perforation of heart during cardiac catheterization and ... · perforation of heart during cardiac...
TRANSCRIPT
Perforation of Heart during Cardiac Catheterizationand Selective Angiocardiography
By P. G. KEATES, M.D., AND G. R. WAGNER, M.R.A.C.P.
CARDIAC catheterization and selectiveangiocardiography are frequently per-
formed in any cardiac diagnostic unit. Minorcomplications, such as arrhythmias, are notuncommon, but major complications are quiterare. This case is reported to show that per-foration of the heart may occur in the courseof these investigations, but may not neces-sarily lead to serious after-effects.
Case ReportThe patient, K.K., a 3-year-old boy, was ad-
mitted to the General Infirmary at Leeds in Janu-ary 1962 for investigation of his congenital heartdisease, with moderate dyspnea and eyanosis oneffort. Physical examination showed normal devel-opment. There was no eyanosis at rest, and thefingers and toes were not clubbed. The peripheralpulses were normal. Inspection of the neck revealeda moderate venous "a" wave. The chest was nor-mal in shape and the heart was rather quiet topalpation although right ventricular pulsationcould just be felt to the left of the sternum. Onauscultation there was a moderately loud ejectionsystolic murmur in the pulmonary area that hadits peak early in systole. The second heart soundwas single.
The chest radiograph showed a normal-sizedheart, a right-sided aortic arch, and some pul-monary ischenmia. The electrocardiogram was in-terpreted as showing sinus rhythm, right axisdeviation, and considerable right ventricular hyper-trophy.The clinical diagnosis made on the basiE of these
findings was Fallot's tetralogy.On January 26, 1962, under rectal thiopental
anesthesia, eardiac catheterization was performedfrom the right long saphenous vein with a no.-6Cournand catheter. The findings indicated a diag-nosis of infundibular pulmoniary stenosis, atrialseptal defect, and ventricular septal defect.To complete the investigation, the Cournand
eatheter was then replaced by a no.-7 National In-
From the Department of Diagnostic Radiology andThoracic Surgical Department, General Infirmary atLeeds, England.
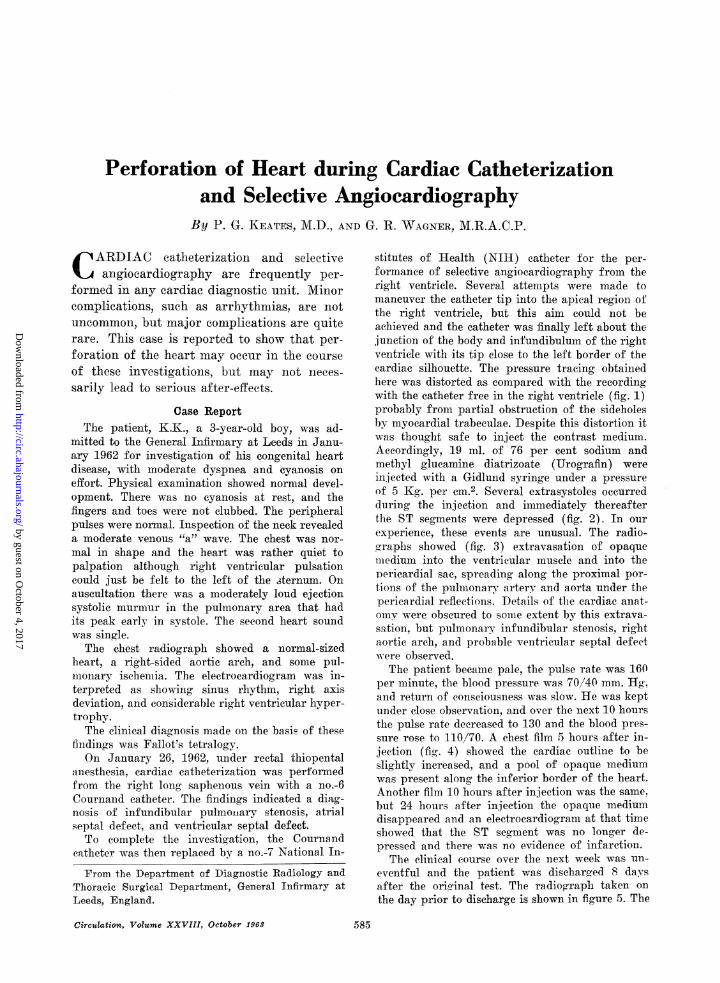
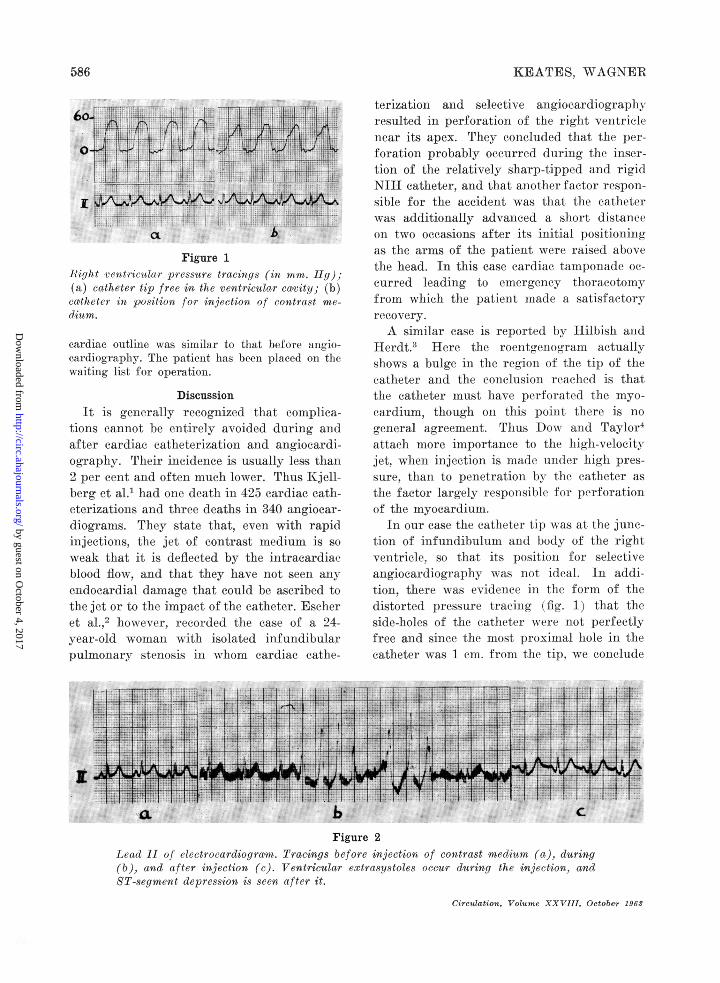
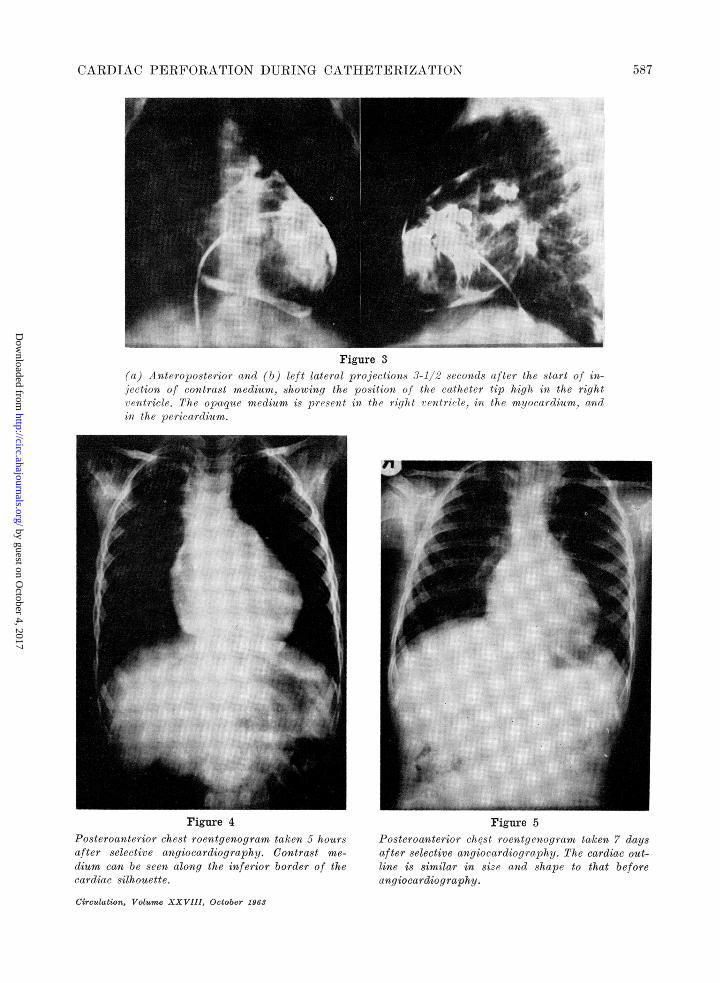
stitutes of Health (NIH) catheter for the per-formance of selective angiocardiography from theright ventricle. Several attempts were made tomaneuver the catheter tip into the apical region ofthe right ventricle, but this aim could not beachieved and the catheter was finally left about thejunction of the body and infundibulum of the rightventricle with its tip close to the left border of thecardiac silhouette. The pressure tracing obtainedhere was distorted as compared with the recordingwith the catheter free in the right ventricle (fig. 1)probably from partial obstruction of the sideholesby myocardial trabeculae. Despite this distortion itwas thought safe to inject the contrast medium.Accordingly, 19 ml. of 76 per cent sodium andmethyl glucamine diatrizoate (Urografin) wereinjected with a Gidlund syringe under a pressureof 5 Kg. per cm.2. Several extrasystoles occurredduring the injection and immediately thereafterthe ST segments were depressed (fig. 2). In ourexperience, these events are unusual. The radio-graphs showed (fig. 3) extravasation of opaquemiiedium into the ventricular muscle and into thepericardial sac, spreading along the proximal por-tions of the pulmonary arterv and aorta under thepericardial reflections. Details of the cardiac anat-omv were obscured to some extent by this extrava-sation, but pulmonarv infundibular stenosis, rightaortic arch, and probable ventricular septal defectwere observed.The patient became pale, the pulse rate was 160
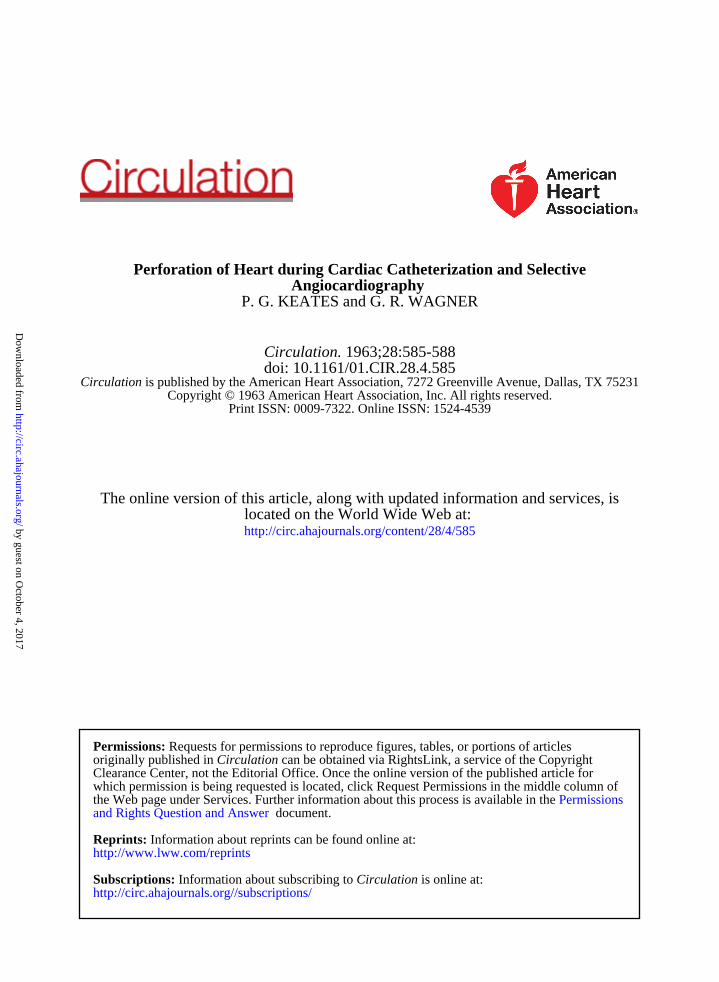
per minute, the blood pressure was 70/40 mm. Hg,and return of conseiousness was slow. He was keptunder close observation, and over the next 10 hoursthe pulse rate decreased to 130 and the blood pres-sure rose to 110/70. A chest film 5 hours after in-jection (fig. 4) showed the cardiac outline to beslightly increased, and a pool of opaque mediumwas present along the inferior border of the heart.Another film 10 hours after injeetion was the same,but 24 hours after injection the opaque mediumdisappeared and an electrocardiogram at that timeshowed that the ST segment was no longer de-pressed and there was no evidence of infarction.
The clinical course over the next week was un-eventful and the patient was discharged 8 daysafter the original test. The radiograph taken onthe day prior to discharge is shown in figure 5. The
Circulation, Volume XXVIII, October 196 6 585
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from
KEATES, WAGNER
Figure 1Right ventricular pressure tracings (in mm. Hg);(a) catheter tip free in the ventricular cavity; (b)coatheter in position for injection of contrast me-dium.
eardiac outline was similar to that before angio-cardiography. The patient has been placed on thewaiting list for operation.
DiscussionIt is generally recognized that complica-
tions cannot be entirely avoided during andafter cardiac catheterization and angiocardi-ography. Their incidence is usually less than2 per cent and often much lower. Thus Kjell-berg et al.1 had one death in 425 cardiac cath-eterizations and three deaths in 340 angiocar-diograms. They state that, even with rapidinjections, the jet of contrast medium is soweak that it is deflected by the intracardiaeblood flow, and that they have not seen anyendocardial damage that could be ascribed tothe jet or to the impact of the catheter. Escheret al.,2 however, recorded the case of a 24-year-old woman with isolated infundibularpulmonary stenosis in whom cardiac cathe-
terization and selective angiocardiographyresulted in perforation of the right ventriclenear its apex. They concluded that the per-foration probably occurred during the inser-tion of the relatively sharp-tipped and rigidNIH catheter, and that another factor respon-sible for the accident was that the catheterwas additionally advanced a short distanceon two occasions after its initial positioningas the arms of the patient were raised abovethe head. In this case cardiac tamponade oc-curred leading to emergency thoracotomvfrom which the patient made a satisfactoryrecovery.A similar case is reported by Hilbish and
Herdt.3 Here the roentgenogram actuallyshows a bulge in the region of the tip of thecatheter and the conclusion reached is thatthe catheter must have perforated the myo-cardium, though on this point there is nogeneral agreement. Thus Dow and Taylor4attach more importance to the high-velocityjet, when injection is made under high pres-sure, than to penetration by the catheter asthe factor largely responsible for perforationof the myocardium.
In our case the catheter tip was at the junc-tion of infundibulum and body of the rightventricle, so that its position for selectiveangiocardiography was not ideal. In addi-tion, there was evidence in the form of thedistorted pressure tracing (fig. 1) that theside-holes of the catheter were not perfectlyfree and since the most proximal hole in thecatheter was 1 cm. from the tip, we conclude
Figure 2Lead II of electrocardiogram. Tracings before injection of contrast medium (a), during(b), and after injection (c). Ventricular extrasystoles occur during the injection, andST-segment depression is seen after it.
Circulation, Volume XXVIII, October 1963
586
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from
CARDIAC PERFORATION DURING CATHETERIZATION
Figure 3(a) Anteroposterior and (b) left lateral projections 3-1/2 seconds after the start of in-jection of contrast medium, showing the position of the catheter tip high in the rightventricle. The op,aque medium is present in the right ventricle, in the myocardium, andin the pericardium.
Figure 4 rigure 5Posteroanterior chest roentgenogram taken 5 hours Posteroanterior chest roentgenogram taken 7 daysafter selective angiocardiography. Contrast me- after selective angiocardiography. The cardiac out-dium can be seen along the inferior border of the line is similar in size and shape to that beforecardiac silhouette. angiocardiography.
Circulation, Volume XXVIII, October 1963
587
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from

5KEATES, WAGNER
that the tip must have been well embedded Inthe myocardium.A study of serial films shows that the
smoothly curved course of the catheter wasflattened during part of the cardiac cycle andat this time the straightening effect must havetended to drive the tip forward into the myo-cardium. The mechanism for the perforationthus appears to us to have been essentiallysimilar to that postulated for the case ofEscher et al.,2 i.e., perforation by the catheterrather than by the jet of contrast medium.
It is well known that small stab wounds inthe heart usually seal spontaneously, and nospecial explanation is needed to account forthe lack of further complications.
In retrospect, we believe that the distortionof the right ventricular pressure tracingshould have been regarded as a warning signthat the side-holes were not free and that itshould have led us to re-position the catheterbefore injecting the contrast medium. Pos-sibly in this way the perforation might havebeen avoided.
SummaryA case is reported in which cardiac cathe-
terization and selective angiocardiographyled to perforation of the heart without anyfurther complications.
It is suggested that distortion of the pres-sure tracing indicates partial obstruction ofthe catheter holes and that it should serve asa warning sign not to proceed with the injec-tion of contrast medium, but to re-positionthe catheter first. Furthermore, inspection ofthe electrocardiogram immediately after theinjection may give an early indicatioii ofmyocardial disturbance in the form of ST-segment depression.
AcknowledgmentWe wish to thank Mr. G. H. Wooler for permis-
sion to publish this case.
References1. KJELLBERG, S. R., MANNHEIMER, E., RUDHE, U.,
AND JONSSON, B.: Diagnosis of CongenitalHeart Disease. Chicago, The Year Book Pub-lishers, Inc., 1955, pp. 94 and 101.
2. ESCHER, D. J. W., SHAPIRO, J. H., RUBINSTEIN,B. M., HURWITT, E. S., AND SCHWARTZ, S. P.:Perforation of the heart during cardiac cathe-terization and selective angiocardiography. Cir-culation 18: 418, 1958.
3. HILBISH, T. F., AND HERDT, J. L. R.: Compli-cations of selective angiocardiography. Radi-ology 75: 197, 1960.
4. Dow, J., AND TAYLOR, D. G.: Angiocardiographictechnic in intracardiae shunts. Brit. J. Radiol.35: 241, 1962.
Medical EtymologyAnother type of change clearly gives us a picture of the status of medical lore in a
given period. Take, for example, the word trachea which was an adjective and meantnothing but rough. It is in the feminine to agree with the word arteria with which it wasoriginally combined. In the time of Aristotle it was believed that the arteria containedair, hence their name, air tubes. Aristotle called the arteries smooth-but he considered thewindpipe a rough artery. What better could tell us of the state of physiology in thatepoch ?-O. H. PERRY PEPPER. Opuscula Medica. (Reprinted from Transactions & Studiesof the College of Physicians of Philadelphia, 4 Ser.. 18: 31, April, 1950).
Circulation, Volume XXVIII, October 1963
588
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from
P. G. KEATES and G. R. WAGNERAngiocardiography
Perforation of Heart during Cardiac Catheterization and Selective
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1963 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.28.4.585
1963;28:585-588Circulation.
http://circ.ahajournals.org/content/28/4/585located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on October 4, 2017
http://circ.ahajournals.org/D
ownloaded from