l situation of l maternal and newborn health - best ngo to ... · no system for assessing training...
TRANSCRIPT
l To understand the community needs, behaviors and perception for MNH Iin urban poor settings.
l To explore various factors (both demand and supply side) affecting care seeking for MNH.
l To assess the preparedness of the urban health system for providing MNH services at various levels of care in terms of infrastructures at various levels of care, HR availability and capacity, logistics, drugs & equipment, referral, recording & reporting, supervision, gove r n a n c e a n d f i n a n c i a l modalities.
Objectives of the Study
DE
MA
ND
SU
PP
LY
Conceptual Framework
Pune City Profile
Gaps in service provision – outreachl Not enough Link workers / ASHAs on ground (120/564)l AWW is the first point of contact. But, poor coordination with ICDS ~
between departmentsl Lack of uniform system for implementation of Urban Health and Nutrition Day(UHND) covering entire cityl Lack of morbidity surveillance and hence late identification and referral of maternal and neonatal morbidityl Lack of uniform system for periodic house visiting, surveillance and monitoring (not in JD of any worker) – hence no follow up
informal at grassroots without formal agreements
Gaps in service provision – utilization of public facilitiesl
l Underutilization of the Govt. schemes – JSY, JSSK, 108 servicesl Poor linkage between primary and secondary / tertiary level facilitiesl Lack of defined population coverage by Urban Primary Health Centres (UHPC)l People were unaware about which services were being provided and wherel Lack of in house diagnostic services at all levels
Under utilization of primary care and major load of MNH handled by secondary and tertiary facility
Gaps in service provision – institutional capacitiesTraining
Management capacities
l
l No dedicated training institution for the urban health and Health and Family Welfare Training Centre (HFWTC), District Training Team (DTT) utilized by rural health training
l Lack of micro planning (top-down approach) l Monitoring and review are facility based rather than population based l No quality assurance mechanisms; Indian Public Health Standards (IPHS) standards for NUHM - lost in files
No system for assessing training needs and capacity building plan
Gaps in service provision – HR, recruitment & workflowl
l No fixed salary or incentives for the outreach staffl Staff on contractual basis – no accountability l No uniformity in recruitment of ASHAs under various schemes and delayed recruitment of ASHAsl Difficulty in retention of ASHAs
Vacant scheduled posts - poor salary structure for Specialists, MOs
l
at Privatel ANC services predominantly limited to enrolment only. Concerns about package of services and qualityl Delivery predominantly in government facilities and limited to tertiary facility and few secondary facilities (undue burden
on tertiary).l Large number of mothers / newborns receive PNC visit within 24 hrs. at facility (due to more than 48 hrs. stay in facility).
However, PNC following facility discharge (home based) significantly poor. l Care seeking for sick newborn is high and predominantly from private sector.l Rationalization of specialist HR services; training on the basic maternal and newborn care are need of the hour.l All the facilities require functional linkages with the primary facilities on one hand and tertiary facilities on the other handl Need to urgently activate outreach sessions, community processes.
ANC was mainly self initiated and equal number go to public and private facilities. However, JSY incentives not available
Conclusions
Maternal and Newborn HealthSituation of
in Urban Slums of PuneKey Findings2016
3.12 million*
Slums566
SlumPopulation1.15 Mn*
(33%)
Density ofPopulation
6500 personsper sq. km.**
LiteracyRate (%)
89.6*
DecadalGrowth Rate
50.08 **
Source: *Census ’11; **City Development Plan, PMC, 2006 - 12
56
15
Existing Urban Health Infrastructure:
Source: http://populationfoundation.in/wp-content/uploads/2015/09/Pune-City-Urban-Health-Profile.pdf
Acknowledgements
This Situation Analysis was carried out by Save the Children's Saving Newborn Lives (SNL) Program in collaboration with the Pune Municipal Corporation (PMC) and the National Health Mission — Government of Maharashtra. The team extends its sincere thankfulness to the National Health Mission— Government of India for the constant encouragement and support. The team is grateful to the National Technical Advisory Group constituted under the program for its continuous inputs and guidance. Acknowledgement goes to all the study participants (recently delivered women, their families; the slum communities, and representative members and organizations; frontline workers, health care providers and staff in the public and private healthcare system; the Municipal Corporation and State Government Officials) who spared their time and enthusiastically participated in the study. The SNL Program is funded by the Bill & Melinda Gates Foundation.
For Further Information, Contact
Saving Newborn Lives, Save the Children1st & 2nd Floor, Plot No. 91, Sector 44, Gurugram- , Haryana
Phone : +91-124-4752000 E-mail: [email protected] Website: www.savethechildren.in122003

75.047.6
31.6
20.3
35.7
39.6
16.828.9
4.7
15-19 Years (64) 20-24 Years (286) 25-29 Years (187)
Study Coverage Geographical Coverage
Results
1 2 3 4 or more
Pregnancy Outcomes
l 25% of RDWs currently in their teens had already experienced multiple pregnancies
l By the age 24 yrs., over 50% RDWs have already had more than one pregnancies
l 70% of the women aged 25-29 yrs. had experienced more than 2 pregnancies
Number of Pregnancy by Age
Once Twice Three & more
N=601
Antenatal Care (ANC) Registration & Services
l A b o u t 6 5 % w o m e n received first ANC before
th4 month
l 15% received first ANC th
session as late as in the 9 month
Place of Ante-natal Examinations
Awareness of Danger Signs in Pregnancy
l
headache and oedema of face/ hands/ legs, most cited symptoms of danger signs
l In case of any danger signs during pregnancy, around one- third would consult a private sector facility
Severe abdominal pain,
N=601
N=601
0%
40%
50%
30%
20%
10%
03 Public Facility
02 Public Facility
01 Public Facility
FrontlineWorkers
Pvt. Hospital
Pvt. Doctor
Others(e.g, LocalProvider)
NotRegisteredAnywhere
21.0
31.1
0.5 1.2
44.1
24.0
5.42.2
N = 601
N = 601
l Pregnancies were frequently registered with Private Hospitals (44%)
l Only 1.7% women registered e i t he r w i th f ron t l i ne workers or at primary health facilities
0%
20%
40%
60%

Immediate Newborn Care
MedicalCollege Hospital
TertiaryHospital
MaternityHome/UFWC
Dispensary/UHP
PrivateHospital/
Clinic
NGO/ TrustHospital
At Home(Visit by doctor/other health care
provider)
Other
Place of Delivery
l Majority of deliveries conducted in private hospital and tertiary care public facilities.
l Those who have not delivered in the govt facilities, cited ‘poor quality of service’, and ‘husband/ family didn’t allow’ as the main reasons.
l Only 10% availed any govt. vehicle for delivery.
l Around 30% deliveries are C-section deliveries ~ Govt.: 20% and Pvt.: 40%
Self Reported Complications During Delivery
l
delivery complications referred to a higher up facility
l 62% of the RDWs never landed up in the referral facility they were referred to, cited it was unnecessary to visit the referred facility
41% of RDWs who had
N=601
l Less than 2.5 kg – 20%
l Huge amount of clustering at 2.5 kg implicating that the recording was 2.5 kg irrespective of their actual weight.
Birth weight recorded
No. of Children
Act
ual W
eig
ht
of
Ch
ild
(K
gs.
)
N= 586
Pre-discharge Counseling
l
signs or critical aspects of newborn care
l Limited discussion of family planning (need or methods)
l The three most popular topics were breast feeding, nutrition and routine immunization
Little discussion on danger
0%10%20%30%40%50%60%70%80%90%
100%
Imm
unis
atio
n
Nut
ritio
us fo
odfo
r M
othe
r
Bre
ast F
eedi
ng
Kee
p B
aby
War
mno
t STS
or
KM
C
Del
ayed
Bat
hing
Um
bilic
al C
ord
Car
e
Ski
n to
Ski
n/
Kan
garo
o M
etho
d
Dan
ger
Sig
ns/
Sym
ptom
s fo
rN
ew B
orn
Bir
th C
ontr
ol/
Fam
ily P
lann
ing
Dan
ger
Sig
ns/
Sym
ptom
s fo
rM
othe
r
88.5 88.0 83.9
63.455.9
46.135.6 35.4 33.3
25.8
N= 586
l Registration of pregnancy usually in the first trimester, but actual ANC starts in the second trimester
l ANC services at outreach almost non-existent; Uptake of ANC was mostly self-initiated
l ANC counselling was reportedly mostly on early initiation of breast feeding and regarding financial preparation
l Awareness on danger signs and pregnancy complications was poor amongst pregnant women
Gaps with respect to Antenatal Care
0%
20%
40%
60%
80%
100%
Baby cried/ breathedeasily immediately
after birth
Baby wiped (dried) as soon as it was born
Breast feeding within1 hour of birth
Something applied to thecord immediately after
cutting
99%
76%
30%
53%
N= 586
l High out of pocket expenditure in private sector deliveries.l Little or no awareness about the entitlement based services (JSY, JSSK), hence, poor
uptake of the same.l Role of health workers was minimal - rarely sought at the time of delivery. l Referral compliance for complications during labour was poor.l Only 30% initiated breast feeding within first hour of child birth.
Gaps with respect to Delivery Services
N=601
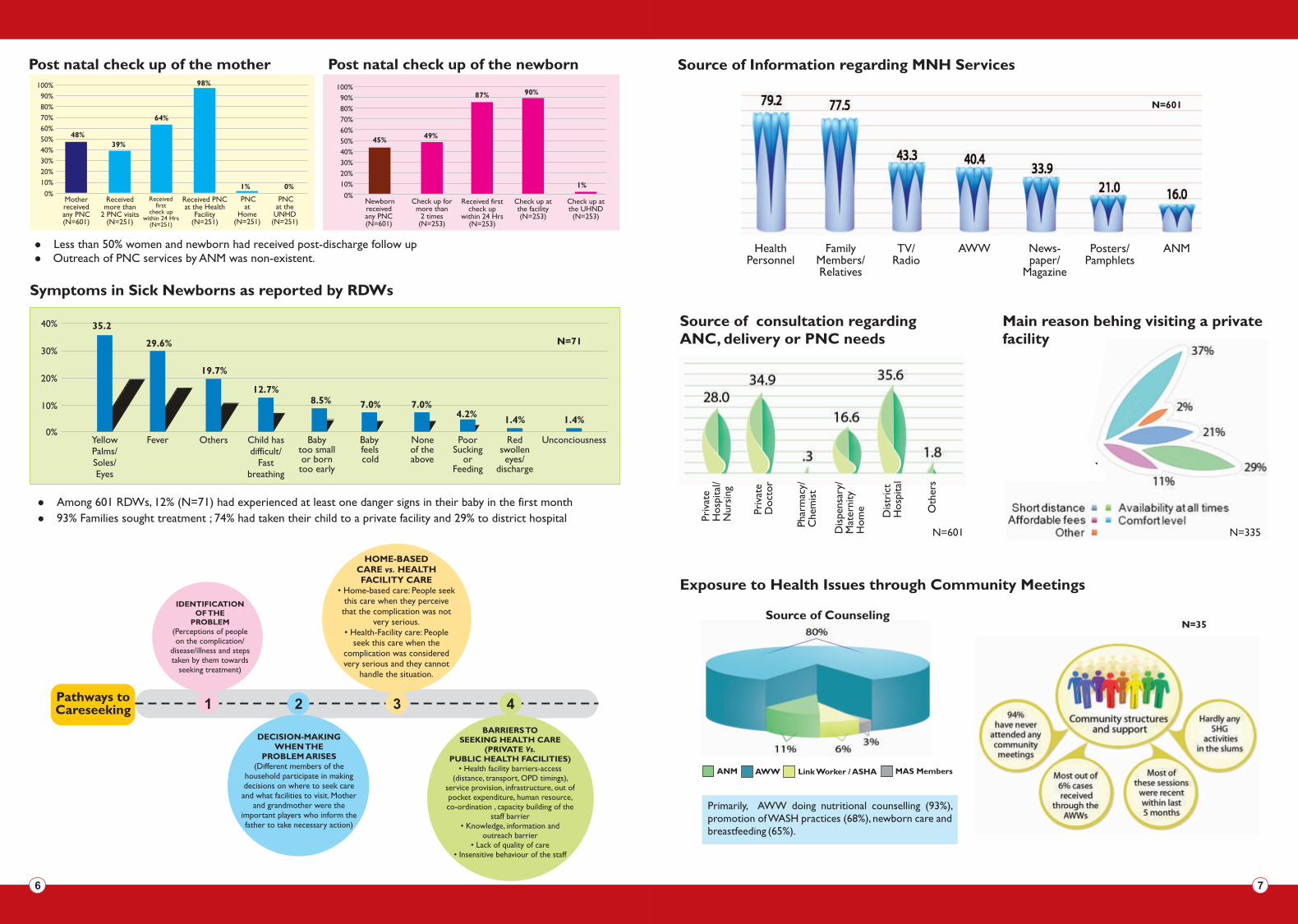
Exposure to Health Issues through Community Meetings
Source of Counseling
ANM MAS MembersAWW Link Worker / ASHA
Post natal check up of the mother Post natal check up of the newborn
l
l Outreach of PNC services by ANM was non-existent.Less than 50% women and newborn had received post-discharge follow up
Source of consultation regardingANC, delivery or PNC needs
Pri
vate
H
osp
ital
/N
ursi
ng
Pri
vate
Doct
or
Pha
rmac
y/C
hem
ist
Dis
pens
ary/
M
ater
nity
Hom
e
Dis
tric
tH
osp
ital
Oth
ers
N=601
Main reason behing visiting a private facility
N=335
Source of Information regarding MNH Services
HealthPersonnel
FamilyMembers/Relatives
AWWTV/Radio
News-paper/
Magazine
Posters/Pamphlets
ANM
N=601
Motherreceived any PNC(N=601)
Received more than
2 PNC visits (N=251)
Received first
check upwithin 24 Hrs
(N=251)
Received PNCat the Health
Facility(N=251)
PNCat the
UNHD(N=251)
PNCat
Home(N=251)
0%
90%
100%
80%
70%
60%
50%
40%
30%
20%
10%
48%
39%
64%
98%
1% 0%
Newbornreceivedany PNC(N=601)
Check up for more than
2 times(N=253)
Received firstcheck up
within 24 Hrs(N=253)
Check up atthe facility(N=253)
Check up atthe UHND(N=253)
0%
90%
100%
80%
70%
60%
50%
40%
30%
20%
10%
45%49%
87% 90%
1%
0%
10%
20%
30%
40% 35.2
29.6%
19.7%
12.7%8.5% 7.0%
4.2%1.4%
N=71
OthersFever Poor Sucking
or Feeding
Yellow Palms/Soles/ Eyes
Child has difficult/
Fast breathing
Baby too smallor born too early
Baby feels cold
Red swollen eyes/
discharge
Unconciousness
7.0%
1.4%
None of the above
Pathways to Careseeking 1 2 3 4
Symptoms in Sick Newborns as reported by RDWs
l
l 93% Families sought treatment ; 74% had taken their child to a private facility and 29% to district hospital
Among 601 RDWs, 12% (N=71) had experienced at least one danger signs in their baby in the first month
N=35
Primarily, AWW doing nutritional counselling (93%), promotion of WASH practices (68%), newborn care and breastfeeding (65%).