labor and delivery - mercy medical center, des moines, iowa
TRANSCRIPT

L A B O R A N D D E L I V E RY
Prepar ing for Bir th • 51
Signs of Labor • 54
Options for Managing Labor Pain• 56
Labor • 62
Bir th • 63
49


51
Throughout your pregnancy, you will find yourself doing a lot of planning. Being
prepared for the experience of having a baby allows you to be a knowledgeable
participant in your care. During childbirth, you and your partner will have many
options. Attending childbirth classes, talking with your physician and using this
book will help you make knowledgeable decisions about the birth of your baby.
Preparing for Your Baby’s BirthThere are three basic areas that are most helpful in getting ready for childbirth:
• Learn as much as you can about your pregnancy and the birth of your child.
Mercy offers a large variety of classes that will help you make informed decisions.
• Prepare physically. Take good care of your body and pay attention to your feelings
and emotions. Your body goes through a number of changes during pregnancy.
Childbirth and exercise classes can help you learn to prepare physically for delivery.
• Learn about the pain management options to make your labor and delivery more
comfortable. Childbirth is different for every woman. Some are able to manage
labor through only pain management techniques or medications and some may
prefer to use a combination of both. It’s important to learn all about the pain
management options so you can make informed choices during labor.
This is an exciting time for you and your family. By being well prepared, you can
share the joy knowing you are giving your baby the best possible start in life. For a
complete list of childbirth education classes, turn to the Expert Care at Mercy
chapter, call (515) 643-MOMS or log on to our website at www.mercydesmoines.org
Preparing for LaborAs your due date approaches, you should begin the final preparations for the arrival
of your baby. During the last month of pregnancy is the time to put the finishing
touches on your nursery, make child care arrangements for older siblings and pack
your bag for the hospital. Checklists are a good way to make sure you have covered
every detail and are ready when your first contraction begins. The following is a list
of items and ideas that will help you get organized for your little one’s arrival.
Take care of as many things in advance as possible
• Complete your pre-admission forms and turn them in to your childbirth
education instructor or mail them to the Mercy Admitting department.
la
bo
r
an
d
de
li
ve
ry
Labor and Delivery

52
• Complete your Birth Plan and Newborn Communication Plan.
• Make sure your nursery is ready and stocked with everything your baby will need.
• Arrange for the care of siblings and pets – always have a backup plan.
• If possible, arrange for help for you and your baby when you return home.
What to Pack for the Hospital For Mom:
• This book
• Birth Plan
• Lotion/oil for massages (unscented)
• Warm socks
• Lip balm
• Picture or small item for focal point
• Back massager
• Warm pack or rice sock
• Robe and slippers
• Nursing bra (if breastfeeding)
• Toothbrush/toothpaste/mouthwash
• Hair care items
• Cosmetics
• Loose fitting clothes to wear home, something from your 4th or 5th month of
pregnancy should be comfortable
For Partner:
• Insurance information
• Snacks for labor
• Swimsuit to wear in shower
• Watch with a second hand
• Change of clothes and toiletries
• Phone numbers of friends and relatives
• Change or phone card
• Books and magazines
• Videos, music tapes or CDs (Mercy’s Birthing Unit is equipped with CD players,
Flat Screen TV/DVD)
• Camera and film, camcorder and batteries
• Leave large amounts of money and valuables at home
53
For Baby:
• Newborn Communication Plan
• Undershirt and sleeper
• Going home outfit and receiving blanket
• Sweater, cap and extra blanket if needed for cold weather
• Infant car seat
• Baby book for footprints
Mercy will provide you with the following things for you and your baby during your stay.
For Mom:
Hospital gowns, disposable underpants and sanitary pads.
For Baby:
Diapers, wipes, thermometer, bulb syringe, soap and circumcision supplies for boys.
Undershirts and blankets are also provided during baby’s hospital stay.
Pre-Labor SignsYour body will undergo many changes during the last few weeks of pregnancy as it
prepares for labor. Pre-labor signs vary. You may experience some of the following
situations during your last weeks of pregnancy:
Braxton-Hicks
Braxton-Hicks contractions feel similar to labor contractions and may occur
throughout pregnancy. However, Braxton-Hicks contractions are usually irregular,
have no predictable pattern, and stop once you change activities. Braxton-Hicks
contractions can occur in late pregnancy and are termed false labor. If you
experience four or more contractions per hour prior to your 37th week of
pregnancy, it is important to notify your physician.
Bloody Show
During pregnancy, thick mucus fills the opening of the cervix. As the cervix begins
to change shape in preparation for labor, the mucus plug is released. The plug may
be tinged with blood, hence the term bloody show. The plug may be released days
or moments before actual labor begins. If the plug is heavily bloodstained, it is
important for you to contact your physician.
Backache
Backaches usually occur with the onset of labor. Try to relax by using cold or warm
packs, showering, or massage. You might also try position changes for relief.
la
bo
r
an
d
de
li
ve
ry

54
Nesting/Spurt of Energy
You may have an impulse to clean or rearrange your house.
Try not to over-exert yourself during this sudden burst of
energy. Instead, rest and prepare for labor.
LaborHow will I know when I am in labor?
Labor is probably the most anticipated stage of pregnancy.
Your due date is the approximate date you can expect to
deliver but it is not unusual to deliver anytime between 38
and 42 weeks from your last menstrual period. Remember
to trust in yourself and your body’s capabilities. This is an
important part of the labor and birth process.
Two Distinct Signs Laborhas Begun1. Your Water Breaks
A rapid gush or trickle of water from the vagina occurs
when the sac of water containing amniotic fluid, which
surrounds the baby during pregnancy, breaks and the
fluid leaks out. When this happens, you won’t feel any
pain, but just a trickle or flow of warm water. Keep in
mind that this is a normal healthy part of labor and
doesn’t harm your baby.
Normal amniotic fluid is clear in color. Be sure to note
any variation in color. Contractions may occur before or
following your water breaking.
It is necessary to call your doctor as soon as your water
breaks, whether or not you have experienced any
contractions.
2. Regular Contractions
Contractions can range in feeling and intensity and they
are usually felt in your lower abdomen or back. They
occur because your uterus is tightening and relaxing to
help open the cervix and push your baby out through the
birth canal. Some women describe them as being similar
When should you goto Mercy?• If your water breaks
• If your contractions are 5 to 7
minutes apart (or as directed by
your physician/midwife)

to menstrual cramps that usually increase in length, strength and frequency as labor
progresses. Some women report contractions as feeling similar to a severe low
backache that also may begin to increase in length, strength and duration. In the
beginning stages of labor, contractions usually occur five to 20 minutes apart and
last about 30 to 45 seconds. Contractions that occur frequently (five minutes apart
or closer) are a sign to call your physician.
Contractions How are contractions timed?
When your physician asks how far apart your contractions are he/she is asking for
the frequency of the contraction. To determine this, you need to time from the start
of the contraction to the beginning of the next contraction. When your uterus
begins getting hard, this is the start of a contraction.
In early labor you may want to keep track of the length of the contraction. This is
timed from when the uterus begins to tighten until it begins to relax.
When you call your doctor, be prepared to answer the following questions:
• How far apart are your contractions ?
• How long are your contractions are lasting?
• Did your water break?
Arriving at MercyWhen you arrive at Mercy, please plan to enter through the East Tower main entrance
located on the east edge of Mercy’s main campus (parking is located directly across
from East Tower entrance). If you arrive during the daytime, please proceed directly
to the third floor (labor and delivery). Wheelchairs are available in the main lobby if
you need assistance. If you arrive between the hours of 9 p.m.-6 a.m., the East Tower
55
6 p
.m.
contraction contraction60 secondsduration
4 minutesinterval
5 minutes apartfrequency
6:0
1 p
.m.
6:0
5 p
.m.
la
bo
r
an
d
de
li
ve
ry

56
courtesy desk will call the labor and delivery floor to notify them that you are coming
or to request that a nurse come to assist you. Once you are in your room, a nurse will
discuss your symptoms and do a vaginal exam to determine cervical dilation and rup-
ture of membranes. This exam also assesses the status of your cervix and position of
your baby’s head. The nurse will also monitor your baby’s heart rate.
Your nurse will go over your prenatal history and discuss your Birth Plan. This is a
good time to discuss any specific labor requests with your nurse.
MANAGING LABORThink about what helps you relax now…do you listen to music, take a bath or
shower, get a massage, talk with a friend, do controlled breathing or go for a walk?
Many of these same techniques will work for you during labor.
Most women are apprehensive about the potential pain of labor and delivery. The
amount of pain each mother experiences is quite different from one woman to the
next, and can be influenced greatly by their preparation for this process. Attending
childbirth education classes are helpful in educating yourself about the birthing
experience. All of the pain options mentioned in this section are taught in your
childbirth education classes.
At Mercy, our staff will provide you with many options to help you minimize
pain during labor. We will do our best to accommodate you with pain-relieving
techniques of your choice. Remember, the safety of mother and baby is always the
first consideration. Our goal is to keep you as comfortable as possible, while
minimizing the risks to you and your baby.
Pain Management Options for Labor• Breathing techniques
• Touch or massage
• Relaxation
• Music
• Position changes
• Encouragement from support person
• Medications
• Aromatherapy
• Water therapy with whirlpool tubs

57
Breathing TechniquesThe way you breathe is closely linked to your ability to relax.
Regular rhythmic breathing can help by providing increased
oxygen for you and your baby and it will help distract
attention from labor contractions.
There are three basic patterns of breathing used during labor:
slow chest, joggers and pant/blow. These breathing patterns
are used during contractions to assist in relaxation and to
ensure adequate oxygen for both mom and baby.
Cleansing BreathsYou should start each contraction with two deep cleansing
breaths. This is done by inhaling through your nose and
exhaling through your mouth. If nasal congestion is a
problem, use all mouth breathing. A cleansing breath is like
a big sigh. It is a signal to your partner that a contraction is
beginning or ending and it is your cue to relax.
At the end of each contraction, take one deep cleansing
breath as a signal the contraction has ended and to give
yourself another charge of oxygen.
Slow Chest BreathingYou should start this breathing pattern when you feel you
need it to help you through a contraction and you should use
it as long as possible.
After you have taken your cleansing breath, start by breathing
slowly in through your nose and out through your mouth at
about 6 to 10 breaths a minute. This breathing is a mid-chest
breathing so you do not want to breathe too shallow or too
deeply. At the end of the contraction, take one deep cleansing
breath.
This is a good time for you to start practicing your other pain
management techniques.
10 Ways for yourlabor partner to say“very good”• You’ve got it!
• That’s good!
• Good work!
• I knew you could do it!
• You make it look easy.
• Wow – nice going!
• Nothing can stop you now.
• You’re doing beautifully!
• I’m very proud of you.
• Way to go!
la
bo
r
an
d
de
li
ve
ry

58
Jogger’s BreathingUse this pattern when you feel you need more help concentrating during a harder
contraction and slow chest is no longer working effectively.
Start this breathing pattern by taking two deep cleansing breaths. Joggers breathing
is two breaths in through your nose and two out through your mouth, as slow or as
fast as you require to stay comfortable. Then at the end of the contraction, take
one deep cleansing breath.
Pant and Blow BreathingThis pattern is a combination of the slow chest and joggers breathing patterns and it
can be used at two different times during labor.
Typically the first time a laboring woman may use this is during a premature urge to
push. This is when you are not totally dilated, but because the baby is so low, you get
the urge to push. Using this pattern will stop you from pushing.
The second instance when you might use this is when you are pushing and the
baby’s head is being born. This breathing keeps you from bearing down and allows
the uterus to slowly push out the baby’s head, causing the pressure change to occur
gradually and giving your provider time to clear the baby’s airway. This breathing
pattern also helps you by giving your perineum time to stretch, avoiding a larger
episiotomy or tear. Both of these breathing patterns are quick and light.
Relaxation Each woman learns to relax in her own way. Practice will help you find the most
effective methods for you. Relaxation is the art of releasing muscle tension, which is
the foundation of comfort during labor. Relaxation will help you become calm,
conserve energy, reduce fatigue and reduce pain.
Massage and Touch
Massage and touch can help you become more comfortable during pregnancy as
well as during labor. Massage works by distracting or disrupting your focus on the
discomfort of the contraction.
Labor Positions
Changing positions frequently helps relieve pain and may speed up labor by adding
the benefits of gravity and changes in the shape of the pelvis. You will learn a vari-
ety of positions in prenatal classes.

59
Using Medications in LaborSome women choose to use medicine to help control pain, nausea and vomiting
during labor. Choices of drugs and methods of administration depend on the
situation and when relief is needed.
The discomfort of labor originates from three sources:
• Uterus contracting
• Cervix dilating
• The lower birth canal stretching
AnalgesicsAnalgesics are pain medications used to take the edge off labor pain. These
medications rarely remove the pain of labor completely, especially at the peak of a
contraction. They do however, make the pain more tolerable and will allow you to
rest more comfortably between contractions.
Side effects of analgesics may include nausea, vomiting, dizziness and drowsiness.
Analgesics may also affect the strength and frequency of your contractions. These
medications are usually used during the earlier phases of labor because they can affect
your baby’s breathing and reflexes if given too close to the time of birth.
EpiduralEpidural anesthesia can provide pain relief for both labor and delivery. To
administer this method the mother sits or is curled-up on her side, and a catheter (a
tiny tube) is placed in her lower back.
The epidural produces numbness of the lower abdomen, legs and birth canal.
Generally administered after labor has been established, the epidural will provide
considerable pain relief for the remainder of labor and delivery.
Side Effects
As with all anesthetics, there are certain side effects and complications associated
with the epidural and spinal anesthesia. These include:
ACCIDENTAL SPINAL BLOCK – If the membrane that confines the fluid
surrounding the spinal cord is punctured with the needle or catheter, an extensive level
of anesthesia may occur. This could cause some temporary difficulty in breathing,
which could require medical attention. It could also cause a headache.
la
bo
r
an
d
de
li
ve
ry

60
INEFFECTIVE PAIN RELIEF – The extent of pain relief
varies. Nearly 85 percent get total pain relief, while the
remaining 15 percent experience partial relief. Occasionally,
there is no relief at all.
HEADACHE – This can result from an accidental tear in the
covering which contains the spinal fluid. The headache is usually
present when you are upright and diminishes when lying down.
The discomfort can often be relieved in a few days by taking
analgesics, lying flat and drinking more fluids. In some severe
cases, a “blood patch” is used to repair the defect. This is
accomplished by injecting a small amount of your own blood
into the same area of the lower back where the epidural or spinal
block was performed.
EFFECT ON LABOR – An epidural may slow down labor,
especially if given too early prior to when true labor begins. It
also may reduce your ability to push during the second stage
of labor and forceps may be required to deliver the baby’s
head.
BLOOD PRESSURE PROBLEMS – A drop in blood pressure
is potentially one of the most common problems encountered.
Your blood pressure will be monitored after placement of the
epidural to detect and treat this problem. To further minimize
the risk, you will receive fluids continuously through an IV
placed in your arm prior to the use of the epidural.
CENTRAL NERVOUS SYSTEM – Light headedness, ringing
in the ears, speech problems, visual symptoms, numbness of
the tongue, loss of consciousness or seizures may follow the
accidental injection of the anesthetic agent into the vein. This
toxic reaction is reduced by using a small “test dose” of
medicine prior to the larger dose required to produce the pain
relief.
BLADDER PROBLEMS – Sensation to the bladder will likely
be dulled, and you may be unable to empty your bladder for
the few hours following delivery. Occasionally, a catheter
must be placed into the bladder to allow it to drain and
empty.
Certain diseases or problems may not allowyou to have an epidural orspinal anesthesia.Conditions which mayindicate this are:
• Significant bleeding problems
• Blood clotting problems
• Infection near the site of
puncture
• Progressive nerve neurological
disorders
• Extensive low-back surgery
• Significant blood pressure
problems
If you have, or suspect youhave, any of the above con-ditions you should reportthem to your physician.

61
MUSCLE SHAKES – Shivering is common with this anesthetic, especially
following delivery. This is usually temporary and requires no special treatment.
INFECTION – This side effect is extremely rare because of the sterile products and
techniques used.
PARALYSIS AND NERVE INJURY – Paralysis and lesser types of nerve injury after
an epidural are extremely rare.
SAFETY – Although the list of complications is quite long and may be frightening
to some, epidural and spinal anesthesia is quite safe. It has become the anesthetic
technique of choice in many centers for women who require considerable pain relief
during labor and delivery.
Spinal BlocksSpinal blocks may be used to help control the pain of labor and delivery. The
anesthetic is injected into the lower back in a single dose through a needle. This is
sometimes combined with the epidural. This produces numbness in the legs and
birth canal. Spinal anesthetics are popular for cesarean deliveries because they
produce a profound and predictable area of numbness.
Pudendal BlockThe pudendal nerve is the source of sensation to the lower portion of the vagina
and rectum. When this nerve is blocked, it creates numbness in the lower birth
canal and perineum. It is a useful technique at birth, just as the baby’s head appears
at the vaginal opening, but it has no effect on the pain from uterine contractions.
This is used in conjunction with prepared childbirth to ease the discomfort in the
vaginal opening upon delivery.
LocalThis anesthetic technique numbs only the area in which it is injected and it is often
used in episiotomies and perineal tears.
GeneralGeneral anesthesia is mostly used for cesarean section births and emergencies. It
requires specialized equipment and personnel trained to administer the medications.
General anesthesia is a needed technique in certain situations for cesarean section
births, but is rarely used for uncomplicated vaginal births.
la
bo
r
an
d
de
li
ve
ry
62
LaborWhat Should I Expect?
The process of labor and delivery is different for every mother. Each experience will
have its own pace and rhythm. Labor consists of four phases. It is important to
learn about each phase of labor, as it will help you understand the childbirth
process.
Phases of Labor
• Labor
• Birth of the baby
• Delivery of the placenta
• Bonding/Recovery
Early LaborDuring early labor, usually the longest stage of labor, women often experience
contractions that tend to last less than a minute, with five or more minutes between
contractions. These contractions serve to thin and begin the process of opening the
cervix for the delivery of the baby. Early labor dilation is between zero to three
centimeters. Dilation refers to the amount your cervix has opened. It is measured
in centimeters, from zero centimeters (no dilation) to 10 centimeters (complete
dilation). Most women maintain normal activities during this phase of labor. Rest is
important during this stage, as labor may take hours to get well established. You are
encouraged to time your contractions to track their pattern. Most physicians
encourage first time mothers to go to the hospital when their
contractions have been five minutes apart for one hour.
Active LaborDuring this phase contractions will grow progressively
stronger and longer, lasting up to 60 seconds or more, and
coming every two to five minutes. The cervix dilates from
four to seven centimeters. At this time, you may choose to
begin pain management techniques.
Transition LaborUsually this phase of labor is the shortest as well as the hardest. Contractions are
intense; lasting 60 to 90 seconds and occurring as close as every two to three
minutes. Dilation is between eight to 10 centimeters.

63
BirthDuring this time, the urge to push or bear down commonly increases as the baby’s
head moves down the birth canal (vagina) and creates pressure on the pelvic floor.
Pushing efforts are most effective if you follow your natural urge to push, and relax
when the urge to push subsides.
Your health care professionals will direct you if a specific pushing position or tech-
nique is necessary. Be sure to stop pushing when you are instructed.
Moments after your baby is born your labor partner will have the opportunity to cut
the umbilical cord. If your newborn is stable, she will be wrapped in a blanket and
laid on your chest. After bonding, the nurse will weigh your baby and get her
footprints for the birth certificate and baby book.
Delivery of the placentaAfter the baby is born, it typically takes only a few contractions for the
placenta to separate from the uterine wall and be delivered.
After the placenta is delivered, mild contractions usually continue as the uterus uses
these contractions to start to shrink back to its pre-pregnancy size. You may be
aware of these contractions, which typically feel like menstrual cramps, over the
course of the first few days after the birth.
Bonding/RecoveryAt this time your health care professional will stitch the episiotomy or any tears that
may need repairing after the birth. The first hour or so after the baby is born, your
nurse will massage your uterus to help your body begin the process of returning to
the pre-pregnancy state.
During this time, your baby will be in a special state of alertness. Use this time to
bond with your baby by touching, talking and interacting. This is also the time to
begin breast or bottle-feeding your new baby.
Cesarean Birth When a vaginal birth is not possible, or poses risks for the mother or baby, your
baby is born by cesarean, or c-section as it is more commonly known. Once a
decision is made, preparation for the surgery usually occurs quickly. Most often, an
epidural or spinal anesthesia is used, allowing the mother to be awake during the
birth. In almost all cases, the labor partner may be present during the surgery.
la
bo
r
an
d
de
li
ve
ry

64
The process requires an incision in the mother’s lower abdomen, through which the
baby is born. A c-section takes approximately 45 minutes after the incision is made.
Often the baby can be seen and touched by the mother immediately after the nurses
check the baby’s health and wrap her in a blanket. Breast or bottle-feeding can begin
after the mother and baby are both stable.
Pain relievers are given after a c-section to improve comfort for the mother. Your
nurse will provide you with information on how to care for the incision, get out of
bed more easily and hold the baby for feeding.
It is important to ask your health care provider what type of incision was made on
your uterus, and how this might affect future births. A uterine incision is vertical
(classical) as opposed to horizontal (low transverse). Remember - the skin incision
isn’t always the same as the uterine incision!
Some conditions which may indicate a Cesarean BirthPLACENTA PREVIA – The placenta blocks the cervical opening.
ABRUPTIO PLACENTA – The placenta prematurely separates from the uterine wall
and interrupts the vital flow of oxygen and nourishment to the baby.
PROLAPSED CORD – A pinched umbilical cord jeopardizes the infant’s blood and
oxygen supply.
ACTIVE MATERNAL HERPES – A vaginal birth exposes the infant to this
potentially lethal infection.
BREECH PRESENTATION – Baby descends feet-first or buttocks-first through the
birth canal and is susceptible to serious injury.
CEPHALOPELVIC DISPROPORTION (CPD) – Infant is too large to pass
unharmed through the mother’s pelvis.
FETAL DISTRESS – Baby has difficulty tolerating labor and her heart rate suddenly
drops or slows.
C-section AnesthesiaSeveral of the previously described anesthesia methods are also effective for
c-section. General, spinal and epidural anesthesia comprise the majority of the
techniques. General anesthesia is most frequently used for certain emergencies
where time becomes critical in delivery of the infant. Many times, the choice
between spinal or epidural for the relief of pain or associated complications, will
not be different to you as a patient. If you had an effective epidural during your
labor, more than likely this technique would be used for your c-section.

65
Many factors are considered in making a selection of the most appropriate
anesthetic for you for your operation. The factors relate to you, your baby and the
technical skill of the trained person administering your anesthetic.
Your choice in this matter will be a valued consideration, but other medical
considerations can override your choice at times.
Remember: A cesarean delivery is a birth! Either way, your birth can be a beautiful
experience. Both vaginal birth and cesarean birth give you what matters most: a
healthy baby in your arms.
Vaginal Birth After Cesarean (VBAC)Vaginal Birth After Cesarean–or VBAC–is giving birth vaginally after having one or
more cesarean sections, or c-sections. The number of women who choose to have a
VBAC is increasing and approximately 70 percent of women who attempt VBAC are
able to deliver vaginally.
One reason to plan for a VBAC is to avoid the surgical risks of a c-section. Cesareans
are generally safe; however, vaginal births have fewer risks and the recovery time is
typically shorter.
Talk to your healthcare provided to see if you can have a vaginal delivery. Today,
most doctors perform low transverse c-sections. VBAC is usually safe after this type
of c-section. Remember that although many women may be candidates for VBAC,
there is a chance that you may need to have a repeat c-section.
Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
la
bo
r
an
d
de
li
ve
ry

Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
66

Y O U R S TAY AT M E R C Y
Infant Secur ity • 69
Visitat ion Pol icy • 69
Newborn Test ing • 70
Addit ional Resources • 71
67

69
We want your stay to be pleasant and comfortable. One nurse will be caring for
both you and your baby during each shift of your hospital stay. Your care will be
personalized for you and your family.
We encourage you to keep your baby with you in your room so you may begin to
bond with each other. This also provides you with the opportunity to practice baby
care with assistance from your nurse. The father or support person is also encour-
aged to get involved in the educational process and the newborn care. Your nurse is
a valuable resource for all of your questions. Take advantage of this opportunity to
enjoy and learn about your new baby.
Infant SecurityThe Mother/Baby Unit staff provides a safe environment for you and your baby. You
will find comfort in knowing that Mercy has a state-of-the-art security system in place
to keep your newborn safe while in the hospital.
The following suggestions will help ensure the safety of your infant during your stay:
• Allow only appropriate staff members to take your baby from your room after you
have checked for their proper identification.
• Never leave your baby alone or unsupervised in your room.
• Always transport your baby in the crib.
• Place your baby’s crib out of direct view of the door.
• Always verify your ID bracelet with the baby’s bracelet after you have been
separated.
• If you are unsure about anyone who comes into your room or asks about your
baby, please call your nurse.
Visitation PolicyIn an effort to support you and your family, and to minimize the risk of infection to
the new baby, Mercy Medical Center suggests the following recommendations
regarding the visit of siblings, grandparents, and others.
• Visiting hours are 7 a.m. to 9 p.m.
• The American Academy of Pediatrics recommends visitors be at least 14 years old,
or a sibling of the newborn, however we support your choice of visitors.
• Visitors should not have been exposed to any contagious diseases in the past two
weeks and must wash their hands well before touching your infant.
Mercy understands your family and friends are very important to you and we will support you in
your choice for visitors.
yo
ur
s
ta
y
at
M
er
cy
Your Stay At Mercy

70
Important phone numbers• Newborn Nursery ..............................................................................................(515) 358-2050
• Lactation Consultants ........................................................................................(515) 358-2082
• Little Miracles Boutique ....................................................................................(515) 358-2080
• Variety Club Neonatal Intensive Care Unit ......................................................(515) 358-4000
Newborn Metabolic ScreeningTo help assure that your baby will be as healthy as possible, a simple blood test is
done before your newborn is discharged. The Newborn Metabolic Screening
program identifies the few infants who may have one of several uncommon birth
defects screened for in this program. With early diagnosis and medical treatment,
complications from these serious conditions, such as mental retardation or even
death, can usually be prevented. Your baby’s pediatrician will be notified of the test
results. More detailed information will be available from your nurse.
Newborn Hearing ScreenBabies must be able to hear in order to learn to speak. This process starts long
before your infant makes their first sound. We know that the critical period for
learning speech and language is from birth to three years old. This is why it is
important to identify hearing impairment and begin treatment as early as
possible. Children with hearing impairment can lead happy and normal lives if
we know about the impairment early. All newborns at Mercy are given an initial
hearing test to determine if further follow up is needed. These tests will not
determine if your newborn is hearing impaired, but will indicate that further
testing should be done when the baby is a few weeks older.
Baby PhotosDuring your hospital stay, a representative from the Mercy Auxiliary will visit
with you about taking your baby’s first photograph. Mercy also offers a website
for you to post your newborn’s first photo so you may share your new addition
with family and friends.
Birth Certificate from the StateThe 1993 session of the Iowa General Assembly passed a law that requires parents of
all newborn children to be charged a $35 fee. This fee covers an automatic birth cer-
tificate to be filed in your county. You will receive a wallet-sized birth certificate
from the Department of Public Health. The law requires Mercy Medical Center to
collect this fee. The automatic birth certificate will show as an itemized charge on

71
the statement you receive following your discharge from
Mercy. Your insurance carrier does not reimburse
the fee; it is an obligation that is left to the new
parents. The fee is waived for those whose
expenses are paid by the state’s medical assis-
tance program (Title XIX) and those consid-
ered to be indigent.
If you have any questions regarding the collec-
tion of this fee, please ask your nurse. You may
also call the Iowa State Department of Health at
(515) 281-4944.
Application for a Social Security Number for BabyYou are able to apply for a social security number for your baby by circling “yes” on
the birth certificate worksheet. The social security card will be mailed to your home
in approximately 90 days.
Additional Resources During Your Stay:LACTATION CONSULTANT SERVICES – Certified lactation nurses are available
for additional breastfeeding assistance and education. Your nurse can coordinate a
visit for you or you may call them directly at (515) 358-2082.
LITTLE MIRACLES LACTATION BOUTIQUE – The Little Miracles Lactation
Boutique offers a wide variety of lactation supplies for purchase and/or rental. The
boutique is located on the second floor of Mercy’s East Tower. For more informa-
tion, please call (515) 358-2080 or visit www.mercydesmoines.org.
SOCIAL SERVICES – A maternal health social worker is available to help with any
concerns you may have. Your nurse can coordinate a visit or you may call (515)
247-4339.
PASTORAL CARE – Chaplains are available to visit with you at any time. Your
nurse can coordinate a visit or you may call (515) 247-3238.
FOOD SERVICES – The Marketplace & Grille, located on A-level, is open from 6:15
a.m. to 7 p.m. Room Service is available to patients from 6:30 a.m. to 6:30 p.m.
daily by calling 4-4444. Patients will receive a menu upon admission.
FAMILY VIOLENCE CENTER – Violence and abuse towards women is on the rise.
If you need someone safe to talk to, contact the Family Violence Center at
(515) 243-6147. Your nurse or the maternal child social worker can assist you with
additional resource information.
yo
ur
s
ta
y
at
M
er
cy

72
Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________

Y O U R C A R E AT H O M E
Nutr it ion • 75
Breast Care • 77
Incis ion Care • 78
“Baby Blues” • 80
Exercise • 81
73


75
You will experience physical and emotional adjustments during the postpartum
period (first six weeks following childbirth). The following instructions will assist you
after leaving the hospital.
Activity/Rest• Rest frequently, especially when the baby is sleeping.
• Avoid lifting objects that weigh more than the baby for the first two weeks.
• Allow others to help with housework. Avoid vacuuming.
• Stair climbing may be unavoidable, but try not to overdo.
• Driving a car can be resumed after you have regained your strength and can
comfortably press on the brake.
If you delivered your baby by Cesarean section, you need to remember that you have
had abdominal surgery. You may find moving, lifting and walking uncomfortable at
first. Pay attention to comfort and avoid getting overly tired. You will find it
necessary to avoid strenuous activity when you go home. During the first weeks,
slowly progress toward resuming normal activities. Short periods of walking
followed by rest are ideal.
NutritionA well-balanced diet is essential for healing and to restore your energy. A healthy
diet consists of foods from the five food groups, which include dairy products, meat,
grains, fruits and vegetables. Fluid intake should be approximately six to eight
glasses of liquid per day. Continue to take your prenatal vitamins.
Mother’s Diet while BreastfeedingMost breastfeeding mothers are able to eat anything they want without problems.
However, there are some babies whose digestive systems are not fully mature.
Spicy and gassy foods like onions, cabbage, broccoli or beans might make your
baby fussy.
Try eating different foods, one at a time, to see how your baby reacts to them. If
something really makes your baby fussy and uncomfortable, don’t eat it for a
couple of weeks. As baby’s digestive system matures, she can handle much more.
• Eat a good healthy diet just like you did during your pregnancy and use the food
pyramid for a guide. Learn to read labels and don’t eat foods with a lot of added
chemicals.
yo
ur
c
ar
e
at
h
om
e
Your Care at Home

76
• Eat about 500 more calories every day in the form of nutritious foods. Drink
plenty of liquids to keep your thirst satisfied and your urine a very light yellow
color.
• You will gradually lose the weight you gained during pregnancy and breastfeeding
usually helps. There will be an initial weight loss of about 15 pounds in the first
few weeks after delivery. After the initial loss, you can maintain that weight or
safely lose one to two pounds a week until you reach your desired weight. Losing
more than two pounds a week could reduce the quantity of milk you produce.
• Make sure you get 1,200 mg. of calcium per day. This equals four servings of
dairy products. One glass of milk, a cup of yogurt and a one-inch cube of cheese,
for example, are each equal to one serving.
• Very little of the caffeine that you drink goes through to the breast milk, but limit-
ing your intake is a good idea. Some babies become restless and fussy from too
much caffeine.
• Alcohol is not good for babies and should be avoided. Alcohol can inhibit the let-
down reflex, and will be present in breast milk at the same concentration as in
mother’s blood stream. Researchers have found that when a mother consumes
even one alcoholic drink, her baby nurses less vigorously and consumes less milk
during a feeding.

77
• Generally, most medications cross into the breast milk, but most do not pose a
problem to your baby. Some medications may be harmful to your baby, so it’s
always better to remind your doctor that you are breastfeeding when he/she
prescribes medications. Mercy’s lactation consultants also serve as a good source
of information as well as your pharmacist.
Breast CareEngorgement is frequently a problem for non-nursing mothers. Wearing a support-
ive bra 24-hours a day, for at least three to four days or until your breasts feel soft,
can help with engorgement. Other helpful hints to alleviate engorgement are:
• Avoid nipple or breast stimulation.
• Place cool compresses or ice packs on your breasts for comfort.
• Avoid heat – even an electric blanket could increase milk production.
• Green cabbage leaves can also be helpful to hasten natural drying up of your
breast milk (Refer to the section on green cabbage under Infant Feeding – page
111.
Self Breast ExamA breast self-exam could save your breast – and your life. The best time to do the
self-exam is right after your period, when breasts are not tender or swollen. If you
do not have regular periods or sometimes skip a month, do it on the same day every
month.
How to do a breast self-exam
1. Lie down and put a pillow under your right shoulder. Place your right arm
behind your head.
2. Use the finger pads of your three middle fingers on your left hand to feel for
lumps or thickening in your right breast. Your
finger pads are on the top third of each fin-
ger.
3. Press firmly enough to know how your
breast feels. If you are unsure how
hard to press, ask your health care
provider. If still uncertain, try to copy
the way your health care provider uses
the finger pads during a breast exam.
Learn what your breast feels like most of the
time. A firm ridge in the lower curve of each
breast is normal.
4. Move around the breast in a set way. You can choose either the circle, the up
yo
ur
c
ar
e
at
h
om
e

78
and down, or the wedge. Do it the same way every time. It will help you make
sure you have gone over the entire breast area.
5. Now examine your left breast using your right hand finger pads.
6. Repeat the examination of both breasts while standing, with one arm behind
your head. The upright position makes it easier to check the upper and outer
part of the breasts (toward your armpit). You may want to do the standing part
of the exam while you are in the shower. Some breast changes can be felt more
easily when your skin is wet and soapy.
If you find any changes, see your doctor right away.
Cesarean Incision CareWash your abdominal incision with soap while
showering. Avoid tub baths until approved by
your physician. Inspect your incision for any signs
of infection, such as redness, swelling, gapping or
drainage. Notify your doctor if any of these occur.
It is not necessary to have a dressing over the inci-
sion. Steri-strips are applied after the skin
staples are removed to aid in keeping the skin edges together during the final healing.
Remove the steri-strips in about seven to 10 days, or when they begin to peel off. Take
pain medication as directed by your physician.
Vaginal flow/CrampingVaginal flow is normal for up to six weeks after delivery. At first, the flow will be
bright red; in a few days it becomes pink, then yellowish and finally a creamy white
discharge. It is important to change your pad frequently.
It may be two to four months before your normal menstrual period returns. The
first few periods may be heavier than normal. Since ovulation may occur even
though you have not reestablished your menstrual cycle, it is possible to become
pregnant. It is advisable to consult your physician in regard to family planning
before you have intercourse.
You may feel some cramping, particularly if this isn’t your first baby. The cramping is
caused by contractions which return the uterus to normal size and prevent excessive
bleeding. Cramping often occurs while the infant is nursing. Acetaminophen /
Ibuprofen products can be helpful for eliminating discomfort. Your uterus will return
to its normal size in five to six weeks.

79
Reasons to call your physicianContact your physician as soon as possible if you are experiencing any of the
following symptoms:
• Flu-like symptoms
• Temperature higher than 100.4 degrees fahrenheit for more than 24-hours
• Post-postpartum blues severe enough to interfere with taking care of yourself or
your baby
• Hot, tender area on your breast or in the armpit
• Pain in your chest and/or lower legs
• Persistent pain or foul-smelling discharge from your episiotomy, C-section
incision or uterus
• Bleeding more than twice the usual menstrual flow and/or blood clots greater than
the size of a golf ball
• Painful urination; foul-smelling urine
Perineal / Hemorrhoidal CareThe perineal area requires good personal hygiene to prevent infection. Follow these
simple guidelines:
• Clean and wipe from front to back after urinating or having a bowel movement
• Change your peri pad frequently, at least every three to four hours
• Sit in a tub of clean warm water for 20 minutes several times each day
• Do not use douches, feminine hygiene sprays or tampons
• You should be able to resume sexual activity in six weeks, or as directed by your
physician
• Continue to use witch hazel pads and sprays as needed for comfort
If hemorrhoids are present, witch hazel pads and hemorrhoidal cream are helpful.
Use your rubber ring or a pillow to make sitting more comfortable.
EliminationConstipation is common during the first days after delivery. To avoid this problem, it
is helpful to eat foods rich in fiber as well as drinking six to eight glasses of fluid.
Foods high in fiber are fruits, vegetables, bran and whole-grain breads and cereals.
Prune juice may also be helpful. If needed, a mild laxative or stool softener may be
used. Call your physician if constipation persists.
Try to urinate every two to four hours. Discomfort before, during or after urination
as well as urine that is cloudy, dark or foul smelling should be reported to your
physician. Drinking more liquids than the suggested daily amount may also help
alleviate the problem.
yo
ur
c
ar
e
at
h
om
e

80
“Baby Blues”Your body will be going through some major hormone changes during the next few
weeks. Along with these changes, many women experience some
degree of mood fluctuations known as “baby blues.” You
may feel thrilled and happy at one moment and a little
depressed the next moment. “Baby blues” are normal
and usually occur from the second day up to four weeks.
Hormonal changes, fatigue, isolation, new and unre-
lieved responsibilities are usually the cause.
Ways to ease the “blues”:
• Get adequate rest. An exhausted mother may have problems with milk
production or the adjustment to motherhood. If possible, plan to have a
relative or friend assist you for the first week so you can sleep when the baby
sleeps. Also, limiting your visitors until you are less tired will help.
• Don’t expect too much from yourself. Until you get used to motherhood and
your baby… be patient.
• Talk with your partner about the mood fluctuations. He is probably getting
concerned and the talk will relieve his fears and gain his support.
Postpartum DepressionThe “baby blues” should not be confused with postpartum depression, which may
occur after eight weeks. Feelings of anxiety, inadequacy, insomnia and lack of
appetite are a few signs of postpartum depression. Postpartum depression requires
professional attention. If you find that you are not able to take care of yourself or
your baby, or if you find that you cannot function normally, then you need to
contact your physician for assistance. Help also is available from the professionals at
the Mercy Franklin Center at (515) 271-6111.
Follow-up ExamYour physician will instruct you when to make your follow-up exam; usually four to
six weeks after delivery. Call your physician’s office to make this appointment after
you go home from the hospital.

ExerciseThe following are examples of abdominal toning exercises that can be started once
your physician gives you permission.
ABDOMINAL BREATHING Lie on your back with your knees bent. Inhale deeply
through the nose. Keep ribs as stationary as possible and allow abdomen to expand
upwards. Exhale slowly but forcefully while contracting the abdominal muscles;
hold for three to five seconds while exhaling.
REACH FOR THE KNEES Lie on your back with your knees bent. While inhaling,
deeply lower chin onto chest. While exhaling, raise head and shoulders slowly and
smoothly and reach for knees with arms outstretched. The body should rise only as
far as the back will naturally bend while waist remains on floor or bed (about six to
eight inches). Slowly and smoothly lower head and shoulders back to starting
position. Relax.
81
yo
ur
c
ar
e
at
h
om
e

82
DOUBLE KNEE ROLL Lie on your back with your knees bent. Keeping shoulders
flat and feet stationary, slowly and smoothly roll knees over to the left to touch floor
or bed. Maintaining a smooth motion, roll knees back over to the right until they
touch the floor or bed. Return to starting position and relax.
LEG ROLL Lie on your back with your legs straight. Keeping shoulders flat and
legs straight, slowly and smoothly lift leg and roll it over to touch the right side of
the floor or bed and return to starting position. Repeat, rolling right leg over to
touch the left side of the floor or bed. Relax.

83
COMBINED ABDOMINAL BREATHING AND SUPINE PELVIC TILT (PELVIC
ROCK) Lie on your back with your knees bent. While inhaling deeply, roll pelvis
back by flattening lower back on floor or bed. Exhale slowly but forcefully while
contracting abdominal muscles and tightening buttocks. Hold for three to five sec-
onds while exhaling. Relax.
BUTTOCKS LIFT Lie on your back with your arms at sides, knees bent and feet
flat. Slowly raise buttocks and arch back. Return slowly to starting position.
yo
ur
c
ar
e
at
h
om
e

84
SINGLE KNEE ROLL Lie on your back with your right leg straight and left leg bent
at the knee. Keeping shoulders flat, slowly and smoothly roll left knee over to the
right to touch floor or bed and then back to starting position. Reverse position of
legs. Roll right knee over to the left to touch floor or bed and return to starting
position. Relax.
ARM RAISES Lie on your back with arms extended at 90° angle from body. Raise
your arms so they are perpendicular and hands touch. Lower slowly.

85
Notes:________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
yo
ur
c
ar
e
at
h
om
e

86
Notes:________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________

C A R I N G F O R Y O U R N E W B A B Y
Taking Baby’s Temperature • 91
Skin and Bath Care • 92
Car Seat Safety • 96
Soothing a Fussy Baby • 99
SIDS Prevention • 100
Infant Feeding Guidel ines • 102
Breastfeeding Resources • 104
87


89
Caring for a new baby can be overwhelming at first. With a little time and
practice, most parents begin to feel confident in their ability to care for their
newborn. You will become familiar with your baby’s unique self; noisy grunts,
sneezes, hiccups, crying and stuffy breathing. You also will become familiar with
baby’s sleep, elimination patterns and feeding cues. We hope the following
information also will assist in your early parenting endeavors.
Newborn CharacteristicsIt is normal for babies to sneeze, yawn, hiccup, cough, cry and get fussy.
Newborns often sound as if they have a stuffy nose. This is considered normal
unless it is significant enough to interfere with your baby’s feedings. In this case
notify your baby’s physician.
Infants also have fussy periods which can be very trying for new parents. You will
learn calming techniques that work for your baby. You should feel comfortable
asking for assistance or relief during these periods. Babies like rhythm, motion
and motor type sounds. Rocking, strolling, baby swings, car rides and bathing
work well. Babies can see well up to about 12 inches and will focus on your face
when you cuddle them. Newborns also have a good sense of
hearing. It is important to talk and sing to your baby. Babies thrive on
close physical contact. You cannot spoil a baby with
tender loving care and attention.
Ca
ri
ng
f
or
y
ou
r
ne
w
ba
by
Caring for Your New Baby

90
Sleep-Wake CycleTypically, babies sleep up to 20 hours a day. They can sleep through noise, so there
is no reason to tiptoe around. Sleeping routines may change as your newborn gets
older.
Six states of infant consciousness
• Quiet or deep sleep: your baby will shut out all input and is in the most
unaroused state.
• Active sleep: your infant may startle easily. Baby’s eyes will be closed but you
may notice their eyelids flutter.
• Drowsiness: your newborn is in an intermediate state that occurs while waking
up or falling asleep.
• Quiet alert state: this is the best opportunity for you and your baby to begin
building a relationship with each other. Your infant will look directly into your
eyes and will respond to your voice and facial expressions. This is the time your
baby makes her first attempt to interact with you. This is a perfect time to talk,
sing or read to your newborn.
• Active alert state: your baby may move her arms and legs rhythmically to get your
attention. This state may appear when your infant is ready to eat or is fussy.
• Crying state: your baby will cry when hungry or uncomfortable. You will learn
to distinguish between different types of crying. Your baby may move out of the
crying state by picking her up and soothing her.
Reasons to call your baby’s physician
If your infant seems “different” than what you would normally expect, she may be
ill. Some signs might include:
• A yellowish discoloration (jaundice) of the skin or whites of eyes
• A change in appetite or poor feeding
• Lethargy (sluggishness)
• Increased irritability, excessive crying, or inability to be consoled
• Fever
• Repeated vomiting and/or diarrhea
• Pale skin
• Although rare, watch for signs of infection at umbilical cord. These signs may
include swelling, redness, drainage or foul odor.

91
Taking Baby’s TemperatureYou should check your baby’s temperature if you think she might be sick. Two
common ways to take a baby’s temperature are “axillary” (armpit) and “rectally” (in
the baby’s rectum or anus). Check with your baby’s physician to determine which
method they prefer. When reporting the temperature reading to the doctor, state the
number and method. Do not add or subtract degrees, but rather let the doctor
calculate it. An example might be “98.6 axillary.” Avoid taking baby’s temperature
after a bath, because it may not be accurate.
To take the temperature under the arm
Place the thermometer under the baby’s armpit.
Hold the baby’s arm over the thermometer
until you get a reading. The normal
temperature is 97.6 to 99 degrees.
Airway SuctioningThe infant normally is able to clear her own
airway by sneezing or snorting. If mucus or milk
interferes with the infant’s breathing to the extent that the
baby is unable to clear the airway, the bulb syringe can be used. The bulb syringe must
be used gently and with caution, and only when the infant is unable to clear her airway.
Overuse of the bulb syringe can cause irritation.
To use the bulb syringe, first press in on the bulb to deflate it. Place gently in the
sides of the mouth or at the base of the nostrils, which ever is necessary. Slowly
release pressure on the bulb to create suction. Cleanse the inside of the bulb with
warm soapy water after using and rinse well.
If you need to replace your bulb syringe, one may be purchased at Mercy’s Outpatient
Pharmacy or the Little Miracles Boutique.
yo
ur
c
ar
e
at
h
om
e

92
Infection ControlThe best way to cut down on the spread of viruses and infection is through good
hand washing with soap and water. Parents and visitors should wash their hands
before handling the baby. You can prevent some illnesses by not taking the baby
outside in severe weather, avoiding crowded areas and encouraging visitors with
colds or contagious illnesses to visit only after they recover.
Cold sores are caused by the herpes simplex virus and can be dangerous to new-
borns, possibly causing serious illness or death. Visitors with cold sores should not
handle your baby. If you have a cold sore, remember to wash your hands well before
touching your baby. Do not touch your cold sore or kiss your baby. You may want
to apply a dressing over the sore to further protect the infant.
Skin and Bath CareA bath is recommended for your newborn every two to three days. It is only necessary
to wash the baby’s face and bottom daily. You should give the bath in a warm area and
never leave your baby unattended during the bath. When giving baby a tub bath add
about two inches of warm water to baby’s bath. Use your wrist or elbow to check the
temperature. Swaddling the infant may make baby easier to handle, and may help calm
a fussy baby.
Before beginning the bath, collect the following items:
• wash cloth • clean clothes
• towels • basin with warm water
• mild soap and shampoo • hair or scalp brush
• clean diaper

93
Giving Baby a BathStart by washing the baby’s face first and diaper area last. Use a mild soap that does not
contain perfumes, dyes or deodorants. Oils, powders or lotions should not be used on
the baby’s skin unless otherwise recommended by the physician. If the infant has dry skin,
a mild lotion that does not contain additives may be used.
Wash the eyelids carefully, using a clean surface of the cloth for each eye. Do not use
soap. Wipe each eye from the inside corner to the outside. Then, wash the face with
a clean washcloth moistened with warm water. Clean the outer part of the ear with a
washcloth. Never insert anything hard, like a cotton swab, into the ear canal.
Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
yo
ur
c
ar
e
at
h
om
e

94
Wash the baby’s body, arms and legs with mild soap and water. Be sure to clean
between the fingers and in the creases of the skin at the neck and bends of arms and
legs. Pat dry. Wash from front to back between baby’s legs.
The shampoo may be done at the beginning or at the end of the bath. Hold the baby
in the “football” position over the sink. Use your finger and thumb to cover both ears.
Using a warm wash cloth or a cupped hand, wet the scalp. Use a mild shampoo to
lather the baby’s scalp. A soft brush may be used during the shampoo. Rinse all the
soap from the scalp and pat dry.
The baby’s scalp should be brushed daily to remove dry skin cells. When brushing
the baby’s hair, frequently brush it against the way it grows in order to cleanse and
stimulate the scalp.
Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________

95
Genital CareGirls
For infant girls, the diaper area should be washed from the front to the back in order to
prevent infection. It is normal to see clear or white discharge from the vaginal area.
Initially, there may be a slightly blood-tinged vaginal discharge. This is in response to
maternal hormones and is normal.
Boys
For baby boys, clean the circumcision by squeezing a wet wash cloth over the penis,
allowing water to dribble over the site. Gently wipe the groin and buttocks. There is no
special care needed for the uncircumcised penis. Do not pull back on the foreskin. Wash
genitals at bath time or when changing a diaper.
Cord Care
Your baby’s umbilical cord should fall off within three weeks. Prior to this time, the
following should be done to keep the cord dry:
• Fold diaper under the umbilical cord area to avoid soiling or irritating the cord.
• If the cord becomes soiled, use warm water to clean the area and pat dry.
It is normal to see a slight amount of bleeding as the cord is falling off.
Although rare, watch for signs of infection. These may include swelling, redness,
drainage or a foul odor. If any signs of infection are noticed, notify your infant’s
physician.
Nail CareHold your infant on your lap facing away from you. Grasp a hand firmly. Trim the
nails straight across, not to a sharp point. Use baby cuticle scissors or an infant
emery board. Watch for snags and sharp edges. Babies tend to tolerate the proce-
dure best during a feeding or while sleeping.
DiaperingYour baby’s diaper should be changed frequently. Urine and stool can irritate baby’s
sensitive skin. While the cord is still present, fold the front of the diaper down so the
cord can be exposed to the air.
If diaper rash develops, wash and rinse the diaper area well. Expose the diaper area
to air two to three times a day. A light coating of Desitin or A&D ointment on a
clean, dry bottom may also be applied. If the diaper rash does not improve with this
treatment within 24-hours, contact your baby’s physician.
yo
ur
c
ar
e
at
h
om
e

96
ClothingIn warm weather there is no need to overdress your infant. Infants usually need
many layers of clothing to stay warm, as do adults in the same environment.
Overdressing will make your baby hot and fussy. Your newborn will let you know if
she is cold by having bluish hands and feet. In this case, warm socks, blankets and
even a hat will help keep your baby warm.
Car Seat SafetyDo you have the instructions for the car seat?
• Follow them and keep them with the car seat. You will need them as your child
gets bigger.
• Be sure to send in the registration card that comes with the car seat. It will be
important, in the event your car seat is recalled.
Does your car have a passenger-side airbag?
• An infant in a rear-facing seat should NEVER be placed in the front seat of a vehi-
cle that has a passenger side airbag.
• It is essential for children 12 and younger to ride in the rear seat.
Is your child facing the right way for both weight and age?
• If you use a seat made only for infants (figure A), always face it backward.
• Infants should ride facing the back of the car until they are one year of age and
weigh 20 pounds. (figures A&B)
• All rear facing seats should be semi-reclined.
• A child weighing more than 20 pounds and one year of age faces forward.
Is the harness snug; does it stay on your infant’s
shoulders?
• The shoulder straps of the car seat go in
the lowest slots for infants riding back-
ward and should fit over the infant’s
shoulders.
• The retainer clip should be placed at
armpit level to keep harness straps on the
shoulders.
• Harness straps should not be twisted.
• Keep light-weight clothing on your child rather than heavy snowsuits. This will keep
the shoulder straps in the proper place. Cover your child and the seat with warm
blankets when going out.
A

97
Have you tried the car seat in your vehicle?
• Not all car seats fit all vehicles.
• When the car seat is installed, be sure it
does not move more than one inch at the
belt path.
• Be sure to read the section on car seats in
the owner’s manual for your car.
Has your child’s car seat been recalled?
• Call the Auto Safety Hotline at
1-800-424-9393 or go to www.nhtsa.gov for a list of recalled seats that need repair.
• Be sure to make any necessary repairs to your car seat immediately.
Hazards of Second Hand SmokeSecond hand smoke includes both exhaled smoke and smoke coming from a burning
cigarette. Tobacco smoke from cigarettes, cigars and pipes is composed of more than
3,800 different chemicals. Research indicates that second hand smoke has a harmful
effect on the respiratory health of children such as:
• Higher rates of lower respiratory illness during the first year of life
• Increased rates of ear infections
• Higher rates of Sudden Infant Death Syndrome (SIDS)
• Developing or worsening childhood asthma
• Increased chance of developing cancer as an adult
It is important to your child’s health not to expose them to second hand smoke by:
• Not allowing anyone to smoke in your home or car
• Using only non-smoking childcare providers
• Avoiding enclosed smoke filled environments
B
yo
ur
c
ar
e
at
h
om
e
Other Safety Guidelines• Never put your baby to bed with a bottle. This causes the risk of tooth
decay, ear infections and choking.
• Never leave your baby unattended on a raised surface.
• Use safety straps for items such as infant seats, high chairs and swings.
• An adult should always test the temperature of the bath water. Never leave your
infant alone in the bath, even for a few seconds.
• Never use a microwave to warm breast milk or formula.

98
SHAKEN BABY SYNDROMEBabies or small children who suffer injury or death from severe shaking or jerking are
victims of what is called Shaken Baby Syndrome. Sometimes a young child’s crying or
need for attention can be more than tired parents or caregivers can cope with. In frus-
tration, without knowing the dangers, they may shake a baby or small child to get
their attention or to make them stop crying.
Children under two can easily be injured from shaking because their weak neck
muscles aren’t strong enough to fully control their head movements. When a child
is shaken, the head whips back and forth, slamming the fragile brain tissue against
the hard skull, causing bruising, bleeding and swelling inside the brain. When the
shaking is combined with throwing the baby against the crib mattress or pillow,
even more force is applied to the brain and more damage can occur.
Most of the time, Shaken Baby Syndrome occurs because a parent or caretaker is
frustrated or angry with a child. Other times, children become victims when a par-
ent or caretaker, not realizing how seriously this behavior can harm, throws a small
child into the air vigorously, plays too roughly, or hits an infant too hard on the
back. Anyone who takes care of a baby or small child should be reminded to never
shake babies or small children.
It is not unusual for infants to cry a lot during the first few months of life. Using a
mental checklist, determine first if your baby is safe, fed, comfortable and clean. If
crying persists, the following comforting techniques may help:
• Remain calm, babies can sense when you are tense.
• Rock your baby or place them in an infant swing.
• Run a vacuum cleaner or turn on a household fan.
• Cuddle the child gently and play soft music. Very young infants can be carried
around in a “snugli” or other type of carrier that holds the infant close to the
body.
If these suggestions do not work, you do not think the baby is ill, and you cannot
take the crying and stress anymore, put the baby in a safe place, such as a crib.
Take a short break, and if possible, call someone to take care of the baby for a
while. There are organizations that can provide help to parents whose patience
has been strained by the burden of caring for an infant who cries continually, or
who might need more help with parenting and coping skills.

Calming Your Baby with the 5 “S’s”
The first “S”—SwaddlingA baby’s first reaction to swaddling is to struggle against it. Swaddling may not
instantly calm fussiness but it will restrain the tendency toward uncontrolled flailing
so that your baby can pay attention to the next “S” that will turn on the calming
reflex.
The second “S”—Side/StomachThe more upset your baby is, the unhappier he or she will on their back. Roll your
baby onto her side or stomach to activate the calming reflex.
The third “S”—ShhhShushing a crying baby makes them feel at peace and back home in the womb, but it
must be done as loud as your baby is crying and close to their ear—or they will not
even notice it. Consider using a radio tuned to loud static, a tape recording of your
hair dryer or a white noise machine.
The fourth “S”—SwingingAs you support your baby’s head and neck, wiggle his or her head in fast, tiny, gentle
movements. Eventually try moving your baby into a swing for gentle, continual,
hypnotic motion. Make sure that the safety strap in the swing is between your baby’s
wrapped legs and the swing is fully reclined and set on the fastest speed.
The fifth “S”—SuckingThe fifth “S” works best after your baby is calmed by the previous four “S’s”. Offer
your breast or a pacifier.
For more information on the Five “S’s”, please discuss with your Mother/Baby Unit
nurse or read, “The Happiest Baby on the Block” by Harvey Karp, M.D. The book or
DVD is available in the Little Miracles Boutique as well as other retail book stores.
99

100
SIDS PreventionMost babies should sleep on their back. But a few babies have health conditions that
might require them to sleep on their tummy. If your baby was born with a birth
defect, often spits up after eating, or has a breathing, lung or heart problem, be sure
to talk to a doctor or nurse about which sleep position to use.
Guidelines to help keep your baby safe:
• Avoid positioning your baby on her stomach when sleeping.
• Eliminate soft bedding from your baby’s sleep area, such as fluffy blankets, com-
forters, bumper pads, pillows and stuffed animals, to prevent suffocation.
• Crib slats should be no more than 23⁄8-inches apart to prevent the baby’s head
from being caught.
• A firm mattress, covered by a crib sheet only, should be snug against crib rails to
avoid arms, legs or the head from being caught.
• Avoid over dressing and bundling the infant.
• Avoid exposing your newborn to second-hand smoke.
Be sure to place baby on tummy when awake during play time.
Tuck the blanket under the
mattress on three sides to
avoid the possibility of your
infant pulling the blanket
over her head.

101
ImmunizationsChildren receive immunizations to protect them from certain childhood diseases. It
is important that your child receives these immunizations because often the diseases
they prevent are very serious.
Most babies do not have any reactions to vaccines. Among those who do, the
majority are minor local reactions such as pain, swelling, redness at the injection site
or a mild fever. These reactions will go away within a day or two.
Signs of severe allergic reaction can include difficulty breathing, hoarseness or
wheezing, hives, paleness, weakness, fast heart beat or dizziness. If any of these
symptoms occur, call your baby’s doctor immediately.
yo
ur
c
ar
e
at
h
om
e

102
Infant FeedingThe decision of whether to breastfeed or formula feed is a personal one. The feed-
ing choice you use will not only provide the nutrients and calories for growth, it
also will provide a special time to get to know and love your baby. By meeting her
hunger needs, by cuddling and interacting with your baby, you will be helping your
newborn to feel secure and loved.
We hope the following information about breastfeeding and formula feeding will
be helpful to you in these first few weeks. Enjoy your baby in this special time of
your life.
General Feeding Guidelines
• Weight gain is the best indicator that your baby is consuming an adequate amount
of milk. Expected weight gain is approximately one ounce per day or five to seven
ounces per week. It is expected that your baby will initially lose a few ounces after
birth. Weight loss should not be excessive or continue past five days of age.
• By the time the baby is five to seven days old, she should be wetting six to eight
diapers a day, having stools and appearing content after feedings.
• Newborns frequently need encouragement to awaken and feed. They may need
to have their blanket and clothing removed to wake up. Gently rubbing baby’s
feet or back also may be effective. If you are concerned about your infant’s
sleepiness or lack of interest in feeding, contact her physician or Mercy Newborn
Nursery at (515) 643-MOMS, option 3.
• For your baby’s comfort, cold breast milk or formula should be warmed to room
temperature or body temperature before feeding the infant. Always test the tem-
perature of warmed liquid on the inside of the wrist to assure the proper tem-
perature.
• Never use a microwave to warm breast milk or formula. Uneven heating could lead
to severe scalding even when the bottle feels luke warm. Heat baby’s bottle by plac-
ing it under warm running water. If a bottle warmer is used, read directions care-
fully and always test for warmth before feeding baby to prevent scalding.
• All babies need the nutrition of breast milk or iron-fortified formula until their
first birthday. Do not feed your baby regular cow’s milk.
Is Baby Hungry?Your baby is a unique little person who will develop his or her own schedule. Watch
for your baby’s feeding cues and feed when your baby awakens and begins to suck
on lips, fingers, fist or roots toward anything that touches baby’s cheek. Breastfed

103
babies normally feed at least every two to three hours. Formula babies tend to feed
every three to four hours. If feedings have been adequate during the day, your baby
may go four to five hours between feedings at night.
Breastfed babies eat more frequently than formula-fed babies do. This is because
breast milk can be easily digested and passes through the stomach quicker than for-
mula. When the baby is full, she may let go of the nipple, slow her sucking or fall
asleep.
Your newborn’s appetite will vary from feeding to feeding. All babies need
to hear your soothing voice and to be cuddled closely during every feeding.
Propping bottles is dangerous and leads to a higher risk of milk entering the baby’s
lungs, which can cause infection. Propping bottles also will lead to an increased
chance of ear infection and tooth decay.
Formula Feeding, Preparation and Bottle CleaningMix formula according to the package directions. Always wash your hands and the top
of the formula container before beginning. Check the expiration date on the can.
Prepare formula with city tap water. If you are unsure of the water source or use well
water, use bottled water for mixing formula.
If you are using concentrated or powdered formula, be sure to add the correct amount
of water as instructed. Too much water can interfere with calories and nutrient con-
tent; too little can cause diarrhea and dehydration.
You can mix one or several formula bottles at a time. Extra bottles must be stored in
the refrigerator and used within 48 hours.
During feedings, always hold your baby with their head higher than the stomach. Tip
the bottle so the baby drinks the formula instead of the air in the bottle.
In the first few months, formula-fed babies may eat better with less spit-up if burped
about three to four times during a feeding.
Wash bottles and nipples in hot, soapy water using a bottle/nipple brush for complete
cleaning. Rinse them in hot water and allow them to air dry. Most bottles can be safely
washed in the top rack of the dishwasher.
The amount of formula your baby needs is fairly individualized. Typically, in the first
two weeks, the newborn takes about two to four ounces per feeding. The amount will
vary depending upon their hunger and will increase as they grow.
If your baby appears to be getting too much or too little during bottle-feeding,
check the nipple for the flow of the milk. Milk should drip steadily from the nipple
yo
ur
c
ar
e
at
h
om
e

104
opening. If not, the nipple may need to be replaced or
the bottle cap may need to be loosened or tightened.
Always discard any formula left in the bottle at the
end of a feeding. Germs grow quickly!
BurpingBurping your baby helps remove the air that
is swallowed during feedings and is a way of rous-
ing a sleepy baby during a feeding. Burp at the
end of the feeding, between breasts, every half- to
one-ounce of formula or when needed to stimu-
late baby. There is no “best way” to burp your
baby. Try these suggestions to see what works best
for your baby.
• Hold the baby upright against your chest (figure
A).
• Place baby seated in your lap with her head sup-
ported under the chin (figure B).
• Lay baby across your knees (figure C).
Pat or rub your baby’s back gently.
BreastfeedingNature intended for babies to have breast milk,
the ideal first food. Breastfed babies have fewer
colds, allergies, ear infections and other health
problems. Breastfeeding is truly a “health choice”
and benefits mothers and babies in many ways.
Even if you only breastfeed your baby for a few
weeks, you will provide yourself and your baby
with important health benefits. Any breast milk a
baby receives is wonderful and the more breast
milk your newborn gets is even better. Be patient
with yourself and your baby as you both learn
about each other and breastfeeding.
A
B
C

105
Getting started
Breastfeeding moms develop a system of supply and demand as they feed their
infants. When your baby latches at the first breast, they may nurse vigorously for five
to 15 minutes. Usually, breastfed babies suckle in bursts of five to six sucks and rest
for five to 10 seconds, then suckle again repeating this pattern until they begin to get
full. Most of the stored milk in your full breast will be emptied in the first five to 15
minutes of suckling and mother’s breasts will produce more milk if the baby contin-
ues to suckle. Approximately two-thirds of your breast milk is made while your baby
suckles at the breast, so don’t feel you have to wait until your breasts feel full to feed
your baby. Switching breasts halfway through feeding helps ensure both breasts get
emptied and stimulated. Babies may nurse on the second breast for a shorter or
longer time depending on their needs. The next time you nurse, start on the breast
that you ended with last or the side that needs to be emptied most.
Key points for successful early breastfeeding in the hospital
• Put the baby to your breast within the first hour after birth
• Keep your baby in your room during your stay
• Watch for feeding cues: awakening, making mouth movements, and fist sucking
• Awaken baby every two to three hours to breastfeed if not awakening on own
• Avoid pacifiers, artificial nipples and supplemental formula
• Listen for baby swallowing at breast
Positioning At BreastMake yourself comfortable so that you will be relaxed. This will usually involve extra
pillows, a comfortable chair, footstool or even a pillow to sit on in those first tender
days. There are several ways to position your baby at your breast.
Football hold
• Position yourself comfortably in a sitting position with extra pillows under your
arm and across your stomach
• Hold the baby’s back and shoulders in the
palm of your hand
• Tuck the baby under your arm, lining up
the baby’s lips with your nipple
• Support your breast to guide it into the
baby’s mouth
• Hold your breast until the baby nurses
easily
yo
ur
c
ar
e
at
h
om
e
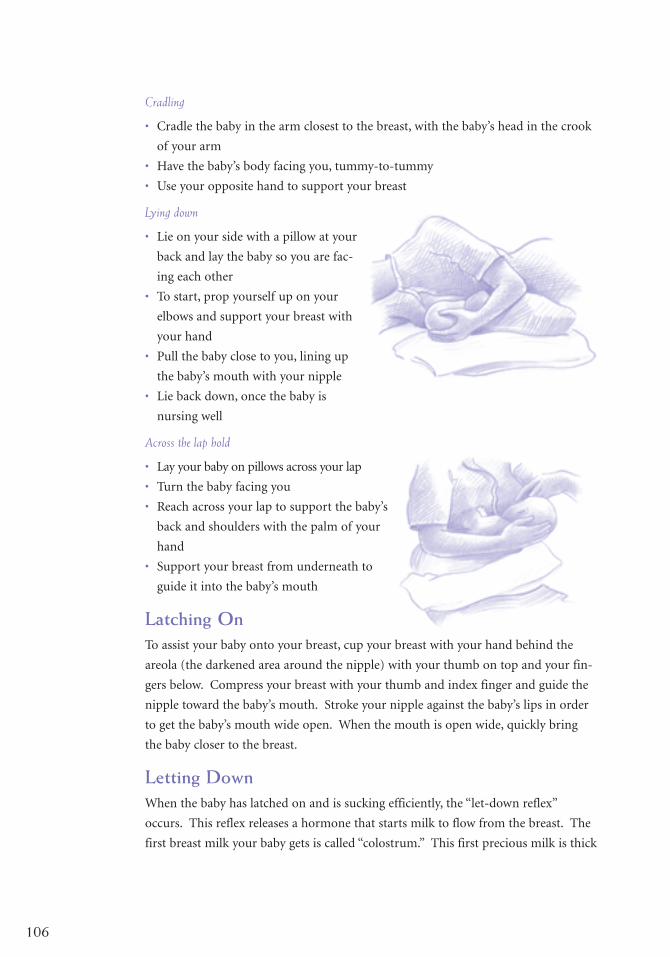
106
Cradling
• Cradle the baby in the arm closest to the breast, with the baby’s head in the crook
of your arm
• Have the baby’s body facing you, tummy-to-tummy
• Use your opposite hand to support your breast
Lying down
• Lie on your side with a pillow at your
back and lay the baby so you are fac-
ing each other
• To start, prop yourself up on your
elbows and support your breast with
your hand
• Pull the baby close to you, lining up
the baby’s mouth with your nipple
• Lie back down, once the baby is
nursing well
Across the lap hold
• Lay your baby on pillows across your lap
• Turn the baby facing you
• Reach across your lap to support the baby’s
back and shoulders with the palm of your
hand
• Support your breast from underneath to
guide it into the baby’s mouth
Latching OnTo assist your baby onto your breast, cup your breast with your hand behind the
areola (the darkened area around the nipple) with your thumb on top and your fin-
gers below. Compress your breast with your thumb and index finger and guide the
nipple toward the baby’s mouth. Stroke your nipple against the baby’s lips in order
to get the baby’s mouth wide open. When the mouth is open wide, quickly bring
the baby closer to the breast.
Letting DownWhen the baby has latched on and is sucking efficiently, the “let-down reflex”
occurs. This reflex releases a hormone that starts milk to flow from the breast. The
first breast milk your baby gets is called “colostrum.” This first precious milk is thick

107
and sticky, but your let-down reflex will help move it to the nipple and the baby.
Signs of let-down vary. You may feel a tingling sensation, warmth, momentary fleet-
ing pain or nothing at all. The sure sign of let-down is your baby swallowing
repeatedly in a suck-swallow rhythm.
The hormone oxytocin that produces the milk let-down reflex also causes cramping
in your uterus. Breastfeeding actually helps the uterus return more quickly to its
pre-pregnant state.
Proper latch-on tips
• Baby’s upper and lower lips are rolled out on the areola
• The mouth is open wide
• You see large jaw movement and hear swallowing
• If nursing is comfortable, you may feel a “tug” or “pull” on your nipple as baby sucks
• Baby’s tongue is down and over lower gums
• Baby’s nose and chin are very close to your breast
Frequency and Length of FeedingsFor the first weeks, you may have to awaken baby for feedings. If you awaken your
baby about every two to three hours during the day, the baby will adjust her days
and nights sooner. Early on, some babies will want to feed as much as every hour or
two at night. By one month, you will usually be feeding baby once or twice at night.
As long as you do not experience nipple pain, let the baby breastfeed as long as she
wants. Usually, it will take a baby approximately 20 minutes to nurse on one breast.
If your baby is still strongly sucking and swallowing after 20 minutes – let her con-
tinue; don’t watch the clock, but watch the baby. Babies will slow down their sucking
as they near the end of a feeding. Most will fall asleep, letting the nipple slide from
their mouth. Remember, the more a baby nurses during the early days, the sooner
your milk supply will come in.
Milk ProductionMilk production is generally influenced by the “supply and demand” principle. The
more a baby nurses, the more milk is produced.
In order to establish your milk supply, nurse frequently, and avoid supplements,
pacifiers and delayed feedings. Supplements of water or formula should be avoided
unless medically indicated, because they decrease the baby’s appetite and time at
your breast. Pacifiers may meet sucking needs that also could be better satisfied at
your breast.
yo
ur
c
ar
e
at
h
om
e

108
The first milk, colostrum, is the perfect start for your baby
and is available in small amounts at first and increases with
each feeding. Usually by the second to fifth day after you
deliver, your milk comes in, meaning more mature milk is
filling your breast in much greater amounts.
As your baby grows, you will notice periods of time when the
baby seems to want to nurse more frequently for longer ses-
sions. This may be a growth spurt. Typical times that this
may happen are three weeks, six weeks, three months and six
months of age. If you are unaware of growth spurts and the
more frequent nursing sessions that go along with them, you
may think your milk supply is inadequate and decide to quit
nursing. The easy remedy is to let your baby nurse more fre-
quently and longer for a day or two until your milk supply
increases to meet the needs of your growing baby.
General Recommendations and BreastCareSuccessful breastfeeding involves avoiding problems before
they happen, and also knowing what to do if problems
arise. The following suggestions will help you avoid some
of the common problems mothers experience with breast-
feeding. Some situations may require additional attention.
Good sources of support and help are lactation consult-
ants, hospital nursery staff, your physician, baby’s physician
or your home care nurse. If symptoms worsen or persist
longer than 24-hours, consult others for assistance.
• Make sure baby is positioned properly at your breast.
• If nipple pain is extreme, you can stop breastfeeding for
24-hours on one or both breasts. It is important, howev-
er, to express milk from your breast at the same frequen-
cy as your baby would nurse. Regular milk expression
will help to prevent further complications.
• You may find your best breastfeeding experiences occur
in a quiet, comfortable and relaxed setting. The “let-
down” reflex will be more efficient in this situation.
• If you need to remove the baby from your breast, gently
break the suction by inserting your finger into the corner
of the baby’s mouth.
Mercy LactationServices, LactationConsultants(515) 358-2082
Little MiraclesBoutique(515) 358-2080
Mother/Baby UnitNursing Staff(515) 358-2050

109
• Air dry your nipples after feedings (10 to 15 minutes without breast pads on and
nursing bra flaps open).
• When you are ready to wean your baby from breastfeeding, do it gradually as
described under Weaning.
Breast and Nipple Care• It is unnecessary to wash your breasts before or after nursing.
• Avoid soap on nipples, it may lead to soreness and cracking.
• Express a small amount of breast milk onto your nipples and gently rub it in after
nursing. Breastmilk has healing properties that can protect or heal sore nipples.
• The routine use of breast cream or ointments is discouraged. They may make the
nipple and areola slick and cause more difficult latch-on.
• Wearing a supportive bra may be helpful for support and comfort. Make sure the
bra fits correctly. A bra that is too tight in the cup or around your rib cage can
lead to engorgement, plugged milk ducts and/or a breast infection. Avoid under-
wire bras.
• Avoid bras or nursing pads with plastic liners, they trap moisture and can lead to
sore nipples.
Breastfeeding Problems You Might HaveLeaking of milk from your breasts can occur in the first weeks of nursing. Nursing pads,
handkerchiefs and other clean cloths are useful for absorbing the leakage. This is normal
in full breasts and will subside when the milk production more closely matches the baby’s
needs. If unexpected leaking happens, you can press firmly against your breasts with your
arms, palm of your hand or fingers to slow or stop the milk flow. Change nursing pads
and bras frequently to keep nipples dry.
Nipple Tenderness/Soreness
Some amount of tenderness at first is normal, but if the baby is positioned correctly
while nursing, nipples should not blister, crack or bleed. Remember to get as much
of the areola (darker area) in the baby’s mouth as possible. Have the infant’s body
facing you and the mouth centered on your nipple. Baby’s mouth should be opened
wide and the bottom lip should be flanged (poked) out. Take your finger and pull
down on the baby’s chin to correct the position if necessary.
yo
ur
c
ar
e
at
h
om
e

110
If your nipples do get sore, try the following:
• Change feeding positions at every feeding. This will help distribute the pressure
of the baby’s gums on a different spot each time you nurse.
• Nurse more often and start on the less tender side.
• Rub breast milk on your nipples after each feeding and let dry. It will actually
help heal them.
• Wear breast shells inside your bra to keep clothing from rubbing on your nipple
and to aid drying.
• Applying ice compresses to your nipples before nursing may help by numbing
your tender nipple for the initial latch-on.
• If you are pumping your breast milk, check the size of the breast cup compared to
your nipple. Too tight a fit or using the pump on too high of a suction setting can
cause tenderness. Use only enough suction to create milk flow.
• If your nipples are cracked or bleeding, rub a very small amount of pure lanolin
breast cream or apply moist healing gel pads on the nipples. The cream doesn’t
have to be removed before the baby nurses. It also helps provide a moisture barri-
er and will allow your nipples to heal faster without forming a scab.
• Expose your nipples to natural sunlight twice a day for 10 to 15 minutes.
• Apply warm wash cloths to your nipples after nursing to help soothe them.
EngorgementEngorgement often happens as your milk comes in two to five days after delivery. This
breast fullness is your milk supply increasing and swelling in your breast tissue. Often
your breasts are so swollen that your nipple flattens out and the baby can’t latch on.
If your breasts get swollen and tender, try the following:
• Express or pump out a little milk before you even try to nurse the baby.
• Nurse often, at least every two to three hours.
• Use a breast pump or hand expression between feedings, if needed.
• Try massaging your breasts before and during feeding.
• Use ice packs on your breast after feedings or pumping to reduce swelling. (A bag
of frozen corn or peas works well).
• Heat is not recommended as it actually increases the swelling in your breast.
• An old folk remedy is to use clean, refrigerated cabbage leaves on your breasts.
Anyone allergic to sulfa medications should not use cabbage.
• Remember, it will get better. Engorgement will only last one to two days.

111
Green Cabbage
Green cabbage can be used to reduce the swelling in your breasts and to help unplug a
duct for milk flow. Prepare the cabbage leaves as described below. Keep cabbage leaves
in place and change leaves every 1- 2 hours or until they become limp and wilted. If
you are using cabbage to unplug a clogged duct, be sure to stop using the cabbage when
you feel relief.
• Discard the two outer leaves of a head of green cabbage.
• Wash the inner leaves and pat dry.
• Take a rolling pin or similar object to crush the leaf and the large vein running
through the leaves. Cutting out the large vein may allow the leaf to fit around the
breast better.
• Pack your breasts in cabbage leaves. Wear your bra to keep cabbage in place.
• Check your breasts frequently, as soon as the milk begins to drip or the breast
feels “different,” remove the cabbage leaves and either try to breastfeed or use a
pump to get the milk flowing.
• Reapply as needed, but not more than three times in a day.
• Attempt to breastfeed or pump at least every two (2) hours.
• Remember, use cabbage only to the point milk is starting to flow and the
breasts are softening.
• At anytime while using the cabbage you notice a rash or irritation to your skin,
stop using it at once.
Plugged Milk DuctIf you don’t empty your breasts when they are full, you could develop a plugged milk
duct. It becomes “stopped up” much like a plumbing pipe. When this happens, you
might notice a small tender spot or lump in your breast. It might happen when the
baby decides to sleep through the night or if you get busy and don’t nurse as often.
Sometimes a tight bra can be pressing on a milk duct.
To relieve a plugged milk duct:
• Get plenty of rest and nurse often
• Apply warm, moist heat to the plugged duct, soak in warm water or take a hot
shower or bath
• Point the baby’s nose and chin toward the plugged duct as they nurse, to more
fully empty that area
• Pay special attention and massage the area while the baby nurses to help with milk
flow
• Use a breast pump after nursing to help move the milk
yo
ur
c
ar
e
at
h
om
e

112
If you have the same symptoms of a plugged duct plus feel achy like you have the
“flu” and a fever, you probably have a breast infection (mastitis). You may develop a
breast infection if you do not treat a plugged duct. If your breast does get infected,
you should use the same treatment as described below and call your physician. An
antibiotic will probably be prescribed for you. Remember to continue nursing fre-
quently because an empty breast will heal faster. Mastitis is not an infection of the
milk; therefore, it is safe to continue breastfeeding your baby.
Mastitis is common during the holiday season due to stress and lack of sleep in a
new mother. Delayed or missed feedings may lead to mastitis.
Breast Infection (mastitis) Treatment• Call your physician for possible antibiotic treatment
• Empty your breast frequently, nurse often
• Use heat and massage to open the affected duct
• Get extra rest and fluids
• Point your baby’s nose and chin to the affected area during nursing to better empty
the duct
• Take medication for fever and achiness
Is Baby Getting Enough?• Feed your newborn eight to 12 times in 24-hours
• Your baby should have a wet diaper for every day of age until your milk is in two to five
days after birth
• By the time your milk is in, between the second and fifth day, you should see six
to eight wet diapers per
24-hours and four or more, possibly up to 10, stools per 24-hours
• The stools should change color from black meconium, to “Army” green, to mus-
tard yellow
• Stools should be loose and seedy
• You should hear your baby swallowing when breastfeeding and see lots of large jaw
motion and sucking
• Your baby should be content for one to two hours between most feedings
• Your breast should feel softer and less full at the end of each feeding

113
Your baby should gain approximately one ounce per day or five to seven ounces per
week. Remember, all babies lose some weight in the first days, but usually start gain-
ing by the fifth day and regain or exceed their birth weight by two weeks of age.
Day Wets StoolsDay 1 1-2 1-2 dark
Day 2 2-3 2-3 dark to greenish-brown
Day 3 3-4 3-4 greenish brown to yellowish
Day 4 3-4 3-4 greenish-brown to yellowish
Days 5-7 6+ 3-4 greenish-brown to yellowish
After four weeks of age, stool patterns change. The volume of stool usually increases
and the frequency decreases. However, each baby is different.
Pacifiers, Bottles andOffering an Occasional Bottle of Expressed Breast MilkBreastfeeding your baby without offering the bottle for the first three to four weeks
will give both of you ample time to become comfortable with nursing. Offering
bottle nipples in the first three weeks often confuses the baby since she must use a
different suck on your breast nipple and the bottle nipple. Sometimes pacifiers will
cause the same confusion for a very young baby. Any time after three weeks, you
may offer a bottle to acquaint your baby with that nipple. An occasional offering of
a bottle (once or twice a week) of expressed breast milk is a way to let dad share in
this special time.
WeaningWeaning begins when your breastfed infant takes food or fluids from a source
other than your breasts. You should determine the right time to begin weaning.
Sometimes your baby will lead you in weaning, or it may be you leading the baby.
You may experience a variety of feelings and concerns as both of you go through
this change.
• Gradual weaning is easiest on both you and the baby. Eliminate one breastfeeding
per day, every two to three days. This method allows your milk supply to decrease
slowly. Breast fullness and discomfort are avoided and your baby has time to
adapt to the change.
yo
ur
c
ar
e
at
h
om
e

114
• Rapid weaning may be necessary due to certain
situations. Replace two to three breastfeedings a
day with formula feedings. Increase the number
of eliminated feedings each day until the baby is
no longer nursing.
• Whenever a timetable is used, it is important to
express enough breast milk to relieve discomfort
and fullness. It may be several drops or an ounce
or two. Using this method, the production and
supply of breast milk slowly decreases. This prevents
the accumulation of milk in the milk ducts that could
lead to a breast infection.
• During weaning, give your baby lots of extra cuddling and love.
• Depending on the age of the baby, substitute a formula feeding by bottle or cup as
indicated.
• Remember, babies need breast milk or formula until their first birthday.
Expressing and Storing Breast MilkExpressing breast milk can be accomplished by using a breast pump or by hand
expression. Expressing may be a way to maintain or stimulate your milk supply. It
is also the way your baby can receive your breast milk when you must be away dur-
ing feedings.
As with anything, expressing milk is an acquired skill. Initially, it may seem awk-
ward and time consuming, but with practice it gets easier.
Breast Pumps
Breast pumps are available in electric and hand pumps. You may want to talk to
other mothers or the Lactation Consultants to find out what pump worked best for
them. Each breast pump is a little different. Be sure to read the directions carefully
before using and cleaning the pump you choose. Mercy Lactation Consultants have
a full line of breastfeeding pumps, accessories and nursing bras available to pur-
chase. For more information, call (515) 643-MOMS, option 4. All purchases are tax
exempt and Master Card, Visa, cash and check are all accepted for payment.
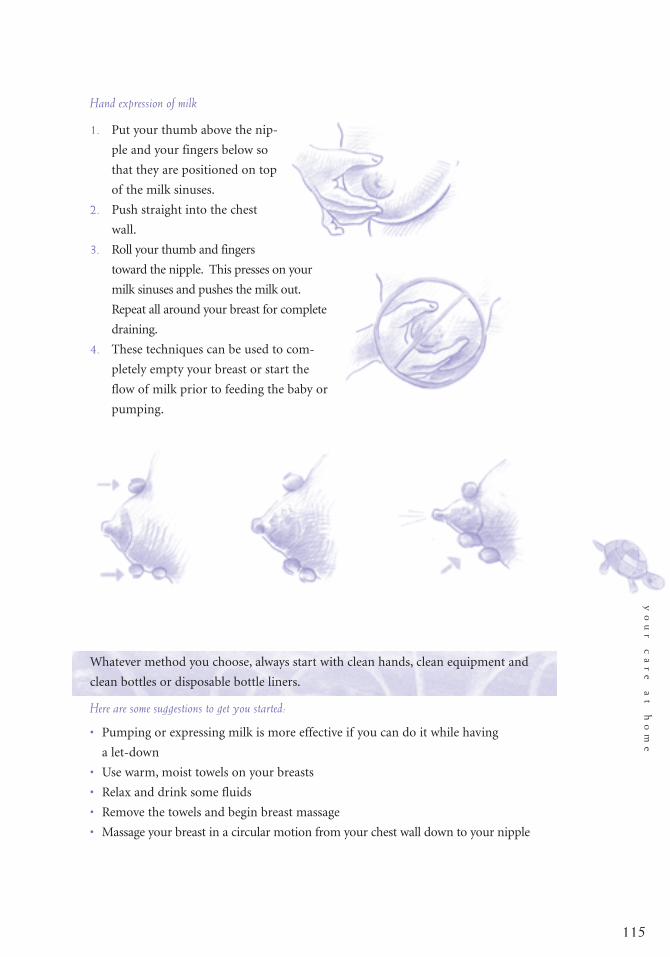
115
Hand expression of milk
1. Put your thumb above the nip-
ple and your fingers below so
that they are positioned on top
of the milk sinuses.
2. Push straight into the chest
wall.
3. Roll your thumb and fingers
toward the nipple. This presses on your
milk sinuses and pushes the milk out.
Repeat all around your breast for complete
draining.
4. These techniques can be used to com-
pletely empty your breast or start the
flow of milk prior to feeding the baby or
pumping.
Whatever method you choose, always start with clean hands, clean equipment and
clean bottles or disposable bottle liners.
Here are some suggestions to get you started:
• Pumping or expressing milk is more effective if you can do it while having
a let-down
• Use warm, moist towels on your breasts
• Relax and drink some fluids
• Remove the towels and begin breast massage
• Massage your breast in a circular motion from your chest wall down to your nipple
yo
ur
c
ar
e
at
h
om
e

116
Storing Breast MilkSometimes it is necessary to store the milk you’ve just expressed. Proper storage is
essential. If you are going to freeze your breast milk, leave some space at the top of
the container. Breast milk, like most liquids, expands as it freezes.
Follow these guidelines and use disposable bottle liners to store milk.
• Mark the date, time and baby’s name on each bag/container if you’ll be taking it
to your day care provider.
• Freeze your milk in two- to four-ounce portions. Smaller amounts thaw quicker
and you will waste less milk.
• You may continue to add small amounts of breast milk to the same container
throughout the day. Chill in the refrigerator until evening. Then freeze the con-
tainer.
Defrosting Frozen Milk• Place milk in the refrigerator the night before you’re going to use it. Refrigerator
defrosting takes 12 hours.
• Place milk under warm running water or in a pan of warm water.
• Never microwave breast milk. This can destroy some of the milk’s immunological
components and possibly burn your baby.
• Fat in breast milk will separate and rise to the top. Gently shake the container to
mix the milk.
• Never refreeze thawed breast milk.
• Remember, the color, consistency and odor of your breast milk may vary depend-
ing on your diet.
• Discard any breast milk you don’t use during a feeding.
Breast Milk Storage GuidelinesRoom Cooler with Refrigerator Self-contained Deep
Temperature three frozen Refrigerator Freezerice packs Freezer Unit
Freshly 4 hours at 24 hours at 5-7 days at 3-4 Months 6-12 monthsExpressed 66-72°F 59°F (15°C) 32-39° at 0°FMilk (19-22°C) (0-4°C) (-19°C)
Thawed Do not store Do not store 24 hours Never NeverBreast Milk refreeze refreeze(Previously thawed thawedFrozen) breast milk breast milk

117
Returning to Work or SchoolYou can work or go to school and continue to breastfeed. When you and your baby
are together, breastfeed frequently to help keep your milk supply steady. When you
are away you can do one of the following:
• Find a caregiver close to work or school. Go to your baby or have your baby
brought to you to breastfeed.
• Arrange for a place to collect and store your breast milk at work or school. Pump
or hand express about every three hours. Keep the milk chilled. Leave your breast
milk with the caregiver to feed the next day.
• Have the caregiver feed your baby formula. You may need to express milk during
the day for comfort in the early weeks.
Gradually adjust to your new schedule by return to work or school part-time in the
beginning if possible.
Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
yo
ur
c
ar
e
at
h
om
e

Notes:
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
118

H E L P F U L I N F O R M AT I O N
Important Phone Numbers • 121
Community Resources • 121
Bibl iography • 124
119


121
Important Phone Numbers
INSURANCE COMPANY______________________________________________
MOTHER’S PHYSICIAN ______________________________________________
BABY’S PHYSICIAN __________________________________________________
MERCY MEDICAL CENTER - DES MOINES ..............................(515) 247-3121
1111 6th Avenue, Des Moines, IA 50314
BEREAVEMENT SUPPORT ..................................................................(515) 247-3207
BIRTHING UNIT ....................................................................................(515) 358-3000
BIRTH CERTIFICATES .......................................................................... (515) 286-3781
CHILDBIRTH CLASS REGISTRATION ........................(515) 643-MOMS, option 1
CLASS CANCELLATIONS - INCLEMENT WEATHER ..............(515) 358-5060
CHILDREN’S CENTER AT MERCY - PEDIATRICS UNIT ..............(515) 247-3300
HOME CARE ..........................................................................................(515) 247-8383
INFANT CPR CLASSES..........................................................................(515) 243-2584
LACTATION CONSULTANTS ............................................................(515) 358-2082
LITTLE MIRACLES LACTATION BOUTIQUE..................................(515) 358-2080
MATERNITY TRIAGE AND TREATMENT UNIT ............................(515) 358-3100
MERCY NURSE ..................................................................(515) 643-MOMS, option 1
MOTHER/BABY UNIT ..........................................................................(515) 358-2000
NEWBORN NURSERY ..........................................................................(515) 358-2050
Answered 24-hours a day for any infant concerns.
PATIENT ADVOCATE ..........................................................................(515) 643-2861
SOCIAL SERVICES ................................................................................(515) 247-4330
VARIETY NEONATAL INTENSIVE CARE UNIT ..............................(515) 358-4000
VISITING NURSE SERVICES ..............................................................(515) 288-1516
Community ResourcesHotline Information
CHILD ABUSE HOTLINE ....................................(515) 283-9222 or 1-800-362-2178
DRUG USE HOTLINE (prevention and treatment information) ....1-800-729-6686
he
lp
fu
l
in
fo
rm
at
io
n
Helpful Information

122
NATIONAL AIDS HOTLINE
(for information, testing, medical care) ..............................................1-800-342-2437
NATIONAL DOMESTIC VIOLENCE HOTLINE
(information, support) ........................................................................1-800-799-7233
NATIONAL SPANISH-LANGUAGE HOTLINE ..............................1-800-344-7432
NATIONAL STD HOTLINE ................................................................1-800-227-8922
POSTPARTUM DEPRESSION SUPPORT ........................................(515) 246-6555
Call family physician or First Call For Help
RAPE CRISIS LINE
(information, support & referral) ........................................................(515) 286-3535
SUICIDE PREVENTION HOTLINE....................1-800-784-2433 or (515) 244-1000
YOUTH AND SHELTER HOTLINE ..................(515) 233-2330 or 1-800-600-2330
Helpful NumbersADOPTION INFORMATION ..............................................................1-800-862-3678
ALCOHOLICS ANONYMOUS (INFORMATION & REFERRAL) ..1-800-711-6375
AUTO SAFETY HOTLINE
(VEHICLE & CAR SEAT INFORMATION) ......................................1-888-327-4236
BIRTH CERTIFICATE AND
PATERNITY INFORMATION ..............................(515) 281-4944 or (515) 281-5871
DES MOINES MOTHERS OF MULTIPLES ......................................(515) 967-4152
EMERGENCY FOOD PANTRY LOCATIONS ..................................(515) 246-6555
FAMILY VIOLENCE CENTER ..............................................................(515) 243-6147
FIRST CALL FOR HELP ........................................................................(515) 246-6555
FOOD FOR WOMEN, INFANTS AND CHILDREN (WIC) .......... (515) 697-6700
HIV/AIDS COUNSELING AND TESTING ........................................(515) 286-2088
IOWA SUDDEN INFANT DEATH (SIDS) ALLIANCE ....................(515) 279-6928
LA LECHE LEAGUE ..............................................1-800-525-3243 or (515) 457-7174
POISON CONTROL ..................................................(515) 241-6254 1-800-352-2222
SOCIAL SECURITY INFORMATION ................................................1-800-772-1213
U.S. CONSUMER PRODUCT SAFETY COMMISSION ................1-800-638-2772
Free Immunizations
CHILD HEALTH INSURANCE PROGRAM......................................1-877-543-7669
HAWKEYE HEALTH INSURANCE FOR CHILDREN ....................1-800-257-8563
HOUSE OF MERCY MEDICAL CLINIC 1409 Clark Street ............(515) 362-6525
POLK COUNTY DEPARTMENT OF SOCIAL SERVICES
1900 Carpenter (ask for General Relief) ..............................................(515) 286-3702
1740 Garfield (ask for General Relief) ..................................................(515) 286-2124

123
he
lp
fu
l
in
fo
rm
at
io
n
Health Departments
Area health departments offer a variety of services, including well-child assessments,
immunizations, WIC and child-development information.
DALLAS COUNTY HEALTH NURSE ................................................(515) 993-3750
MADISON COUNTY BOARD OF HEALTH ....................................(515) 463-2636
POLK COUNTY HEALTH DEPARTMENT .................................... (515) 286-3798
WARREN COUNTY HEALTH NURSE ..............................................(515) 961-1003
Poison Control Centers
IOWA POISON CONTROL CENTER ..............1-800-352-2222 or 1-800-272-6477
Mental Health Services
Area mental health services that offer counseling, referral and education opportunities.
MERCY FRANKLIN HELP LINE ..........................................................(515) 271-6111
POLK COUNTY MENTAL HEALTH SERVICES ..............................(515) 283-9111
Child Care Information
These groups offer assistance locating names and numbers of licensed childcare
providers.
CHILD CARE RESOURCE & REFERRAL
OF CENTRAL IOWA ....................................................286-3536 or 1-800-722-7619
Other Important Numbers
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________

124
Bibliography1. Americanbaby.com
2. Babycentral.com
3. Dr. Koop Lifecare Corporation; www.drkoop.com
4. The National Women’s Health Information; www.4woman.org/faq/folic.htm
5. iVillage.com, The Women’s Network;
www.ivillage.com/topics/family/pregnancy
6. About Network; http://pregnancy.about.com/cs/pregnancy/
7. “How Your Baby Grows,” March of Dimes
8. “Be Good to Your Baby Before it is Born,” March of Dimes
9. “Think Ahead for a Healthy Baby,” March of Dimes
10. “Eating for Two,” March of Dimes
11. “A Miracle in the Making,” Bruce Hayman, Budlong Press Company, 1999
12. “Pregnancy Labor and Birth Guide,” Pampers Parenting Institute,
Proctor & Gamble, 2000
13. “Prenatal Care – 9 Months,” March of Dimes
14. “Sexually Transmitted Diseases – What you should know,”
March of Dimes
15. Babycenter.com, the Web’s leading information source on pregnancy
and baby; Growth and Development
16. American Cancer Society, How to do a Self Breast Exam
17. National Highway Transportation Safety Association
18. “The Happiest Baby on the Block: The New Way to Calm Crying and Help Your
Newborn Baby Sleep Longer,” Harvey Karp, M.D., Bantam Dell, 2002
19. SIDS Alliance, What Every Parent Should Know, Reducing the Risks
20. National Immunization Program–Parent’s Guide to Childhood Immunization

125
Notes:________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________

126
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
________________________________________________
______________________________________
____________________________________
____________________________________
____________________________________
____________________________________