krzywosinski pbls
DESCRIPTION
bTRANSCRIPT

TARIN KRZYWOSINSKIGroup B
PBL Session #1
Case 1
SUBJECTIVE20 y/o male PTC with a non-radiating, throbbing pain and tingling in his right ankle. Pt also states that his R knee is painful at the lateral aspect. Pt describes the pain as constant and rates it an 8/10. The pain has been present for 6 months and is getting worse. Pt states that he has tried wearing Spenco arch supports and softer soled shoes but neither has helped. Pt states that Tylenol also does not relieve the pain. Pt states that walking and rollerblading makes the pain worse.
Allergies: Penicillin: gets itching and a rash Medications: 3 units of regular insulin in the AMDiagnosed Diseases: uncontrolled DM type 1, diagnosed 3 years agoChildhood Disease: noneImmunizations: UTDSurgical History/Hospitalizations: none Social History: Pt denies smoking and illicit drug use. Pt states he is a social drinker and has 3 beers on the weekends. Pt states he is single. Pt denies being employed and states he lives with one of his parents.Family History: Dad died at age 50 of DM complications and alcohol abuse. Mom is alive and has uncontrolled HTN. ROS: Pt denies weight loss, N/V/D, fatigue, changes in vision or hearing, sore throat, headaches, rashes, SOB, chest pain, murmurs, changes in urination, abdominal discomfort, muscle weakness, mood changes. Overall the review of systems is unremarkable.
OBJECTIVEVitals: Ht: 6’2”; W: 185 lbs; other vital signs are normalGeneral: AOx3Integument: HPK on 2nd met head at the plantar aspect, bil. Hair to the level of the digits. Nails are normal thickness and color digits 1-5, bil. Vascular: DP/ PT pulses 2/4, bil. No varicosities noted. Mild edema at the medial aspect of the R ankle. Erythema noted medial to the TNJ, right. No varicosities noted.Neurological: sharp/dull and proprioception intact, bil. SWMF and vibratory sense diminished, bil. Achilles and patellar reflexes 2/4, bil.MSK/Gait: Hammer digits 4-5, bil. Muscle Strength 5/5 for all muscle groups but weakness at the Tibialis Posterior, R. POP noted along the navicular and cuneiform joint, at the medial aspect of the ankle, and at the peroneal tendons, bil. Pain during passive inversion. Negative heel raise test. Biomechanical Exam:
Angle of gait: R: 24 abducted, L: 12 abductedLimb length: L: hip tilted, superior to R hip = L superior static pelvic tiltHip: R: Knee Extended: 20 int/23 ext, L: 21 int/24 ext
Knee Flexed: R: 24 int/26 ext, L: 24 int/28 extMalleoli: R: 13 ext, L: 15 extSTJ ROM R: 0 in/6 ev; L: 20 inv, 10 ev = limited ROM on R
STJNP, R: 4 valgusSTJNP, L: 0
MTJ: R: 4 inv; L: 6 evAnkle DF: KE 5 and KF 10, bil1st Ray: 5 DF and 5 PF, bil1st MTP: R: unloaded 55, loaded 30; L: 60 unloaded, 32 loadedTI: R: 0, L: 0
NCSP:

R: 4 valgus + 0 = 4 valgusL: 0 + 0 = 0 degrees
Max Pronation:R: 6 everted + 0 = 6 evertedL: 10 everted + 0 = 10 everted
RCSPR: 4 valgus, fully compensatedL: 6 varus, fully compensated
Labs/X-rays:Harris & Beath Projection, bil: open middle and posterior STJ on L, narrowed middle and closed posterior STJ facets on R consistent with posterior STJ coalition
Lateral Projection of the Foot, bil: halo sign, talar beaking, rounding of lateral talar process and noted osseous fusion of posterior STJ consistent with coaltion. Flat foot noted with decreased calcaneal inclination angle consistent with pes planus, bil.
DP Foot Projection, bil: HAV, bil but more pronounced on the LLateral Oblique Ankle Projection, bil: L: talar dome is intact.
ASSESSEMENT1. STJ Coalition of the posterior facet, R2. Structural Hallux Limitus, bil3. HAV, bil.4. HDS 4-5, bil5. Gastrocnemius equinus, bil
Other Possible Differentials:1. PTTD2. OCD3. Tarsal Tunnel Syndrome4. Peroneal Spastic Flatfoot5. Lateral Ankle Sprain
PLANPerformed focused podiatric H&P. Discussed conservative Tx options with pt. Instructed pt to RICE the area and immobilize his foot as much as possible. Prescribed Naproxen 600 mg q 6 hrs and accommodative orthoses for the pt and instructed him to wear his orthoses in his shoes. If pain persists and conservative Tx fails, discussed the possibility of STJ arthrodesis. Pt RTC in 2 weeks.
Orthotic Prescription: cast pt pronated, because can’t get the pt to neutral

NOTES:
Case 2SUBJECTIVE30 y/o African American male PTC complaining of pain on the bottom of his left arch and heel. Pt states that the problem started 2 months ago when he started training for the Chicago Marathon. Pt states pain reaches a 6 or 7/10 on the pain scale. Pt states that the pain is worse after standing for a long period of time and after running long distances. Pt states his normal routine is 3 miles 3 times a week. Pt states he has tried new running shoes but that has not seem to help. Pt states nothing seems to make it better. Pt states he has not had this problem before.
Allergies: Nickel and Chrome gives him a rashMedications: Prednisone 10 mg for 3 monthsDiagnosed Diseases: Sickle Cell Anemia, Sarcoidosis diagnosed 1 year ago, Gouty Arthritis Childhood Disease: unknownImmunizations: Pt states they are UTDSurgical History/Hospitalizations: Hospitalized for a Sickle Cell Anemia Attack 4 years agoSocial History: Pt works as a ticket agent for American Airlines. Pt denies smoking and illicit drug use but drinks alcohol socially. Pt states he lives alone.Family History: Brother- Juvenile Rheumatoid Arthritis, Father- flat feet, was discharge from the military. Mother- + for sickle cell trait. ROS: Pt denies any weight gain, respiratory changes, neurological manifestations, or GI issues. Positive findings associated with his systemic diseases.
OBJECTIVEVitals: unremarkableGeneral: well nourished, cooperative male, AOx3 in moderate distressIntegument: Diffuse callus noted at the plantar aspect of met heads 3-5, bil. Hair to the level of the digits, bil. Skin is warm, bil. Vascular: DP and PT 2/4, bil. Mild edema, erythema noted at the plantar medial heel, left.Neurological: Intact sharp/dull and proprioception bil. Patellar and Achilles reflexes 2/4, bil. MSK/Gait: POP at the plantar and medial aspect of the left heel. No pain is present with AJ ROM. Muscle strength 5/5 in all muscle groups, bil. Contracted digits 4-5, bil with mild varus rotation of the 5th toe, bil.Biomechanical Exam:Limb length:
True R: 87.5 cm, L: 88.5 cmApparent R: 97.5 cm, L: 98 cm
Hip: 45/45 int/ext, bilKnee: genu valgumMalleoli: 15 ext R, 18 ext LSTJ R 16 inv/6 ev; L: 26 in/6 ev
STJNP: 4 inv, bilMTJ: 3 inv, bilAnkle DF: 5 KE, 10 KF, bil1st ray R: 5 mm DF, 3 mm PF; L: 5 mm DF, 5 mm PF1st MTP: R: 50 DF unloaded /25 PF; L: 50 DF/25 PFTibial Influence 4 inv, bilNCSP:
R: 4 varus + 4 varus = 8 varusL: 4 varus + 4 varus = 8 varus
Max Pronated:R: 6 everted + 4 inverted = 2 evertedL: 6 everted + 4 inverted = 2 everted
RCSP:R: 2 valgus, partially compensated with the FF 1 degree still off the floorL: 2 valgus, partially compensated with the FF 1 degree still off the floor

X-ray: lateral foot: osteoporosis, increased trabecular pattern in the calcaneus, heel spur, left
ASSESSEMENT1. Paget’s Disease2. Pathologic Calcaneal Fracture, left2. Combined Partially Compensated Limb Length Discrepancy, R limb shorter3. Gastrocnemius Equinus, bil4. Structural Hallux Limitus, bil
Other possible Diagnoses:1. Plantar Fasciitis, L 2. AVN of the Calcaneus, L3. Medullary Infarct of Calcaneus, L4. Osteitis of Garre of Calcaneus, L5. PTTD, L
PLANPerformed a focus podiatric H & P. Discussed possible treatment options with patient. Ordered serum alkaline phosphatase and ESR labs. Recommended to pt to RICE and stop running at this time. Prescribed Ibuprofen 800 mg 1 tab PO q6h and Alendronate 40 mg QD 30 min before meals for 6 months. Also prescribed orthoses for the pt. Pt is to RTC in 2 weeks for f/u.
Orthosis prescription: functional, cast pt in neutral, post to RF deformity (because really not much deformity in the forefoot), extrinsic post and intrinsic post combo so not so much into the foot, Kirby skive: 1mm=2 degrees**** 4 mm Kirby=8 degree post (intrinsic post) and a 3 degree FF post to keep the STJ in neutral after heel liftMedical management: Paget’s aka Osteitis Deformans, phalens test: evert the foot and try to put pressure on the medial side of the foot (to r/o baxter’s nerve entrapment), watch for hat or shoe size changes, other bisphonate risondronate (Ectanol). Know the phases of paget’s for the EXAM, males greater than females, continually monitor because it can become malignant osteosarcoma. Know the drug etindronate


Case 3SUBJECTIVE25 y/o male PTC complaining of a sharp and nagging heel pain. Pt states it is located at the medial and lateral plantar aspects of the L heel. Pt states that the pain fluctuates but has been constant since he had reconstructive surgery for his flat left foot 6 months ago. Pt states that standing or walking for a long period of time makes the pain worse. Pt states he was referred here to get orthotics by the surgeon who performed the reconstructive surgery. Pt states that the surgeon who performed the surgery was a podiatrist.
Allergies: NKDAMedications: deniesDiagnosed Diseases: deniesChildhood Disease: deniesImmunizations: UTDSurgical History/Hospitalizations: deniesSocial History: Pt states he is unemployed and denies tobacco, alcohol, or illicit drug use. Pt states that he exercises on a regular basis in his gym shoes that very worn out and over two years old.Family History: Non-contributoryROS: Pt denies weight loss, headaches, N/V. EENT: Pt states he wears glasses MSK: Pt states he has arthritis in his L shoulder, ankle, and thumb.
OBJECTIVEVitals: T: 97.9 F, RR: 18 bpm; Pulse: 78 bpm; BP: 145/88 mmHg; Height: 6’0”, W: 380 lbs.General: cooperative, obese, and euthymic, AOx3, alert in moderate distressIntegument: Diffuse HPK sub 1st and 5th met heads, R. Diffuse plantar medial heel, bil, pinpoint nucleated planter posterior heel, L. Surgical scars dorsal medial ankle, left. 3cm lateral calcaneus, L.Vascular: PT, DP 1/4, bil. CFT<3 sec all digits, bil. Minimal non-pitting edema noted at L ankle. Neurological: proprioception, vibratory, and sharp/dull intact, bil.MSK/Gait: decreased medial arch, bil L>R. POP at medial and lateral aspect of L heel. Prominent styloid process bil. Pain at anterior aspect of L ankle with ankle DF. Gait: apropulsive with adductory twist, L foot with decreased angle of gait, bil. Marked pronation with everted calcaneus, bil. 1st MTPJ and IPJ plantarflexed during midstance, L.
Biomechanical Exam:Postural: unable to evaluateHip Joint: deferred due to sizeKnee: marked abduction of tibia on femur, bilMalleolar:13 ext, bilSTJ R: 3 inv/0ev; L: 8 in/0ev
STJNP: R: 4 inv; L: 2 invMidtarsal Joint: R: 10 inv, L: 12 inv
Ankle R: -4 KE, -4 KF; L: 4 KE, 5 KF1st ray: 2mm DP, 5 mm PF, bil1st MTP: unloaded R: 28 R; L: 25 LTI : R: 4 ev; L:6 ev
NSCP:R: 4 inverted + 4 everted = 0L: 2 inverted + 6 everted = 4 valgus
Max Pronated:R: 0 eversion + 4 everted = 4 valgusL: 0 eversion + 6 everted = 6 valgus
RCSP:R: 4 valgus, partially compensated with FF still off the floor 6 degreesL: 6 valgus, partially compensated with FF still off the floor 10 degrees

Xrays:AP, bil. Nonunion of 1st cuneonavicular arthrodesis, L. Increased metatarsus adductus angle, L>R. Decreased joint space of 1st MTPJ, L. Lateral foot, bil: talonaviuclar fusion, L. Healed osteotomy of calcaneus indicated by sclerotic line, L. Screw backing out of the posterior calcaneus, L
ASSESSEMENT1. Metatarsus Adductus, bil2. 1. Nonunion of cuneionavicular fusion, L3. FF Supinatus, bil4. DJD 1st MTP, L. 5. Gastro-soleal equinus, bil.6. Genu Valgum7. Plantarflexed 1st ray, bil8. Structural hallux limitus, bil
Other differentials:1. Tarsal Tunnel2. CRPS2. DJD Secondary to surgery3. Tendinitis4. Plantar Fasciitis 5. Pes Planus
PLANPerformed a focused podiatric H & P. Discussed treatment option with patient on how to conservatively address the patient’s chief complaint. Refer pt back to surgeon for further assessment to address metatarsus adductus. Prescribed the pt a CAM boot to offload the L foot and debrided the nucleated lesion on the posterior heel, left. Informed the pt that once metatarsus adductus is addressed by his surgeon and his screw in his heel is removed, he should come back for casting of orthoses. Referred the pt to a local nutritionist to provide him with dietary modifications to assist him in losing weight. Pt to RTC in 2 weeks for f/u.
NOTES: FUNCTIONALS WILL NOT WORK FOR THIS PT. Accommodative casted pronated.
Orthotic: accommodative pronated device, partial WB, take the screw out and ***KNOW THE PROCEDURES for this deformity (surgery), HHS (<3 y/o), osseous procedures for this (fowler) Berman-Gartland, Lepird, McCormick and blount, staytler and VanDerWalt, Peabody and Muro, Johnson, Cotton, Koutsigiannas
Medical Management: shortened the medial column and lengthened the lateral column, by fusing it you’re taking away the pronation the pt needed to compensate, so he is going to continue to pronate through it and cause a non-union, want him to lose weight before you do another surgery, sent him to a nutrionist, Sx failed because he had met adductus that wasn’t addressed, he was overweight, he has equinus, surgeon picked a procedure that took away his means of compensating for the deformity, consider FF supinatus with a FF varus of equal to or greater than 8.
For this pt, accommodative casted pronated would have worked best. With orthoses, this pt achieved an 80% reduction in pain, the only thing causing him pain still was the screw backing out.


Case 4SUBJECTIVE44 y/o African American female PTC for f/u of an ulcer on her L foot. Pt states the ulcer is located underneath her big toe. Pt states she has had the ulcer for 10 months and it hasn’t gotten worse to her knowledge. The ulcer does not cause her any pain or discomfort. She was previously treated for the ulcer with casting, surgical shoes, debridement, and antibiotics. Pt states the ulcer had healed but now it is back again.
Allergies: NKDAMedications: NPH 30 units QDDiagnosed Diseases: DM Type 2 for 4 years Childhood Disease: deniesImmunizations: UTDSurgical History/Hospitalizations: deniesSocial History: Pt states she is a PE teacher and coaches extracurricular sports. Pt states she works out with the team. Pt relates to being single, has no children, and lives alone. Denies tobacco, alcohol, and illicit drug use. Family History: noncontributory ROS: Pt denies weight loss, fatigue, headaches, vision changes, hearing problems, SOB, palpitations, and diarrhea.
OBJECTIVEVitals: stable; Accucheck: 148 mg/dl 2 hours post-prandialGeneral: AOx3, NADIntegument: no HPKs noted. Plantar proximal L hallux Wagner Grade 2 ulcer, 1 cmx1cmx0.2cm. Beefy red granulation tissue with mild odor, hyperkaratotic border, and mild serous drainage from the wound. No tissue necrosis noted.Vascular: DP, PT palpable, bil. CFT< 2 sec in all digits. No varicosities noted. Slight edema at the L hallux. Neurological: SWMF 6/10, L and 8/10, R. Proprioception intact. Decreased sharp/dull and vibratory intact to the level of the midfoot, bil. MSK/Gait: Severely pronated, bil. Digits 2-5 contracted at PIPJ, bil. No POP or with ROM in all pedal joints, bil. Biomechanical Exam:
Angle of gait: R: 15 abd, L: 18 abdBase of gait: 3 inch, bilContact & propulsive phases decreased and midstance increased. IP joint was symmetrical, bil.Malleoli: 18 ext bilSTJ: R: 20 inv/8 ev, R, 2 inv NP; L 18 inv/7 ev NP 2 inv L
STJNP: R: 2 varus; L: 2 varusMidtarsal: R: 2 inv, L: 4 invAnkle DF: KE 0, KF 2, bil1st ray R: 5 mm PF and DF; L 6 mm DF, 4 mm PF1st MPJ: R 50 NWB, 34 WB; L 34 NWB, 20 WBTibial Influence 2 inv, bil
NCSP: R: 2 inverted + 2 inverted = 4 varusL: 2 inverted + 2 inverted = 4 varus
Max pronated:R: 2 inverted + 8 everted = 6 evertedL: 7 everted + 2 inverted = 5 everted
RCSP:R: 2 varus, fully compensatedL: 4 varus, partially compensated with the FF still 3 degrees off the ground
X-rayLateral Projection foot, bil: Pes Valgus, bil. Decreased area of density noted at the distal phalanx of the hallux consistent with an MTJ fault and arthritis
ASSESSEMENT

1. Wagner Grade 2 ulcer, L hallux2. Structural Hallux Limitus, bil3. Gastrosoleal Equinus, bil
Differentials:1. Pes Planus1. Structural Hallux Limitus2. OM, L hallux3. Charcot
PLANDiscussed treatment options with pt. Debrided ulcer on L hallux and applied Silvercell to the area. Applied an Unna boot to the patients left leg to relieve pressure around the ulceration. Pt RTC for f/u in 1 week. Prescription for orthoses will be given after the ulcer heals for long term care.
Orthotic: accommodative cast PWB, shoes- toe rocker or FF rocker, do NOT do a sweet spot because will actually cause more sheer forces on the area (digits are just too hard to control)Medical management: VIPs of wound care, cardinal signs of infection debridement, wound care products (silver product, regranix- PDF in a gel form) Shimmy shoe- shoe with a metatarsal bar that can be moved or adjusted. Toe rocker shoe modification, check albumin to see if tissue will heal (normal 3.5-5), Total contact cast, instant total contact castKnow Wagner classification; would be grade 2, colonized but not infectedNeed growth factors and vascularity in order for granulation tissue to form, can be inhibited by MMPs; debride and irrigate in order to remove some of the MMPs, may also consider products such as silvadene, isosorb, calcium alginate with silver, restore ag, acticoat (can stay on for up to 3 days; acitcoat 7 lasts 7 days), silverlon (nylon interwoven with silver, very expensive), prisma (promogran is the version w/o silver), hydroferro blue (non-silver product, very effective against MMPs, acts like sponge to remove exudate, kept on for 2-3 days, if it turns from blue to white, then it needs to be removed), granX (contains only 1 growth factor, must be kept refrigerated), Accuzyme & Panafil (both removed from the market but were very effectiveBio-engineered substrates: Dermagraft, Apligraft, Graft jacket (cadaveric tissue), Oasis; (Procine and bovine products, need to watch out for allergies and religions that don’t use pork), Medahoney (leptosporine bees honey, remove the spores, it’s pro-granulation substance and inhibits bacterial growth)


Case 5: SUBJECTIVE47 y/o female PTC with pain on her medial left ankle. Pt is unsure of when it started but states it is a constant pain that has gradually been getting worse over the last few months. Pt states when the pain is the worst it is a 5/10. Pt states she is having difficulty walking at the end of the day after her daily aerobics class. Pt states she has tried taking Advil and has changed her shoes. Pt states her PCP referred her to your office.
Allergies: NKDAMedications: Norvasc 5 mg, Metformin 500 mg QDDiagnosed Diseases: DM 2 for 5 years, HTNChildhood Disease: deniesImmunizations: UTDSurgical History/Hospitalizations: deniesSocial History: Pt states she is a lawyer and teaches aerobics twice a week. Pt relates to having 3 glasses of wine a week but denies use of tobacco. Pt states she lives by herself.Family History: Mom has RA, Father died of a heart attack. ROS: Pt denies fatigue, weight loss/gain. ROS is unremarkable other than DM and HTN.
OBJECTIVEVitals: stable, non-contributory. Accucheck: 128 mg/dl 4 hours post prandialGeneral: AOx3Integument: non-contributoryVascular: DP/PT 2/4, bil. Hair to digits, bil. Neurological: Epicritic sensation intact, bil. SWMF 10/10, bil. MSK/Gait: POP along navicular and inferior to medial malleolus at the L. Pes planus, bil but greater on the L. FF Abduction of L foot in stance during gait. Muscle strength: 5/5, bil. but 4/5 for PT on the left. PT tendon is central to the medial malleolus which is more apparent on the L. Contracted 5th digit, bil.Biomechanical Exam:
Base of gait R: 2 in, L: 5 inLimb length: True R 98, L 99; Apparent R 101, L 101. Shoulder drop L. Asymmetric arm swing LHip: R: 25 int 30 ext KE, 30 int 32 ext KF; L: 23 int 28 ext KE, 26 int 30 ext KFMalleoli: R: 14 ext; L: 20 extSTJ: R: 24 inv/10 ev, np 0; L: 22 in/14 ev; NP 2
STJNP: R: 0L: 2 everted
MTJ: R: 2 ev, L: 4 evAKJ DF: 5 KE, 10 KF, bil1st ray 3 DF, 7 PF, bil1st MTP r: 50 unloaded, 30 loaded; L 45 unloaded, 25 loadedTI 2 inverted, bil
NCSP:R: 0 + 2 inverted = 2 varusL: 2 everted + 2 inverted = 0
Max Pronation:R: 10 everted + 2 inverted = 8 evertedL: 14 everted + 0 = 14 everted
RCSP:R: 2 varus, fully compensatedL: 4 varus, fully compensated
X-rayAP foot, bil: subchondral sclerosis of 1st MTP, bil consistent with DJD of 1st MTPJ. Mild HAV on the R. Digitis equinity varus, bil.

Lateral L foot: mild breech at the MTJ, Anterior displaced cyma line consistent with a pronated foot structure. Moderate MPE. R: mild breech at MTJ, narrowed TNJ, cyma line is anteriorly displaced.
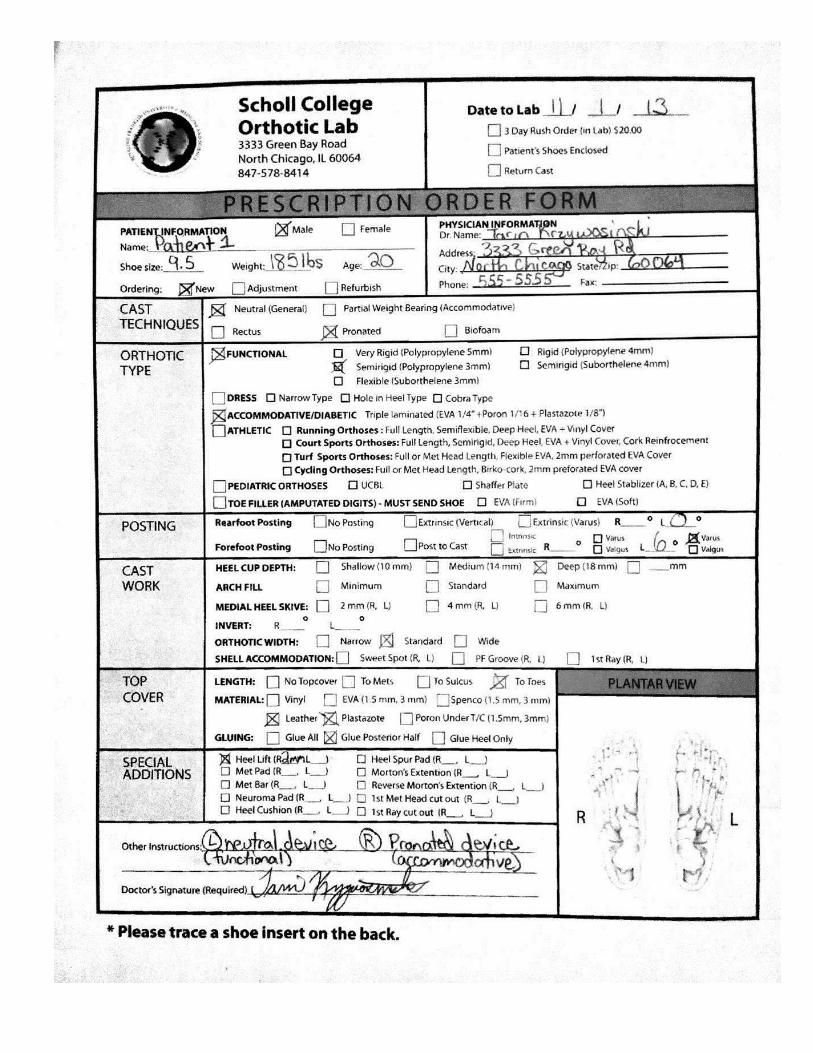
ASSESSEMENT1. PTTD Stage 2, Left2. True Fully Compensated Structural Limb Length Inequality with shorter R limb3. DJD 1st MTPJ4. Plantarflexed 1st ray, bil 5. HDS 5th digit, bil6. Gastrocnemius equinus
Other possible diagnoses:1. OA2. Tarsal Tunnel Syndrome3. Accessory Navicular bone, left4. Spastic Flat Foot
PLANPerformed focused podiatric H & P. Discussed treatment options with the pt. Prescribed orthoses for the pt and instructed her to RICE and offload foot. Prescribed Naproxen 600 mg q6hrs. Taped the pt’s left foot in a high dye fashion to provide support for the foot. Discussed surgical options if pain progresses and STJ becomes rigid. Pt to RTC 1 week for f/u.
Orthoses: R: RF deformity is WNL, so post with heel perpendicular, and really no FF post, L: 4 degree intrinsic post with reverse moton’s extension or metatarsal bar (2mm bar), 2 degrees on the right, 4 on the left (can’t do 1st ray cut out because FF valgus, toe would go into the floor) need to make sure they fit into her shoes, fluffy wedgeMedical management: Johnson and Strom Classification, Rosenburg Classification (radiographic, ultrasound), Conti Classification, single/double heel raise test, jack test, Hinterman test, too many toes sign, Positive Helbing’s sign (lateral bowing of the Achilles tendon), check muscle strength against Plantarflexion and inversion, palpate the tendon. Obesity, HTN , DM causes glycosylation of collagen fibers to decrease elasticity. High Dye (low dye with cross over J) and low dye.Possible tx: physical therapy, Richie brace, NSAIDs, taping, CAM boot


Case 6: SUBJECTIVE14 y/o male PTC with his mother who states her son has a high arch and difficulty walking. Pt states he first noticed it 2 years ago when he was running, and it happens when he plays basketball. Pt states it is getting worse and is constant in both feet. Pt’s mother says the pediatrician told her he suspected Becker’s Muscular Dystrophy and that she should take her son to get a work up from another doctor. Pt’s mother states that her son has currently not had any treatment. Pt’s mother states she wanted a second opinion and thought the podiatrist could help because it involves his feet.
Allergies: seasonal allergies; dogs and catsMedications: Zyrtec 10 mg for allergies PRNDiagnosed Diseases: DeniesImmunizations: UTDSurgical History/Hospitalizations: PE tube at 4 y/oSocial History: Pt states he is in 8th grade and loves to play basketball. Pt denies tobacco, alcohol, illicit drug use.Family History: Pt states he is the first born of 3 total children and that his younger brother and sister are healthy. Pt’s mom states that she and the boy’s father are alive and well.ROS: Pt denies F/C/N/V. Pt relates to persistent UTIs at age 6 but no pathology revealed. Pt’s mother states her son had a UPT that showed normal collection and a normal IVP.Obstetrics: Pt’s mother states she delivered the boy by C section at term due to fetal tachycardia. Pt’s mother denies any postnatal complications or resuscitation. Pt’s mother states the birth weight was 7 lbs 14 oz and his milestones are as follows: Sat: 6 mo, Walked: 11 mo, potty trained at 2.5 yrs.
OBJECTIVEVitals: T 98.6 F, P 100 bpm, RR 16 bpm, BP: 126/80 mmHgGeneral: AOx3 NADIntegument: color, texture, temp all normal.Vascular: DP/PT, popliteal and femoral 1/4 bil. Neurological: DTRs absent, bil. Sharp/dull intact, bil. Vibratory intact, bil. Normal muscle tone. CNs intact. MSK/Gait: intrinsic muscles in hands are atrophied. STJ in version 35, eversion 3, bil. Ankle DF: 0 KE and KF, bil. Spine is straight & hips are stable. Proximal strength: 5/5 in all extremities but distal strength 4/5 in all extremities. Gait: toe-to-hell pattern, bil. Feet in cavo-varus position with inverted heels, bil.Biomechanical Exam:
AJ DF: KE, 0 bil; 10 KF, bil. STJ: R 35 inv, 3 ev; L 35 inv, 3 ev
STJNP: R: 8 varusL: 9 varus
MTJ: 6 valgus 1-5 and 2 valgus 2-5, bil.1st ray: 0 DF, 12 PF, bil1st MTJ: R: 65 unloaded, 35 loaded; L: 68 unloaded, 30 loaded TI: 2 varus, bil
NCSPR: 8 varus + 2 varus = 10 varusL: 9 varus + 2 varus = 11 varus
Max PronationR: 3 eversion + 2 inverted = 1 valgusL: 3 eversion + 2 inverted = 1 valgus
RCSP:R: 1 valgus, partially compensated with the FF 1 degree still off the floorL: 1 valgus, partially compensated with the FF 1 degree still off the floor
X-rayDP, bil: open growth plates, metatarsus adductus, bil, laterally deviated talar head

Lateral Foot, bil: Decreased talar declination, increased calcaneal inclination angle, posteriorly displaced cyma line
Labs: CPK 135 (normal 200), Aldolase 5 (normal 2.7-8.8), NCV in Tibial and common peroneal was 10 m/s (normal 5) EMG: neuropathic
ASSESSEMENT1. Becker Muscular Dystrophy2. Congenital Rigid Plantarflexed 1st ray, bil3. Metatarsus Adductus, bil.4. HDS
Other Possible Diagnoses:1. CMT Disease2. Duchenne’s Muscular Dystrophy3. Emery Dreifuss4. Myasthenia Gravis
PLANPerformed focused podiatric H & P. Discussed treatment options with pt and his mother. Referred pt to muscular dystrophy clinic. Prescribed AFO and physical therapy for pt. If contractures become problematic, surgical release of the soft tissue structures were discussed. Pt RTC in 3 weeks.
NOTES: WOULD NOT SEE THE DIMINISHED NVCs with BECKERS, which is probably why it is NOT Beckers.
Orthotic prescription: has a foot drop, dorsiflexory assist or spring leaf brace to fix it)Medical Management: weakness was proximal instead of distal, CPK outcome, NCVs,Sx. DFWO, Koutsi, Steindler stripping, Watkins procedure, transferring TA is contraindicated because muscle is already weak; DwyerHNPP—foot stays asleep for long time (similar to CMT Type 1A)Initial tx: Richie brace with dorsiflexory assist, physical therapy; probably wouldn’t use an orthotic rx

Case 7SUBJECTIVE45 y/o male PTC complaining of heel pain in both heels. Pt states the pain started 2 months ago on the bottom of his heels. Pt describes the pain as a constant and that is the worst when getting out of bed in the morning. Pt rates it as 8/10 and states he has tried wearing gym shoes but it does not seem to help.
Allergies: NKDAMedications: Lasix, Metformin, Atenolol, Simvastatin Diagnosed Diseases: HTN, DM type 2, hypercholesterolemiaChildhood Disease: deniesImmunizations: unknownSurgical History/Hospitalizations: deniesSocial History: Pt states his is an inventory stocker at home depot. Pt states he smokes but denies drinking and illicit drug use. Pt states he is single.Family History: Pt state his mother and father died of abdominal cancer ROS: Pt denies F/C/N/V but relates to lower back pain but has not been evaluated or treated.
OBJECTIVEVitals: unremarkableGeneral: AOx3. Moderate distress.Integument: unremarkable Vascular: DP/PT are 2/4, bil. CFT < 3 sec. No edema noted.Neurological: Sensation is grossly intact. SWMF: 10/10, bilMSK/Gait: POP of the medial tubercle of calcaneus, bil. Pain on POP of central heel bil; POP of peroneal tendons. Negative Tinel’s sign. ROM: limited ankle DF; unable to attain 90 degrees with knee extended or flexed. Gait: normal and propulsive.
Biomechanical Exam:Angle: 15, bilBase: 2 inch, bilPostural: R: 95.7 T, 106.0 A; L: 96.0 T, 106.0 AAJ DF KE: -12 R, -15 L; KF: -1 R, -12 LSTJ: R: 18 inv, 5 ev; L: 15 inv, 4 evSTJNP:
R: 4 varusL: 3 varus
MTJ: 1-5: R: 9 varus; L: 8 varusMTJ 2-5: R: 7 varus; L: 5 varus1st Ray: R: DF: 12 mm, PF: 8 mm; L: DF: 11 mm, PF: 5 mm PF
NP: R: 2 mm DF; L: 3 mm DF1st MTPJ: R: 38 unloaded, 8 loaded; L: 35 unloaded, 10 loaded TI: R: 3 varus; L: 2 varus
NCSP:R: 4 inverted + 3 inverted = 7 varusL: 3 inverted + 2 inverted = 5 varus
Max Pronated:R: 5 eversion + 3 inversion = 2 valgusL: 4 eversion + 2 inversion = 2 valgus
RCSP:R: 2 valgus, partially compensated with the FF still 5 degrees off the groundL: 2 valgus, partially compensated with the FF still 1 degree off the ground
X-rays: Lateral foot: Calcification at insertion of Achilles and plantar fascia, peroneal tendons seen on lateral and
DP, worse on left than right, entheseopathyDP: accessory sesamoids and calcification of 1st MPJ capsule-R

L: hyperostosis on medial aspect of distal phalanx of hallux and calcification lateral to fibular sesamoid
Spine: bamboo spine
Labs: HLA B27 Positive, increased ESR
ASSESSEMENT1. DISH2. Entheseopathy of Achilles causing Boney/Soleal Equinus, bil 3. MPE, bil.4. Combined structural and functional hallux limitus, bil.5. DJD 1st MTPJ6. Digniti Equinti Varus, bil.
Other possible Diagnoses:1. Ankylosing Spondylitis2. Plantar Fasciitis3. Reiter’s disease4. Myositis ossificans
PLANPerformed focused podiatric H & P. Discussed treatment options with pt regarding short term and long term care. Referred pt to rheumatologist for a consult. Prescribed PT, orthoses, and Ibuprofen 600 mg q6hrs for the pt. Low dye taping applied to both of the pt’s feet. Discussed possible steroid injection at future visit. Pt to RTC in 2 weeks for f/u.
Orthotic Prescription: 1. functional orthotic- posted 6 degrees (according to his #s, I think mine are different)Refer to the rheumatologist (HLA-B27 generally positive in many autoimmune dz)Accommadative partial WB


Case 8 SUBJECTIVE37 y/o male PTC complaining of a non-healing ulcer after a left foot transmetatarsal amputation that occurred a month ago. The pt states there is no pain associated with the ulcer, but that it has gotten worse since he was discharged from surgery. Pt states he has noticed drainage and gangrene near the ulcer. Before he was discharged, he states he was diagnosed with a MRSA infection. He is currently taking IV vancomycin. Pt stated he arrived at the office using a transportation serve and states he wears a wedge rocker shoe most of the time.
Allergies: NKDAMedications:
Humulin 70/30- SubQ suspension 15 units at bed time, and 20 units in the morningNephedapine 30 mg QDRenvela 800 mg TIDSensopar 30 mg QDBaby Aspirin 81 mg QD50 mg Atenolol, QD20 mg Enalopril BID2.5 mg Midoxidil BID20 mg Omeprazole QD
Diagnosed Diseases: DM 2 w/neurological manifestations, end stage renal disease, dialysis for renal failure, HTN, GERD, recent MRSA infectionChildhood Disease: denies Immunizations: UTDSurgical History/Hospitalizations: Pt states he had surgery on Dec 7, 2012 for transmetatarsal amputation of the L foot and a digital amputation previouslySocial History: Pt states he is on disability and lives with family membersFamily History: non-contributoryROS: Pt denies fevers, chills, sweats, palpitations, SOB, arthritis, headache, sinus issues, or urinary issues. Pt relates to having kidney failure.
OBJECTIVEVitals: unremarkable General: AO x3Integument: Warm & dry. Serosanginous & serous drainage from the L foot. 5 cmx19.4x5.5cm. Sinus tracts 3cm at 8 o’clock, 4.5 cm at 2 o’clock, 4 cm at 12 o clock. Depth is varied. Moderate tunneling and undermining. Necrotic and gangrenous tissue within the wound and at the periphery of the wound. Hypergranulation and fibrin deposition but nonviable tissue due to orientation of the sinus tract. No epithelization noted. There is exposed muscle, tendon, and fascial layers. Edema around the wound w/callus around the periphery. Escher with gangrenous tissue along the wound edge. Vascular: Left PT is nonpalp; monophasic & strong on Doppler; all others are normal. Edema noted around the wound. No heart murmurs and normal rhythm.ABI: DP and PT could not be calculated on R or L leg. Noncompressible suggesting calcific arteriosclerosis. Arterial Doppler: non-diagnostic due to incompressible vessels and elevated pressure in the L leg. Suggested other arterial imaging modalities such as CT or ultrasound. Neurological: neurotrophic due to DM 2; decreased sharp/dull sesnsationMSK/Gait: Normal ROM, strength. No tenderness in foot or ankle.
X- rays: negative for OM (we were not shown these)
ASSESSEMENT1. Previous Ulcer with MRSA (Wagner Grade 4), Left2. Previous OM, left hallux

3. Monckeberg’s Arteriosclerosis PLANPerformed focused podiatric H & P. Discussed both short term and long term treatment options with pt. (Note: pt eventually healed after wound vac use so now discussed the next step with the healed foot.) Discussed with the patient the use of custom molded shoes with a heel to toe rocker and orthoses. Prescribed orthoses for the patient and a toe filler. Pt RTC in 2 weeks for f/u.
Orthotic prescription: TMA filler, custom molded high top/extra depth shoe, MILD support at the ankle2. solid AFO with custom molded shoe, could do severe rocker, could do extended shankAFO, with filler and rocker is best for this pt
