king asthma copd 04-09-14 handout.ppt
TRANSCRIPT

1
TalmadgeE.King,Jr.,M.D.KrevinsDistinguishedProfessorofMedicine
Chair,DepartmentofMedicineUniversityofCaliforniaSanFrancisco(UCSF)
SanFrancisco,CA
CurrentStrategiesforAsthmaandCOPD
Asthma3
ASTHMA
• Achronicinflammatorydiseaseoftheairways;
• Chronicinflammationleadstohyperresponsivenesstostimuli;
• Variableandreversibleairflowobstruction.

2
Asthma• Acommonchronicdiseasesworldwide
– ~300millionpersonsareaffectedworldwide.
– ~14.9millionpersonsintheUS
– DramaticincreasesintheprevalenceofatopyandasthmainWesternizedcountriesandmorerecentlyinless‐developednations.
– Responsibleforabout• 500,000hospitalizations,
• 5,000deaths,and
• 134milliondaysofrestrictedactivityayear
Asthma• Optimalmanagementofasthma(wearebetter!)
– improvesqualityoflife
– decreasesthepoolofthoseatriskfordeath
– saveshealthcarecostsinemergencycare
DiagnosisofAsthma:3Steps1. Obtainahistoryofepisodic symptoms
ofairflowobstruction
2. Demonstratethatairflowobstructionisatleastpartiallyreversible
3. Excludealternativediagnoses =particularlyCOPDandvocalcordobstructioninadults,andaspirationandcysticfibrosisinchildren.
AlternativeDiagnoses• COPD
• Vocalcorddysfunction
• CHF
• Pulmonaryembolism
• Drug‐inducedcough
• Pulmonaryinfiltrationwitheosinophilia
• Obstructivesleepapnea
• Mechanicalobstruction– e.g.benignormalignanttumor

3
CluestoDiagnosis•Recurrentepisodesofwheezing
• Troublesomecoughatnight
• Coughorwheezeafterexercise
• Cough,wheezeorchesttightnessafterexposuretoairbornedust,allergens
• Coldsthat“gotothechest” ortakemorethan10daystoclear
SpirometryEstablishestheDiagnosis
• Bydemonstratingobstruction:
– FEV1 <80%predicted
– FEV1/FVC<65%predictedorbelowthelowerlimitofnormal
• Bydemonstratingreversibility:
– FEV1 increases>12%and atleast200mL
MeasurementofPeakFlow• Whenspirometryisnormalbutpatientsstillhavesymptoms,followupwithpeakflowmonitoringfor1‐2weeksuponarisingandintheafternoonbeforeandafterinhaledbronchodilator.
• Differenceof20%betweenhighandlowreadingsonsamedaysuggestsasthma.
AsthmaGuidelines4EssentialComponents
1. Assessment&monitoring
2. Patienteducation
3. Controloffactorscontributingtoasthmaseverity
4. Pharmacologictreatment
National Asthma Education and Prevention Program: Expert panel Report 3

4
• StepwiseapproachtomanagingRxexpandedto6stepswithrepositionedmedications
• Emphasisonpatienteducation/partnership
– educationatallpointsofcare
• Moreattentiontocontrolofenvironmentalfactorsorcomorbidconditions
– multifacetedapproaches
– considerationofSQimmunotherapyinpersistentasthma
– benefitfromtreatingcomorbidconditions
AsthmaGuidelines
Assessment&
Monitoring
Asthma Care: 4 Essential
Components
1
Assessment&Monitoring• AssessasthmaseveritytoinitiateRx(basedoncurrent impairment)
• AssessasthmacontroltomonitorandadjustRx(basedontherisk offuturenegativeevents)
• Stepwiseapproach– Schedulefollow‐upcare
– assesscontrol
– medicationtechnique
– writtenactionplan
– adherenceateachvisit
Severityvs.Control•SEVERITY =intrinsicintensityofthediseaseprocess
–Emphasizedforinitiating therapy
•CONTROL =degreeofsuccessofRx
–Emphasizedformonitoringandadjustingtherapy
Eur Respir J. 2008 Sep;32:545-54

5
AssessmentofImpairment• Keyelementsofimpairment:
– Patient’srecallofsymptoms
– Nighttimeawakenings
– Physicalactivity(esp.interferencewithnormalactivity)
– Needforrescuemedicationsinthepreceding2to4weeks(Short‐actingbeta2 agonistuse)
– Frequencyandseverityofexacerbations
– Qualityoflife
– Currentpulmonaryfunction
AssessmentofImpairment
• Patient‐centric,validatedtoolstoevaluatethecurrentasthmacontrolinclude:
– AsthmaTherapyAssessmentQuestionnaire(ATAQ)
– AsthmaControlQuestionnaire(ACQ)
– AsthmaControlTest(ACT)Aidan A. Long, MD: www.peerviewpress.com/d/p131
DetermineSeverityWhenInitiatingTherapy
ComponentsofSeverity
INTERMITTENTPERSISTENT
Mild Moderate Severe
Symptoms <2days/week >2days/week Daily Allday
Nighttimeawakenings <2days/month 3‐4x/month >1/week Upto7x/week
Short‐actingbeta2 agonistuse
<2days/week >2days/week Daily Severaltimesaday
Interferencewithnormalactivity None Minor Some Extreme
LungFunction FEV1 normal FEV1 >80% FEV1 60‐80% FEV1<60%
<2
DetermineSeverityWhenInitiatingTherapy
ComponentsofSeverity
INTERMITTENTPERSISTENT
Mild Moderate Severe
Symptoms <2days/week >2days/week Daily Allday
Nighttimeawakenings <2days/month 3‐4x/month >1/week Upto7x/week
Short‐actingbeta2 agonistuse
<2days/week >2days/week Daily Severaltimesaday
Interferencewithnormalactivity None Minor Some Extreme
LungFunction FEV1 normal FEV1 >80% FEV1 60‐80% FEV1<60%

6
AssessmentofRisk
Aidan A. Long, MD: www.peerviewpress.com/d/p131
ClassificationofAsthmaSeverity:BasedonRisk
Exacerbationsrequiringuseoforalsteroids
IntermittentPersistent
Mild Moderate Severe
0‐1/yr
>2/yrLesssevere,
Longerinterval
>2/yr
>2/yrMoresevere,shorterinterval
InitialTreatment:Basedon
ClassificationofSeverity
6StepsofAsthmaManagement
Step
1

7
6StepsofAsthmaManagement
Aidan A. Long, MD: www.peerviewpress.com/d/p131
Persistent Asthma
Step
2
6StepsofAsthmaManagement
Aidan A. Long, MD: www.peerviewpress.com/d/p131
Persistent Asthma
Step
3
6StepsofAsthmaManagement
Aidan A. Long, MD: www.peerviewpress.com/d/p131
Persistent Asthma
Step
4
6StepsofAsthmaManagement
Aidan A. Long, MD: www.peerviewpress.com/d/p131
Persistent Asthma
Step
5

8
6StepsofAsthmaManagement
Persistent Asthma
Step
6
6StepsofAsthmaManagement
StepsinICSDosagesLow Medium High
Vanceril84mcg/puff
2‐6puffs 6‐10puffs >10puffs
Pulmicort DPI200mcg/inhalation
1‐2inhalations 2‐3 >3
Flovent110mcg/puff
2puffs 2‐6puffs >6puffs
Aerobid250mcg/puff
2‐4puffs 4‐8puffs >8puffs
MometasoneDPI200mcg/inhalation
1inhalation 2 3
Oncetreatmentisestablished,theemphasisisonassessingasthmacontroltodetermineifthegoalsfortherapyhave
beenmetandifadjustmentsintherapy(stepuporstepdown)
wouldbeappropriate.

9
AfterInitialClassificationofSeverity,DetermineLevelofControl
ControlVeryPoorlycontrolled
Notwellcontrolled
WellControlled
Symptoms <2days/wk >2days/wk Allday
Nighttime
Awakenings<2/mo 1‐3x/wk >4/wk
Interferencewithnormalactivity None Some Extreme
SABAuse <2days/wk >2days/wk Several/day
FEV1 orpeakflow >80%best 60‐80%best <60%best
ACTquestionnaire >20 16‐19 <15
TheAsthmaControlTest
SOB
Interference with daily activities
Nighttime awakening
SABA inhaler use
Overall rating
5
5
5
5
5
25
Worse Better
Adjust TreatmentbasedonControl
ControlVeryPoorlycontrolled
Notwellcontrolled
WellControlled
Step
Maintain,
Considerstepdown ifwellforatleast3months
Stepupby1step Stepupby1‐2steps
Oralsteroids?
No No Considershortcourse
FollowupRegular,
Q1‐6mos
Reevaluate
In2‐ 6wks
Reevaluate
In2weeks
BeforeStep‐upofTherapy
•Reviewadherence
• Inhalertechnique
•Environmentalcontrol
•Co‐morbidconditions

10
PatientEducation
Asthma Care: 4 Essential
Components
2
PatientEducation/Partnership
• Self‐managementeducation
– Teachandreinforceself‐monitoring
•signsofworsening(symptomsorpeakflow)
•differencebetweenlong‐termcontrolandquickreliefmedications
•correctinhalertechnique
•avoidingenvironmentaltriggers
– Awrittenasthmaactionplan
PeakFlowMeters• Establishpatient’spersonalbestvalueandevaluatetheresponsetochangesintherapy.
• Patientswithmoderatepersistentandseverepersistentasthmamaybenefitfromhavingapeakflowmeterathomeandmeasuringtheirleveluponarisingeachmorning.
PEF values(personal best, 80%,
50%)
Controller and
quick-relief medicine plan

11
NormalPeakFlowVariesbyGender,Age,Ethnicity
PeakFlowMeters:Caveats• Extremelywidevariabilityeveninthepublishedpredictedpeakexpiratoryflowreferencevalues
• Effortdependent
• Pooratdetectingmildobstruction
• Referencevaluesdifferforeachbrandofmeter– normativebrand‐specificvaluescurrentlyarenotavailableformostbrands
• Helpsinmonitoringbutnotdiagnosis– Particularlyusefulforpatientswithoutgoodabilitytosensesymptoms
InhalerTechnique
43
InhalerTechnique
44

12
EnvironmentalFactors
&ComorbidConditions
Asthma Care: 4 Essential
Components
3
Environmentalfactorsandcomorbidconditions
•Reviewexposures
–adviseonwaystoreduceexposure
–Inpatientswithpersistentasthma,considerskinallergytestingandimmunotherapy
• Comorbidconditions
–ABPA,GEreflux,obesity,OSA,rhinitis&sinusitis, stress, depression, tobacco
Medications
Asthma Care: 4 Essential
Components
4
Medications• Long‐termcontrolmedications– InhaledCorticosteroids(ICS)
– Longactingbetaagonists(LABA)–salmeterol/formoterol– last>12h•NOTformonotherapy/tobeusedwithICS(Step3‐4)
– Cromolynsodium/nedocromil•Step2(Mildpersistent)
•PreventiveRxbeforeexerciseorexposuretoallergens
– Immunomodulators– omalizumab(anti‐IgE)•AdjunctiveRxifallergiesandStep5‐6care(Severepersistent)
•Administeredwhereequippedtotreatanaphylaxis

13
SteroidTreatmentTips• Inhaledcorticosteroidsshouldbeusedforallpersistent asthma
• ICSmustbeusedwithLABA(salmeterol)
– duetohigherthanexpecteddeathrateswithLABAalone
• Fivedaycourseoforalcorticosteroidsdoesnotrequiretaper
• SmokersmayrequirehigherICSdoses
Summary• Stepwiseassessmentusedforinitialtherapyandadjustmentoftherapy
• LABAhasnorolealone
– onlyifusedtogetherwithICS
• ICSwithallpersistentasthma
• Patientstobepartnersincare
– asthmacontroltestformonitoring
– writtenasthmaactionplanforassessment/Rx
SmokersareDifferent
• Upto1/3ofasthmaticssmoke
• 44non‐smokersand39lightsmokerswithmildasthmaassignedtoICS2xdayorLTA1xday
– EvenwithsimilarFEV1,smokershadworsequalityoflife,moresymptoms
– ICSreducedsputumeosinophilsinboth
– ICSimprovedFEV1onlyinnon‐smokers
– LTAimprovedAMpeakflowonlyinsmokersLazarus et al. Am J Respir Crit Care Med. 2007;175:783-90

14
COPD
53
COPD•Apreventableandtreatablediseasestatecharacterizedbyairflowlimitationthatisnotfullyreversible.
• Airflowlimitation
– usuallyprogressiveand
– associatedwithanabnormalinflammatoryresponseofthelungstonoxiousparticlesorgases,primarilycausedbycigarettesmoking. Celli B. R. Chest 2008;133:1451-1462
COPD•Coughorwheeze•Sputumproduction•Dyspnea•Chesttightness•Worseningqualityoflife(oftenwithoutclearrecognition) Celli B. R. Chest 2008;133:1451-1462
COPD•Highlyprevalent(7to19%;M>W;white>blacks;increaseswithage)•Underdiagnosed(~12M),•Undertreated,•Underperceived,and•Verycostlycare(~$49.9Bin2010)

15
AnAcceleratedDeclineInLungFunctionIsTheSingleMostImportantFeatureOfCOPD
3rd-ranked cause of death in
the US (~100,000 each
year).
COPD:Cigarettesmoking
• Mostimportantriskfactor.
• Smokingleadsto– aninflammatoryresponse,
– oxidativestress,
– lungdestruction,and
– interferencewithlungrepair
Smokers
Smoker, Severe COPD
Immunostaining with monoclonal antibody anti-CD45
Leukocyte Infiltration in COPD
Smoker, Mild COPD
COPD:Smokingcessation
•SlowstheaccelerateddeclineinCOPD‐relatedFEV1
•Reducesall‐causemortalityratesby27%(byreductioninCVmortality)
16
COPD•ThemortalityratefromCOPDforwomenhasdoubledoverthepast20yrs.
• Somestudiessuggestthatwomenaremoresusceptibletotheeffectsoftobaccosmokethanmen
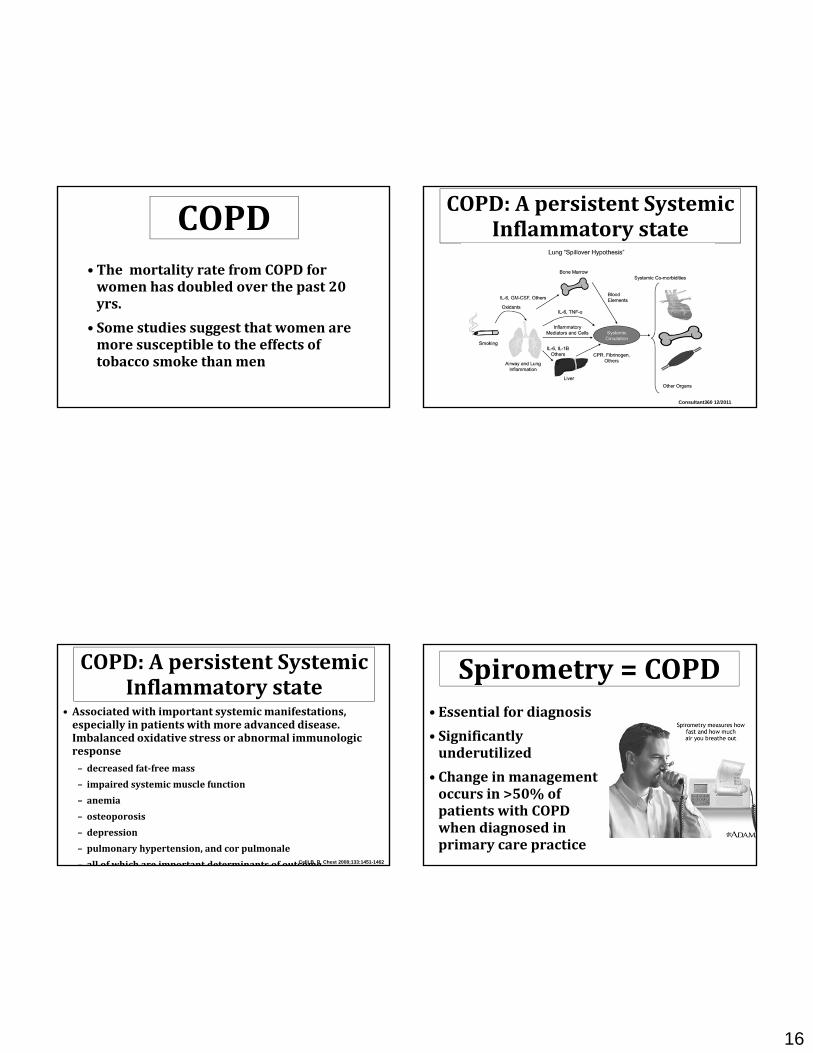
COPD:ApersistentSystemicInflammatorystate
Consultant360 12/2011
COPD:ApersistentSystemicInflammatorystate
• Associatedwithimportantsystemicmanifestations,especiallyinpatientswithmoreadvanceddisease.Imbalancedoxidativestressorabnormalimmunologicresponse– decreasedfat‐freemass
– impairedsystemicmusclefunction
– anemia
– osteoporosis
– depression
– pulmonaryhypertension,andcorpulmonale
– all of which are important determinants of outcomeCelli B. R. Chest 2008;133:1451-1462
Spirometry=COPD•Essentialfordiagnosis
• Significantlyunderutilized
• Changeinmanagementoccursin>50%ofpatientswithCOPDwhendiagnosedinprimarycarepractice

17
WhoShouldGetSpirometry?
Smoker/ex‐smoker>40yrsoldwhosays‘yes’to:
•Doyoucoughregularly?
•Doyoucoughupphlegmregularly?
•Doevensimplechoresmakeyoushortofbreath?
•Doyouwheezewhenyouexertyourself,oratnight?
•Doyougetfrequentcoldsthatpersistlongerthanthose of other people you know?
ApproachtoPatientswithCOPD
Celli B. R. Chest 2008;133:1451-1462
BODEIndex:ClassificationofSeverityClassificationofSeverity

18
GOLDGuidelines:COPDManagement
•Assessandmonitorthedisease
•Reduceriskfactors
•ManagestableCOPD
•Manageexacerbations
COPD:aTreatableDisease
• Overallgoalsoftreatment
– topreventfurtherdeteriorationinlungfunction,
– improvesymptomsand
– qualityoflife,
– treatcomplications,and
– prolongameaningfullife
Celli B. R. Chest 2008;133:1451-1462
COPD:aTreatableDisease• Improvedsurvivalfoundwith:
– Smokingcessation– Long‐termoxygentherapyinhypoxemicpatients– Noninvasivemechanicalventilationinsomepatientswithacute‐on‐chronicrespiratoryfailure
– LVRSforpatientswithupper‐lobeemphysemaandpoorexercisecapacity
• TheTORCH(TowardsaRevolutioninCOPDHealth‐‐ >6,000patients)– Combinationofsalmeterolandfluticasoneimprovedlungfunctionandhealthstatus,AND
– Relativeriskofdyingdecreasedby17.5%(overthe3yearsofthestudy).
• Pulmonaryrehabilitationandlungtransplantationimprovesymptomsandthequalityoflife
Celli B. R. Chest 2008;133:1451-1462
TherapeuticOptionsforPatientsatRiskforCOPDandThoseWithEstablishedDisease
Celli B. R. Chest 2008;133:1451-1462
LAMA =LA muscarinic agent
LVR = lung volume reduction
MV = mechanical ventilation.
19
COPD:ImportanceofHyperinflation
• Dyspneaperceivedduringexercise,includingwalking,morecloselyrelatestothedevelopmentofdynamichyperinflation thantochangesinFEV1.
• Improvementinexercisebroughtaboutbyseveraltherapies(bronchodilators,oxygen,lungvolumereductionsurgery,andevenrehabilitation)ismorecloselyrelatedtodelayingdynamichyperinflationsthanbyimprovingthedegreeofairflowobstruction. Celli B. R. Chest 2008;133:1451-1462
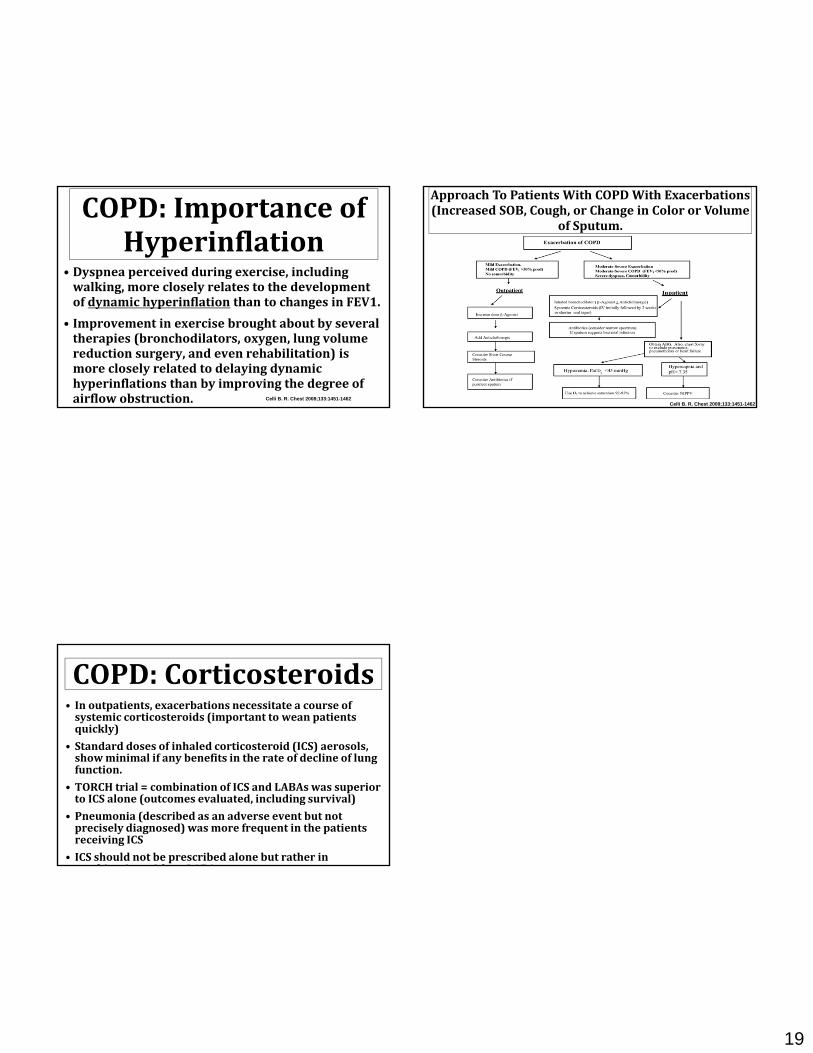
ApproachToPatientsWithCOPDWithExacerbations(IncreasedSOB,Cough,orChangeinColororVolume
ofSputum.
Celli B. R. Chest 2008;133:1451-1462
COPD:Corticosteroids• Inoutpatients,exacerbationsnecessitateacourseofsystemiccorticosteroids(importanttoweanpatientsquickly)
• Standarddosesofinhaledcorticosteroid(ICS)aerosols,showminimalifanybenefitsintherateofdeclineoflungfunction.
• TORCHtrial=combinationofICSandLABAswassuperiortoICSalone(outcomesevaluated,includingsurvival)
• Pneumonia(describedasanadverseeventbutnotpreciselydiagnosed)wasmorefrequentinthepatientsreceivingICS
• ICSshouldnotbeprescribedalonebutratherinbi ti ith LABA