lawrence-douglas county health board
TRANSCRIPT

Our mission is to advance policies, practices and programs that promote health for all, prevent disease and protect the environment
P R O F E S S I O N A L I S M • IN T E G R I T Y • C O M P A S S I O N • T E A M W O R K
Lawrence-Douglas County Health Board September 16, 2019
5:00 p.m.
Agenda: Approximate time 1:30
1. Call to order, Steve Fawcett
2. Welcome new Board Member Diana Malott 5 minutes
3. Public Comment remarks limited to 5 minutes 5 minutes
4. Approval of agenda, Steve Fawcett 2 minutes
5. Approval of minutes of August 19, 2019 meeting, Steve Fawcett 3 minutes
6. Approval of August monthly financial report, Michele Hammann 5 minutes
7. New Business (action needed). 25 minutes
a. Consider changes to the monthly financial report b. Consider transition to new accounting software in 2020
8. Director’s Report 45 minutes
a. Review 2019 Employee Satisfaction Survey responses b. Clinic Supervisor transition planning c. Receive Suicide Issue Brief d. City Commission Candidate Forum e. Follow up information regarding client satisfaction survey f. Public Health Law Summit
9. Adjournment
Next Regularly Scheduled Meeting Date Board Meeting –Monday, October 21, 2019
Future Business
Consider proposals for banking services
Future Opportunity Filter
MINUTES Lawrence-Douglas County Health Board
August 19, 2019 CALL TO ORDER The monthly meeting of the Lawrence-Douglas County Health Board was held Monday, August 19, 2019. Vice chair Vern Norwood called the meeting to order at 5:02 p.m. PUBLIC COMMENT There was no public comment. APPROVAL OF AGENDA Dan Partridge stated we need approval to pay for the video in item number 7d on Pregnant Mothers Stop Smoking Campaign. Shanda Hurla made a motion to approve the August 19, 2019, agenda knowing item 7d will be asking for approval to pay for video on Pregnant Mothers Stop Smoking Campaign. Michael Williams provided the second and the motion passed. REVIEW AND APPROVE MINUTES OF JULY 15, 2019 Michael Williams made a motion that the Minutes of July 15, 2019, be approved. Sandy Praeger provided the second and the motion passed. REVIEW AND APPROVE JULY MONTHLY FINANCIAL REPORT Dan Partridge, director reviewed the July Monthly Financial Report. Sandy Praeger moved that the July Monthly Financial Report be approved. Michael Williams provided the second and the motion passed.
200 Maine, Suite B Lawrence, KS 66044-1357
OFFICE: 785/843-3060 FAX: 785/843-3161
CLINIC: 785/843-0721 FAX: 785/843-2930
200 Maine, Suite B Lawrence, KS 66044-1357
OFFICE: 785/843-3060 FAX: 785/843-3161
CLINIC: 785/843-0721 FAX: 785/843-2930

Minutes Page 2 August 19, 2019
PROGRAM REPORT – REVIEW PEFORMANCE MANAGEMENT REPORT Dan Partridge, director, reviewed the second quarter performance report on Positive Client Relationships, Culture and Value Alignment, Community Service Leadership and Financial Stewardship. The client satisfaction survey is at 98 percent. Clients now receive this survey the minute their visit is completed. We are also offering a gift card for clients to participate in the survey. The partner satisfaction survey was sent to 60 partners twice a year and is composed of 12 questions. Our target goal for this survey is an average score of 48 and our average was 51 in the second quarter. The goal of convening community health forums is 10 and we convened 17 this quarter. Dan stated the living wage of $16.25 per hour will be in place January 1, 2020. The goals of percent of insured clients with in-network insurance coverage is 80 percent and we reached 70 percent. The goal for clinic fee revenue is $90,948 and we collected $77,191. DIRECTORS REPORT Review of Wage Band Adjustments Included in the 2020 Budget Dan Partridge, director, reported increasing the living wage to $16.25 per hour has an affect on other wage bands. Dan stated this proposed new set of wage bands will be incorporated in the 2020 budget. City Commission Candidate Forum Dan Partridge, director, reported we have tentatively set the date of September 12th at 6 p.m. at the Lawrence Public Library for the candidate forum. More details to follow. Update on Review of Project LIVELY Program Linda Craig, clinic services director, reported meeting with community partners in senior services to review how senior needs are currently being addressed and identifying the areas we may be duplicating services or have gaps. They talked about how to work better to identify when to pass services to each other. Partners are looking to see if their role is care coordination or care management. They plan to meet again to determine how to move forward.

Minutes Page 3 August 19, 2019
Review Public Perception Data Collected During Enhanced Behavioral Risk Factor Surveillance Systems (BRFSS) Data Collection George Diepenbrock, communications officer, reported the Docking Institute of Public Affairs at Fort Hays State University, conducted a survey regarding health patterns for Douglas County residents. The survey began in December of 2018 and ended in May 2019. There were 1,500 completed interviews most done by phone. The final three questions were regarding their experience with the Lawrence-Douglas County Health Department. Of the 1,500 interviews, 740 said they had no experience with the Health Department. Those 558 who had heard of the Health Department said their experience was good. Eighty-three percent who had experience with us said we do our job “well” or “very well.” Most have a positive impression of our reputation in the community, though 487 people also reported they did not know or were unsure of our reputation. We are seeing we are best known for clinic services and regulatory enforcement. George stated we still face the challenge of a large number of people who haven’t used our services and don’t recognize our work in the community. However, most people who know us think highly of us. People associate us with advocating for a healthier community and encouraging healthier behaviors. The next steps are to build on our successes, connecting people to our services, engagement on community health, equity and informatics. Tangible projects include website redesign in January 2020, updating our brand/logo and sustain momentum of Healthier Together/mySidewalk. As a brand tagline, the Board liked Health for All. George also presented a 30-second video on the Pregnant Mothers Stop Smoking Campaign. By consensus, the Board approved entering into a contract with Midco to do a 2-month commercial for $2,000. Announcements The Health Department received the Gold Premiere USDA award for breastfeeding support to WIC families. Other New Business 1. The next scheduled Health Board meeting will be Monday, September 16, 2019, at
5 p.m. in the first-floor meeting room.

Minutes Page 4 August 19, 2019
ADJOURNMENT The Board meeting was adjourned at 6:05 p.m. on a motion by Verdell Taylor and a second by Sandy Praeger. Respectfully submitted, Dan Partridge Secretary Present: Shanda Hurla
Vern Norwood Shannon Oury Sandy Praeger
Verdell Taylor Michael Williams Other: Charlie Bryan
Linda Craig George Diepenbrock
Colleen Hill Sonia Jordan
Josephine (intern)

Lawrence-Douglas County Health Department August 2019 Notes for Financial Reports
Income & Expense Statement
Revenues City & County Operating Revenue: The 2nd half of City and County funding was received in the prior month, and
on track with the year to date budgeted amounts for both City and County. Contract Services: Payments increased for the month of August by $1480, low compared to budget for the month
and about 39K year to date. Program Fees: Payments continued to increase for the month of August by about $4K and on track with the year
to date budgeted amounts. Federal & State Grants: Federal grant receipts increased from the prior month by 286K and on track with the
year to date budgeted amounts. State grants increased from the prior month by 78K and on track with the year to date budgeted amounts.
Expenses Gross Salaries and Wages / Payroll Taxes: Continue to trend less than budget totaling $173k less year to date. Contractual Services: Under budget for the month of August and $54k over budgeted amount year to date, in
part due to outsourcing of the payroll, accounts payable and financial statement functions and consulting agreement with SS&C.
Other Exp./Equipment: Exceeded budget. Large purchase in the amount of $12,500 “Douglas County Administration – My Strength” grant expense.
Capital Purchases: See detail as outlined on the 2019 Funded Depreciation expenditures.
Balance Sheet General/Operating
Balance increased in August by $203,479 to $1,486,834 Board Designated Reserve Fund Balance increased in August by $117 due to recording interest Kay Kent Public Health Service Award Fund Balance increased in August by $6 due to recording interest Funded Depreciation Balance increased in August due to grant money in the amount of $13,134 transferred from the
General/Operating account to the Funded Depreciation account. Capital purchase in the amount of $4,919 was written out of the account. See detail as outlined on the 2019 Funded Depreciation expenditures.
Vendor payment and payroll lists are included for the month of August.

Lawrence-Douglas County Health DptNEWCOA
Income Statement SubType(Original Budget to Actual Comparison)
For the period of 8/1/2019 Through 8/31/2019
9/6/19
3:19:24 PM
Actual Budget Variance
Current Period
Actual Budget Variance
Year To DateAnnual
Budget
Revenues
$0.00 $0.00 $0.00 $350,500.00 $350,482.00 $18.00 City Operating $700,964.00
0.00 0.00 0.00 824,116.00 412,058.00 412,058.00 County Operating $824,116.00
1,480.00 38,165.17 (36,685.17) 90,006.76 129,221.36 (39,214.60)Contract Services $176,222.04
63,008.15 38,499.99 24,508.16 307,497.96 307,999.92 (501.96)Program Fees $461,999.88
300,894.00 91,148.15 209,745.85 704,627.32 729,185.20 (24,557.88)Federal Grant $1,093,777.80
78,678.18 29,245.09 49,433.09 235,808.22 233,960.72 1,847.50 State Grant $350,941.08
15,000.00 0.00 15,000.00 92,457.70 75,000.00 17,457.70 Local/Private Grant $75,000.00
764.83 133.33 631.50 15,131.15 1,066.64 14,064.51 Interest $1,600.46
0.00 0.00 0.00 122.12 0.00 122.12 Other Revenue $0.00
4,000.00 120.83 3,879.17 30,004.65 966.64 29,038.01 Other Revenue $1,449.96
$266,512.60 Net Revenues $197,312.56 $410,331.40 $2,239,940.48 $2,650,271.88 $463,825.16 $3,686,071.22
Program Expenses
$158,870.52 $183,026.76 $24,156.24 $1,291,475.11 $1,464,214.08 $172,738.97 Gross Salaries & Wages $2,196,321.12
11,368.96 14,001.58 2,632.62 92,595.11 112,012.64 19,417.53 Payroll Taxes (SS & MC) $168,018.96
757.54 0.00 (757.54) 202,845.90 177,061.08 (25,784.82)Insurance - Health $177,061.08
16,133.03 17,112.83 979.80 140,816.54 136,902.64 (3,913.90)KPERS $205,353.96
161.01 896.83 735.82 2,122.13 7,174.64 5,052.51 Insurance - Unemployment $10,761.96
70.99 2,260.58 2,189.59 22,091.56 18,084.64 (4,006.92)Insurance - Work Comp $27,126.96
0.00 378.34 378.34 100.00 3,026.72 2,926.72 Insurance - Prof Liability $4,540.08
1,718.33 18,403.51 16,685.18 200,844.56 147,228.08 (53,616.48)Contractual Service Expenditure $220,842.12
304.40 35.00 (269.40) 1,394.33 280.00 (1,114.33)Employment Ads $420.00
1,118.62 820.83 (297.79) 5,398.40 6,566.64 1,168.24 Interpreters $9,849.96
2,300.00 833.33 (1,466.67) 9,569.06 6,666.64 (2,902.42)Health Education/Promotion Advertis $9,999.96
523.31 641.67 118.36 3,675.43 5,133.36 1,457.93 Bank & Credit Card Fees $7,700.04
0.00 300.00 300.00 1,347.44 2,400.00 1,052.56 Commercial Travel $3,600.00
599.54 739.92 140.38 8,066.76 5,919.36 (2,147.40)Meals $8,879.04
0.00 822.41 822.41 8,678.08 6,579.28 (2,098.80)Lodging $9,868.92
860.00 1,397.59 537.59 19,918.00 11,180.72 (8,737.28)Registration $16,771.08
156.26 834.33 678.07 2,791.86 6,674.64 3,882.78 Copying & Printing $10,011.96
$47,563.00 Total Program Expenses $242,505.51 $103,374.89 $2,117,105.16 $2,013,730.27 $194,942.51 $3,087,127.20
General & Administrative Expenses
$4,919.00 $0.00 $(4,919.00) $157,349.20 $0.00 $(157,349.20)Capital Purchases $0.00
1,756.47 2,447.50 691.03 22,777.84 19,580.00 (3,197.84)Phone & Communications $29,370.00
330.40 797.50 467.10 5,619.89 6,380.00 760.11 Postage & Delivery $9,570.00
645.26 444.08 (201.18) 7,616.22 3,552.64 (4,063.58)Publications & Subscriptions $5,328.96
0.00 123.00 123.00 1,212.26 984.00 (228.26)Repair & Maintenance $1,476.00
893.08 12,899.16 12,006.08 38,573.12 103,193.28 64,620.16 Service & Licensing Contracts $154,789.92

Lawrence-Douglas County Health DptNEWCOA
Income Statement SubType(Original Budget to Actual Comparison)
For the period of 8/1/2019 Through 8/31/2019
9/6/19
3:19:24 PM
Actual Budget Variance
Current Period
Actual Budget Variance
Year To DateAnnual
Budget
410.40 416.67 6.27 3,855.23 3,333.36 (521.87)Medical Fees $5,000.04
6,502.96 6,700.00 197.04 71,932.64 53,600.00 (18,332.64)IT Consultation Fees $80,400.00
401.56 291.66 (109.90) 3,570.47 2,333.28 (1,237.19)Legal Fees $3,499.92
0.00 957.67 957.67 5,375.00 7,661.36 2,286.36 Physician Fees $11,492.04
0.00 768.85 768.85 5,837.48 6,150.80 313.32 Dues $9,226.20
0.00 62.50 62.50 150.00 500.00 350.00 Business Administration Fees $750.00
534.00 791.74 257.74 10,465.00 6,333.92 (4,131.08)Insurance - Non-Payroll Related $9,500.88
300.00 460.17 160.17 2,903.20 3,681.36 778.16 Laboratory $5,522.04
2,634.80 2,025.34 (609.46) 15,806.87 16,202.72 395.85 Mileage/Tolls/Parking $24,304.08
(173.75) 585.42 759.17 650.92 4,683.36 4,032.44 Miscellaneous $7,025.04
3,369.29 1,700.42 (1,668.87) 13,872.50 13,603.36 (269.14)Medical Supplies $20,405.04
14,729.66 14,426.17 (303.49) 90,258.33 115,409.36 25,151.03 Pharmacueticals $173,114.04
48.90 1,305.25 1,256.35 9,466.90 10,442.00 975.10 Office Supplies $15,663.00
1,312.06 2,708.91 1,396.85 19,941.11 21,671.28 1,730.17 Other Supplies $32,506.92
$11,297.92 Total General & Administrative Expenses $49,912.01 $(87,938.10)$399,296.08 $487,234.18 $38,614.09 $598,944.12
$15,436.79 $2,516,401.24 $2,500,964.45 $58,860.92 $292,417.52 $233,556.60 Total Expenses $2,516,401.24
Income (Loss) from Operations $230,268.56 $149,307.43 $(95,104.96) $(276,460.76)$325,373.52 $425,768.19 ($0.10)
Other Expense
$(12,712.43) $0.00 $(12,712.43) $(29,617.12) $0.00 $(29,617.12)Other Exp/Equipment $0.00
$(12,712.43)Total Other Expense $0.00 $(29,617.12)$0.00 $(29,617.12)$(12,712.43) $0.00
$217,556.13 Net Income (Loss) $312,661.09 $(276,460.76) $396,151.07 $119,690.31 $(95,104.96) ($0.10)

2019 Financial Performance
0
200000
400000
600000
800000
1000000
$
RevenueBudgeted Revenue Actual Revenue
-
250
500
750
1,000
$
Thousands
RevenueBudget Actual
-
250
500
750
$
Thousands
Expenditures Budget Actual
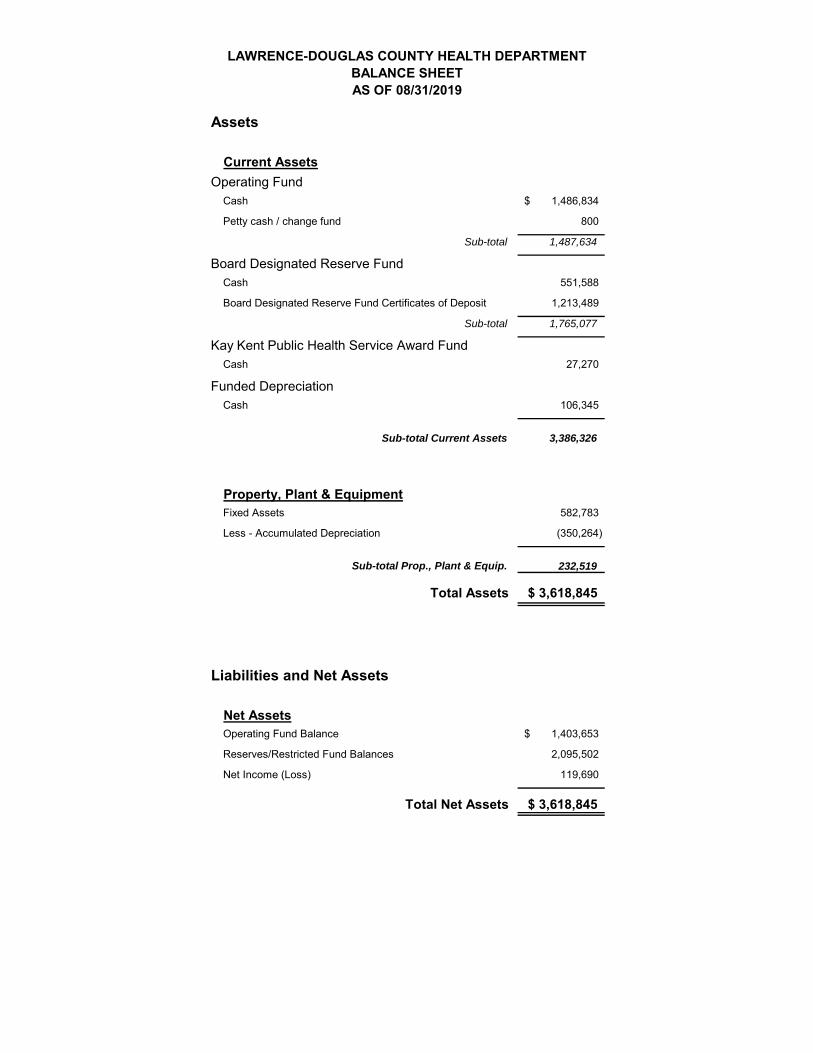
LAWRENCE-DOUGLAS COUNTY HEALTH DEPARTMENTBALANCE SHEET AS OF 08/31/2019
Assets
Current Assets
Operating FundCash 1,486,834$
Petty cash / change fund 800
Sub-total 1,487,634
Board Designated Reserve FundCash 551,588
Board Designated Reserve Fund Certificates of Deposit 1,213,489
Sub-total 1,765,077
Kay Kent Public Health Service Award FundCash 27,270
Funded DepreciationCash 106,345
Sub-total Current Assets 3,386,326
Property, Plant & EquipmentFixed Assets 582,783
Less - Accumulated Depreciation (350,264)
232,519
Total Assets 3,618,845$
Liabilities and Net Assets
Net AssetsOperating Fund Balance 1,403,653$
Reserves/Restricted Fund Balances 2,095,502
Net Income (Loss) 119,690
Total Net Assets 3,618,845$
Sub-total Prop., Plant & Equip.

2019 Funded Depreciation Purchases
For the period endingAugust 31, 2019
Month Purchased Price
January EMR Project Management Fee - Wyandotte 9,500$ February CDP Initial Phase Costs 5,933 March Laser Logic 3,829 April Scott Rice - Office Furniture 4,771 April Mcubed Technologies - Computers and Scanners 52,982 May Missouri Door Co - Auto. Hanicap Door Operators 8,201 May Johnson Controls - Access Control 2,837 May Custom Data - Project Kickoff and Travel 4,958 May Qless - Support & Command 2,750 May Mcubed Technologies - Barcode Scanner/Cradles 341 May Mcubed Technologies - Label Printer/Printer Server 920 June Custom Data - System Config/Data 14,874 June Custom Data - Milestone 2 12,659 June Custom Data - Data Extract & Delivery Auto 13,000 June Custom Data - Training & Implementation 9,916 July CDP - Reports Configuration Complete 4,958 August Migali Scientific - Refridgerator 4,919
Year to Date Purchases 157,349$

A Brief Overview, Implementation & Pricing Plan
For
Lawrence‐Douglas County Health Department
By
SS&C Solutions, Inc.

Best‐in‐Class Solution Architecture
Payroll Journal
New Employees & Changes
Billings, Cash Collections, Census
Time Clock
• Real Time, Integrated, Best in Class Accounting System
• Not for Profit Focused
• Open Architecture ‘Speaks’ with Other Open Systems to Allow for Custom Designed Accounting System
• Custom Designed Financial Reports and Dashboards
• Cloud Hosted System that Doesn’t Require Perpetual & Expensive Updates

17pt Centred Running Footer Text Here – Title determines Length
Track and report accurately to get the most for your mission
Centralize all grant documents and details for secure, comprehensive views, regardless of award type or funding source—corporate, foundation, government, or other.
Easily report and compare budget to actuals on grants that have reporting periods that differ from or cross your organization’s fiscal year. You don’t need spreadsheets to know where you stand.
Extend your grant records to include details unique to your program delivery using easy business user configuration. Search and report on these details along with the financial data and impact metrics for each grant.
Capture accurate costs for reimbursement
Associate accounting entries with grants and flag reimbursable costs at entry to reduce billing errors. Then gather eligible charges for reporting and billing with the click of a button. You never miss a charge or overstate amounts.
Use integrated timekeeping data and easily tie employee efforts per grant to timesheets. Or, employees can track and report time and approvals directly in Sage Intacct.
You can bill indirect costs based on a negotiated rate, specific rate, or markup based on the type of expense.
If your nonprofit manages several grants or relies on grants for a majority of your funding, Sage Intacct Grants Tracking and Billing is the most comprehensive and flexible grants management functionality available within a financial management solution. Manage your grants efficiently and accurately with the goal of ensuring compliance with grant requirements to achieve your mission’s success.
D a t a s h e e t
Nonprofit Grants Tracking and Billing:
Ensure Compliance with Grant Requirements
Achieve mission success with efficient and accurate grant tracking, reporting, and
reimbursement
Sage Intacct - Copyright 2018

27pt Centred Running Footer Text Here – Title determines Length
To learn more about how Sage Intacct can help you achieve your mission more efficiently, visit: https://www.sageintacct.com/nonprofit-accounting-software or contact us at 877-968-0600.
Ensure mission delivery with more control and visibility
With centralized task tracking for grants and projects, everyone has visibility into what needs to be done and when.
Monitor spending and track with the budget plan as the grant is used.
Meet deadlines and easily collaborate with other team members to deliver on conditions and milestones.
Couple with Sage Intacct Resource Management to extend project tracking and delivery, including staffing, capacity, and utilization capabilities.
Ease compliance and audits
With centralized grant records and reports, your staff and auditors have a single, shared source of truth.
You can track funding details and tie deliverables to tasks. Progress monitoring helps you ensure timely delivery of your performance requirements.
Asserting expenses as reimbursable during transaction entry provides a clear audit trail for qualified expenses.
Couple with Sage Intacct Nonprofit Revenue Management for conditional grants to further track barriers, automate recognition as milestones are achieved, and streamline compliance for stress-free audits.


• Allocations are used to spread amounts (usually costs) across different reporting areas (dimensions). This can serve as a very powerful tool to enable operational insights for analysis into fully loaded costs and profit margins.
• Allocations for amounts related to billing and revenue recognition may be heavily regulated with compliance requirements that may not match to the same methodology appropriate for operational insights.
Allocations Process
Operational insights
Billing & Rev Rec
BOTH
5

Transaction Allocations
6
(1) Enable in GL config, (2) maintain definitions in GL (treat as uneditable for auditability), (3) use in AP, AR, GL

Dynamic Allocations
7

Transaction vs. Dynamic Allocations
• Transaction Allocations • Pricing consideration: Included as
part of the Core Financials product and are configured & maintained in the GL
• Requirements consideration:Intended for use during transaction entry with parameters being known up front. Fixed percentages or amounts are defined in advance of the transaction.
• Dynamic Allocations • Pricing consideration: Requires an
additional subscription• Requirements consideration:
Applied as after‐the‐fact account amount distributions on a periodic basis. The dynamically generated allocations also automatically create journal entries with verifiable calculations attached so you can see how the debits and credits were derived from the source and basis amounts.
8

• Requirement Details
• Under Uniform Guidance (2 CFR 200)A non‐Federal entity that expends $750,000 or more in Federal awards during the non‐Federal entity's fiscal year must have a “single audit” and conform to very specific reporting requirements.
• SEFA report lists the organizations’ expenditures during the period covered by each grant, from each federal agency
• Can easily build a Financial report, with the use of Custom Fields
• State grants/contracts may have similar requirements
Schedule of Expenditures of Federal Awards (SEFA)
9

• Workflows reflect the overall flow of a document through its designated lifecycle from start to finish
Purchase Order Workflows
10

Purchasing Process – Value Approval‐ Use Case
11
• Purchase Order would route to all Level 2 approvers, requiring one (1) person to approve at that level
• Routing is not sequential, and jumps to the approver with appropriate authorization
• Any rejection stops the approval flow
• Requester is notified if email notifications are enabled
Purchase Order = $2,750.00 Level 1
Approver$0 ‐ $999
Level 2 Approver$1K ‐$9,999.99
Level 3 Approver$10K +
Approval Routing
One(1) approver required for each level

Purchasing Process – Value Approval Progressive‐ Use Case
12
• Purchase Order would route to Level 1 approver until approved, then Level 2, then Level 3, requiring one (1) person to approve at each level
• Routing is sequential, and follows the defined Approval Levels, going from lowest to highest needed
• Any rejection stops the approval flow
• Requester is notified if email notifications are enabled
Purchase Order =
$12,750.00 Level 1 Approver$0 ‐ $999
Level 2 Approver$1K ‐$9,999.99
Level 3 Approver$10K +
Approval Routing
One(1) approver required for each level

Role Comparison Grid
13
Application Permission Employee User Business User Project Manager CRM Warehouse
Purchasing Create Purchase Requisitions Yes Yes Yes No Yes
Create Recurring Purchase Requisitions No Yes No No Yes
Edit Purchase Requisitions Yes Yes Yes No Yes
Delete Purchase Requisition Yes Yes Yes No Yes
Approve Purchase Requisitions Yes Yes Yes No Yes
Convert Purchase Requisition No Yes Yes No Yes
Create Purchase Order No Yes Yes No Yes
Create Recurring Purchase Order No Yes No No Yes
Edit Purchase Order No Yes Yes No Yes
Delete Purchase Order No Yes Yes No Yes
Approve Purchase Order Yes Yes Yes No Yes
Convert Purchase Order No Yes Yes No Yes
Create Purchase Invoice No Yes Yes No Yes
Edit Purchase Invoice No Yes Yes No Yes
Create Recurring Purchase Invoice No Yes No No Yes
Delete Purchase Invoice No Yes Yes No Yes
Approve Purchase Invoice Yes Yes Yes No Yes
Run Purchasing Reports Yes Yes Yes No Yes
Accounts Payable Create AP Bill No Yes No No No
Create Recurring AP Bill No Yes No No No
Edit AP Bill No Yes No No No
Approve AP Bill Yes Yes Yes No No
Create AP Payment No Yes No No No
Edit AP Payment No Yes No No No
Approve AP Payment No Yes No No No

• https://resources.sageintacct.com/nonprofits/sage‐intacct‐product‐tour‐for‐nonprofit‐organizations
Additional Demo Website

Implementation Plan

Lawrence Douglas County Health Department
Intacct Implementation Plan
Internal Time Intacct / SS&C Time
Step 1) Preliminary Considerations 8 12
Review current structure, chart of accounts and users
Determine Read Only vs Full Use vs Approver Users
Determine how many years of data to convert
Determine key dimensions for report building
Determine non financial data for tracking
2) Determine modules within Intacct vs Partner systems 4 2
General Ledger Intacct
Financial Reporting Intacct
Grant Tracking Intacct
Cash Management Intacct
Purchase Orders Intacct
Accounts Payable Intacct
Accounts Receivable Intacct
Hours Tracking Current Software
Payroll Processing SS&C or consider ADP for HR Solutions
Medical Billing ezEMR
3) Finalize contract with Intacct for monthly services plan 1 1
$350‐$1750 based on number of users or enhanced grant tracking / allocations
4) Clean up lists for import/setup 24 8
Grants Chart of Accounts
Locations Statistical Accounts
Department Account Groups
Employee Types Allocations
Customers (billing) Vendors
5) Configure bank accounts, savings accounts, debit/credit cards 4 4
Setup online integration Order check stock
6) Finalize integration with outside software as appropriate 8 24
Build Test
7) Migration of historical data ‐ 1 year 0 16
8) Build out of entire system and custom reporting and dashboards ‐ up to 4 4 50
9) Training 40 16
Total Hours 93 133
200$ Intacct / SSC rate
26,600$ Extended

Pricing – Small Business vs Full Use • Two levels of pricing based upon the modules selected for use by the Health Department
• Basic Small Business Use, with the number of Full Users, Review Users and Purchase Order Users that we need would be about $350 per month.
• Full Business Use, with the appropriate number of users• With Dynamic Allocations & Enhanced Grant Tracking & Billing = $1,750 per month
• With only Dynamic Allocations = $1,350 per month
We can always upgrade at a later date to Full Business Use

• SS&C has been an IAP with Intacct for over 7 years completing 30+ implementations for our clients
• An IAP with Intacct, has access to the platform’s monthly fees at a decreased rate because our clients are ‘outsourcing’ most of their accounting functions to SS&C.
• The LDCHD dataset is on the SS&C ‘dashboard’ with Intacct. If you choose to take all of your accounting processes in house or move to a different provider, that data & setup is yours and it will be ‘rehomed’ to that new provider or your own dashboard. The fees will change and in some cases increase significantly. There is no ‘cancellation fee’ with SS&C and we will help you with the transition.
Intacct Accounting Partner (IAP) vs Reseller

Michele C. Hammann, CPA, CVA
Chief Strategy Officer
SS&C Solutions, Inc.
785‐856‐5480
THANK YOU

Employee Survey ‐ 2019
3.3
3.2
2.9
3.2
2.9
3.4
3.6
3.1
2.4
2.9
3.4
3.2
Understand expectations
Chance to use my strengths
Recognized for excellent work
Challenged to grow
Supportive Manager
Understand how I advance our mission
Teammates share core values
Workplace supports new ways of doing things
Communication to understand what is going on
Work place is a trustworthy environment
Work place is supportive of different perspectives
Degree I am satisfied with my employment
Health Department
Health DepartmentN = 36 Response Rate = 92%
Neutral Strongly Agree / Strongly Disagree / Very Dissatisfied

Employee Survey ‐ 2019 Historical Trend
3.333.23
3.10
3.31
3.49
3.333.25
3.17
2.89
3.29
3.64
3.17
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
At work, I clearlyunderstand what isexpected of me
I have a chance to use mystrengths every day at
work
I know I will berecognized for excellent
work
In my work, I am alwayschallenged to grow
My teammates have myback
Overall level ofsatisfaction with your job
Historical Employee Survey Responses 2016‐2019
Strongly Agree
Agree
Neutral
Disagree
StronglyDisagree

Employee Survey ‐ 2019 Open‐ended responses
What is the single most important issue for our workplace culture? I wish I knew more about:
communication and trust why/how decisions are made
treating clients and staff with respect and dignity
I believe communication has always been and will be an important issue. changes that administration is considering for the agency
Equity throughout the agency- If we are trying to operate more like a business, staff wages should be in line with other organizations (governmental and private). Since clinic staff don't have flexible hours (due to staffing needed to operate clinic), ensuring that an hour lunch is available for all clinic staff (should staff choose to use it) is a way to improve equity in this area.
Communication about the Health Department's financial picture during general staff meetings and how staff members' work contributes to the agency's solvency would be really beneficial. This would help us all understand how what we do each day contributes to the agency's continued successes.
I have really enjoyed the attempts to foster a greater work community and would like to continue to see more
I think one of the most important issues is getting staff engaged and excited for the jobs we do. Public Health is hard, especially when your schedule revolves around clients on the day-to-day. Having adequate time to recharge, equitable lunch breaks, adequate staffing, instilling a clinic day where clinic is closed over lunch or closes earlier, retreats for all staff devoted to preventing compassion fatigue, developing a better sense of overall unity, and reigniting the passion of staff could contribute to engaging staff and preventing moral injury/burnout.
I am interested in lunch-and-learn opportunities and developing camaraderie with other staff members over the lunch hour, especially my own team. I would also be interested in knowing about the review process/implementation of actions that result from this employee satisfaction survey.
Clear communication and support to achieve goals. Trust ranks up there too. Key stake holders in the community
I continue to see a divide between upstairs and downstairs. Sometimes it feels as if there is a lack of communication between what goes on in clinic and how we could make it better vs. what the perception of what goes on in clinic.
The new makeup of the committees?
Communication and transparencyHow the other departments of the HD function, such as Environmental services, Healthy Families, Family Planning working w/ Heartland etc.
I think we get into a silo mentality and that creates missed opportunities for collaboration. I'd like to see more connectedness and collaboration - especially utilizing our clinicians andtheir expertise in broader community health planning.
Ways to collaborate across departments.
respect Why there is no place on this survey to address specific issues or suggested improvements?
structural clarity around accountability and roles in decision-making.
I think communication across teams and between Admin and other staff could be improved.
Decision-making processes.
That we continue to invite (specifically & intentionally) our community members/employees to participate in the discourse of public health issues.
Epidemiology & Environmental Health
Encouraging buy-in among all employees to connect what we each do to the big picture of public health, especially in reinforcing meaningful action via the CHP, addressing health inequities and the goals of our Strategic Plan.
How to bridge gaps reaching different segments of the population who might be experiencing certain health inequities either by connecting them to our services or something else that can help them.
Communication seems to be the most important issue. There have been many times where employees are unaware of certain events, changes, etc.
Where the health department is trying to be in 7-10 years - goals
Trusting environment If we are more focused on equal opportunities or equal outcomes?
Communication and support for growth outside of job duties. Why departmental-wide decisions are made.
Flexibility.
trust Administrative and leadership policies and projects
Trust in administration. Not sure all new administration has public health lens and compassion/empathy as a inherent value.
How all programs are included and supported by strategic plan.
That we all could understand what all do and acknowledge that each program as value and is very important.
Open and transparent communication
Continuing the equity work to ensure that our agency is a leader in the field.
Trust
health equity across the board, open communication, pure transparency the budget process
It is so hard to pinpoint just one issue because so many things are interwoven to create a strong workplace culture but perhaps communication is where it begins. Communication and relaying information is critical to the workplace because that portrays an image of trust. Trust can make an employee feel valued and if an employee feels valued you have a more productive worker.
Informatics program
Listening to each other
Trust between administration and staff.

I receive the communication I need to understand what is going on and why we engage in programs and practices the way we do
Strongly Agree Agree Neutral Disagree Strongly Disagree
Blank
Informatics
Healthy Families/Dads
Env. Health
CH/Admin
Clinic

I experience our workplace as a trustworthy environment
Strongly Agree Agree Neutral Disagree Strongly Disagree
Blank
Informatics
Healthy Families/Dads
Env. Health
CH/Admin
Clinic

Douglas County Suicide
Scope of Suicide Problem Key findings
Suicides in Douglas County
• Increasing rates that are higher than U.S.
• Males 3.5 more likely to die of suicide
• 1/2 people who die under the age of 45
• Firearms involved in almost 1/2 of suicides and 78% of all firearm deaths
Suicide attempts in Douglas County
• Females 2x more likely to attempt suicide than males
• Half ED attempt patients under age 21
• Poisoning involved in almost 1/2 attempts
• Highest attempt rates in 10-19 year old group and more attempts treated in ED in this age group
Suicide Ideations in Douglas County
• Half of ED ideation patients under age 27
• Highest ideation rates in 10-19 age group • Males and females equally likely to be
treated in ED for ideations
• Males 30 and 64 years old have higher ideation rates than females
Data Brief September 2019
Suicide accounts for almost 80% of all violent deaths in Douglas County (85 suicides versus 22 homicides for 2013-2017)
and 78% of all firearm-related deaths.
Like Kansas, suicide is the 8th leading cause of death in
Douglas County accounting for 85 deaths from 2013-
2017 but it is the fourth leading cause of death when
years of potential life lost is used as a metric (Figure 2).
Suicide is a public health problem both nationally and locally. Since 1999, suicide rates for males and females have increased in the U.S. and Kansas. During this time, Kansas saw an overall increase in the suicide rate of 45% - the 5th largest percent increase in the nation. In Douglas County, suicide rates have increased 84% since 1993. The differences in these rates are statistically significant (Figure 1). The purpose of this brief is to describe who in Douglas County
is dying of suicide and who is being treated in the ED for suicide
ideations and suicide attempts.
Suicide Attempts and Ideations
Suicide ideations include thoughts of dying
and may include a plan to commit suicide.
Nationally, about 4.3% of adults had suicide
ideations(2017). The group with the highest
amount of ideation are those aged 18-25 years
(10.5%).
A suicide attempt is the strongest predictor for
future suicide ideation, another suicide attempt
and death by suicide. Nationally, the
prevalence of suicide attempts in the past year
is highest among adults 18-25 years old (2017).
Cancer 1 1
Heart Disease 2
3Unintentional Injuries 3
2
Chronic lower respiratory disease 4
5Stroke 5
7
Alzheimer's disease 6
10
Diabetes 7
6
Suicide 8
4
Influenza & pneumonia 9
8
Parkinson's Disease 10
12
Cause of Death, Rank YPLL Rank
Data Source: Kansas Department of Health and Environment, Bureau of Epidemiology and Public Health Informatics
Figure 2. Suicide is the 8th leading cause of death in Douglas Countybut the 4th leading cause of death by years of potential life lost (YPLL)
3.4 3.2
5.26.8
Female6.2
8.5 9.1
13Douglas County
12.4
15.614.5 15.2
21.4
18.7
Male25.5
1993-1997 1998-2002 2003-2007 2008-2012 2013-2017
Data Source: KDHE, Bureau of Epidemiology and Public Health Informatics
Note: female rates are unstable and unreliable** Increase is statitically significant from 1993-1997 to 2013-2017
& Increase in male rates is not statistically significant
Figure 1. Douglas County Suicide Rates** have increased 84% Male Suicide Rates have increased& 76% from 1993-1997 to 2013-2017
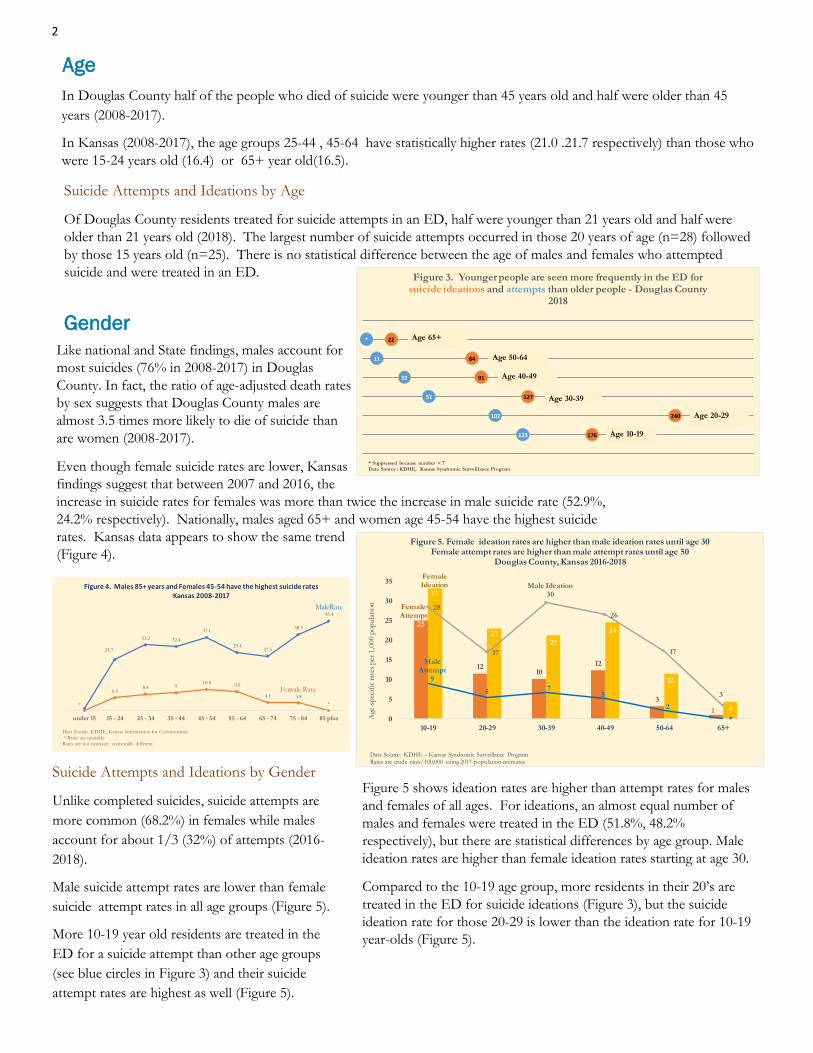
2
Age
In Douglas County half of the people who died of suicide were younger than 45 years old and half were older than 45
years (2008-2017).
In Kansas (2008-2017), the age groups 25-44 , 45-64 have statistically higher rates (21.0 .21.7 respectively) than those who
were 15-24 years old (16.4) or 65+ year old(16.5).
Suicide Attempts and Ideations by Age
Of Douglas County residents treated for suicide attempts in an ED, half were younger than 21 years old and half were
older than 21 years old (2018). The largest number of suicide attempts occurred in those 20 years of age (n=28) followed
by those 15 years old (n=25). There is no statistical difference between the age of males and females who attempted
suicide and were treated in an ED.
Gender
Like national and State findings, males account for
most suicides (76% in 2008-2017) in Douglas
County. In fact, the ratio of age-adjusted death rates
by sex suggests that Douglas County males are
almost 3.5 times more likely to die of suicide than
are women (2008-2017).
Even though female suicide rates are lower, Kansas
findings suggest that between 2007 and 2016, the
increase in suicide rates for females was more than twice the increase in male suicide rate (52.9%,
24.2% respectively). Nationally, males aged 65+ and women age 45-54 have the highest suicide
rates. Kansas data appears to show the same trend
(Figure 4).
Figure 5 shows ideation rates are higher than attempt rates for males
and females of all ages. For ideations, an almost equal number of
males and females were treated in the ED (51.8%, 48.2%
respectively), but there are statistical differences by age group. Male
ideation rates are higher than female ideation rates starting at age 30.
Compared to the 10-19 age group, more residents in their 20’s are
treated in the ED for suicide ideations (Figure 3), but the suicide
ideation rate for those 20-29 is lower than the ideation rate for 10-19
year-olds (Figure 5).
Suicide Attempts and Ideations by Gender
Unlike completed suicides, suicide attempts are
more common (68.2%) in females while males
account for about 1/3 (32%) of attempts (2016-
2018).
Male suicide attempt rates are lower than female
suicide attempt rates in all age groups (Figure 5).
More 10-19 year old residents are treated in the
ED for a suicide attempt than other age groups
(see blue circles in Figure 3) and their suicide
attempt rates are highest as well (Figure 5).
176123
240102
12751
9132
8411
22*
* Suppressed because number < 7
Data Source : KDHE, Kansas Syndromic Surveillance Program
Figure 3. Younger people are seen more frequently in the ED for suicide ideations and attempts than older people - Douglas County
2018
Age 10-19
Age 20-29
Age 30-39
Age 40-49
Age 50-64
Age 65+
25.7
33.2 32.4
37.1
29.427.5
38.5
MaleRate45.4
*
6.58.4 9
10.89.5
4.1Female Rate
3.8
*
under 15 15 - 24 25 - 34 35 - 44 45 - 54 55 - 64 65 - 74 75 - 84 85 plus
Data Source: KDHE, Kansas Information for Communities
* Rates are unstable
Rates are not necessary statistically different
Figure 4. Males 85+ years and Females 45-54 have the highest suicide rates Kansas 2008-2017
Female Attempt
25
1210
12
3
1
Female Ideation
33
2321
24
12
4
Male Attempt
9
5 75
2
*
28
17
Male Ideation 30
26
17
3
0
5
10
15
20
25
30
35
10-19 20-29 30-39 40-49 50-64 65+
Age
-sp
ecif
ic rat
es p
er 1
,000 p
op
ula
tio
n
Data Source: KDHE – Kansas Syndromic Surveillance Program
Rates are crude rates/100,000 using 2017 population estimates
Figure 5. Female ideation rates are higher than male ideation rates until age 30Female attempt rates are higher than male attempt rates until age 50
Douglas County, Kansas 2016-2018

3
Race/Ethnicity
Most (91.9% females and 90.0% males) Douglas County
residents who die of suicide (2013-2017) are White non-
Hispanic. Suicides occurs in the other racial and the Hispanic/
Latino groups in Douglas County, but the numbers are too
small (n < 10) to do small group analyses.
In Kansas (2013-2017) suicide rates are higher for White
Kansans (16.5 per 100,000) than for Black Kansans (8.7% per
100,000). However, the highest suicide rate (27.2) in Kansas
occurs in “other racial group”. According to CDC, American
Indian, Alaska Natives have highest rates of suicide of any
racial/ethnic group in the U.S.; however, there is no evidence
that this is the case in Kansas. Nationally, suicide rates have
increased 10% for Blacks between 2015 and 2016 and 9% of
Latinos, compared to a 1% increase for Whites.
Suicide Attempts and Suicide Ideations by race/
ethnicity
Like deaths due to suicide, White Douglas County
residents comprised most (75.6%) of the suicide
attempts and suicide ideations (76.4%) treated in the
ED in 2018, followed by those who were classified as
“Other” (10.8%), Black (8.0%) and American Indian
(4.0%). Compared with the population of Douglas
County, the proportion of White suicide attempt
patients treated in the ED is lower (87.3%, 75.6%
respectively). Conversely, the proportion of Black
suicide attempt patients is higher than the proportion
of Black residents in the population (8.0%,6.1%
respectively). A similar pattern is seen for ideations
with 9.5% of the ideation patients being Black.
External Cause
Like national and State data, firearms are the most common external cause accounting for 48.7% of deaths due to suicide
in Douglas County, followed by suffocation (25%) and poisoning (16.5%). This pattern has not changed significantly
since 2008 (Figure 6).
A majority (54.8%) of males in Douglas County died from firearms, followed by suffocation and poisoning (23.5% and
13.9%). For females, an almost equal number of
women died from firearms (29.7%), suffocation
(29.7%) and poisoning (24.3%).
National data suggests that the method of suicide
differs by age group and sex. Except for those
age 10-14, firearms are the most frequent external
cause for males and are the first or second most
frequent external cause for females. Suffocation
is the primary cause of death for females 10-14
years and suffocation and firearms each account
for about 1/2 of suicides in males 10-14 years.
Suicide Attempts by External Cause
Compared to deaths due to suicides, a different
picture emerges for suicide attempts treated in
the ED. In 2016-2018, 43% of suicide attempts
in Douglas County involved poisonings,
followed by injuries due to sharp objects or
cutting (28%), and unspecified mechanism
(23.5%). Attempting suicide by other individual
methods (e.g., firearm, smoke/burn,
electrocution, blunt force) are too small to
report separately (n < 6). Figure 7 shows males
and females use similar methods when
attempting suicide.
Female Attempts
261
17
163
*
131
6
Male Attempts
106
*
72
7
67
24
Poisoning Poisoning + other
mechanism
Sharp/Cut Asphyxiation Unspecified
mechanism
Other
* number suppressed because n < 6
Data Source: KDHE Bureau of Epidemiology and Public Helath Informatics
Figure 7. Poisonings and cutting are the most common external cause of suicide attempts for males and females -
Douglas County, Kansas 2016-2018
8
11
14
2008-2012
34
7
14
24
2013-2017
40
Other
Poisoning
Suffocation
Firearm
External Mechanisms reported as other if n < 6
Data Source: KDHE Bureau of Epidemiology and Public Health Informatics
Figure 6. Firearms, suffocation and poisoning account for 90% of deaths by suicide
Douglas County 2008-2017

4
Figure 8. Number of Suicide Ideations and Attempts treated in ED - Douglas County Cities
Lecompton is not included in this analysis because the number of people treated for attempts or ideations was less than 6 in each of the age categories.
14
Attempt8
12
0
2221
Ideation16
10 10
10-19 20-29 30-39 40-49 50-64 GE 65
No data indicates suppressed date due to n < 6 or no cases
Data Source: KDHE, Kansas Syndromic Surveillance Program
Baldwin City 2016-2018
Attempt12
24
60
Ideation38
28
8
16
0
10-19 20-29 30-39 40-49 50-64 GE 65
No data indicates suppressed date due to n < 6 or no cases
Data Source: KDHE, Kansas Syndromic Surveillance Program
Eudora 2016-2018
261 Attempt226
114 98
3911
435
559
Ideation349
284
220
46
10-19 20-29 30-39 40-49 50-64 GE 65
No data indicates suppressed date due to n < 6 or no cases
Data Source: KDHE, Kansas Syndromic Surveillance Program
Lawrence 2016-2018
For people 25-49 years old who die of suicide, a majority (58.5%) are
single, followed by almost equal numbers of people who are divorced
or married (20% and 26% respectively). For those 50-64 years old,
fewer people (18%) who die from suicide are single, and there are
similar numbers of married and divorced (38.5% and 30.8%
respectively). For those 65 years old or older, almost equal numbers
of people are either married or widowed (48% and 44% respectively).
Geography
Over a ten-year time period (2008-2017), 82% of people
who died of suicide were from Lawrence, followed by 9%
from Baldwin and 6% from Eudora. Baldwin City had
the highest crude rates of suicide 2.86 per 1,000
population, followed by Eudora and Lawrence (1.46 and
1.38 per 1,000 respectively.) (U.S. Census Bureau, 2014).
Suicide Attempts and Suicide Ideations by Geography
Figure 8 shows that in the three largest cities in the County,
younger residents are treated more frequently in the ED for
ideations and attempts than other age groups.
Marital Status
Most people (95%) younger than 25 years old
who die of suicide are single. This finding is not
surprising as most people in Douglas County less
than 25 years old are single.
Often referred to as deaths due to despair, suicides along with deaths from drug overdoses and alcohol poisoning are
responsible for recent decreases in life expectancy. In Douglas County, suicide is the 8th leading cause of death but is
the 2nd cause of death for those 15-44 years of age. Existing data sources allow us to look at demographics and
external causes of injury. Firearms are the most common cause of suicide in males and have become as common a
method in females as well. While Douglas County males are more likely to die of a suicide, it is interesting that they are
much less likely to attempt a suicide. At the same time, males are just as likely to have suicidal ideations as females, but
the rates of these ideations are different for males and females in different age groups.
Of particular concern are the number of suicide attempts and ideations in those age 10-19 years in Douglas County.
Nationally, there has been a marked increase in the number suicide attempts and ideations treated in the ED among
youth 10-19 years old. Risk factors for youth suicide include rape, bullying victimization, sadness or depression,
vomiting or taking laxatives to lose weight, and using substances. Moreover, Kansas Communities that Care data
suggest that students who vape or smoke may also be at risk for suicide ideations.
Conclusion

5
There is an urgent need to understand the root causes of suicide, attempts and ideation in our community. Suicide is usually
caused by multiple factors. In addition to mental health conditions and prior suicide attempt, other factors include social and
economic factors, access to lethal means, and poor coping and problem solving skills. Our community has embraced Zero
Suicide which sets an aspirational goal of zero suicides among people who access health services. As an adjunct to this
effective prevention approach , other community approaches should be explored. For example, in Washington County,
Oregon, their in-depth analyzes of people who died of suicide suggested that knowing the community factors associated
with suicides allowed them to institute prevention measures that complemented their Zero Suicide initiative and prevented
suicides. For example, they found that the most prevalent risk factors for suicide were depressed mood and experiencing a
crisis. In their community, an eviction crisis was common. When the police changed their protocol to have a mental health
professional with the police at the time of an eviction, the number of suicides after this type of crisis decreased. Additionally,
investigators also noticed that several people surrendered their healthy pets to the animal shelter before they died by suicide.
After training the animal shelter staff and volunteers to question (“Are you thinking of killing yourself”), persuade and refer
(Get person on the line to the suicide prevention line) (QPR), they were able in three months to intervene with 7 people who
intended to die by suicide.
Overall, it is clear that suicide, suicide attempts and suicide ideation occur across the life span. There is a continuing need to
identify and support people in need and creating a protective environment. Elderly men in particular are at high risk for
suicide and may not talk about their feelings or intentions. It is known that chronic health issues and economic or financial
strain, such as difficulty covering medical, food and housing expenses may increase a person’s risk for suicide. Lack of social
connectedness is also one of chief causes of suicide. . The current efforts to strengthen access and delivery of suicide care
will benefit those with contact with the medical care system and will address many prevention strategies including teaching
coping and problem-solving skills. And finally, preventing suicide and addressing the health care needs of persons at risk
for suicidal behavior require public health information-sharing efforts that raise awareness and provide evidence of effective
community-wide interventions.
Methods
The KDHE multiple cause-of-death research files from 2008-2017 were used to identify deaths due to suicide. Cause of
death referred to in this report is the primary or underlying cause of death, which is defined as the disease or injury that
initiated the chain of events leading directly to death, or the circumstances of the accident or violence that produced the
fatal injury. The underlying cause of death is established through a system called the International Statistical
Classification of Diseases and Related Health Problems, 10th Revision (ICD-10). This system promotes uniformity and
comparability in the collection and presentation of mortality data. All analyzes were conducted using SAS 9.4.
Suicides were defined as the underlying cause of death codes: U03, X60-84, and Y87.0(7). Suicide deaths were
categorized by external cause of suicide using the ICD-10 underlying cause-of-death codes: firearms (X72-X74),
suffocation (X70), poisoning (X60-X69), and other means (U03, X71, X75-X84, and Y87). Poisoning includes both
drug and nondrug (e.g., toxic substances or gases) intoxications. Suffocation includes hanging, asphyxiation, and other
mechanical and nonmechanical threats to oxygenation (e.g., trapped in low oxygen environment). Other means include
mechanisms such as cutting and piercing, falls and jumping, burns from fire, hot substances, and hot liquids; and
transportation. References to rates being significantly higher or lower indicate that differences are statistically significant
at the 0.05 level.
Cases of Douglas County residents who were treated in an ED for a suicide attempt or ideation were identified using
ESSENCE (Kansas Syndromic Surveillance Program). Suicide ideation was defined as ICD-10 CM codes R45.851 or
R45851. Currently, there is no CDC injury matrix for classifying the external mechanisms for non-fatal suicide attempts
and intentional self harm. The ICD-10 CM codes that were used to define suicide attempts are listed in Appendix 1.
This list was developed with a team of clinicians and coders at LMH-H in Lawrence Kansas. These ICD-10 codes were

6
Burstein B, Agostino H, Greenfield B. (2019). Suicidal attempts and ideation among children and adolescents in US Emergency Departments, 2007-2015. JAMA Pediatrics. Doi: 10:1001/jamapediatrics.2019.0464. https://jamanetwork.com/journals/jamapediatrics/article-abstract/2730063 (Accessed 10/30/2019) CDC Vitalsigns. (June 2018). Suicide rising across the US: More than an mental health concern. https://www.cdc.gov/vitalsigns/suicide/index.html (Accessed 10/30/2019) Hedegard H, Schoenbaum M, Claassen C, Crosby A, Holland K, Proescholdbell S. (2018). Issues in developing a surveillance case definition for nonfatal suicide attempt and intentional self-harm using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) coded data. National Health Statistics Reports; no 108., 1-19, Hyattsville, MD: National Center for Health Statistics. https://www.ncbi.nlm.nih.gov/pubmed/29616901 (Accessed 10/20/2019) Hedegaard H, Curtin SC, Warner M. (2018). Suicide rates in the United States continue to increase. NCHS Data Brief,
no 309. Hyattsville, MD: National Center for Health Statistics.
Heron M.. (2019). Deaths: Leading causes for 2017. National Vital Statistics Reports; vol 68 no 6. Hyattsville, MD: National Center for Health Statistics. Accessed July 2, 2019. https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_06-508.pdf
Houchen CJ, Huang C, Lin W. (April, 2018). Deaths by suicide: Disparities in the sunflower state. https://
www.khi.org/policy/article/18-09 (accessed 8/30/2019)
KDHE, Kansas Annual Summary of Vital Statistics (2017). Table E5: Ten leading causes of death by population group
and sex of decedent. http://www.kdheks.gov/phi/AS_Tables/AS_2017_Tables_and_Figures/general_mortality/
Table_E5.pdf (Accessed 7/2/2019).
Leavitt RA, Ertl A, Sheats K, Petrosky E, Ivey-Stephenson A, Fowler KA. (2018). Suicides among American Indian/Alaska Natives – National Violent Death Reporting System, 18 States, 2003-2014. MMWR Morg Mortal Wkly Rep, 67: 237-242. DOI: http://dx.doi.org/10.15585/mmwr.mm6708a1external icon (accessed 8/30/2019)
Moore BJ, Stocks C, & Owens PL. (September, 2017). Trends in Emergency Department Visits, 2006-2014. Health Care Cost and Utilization Project. Agency for Health Care Research and Quality. Statistical Brief #227. https://
scholar.google.com/scholar?hl=en&as_sdt=0%2C5&as_vis=1&q=hcup+statistical+brief+%23227&btnG= (accessed 8/30/2019).
References
categorized into the external cause categories found in the ICD-10 injury mortality matrix https://www.cdc.gov/nchs/data/
ice/icd10_transcode.pdf . These categories were then collapsed into 6 categories: Poisoning which included drugs and not
toxic substances, poisoning plus another mechanism, cut or pierce, asphyxiation, unspecified attempt, and other.
Very few cases had both an ideation and attempt code, but when both of these codes were found, the case was coded as an
attempt. Age-adjusted rates for suicides were obtained from KDHE’s Kansas Information for Communities http://
kic.kdheks.gov/ using the 2000 standard U.S. population. Rates in Figure 1 are age-adjusted per 100,000 population.
Age-specific rates in Figure 4 are per 100,000 population. Age-specific rates in Figure 5 are per 1,000 population. When
rates are unreliable due to small numbers, this is noted in the graph footnote. Crude rates were calculated using the U.S.
Census Bureau’s population estimates as a denominator. When frequencies are reported, numbers less than 6 are suppressed
and are indicated either as a * or a 0.

7
Oakley, David. (May, 2015). Suicides among Kansas residents, 2004-2013. KDHE, Kansas Health Statistics Report, no. 64: 1-4. http://www.kdheks.gov/phi/data_briefs/31_Suicide_2016.pdf (Accessed 8/30/2019).
Oakley D, Crawford G. (December, 2017). Suicide in Kansas, 2016. BEPHI Data Brief, No. 31. http://www.kdheks.gov/phi/data_briefs/31_Suicide_2016.pdf (Accessed 10/30/2019).
Park-Lee, E, Hedden, S.L., and Lipari, R.N. (March 14, 2018). Suicidal thoughts and behavior in 33 metropolitan statistical areas update: 2013-2015. The CBHSQ Report:, Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, Rockville, MD. https://www.samhsa.gov/data/sites/default/files/report_3452/ShortReport-3452.html (Accessed 8/30/2019).
Repp KK, Hawes E, Rees KJ, Lovato C, Knapp A, Stauffenberg M (2019). Evaluation of a novel medicolegal death
investigator-based suicide surveillance system to the National Violent Death Reporting System. American Journal of
Forensic Medicine and Pathology 40(3):227-231.
Stabler M, Perveen G, Haskett, L, & Hart L. (2016). Forced sexual intercourse and suicide attempt among Kansas high
school students: Kansas Youth Risk Behavior Survey 2011-2013. Kansas Health Statistics Report, No. 70. http://
www.kdheks.gov/phi/khsnews/khsr70.pdf (Accessed 8/30/2019).
Stone DM, Simon TR, Fowler KA, et al. (2018). Vital Signs: Trends in State suicide rates – United States, 1999-2016
and circumstances contributing to suicide states – 27 States. 2015. MMWR Morb Mortal Wkly Rep 67: 617-624.
https://www.cdc.gov/mmwr/volumes/67/wr/mm6722a1.htm (Accessed 8/30/2019).
Stone D, Holland K, Bartholow B, Crosby A, Davis S, Wilkins N (2017). Preventing Suicide: A technical package of
policy, programs and practices. Atlanta, GA: National Center for Injury Prevention and Control. Centers for Disease
Control and Prevention. https://www.cdc.gov/violenceprevention/pdf/suicideTechnicalPackage.pdf (Accessed 8/30/2019)
Trust for America’s Health. Pain in the Nation Update: Deaths from alcohol, drugs and suicide reach the highest level
ever recorded https://www.tfah.org/wp-content/uploads/2019/03/TFAH-2019-PainNationUpdateBrief-06.pdf (accessed
8/30/2019).
U.S. Census Bureau (2014). ACS Demographic and Housing Estimates (2014 5-year estimates). Retrieved from https://data.census.gov/cedsci/table?q=population%20of%20Eudora,%20Kansas&lastDisplayedRow=33&table=DP05&tid=ACSDP5Y2014.DP05&g=1600000US2021675&hidePreview=true&y=2014 (Retrieved 8/30/2019)
https://data.census.gov/cedsci/table?q=population%20of%20Baldwin%20City,%20Kansas&lastDisplayedRow=33&table=DP05&tid=ACSDP5Y2014.DP05&g=1600000US2003900&hidePreview=true&y=2014
https://data.census.gov/cedsci/table?q=population%20of%20Lawrence,%20Kansas&lastDisplayedRow=33&table=DP05&tid=ACSDP5Y2014.DP05&g=1600000US2038900&hidePreview=true&y=2014
8
U.S. Census Bureau (2017). ACS Demographic and Housing Estimates (2017 5-year estimates). Retrieved from
https://data.census.gov/cedsci/table?q=Race%20Douglas%20County,%
20Kansas&lastDisplayedRow=82&table=DP05&tid=ACSDP5Y2017.DP05&g=0500000US20045&hidePreview=true
https://data.census.gov/cedsci/table?q=population%20of%20Lawrence,%20Kansas&lastDisplayedRow=33&table=DP05&tid=ACSDP5Y2017.DP05&g=1600000US2038900&hidePreview=true&y=2017
https://data.census.gov/cedsci/table?q=population%20of%20Baldwin%20City%20city,%20Kansas&lastDisplayedRow=36&table=DP05&tid=ACSDP5Y2017.DP05&g=1600000US2003900
https://data.census.gov/cedsci/table?q=population%20of%20Eudora%20city,%20Kansas&lastDisplayedRow=34&table=DP05&tid=ACSDP5Y2017.DP05&g=1600000US2021675
Woolf, SH, Chapman, DA, Buchanich, JM, Snellling LK, et al (May, 2018). Why are death rates rising in the White population of Kansas: The role of Stress-related conditions. Center on Society and Health. University of Pittsburg. https://www.khi.org/assets/uploads/news/14831/mortality_study_final.pdf (accessed 8/30/2019).

DCCF
COMMUNITY
CONVENING
Please jo in us to d iscuss Behavioral Health in Douglas County
Monday, September 23, 2019
5:30pm - 7:30pmTheatre Lawrence
4660 Bauer Farm Dr .

Special thanks to our partners Generous Change, Hall Center forthe Humanities, and media sponsor Lawrence Journal-World.
BIG IDEAS FOR PREVENTION AND HOPEWe invite you to join experts working on BIG IDEAS to improve thehealth of our community.
BIG IDEA Contributors:Dr. Stephen Ilardi, Professor of Psychology, University of KansasGina Meier-Hummel, KS Youth Suicide Prevention CoordinatorLori Alvarado, Chief Executive Officer, DCCCASarah Humbert, Board Member, Van GoNancy Jackson, Generous ChangePatrick Schmitz, Chief Executive Officer, Bert NashSteve Splichal, Superintendent, Eudora Public SchoolsBob Tryanski, Dir. of Behavioral Health Projects, Douglas CountyYOU!