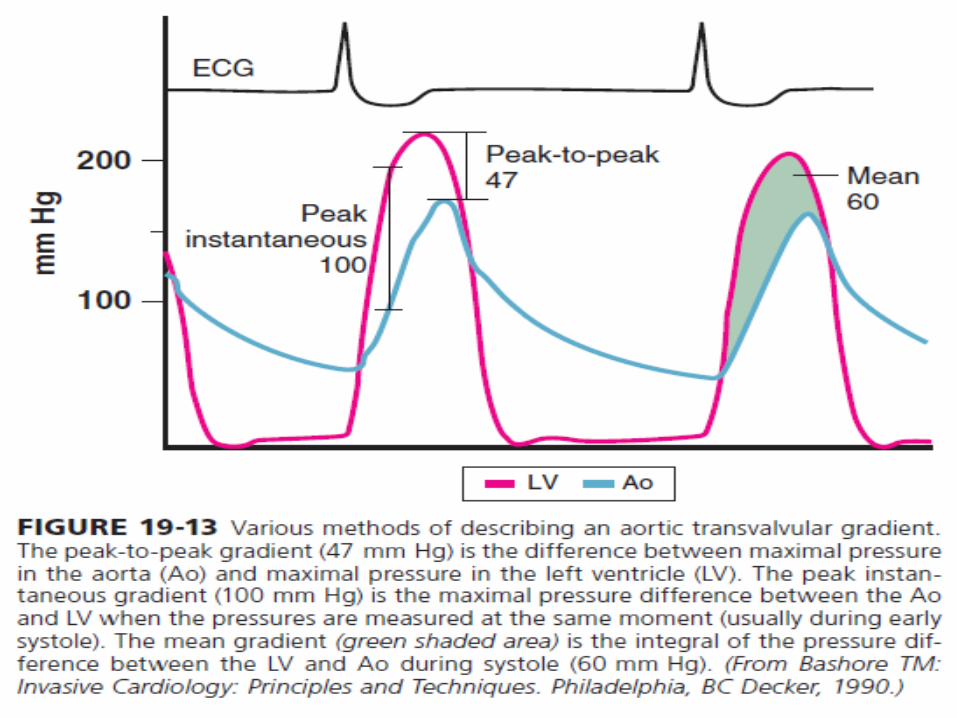
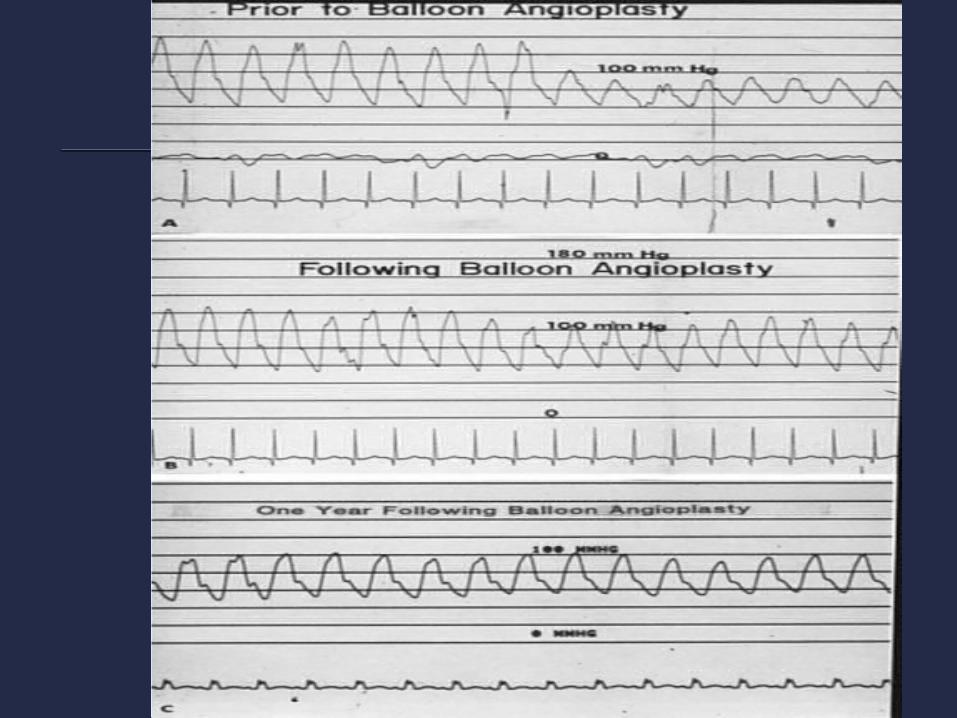
Pressure Gradients
Across the valve –Mitral valve,Aortic valve
Peripherally – Coarctation of aorta
Intraventricularly
Assessing the severity of stenosis,valve area,resistance
Cardiac output
Mitral Stenosis Simultaneous LV,LA pressure tracings. Check zero pressures of the PCWP,FA,LV after catheters and
sheath have been flushed. LV pressure tracing 200mmHg scale at 50 mm/sec paper
speed. PCWP pressure tracing 40 mm Hg scales at 50mm/sec paper
speed. Use 100mm/sec speed if a mitral valve gradient is present.


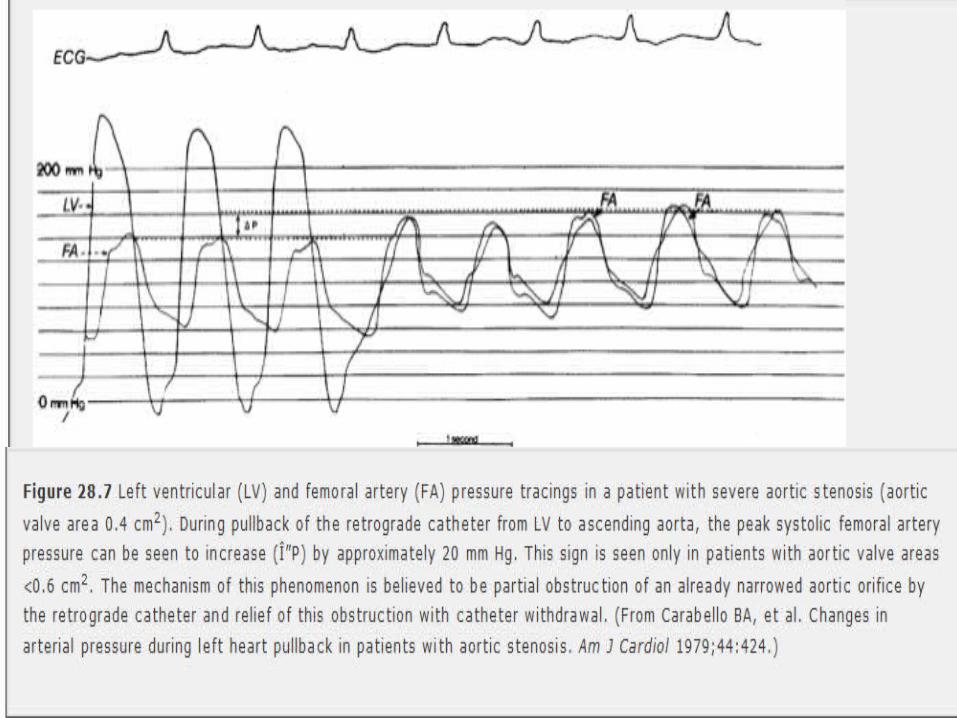
Aortic valve stenosis Advance a pigtail into the LV. Check the zero pressures of both sheath and pigtail catheter
after flushing. Record LV and FA pressure (25mm/sec speed,200mmHg
scale) 100mm/sec speed if an aortic valve gradient is present.
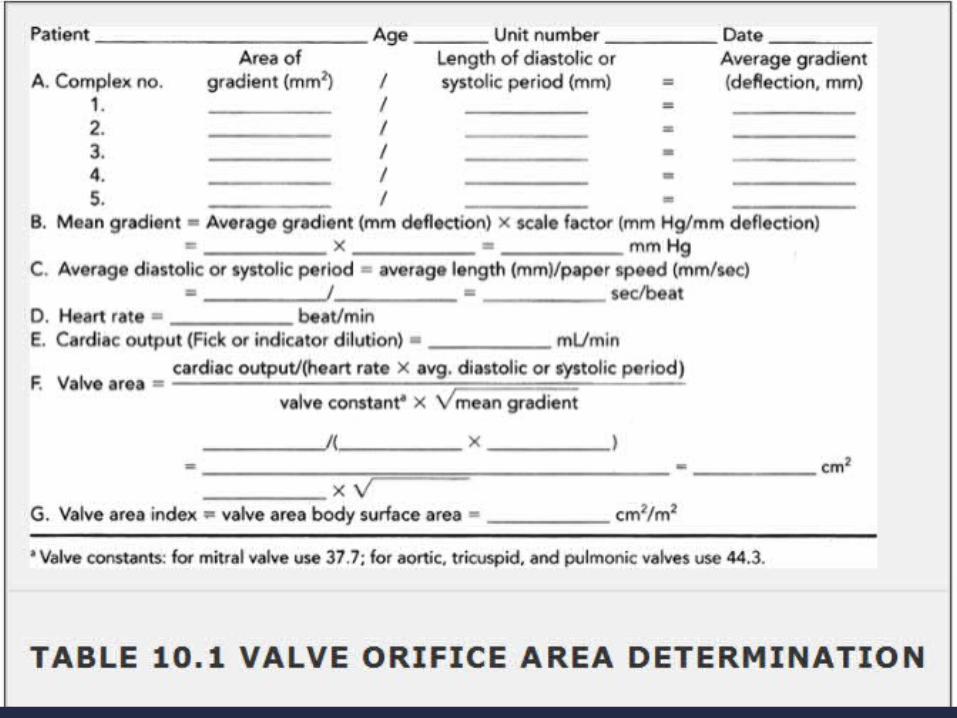
Determination of pressure gradients


Gorlin and Gorlin equation


Valve area



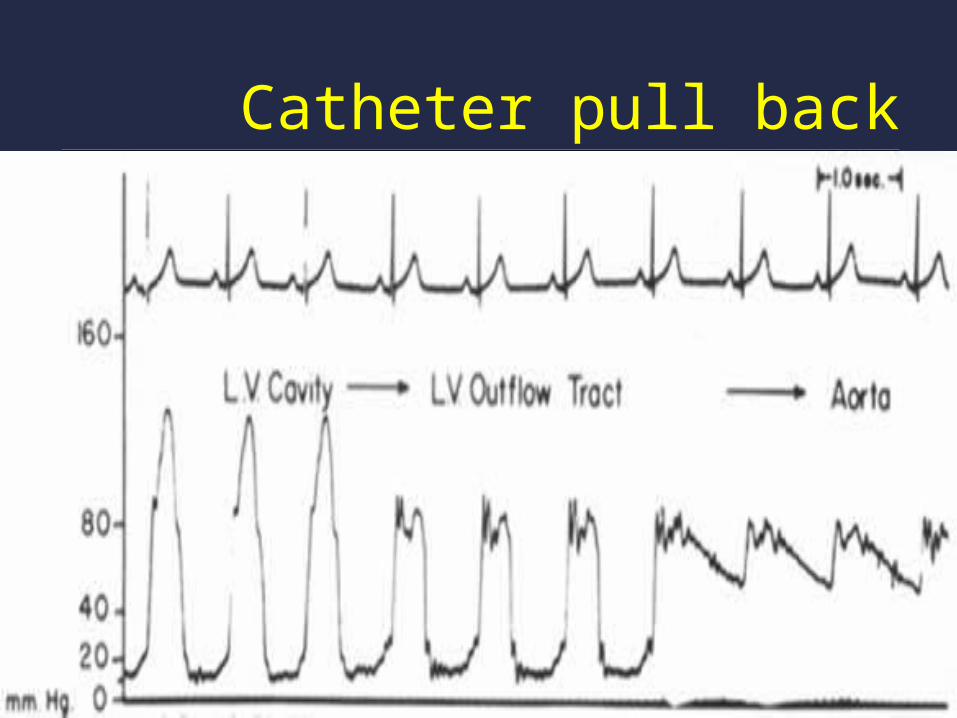
Catheter pull back


Complications
Access site complications.
Contrast induced reactions.
Procedure related complications.

Conclusion
Left heart catherization has a significant role in quantifying the
pressure gradients across the valve and within the left ventricle.
Mostly being used presently during therapeutic indications rather
than diagnostic indications.
Optimal pressure tracings with all necessary precuations and
knowing the limitations of each helps in judging the severity of
the clinical condition to the nearest accuracy..
