last smallpox victim on earth. prionsprotozoavirusesbacteria little nasty things amebae (dysentary)...
TRANSCRIPT

Last Smallpox Victim on
Earth

PrionsProtozoa VirusesBacteria
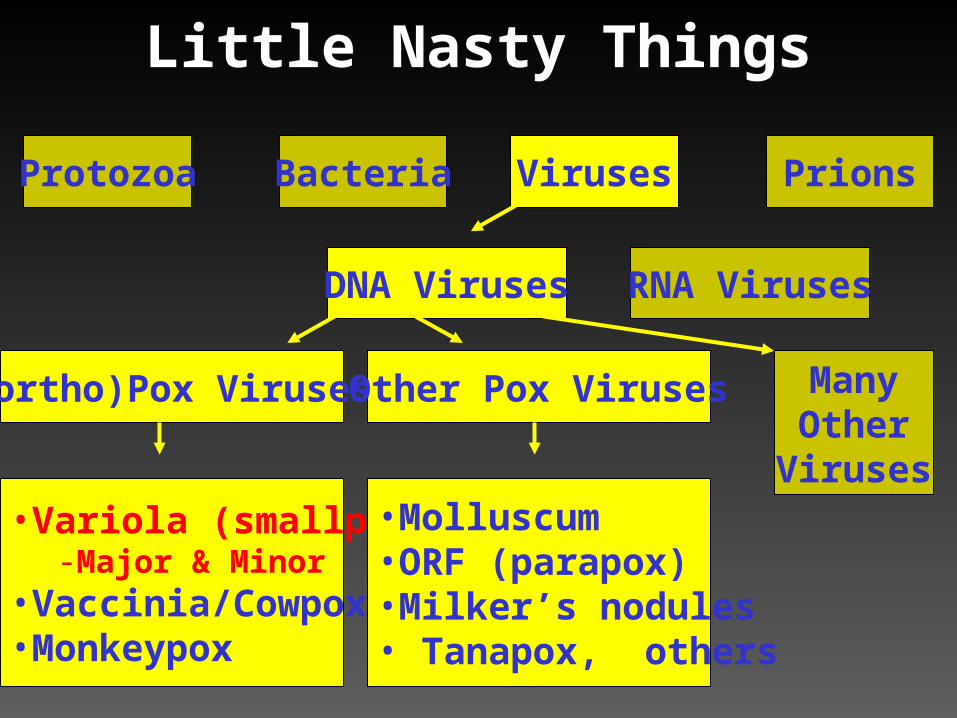
Little Nasty Things
Amebae (dysentary)Plasmodium (malaria)
Mad Cow DiseaseVariant CJD

PrionsProtozoa VirusesBacteria
Little Nasty Things
Amebae (dysentary)Plasmodium (malaria)
Mad Cow DiseaseVariant CJD
E. coli
B. anthracis (Anthrax)
Y. pestis (Plague)
Influenza
Varicella (Chickenpox)
Variola (Smallpox)

RNA VirusesDNA Viruses
Little Nasty Things
PrionsProtozoa VirusesBacteria
RNA VirusesDNA Viruses
Little Nasty Things
(ortho)Pox Viruses
PrionsProtozoa VirusesBacteria
•Variola (smallpox)-Major & Minor
•Vaccinia/Cowpox•Monkeypox
Other Pox Viruses
•Molluscum•ORF (parapox)•Milker’s nodules• Tanapox, others
ManyOther
Viruses

An Orthopox Virus
•Variola (smallpox)-major-minor
•Vaccinia

Variola minor, early 1900’s

Variola minor, early 1900’s

Variola minor, early 1900’s

Epidemiology
• Winter & Early spring – Like measles and chickenpox– Virus killed by heat and humidity
• Age Distribution– Historically affected younger children and
unvaccinated persons– Outbreak now would match age distribution of
population since there is little immunity
Transmission
• Person Person– Primarily droplet, or aerosol– No animal reservoir or vector
• Very contagious, but less than measles or chickenpox
– Less transmissible (lower 2° attack rates)
– Persons are very sick before contagious

18th Century: Native American Blankets

Time Course of Infection
Entry through Oropharynx or Lungs
Virus Multiplies in Lymph Nodes
Spreads through Bloodstream (1° viremia)
Multiplies again in Lymph nodes, Spleen, Bone Marrow
Spreads through Bloodstream (2° viremia)Prodrome: Fever, Headache, Backache, SICK!
Multiplies in mouth and Dermis (deep layer of skin) Rash
NOT Infectious(12-14 d )
NOT Infectious(2-4 d)
VERY Infectious

Fever Curve of Typical Smallpox Case





Last case of smallpox in Bengledesh
(now healthy)

Early Chickenpox

Chickenpox: Varicella-Zoster Virus (VZV)

Chickenpox: Superficial Vesicles

Chickenpox
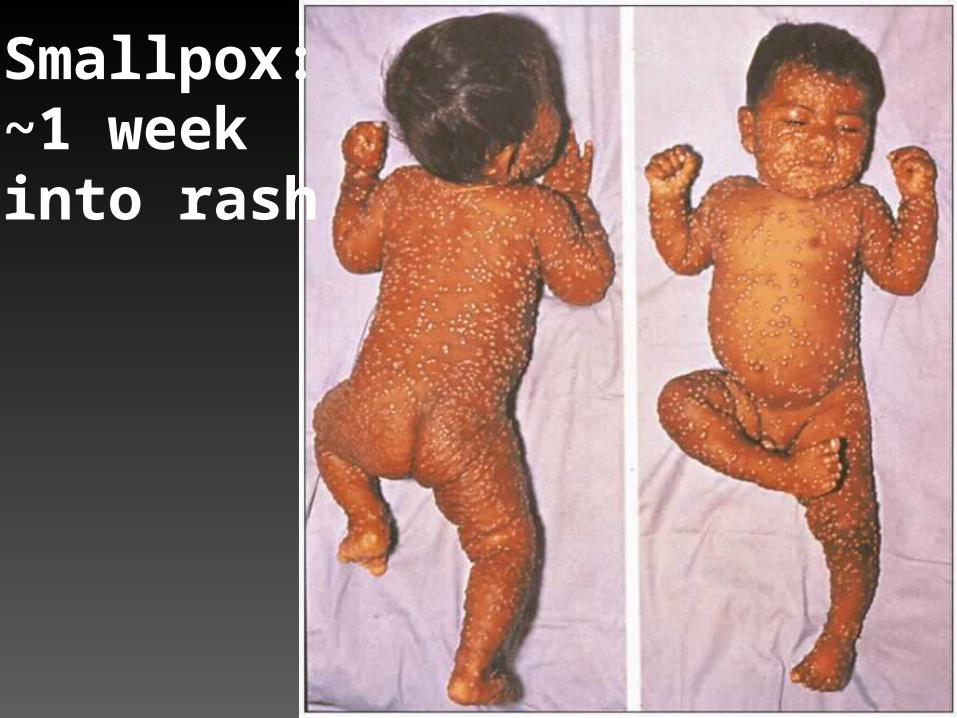
Smallpox:~1 week into rash

Chickenpox

ChickenpoxDifferent sizes & stages

Smallpox

Coxsackie A16Virus

Smallpox

Molluscum Contagiosum

Molluscum Contagiosum

Man Severely Ill with Smallpox

Smallpox Lesions:
Start on Face, (fore)Arms, Mouth
Palms and Soles
Deeply Embedded into Skin
Similar Stage of Development
Occur in Very Sick Persons

Smallpox Complications• Hemorrhagic-type Smallpox: 1 in 20 cases
– More common in pregnant women
• Flat-type Smallpox: 1 in 20 cases
• Encephalitis– Variola major: 1 in 500 cases– Variola minor: 1 in 2000 cases
• Ocular Infection– Blindness in 1% of cases
• Infection transmitted to child in late pregnancy

Case Presentation• 20 y/o woman with Fever, Misery X 2 days• Today, rash appeared on face & arms• Temp 103oF Blood Pressure106/78
Pulse 116/minute Breathing Rate 18/minute• Mentally sound, Lungs clear
• Scattered macules (“spots”) and vesicles noted
• Diagnosis – Chicken pox (Varicella Zoster virus)
• Treatment – oral Acyclovir, recheck in 2 days

What if this wasn’t Chickenpox?
• Patient had history of chickenpox as a child– Unusually severe for atypical or second infection
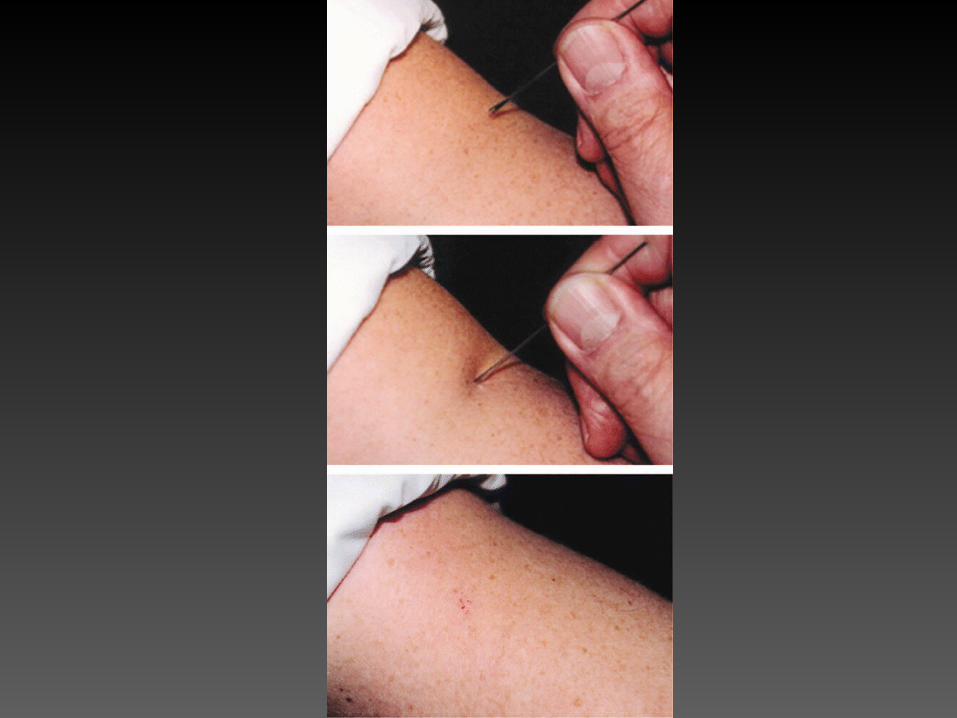
• Need to Diagnose Smallpox ASAP
– “Needle in a haystack”
What if this wasn’t Chickenpox?
• Patient had history of chickenpox as a child– Unusually severe for atypical or second infection
• Need to Diagnose Smallpox ASAP
– “Match in a haystack”
Infection Control Nightmare(Yugoslavia 1972)
1 case Vaccination of 20,000,000

Hospital Infection Control
•Respiratory Isolation Critical
•NOTIFY IMMEDIATELY
–Hospital Infection Control
–Local Health Department

CDC’s Interim Smallpox Response Plan
Self-declared “Work in Progress”

Smallpox Response Plan
• Surveillance• Outbreak Investigation• Outbreak Containment
–Vaccination–Quarantine/Isolation
• Public/Media Communication

Smallpox Response Plan
• Surveillance• Outbreak Investigation• Outbreak Containment
–Vaccination–Quarantine/Isolation
• Public/Media Communication

Smallpox Response Plan
• Surveillance• Outbreak Investigation• Outbreak Containment
–Vaccination–Quarantine/Isolation
• Public/Media Communication

Smallpox Response Plan
• Surveillance• Outbreak Investigation• Outbreak Containment
–Vaccination–Isolation/Quarantine
• Public/Media Communication

Smallpox Response Plan
• Surveillance• Outbreak Investigation• Outbreak Containment
–Vaccination–Quarantine/Isolation
• Public/Media Communication
Surveillance• Pre-event (baseline) Rash Surveillance• Notification for suspected smallpox case,
outbreak, contamination or distribution: – Local Health Department– State Health Department CDC
• Emergency Preparedness and Response Branch • Bioterrorism Preparedness and Response Program• Poxvirus Section, Division of Viral and Rickettsial
Diseases
• Case Definitions and Clinical Appearance

Surveillance: Case Definition
• Major Criteria– Fever > 102°F before rash onset– Classical smallpox lesions– Lesions at same stage of development
• Minor Criteria– Patient is “toxic” or moribund– Rash began on forarms, face, or mouth– Rash includes palms and soles– Centrifugal distribution (extremities > trunk)– Slow evolution of rash

Surveillance:Smallpox Case Categories• Low Probability
– No Fever– Fever and no other major and <4 minor criteria
• Moderate Probability: Fever +– 1 other major, or– > 4minor criteria
• High Probability: all 3 major criteria
Outbreak Investigation• Active Surveillance for Smallpox
– Local, state, national, international
• Surveillance for Adverse Vaccine Reactions
• Epi Investigation of Cases
• Contact Tracing
• Specimen Collection & Transportation
• Laboratory Confirmation (at CDC )– Detecting Smallpox Directly in Tissues– Viral Culture– Molecular Fingerprinting using PCR
Outbreak Containment:Vaccination Activities
• CDC vaccine deployment strategy
• Set up vaccination clinics
• Educate a pool of vaccinators– Recognize vaccine “take”– Recognize and treat adverse events– Safe handling of vaccine
• MASS VS. TARGETED VACCINATION?
Outbreak Containment:Ring Vaccination
• Strategy used for smallpox elimination
• Avoids recurring cost of mass vaccination
• Avoids unacceptably high, recurring risk of mass vaccination
• Strengthen public health surveillance infrastructure for ALL infectious diseases– Smallpox vaccine prevents only smallpox

Isolation of Smallpox Victim in Australia

Outbreak Containment:Isolation Categories
• Isolation Units (smallpox hospitals): contagious persons
• Observation Units (for persons with fever but no rash after smallpox contact): possibly contagious persons awaiting triage
• Home Fever Surveillance with travel restriction: for exposed or vaccinated persons
Outbreak Containment:Levels of Quarantine
• Education/Notification
• Suspension of Gatherings
• Restriction on Travel
• Blockade (“cordon sanitaire”) and community-wide interventions

Communication• Training for Local/State Health Departments
– Webcasts– Workshops
• Direct public education
• During an Event: – Contact Information– Education of General Public– Media Relations

Other Critical Issues
• Infrastructure Development
• Inter-Agency Coordination
Final Thoughts• Smallpox can be recognized early in the
course of an outbreak, incumbent on:– Provider and public awareness– Public health surveillance capacity
• Outbreaks probably not avoidable, but could (theoretically) be contained– Prodromal symptoms– Rash identifiable– Contagious persons unlikely to travel extensively

Final Thoughts II• Public health agencies will play a critical role in
incident command (i.e., what do we do now?)– Important but political– Uncomfortable decisions
• Unprecedented (not yet available) public health “surge capacity” is crucial to early outbreak containment – Dual-use infrastructure may become
important method of efficiently using smallpox resources

Questions & Answers
Smallpox plan available at:
http://www.bt.cdc.gov/DocumentsApp/Smallpox/RPG/index.asp

Summary III
Cancer
AIDS
Summary IV
Cancer
AIDS

Summary V
Bioterrorism

Summary VI
Cancer
AIDS BT
Summary VII
Cancer
AIDS
BT

Smallpox Vaccination Complications(a live virus vaccine)
• Disseminated vaccinia
• Eczema vaccinatum
Points:
• For each 1 million vaccinated, there were ~ 250 complications• Vaccine immune globulin (VIG) Rx is needed - short supply
Pre-AIDS!