kathiresan isa amsterdam 052415 final final - … · eli lilly!! merck! merck! bayer healthcare!...
TRANSCRIPT

Disclosures
Scientific Advisory Board Research Grants
Regeneron Genetics Center Aegerion
Eli Lilly
Merck
Merck Bayer Healthcare
Novartis Regeneron
Amarin
Celera

Developing medicines that mimic the natural successes of the genome
Sekar Kathiresan, MD Director, Preventive Cardiology, MGH
Associate Professor of Medicine, Harvard Medical School Institute Member, Broad Institute
ISA 2015
May 24, 2015

http://www.cdc.gov/nchs/data/dvs/deaths_2010_release.pdf
Myocardial infarction: ���leading cause of death in US and worldwide

Major unmet need: ���only 2 therapies to prevent FIRST MI & ���
both with modest efficacy ���
• Aspirin • Statins
Prevents clotting Reduces relative risk by ~15%
Lowers LDL Reduces relative risk by ~25%

Problem:
Only about 5% of medicines in development succeed into clinic

Two reasons stand out:
Poorly predictive models

Two reasons stand out:
Poorly predictive models Don’t know impact of blocking a gene over
many years

Idea:
Identify naturally-occurring mutations that protect against disease &
develop medicines that mimic them



MI

Medicines that mimic natural successes of the genome
MI

Initial example for MI
PCSK9
1 in 50 blacks
Lower LDL
80% lower risk
alirocumab, evolocumab, bococizumab
Abifadel, Nat Genet (2003)
Cohen, N Engl J Med (2006)
Stein, N Engl J Med (2012)
MI

Are there more examples for MI?

Outline
Results: Risk Mutations
LDLR, APOA5 Protective Mutations
NPC1L1, LPA LPL, APOC3
Two Human Genetics Experiments
Experimental Approach

Outline
Results: Risk Mutations
LDLR, APOA5 Protective Mutations
NPC1L1, LPA LPL, APOC3
Two Human Genetics Experiments
Experimental Approach
Ascertain MI cases & controls
Cases with MI Controls free of MI

Characterize genome in each person for NULL mutations
Variant in Exon
AATCATCGATGT
AATCATTGATGT
Synonymous
Missense
Nonsense
Splice site Null mutations
Indel frameshift

Normal: 2 working copies of a gene

With null mutations: ���one or two copies of a gene broken
Heterozygous null Homozygous null

Why focus on null mutations?���
Heterozygous null
Most therapies inhibit target gene
(rather than activate target)

Test if carriers of null mutations in a given gene are protected against MI
Cases with MI Controls
Cases Controls
Cumulative frequency of
null mutations in gene
X %
Y %

Protective signal: frequency of null mutations greater in disease-free controls than cases
Cases with MI Controls
Cases Controls
Cumulative frequency of
null mutations in gene
X %
Y %
Risk gene
X > Y
Protective gene
Y > X

Outline
Results: Risk Mutations
LDLR, APOA5 Protective Mutations
NPC1L1, LPA LPL, APOC3
Two Human Genetics Experiments
Experimental Approach

Study design: MI/CHD cases & controls
Exome Sequencing
Cases N=5K
Controls N=5K
Cases N=60K
Controls N=120K
Exome Chip Genotyping
Do et al., Nature 2015
Stitziel et al., Under Review
Systematically search for Protective Mutation signal across each of ~18,000 genes

Outline
Results: Risk Mutations
LDLR, APOA5
Two Human Genetics Experiments
Experimental Approach
Protective Mutations NPC1L1, LPA LPL, APOC3

Early MI risk mutation signal for ���each of 18,000 genes

One gene stands out
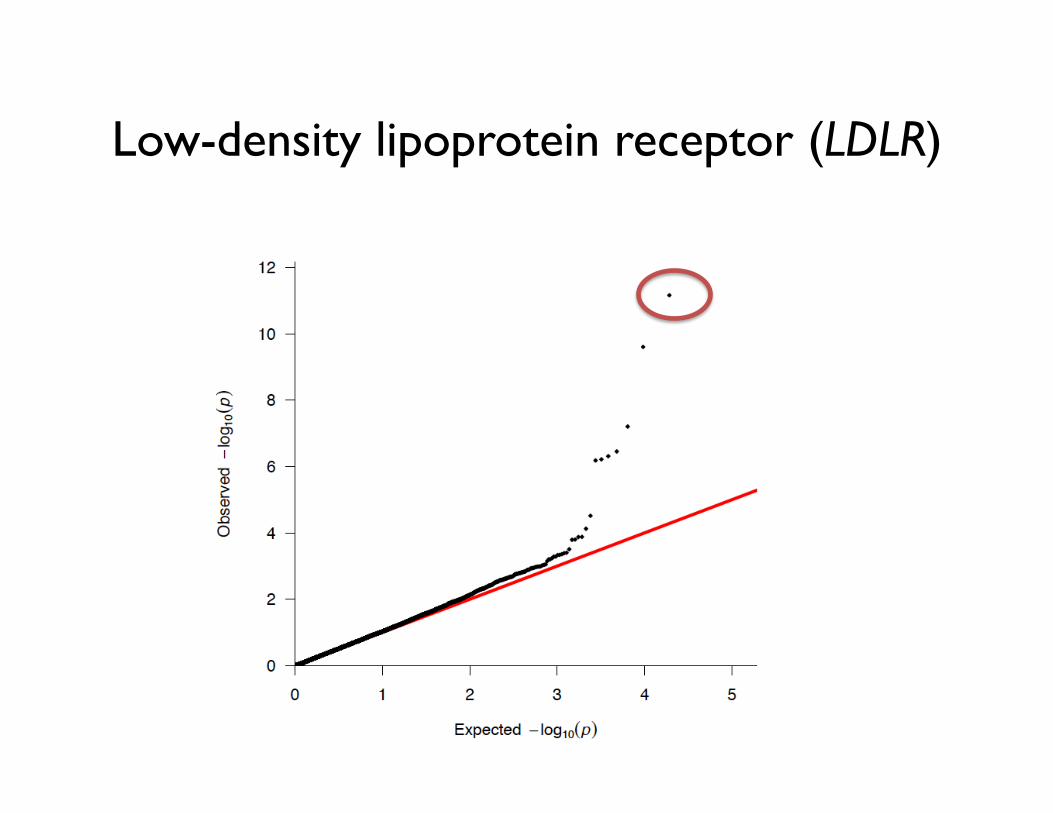
Low-density lipoprotein receptor (LDLR)

Do et al., Nature (2015)
Clinical Effect
Low-density lipoprotein receptor (LDLR)
1 in 217 carrier
Loss of function mutations at LDLR lead to familial hypercholesterolemia (FH) & increase MI risk
LDL +75%
MI
4-fold
Gene

Where does this oft-quoted come from?
Textbooks: FH carrier frequency is 1 in 500
Nordestgaard, Eur Heart J (2013)

Goldstein, J Clin Invest 52:1544, 1973

Patients with early-onset MI Men or women <60y
Controls without MI
1 in 500 with total cholesterol > 285 mg/dl
In 1973, Goldstein defined FH as TC > 285 mg/dl

0.2% = 1 in 500
Goldstein, J Clin Invest 52:1544, 1973

Patients with early-onset MI Controls without MI
LDLR mutations in cases: 1 in 51
LDLR mutations in controls: 1 in 217
In sequencing era, we (and others) have refined this estimate to
~ 1 in 200

Do et al., Nature (2015)
Clinical Effect
Low-density lipoprotein receptor (LDLR)
1 in 217 carrier
Loss of function mutations in APOA5 also increase MI risk [as well as plasma triglyceride-rich lipoproteins (TRL)]
Apolipoprotein A5 (APOA5)
LDL +75%
MI
4-fold
1 in 158 carrier
Gene
TRL
+60% MI
2-fold

Outline
Results: Risk Mutations
LDLR, APOA5
Two Human Genetics Experiments
Experimental Approach
Protective Mutations NPC1L1, LPA LPL, APOC3

NPC1L1���Niemann-Pick C1-Like 1

Clinical question
Will addition of an LDL-lowering medicine on top of statin
improve clinical outcomes?

Ezetimibe (Zetia) lowers LDL by blocking cholesterol absorption by 50%
• Ezetimibe targets NPC1L1 gene in the intestine
Francis, CMAJ (2005)
Acetyl CoAyy
Cholesterol biosynthesisol bol b
Bile acid biosynthesis
Bile acids
Bile
Bile acids
Enterohepaticcirculation
Terminal ileum
Sterols
Bile acids
Diet
Upper small intestine
Lipoprotein synthesis
LDL receptorLLDL
Plasmacompartment
Liver
Lymphatics
Chylomicrons
Cholesterol
s
Ezetimibe
Statins

It was uncertain if lowering LDL through ezetimibe would
reduce risk for MI
Human genetics experiment
to address this issue

NPC1L1 null mutations and ezetimibe both reduce protein function by ~50%
Genetics
Pharmacology
Heterozygous null – protein function reduced
lifelong by 50%
Ezetimbe treatment reduces cholesterol absorption by 54%
Sudhop, Circulation (2002)

Genetics mimics pharmacology
People who carry NPC1L1 null mutations:
it’s as if they had been given ezetimibe lifelong

Our two hypotheses:
When compared with non-carriers, carriers of NPC1L1 null mutations will have:
1. lower LDL cholesterol
2. lower risk for MI

NPC1L1 null mutations: nonsense, splice, frameshift���seen in ~ 1 in 650 in the population
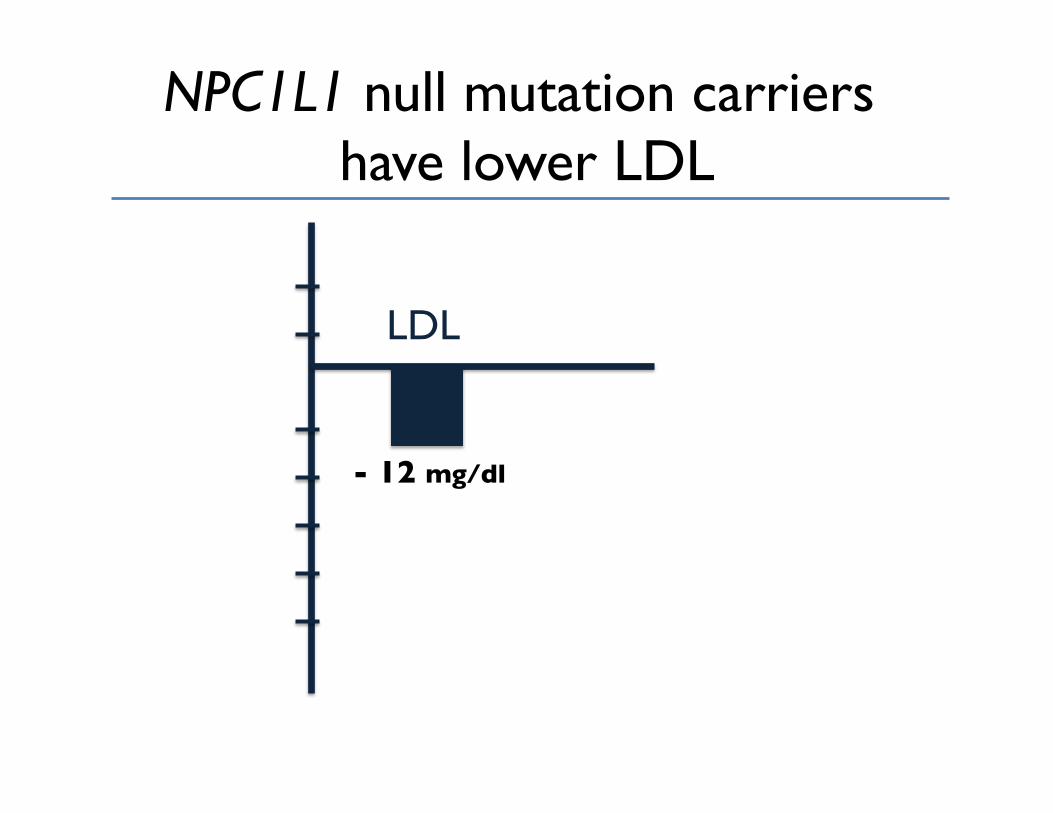
NPC1L1 null mutation carriers ���have lower LDL
- 12 mg/dl
LDL

NPC1L1 null mutation carriers have lower LDL and protected against MI
- 12 mg/dl
- 53%
LDL MI
Nate Stitziel, MD, PhD Hong-Hee Won, PhD
N Engl J Med Epub 2014 Nov 12

These genetic results predict that ezetimibe should reduce MI risk

…a week later,
at American Heart Association 2014

IMProved Reduction of Outcomes: Vytorin Efficacy International Trial A Multicenter, Double-Blind, Randomized Study to Establish the Clinical Benefit and Safety of Vytorin (Ezetimibe/Simvastatin Tablet) vs Simvastatin Monotherapy in High-Risk Subjects Presenting With Acute Coronary Syndrome

Patients stabilized post ACS ≤ 10 days: LDL-C 50–125*mg/dL (or 50–100**mg/dL if prior lipid-lowering Rx)
Standard Medical & Interventional Therapy
Ezetimibe / Simvastatin 10 / 40 mg
Simvastatin 40 mg
Follow-up Visit Day 30, every 4 months
Duration: Minimum 2 ½-year follow-up (at least 5250 events)
Primary Endpoint: CV death, MI, hospital admission for UA, coronary revascularization (≥ 30 days after randomization), or stroke
N=18,144
Uptitrated to Simva 80 mg if LDL-C > 79 (adapted per
FDA label 2011)
Study Design *3.2mM
**2.6mM
Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:205-12
90% power to detect ~9% difference
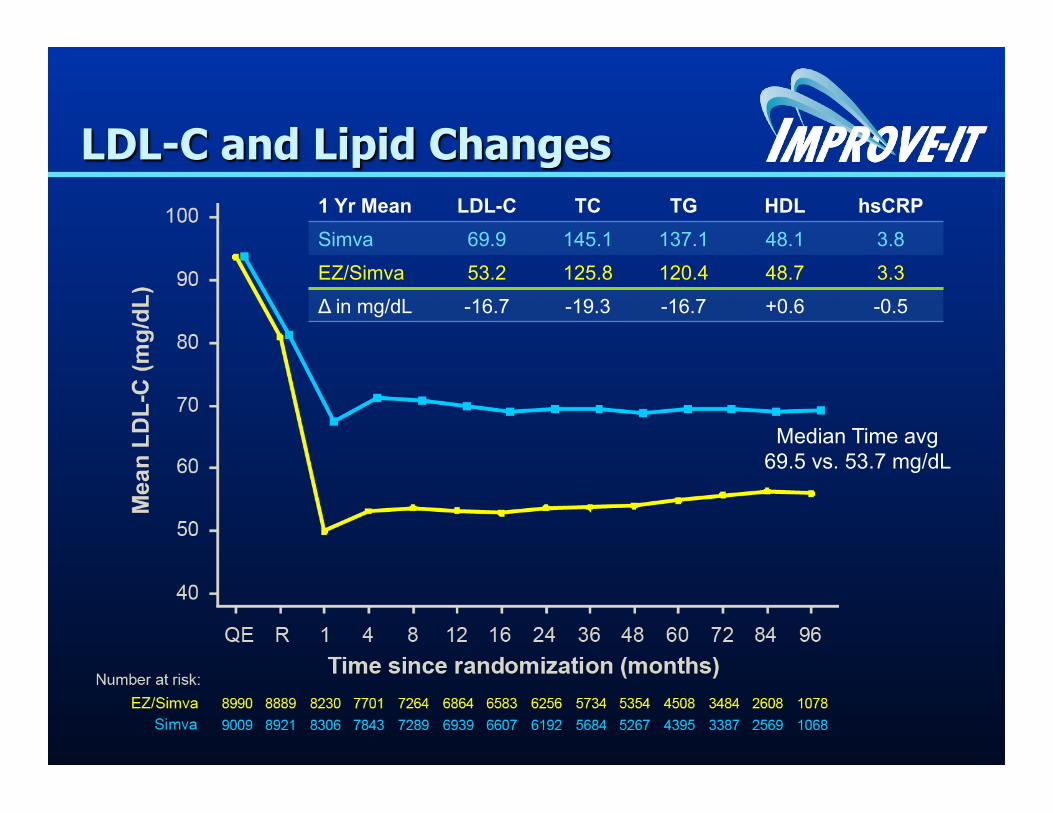
LDL-C and Lipid Changes 1 Yr Mean LDL-C TC TG HDL hsCRP Simva 69.9 145.1 137.1 48.1 3.8
EZ/Simva 53.2 125.8 120.4 48.7 3.3
Δ in mg/dL -16.7 -19.3 -16.7 +0.6 -0.5
Median Time avg 69.5 vs. 53.7 mg/dL

Primary Endpoint — ITT
Simva — 34.7% 2742 events
EZ/Simva — 32.7% 2572 events
HR 0.936 CI (0.887, 0.988) p=0.016
Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization (≥30 days), or stroke
7-year event rates
NNT= 50

Compare genetics vs pharmacology
- 12 mg/dl
- 53%
LDL MI
- 15 mg/dl - 6.4%
LDL MI
NPC1L1 null mutations
Ezetimibe

Hypothesis: lifelong lower LDL ���amplifies effect on MI
- 12 mg/dl
- 53%
LDL MI
- 15 mg/dl - 6.4%
LDL MI
Ezetimibe NPC1L1 null mutations

“You can never be too rich or have too low an LDL.”
…Eugene Braunwald, MD

LPA���Lipopoproetin (a)

Null mutations at LPA lower Lp(a) and reduce MI risk
Ogorelkova, Gruber, Uttermann, Hum Mol Genet (1999) Lim et al., PLoS Genetics (2014)
Lipoprotein (a) (LPA)
1 in 13 carrier
Gene Null mutations
c.4974-2A>G & c.4289+1G>A
Clinical Effect
Lp(a) MI
-60% -14%
Outline
Results: Risk Mutations
LDLR, APOA5
Two Human Genetics Experiments
Experimental Approach
Protective Mutations NPC1L1, LPA LPL, APOC3

LPL ���Lipoprotein lipase

Wittrup et al., Circulation (1999) Varbo et al., J Am Coll Cardiol (2013) Stitziel et al., under review
Lipoprotein lipase (LPL)
1 in 10 carrier
Null mutation at LPL lowers TRL, increases HDL, and reduces MI risk
Gene Null mutations
S447X
Clinical Effect
TRL MI
-10% -17%

APOC3���
Apolipoprotein C-III

Crosby et al. N Engl J Med (2014)
Clinical Effect Apolipoprotein C-III (APOC3)
TRL MI
-39%
IVS1-2GàA IVS2+1GàA
R19X
1 in 150 individuals are heterozygous for
null mutations
Apolipoprotein C-III gene: ���Heterozygous null mutations lower triglycerides

Crosby et al. N Engl J Med (2014)
TRL MI
-39% -40%
IVS1-2GàA IVS2+1GàA
R19X
1 in 150 individuals are heterozygous for
null mutations
Apolipoprotein C-III gene: ���Heterozygous null mutations protect against MI
Clinical Effect Apolipoprotein C-III (APOC3)



These genetic results predict that inhibition of APOC3 should reduce MI risk

TG
- 43%
• Administration of therapeutic to healthy human volunteers
• APOC3 level by 70%
Graham, Circ Res (2013)

TG
- 43%
MI ? • Administration of therapeutic to healthy human volunteers
• APOC3 level by 70%
Graham, Circ Res (2013)
Why are APOC3 mutation ���carriers protected?
People WITHOUT mutation (RR)
People WITH mutation (RX)

Oral fat challenge test��� in mutation non-carriers and carriers
People WITHOUT mutation (RR)
People WITH mutation (RX)
Dietary fat challenge

After a high-fat meal, ���plasma triglycerides normally increase
Pollin, Science 2008

In APOC3 null mutation carriers, ���triglycerides increase is markedly blunted
Pollin, Science 2008

Now, six protective mutation examples for MI
PCSK9
NPC1L1
LPA
LPL
APOC3
ANGPTL4
1 in 50 blacks 1 in 150 1 in 13 1 in 10 1 in 150 1 in 500
LDL LDL Lp(a) TRL TRL TRL
80% lower risk
53% lower risk
14% lower risk
17% lower risk
40% lower risk
57% lower risk
alirocumab, evolocumab, bococizumab
ezetimibe Antisense in development ?
Antisense in development
Monoclonal antibodies in development
MI
Take Home #1: Multiple genes suggest ���post-prandial lipoprotein metabolism ���
as key mechanism for atherosclerosis (beyond LDL)
Zilversmit, Circulation (1979)

Post-prandial TRL metabolism genes ���with compelling human genetic evidence
Lipoprotein Lipase
APOA5
APOC3 ANGPTL4 ANGPTL3

Mutations in all five genes affect plasma TRL,���in 4 affect MI risk,���
3 with protective null alleles
Lipoprotein Lipase
APOA5
APOC3 ANGPTL4 ANGPTL3

HDL
LDL
IDL VLDL Chylomicron Remnant
apo A-I apo B apo B apo B apo B48
Cholesterol Triglyceride
Take Home #2: human genetic studies uniformly point to apoB-containing lipoproteins as
key drivers of atherosclerosis
Lp(a)
apo B
apo(a)
Triglyceride-rich lipoproteins (TRLs)

Leverage naturally-occurring variation in target genes to anticipate
efficacy (and side effects) of medicines

Acknowledgments Kathiresan laboratory Broad Genomics Platform
Stacey Gabriel, PhD
Collaborators
Funding
MGH: Research Scholar Award