l11 pemeriksaan limfonodi 2014
DESCRIPTION
hTRANSCRIPT
JURUSAN KEDOKTERAN GIGI UNSOEDJURUSAN KEDOKTERAN GIGI UNSOED

Tujuan umum : untuk memperoleh informasi mengenai status kesehatan pasien
Tujuan definitif :- Identifikasi status normal- mengetahui variasi keadaan normal dgn
cara menvalidasi keluhan dan gejala pasien
- Penapisan / screening keadaan pasien- Pemantauan kesehatan / penyakit pasien
saat ini
4 teknik pemeriksaan fisik (universal) :1. Inspeksi : melihat &mengevaluasi pasien
secara visual
2. Palpasi : menyentuh, merasakan dengan tangan
3. Perkusi : menepuk permukaan tubuh secara ringan & tajam untuk menentukan posisi, ukuran dan densitas struktur atau cairan atau udara dibawahnya
4. Auskultasi : mendengar suara tubuh pada paru-paru, jantung, pembuluh darah dan bagian dalam / viscera abdomen
1. Inspeksi• Inspeksi : melihat & mengevaluasi
pasien secara visual• Konsentrasi – natural memperhatikan
pasien secara seksama, persisten dan tidak terburu-buru
• Perhatikan bila terdapat luka, massa abnormal, ataupun asimetri wajah dan leher.
• Gunakan pula indera pendengaran dan penciuman utk validasi visual

2. palpasi
• Palpasi : menyentuh, merasakan dengan tangan
• Merupakan langkah ke 2 stlh inspeksi• Menggunakan bagian tangan yg paling
sensitif utk palpasi• Gunakan pads atau ujung jari bag. distal
ruas interphalangeal – ujung saraf sensitif terkelompok slg berdekatan
• Dorsum tangan utk pengukuran kasar suhu tubuh
• Jenis palpasi : ringan, medium, dalam

• Palpasi ringan : superfisial, lembut, berguna utk menilai lesi permukaan/ dlm otot, juga dpt membuat pasien relaks sebelum palpasi medium dan dalam. letakkan scr ringan ujung jari pd kulit pasien, gerakkan jari secara memutar
• Palpasi medium utk menilai lesi medieval pd peritoneum dan massa, nyeri tekan, pulsasi & nyeri lakukan dgn menekan permukaan telapak jari 1-2 cm ke dalam tubuh pasien menggunakan gerakan sirkuler/memutar
• Palpasi dalam utk menilai organ dalam rongga tubuh, dpt dilakukan dgn 1 atau 2 tangan, gerakan sirkuler menekan 2-4 cm

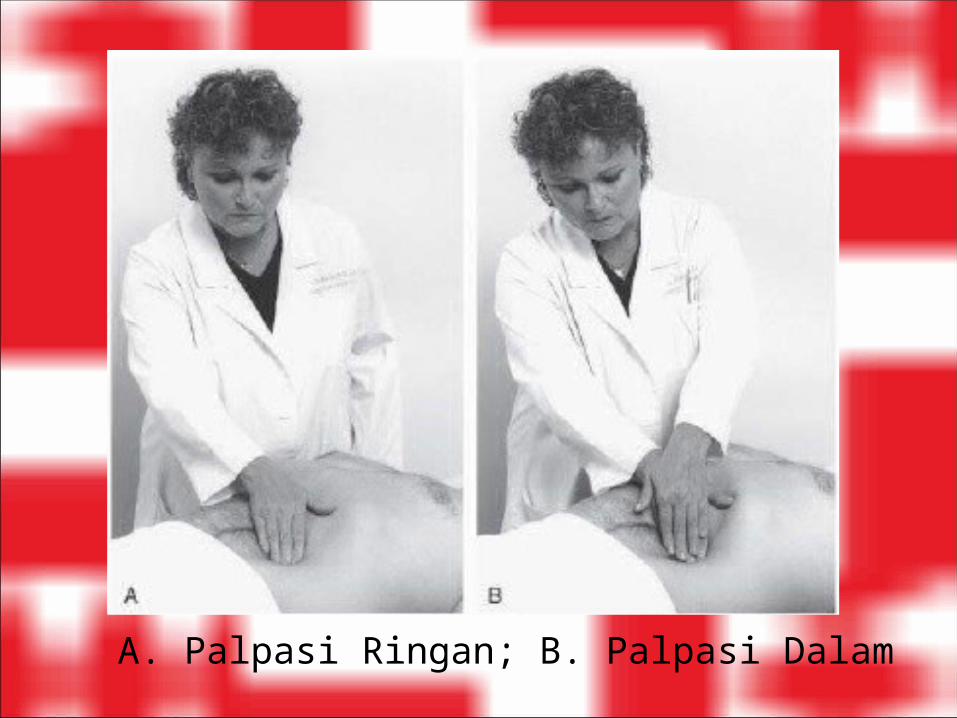
A. Palpasi Ringan; B. Palpasi Dalam
3. Perkusi
• Perkusi : menepuk permukaan tubuh secara ringan & tajam untuk menentukan posisi, ukuran dan densitas struktur atau cairan atau udara dibawahnya
• 2 cara : langsung & tak langsung• Pleksimeter & Plessimeter

Perkusi jari tidak langsung
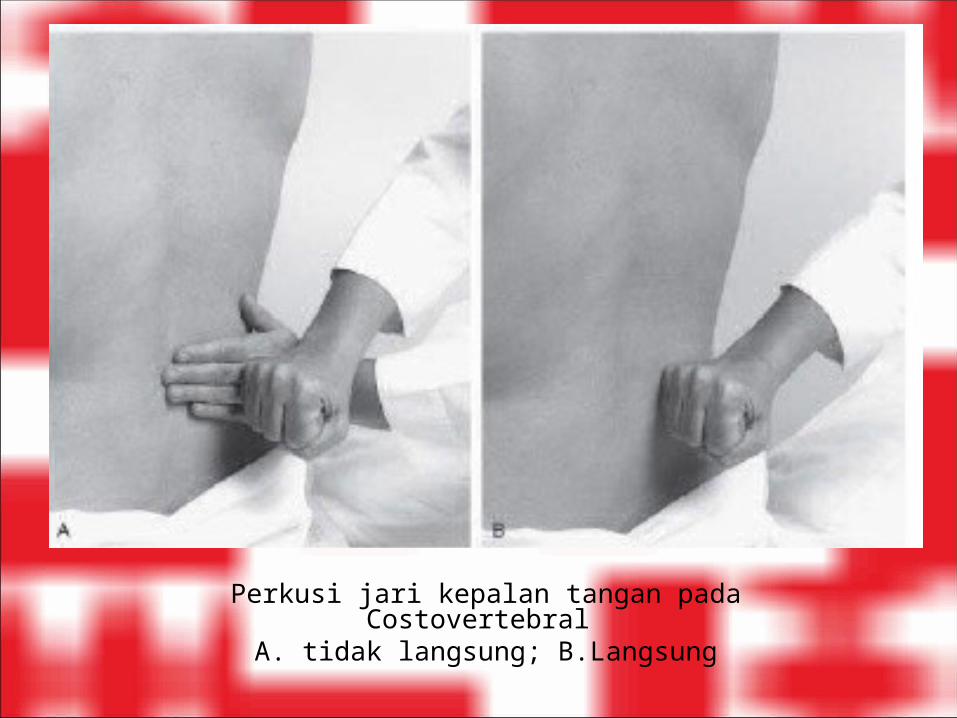
Perkusi jari kepalan tangan pada Costovertebral A. tidak langsung; B.Langsung

4. auskultasi
• Auskultasi : mendengar suara tubuh pada paru-paru, jantung, pembuluh darah dan bagian dalam / viscera abdomen
• Menggunakan stetoskop

Pemeriksaan ekstra oral

LIMFONODI• Lymph nodes / Limfonodi/ Nodus Limfatika adalah
struktur kecil, lunak, bulat atau oval yg dpt ditemukan di seluruh tubuh dan berhubungan satu sama lainnya dlm model spt rantai oleh kanal serupa pemb.darah.
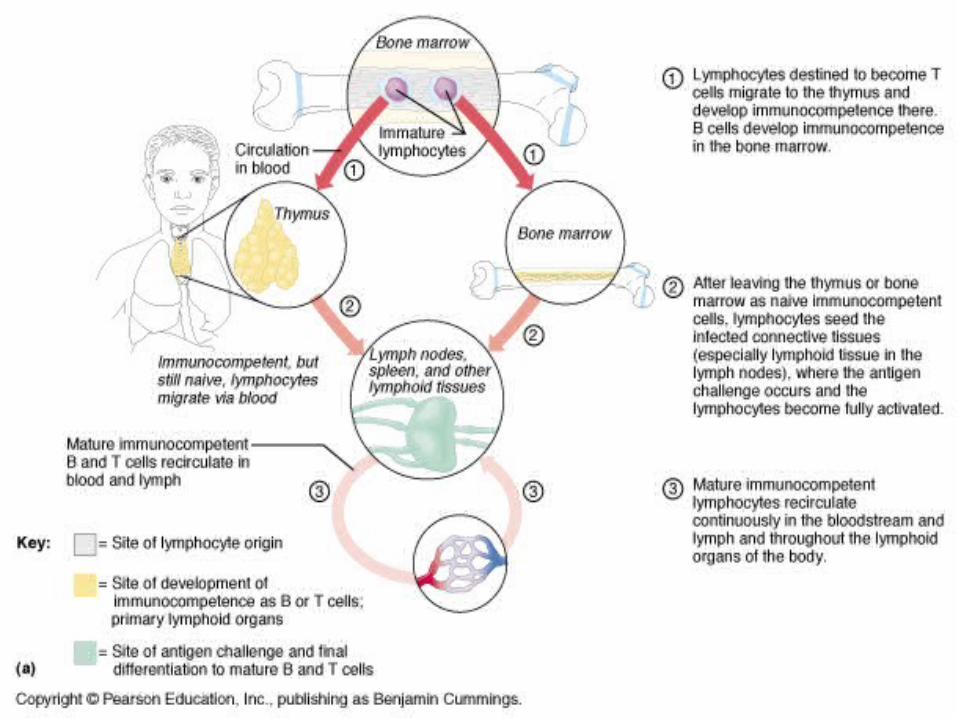

• Setiap limfonodi diselubungi oleh suatu kapsul yg terdiri dari jar.ikat. Di dlm kapsul, nodus mengandung sel2 imun (limfosit dan makrofag) maturasi awal limfosit di centrum germinale cortex limfonodi.
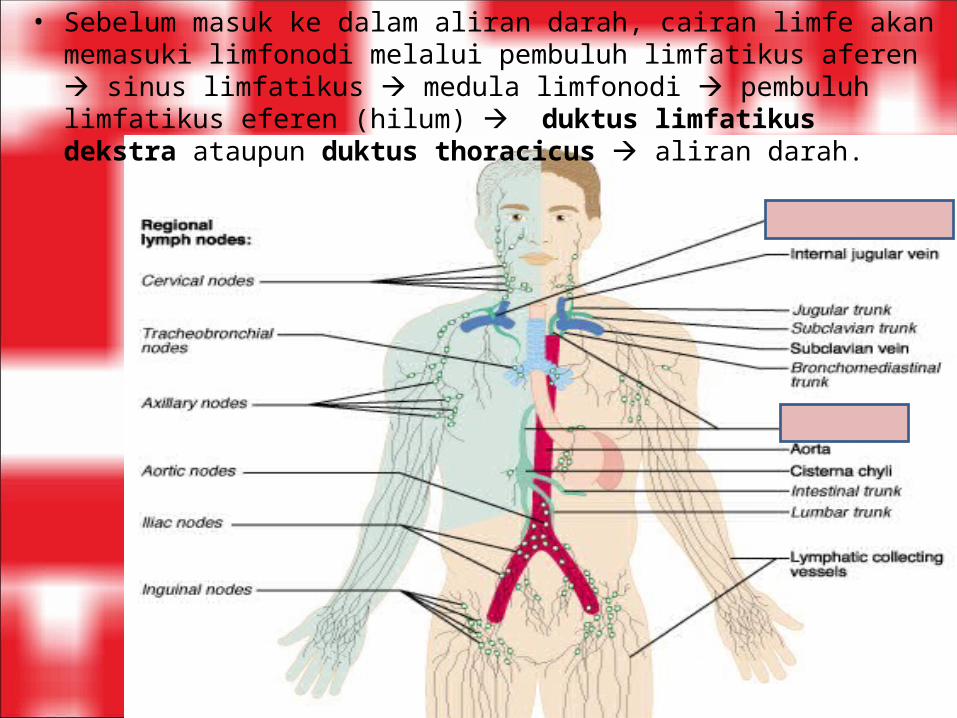
• Sebelum masuk ke dalam aliran darah, cairan limfe akan memasuki limfonodi melalui pembuluh limfatikus aferen sinus limfatikus medula limfonodi pembuluh limfatikus eferen (hilum) duktus limfatikus dekstra ataupun duktus thoracicus aliran darah.
• Limfonodi yg membengkak dikenal dengan istilah Lymphadenopathy atau Lymphadenitis.
• Limfonodi membengkak ketika aktif akibat proses infeksi, inflamasi, kanker dan penyebab lain.
• Pd pemeriksaan perlu diperhatikan :1. teraba/ tidak
2. jumlah dan ukuran (single/ multiple; ada perbesaran/ tidak normal < 1cm) 3. tenderness (sakit / tidak sakit saat dipalpasi) 4. konsistensi (keras/ kenyal/ lunak) 5. mobilitas (bergerak/ tidak) 6. lokasi (unilateral/ bilateral)
Pemeriksaan LIMFONODI KEPALA-LEHER
Interpretasi hasil Pemeriksaan Limfonodi Kepala-leher: •Normal : tidak teraba, tidak sakit
•Kelainan Akut : teraba, ada pembesaran, dpt bergerak, lunak, dan sakit •Kelainan Kronis : teraba, ada pembesaran, dpt bergerak, kenyal, dan tidak sakit •Kanker yg menyebar ke Limfonodi (metastase): teraba, keras, tidak sakit, dan tidak bergerak
•Kanker pd Limfonodi Limphoma nodes : firm and rubbery Hiperplastic nodes : soft

Penyebab Limfadenopati/ Limfadenitis : Penyebab umum limfadenopati adalah proses inflamasi dan infeksi :a.Kronik : ISPA, infeksi dental, tonsillitis-pharyngitis, stomatitis, atau dermatitis, tuberculosis, syphilis.b.Akut : infeksi bakteri (mis. abses akut), virus dan ricketsia (mis. mumps, herpes zoster, herpes simpleks, Erythema Multiforme), infeksi mononukleosis
Penyebab yg jarang terjadi:a.Metastase tumor pada limfonodib.Neoplasma pd sistem limfatika, misal : limfoma, limfosarkoma, Penyakit Hodgkin, leukimia, reticular cell sarcoma
Note : •Gradually enlarging groups of nodes in the absence of local infection and inflammation are a significant finding that suggests either systemic disease (eg, infectious mononucleosis or generalized lymphadenopathy associated with human immunodeficiency virus [HIV] infection) or a lymphoid neoplasm (lymphoma or Hodgkin’s disease)
•such a finding justifies examination for (or inquiry about) lymphoid enlargement at distant sites, such as the axilla, inguinal region, andspleen, to confirm the generalized nature of the process.

Teknik Pemeriksaan Palpasi Limfonodi Kepala-Leher
Klasifikasi anatomi limfonodi leher-kepala
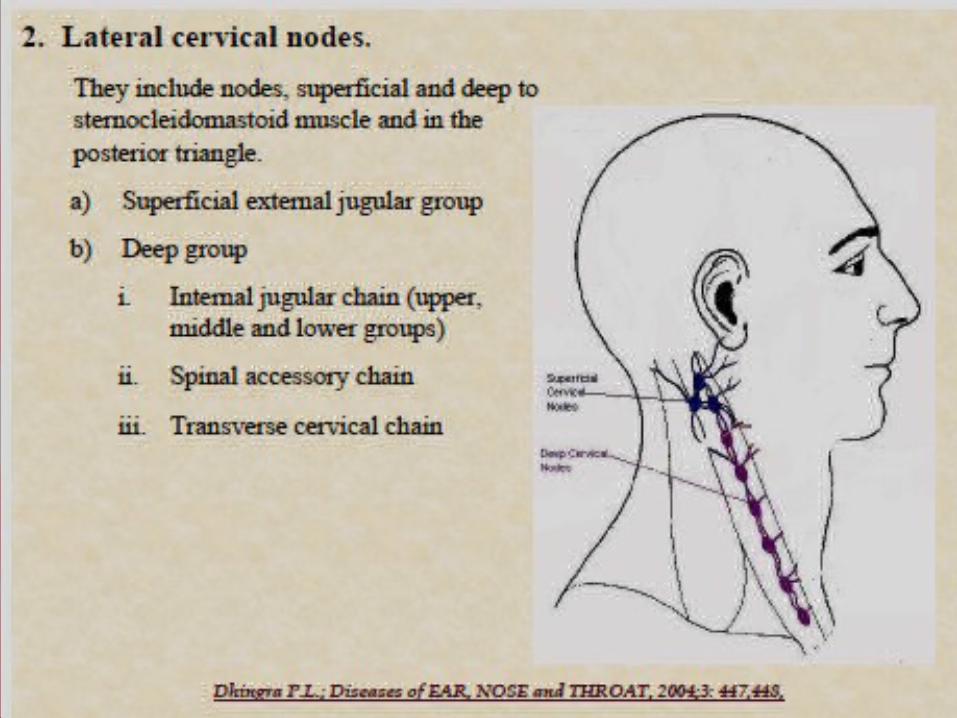
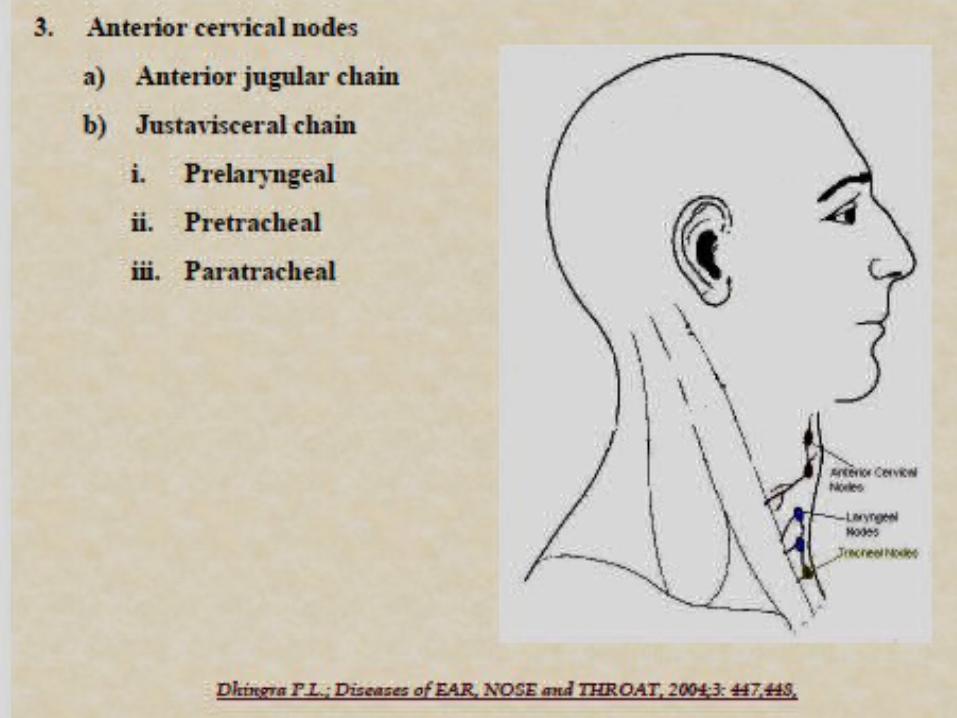
Berdasarkan anatomi limfonodi leher kepala dapat dibedakan mjd 3 :1.Upper Horizontal Chain of Nodes2.Lateral Cervical Nodes3.Anterior Cervical Nodes


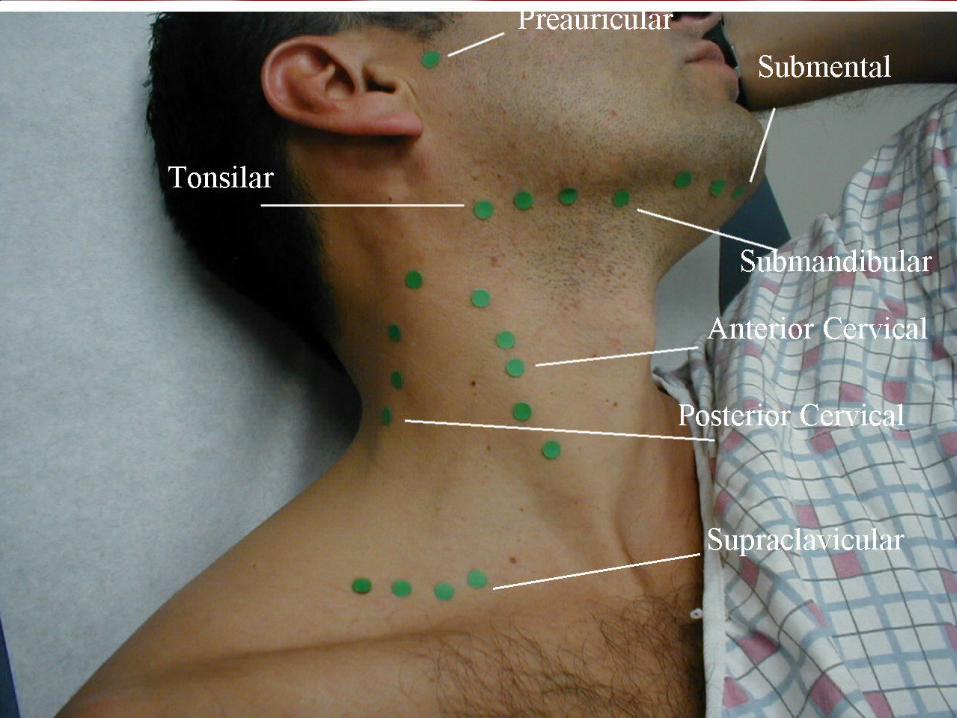
• Lokasi Limfonodi Kepala-Leher :1. Ln. Occipital - At the base of the skull2. Ln. Postauricular (Ln. Mastoidea) - Behind the ear3. Ln. Preauricular - In front of the ear4. Ln. Parotid – At the parotid glands/ cheeks Ln. Tonsillar - At the angle of the jaw 5. Ln. Submandibular - Under the jaw on the side 6. Ln. Submental - Under the jaw in the midline
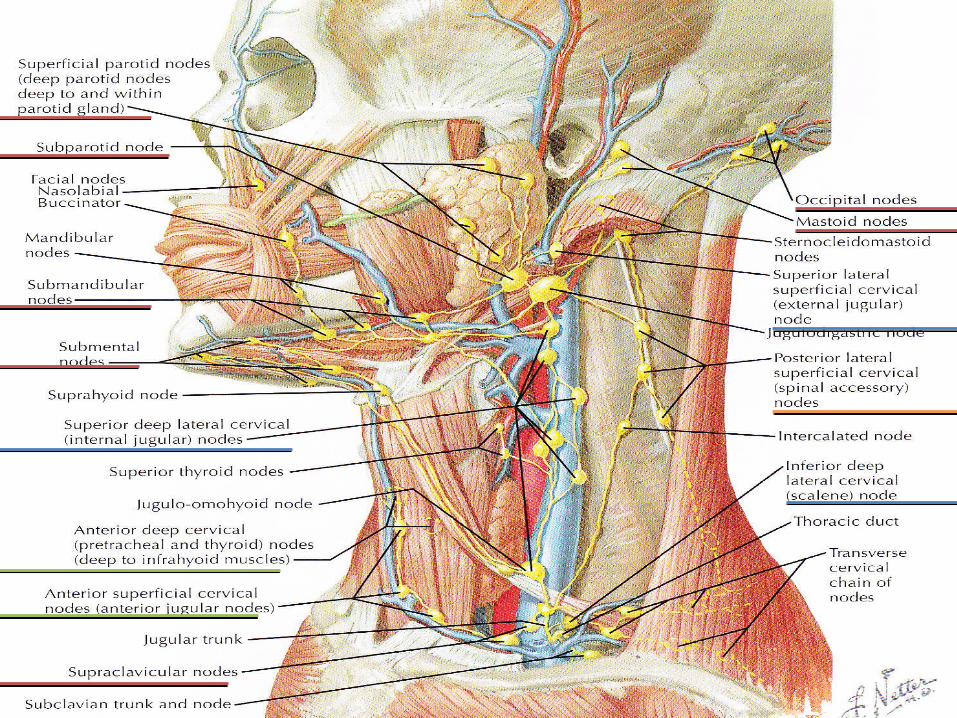
Lokasi & DRAINASE LIMFONODI Kepala-Leher
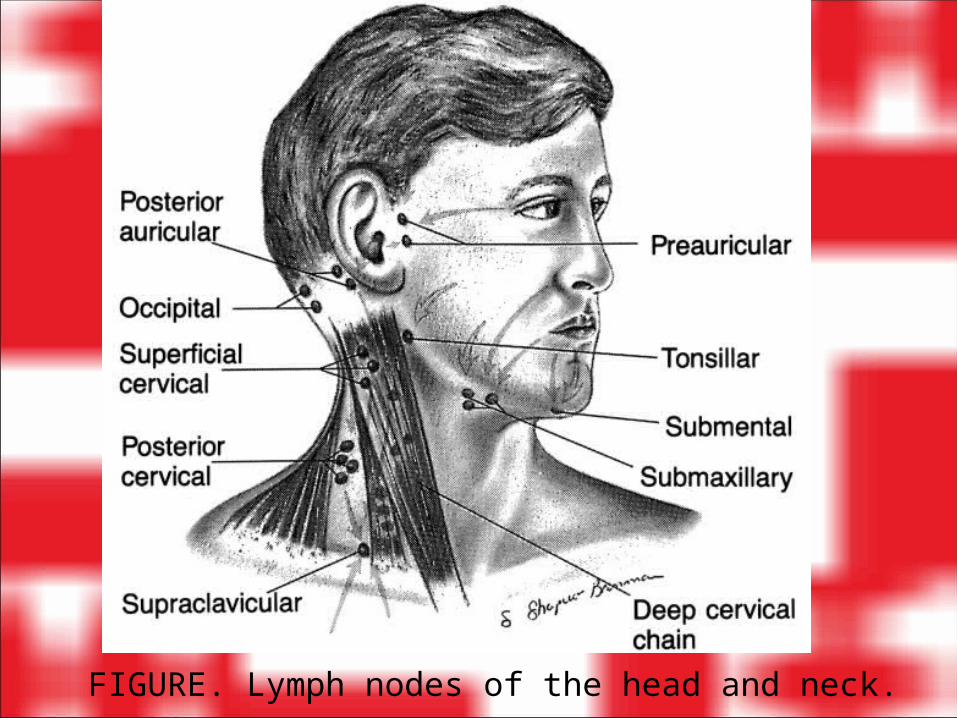
FIGURE. Lymph nodes of the head and neck.

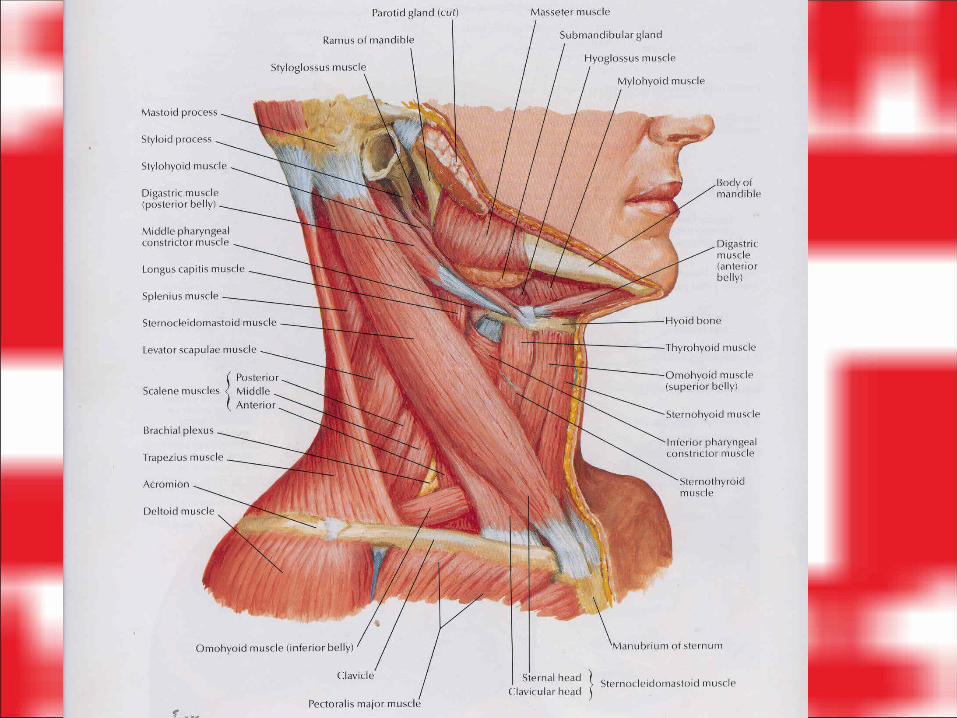
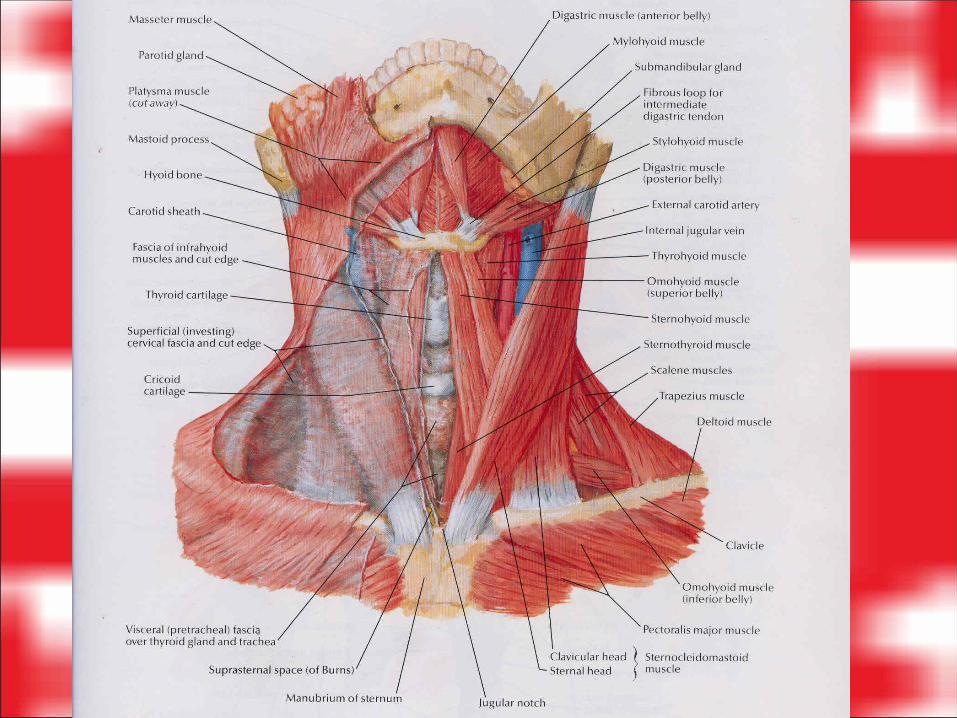
7. Ln. Anterior Cervical – in front of the sternomastoid muscle8. Ln. Superficial Lateral Cervical – above the sternomastoid muscle 9. Ln. Deep Lateral Cervical (Superior-Posterior) – between the sternomastoid muscle and cervical fascia below the sternomastoid and cannot be palpated without getting underneath the muscle10. Ln. Posterior Cervical in the posterior triangle close to the anterior border of the trapezius muscle.11. Ln. Supraclavicular - In the angle of the sternomastoid and the clavicle

FIGURE. Lymph nodes of the head and neck.
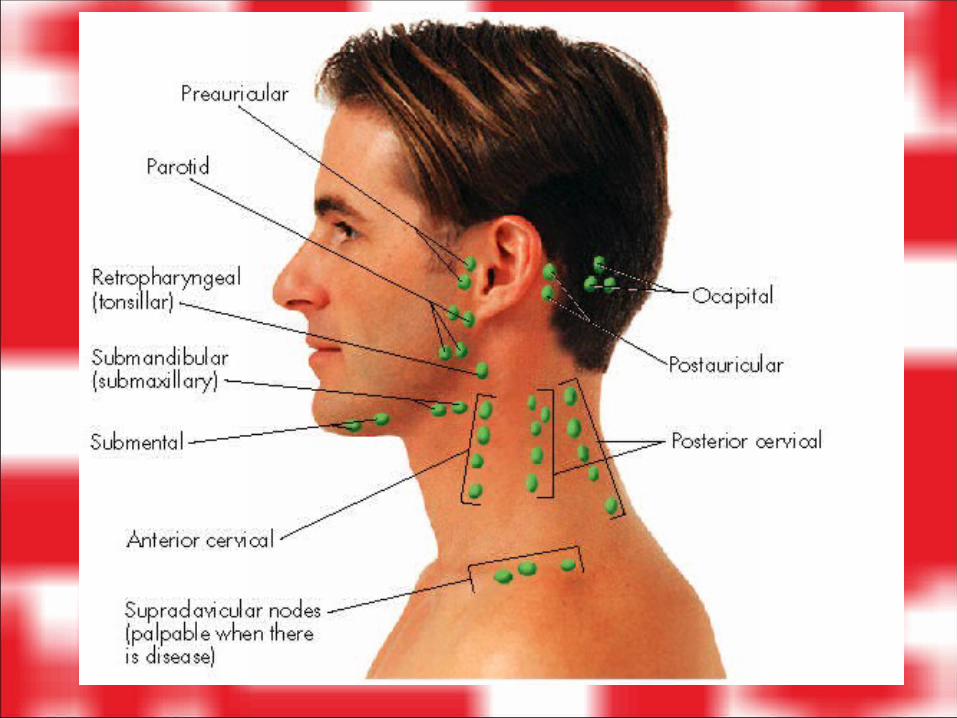

A.SubmentalB.SubmandibularC.ParotidD.PreauricularE.PostauricularF.OccipitalG.Anterior cervicalH.Posterior cervicalI. Supraclavicular

1. Ln. occipital (1-3 buah) •Afferent vessels : drain the occipital region of the scalp.•Efferents vessels :pass to the Ln. superior deep cervical.
Drainase Limfonodi Kepala-Leher
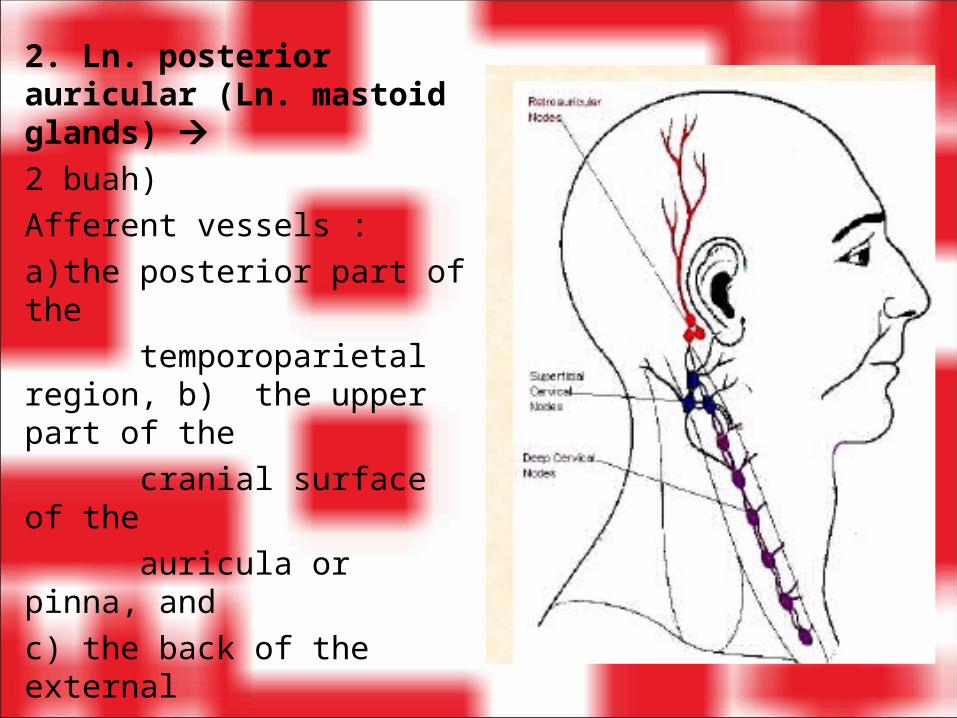
2. Ln. posterior auricular (Ln. mastoid glands) 2 buah)Afferent vessels : a)the posterior part of the temporoparietal region, b) the upper part of the cranial surface of the auricula or pinna, and c) the back of the external acoustic meatus
Efferents vessels : pass to the Ln.superior deep cervical.
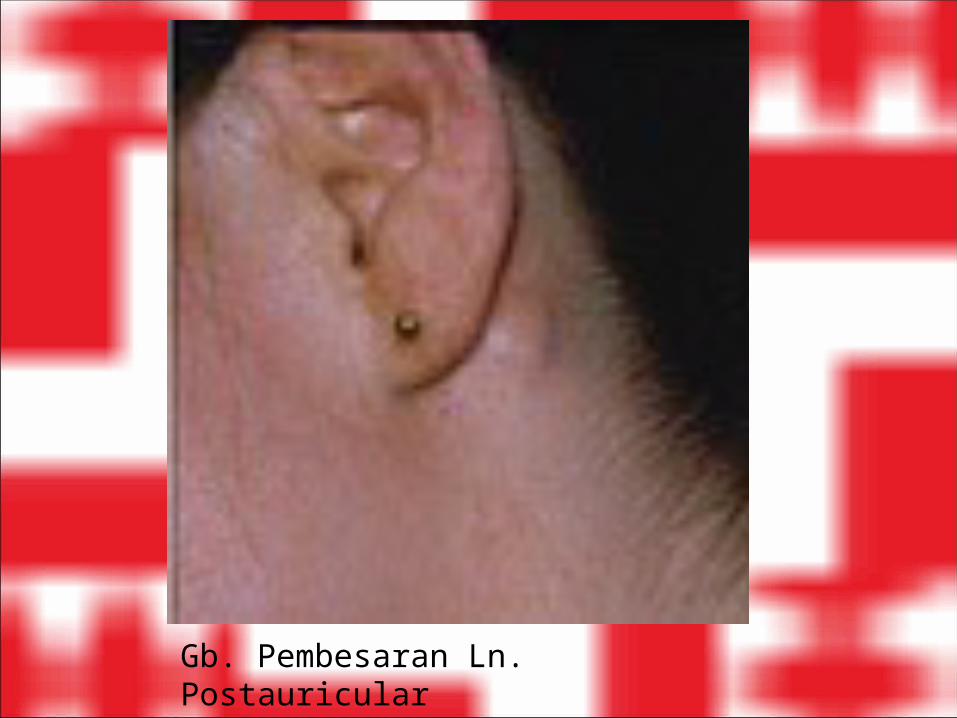
Gb. Pembesaran Ln. Postauricular
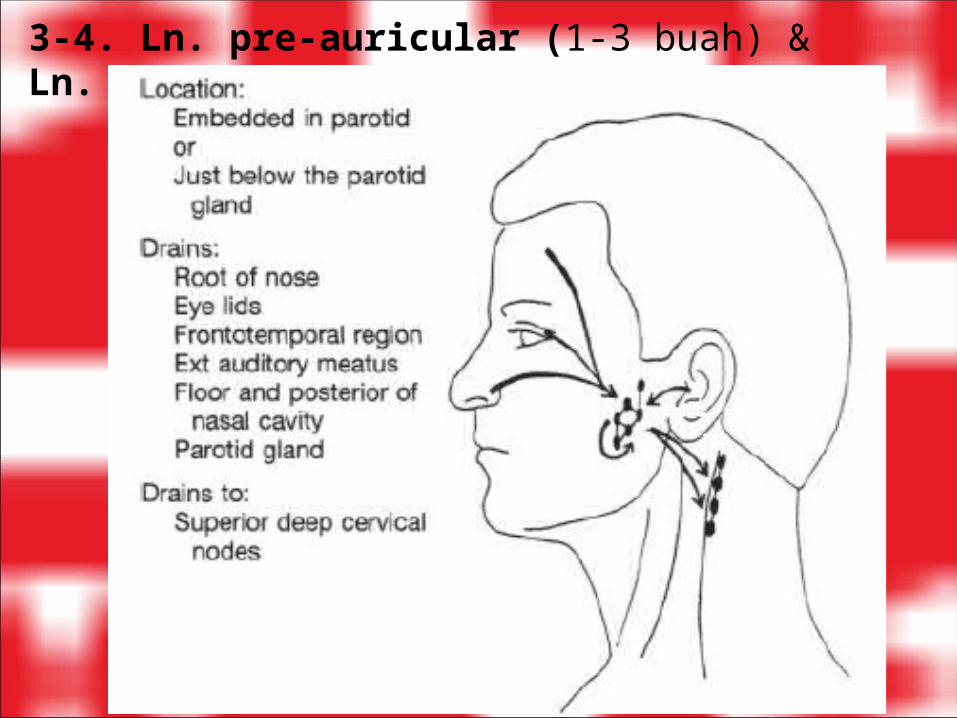
3-4. Ln. pre-auricular (1-3 buah) & Ln. Parotid

5. Ln. Submandibular (3-6 buah)

6. Ln. Submental (2-8 buah)
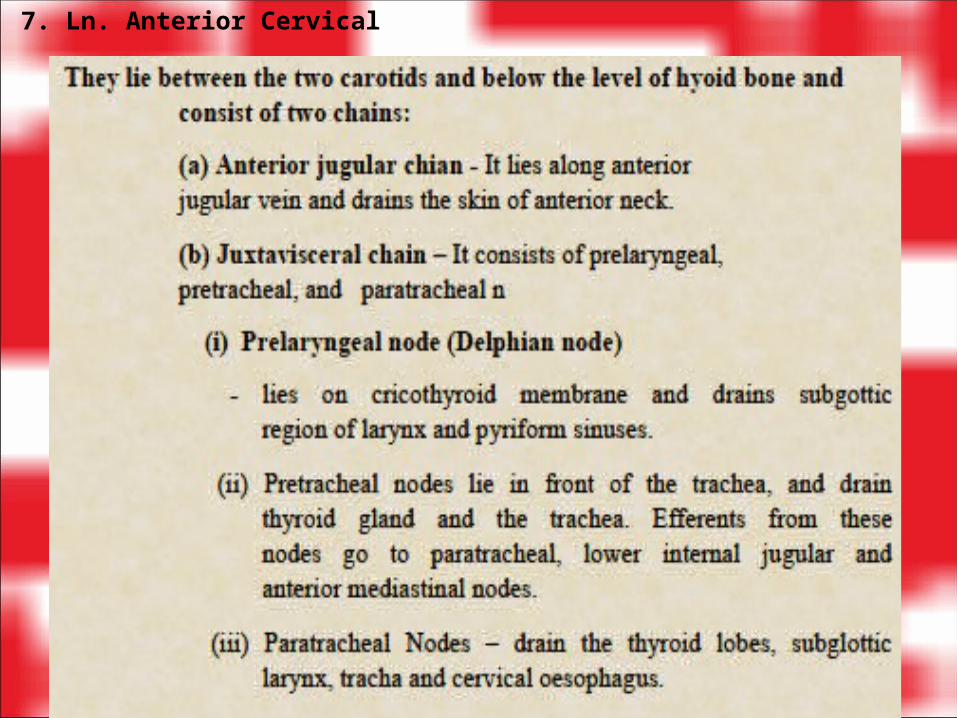
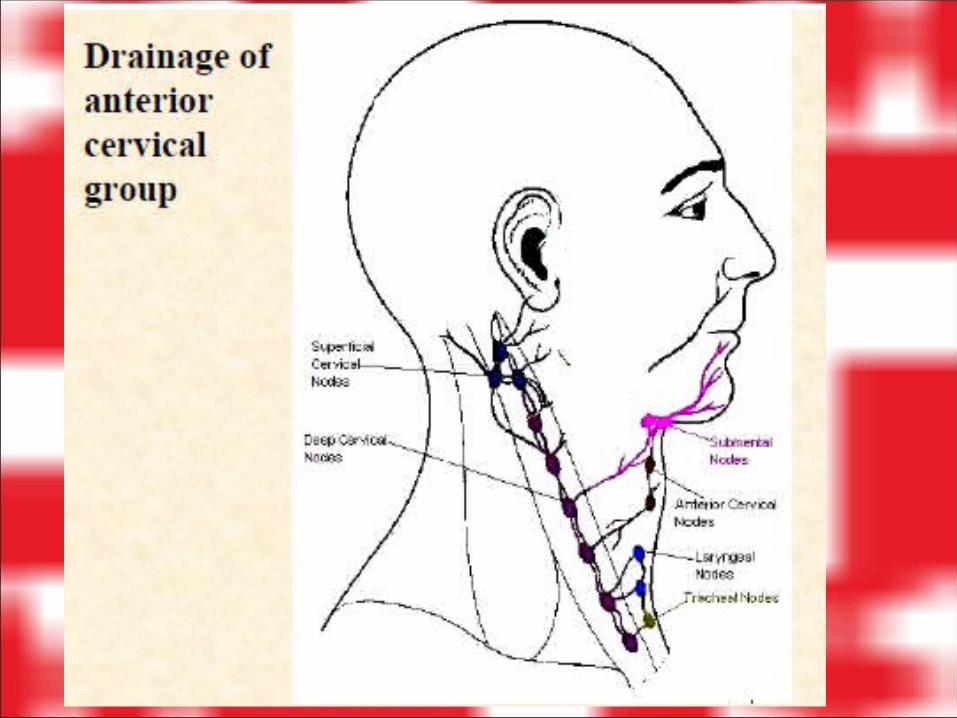
7. Ln. Anterior Cervical
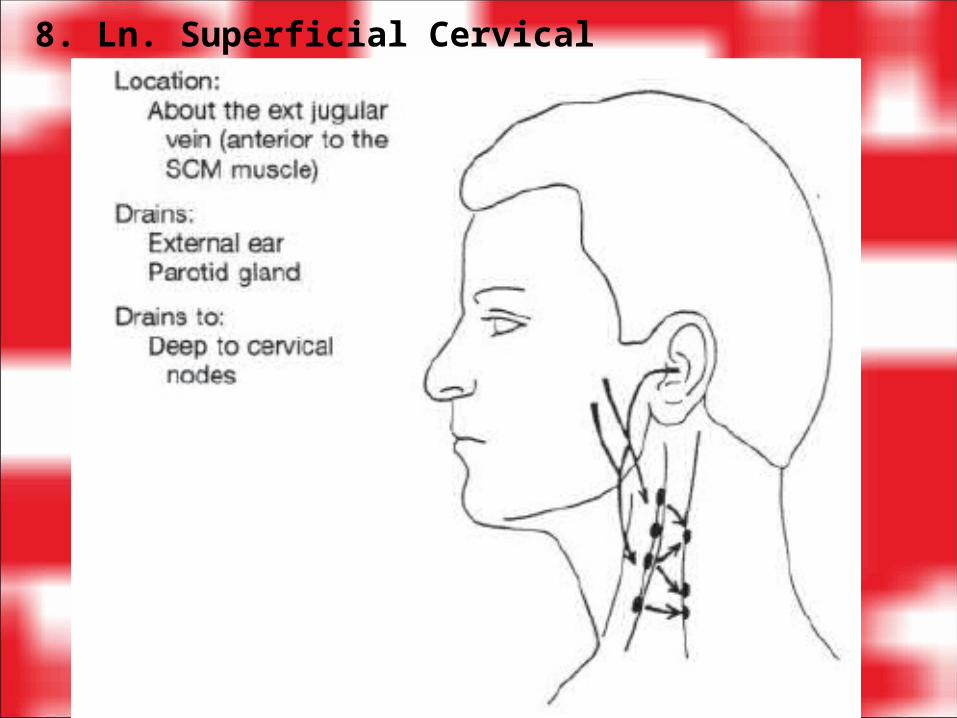
8. Ln. Superficial Cervical
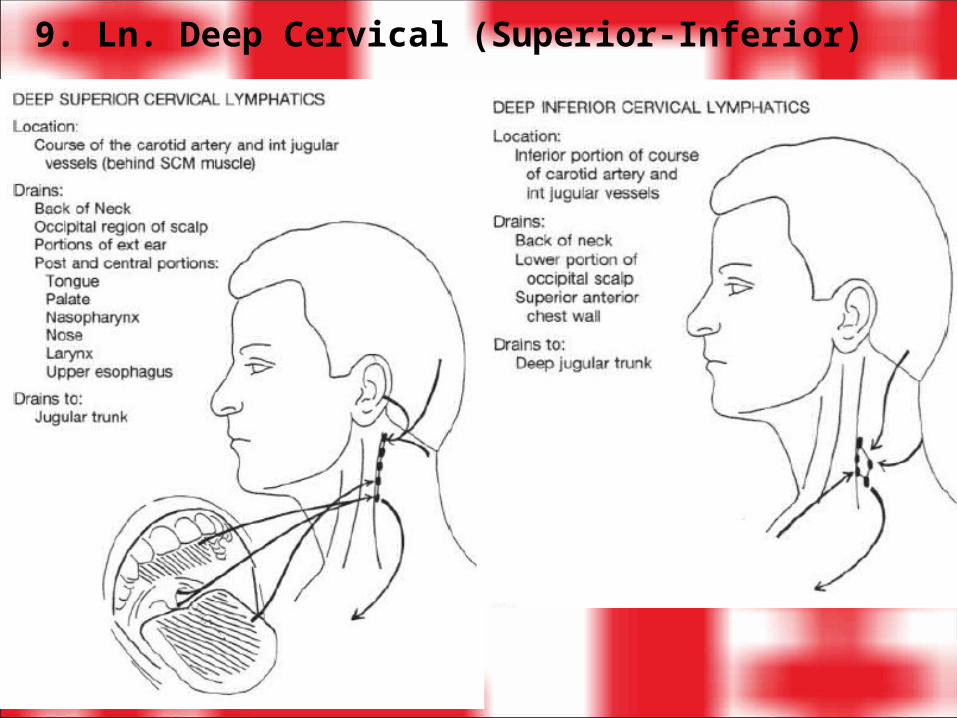
9. Ln. Deep Cervical (Superior-Inferior)
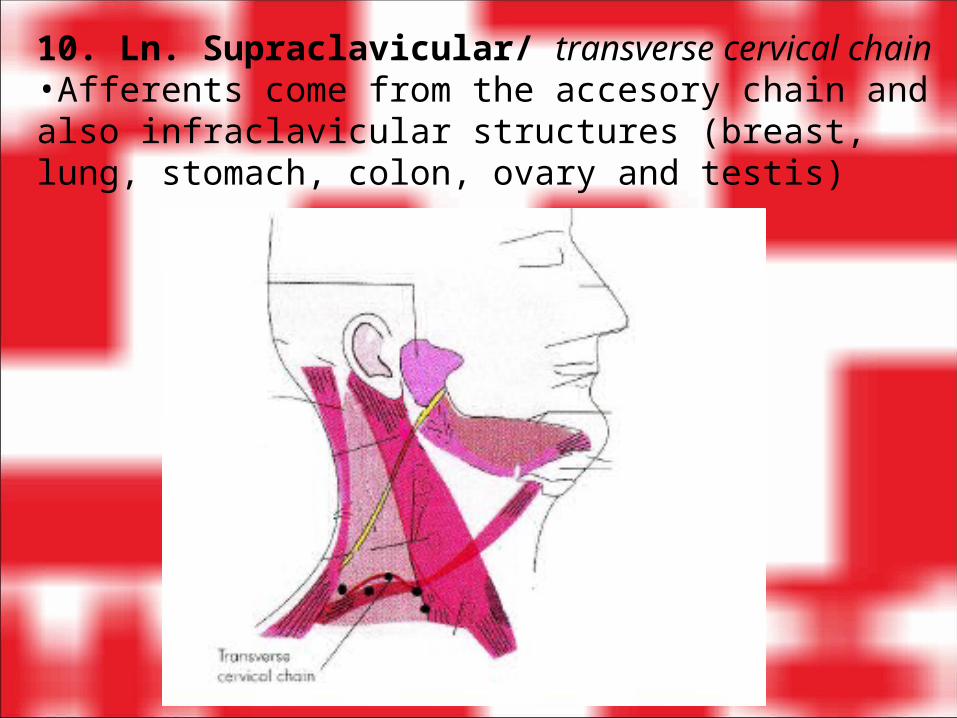
10. Ln. Supraclavicular/ transverse cervical chain•Afferents come from the accesory chain and also infraclavicular structures (breast, lung, stomach, colon, ovary and testis)
Palpasi scr sistematis limfonodi kepala leher menggunakan ujung jari telunjuk dan jari tengah.•Palpasi Limfonodi Kepala : occipital – postauricular – preaulicular – parotid – submandibular – submental •Palpasi Limfonodi Leher : anterior cervical – posterior cervical – posterior cervical deep – supraclavicular
•Catat : 1. teraba/ tidak 2. jumlah dan ukuran (single/ multiple; perkiraan diameter dlm mm) 3. tenderness (sakit / tidak sakit saat dipalpasi) 4. konsistensi (keras/ kenyal/ lunak) 5. mobilitas (bergerak/ tidak) 6. lokasi (unilateral/ bilateral)
TEKNIK PALPASI LIMFONODI

Ln. Occipital

Ln. Post Auricular

Ln. Submandibular
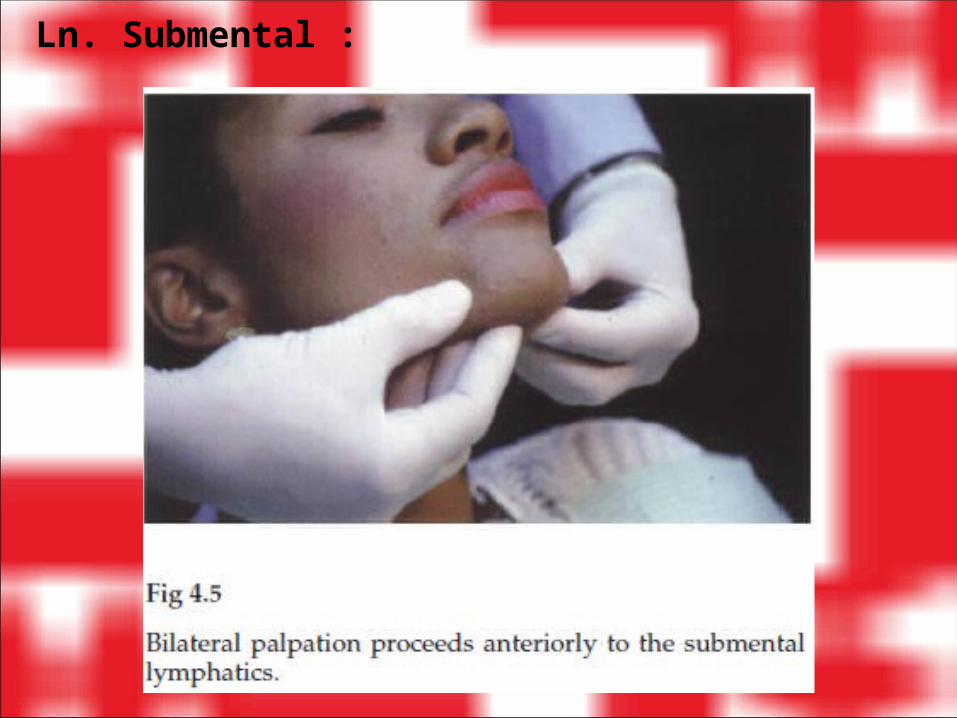
Ln. Submental :

Ln. Anterior Cervical identifikasi m.sternomastoideus terlebih dahulu.
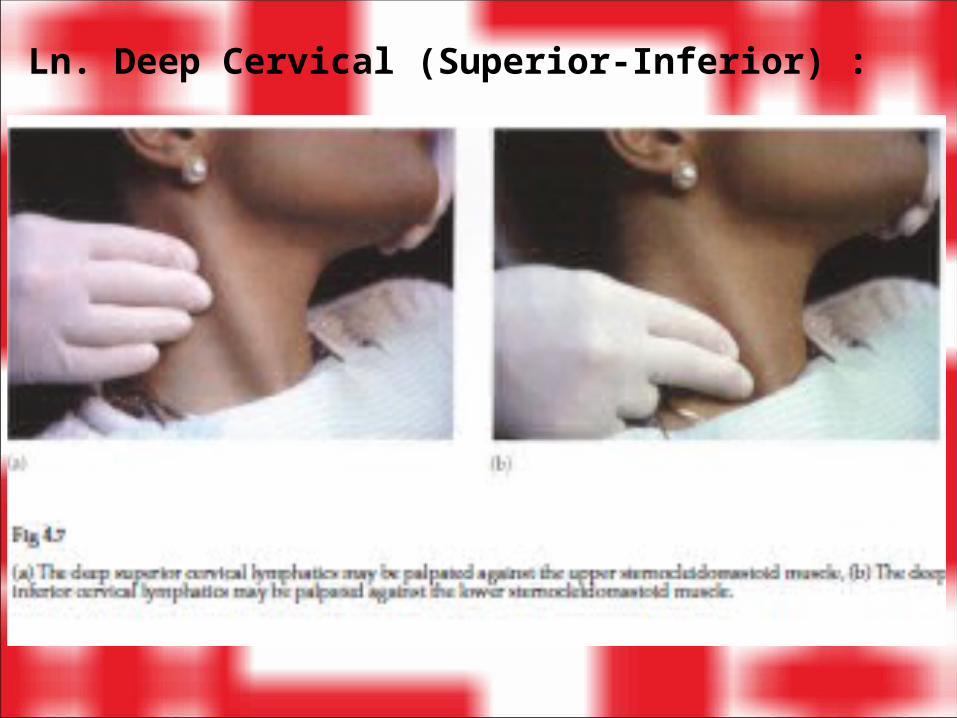
Ln. Deep Cervical (Superior-Inferior) :
American Cancer Society. American Cancer Society Guidelines for the Early Detection of Cancer. Atlanta, GA: American Cancer Society, 2006. Available at: http://www.cancer.org/docroot/PED/content/PED_2_3X_ACS_Cancer_Detection_Guidelines_3 6.asp?sitearea=PED. Accessed August 21, 2006.
Barkauskas V, Stoltenberg-Allen K, Baumann L, et al. Health and Physical Assessment, 3rd ed. St. Louis: Mosby-Year Book, 2002.
Bates B. 1995. Physical Examination and History taking 6th Edition. Philadelphia : JB LipincottCenters for Disease Control. Standard Precautions Excerpt from Guideline for Isolation Precautions
in Hospitals: Preventing T ransmission of Infectious Agents in Healthcare Settings 2007. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. Available at: http://www.cdc.gov/ncidod/dhqp/gl_isolation_standard.html. Accessed April 7, 2008.
Goodfellow L. Physical assessment: a vital nursing tool in both developing and developed countries. Cri t Care Nurs Q 1997; 20(2):6-8.
Harris R, Wilson-Barnett J, Griffiths P, et al. Patient assessment: validation of a nursing instrument. Int J Nurs Stud 1998;35: 303-313.
National Institute of Occupational Safety and Health (NIOSH). Recommendations for the Prevention of Natural Rubber Latex Al lergy. Cincinnati, OH: National Institute of Occupational Safety and Health, 1998. NIOSH Publication No. 98-113.
Pomeranz A. Physical assessment. Pediatr Cl in North Am 1998;45: xi,1.Seidel H, Ball J, Dains J, et al. Mosby's Guide to Physical Examination, 6th ed. St. Louis: Mosby-Year
Book, 2006.U.S. Department of Health and Human Services. Healthy People 2010: National Health Promotion
and Disease Prevention Objectives. Washington, DC: Public Health Services, 1999.