lactate measured in diluted and undiluted - clinical chemistry
TRANSCRIPT

2430 CLINICAL CHEMISTRY, Vol. 38, No. 12, 1992
donor liver and early outcome oftransplantation. Transplant Proc1991;23:1575-8.4. Schroeder TJ, Gremse DA, Mansour ME, et a!. Lidocainemetabolism as an index of liver function in hepatic transplantdonors and recipients. Transplant Proc 1989;21:2299-301.5. Nation RL, Peng GW, Chiou WL. High-performance liquidchromatographic method for the simultaneous determination ofhidocaine and its N-dealkylated metabohites in plasma. J Chro-matogr 1979;162:466-73.6. Hill J, Roussin A, Lelorier J, Caille G. High-pressure liquidchromatographic determination of lidocaine and its active do-ethylated metabohites. J Pharm Sci 1980;69:1341-2.7. Verbesselt R, Ijandramaga TB, De Schepper PJ. High-perfor-mance liquid chromatographic determination of 12 antiarrhyth-mic drugs in plasma using solid-phase column extraction. TherDrug Monit 1991;13:157-65.8. Chen Y, Potter JM, Ravenscroft PJ. A high-performance liquidchromatographic method for the simultaneous determination ofMEGX and hignocaine. J Chromatogr 1992;574:361-4.9. Chen Y, Potter JM, Ravenscroft PJ. A quick, sensitive HPLC
CLIN. CHEM. 38/12, 2430-2434 (1992)
assay for MEGX and hignocaine in serum/plasma using solid-phaseextraction. Ther Drug Monit (in press).10. Bland JM, Altman DG. Statistical methods for assessingagreement between two methods of clinical measurement. Lancet1986;i:307-10.
11. Scott CB, Henderson A, Potter JM, et al. Impaired hepaticmetabolism of IV lignocaine as an index of cellular damage fromcarbon monoxide poisoning. Med J Aust 1992;156:367.12. Schroeder TJ, Tasset JJ, Poses AJ. Lidocaine metabolism asan indicathr of liver function. Am Assoc Cliii Chem TDM-T1990;12(3):7-13.13. Thomson AH, Kelnian AW, Vane PJ, Hills WS, Whiting B.Changes in hignocaine disposition during long-term infusion inpatients with acute ventricular arrhythmias. Ther Drug Momt1987;9:283-91.14. Sherwin JE. Liver function. In: Kaplan LA, Pesos AJ, eds.Clinical chemistry. St. Louis, MO: CV Mosby, 1984:420-38.15. Potter JM, Hickman PE, Balderson GA, Lynch SV, Strong R.Lignocaine metabolism and MEGX production in the liver trans.plant donor. Transplant Proc 1992;24:198-9.
Lactate Measured in Diluted and Undiluted Whole Blood and Plasma: Comparison ofMethods and Effect of Hematocrit
John Toffaletti, Mary Ellen Hammes, Rudethia Gray, Beverly Lineberry, and Billy Abrams
We evaluated a new analyzer that measures lactate inundiluted whole blood by direct (or undiluted) amperom-etry [Nova Stat Profile 7 Analyzer (SP7); Nova Biomedi-cal, Waltham, MA] by comparing it with two other anaiyz-ers, one for measuring lactate in whole blood by indirect(or diluted) amperometry [Model 2300; Yellow SpringsInstrument Co. (YSI), Yellow Springs, OH] and another formeasuring lactate in plasma by enzymatic coiorimetry(aca; Du Pont Co., Wilmington, DE). All between-methodcomparisons of the three methods showed that the resultsfor plasma were comparable (S�1� = 0.24-0.33 mmol/L).Within-method comparisons by the YSI differed substan-tiaily between plasma and whole blood (Si,,, = 0.48
mmoi/L), but within-method comparisons by the SP7produced better agreement between plasma and whole
blood � = 0.18 mmol/L). The difference betweenwhole blood and plasma by YSI is reiated to hematocrit,with the greatest differences noted for samples with thehighest hematocrit. Serum lactate measured by SP7 hadbetween-day imprecision (CV) ranging from 1 2% at 0.5mmoi/L to 4.2% at 3.7 mmoi/L, showed a linear standardcurve to at least 1 1 .5 mmol/L, and was independent ofhematocrit. There was a mean bias of �-0.4 mmol/L forresults in the reference range for both plasma and whole
blood by SP7 compared with plasma results by either acaorYSi.
AdditIonal Keyphrases: amperometry . enzymatic co!orimetiycompared
Measuring blood lactate concentrations is importantfor detecting impaired circulatory and tissue oxygen-ation in critical-care patients (1-4). Because most crit-ical-care monitoring requires rapid availability of re-
sults, methods that measure lactate quickly in wholeblood are desirable. Although an analyzer that mea-sures lactate in whole blood both rapidly (45 s) and in a
small sample volume (25 �L) is available (5), themethodology requires dilution of whole blood before
measurement oflactate, introducing an analytical error
that increases with increasing hematocrit. An equationmay be used to correct for hematocrit (5), but this has atleast two drawbacks: correction ofresults by equation isinherently inaccurate, and correction requires measur-ing one or more additional variables. Furthermore,direct measurements in plasma and whole blood, bydetecting the molahity of constituents such as glucose(6), detect the physiologically and clinically relevantquantity. Therefore, the availability of a direct-readingelectrode method for measuring lactate in whole bloodthat is unaffected by hematocrit would be desirable forcritical-care monitoring.
Materials and Methods
Blood Gas Services, Division of Clinical Laboratories, Depart-ment ofPathology, P0 Box 3015, Duke University Medical Center,Durham, NC 27710.
Received March 13, 1992; accepted July 24, 1992.
Instrumentation. The enzymatic colorimetric methodfor the aca (Du Pont Co., Wilmington, DE) uses rabbitmuscle lactate dehydrogenase (EC.1.1.1.27) to catalyze
the oxidation ofL-lactate to pyruvate with simultaneous

CLINICAL CHEMISTRY, Vol. 38, No. 12, 1992 2431
reduction of NAD�. The formation of NADH, which is
proportional to lactate concentration, is monitored asthe difference in absorbance at 340 run (analytical) and
383 nm (background). The method requires 40 p�L of
serum, plasma, or cerebrospinal fluid (CSF).The diluted amperometric method of the YSI Model
2300 (Yellow Springs Instrument Co., Yellow Springs,OH) was described previously (5). This method uses a
lactate-sensitive electrode in which L-lactate oxidase isattached to one of the membrane layers covering the
electrode. This method measures lactate in 25 p.L ofwhole blood, plasma, or CSF diluted with 600 �L of
buffer.
The undiluted amperometric method on the Nova
Stat Proffle 7 analyzer (SP7; Nova Biomedical,Waltham, MA) uses a lactate-sensitive electrode inwhich L-lactate oxidase is immobilized on a membrane
covering an amperometric electrode. The reactions aresimilar to those for the YSI method (5). Briefly, lactate
oxidase generates hydrogen peroxide from lactate and
oxygen. The H202 diffuses to a platinum anode held at apotential of +0.7 V relative to a silver reference cathode.The H202 is then oxidized to 02 at the amperometricelectrode. The method measures lactate in 190 �L ofwhole blood, plasma, or CSF. The instrument is cali-brated with aqueous solutions containing lactate at
either 1, 3, or 10 mmol/L.
Cost and longevity ofmembranes. During the 50 daysof our study, we changed the lactate electrode mem-
brane (part no. 09925) on the SP7 eight times. Thus,new membranes were required about every 6 days. As of
November 1991, lactate membranes cost -�--$14 each.Over the past year, lactate membranes for the YSI haverequired changing about every 7 days. As of November
1991, the list price for the YSI electrodes was ‘-$20each. For the Du Pont aca, individual lactate reagentpacks had a 1991 list price of $2.09.
Controls. We used both aqueous and serum-basedmaterials as controls. The aqueous material was sup-
plied by Nova as the Stat Profile Control, levels 1, 2, and3. The ranges (in mmol/L) for each were as follows:0.3-0.7, 1.0-1.4, and 3.4-4.2, respectively.
The serum-based materials were prepared from
pooled sera that contained both normal and high con-
centrations of lactate. Individual portions of each poolwere frozen in 2.5-mL plastic screw-cap tubes. Theseportions were stored frozen and were thawed on the day
of analysis.Blood-collection devices. We used the following blood-
collection devices: 20-mL plain syringes (Becton Dickin-son Co., Rutherford, NJ); 3-mL syringes with 40 kIU/L
calcium-titrated lyophilized heparin (Radiometer Amer-ica, Westlake, OH); 3-mL syringes with 15 kJU/L dry
lithium heparin (Martell Medical Products, Temecula,CA); 3-mL evacuated tubes containing 1.5 mg of lithium
iodoacetate and 43 RI oflithium heparmn (Becton Dick-inson); and 7-mL evacuated tubes containing 15 kIUIL
lithium heparin (Becton Dickinson).Our results corroborated the reference interval for
venous plasma lactate established at Duke Medical
Center, 0.5-2.2 mmol/L. This range was determined in
plasma from blood collected into fluoride/oxalate tubesfrom ‘-30 apparently healthy individuals and analyzedwith the Du Pont aca. The upper limit of 2.2 mmolIL
included �95% of the results.Whole blood andplasma for rnethod-compari�on stud-
ies. Immediately after collecting blood in 3-mL heparin-ized syringes containing 15 kIUfL lithium heparin, we
transferred ‘-2 mL of blood to 2.5-mL capped plastictubes and centrifuged the tubes to obtain plasma. The
original heparinized whole blood was analyzed as soon
as possible.Modification ofhematocrit in whole-blood samples. To
obtain samples with either high or low hematocrits, we
centrifuged the whole-blood samples from several vol-unteers and then selectively removed either plasma (toincrease hematocrit) or erythrocytes (to decrease hemat-
ocrit).
Volunteers. We collected blood both from apparently
healthy people and from patients during surgery (ages19-65 years). All had read and signed a consent formapproved by the Duke Medical Center Review Board forClinical Investigations.
Interfereru,e studies. To study the effect of potentiallyinterfering compounds, we prepared concentrated aque-ous solutions (100 or 200 m.mollL) of the followingchemicals: L-ascorbic acid (176.1 g/mol; Fisher Scien-tific, Fair Lawn, NJ); pyruvic acid, sodium salt (110
g/mol); acetoacetic acid, lithium salt (108 g/mol); andf3-hydroxybutyric acid, sodium salt (126.1 g/mol), allfrom Sigma Chemical Co., St. Louis, MO.
Statistical cakulations. The regression equations, cor-relation coefficients (r), and standard errors of y on x(S,,�) were calculated by least-squares analysis as de-
scribed by Barnett (7). The established methods used forcomparison (x) were in priority of higher to lower val-
ues: plasma by aca, plasma by YSI, whole blood by YSI.
Results
Within-analyzer and between-analyzer comparisons.
The results for lactate measured in whole blood andplasma by the two methods are compared in Table 1.Although there is a large variability between the
plasma and whole-blood results by YSI � 0.48mmol/L), the plasma-whole-blood variability is rela-
Table 1. Summary of Whole-Blood (WB) and Plasma
(P) Comparisons between Methods
syx,n r mmol/L
81 SP7-P = 0.92 (YSI-P) + 0.46 mmol/L 0.993 0.33
68 SP7.P 0.91 (aca-P) + 0.63 mmoVL 0.993 0.3379 SP7-WB = 0.95 (SP7-P) + 0.1 5 mmoVL 0.997 0.1881 SP7-WB = I .1 9 (YSI-WB) + 0.82 mmol/L 0.965 0.7281 SP7-WB = 0.86 (YSI-P) + 0.67 mmoVL 0.991 0.3355 SP7WB = 0.86 (aca-P) + 0.81 mmoIIL 0.990 0.34
70 YSI-P = 1 .00 (aca-P) + 0.1 9 mmol/L 0.997 0.24
81 YSI-WB = 0.73 (YSI-P) - 0.23 mmoVL 0.974 0.4855 YSI-WB = 0.72 (aca-P) - 0.02 mmoVL 0.982 0.39
Equation

MeanSD95% reference interval
n = 19.
lactate concentration, we collected blood into 20-mLsyringes. We then distributed the blood from each sy-
ringe into three blood-collection containers: one syringe
with 40 kIi.JIL calcium heparin, one tube with 15 kIU/Llithium heparin, and one tube with 15 kIU/L lithium
heparin and 0.15 g/L lithium iodoacetate. To serve as
the control sample from each donor, whole blood col-lected without anticoagulant was analyzed by SP7
within 2 mm after collection to provide results mini-
mally affected by either cellular metabolism or antico-
agulants (8).Although the mean differences from results for the
control sample differed little among the three containersstudied, both the syringe containing 40 kIU/L dry cal-
cium-titrated heparin and the evacuated tube contain-
ing 15 kfl.JIL dry lithium heparin gave the most consis-
tent results (in mmollL), -0.2 ± 0.14 (mean ± SD,
range -0.3 to 0.1) and 0.07 ± 0.16 (range -0.3 to 0.3),
respectively. The calcium heparin syringe showed theleast variability, closely followed by the lithium heparin
tube. lodoacetate heparin tubes gave the highest van-
ability (0.06 ± 0.30 mmolfL), with differences ranging
from -0.5 to +0.5 mmol/L. This suggests that hepanin isa satisfactory anticoagulant if samples are either stored
in ice or analyzed soon after collection.
Effects of storage time and temperature on lactate
concentrations. We collected both plasma and hepanin-
ized whole blood (containing 15-20 kIUIL heparin) fromfive volunteers to establish the effects of storage timeand temperature on the stability of lactate concentra-tions measured by the SP7. Our data showed that
plasma was quite stable: storage on ice showed no
detectable change after 120 mm, and plasma stored at
room temperature changed by only 0.1 mmolJL after 120mm. Whole blood was also stable when stored in an icebath, changing by 0.1 mmolJL after 60 mm and by 0.2mmol/L after 120 mm. Although the above conditions
would be acceptable for at least 60 mm, in whole bloodstored at room temperature lactate increased by --0.5
mmol/L after 30 mm. Clearly, room-temperature stor-
age of heparinized whole blood must be avoided.Potential interferents. To determine the effect of pa-
____ tential interfering substances on lactate measured by
SD cv, s the SP7, we diluted serum 9:1 with a solution contain-ing, per liter, either 160 mmol of NaC1 (control), 200
8.5 mmol of acetoacetate, 100 mmol of pyruvate, 200 mmol6.3 of /3-hydroxybutyrate, or 100 mmol of ascorbate. To0 avoid the possible enzymatic conversion of pyruvate to
0 0 lactate in serum, we also studied the potential interfer-I .1 ence of pyruvate by diluting 100 mmol/L pyruvate 9:10.6 with an aqueous solution containing 5 mmol/L lactate.5.0 The results indicate that only ascorbate at 10 mmol/L6.2 had a detectable effect, lowering the measured lactate1 .4 concentration by 0.3 mmol/L. Because 10 mmolfL ascor-1 .5 bate is 50- to 100-fold greater than the usual plasma
concentration, ascorbate would rarely, if ever, interfere12.1 with the amperometric measurement of lactate.
� Effect ofhematocrit on differences in lactate concentra-. tion. To study the effect ofhematocrit on lactate results,
- we adjusted hematocrits to 0.18-0.69 by selectively
YSI
1.36
0.440.5-2.2
Table 3. PrecIsion of Lactate Measurements byUndiluted Amperometry (SP7)
Lactate, mmol/L
Aqueous
Serum
Serum
Between-day (n = 41)Aqueous
AqueousAqueous
0.5 0.061.2 0.033.7 0.15
a Aqueous or serum-based control material.
2432 CLINICAL CHEMISTRY, Vol. 38, No. 12,1992
tively small by SP7 (S� = 0.18 mmolIL). The compari-
sons between aca and YSI for plasma give less variabil-ity (S�� = 0.24 mmol/L) than do the comparisons
between either aca and SP7 or YSI and 5P7 (S�� = 0.33mmol/L). The y-intercept data are higher by 0.5-0.8
mmol/L for SP7 compared with either aca or YSI.Because hematocrit is not an issue in plasma compari-
sons, these differences may be due either to calibrationset points or plasma water content (6). Correcting for
plasma water content (dividing aca results by 0.93) didnot improve agreement; we conclude that differences incalibration set points accounted for the bias.
We collected 19 samples from persons having a lactate
concentration within our reference interval of 0.5-2.2mmol/L (venous plasma by colorimetric method) (Table
2). In this range of lactate concentrations, results from
both amperometric methods (SP7 and YSI) were higherthan by the colorimetric method (aca); results from SP7
were the highest, -0.4 mmol/L higher than by aca.
Precision. Between-day precision was determined by
analyzing three concentrations of aqueous controls for41 days. Within-run precision was studied by analyzing
the three aqueous controls and two pools of human
serum 20 times on each of 2 days. Results of between-day and within-run precision are shown in Table 3.
Blood-collection containers for lactate analyses. From
each of 10 healthy volunteers, some of whom had exer-
cised before blood was collected to increase the blood
Table 2. Lactate Concentrations (mmol/L) In PlasmaSamples in the aca Reference Interval
ace SP7
1.17 1.56
0.48 0.450.4-2.1 0.7-2.5
Matsrlal Mean
Within-run (n = 20)Aqueous 0.5 0.04
0.03Aqueous 1.2 0
3.7 0.040.02
1.3 0.070.08
7.9 0.110.12
12
10
,27‘20
I2
I023 133 Ii
CLINICAL CHEMISTRY, Vol. 38, No. 12, 1992 2433
removing either packed erythrocytes or plasma from 25
samples of blood that had settled in syringes. As ex-
pected from a previous study (5), hematocrit was signif-
icantly related to the difference between lactate in
whole blood measured by YSI and in either plasma
measured by YSI or whole blood measured by 5P7
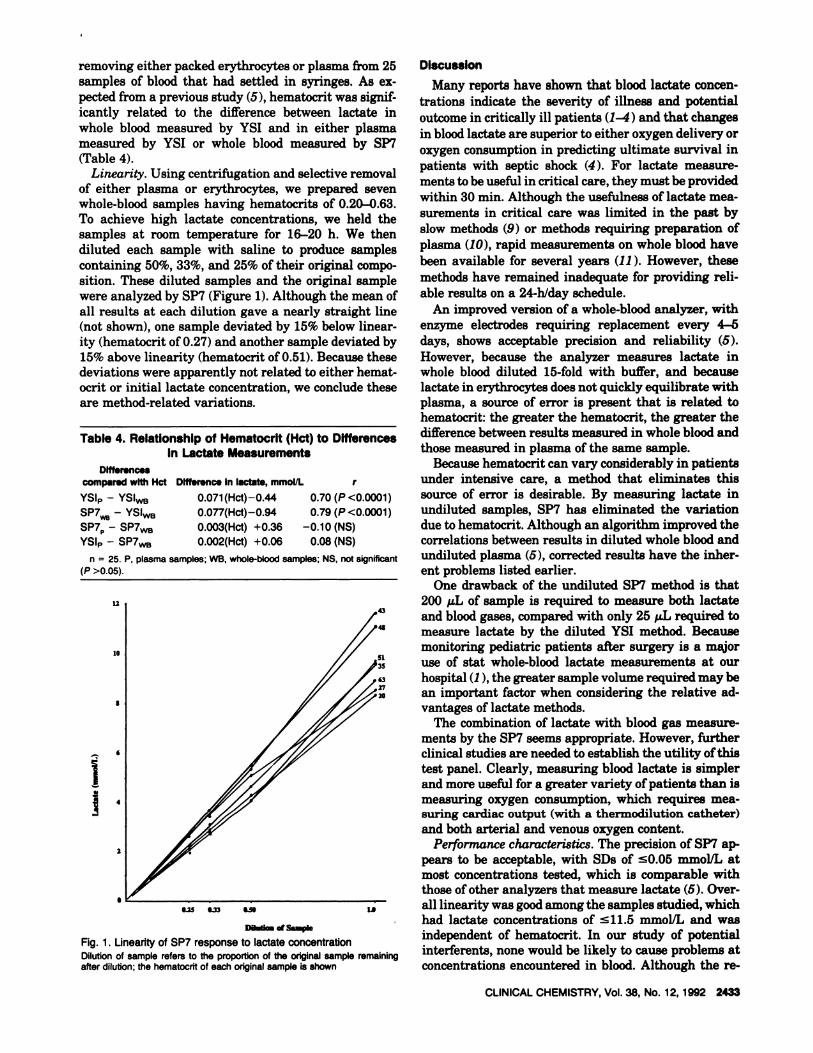
(Table 4).Linearity. Using centrifugation and selective removal
of either plasma or erythrocytes, we prepared sevenwhole-blood samples having hematocrits of 0.20-0.63.
To achieve high lactate concentrations, we held thesamples at room temperature for 16-20 h. We then
diluted each sample with saline to produce samples
containing 50%, 33%, and 25% of their original compo-sition. These diluted samples and the original sample
were analyzed by SP7 (Figure 1). Although the mean ofall results at each dilution gave a nearly straight line(not shown), one sample deviated by 15% below linear-
ity (hematocrit of 0.27) and another sample deviated by
15% above linearity (hematocrit of 0.51). Because thesedeviations were apparently not related to either hemat-
ocrit or initial lactate concentration, we conclude these
are method-related variations.
Table 4. RelatIonship of Hematocrlt (Hct) to DifferencesIn Lactate Measurements
Dlffessncss
comparsd wIth Hct Difference In lactate, mmolIL r
YSI� - YSIWB 0.071(Hct)-0.44 0.70 (P <0.0001)
� � YSI� 0.077(Hct)-0.94 0.79 (P <0.0001)SP7� - SP7�8 0.003(Hct) +0.36 -0.10 (NS)YSI� - SP7WB 0.002(Hct) +0.06 0.08 (NS)
n = 25. P. plasma samples; WB, whole-blood samples; N5. not significant
(P >0.05).
Da�l_�sa_
Fig. 1 . Linearity of SP7 response to lactate concentrationDilution of sample refers to the proportion of the original sample remainingafter dilution; the hematocrft of each original sample is shown
Discussion
Many reports have shown that blood lactate concen-trations indicate the severity of illness and potential
outcome in critically ill patients (1-4) and that changes
in blood lactate are superior to either oxygen delivery or
oxygen consumption in predicting ultimate survival in
patients with septic shock (4). For lactate measure-
ments to be useful in critical care, they must be provided
within 30 mm. Although the usefulness oflactate mea-
surements in critical care was limited in the past by
slow methods (9) or methods requiring preparation of
plasma (10), rapid measurements on whole blood have
been available for several years (11 ). However, these
methods have remained inadequate for providing reli-
able results on a 24-h/day schedule.
An improved version of a whole-blood analyzer, with
enzyme electrodes requiring replacement every 4-S
days, shows acceptable precision and reliability (5).However, because the analyzer measures lactate inwhole blood diluted 15-fold with buffer, and becauselactate in erythrocytes does not quickly equilibrate with
plasma, a source of error is present that is related to
hematocrit: the greater the hematocrit, the greater the
difference between results measured in whole blood and
those measured in plasma of the same sample.
Because hematocrit can vary considerably in patients
under intensive care, a method that eliminates this
source of error is desirable. By measuring lactate inundiluted samples, SP7 has eliminated the variation
due to hematocnit. Although an algorithm improved the
correlations between results in diluted whole blood and
undiluted plasma (5), corrected results have the inher-
ent problems listed earlier.One drawback of the undiluted SP7 method is that
200 �AL of sample is required to measure both lactate
and blood gases, compared with only 25 p.L required to
measure lactate by the diluted YSI method. Because
monitoring pediatric patients after surgery is a major
use of stat whole-blood lactate measurements at our
hospital (1 ), the greater sample volume required may bean important factor when considering the relative ad-
vantages of lactate methods.The combination of lactate with blood gas measure-
ments by the SP7 seems appropriate. However, further
clinical studies are needed to establish the utility of thistest panel. Clearly, measuring blood lactate is simpler
and more useful for a greater variety ofpatients than ismeasuring oxygen consumption, which requires mea-suring cardiac output (with a thermodilution catheter)
and both arterial and venous oxygen content.
Performance characteristks. The precision of SP7 ap-
pears to be acceptable, with SDs of sO.05 mmol/L atmost concentrations tested, which is comparable withthose ofother analyzers that measure lactate (5). Over-
alllinearity was good among the samples studied, which
had lactate concentrations of �11.5 mmollL and was
independent of hematocrit. In our study of potentialinterferents, none would be likely to cause problems at
concentrations encountered in blood. Although the re-

2434 CLINICAL CHEMISTRY, Vol. 38, No. 12, 1992
ducing substance ascorbate, at -100-fold a normal con-
centration, lowered lactate slightly (by 0.3 mmolIL), this
should not be significant in any samples from patients.
The main concern we have with lactate measured by
the SP7 method described here is that the results,
particularly at lower concentrations, appear to be --0.3-
0.4 mmol/L higher than other methods. Correcting for
the average difference in water content ofplasma (0.93)
did not appreciably lower this bias between methods;
therefore, we conclude that the calibration set points for
the SP7 should be modified by the manufacturer.
The necessity to change the lactate oxidase mem-
brane about every 6 days may be acceptable for opera-
tion in high-test-volume clinical laboratories. However,
for laboratories with fewer tests for lactate, a cost of
--$14 for each membrane may be comparable with the
prepackaged colorimetric (aca) test pack.
By comparing results from anticoagulated blood with
results from uncoagulated blood analyzed immediately
after collection, we show that heparin is a satisfactory
anticoagulant and is preferred over heparinized tubes
containing iodoacetate. However, whole-blood samples
must be kept in ice until they are either analyzed or
centrifuged to obtain plasma. Whole blood appears to be
stable for at least 60 mm when stored in an ice bath.
With a slight adjustment of calibrator set points, theSF7 method for lactate can provide potentially accurate,precise, and linear results in an analyzer that is inde-pendent of hematocrit. Because the analyzer also mea-
sures pH, Pco2, and P02, further studies are needed to
CLIN. CHEM. 38/12, 2434-2489 (1992)
establish the clinical value of this apparently logicalcombination of tests in critical care.
We acknowledge the financial support of Nova Biomedical in
this study.
References1. Toffaletti JG. Blood lactate: biochemistry, laboratory methods,and clinical interpretation. Crit Rev Clin Lab Sci 1991;28:253-68.2. Rashkin MC, Bosken C, Baughman RP. Oxygen delivery incritically ill patients: relationship to blood lactate and survival.Cheat 1985;87:580-4.3. Vincent J-L, Dufaye P, Berre J, Leeman M, Degante J-P, KahnRJ. Serial lactate determinations during circulatory shock. CritCare Med 1983;11:449-51.4. Bakker J, Coffernils M, Leon M, Gris P, Vincent J-L Bloodlactate levels are superior to oxygen-derived variables in predict-ing outcome in human septic shock. Chest 1991;99:956-62.5. Wandrup J, Tvede K, Grinsted J, Jordening H. “Stat” measure-ments of L-lactate in whole blood and CSF assessed. Cliii Chem1989;35:1740-3.6. Fogh-Andersen N, Wimberley PD, Thode J, Siggaard-Andersen0. Direct reading glucose electrodes detect the molality of glucosein plasma and whole blood. Clin Chim Acta 1990;189:33-8.7. Barnett RN. Clinical laboratory statistics, 2nd ed. Boston:Little, Brown, 1979:50-2.8. Toffaletti J, Ernst P, Hunt P, Abrams B. Dry electrolyte-balanced heparinized syringes evaluated for determining ionizedcalcium and other electrolytes in whole blood. Cliii Chem 1991;37:1730-3.9. Marbach EP, Weil MH. Rapid enzymatic measurement of bloodlactate and pyruvate: use and significance ofmetaphosphoric acidas a common precipitant. Clin Chem 1967;13:314-25.10. Westgard JO, Lahmayer BL, Birnbaum ML. Use of the DuPont “Automatic Clinical Analyzer” in direct determination oflactic acid in plasma stabilized with sodium fluoride. Cliii Chem1972;18:1334-8.11. Geyssant A, Dormois D, Barthelemy JC, Lacour JR. Lactatedetermination with the lactate analyzer LA 640: a critical study.Scand J Clin Lab Invest 1985;45:145-9.
Performance of an Enzyme-Linked Immunosorbent Assay System for Antibodies toHepatitis C Virus with Two New Antigens (ci 1/c7)
Miho Saito,’ Akira ase2 Tomiko Kashiwakuma,’ Michinori Kohara,’ Masahito Sugi,’ Keizaburo Mlki,�TakayUki Yainamoto,3 Hiroyuki Mon,3 Yohsuke Ohta,3 Eiji Tanaka,4 Kendo Kiyosawa,4 Selichi Furuta,4Masanobu Wakashima,5 Satoshi Tanaka,5 and Nobu Hattori5
We developed an enzyme-linked immunosorbent assay(ELIsA) system for antibodies to the hepatitis C virus(HCV), using two new recombinant antigens (ci 1 and c7)derived from the HCV genome. The performance of this
1 Tonen Corporation, Fundamental Research Laboratory, 1-3-1,
Nishiteurugaoka, Ohi-Machi, Iruma-Gun, Saitama 354, Japan.2 Author for correspondence.
3 International Reagents Corporation, 1-1-2, Murotani, Nishi-Ku, Kobe 651-22, Japan.
4 Department of Internal Medicine, Shinshu University Schoolof Medicine, Matsumoto 390, Japan.
5 Liver Unit, The Tokyo Metropolitan Komagome Hospital,Tokyo 113, Japan.
Received March 2, 1992; accepted July 21, 1992.
ELISA system (Imucheck HCV Ab) was examined. The CVvalues for both intra-assay precision and reproducibility ofidentifying HCV antibody in the panel sera ranged from3.5% to 6.4%. The blood elements in serum and antico-agulants did not interfere in this ELISA system. The spec-ificity of Imucheck HCV Ab to samples from patients withnon-A, non-B (NANB)-type chronic hepatitis, liver cirrho-sis, and hepatocellular carcinoma was 93.7%, 93.5%, and
� 81 .4%, respectively. These results are more sensitivethan those obtained by the first-generation anti-HCV ELISAsystem. In the samples from patients with NANB-typeacute hepatitis, Imucheck HCV Ab enabled detection ofHCV antibodies at an early stage. This system increasedthe sensitivity for blood donor screening and for monitor-ing patients with acute hepatitis.