leadership weekend 2020 presentation-use weekend 2020...criteria median follow up (years) primary...
TRANSCRIPT

1/9/2020
1
Pearls of Practice: Managing Common Conditions in Pharmacy
Presented by:Lindsay Sheehan, PharmD, CDE, CPP
Kayla Morgan, PharmD, CDE, CPP, BCACPKristy Brittain, PharmD, BCPS, CDE
Disclosure
The speakers have no relevant financial relationships to disclose.
1
2
3

1/9/2020
2
Pharmacist Objectives
Upon completion of this activity, the pharmacist will be able to:1. Describe a pharmacist and pharmacy technician’s role in
chronic disease state management 2. Identify updates in diabetes care including current guidelines,
new medications, and continuous glucose monitors3. Summarize changes in the anticoagulation landscape with the
increasing role of Direct Oral Anticoagulants (DOACs)4. Identify updates in asthma care including current guidelines
and new medications5. Apply therapeutic updates to patient case scenarios
Technician Objectives
Upon completion of this activity, the pharmacy technician will be able to:1. Describe a pharmacist and pharmacy technician’s role in
chronic disease state management 2. Identify new medications and devices for use in diabetes,
anticoagulation, and asthma
Type 2 Diabetes Update
4
5
6

1/9/2020
3
9. Pharmacologic Approaches to Glycemic Treatment
› Treatment decisions for Type 2 Diabetes should consider:› Efficacy› comorbidities such as ASCVD, CKD, and heart failure› hypoglycemia risk› effect on body weight› side effects› cost› patient preference
ADA’s Standards of Medical care in Diabetes‐2020
Diabetes Medications Drug/route Efficacy Weight
changeCV effect
ASCVD CHF
Renal Clinical Pearls
Metformin High
↓ hepatic glucose output
Neutral or modest ↓
Potential benefit
Neutral -CI with GFR < 30-If GFR < 45, don’t start-If on metformin and GFR falls to 30-45 consider decreasing dose.
GI side effects common (ER formulation and taking with meals may help)B12 deficiency
SGLT-2 Inhibitors
empagliflozin*canagliflozin*dapagliflozinertugliflozin
Intermediate
↓ glucose reabsorption in kidneys
Loss Benefit*
empa-gliflozin FDA approved for CVD benefit
Benefit
empa-gliflozin, cana-gliflozin, and dapa-gliflozin
Progression of Diabetic Kidney disease: Benefit (canagliflozin, empagliflozin, dapagliflozin)
Renal dose adjustments required. Don't start if GFR < 45 (< 60 for ertugliflozin)
-BBW: Amputation (canagliflozin)-Bone Fractures (canagliflozin)-DKA-Genitourinary infections-Volume depletion, hypotension-increased LDL-Fournier's gangrene
Am erican Diabetes Association. 9. Pharm acologic approaches to glycem ic treatm ent: Standards of M edical Care in Diabetes—2019 [web annotation]. Diabetes Care 2019;42(Suppl. 1):S90–S102.
SGLT2 inhibitors trialsTrial Intervention Main
inclusion Criteria
Median follow up
(years)
Primary outcome
Results/Conclusion
Intervention Placebo
EMPA-REG OUTCOME(n=7,020)
empagliflozin/placebo
Type 2 diabetes and preexisting CVD
3.1 CV death, MI, and stroke
490 patients (10.5%) 282 patients (12.1%)
HR 0.86 [95% CI 0.74-0.99], P=0.04 for superiority. Lower rates of death from CV cause (38% relative risk reduction), hospitalization for HF (35% relative risk reduction, and death from any cause (32% relative risk reduction).
DECLARE-TIMI 58(n=17,160)
dapagliflozin/ placebo
Type 2 DM and established ASCVD or multiple ASCVD risk factors
4.2 CV death, MI, and stroke, or hospital-ization for HF
8.8% 9.4%
Primary safety outcome: noninferiority to placebo with respect to MACE (p<0.001).Primary efficacy outcome: did not lower rate of MACE; HR 0.93 (95% CI 0.84-1.03) P=0.17.Decreased rate of CV death or hospitalization for HF (4.9% vs 5.8% HR 0.83 (95% CI 0.73-0.95) p=0.005).27% reduction in hospitalization for HF
References 7,8. Abbreviations: CV= cardiovascular disease, ASCVD=atherosclerotic cardiovascular disease, MI=myocardial infarction, HF=heart failure, HR=Hazard ratio, CI=confidence interval, MACE=Major Adverse Cardiac Event
7
8
9

1/9/2020
4
SGLT2 inhibitor trials
Trial Intervention Main inclusion Criteria
Median follow up
(years)
Primary outcome
Results/Conclusion
Intervention Placebo
CANVASandCANVAS-R(n=10,142)
canagliflozin/ placebo
Type 2 diabetes and preexisting CVD at >30 years of age or > 2 CVD risk factors at >50 years of age
3.6 CV death, MI, and stroke
26.9 participants/1000
patient-years
31.5 participants/1000 patient-
years
HR 0.86 [95% CI 0.75–0.97]. Canagliflozin significantly reduced the composite outcome.Increased risk of lower limb amputation (6.3 vs 3.4 participants/1000 patient-years, HR 1.97 [95% CI 1.41-2.75].
CREDENCE(n=4,401)
canagliflozin/ placebo
Type 2 DM and chronic diabetes related kidney disease
2.62
trial ended early
End stage kidney disease, doubling of Scr or death from renal or CV causes
43.2 per 1000 patient-years
61.2 per 1000 patient-years
HR 0.70 [95% CI 0.59-0.82], P=0.00001.Relative risk of the primary outcome 30% lower in the canagliflozin arm. Lower risk of CV death, MI, or stroke (HR 0.80 [CI 0.67-0.95] P=0.01) Lower risk of hospitalization for HF (HR 0.61 [CI 0.47-0.80] P<0.001).No difference in rates of amputation or fracture.
References 10, 11.
Diabetes Medications Drug/route Efficacy Weight
changeCV effect
ASCVD CHF
Renal Clinical Pearls
GLP-1 analogs
BID: exenatide Daily: liraglutide, lixisenatideWeekly: exenatide ER, dulaglutide, semaglutide
High
↑ insulin release with foodSlows gastric emptyingPromotes satietySuppresses glucagon
Loss Benefit: liraglutide, sema-glutide, and dula-glutide
Neutral Liraglutide has shown to decrease progression of diabetic kidney disease
-FDA BBW: Thyroid C-cell tumors -GI side effects (nausea, diarrhea, vomiting)-Injection site reactions-possibly acute pancreatitis risk?
DPP-4 inhibitors
alogliptinlinagliptinsaxagliptinsitagliptin
Intermediate
Prolong gut hormone↑ insulin secretionDelay gastric emptying
Neutral Neutral Potential risk with saxagliptin and alogliptin
Renal dose adjustments for all except linagliptin
-Potential risk for pancreatitis -Low risk for hypoglycemia-SE: headache, joint pain, flu-like symptoms
Am erican Diabetes Association. 9. Pharm acologic approaches to glycem ic treatm ent: Standards of M edical Care in Diabetes—2019 [web annotation]. Diabetes Care 2019;42(Suppl. 1):S90–S102.
GLP‐1 analogs and cardiovascular disease trialsTrial Intervention Main
inclusion Criteria
Median follow up
(years)
Primary outcome
Results/Conclusion
Intervention Placebo
LEADER(n=9,340)
Liraglutide/placebo
Type 2 DM, preexisting CVD, CKD, or HF at >50 y/o, or CVD risk at > 60 y/o
3.8 CV death, MI, or stroke
608 patients (13%) 694 patients (14.9%)
HR 0.87 [95% CI 0.78-0.97], P<0.001 for noninferiority, P=0.01 for superiority. 15% reduction in all-cause mortality
SUSTAIN-6(n=3,297)
Semaglutide/placebo
Type 2 DM, preexisting CVD, CKD, or HF at >50 y/o, or CVD risk at > 60 y/o
2.1 CV death, non fatal MI, and nonfatal stroke
108 patients (6.6%) 146 patients (8.9%)
HR 0.74 [95% CI 0.58-0.95], P<0.001 for non-inferiority, P=0.02 for superiority. Powered to test noninferiority. No significant difference in CV mortality.
References 2,3
10
11
12

1/9/2020
5
GLP‐1 analogs and cardiovascular disease trialsTrial Intervention Main
inclusion Criteria
Median follow up
(years)
Primary outcome
Results/Conclusion
Intervention Placebo
EXSCEL(n=14,752)
Exenatide ER/placebo
Type 2 DM with or w/o preexisting CVD
3.2 CV death, MI, or stroke
839 patients (11.4%) 905 patients (12.2%)
HR 0.91 [95% CI 0.83– 1.00], P< 0.001 for noninferiority. Not superior to placebo P=0.06. All-cause mortality was lower in the exenatide arm.
ELIXA(n=6,068)
lixisenatide/ placebo
Type 2 DM, ACS within 180 days
2.1 CV death, MI, stroke, or hospital-ization for unstable angina
406 patients (13.4%) 399 patients (13.2%)
HR 1.2 [95% CI 0.89–1.17]. P<0.001 for non-inferiority, but did not show superiority (P=0.81).
REWIND(n=9,091)
dulaglutide/ placebo
Type 2 DM with preexisting CVD or risk CV risk factors
5.4 CV death (including unknown cause), MI, or stroke
594 patients (12%) 663 patients (13.4%)
HR 0.88 [95% CI 0.79-0.99], P=0.026. All cause mortality did not different between the groups P=0.067.
References 4,5,6. Abbreviation ACS=Acute Coronary Syndrome
Diabetes Medications Drug/route Efficacy Weight
changeCV effect
ASCVD CHF
Renal Clinical Pearls
Thiazolidinediones
pioglitazonerosiglitazone
High
↑ insulin sensitivity
Gain Potential benefit
Increased risk
No dose adjustments, but caution in renal impairment due to fluid retention.
-Avoid in patients with heart failure-monitor weight gain and edema-Bone fractures-Bladder cancer (pioglitazone)
Sulfonylurea
glipizide (XL), glimepiride, glyburide
High
Stimulates insulin release
Gain Neutral Neutral Renal impairment can increase risk of lows. Avoid glyburide, initiate glipizide and glimepiride at lower doses.
-Increased risk of hypoglycemia. Especially with longer acting products.-Cheap
Diabetes Care 2019 Jan; 42 (Supplement 1): S103‐S123. https://doi.org/10.2337/dc19‐S010
Standards of Medical Care in Diabetes Section 9
Pharmacologic Therapy for Type 2 Diabetes
13
14
15

1/9/2020
6
Pharmacologic
Approaches to Glycemic Management:Standards of Medical Care
in Diabetes ‐ 2020. Diabetes Care 2020;43(Suppl. 1):S98-S110
Pharmacologic
Approaches to Glycemic Management:Standards of Medical Care
in Diabetes ‐ 2020. Diabetes Care 2020;43(Suppl. 1):S98-S110
Pharmacologic
Approaches to Glycemic Management:Standards of Medical Care
in Diabetes ‐ 2020. Diabetes Care 2020;43(Suppl. 1):S98-S110
16
17
18

1/9/2020
7
Intensifying to Injectable Therapies
Pharmacologic Approaches to Glycemic
Management:Standards of Medical Care in Diabetes ‐ 2020.
Diabetes Care 2020;43(Suppl. 1):S98-S110
Intensifying to Injectable Therapies
Pharmacologic Approaches to Glycemic
Management:Standards of Medical Care in Diabetes ‐
2020. Diabetes Care 2020;43(Suppl. 1):S98-S110
Intensifying to Injectable Therapies
Pharmacologic Approaches to Glycemic
Management:Standards of Medical Care in Diabetes ‐ 2020.
Diabetes Care 2020;43(Suppl. 1):S98-S110
19
20
21
1/9/2020
8
› First oral GLP‐1 receptor agonist › Indicated in adjunct to diet and exercise to improve BG in
adults with type 2 diabetes› Co‐formulated with salcaprozate sodium which facilitates
absorption in the stomach› Administration:
– Empty stomach and no more than 4 ounces of plain water– > 30 minutes before food, drink, or other medications– Recommend eating 30‐60 minutes after the dose – Do not split, crush, or chew
› Dosing:– 3 mg PO daily x 30 days (not a therapeutic dose)– Then increase to 7 mg PO daily for at least 30 days– If further glycemic control needed can increase to 14 mg PO daily
Oral Semaglutide (RybelsusⓇ)
› Max concentration reached in 1 hour› Steady state achieved in 4‐5 weeks› Precautions:
– not to be used for type 1 DM, pregnancy/lactation, patients < 18 y/o, h/o pancreatitis
› Drug interactions:– insulin and sulfonylureas– levothyroxine
› Patient counseling:– nausea, vomiting, diarrhea most common side effects– thyroid C‐cell tumors seen in rats – stop medication if suspect pancreatitis – worsening renal failure with dehydration
Oral Semaglutide (RybelsusⓇ)
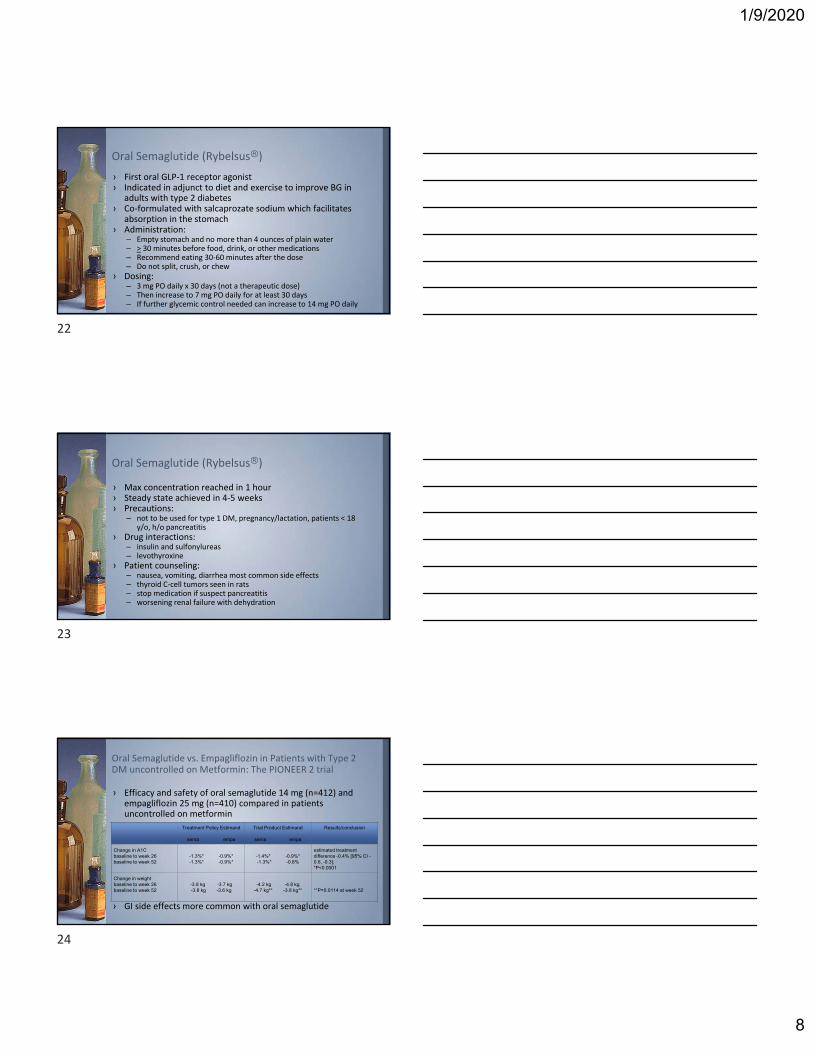
› Efficacy and safety of oral semaglutide 14 mg (n=412) and empagliflozin 25 mg (n=410) compared in patients uncontrolled on metformin
› GI side effects more common with oral semaglutide
Oral Semaglutide vs. Empagliflozin in Patients with Type 2 DM uncontrolled on Metformin: The PIONEER 2 trial
Treatment Policy Estimand
sema empa
Trial Product Estimand
sema empa
Results/conclusion
Change in A1C baseline to week 26 baseline to week 52
-1.3%* -0.9%*-1.3%* -0.9%*
-1.4%* -0.9%*-1.3%* -0.8%
estimated treatment difference -0.4% [95% CI -0.6, -0.3]; *P<0.0001
Change in weight baseline to week 26baseline to week 52
-3.8 kg -3.7 kg-3.8 kg -3.6 kg
-4.2 kg -4.8 kg-4.7 kg** -3.8 kg** **P=0.0114 at week 52
22
23
24
1/9/2020
9
Continuous Glucose Monitors (CGMs)
› Commonly used for diagnosis and assessment of glycemic control
› Cons– Correlates to an average blood sugar– May be inaccurate in some cases
Hemoglobin A1c
› Traditional method for patients and providers to monitor blood sugars on a day‐by‐day basis
› Cons– Painful and cumbersome for patients– Variety of testing supplies required– Checks blood sugar in that specific moment– May require multiple checks throughout the day to get an idea of
trends
Fingerstick Blood Glucose Monitoring
25
26
27

1/9/2020
10
› Typically consists of a sensor, transmitter, and reader/receiver– Sensor is inserted under the skin (usually abdomen or back of arm)– Sensor measures interstitial glucose– Transmitter sends information wirelessly to a reader/monitor
› Allows for continuous feedback on glucose› Data can be downloaded to computer or smart device
Continuous Glucose Monitoring (CGM)
› Takes time for glucose to diffuse from the capillary to the interstitial space– Interstitial glucose tends to lag behind if blood sugars are rapidly
changing
Interstitial Glucose vs. Blood Glucose
› Shows glucose trends and provides dynamic data about direction blood sugar is heading
› Continuous feedback of impact of medications, diet, and exercise on sugars
› Some products alert users to hypoglycemia– Safer for patients with hypoglycemia unawareness
› Requires fewer fingersticks› May improve glycemic control and reduce glycemic
variability
Benefits of CGM
28
29
30

1/9/2020
11
Available Personal CGM SystemsCGM System Details
Sensor Duration
Warm-Up Time
Calibration
Abbott FreeStyle Libre Personal® ▪ Records data every 15 minutes
▪ Does not communicate continuously with reader; Must scan every 8 hours
▪ Reader has built-in blood glucose meter▪ Compatible with iPhone 7 and later through the LibreLinkTM
app▪ Displays current sensor glucose reading, visual alerts, and
trend arrows▪ Has text-to-speech option when enabled
14 days 1 hour Not required
Dexcom G6®
▪ Collects glucose readings every 5 minutes▪ Transmitter battery lasts 3 months▪ Receiver can include a touch-screen receiver, smartphone,
smartwatch, or Tandem X2 insulin pump▪ Application available in Apple App Store and Google Play
Store▪ Displays current sensor glucose reading, trend arrows, and
customizable alerts/alarms
Up to 10 days
2 hours
Not required
Can choose to calibrate
American Diabetes Association. Continuous glucose monitors- Consumer Guide 2018. Diabetes Forecast. http://main.diabetes.org/dforg/pdfs/2018/2018-cg-continuous-glucose-monitors.pdf (accessed Jan. 6, 2019).FreeStyle LibreLink App. Freestyle Libre. https://www.freestylelibre.us/system-overview/continous-glucose-monitor-app.html (accessed Jan. 19, 2019).Abbott’s Freestyle Libre 14 day flash glucose monitoring system now approved in U.S. Abbott. https://abbott.mediaroom.com/2018-07-27-Abbotts-FreeStyle-R-Libre-14-Day-Flash-Glucose-Monitoring-System-Now-Approved-in-U-S (accessed Jan. 19, 2019). Dexcom G6 continuous glucose monitoring system user guide. Dexcom, Inc. https://s3-us-west-2.amazonaws.com/dexcompdf/G6-CGM-Users-Guide.pdf?_ga=2.61291948.1830682920.1549243176-1258106527.1549243176 (accessed Jan. 19, 2019).Images: Continuous glucose monitoring system. Freestyle Libre. https://www.freestylelibre.us/ (accessed Jan. 19, 2019).Make knowledge your superpower with the new Dexcom G6® CGM. Dexcom, Inc. https://www.dexcom.com/get-started-cgm/40?sfc=701f30000018vibAAA&gclid=EAIaIQobChMIw-2n_IbV4AIV0pCfCh2HJwTQEAAYASAAEgLAsvD_BwE (accessed Jan. 19, 2019).
Available Personal CGM Systems
CGM System DetailsSensor
DurationWarm-Up
TimeCalibration
Medtronic Guardian Connect 3®▪ Collects glucose readings every 5 minutes▪ Compatible with Apple devices▪ Does not require purchase of extra device▪ Uses rechargeable transmitter which must be recharged
weekly▪ Displays sensor glucose data, trends, and
customizable/predictive alerts▪ Determines glucose patterns using Sugar.IQTM Diabetes
Assistant ▪ Data automatically uploads to CareLinkTM Personal software
Up to 7 days 2 hoursAt least twice
daily; Every 12 hours
Senseonics Eversense XL®
▪ Sensor is professionally inserted under skin▪ Transmitter with rechargeable battery is placed on top of
sensor placement site▪ Automatically sends glucose reading to mobile app every 5
minutes▪ Provides on-body vibrating alerts when glucose is low or high▪ Displays sensor glucose data, trends, and
customizable/predictive alerts
Up to 90 days
24 hours2-4 times daily depending on
calibration phase
Guardian Connect vs. Freestyle Libre. Medtronic Diabetes. https://guardianconnect.medtronic-diabetes.co.uk/guardian-connect-vs-freestyle-libre# (accessed January 19, 2019).American Diabetes Association. Continuous glucose monitors- Consumer Guide 2018. Diabetes Forecast. http://main.diabetes.org/dforg/pdfs/2018/2018-cg-continuous-glucose-monitors.pdf (accessed January 6, 2019).Eversense User Guide. Food and Drug Administration. https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160048c.pdf (accessed February 6, 2019).Images: Guardian Connect CGM System. Medtronic Diabetes. https://www.medtronicdiabetes.com/products/guardian-connect-continuous-glucose-monitoring-system (accessed January 19, 2019).Eversense: the only long-term continuous glucose monitoring (CGM) system. Senseonics, Inc. https://www.eversensediabetes.com/products/ (accessed February 6, 2019).
Comparing Personal CGM Features
FeaturesAbbott FreeStyle Libre Personal®
Dexcom G6® Medtronic Guardian Connect 3®
Senseonics Eversense XL®
No Calibration Required X X
Ability to Share Data X X X X
Customizable Alerts X X X
Predictive Alerts X X X
Handheld Reader/ Receiver Available
X X
Compatible with Apple Products X X X X
Compatible with Android Products X X X
Equipped with Data Analysis System
X
Location of Sensor Placement Back of Upper ArmAbdomen,
Upper Buttocks*Abdomen Upper Arm
Mean Absolute Relative Difference
9.4% 9.0% 9.1% 8.5%
*Only for patients 2-17 years old
Continuous glucose monitoring system. Freestyle Libre. https://www.freestylelibre.us/ (accessed Jan. 19, 2019).Abbott’s Freestyle Libre 14 day flash glucose monitoring system now approved in U.S. Abbott. https://abbott.mediaroom.com/2018-07-27-Abbotts-FreeStyle-R-Libre-14-Day-Flash-Glucose-Monitoring-System-Now-Approved-in-U-S (accessed Jan. 19, 2019). Dexcom G6 continuous glucose monitoring system user guide. Dexcom, Inc. https://s3-us-west-2.amazonaws.com/dexcompdf/G6-CGM-Users-Guide.pdf?_ga=2.61291948.1830682920.1549243176-1258106527.1549243176 (accessed Jan. 19, 2019).Guardian Connect CGM System. Medtronic Diabetes. https://www.medtronicdiabetes.com/products/guardian-connect-continuous-glucose-monitoring-system (accessed January 19, 2019).Eversense User Guide. Food and Drug Administration. https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160048c.pdf (accessed February 6, 2019).
31
32
33
1/9/2020
12
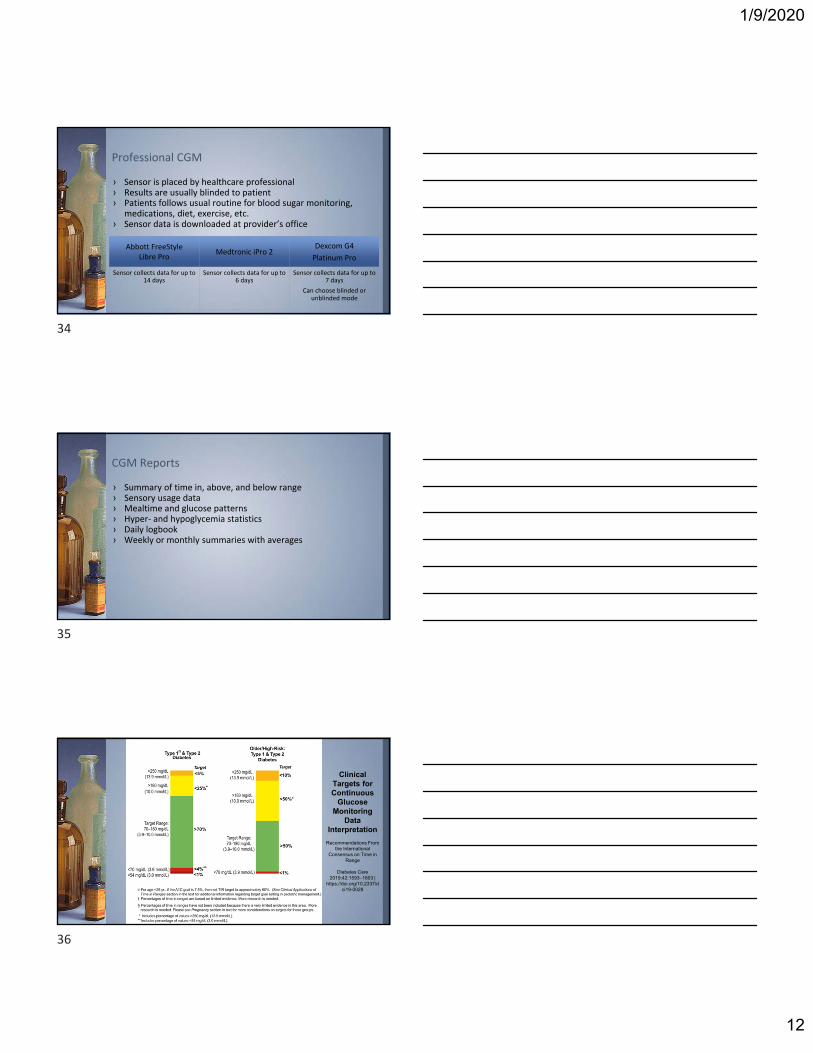
› Sensor is placed by healthcare professional› Results are usually blinded to patient› Patients follows usual routine for blood sugar monitoring,
medications, diet, exercise, etc.› Sensor data is downloaded at provider’s office
Professional CGM
Abbott FreeStyle Libre Pro
Medtronic iPro 2Dexcom G4
Platinum Pro
Sensor collects data for up to 14 days
Sensor collects data for up to 6 days
Sensor collects data for up to 7 days
Can choose blinded or unblinded mode
› Summary of time in, above, and below range› Sensory usage data› Mealtime and glucose patterns› Hyper‐ and hypoglycemia statistics› Daily logbook› Weekly or monthly summaries with averages
CGM Reports
Clinical Targets for Continuous
Glucose Monitoring
Data Interpretation
Recommendations From the International
Consensus on Time in Range
Diabetes Care 2019;42:1593–1603 |
https://doi.org/10.2337/dci19-0028
34
35
36

1/9/2020
13
Example CGM report: Glucose Pattern Summary
37
Example CGM report
38
Monthly Summary
37
38
39

1/9/2020
14
Example CGM report: Daily summary
40
Example Personal CGM report: Daily summary
41
Anticoagulation Update
40
41
42

1/9/2020
15
› Atrial fibrillation
› Venous thromboembolism
› Cerebrovascular accident
› Myocardial infarction
› Prosthetic heart valves
› Hypercoagulable states
Common Indications for Anticoagulation
› Changing prescribing landscape
› Expanded indications
› Expanded contraindications/precautions
› Atrial fibrillation guideline update
› National patient safety goals
So what is new?
› Vitamin K antagonists (VKA), such as warfarin, have been the mainstay of oral anticoagulation therapy for many years
› Direct oral anticoagulants (DOACs) are now commonly prescribed alternatives
› DOACs may serve as more appealing therapy choices than warfarin
Changing Anticoagulation Landscape
Shehab N, Lovegrove MC, Geller AI. US Emergency Department Visits for Outpatient Adverse Drug Events, 2013-2014.JAMA. 2016 Nov 22;316(20):2115-2125.
43
44
45

1/9/2020
16
DOAC Pros
› Less frequent monitoring› Fixed dosing› Fewer drug interactions› Fewer diet interactions› Rapid onset› Short half‐life› Improved safety profile in
trials
What’s the big deal?
DOAC Cons
› Monitoring still requires› Dose adjustments› Drug interactions still exist› Strict adherence needed› Cost› Less frequent contact with
healthcare professionals› False perception of safety
Burnett AE, Mahan CE, Vazquez SR, et. al. Guidance for the practical management of the direct oral anticoagulants (DOACs) in VTE treatment. J Thromb Thrombolysis. 2016 Jan;41(1):206-32.
› Most common prescribing errors: dosing, administration, duration
› Several studies suggest inappropriate DOAC dosing occurs in 12.8‐34% of patients
Appropriateness of DOAC Prescribing
Whitworth MM, Haase KK, Fike DS, et. al. Utilization and prescribing patterns of direct oral anticoagulants. Int J Gen Med. 2017. 10: 87–94.Moudallel S, Steurbaut S, Cornu P, Dupont A. Appropriateness of DOAC Prescribing Before and During Hospital Admission and Analysis of Determinants
for Inappropriate Prescribing. Front Pharmacol. 2018; 9:1220.
Commercial
› Copay assistance cards› Deductible issue
Medicare
› Deductible up to $415› Copay $25‐45› Coverage gap after $3,820› Catastrophic coverages after $8,139
Manufacturers Patient Assistance Programs
Medicare’s Extra Help Program
CostDOAC AWP
per 30 days
Copay Card
per 30 days*
apixaban $533 $10
rivaroxaban $540 $10
dabigatran $519 $0
edoxaban $436 $4
betrixaban $540 $50 first fill
$0 after
*Eligibility and restrictions apply
46
47
48

1/9/2020
17
Centers for Disease Control and Prevention (CDC) study (2016):
› Oral anticoagulants caused more emergency department visits than any other class of drugs
› >50% of these visits led to hospitalization
Anticoagulants and ER Visits/Hospitalizations
Shehab N, Lovegrove MC, Geller AI. US Emergency Department Visits for Outpatient Adverse Drug Events, 2013-2014.JAMA. 2016 Nov 22;316(20):2115-2125.
Vitamin K Antagonist and Direct Oral Anticoagulants (DOACs)
Anticoagulants
Anticoagulants: Vitamin K Antagonist
Drug Indication Dose Dose Adjustments Clinical Pearls
warfarin -Atrial fibrillation-Venous thromboembolism prevention and treatment-Embolism prophylaxis and treatment in setting of prosthetic cardiac valves-Reduce risk of embolism following MI
Individualized based on patient specific factors and INR
Renal: No adjustments
Hepatic: Monitor closely and adjust based on INR
Drug Interactions: Monitor closely and adjust based on INR
-Consistency from week to week and open communication with managing providers is key
Coumadin (warfarin) [package insert].Princeton, New Jersey: Bristol-Myers Squibb Company; 2011.
49
50
51

1/9/2020
18
Anticoagulants: Direct Thrombin Inhibitors
Drug FDA Approved Indications
Dose Dose Adjustments Clinical Pearls
dabigatran Atrial fibrillation 150mg BID Renal:Atrial fibrillation:
CrCl 15-30mL/min: 75mg BIDDVT/PE:
CrCl <30mL/min: No recommendationVTE Prevention Post-hip:
CrCl <30mL/min: Avoid use
Hepatic:Mod impairment (Child-Pugh B):
No adjustmentSevere impairment:
Use not recommended
Drug Interactions:P-gp inhibitors
Afib with CrCl 30-50 mL/min: 75mg BIDVTE or CrCl < 30 mL/min: avoid use
Take 2 hours before verapamil, H2 blockers, PPIs
-Cannot be given via tube
-60% dialyzed out
-Store in original container; use open bottle within 4 months
-Discontinuation prior to surgery
- CrCl ≥50: 1-2 days- CrCl <50: 3-5 days
DVT/PE treatment and prevention of recurrence
150mg BID after 5-10 days or parenteral anticoagulant
VTE prevention post-hip replacement
110mg x 1, then 220mg daily x 28-35 days post-op
Pradaxa (dabigatran) [package insert].Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc; 2019.
Anticoagulants: Factor Xa Inhibitors
Drug FDA Approved Indications
Dose Dose Adjustments Clinical Pearls
rivaroxaban Atrial fibrillation 20mg daily with evening meal
Renal:Atrial fibrillation:
CrCl 15-50mL/min: 15mg dailyCrCl <15mL/min: Avoid use
DVT/PE:CrCl <30mL/min: Avoid use
VTE Prevention Post-hip:CrCl <30mL/min: Avoid use
Hepatic:Child-Pugh B or C: Avoid use
Drug Interactions:P-gp inhibitors + strong CYP3A4 Inhibitors (ketoconazole, itranzonazole, ritonavir, conivaptan): Avoid useP-gp inducers + strong CYP3A4 Inducers (carbamazepine, phenytoin, rifampin, St John’s wort): Avoid use
-Can be crushed and given via G-tube; not J-tubes
-Not dialyzable
-Discontinuation prior to surgery
- 24hr low risk bleed- 48hr high risk bleed
DVT/PE treatment
15mg BID with food x 21 days, then 20mg daily with evening meal
DT/PE prevention of recurrence
After 6 months of treatment: 10mg daily
VTE prevention post-hip or knee replacement
10mg dailyx12 days kneex 35 days hip
Xarelto (rivaroxaban) [package insert].Titusville, NJ: Janssen Pharmaceuticals, Inc; 2019.
Anticoagulants: Factor Xa Inhibitors
Drug FDA Approved Indications
Dose Dose Adjustments Clinical Pearls
rivaroxaban Reduction of CV death, MI, stroke in chronic CAD or PAD
2.5mg BID + aspirin 75-100 mg daily
Xarelto (rivaroxaban) [package insert].Titusville, NJ: Janssen Pharmaceuticals, Inc; 2019.
52
53
54

1/9/2020
19
› Randomized 27,395 patients with stable CAD or PAD to rivaroxaban 2.5mg BID + aspirin, rivaroxaban 5mg BID, or aspirin 100mg daily
COMPASS Trial
Major bleeding events more common in rivaroxaban + aspirin group vs aspirin alone (3.1% vs. 1.9%, HR 1.7; 95% CI 1.40‐2.05; P<0.001)‐ Mostly GI bleeds‐ No difference in fatal bleeding,
intracranial bleeding, or critical organ bleeding
Eikelboom JW, Connolly SJ, Bosch K, et. al. N Engl J Med. 2017 Oct 5; 377(14): 1319-1330.
Anticoagulants: Factor Xa Inhibitors
Drug FDA Approved Indications
Dose Dose Adjustments Clinical Pearls
apixaban Atrial fibrillation 5mg BID Renal:Atrial fibrillation:
At least 2 of : Age ≥80, Wt <60kg, SCr ≥1.5: 2.5mg BID
DVT/PE:No adjustment
VTE Prevention Post-hip:No adjustment
Hepatic:Severe: Avoid use
Drug Interactions:P-gp inhibitors + strong CYP3A4 Inhibitors (ketoconazole, itranconazole, ritonavir, conivaptan): 2.5mg BID or Avoid useP-gp inducers + strong CYP3A4 Inducers (carbamazepine, phenytoin, rifampin, St John’s wort): Avoid use
-Can be crushed and given via tubes
-Not dialyzable
-Discontinuation prior to surgery
- 24hr low risk bleed- 48hr high risk bleed
DVT/PE treatment
10mg BID x 7 days, then 5mg BID
DT/PE prevention of recurrence
After 6 months of treatment: 2.5mg BID
VTE prevention post-hip or knee replacement
2.5mg BIDx12 days kneex 35 days hip
Eliquis (apixaban) [package insert].Princeton, NJ: Bristol-Myers Squibb Company. New York, NY: Pfizer Inc; 2019.
55
56
57

1/9/2020
20
Anticoagulants: Factor Xa Inhibitors
Drug FDA Approved Indications
Dose Dose Adjustments Clinical Pearls
edoxaban Atrial fibrillation 60mg once daily
Renal:Atrial fibrillation:
CrCl >95 mL/min: Avoid useCrCl 15-50 mL/min: 30mg dailyCrCl <15 mL/min: Avoid use
DVT/PE:CrCl 15-50 mL/min: 30mg dailyCrCl <15 mL/min: Avoid use
Hepatic:Moderate or severe: Avoid use
Drug Interactions:Strong P-gp inhibitors in DVT/PE patients (quinidine, verapamil, azithromycin, clarithromycin, erythromycin, itraconazole, ketoconazole): 30mg daily Rifampin: Avoid use
-Can be crushed and given via tubes
-Not dialyzable
-Discontinuation prior to surgery
- 24hr low risk bleed- 48hr high risk bleed
DVT/PE treatment
60mg once daily after 5-10 days of parenteral anticoagulant
Savaysa (edoxaban) [package insert].Basking Ridge, NJ: Daiichi Sankyo, Inc; 2019.
Anticoagulants: Factor Xa Inhibitors
Drug FDA Approved Indications
Dose Dose Adjustments Clinical Pearls
betrixaban Prophylaxis of VTE in patients hospitalized for acute medical illness who are at risk for VTE complications due to moderate or severe restricted mobility and other risk factors
160mg x 1, then 80mg daily with food x 35-42 days
Renal:CrCl 15-30 mL/min: 80mg x 1, 40mg daily x 35-42 days
Hepatic:Not recommended
Drug Interactions:Strong P-gp inhibitors (amiodarone, azithromycin, verapamil, ketoconazole, clarithromycin): 80mg x 1, 40mg daily
-Unknown if dialyzable
Bevyxxa (betrixaban) [package insert].South San Francisco, CA: Portola Pharmaceuticals, Inc; 2019.
58
59
60

1/9/2020
21
2019 AHA/ACC/HRS Focused Update on 2014 Guideline for Management of Patients with Atrial Fibrillation
January CT, Wann LS, Calkins H, et al. Circulation. 2019; 140: e125-e151.
Section 4.1.1: Selection of Anticoagulant Regimen
› Oral anticoagulants recommended for high risk patients – Now includes edoxaban
› Exclusion criteria for CHA2DS2‐VASc and use of DOACs– Defined as moderate to severe mitral stenosis or mechanical
heart valves› Based on RE‐ALIGN trial, mechanical heart valves are a
contraindication to all DOACs
Atrial Fibrillation Guideline Update
January CT, Wann LS, Calkins H, et al. Circulation. 2019; 140: e125-e151.
› Patients with aortic or mitral valve replacement were assigned 2:1 to either dabigatran or warfarin
› Terminated prematurely due to excess off thromboembolic and bleeding events with dabigatran– Ischemic stroke: 5% with dabigatran vs 0% with warfarin– Major bleeding: 4% with dagibatran vs 2% with warfarin
RE‐ALIGN: Dabigatran versus Warfarin in Patients with Mechanical Heart Valves
Eikelboom JW, Connolly SJ, Brueckmann M, et. al. N Engl J Med. 2013; 369: 1206-1214.
61
62
63

1/9/2020
22
Section 4.1.1: Selection of Anticoagulant Regimen
› DOACS in patients with renal/hepatic impairment– All DOACs have FDA approval for use in some degree of renal
dysfunction– Dabigatran, rivaroxaban, and edoxaban NOT recommended in
end‐stage CKD– Use of warfarin or apixaban may be reasonable in
dialysis‐dependent patients – DOACs not recommended in severe hepatic impairment
Atrial Fibrillation Guideline Update
January CT, Wann LS, Calkins H, et al. Circulation. 2019; 140: e125-e151.
Section 6.1.1: Prevent on Thromboembolism
› Atrial fibrillation or flutter >= 48 hr (or when duration unknown) anticoagulation is recommended for at least 3 weeks prior and 4 weeks after cardioversion– Upgraded to Class I Recommendation
› Atrial fibrillation or flutter <48 hr with CHA2DS2‐VASc >= 2 in mean and >= 3 in women, administration of heparin or DOAC is reasonable as soon as possible before cardioversion– Downgraded to Class IIa
Atrial Fibrillation Guideline Update
January CT, Wann LS, Calkins H, et al. Circulation. 2019; 140: e125-e151.
NEW RECOMMENDATIONS
› DOACS recommended over warfarin where eligible except in those with moderate‐severe mitral stenosis or mechanical heart valve
› Weight loss and risk factor modification is recommended for overweight/obese patients
Atrial Fibrillation Guideline Update
January CT, Wann LS, Calkins H, et al. Circulation. 2019; 140: e125-e151.
64
65
66

1/9/2020
23
› 4 RCT comparing DOACs to warfarin– Consistent non‐inferiority evidence for combined end
point of stroke or systemic embolism– Superior safety profile
› DOACS recommended as first line therapy for eligible patients
DOACs vs. warfarin
Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–51.Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–91.
Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–92. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–104.
https://medium.com/@rajeetsingh/once-you-see-a-bandwagon-its-too-late-e067c94529c4https://engagevideomarketing.com/case-study/why-you-cant-just-jump-on-the-online-id b d /
› Autoimmune disorder where antibodies attack phospholipids
› Increased risk for venous and arterial embolism › May never have signs or symptoms until experience a
thrombotic event› Diagnosis requires antibody testing
Antiphospholipid Syndrome (APS)
Meroni PL, Borghi MO, Raschi E, Tedesco F. Pathogenesis of antiphospholipid syndrome: understanding the antibodies. Nature Reviews Rheumatology. 2011. 7: 330-339.
67
68
69

1/9/2020
24
› Increased rate of recurrent thrombotic events when treated with DOAC compared to warfarin– APS triple positive (lupus anticoagulant, anticardiolipin, and anti‐
beta‐2 glycoprotein I antibodies) are at highest risk for treatment failure
› Consider switching patients with APS to warfarin
Anticoagulant Choice with APS
Pengo V, Denas G, Zoppellaro G, et al. Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood. 2018. 132(13): 1365–71.
NPSG.03.05.01: Reduce the likelihood of patient harm associated with the use of anticoagulant therapy.
› Revised July 2019 to include DOAC management› Acknowledges rise in adverse drug events associated with
DOACs
National Patient Safety Goal (NPSG)
The Joint Commission on Accreditation of HealthCare Organizations. National Patient Safety Goal for Anticoagulant Therapy. Retrieved from: https://www.jointcommission.org/assets/1/18/R3_19_Anticoagulant_therapy_FINAL2.PDF
EP 1: Approved protocols and evidence‐based practice guidelines for the initiation and maintenance of anticoagulant therapy that address:
› Medication selection› Dosing› Drug‐drug interactions› Drug‐food interactions
NPSG Elements of Performance
The Joint Commission on Accreditation of HealthCare Organizations. National Patient Safety Goal for Anticoagulant Therapy. Retrieved from: https://www.jointcommission.org/assets/1/18/R3_19_Anticoagulant_therapy_FINAL2.PDF
70
71
72

1/9/2020
25
EP 4: Written policy addressing the need for baseline and ongoing laboratory tests to monitor and adjust anticoagulant therapy
EP6: Provides education to patients and families specific to the anticoagulant medication prescribed
NPSG Elements of Performance
The Joint Commission on Accreditation of HealthCare Organizations. National Patient Safety Goal for Anticoagulant Therapy. Retrieved from: https://www.jointcommission.org/assets/1/18/R3_19_Anticoagulant_therapy_FINAL2.PDF
› Ensure appropriate indication› Ensure appropriate dose› Manage drug interactions› Address barriers
– cost– adherence
› Monitoring› Patient education› Perioperative management› Transitions of care
Role of Pharmacists
› Indication› Dosing and administration› Adherence› Importance of monitoring and follow ups› Potential adverse events
– Signs/symptoms of thrombosis– Signs/symptoms of bleeding
› Potential drug interactions› Periprocedural management
Education
73
74
75
1/9/2020
26
Available studies suggest pharmacist‐run DOAC education and monitoring services may reduce medication related adverse drug events
Reduce expenses through avoided complications
› ADEs› Emergency room visits› Hospital admissions
Pharmacist Impact
Shore S, Carey EP, Turakhia MP, et. al. Adherence to dabigatran therapy and longitudinal patient outcomes: Insights from the Veterans Health Administration. Am Heart J. 2014 Jun. 167(6): 810–817.
Erikson AK. Pharmacist management improves dabigatran adherence. PharmacyToday. 2015 Jun. 21 (6): 12.Ashjian E, Kurtz B, Renner E, et. al. Evaluation of a pharmacist-led outpatient direct oral anticoagulant service. Am J Health Syst Pharm. 2017 Apr 1;74(7):483-489.
› Extremes of body weight
› Age
› Renal dysfunction
› Hepatic dysfunction
Dosing in Special Populations
Weight > 120 kg and/or BMI > 40 kg/m2
› Concern for inadequate dosing/thrombosis› Limited clinical date› International Society of Thrombosis and Hemostasis and
Anticoagulation Forum recommend against use of DOACS in this population
Weight < 49 kg
› Concern for drug accumulation and toxicity
Extremes of Body Weight
Atrium Health. November 2018. Direct Oral Anticoagulants (DOACs) Pharmacy Dosing Guideline. Unpublished internal document.Martin K, Beyer-Westendorf J, Davidson BL, Huisman MV, Sandset PM, Moll S. Use of the direct oral anticoagulants in obese patients: guidance from the SSC of the ISTH. J
Thromb Haemost 2016; 14:1308-1313.
76
77
78

1/9/2020
27
› Increasing age can increase risk of bleeding› Close attention to renal function› Fall risk
Age
Atrium Health. November 2018. Direct Oral Anticoagulants (DOACs) Pharmacy Dosing Guideline. Unpublished internal document.Benedetti G, Neccia M, Agati L. Direct oral anticoagulants in elderly patients with non valvular atrial fibrillation: state of evidence. Minerva Cardioangiol. 2018 Jun; 66 (3):301-313.
DOAC Elimination
Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol 2018; 71: 2162.
› Safe and effective with mild‐to‐moderate impairment
› Insufficient evidence to predict safety and efficacy with CrCl
<30 mL/min
› Severe/end‐stage CKD (non‐hemodialysis with CrCl <15)
– <20 mL/min mostly excluded from trials
› End‐Stage CKD on diaylsis
– Apixaban: no dose adjustment necessary if
treatment/ppx DVT/PE or if afib and not >= 80yo with
body wt <= 60kg
– Recommendation based on a SINGLE PK/PD study
Renal Dysfunction
Atrium Health. November 2018. Direct Oral Anticoagulants (DOACs) Pharmacy Dosing Guideline. Unpublished internal document.Ha JT, et al. Benefits and Harms of Oral Anticoagulant Therapy in Chronic Kidney Disease: A Systematic Review and Meta-analysis. Ann Intern Med. 2019; 171(3):181-189.
79
80
81

1/9/2020
28
› Increased risk for thrombosis
– Decreased production of endogenous anticoagulants
(Protein C, antithrombin)
– High circulating levels of procoagulants
– Increased platelet aggregation
– High risk of VTE even with increased INR
› Increased risk for bleeding
– Decreased production of coagulation factors
– Thrombocytopenia
– Increased fibrinolysis
Hepatic Dysfunction
Qamar A, Vaduganathan M, Greenberger NJ, Giugliano RP. Oral anticoagulation in patients with liver disease. J Am Coll Cardiol 2018; 71: 2162.
› Consider for– Extremes of body weight– Drug interactions– Renal impairment– Elderly– Treatment failure– Acute bleeding
› Issues/Concerns– High interpatient variability– No defined therapeutic ranges– Availability of drug‐specific assays
Lab Monitoring: Anti‐Xa Levels
Goddelin RC, Adcock DM, Douxfils J. An update on laboratory assessment for direct oral anticoagulants (DOACs). Int J Lab Hematol. 2019 May;41 Suppl 1:33-39.Connors JM. Testing and monitoring direct oral anticoagulants. Blood. 2018 Nov 8;132(19):2009-2015
82
83
84

1/9/2020
29
› Renal and Hepatic Function› Hemoglobin/Hematocrit
› Frequency?– Limited evidence– Facility/provider specific– Rule of Thumb
› Baseline› Repeat at least yearly
Other Monitoring
Atrium Health. November 2018. Direct Oral Anticoagulants (DOACs) Pharmacy Dosing Guideline. Unpublished internal document.January CT, Wann LS, Calkins H, etal. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With
Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2019;Jan 28:[Epub ahead of print].
Conway SE, Hwang AY, Ponte CD et al. Laboratory and Clinical Monitoring of Direct Oral Anticoagulants: What Clinicians Need to Know. Pharmacotherapy 2017; 37(2)236-248
› Changing prescribing landscape
› Expanded indications
› Expanded contraindications/precautions
› Atrial fibrillation guideline update
› National patient safety goals
So what is new?
Asthma Update
85
86
87

1/9/2020
30
● 25.7 million people in the United States (8.4% of the population)○ Globally 1‐18% of the population○ Most common chronic disease among children (highest 0‐17 years)
● Accounts for 1.6% of all ambulatory care visits○ 10.6 million physician office visits○ 1.2 million hospital outpatient visits
● Leading case of preventable hospitalizations in the US○ 479,000 hospitalizations○ 2.1 million ED visits
Asthma
● “Pediatric” disease as most are diagnosed by 5 years of age○ Up to 50% of patients have symptoms by the age of 2 ○ 30‐40% of cases persist into adulthood
● Low mortality rate (80‐90% are preventable)○ Most deaths occur out of the hospital○ Deaths due to (1) inadequate assessment OR (2) inadequate
therapy○ EDUCATION AND ACCESS ARE KEY!
Asthma
Genetic predisposition and environmental interactions
● Socioeconomic status● Family size● Exposure to second‐hand smoke● Allergen exposure● Ambient air pollution● Urbanization● Viral respiratory infections (RSV, rhinovirus)
Risk Factors for Asthma
88
89
90

1/9/2020
31
Genetic predisposition and environmental interactions
● Socioeconomic status● Family size● Exposure to second‐hand smoke● Allergen exposure● Ambient air pollution● Urbanization● Viral respiratory infections (RSV, rhinovirus)
Lower risk of asthma: children exposed to bacteria, those with large number of older siblings, early enrollment in childcare, exposure to cats/dogs/farm animals, low antibiotic exposure
Risk Factors for Asthma
● Atophy● Onset during school age● Presence of bronchial hyper‐responsiveness (BHR)
Predictors of Adult Asthma
● Airflow obstruction● BHR● Airway inflammation
● Disease of exacerbation and remission
Characteristics of Asthma
91
92
93

1/9/2020
32
● Shortness of breath● Chest tightness● Coughing (particularly at night)● Wheezing● Whistling sound while breathing
*Occur in association with exercise/allergens or spontaneously
● Expiratory wheezing on auscultation, dry hacking cough, or signs of atophy
● Laboratory: spirometry, peak expiratory flow
Clinical Presentation of Asthma
● Poor inhaler technique● Poor medication adherence● Incorrect diagnosis of asthma● Comorbid/complication factors/conditions● Ongoing exposure to sensitizing or irritant agents
Contributors to Poor Control of Asthma
94
95
96

1/9/2020
33
● Poor inhaler technique● Poor medication adherence● Incorrect diagnosis of asthma● Comorbid/complication factors/conditions● Ongoing exposure to sensitizing or irritant agents
Contributors to Poor Control of Asthma
● Watch the patient use their inhaler.○ Watch pa ent → Show correct method → Watch again
● Discuss adherence and barriers to use.○ Ask about beliefs, cost of medications and refill frequency.○ Empathetic discussion.
● If possible, remove potential risk factors○ Smoking, beta‐blockers, NSAIDs, allergen exposure
● Assess/manage comorbidities○ Rhinitis, obesity, GERD, obstructive sleep apnea,
depression/anxiety● Consider step‐up treatment
Investigating Poor Symptoms Control
● Aerosol therapy: site specific and enhances therapeutic ratio○ Short‐acting beta agonists: rapid bronchodilation○ Inhaled corticosteroids: enhanced lung activity with minimal
systemic activity
Treatment of Asthma
97
98
99

1/9/2020
34
Short acting beta‐agonists (SABA)
Long acting beta‐agonists (LABA)
Inhaled corticosteroids (ICS)
LABA/ICS Combinations
Common Products in Use Today
100
101
102

1/9/2020
35
SABAs and LABAs
SABA
Albuterol HFA MDI or Respiclick ProAir HFA, Proventil HFA, Ventolin HFA
Albuterol Nebulizer Solution AccuNeb
Levalbuterol HFA MDI Xopenex HFA
Levalbuterol Nebulizer Solution Xopenex
LABA
Formoterol DPI Foradil Aerolizer
Salmeterol DPI Serevent Diskus
Vilanterol In combination products only
ICSs
Beclamethasone HFA MDI Qvar
Budesonide DPI Pulmicort Flexhaler
Budesonide Nebulizer Solution Pulmicort Respules
Ciclesonide HFA MDI Alvesco
Fluticasone HFA MDI Flovent HFA
Fluticasone DPI Flovent Diskus
Fluticasone DPI Arnuity Ellipta
Mometasone DPI Asmanex Twisthaler
ICS/LABA Combos
Budesonide / Formoterol HFA MDI Symbicort
Mometasone / Formoterol HFA MDI Dulera
Fluticasone / Salmeterol DPI Advair Diskus
Fluticasone / Salmeterol HFA Advair HFA MDI
Fluticasone / Vilanterol DPI Breo Ellipta
103
104
105

1/9/2020
36
Global Initiative for Asthma (GINA)
● Not a guideline but an evidence‐based strategy focused on translation into clinical practice
● Recently update in mid 2019
Summary Points:
● Inhaled SABA has been first‐line treatment for over 50 years● Regular or frequent use of SABA is associated with adverse
effects● Higher use of SABA is associated with adverse clinical
outcomes
GINA Updates for Asthma
Major Changes:
● For safety, no longer recommends SABA‐only treatment for Step 1
● Now recommends all adults and adolescents should receive symptom‐driven or regular low dose ICS‐containing controller treatment to reduce the risk of serious exacerbations
New guidance for adults/adolescents and children 6‐11 years.
GINA Updates for Asthma
Adults and Adolescents
GINA Update
106
107
108

1/9/2020
37
No evidence to support SABA‐only
Low dose formoterol/budesonide prn avoids severe exacerbations in 1 in 16 patients with mild asthma versus albuterol alone
GINA Update: Step 1
109
110
111

1/9/2020
38
GINA Update: Step 1
Low dose ICS plus prn SABA
● Reduces risk of severe exacerbations, hospitalizations and death
● Serious exacerbations halved even in patients with symptoms 0‐1 days per week
As‐needed low dose ICS‐formoterol
● Direct evidence from 2 large studies (non‐inferiority) for severe exacerbations versus low dose ICS with prn SABA
● 64% reduction in severe exacerbations versus SABA‐only treatment
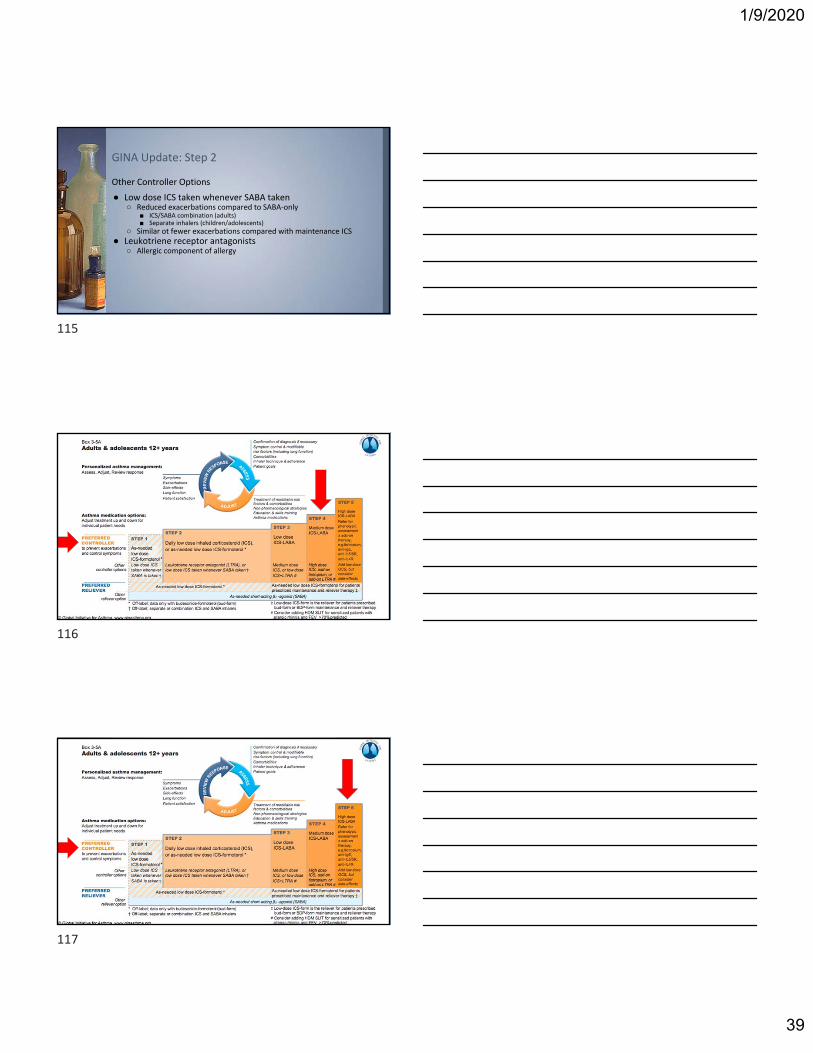
GINA Update: Step 2
112
113
114
1/9/2020
39
Other Controller Options
● Low dose ICS taken whenever SABA taken○ Reduced exacerbations compared to SABA‐only
■ ICS/SABA combination (adults)■ Separate inhalers (children/adolescents)
○ Similar ot fewer exacerbations compared with maintenance ICS● Leukotriene receptor antagonists
○ Allergic component of allergy
GINA Update: Step 2
115
116
117

1/9/2020
40
Children 6‐11 years
GINA Update
118
119
120

1/9/2020
41
121
122
123

1/9/2020
42
Inhaler Technique: MDI
124
125
126

1/9/2020
43
Inhaler Technique: MDI with Spacer
Inhaler Technique: Diskus Inhaler
Inhaler Technique: Diskus Inhaler
127
128
129

1/9/2020
44
Inhaler Technique: Respiclick
Questions?
CE CODE:
130
131
132

1/9/2020
45
1. American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: Standards of Medical Care in Diabetes—2019 [web annotation]. Diabetes Care 2019;42(Suppl. 1):S90–S102.
2. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016;375:1834‐44.
3. Marso SP, Daniels GH, Brown‐Frandsen K, et al. Liraglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016;375:311‐22.
4. Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome5. Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double blind,
randomised placebo‐controlled trial. Lancet 2019. 6. Holman RR, Bethel MA, Mentz RJ, et al.; EXSCEL Study Group. Effects of once‐weekly exenatide on cardiovascular outcomes in type 2 diabetes.
N Engl J Med 2017;377:1228–12397. Zinman B, Wanner C, Lachin JM, et al.; EMPAREG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2
diabetes. N Engl J Med 2015;373:2117– 2128.8. Fitchett D, Butler J, van de Borne P, et al.; EMPA‐REG OUTCOME trial investigators. Effects of empagliflozin on risk for cardiovascular death
and heart failure hospitalization across the spectrum of heart failure risk in the EMPAREG OUTCOME trial. Eur Heart J 2018;39:363– 370.9. Wiviott SD, Raz I, Bonaca MP, MOsenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire
DK, Wilding JPH, Ruff CT, Gause‐Nilsson IAM, Fredrisksson M, Johansson PA, Langkilde AM, Sabatine MS; for the DECLARE‐TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019;380:347‐357
10. Neal B, Perkovic V, Mahaffey KW, et al.; CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017;377:644–657 10.
11. Perkovic V, Jardine MJ, Neal B, et al., on behalf of the CREDENCE Trial Investigators. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med 2019;380:2295‐306
12. RYBELSUS [package insert]. Plansboro, NJ: Novo Nordisk Inc; September 201913. Helena W. Rodbard, Julio Rosenstock, Luis H. Canani, Chaicharn Deerochanawong, Janusz Gumprecht, Soren Ostergaard Lindberg, Ildiko
Lingvay, Anette Luther Sondergaard, Marianne Bach Treppendahl, Eduard Montanya for the PIONEER 2 Investigators. Oral Semaglutide versus Empagliflozin in Patients with Type 2 Diabetes Uncontrolled on Metformin: The PIONEER 2 trial. Diabetes Care 2019 Sep;dc190833
14. Pharmacologic Approaches to Glycemic Management: Standards of Medical Care in Diabetes - 2020. Diabetes Care 2020;43(Suppl. 1):S98-S110
Diabetes Updates References
1. American Diabetes Association. Continuous glucose monitors- Consumer Guide 2018. Diabetes Forecast. http://main.diabetes.org/dforg/pdfs/2018/2018-cg-continuous-glucose-monitors.pdf (accessed Jan. 6, 2019).
2. FreeStyle LibreLink App. Freestyle Libre. https://www.freestylelibre.us/system-overview/continous-glucose-monitor-app.html (accessed Jan. 19, 2019).3. Abbott’s Freestyle Libre 14 day flash glucose monitoring system now approved in U.S. Abbott. https://abbott.mediaroom.com/2018-07-27-Abbotts-FreeStyle-
R-Libre-14-Day-Flash-Glucose-Monitoring-System-Now-Approved-in-U-S (accessed Jan. 19, 2019). 4. Dexcom G6 continuous glucose monitoring system user guide. Dexcom, Inc. https://s3-us-west-2.amazonaws.com/dexcompdf/G6-CGM-Users-
Guide.pdf?_ga=2.61291948.1830682920.1549243176-1258106527.1549243176 (accessed Jan. 19, 2019).Images: Continuous glucose monitoring system. Freestyle Libre. https://www.freestylelibre.us/ (accessed Jan. 19, 2019).
5. Make knowledge your superpower with the new Dexcom G6® CGM. Dexcom, Inc. https://www.dexcom.com/get-started-cgm/40?sfc=701f30000018vibAAA&gclid=EAIaIQobChMIw-2n_IbV4AIV0pCfCh2HJwTQEAAYASAAEgLAsvD_BwE
6. Guardian Connect vs. Freestyle Libre. Medtronic Diabetes. https://guardianconnect.medtronic-diabetes.co.uk/guardian-connect-vs-freestyle-libre# (accessed January 19, 2019).
7. American Diabetes Association. Continuous glucose monitors- Consumer Guide 2018. Diabetes Forecast. http://main.diabetes.org/dforg/pdfs/2018/2018-cg-continuous-glucose-monitors.pdf (accessed January 6, 2019).
8. Eversense User Guide. Food and Drug Administration. https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160048c.pdf (accessed February 6, 2019).9. Images: Guardian Connect CGM System. Medtronic Diabetes. https://www.medtronicdiabetes.com/products/guardian-connect-continuous-glucose-
monitoring-system (accessed January 19, 2019).10. Eversense: the only long-term continuous glucose monitoring (CGM) system. Senseonics, Inc. https://www.eversensediabetes.com/products/ (accessed
February 6, 2019).11. Continuous glucose monitoring system. Freestyle Libre. https://www.freestylelibre.us/ (accessed Jan. 19, 2019).12. Abbott’s Freestyle Libre 14 day flash glucose monitoring system now approved in U.S. Abbott. https://abbott.mediaroom.com/2018-07-27-Abbotts-FreeStyle-
R-Libre-14-Day-Flash-Glucose-Monitoring-System-Now-Approved-in-U-S (accessed Jan. 19, 2019). 13. Dexcom G6 continuous glucose monitoring system user guide. Dexcom, Inc. https://s3-us-west-2.amazonaws.com/dexcompdf/G6-CGM-Users-
Guide.pdf?_ga=2.61291948.1830682920.1549243176-1258106527.1549243176 (accessed Jan. 19, 2019).14. Guardian Connect CGM System. Medtronic Diabetes. https://www.medtronicdiabetes.com/products/guardian-connect-continuous-glucose-monitoring-system
(accessed January 19, 2019).15. Eversense User Guide. Food and Drug Administration. https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160048c.pdf (accessed February 6, 2019).16. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes
Care 2019;42:1593–1603 | https://doi.org/10.2337/dci19-0028
CGM References
1. Sorkness CA, Blake KV, Asthma. In: Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells, BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10 e New York, NY: McGraw Hill.
2. Fanta C. An overview of asthma management. UpToDate. Accessed 13 December 2019.
3. Global Initiative for Asthma. 2019 GINA Report, Global Strategy for Asthma Management and Prevention. https://ginasthma.org/gina-reports/ Accessed 13 December 2019.
4. Beasley R, et al. Controlled trial of budesonide‐formoterol as needed for mild ashtma. N Eng J Med 2019; 380(21): 2020‐30.
5. O’Byrne P, et al. Inhaled combined budesonide‐formoterol as needed in mild asthma. N Eng J Med 2018; 378(20):1865‐76.
6. COPD Foundation Education Videos https://www.youtube.com/user/COPDFoundation Accessed 13 December 2019.
Asthma References
133
134
135