kath_dch treatment guidelines
DESCRIPTION
Health document for practicing doctorsTRANSCRIPT
TREATMENT TREATMENT TREATMENT TREATMENT GUIDELINESGUIDELINESGUIDELINESGUIDELINES 2010201020102010
CHILD HEALTH DIRECTORATE CHILD HEALTH DIRECTORATE CHILD HEALTH DIRECTORATE CHILD HEALTH DIRECTORATE
KOMFO ANOKYE TEACHING HOSPITAL KOMFO ANOKYE TEACHING HOSPITAL KOMFO ANOKYE TEACHING HOSPITAL KOMFO ANOKYE TEACHING HOSPITAL
KUMASIKUMASIKUMASIKUMASI ---- GHANAGHANAGHANAGHANA
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
i
TABLE OF CONTENTS
TABLE OF CONTENTS ........................................................................................................................................................ I
FOREWORD ..................................................................................................................................................................... V
PREFACE TO HANDBOOK ON DEPARTMENTAL PROTOCOLS ........................................................................................... VI
PROTOCOL REVIEW COMMITTEE ...................................................................................................................................VII
LIST OF CONTRIBUTORS ................................................................................................................................................. VIII
1.0 PAEDIATRIC RESUSCITATION ............................................................................................................................ 1
1.1.0 CARDIOPULMONARY RESUSCITATION ................................................................................................................... 1
SUMMARY OF ABCD MANEUVERS .............................................................................................................................. 3
1.2.0 AIRWAY AND BREATHING MANAGEMENT PROTOCOL ........................................................................................... 4
1.3.0 ASYSTOLE ............................................................................................................................................................... 5
1.3.1 FIRST STEPS ....................................................................................................................................................... 5
1.3.2 PULSELESS ELECTRICAL ACTIVITY �Not Shockable � Remember PEA ........................................................... 5
1.3.3 ASYSTOLE � Not shockable � Remember DEAD ....................................................................................... 5
1.2.0 ANAPHYLAXIS.......................................................................................................................................................... 7
ANAPHYLAXIS TREATMENT ALGORITHM .................................................................................................................... 9
2.0 NEUROLOGICAL DISORDERS ............................................................................................................................ 11
2.1.0 CONVULSIONS / SEIZURE DISORDERS ................................................................................................................... 11
2.1.1 DEFINITIONS AND CLASSIFICATION .................................................................................................................. 11
2.1.2 GENERAL AETIOLOGY OF CONVULSIVE DISORDERS ........................................................................................ 12
2.1.3 DIAGNOSIS........................................................................................................................................................ 12
2.1.4 ACUTE MANAGEMENT OF SEIZURES / CONVULSIONS ..................................................................................... 13
ACUTE MANAGEMENT .............................................................................................................................................. 15
2.1.5 OTHER INVESTIGATIONS TO SUPPORT DIAGNOSIS OF EPILEPSY ..................................................................... 16
2.1.6 DIFFERENTIAL DIAGNOSIS ................................................................................................................................ 18
2.1.7 ANTIEPILEPTIC DRUG (AED) THERAPY .............................................................................................................. 19
2.1.8 SURGERY FOR EPILEPSY .................................................................................................................................... 22
2.1.9 PSYCHOLOGICAL MANAGEMENT ..................................................................................................................... 22
2.1.10 OTHER PROBLEMS ASSOCIATED WITH EPILEPSY THAT NEED THE PHYSICIANS ATTENTION ......................... 22
2.1.11 INTEGRATED EPILEPSY SERVICE (MULTI-DISCIPLINARY) ................................................................................ 23
2.1.12 OUTCOME OF TREATMENT ............................................................................................................................ 23
2.2.1 ACUTE FLACCID PARALYSIS ................................................................................................................................... 24
2.2.2 MANAGEMENT OF POLIOMYELITIS ....................................................................................................................... 25
2.2.3 MANAGEMENT OF GUILLAIN-BARRE SYNDROME................................................................................................. 25
2.3.0 ACUTE ENCEPHALOPATHY / NON TRAUMATIC COMA .......................................................................................... 26
2.3.1 SOME COMMONLY USED COMA SCALES .............................................................................................................. 28
3.0 CARDIAC DISORDERS ...................................................................................................................................... 30
3.1.0 ACUTE HYPERTENSION ......................................................................................................................................... 30
3.2.0 HEART FAILURE ..................................................................................................................................................... 32
3.3.0 INFECTIVE ENDOCARDITIS (IE) .............................................................................................................................. 34
3.4.0 RHEUMATIC HEART DISEASE ................................................................................................................................. 36
3.5.0 TETRALOGY OF FALLOT (TOF) AND HYPERCYANOTIC (TET) SPELL ......................................................................... 38
4.0 HAEMATOLOGICAL DISORDERS ....................................................................................................................... 39
4.1.0 SICKLE CELL DISEASE ............................................................................................................................................. 39
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
ii
4.1.1 INFECTION (MALARIA/SEPSIS/PNEUMONIA/OSTEOMYELITIS/UTIS ETC) ........................................................ 39
4.1.2 HYPERHEMOLYTIC CRISIS ................................................................................................................................. 40
4.1.3 SPLENIC SEQUESTRATION (MASSIVE RBCS + PLASMA SEQUESTRATION IN SPLEEN) ....................................... 40
4.1.4 APLASTIC CRISIS (CESSATION OF ERYTHROPOIESIS) ......................................................................................... 40
4.1.5 VASO-OCCLUSIVE CRISIS ................................................................................................................................... 41
4.1.5.1 PRIAPISM .............................................................................................................................................................................. 42
4.1.5.2 ACUTE CHEST SYNDROME (PNEUMONIA/INFARCT) ......................................................................................................... 42
4.1.5.3 CVA ........................................................................................................................................................................................ 42
4.1.6 INDICATIONS FOR BLOOD TRANSFUSION: ....................................................................................................... 42
4.1.7 CHRONIC COMPLICATIONS ............................................................................................................................... 42
4.2.0 ANAEMIA TRANSFUSION ALGORITHM .................................................................................................................. 44
5.0 INFECTIOUS DISEASES ..................................................................................................................................... 45
5.1.0 MENINGITIS .......................................................................................................................................................... 45
5.2.0 SEVERE MALARIA .................................................................................................................................................. 48
5.2.1 CEREBRAL MALARIA ......................................................................................................................................... 48
5.2.2 MALARIA TREATMENT SUMMARY IN MALARIA ENDEMIC REGION ................................................................. 50
5.3.0 TETANUS ............................................................................................................................................................... 51
6.0 MALNUTRITION.............................................................................................................................................. 53
6.1.0 DEFINITION AND GENERAL GUIDELINES .......................................................................................................................... 53
CLASSIFICATION OF MALNUTRITION .............................................................................................................................................. 53
CLINICAL MANAGEMENT ................................................................................................................................................................. 53
6.1.1 TREATMENT OF SPECIFIC PROBLEMS OF THE SEVERELY MALNOURISHED ........................................................... 54
6.1.2 ROUTINE TREATMENT FOR THE MALNOURISHED ................................................................................................ 55
6.1.3 IMPORTANT THINGS NOT TO DO .......................................................................................................................... 55
6.1.4 SUMMARY OF WHO RECOMMENDATION FOR DIAGNOSIS AND MANAGEMENT OF SEREVE ACUTE
MALNUTRITION (SAM) IN CHILDREN ............................................................................................................................. 56
6.1.5 GUIDANCE TABLE TO IDENTIFY THE TARGET WEIGHT FOR DISCHARGE ................................................................ 57
7.0 NEONATAL DISORDERS ................................................................................................................................... 58
7.1.0 INTRODUCTION..................................................................................................................................................... 58
7.1.1 NEONATAL RESUSCITATION .................................................................................................................................. 58
RISK FACTORS ASSOCIATED WITH THE NEED FOR RESUSCITATION .......................................................................... 58
A B C’s of RESUSCITATION ......................................................................................................................................... 59
RESUSCITATION ALGORITHM .................................................................................................................................... 60
BAG-AND-MASK VENTILATION .................................................................................................................................. 61
CHEST COMPRESSIONS .............................................................................................................................................. 62
ENDOTRACHEAL INTUBATION ................................................................................................................................... 63
7.2.0 BIRTH ASPHYXIA .................................................................................................................................................... 66
7.2.1 CLINICAL STAGES OF BIRTH ASPHYXIA (Perinatal Hypoxic Ischemic Encephalopathy) .................................... 68
7.3.0 NEONATAL SEIZURES: ........................................................................................................................................... 69
7.4.0 ANAEMIA IN THE NEWBORN ................................................................................................................................. 70
7.4.1 COMMON CAUSES OF ANAEMIA IN THE NEWBORN ....................................................................................... 70
7.4.2 CLINICAL FEATURES OF ANAEMIA IN THE NEWBORN ...................................................................................... 71
7.4.3 MANAGEMENT ................................................................................................................................................. 72
7.5.0 GUIDELINES FOR THE MANAGEMENT OF RESPIRATORY DIFFCULTY IN THE NEWBORN ....................................... 74
7.6.0 FEEDING PROTOCOL FOR BABIES ADMITTED TO THE MOTHER BABY UNIT, ......................................................... 75
7.7.0 GUIDELINES FOR THE MANAGEMENT OF NEONATAL JAUNDICE .......................................................................... 78
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
iii
7.7.1 PREPARATION FOR AN EXCHANGE BLOOD TRANSFUSION. ............................................................................. 78
7.7.2 PERFORMING THE EXCHANGE BLOOD TRANSFUSION (EBT) ............................................................................ 79
7.8.0 GUIDELINES TO THE MANAGEMENT OF THE HIV EXPOSED BABY ......................................................................... 80
7.9.0 MANAGEMENT OF COMMON BIRTH INJURIES ..................................................................................................... 81
7.9.1 CEPHALHAEMATOMA ...................................................................................................................................... 81
7.9.2 SUBGALEAL/SUBAPONEUROTIC HAEMATOMA ............................................................................................... 81
7.9.3 FRACTURED FEMUR ......................................................................................................................................... 81
7.9.4 FRACTURED HUMERUS .................................................................................................................................... 82
7.10.0 MANAGEMENT OF NEONATAL TETANUS (NNT) ................................................................................................. 83
7.10.1 AIMS OF MANAGEMENT ................................................................................................................................ 83
7.10.2 SPECIFIC STEPS TO TAKE ................................................................................................................................. 83
7.11.0 KANGAROO MOTHER CARE (KMC) ...................................................................................................................... 84
7.12.0 ANTIBIOTIC PROTOCOL FOR BABIES ADMITTED TO MBU ................................................................................... 85
8.0 FLUID & METABOLIC DISORDERS ..................................................................................................................... 86
8.1.0 DIABETIC HYPERGLYCEMIC CRISIS/COMA ............................................................................................................. 86
9.0 ONCOLOGICAL DISORDERS ............................................................................................................................. 88
9.1.0 METABOLIC AND ONCOLOGIC EMERGENCIES ...................................................................................................... 88
9.1.1 TUMOUR LYSIS SYNDROME .................................................................................................................................. 88
9.1.2 FEBRILE NEUTROPENIA ......................................................................................................................................... 89
9.2.0 BASIC INVESTIGATIONS FOR ALL ONCOLOGY PATIENTS ....................................................................................... 90
9.3.0 RETINOBLASTOMA ................................................................................................................................................ 91
9.4.0 RHABDOMYOSARCOMA ....................................................................................................................................... 92
9.5.0 BURKITT’S LYMPHOMA ......................................................................................................................................... 93
9.6.0 HODGKIN’S LYMPHOMA ....................................................................................................................................... 95
9.6.1 TREATMENT PATHWAY IN STAGE II +III HODGKIN’S DISEASE ................................................................................ 96
9.7.0 WILM’S TUMOUR .................................................................................................................................................. 97
9.8.0 PAEDIATRIC ACUTE LYMPHOBLASTIC LEUKAEMIA (ALL) ....................................................................................... 98
9.8.1 PRE-TREATMENT PHASE ................................................................................................................................... 98
9.8.2 REGIMEN A INDUCTION ................................................................................................................................... 98
9.8.3 REGIMEN B INDUCTION ................................................................................................................................... 99
9.8.4 MAINTENANCE ................................................................................................................................................. 99
9.9.0 SOME COMMON DRUGS USED IN PAEDIATRIC ONCOLOGY PATIENTS ............................................................... 104
10.0 PAEDIATRIC EMERGENCIES ......................................................................................................................... 105
10.1.0 HYPOGLYCAEMIA .............................................................................................................................................. 105
10.2.0 FLUID THERAPY ................................................................................................................................................. 107
10.2.1 SHOCK ............................................................................................................................................................... 107
10.2.2 NORMAL MAINTENNANCE FLUIDS ................................................................................................................... 109
10.2.3 DIARRHEA AND DEHYDRATION ......................................................................................................................... 111
10.2.4 DIARRHOEA / DEHYDRATION (EXCLUDING SEVERE MALNUTRITION) ALGORTHM ........................................... 113
11.0 RENAL DISORDERS ...................................................................................................................................... 114
11.1.0 GENERAL GUIDE FOR ALL RENAL CASES ............................................................................................................ 114
11.2.0 DIETARY ADVICE FOR RENAL CASE .................................................................................................................... 115
11.3.0 NEPHRITIC SYNDROME (ACUTE GLOMERULONEPHRITIS) ................................................................................ 116
11.3.1 CLINICAL DEFINITION/CRITERIA ................................................................................................................... 116
11.3.2 MANAGEMENT GUIDELINES FOR NEPHRITIC SYNDROME (AGN) ................................................................ 116
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
iv
11.3.3 COMPLICATIONS & THEIR MANAGEMENT ................................................................................................... 117
11.4.0 NEPHROTIC SYNDROME.................................................................................................................................... 119
11.4.1 CLINICAL DEFINITION/CRITERIA FOR NEPHROTIC SYNDROME: ................................................................... 119
11.4.2 MANAGEMENT GUIDELINES FOR NEPHROTIC SYNDROME.......................................................................... 119
11.4.3 SECONDARY CAUSES OF NEPHROTIC SYNDROME ........................................................................................ 123
11.4.4 COMPLICATIONS OF NEPHROTIC SYNDROME & THEIR MANAGEMENT ...................................................... 124
11.5.0 URINARY TRACT INFECTION .............................................................................................................................. 126
11.6.0 ACUTE RENAL FAILURE ...................................................................................................................................... 128
11.7.0 CHRONIC RENAL FAILURE/CHRONIC KIDNEY DISEASE ...................................................................................... 132
12.0 RESPIRATORY DISORDERS ........................................................................................................................... 134
12.1.0 INTRODUCTION ................................................................................................................................................ 134
12.2.0 RESPIRATORY FAILURE ...................................................................................................................................... 135
12.3.0 CROUP .............................................................................................................................................................. 136
12.4.0 ASTHMA ............................................................................................................................................................ 139
12.5.0 APPROACH TO PNEUMONIAS ........................................................................................................................... 144
12.6.0 ATYPICAL PNEUMONIAS ................................................................................................................................... 146
12.7.0 PAEDIATRIC PULMONARY TUBERCULOSIS ........................................................................................................ 147
13.0 MISCELLANEOUS DISORDERS ...................................................................................................................... 149
13.1.0 SNAKE BITES ...................................................................................................................................................... 149
13.1.1 RECOGNITION OF VENOMOUS SNAKES ....................................................................................................... 149
13.1.2 CLINICAL FEATURES ...................................................................................................................................... 149
13.1.3 MANAGEMENT ............................................................................................................................................. 150
13.1.4 INDICATION FOR ANTIVENOM ..................................................................................................................... 150
13.1.5 ADMINISTRATION OF ANTIVENOM .............................................................................................................. 151
13.2.0 POISONING IN CHILDREN .................................................................................................................................. 152
13.3.0 SPECIFIC POISONING ......................................................................................................................................... 155
13.3.1 HYDROCARBONS .......................................................................................................................................... 155
13.3.2 CAUSTIC INGESTIONS ................................................................................................................................... 156
13.3.3 IRON POISONING .......................................................................................................................................... 157
13.3.4 PESTICIDES.................................................................................................................................................... 158
14.0 APPENDIX .................................................................................................................................................. 159
DRUGS IV/IO INFUSIONS TABLE ................................................................................................................................... 159
DRUG COMPATIBILITY TABLE ....................................................................................................................................... 160
DIGOXIN DIGITALIZATION AND MAINTENANCE DOSE TABLE ...................................................................................... 160
USEFUL FORMULAES ................................................................................................................................................... 161
RESPIRATORY AND HEART RATE REFERENCE FOR AGE ................................................................................................ 162
ESTIMATING BODY SURFACE AREA .............................................................................................................................. 162
WHO WEIGHT-FOR-LENGTH REFERENCE TABLE (45 -86CM) ....................................................................................... 163
WHO WEIGHT-FOR-LENGTH REFERENCE TABLE (87 -120CM) ..................................................................................... 164

Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
v
FOREWORD Over a decade ago the first treatment protocol for the department was developed.
With the changing world and new advances in medicine, our energetic, Residents and Specialists under the
current Head of Department, Dr Addo-Yobo, have upgraded the previous one.
It does not replace the textbook but inspires the user and introduces to the Doctor and patient simple
practical and effective treatment within the subregion.
Definitely the time spent on this is worth the effort and will surely bring smiles to the faces of patients.
Prof. Ben Baffoe Bonnie
MD, FAFpaed, FWACPpaed, FGCP
Consultant Paediatrician
Second Head of Department, Child Health.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
vi
PREFACE TO HANDBOOK ON DEPARTMENTAL PROTOCOLS
Established in 1975, the Department of Child Health, Komfo Anokye Teaching Hospital/School of Medical
Sciences, KNUST has seen significant developments from a clinical staff of less than 10 to the current state
as a centre for postgraduate training with of over 60 doctors, about 70% of whom are house officers and
residents. Certainly the number of clients and scope of services provided have also increased thus making it
necessary to develop subspecialty in the context of our practice.
From a twin general paediatric ward with a nursery in the 1980s the department now has 5 subunits based
on subspecialty. These are, Mother Baby Unit (MBU), Paediatric Emergency Unit (PEU), and three wards for
Cardiovascular/Respiratory, Haematology/Oncology and Infectious diseases (HIV)/Malnutrition/Renal
disorders respectively. All wards in addition take on patients with other miscellaneous disorders.
The first manual on paediatric protocols was written under the headship of the late Professor A.P. Asafo-
Agyei, the first Head of Department in the late 1980s as a pocket book. Since then, various departmental
protocols have been developed in specific areas on different wards at different times.
This current manual/handbook of paediatric treatment guidelines is an update of all previous forms and
versions from various wards and has been organized in accordance with functional structure of the
department as a quick treatment guide for House officers, Residents and other doctors, for the
management of a number of neonatal and general paediatric disorders as well as emergencies, as are
commonly seen. It is the joint effort of specialists and consultants from our various subunits.
It is hoped that this manual would continue to be useful to medical officers, residents as they leave our
teaching hospital and other clinical child health care practitioners outside the teaching hospital would also
find it helpful in the management of their patients.
The Department is especially grateful to members of the protocol review committee for compiling and
organizing the manual. It is our hope that the content would be updated yearly in accordance with current
paediatric practice.
E.O.D ADDO-YOBO Bsc, MB CHB, DTCH, MSc, MWACP, MD, FGCP
HEAD OF DEPARTMENT
2010
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
vii
PROTOCOL REVIEW COMMITTEE Dr. Justice Sylverken (Chairman)
Dr. E.O.D Addo-Yobo
Dr. Charles K.A. Poku
Dr. Alex Osei-Akoto
Dr. Sampson Antwi
Dr. Daniel Ansong
Dr. (Mrs) Gyikua Plange-Rhule
Dr. Joslin A. Dogbe
Dr. Samuel Blay Nguah
Dr. Charles K. Hammond
Dr. Emmanuel Ameyaw
Dr. Frank Serebour
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
viii
LIST OF CONTRIBUTORS
SECTION CONTRIBUTORS
1. Paediatric Resuscitation - Dr. Justice Sylverken
- Dr Charles K.A Poku
2. Neurological disorders - Dr. Charles K. Hammond
- Dr. Joslin A. Dogbe
- Dr. Justice Sylverken
3. Cardiac Disorder - Dr. Samuel Blay Nguah
- Dr. Justice Sylverken
4. Haematological Disorders - Dr. Alex Osei-Akoto
- Dr. Justice Sylverken
Dr Daniel Ansong
5. Infectious Disease - Dr. Justice Sylverken
Dr. Daniel Ansong
6. Malnutrition - Dr. Sampson Antwi
- Dr. Justice Sylverken
7. Neonatal Disorders - Dr. (Mrs) Gyikua Plange-Rhule
- Dr. Priscilla Wobil
- Dr. Frank Serebour
8. Fluid and Metabolic Disorders - Dr. Justice Sylverken
9. Oncology Disorders - Dr. Vivian Paintsil
- Dr. Alex Osei-Akoto
Dr Charles K. Hammond
- Dr. Justice Sylverken
10. Paediatric Emergencies - Dr. Justice Sylverken
- Dr. E.O.D. Addo-Yobo
11. Renal Disorders - Dr. Sampson Antwi
- Dr. Charles K.A. Poku
12. Respiratory Disorders - Dr. Samuel Blay Nguah
- Dr. E.O.D. Addo-Yobo
- Dr. Anthony Enimil
- Dr. Justice Sylverken
13. Snake Bite - Dr. Justice Sylverken
14. Poisoning in Children - Dr. Justice Sylverken
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
1
1.0 PAEDIATRIC RESUSCITATION 1.1.0 CARDIOPULMONARY RESUSCITATION
INDICATION
• Cardiac arrest.
• Respiratory arrest.
• Cardiopulmonary arrest
• No valid Do Not Attempt Resuscitation order.
CONTRAINDICATION
• Rigor mortis
• Dependent lividity
• Corneal clouding
• Decapitation
• No physiologic benefit can be expected because the patient’s vital functions have deteriorated
despite maximum therapy for specific conditions.
ASSESSMENT
Rarely is cardiopulmonary arrest (CPA) a sudden event in children. Prior to CPA, signs due to underlying
aetiology will predominate and may include the following:
Tachycardia, bradycardia.
Tachypnoea, dyspnoea, bradypnoea.
Grey, mottled colouring.
Stupor.
Without intervention, patients may progress to:
Apnea.
Pulselessness / asystole.
Cyanosis.
Unresponsiveness.
Dilated, fixed pupils.
Later findings of irreversible death:
Rigor mortis
Dependent lividity
Corneal clouding
INITIAL INVESTIGATION
Blood glucose is mandatory
Other laboratory investigations are rarely useful during CPR, may consider the following;
Blood gases, BUN, creatinine, electrolytes,full blood count, LFT’s & toxicology.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
2
TREATMENT
ABCDs
Rapid and sequential assessment of the ABCs.
a. Airway patency
Insure airway patency, by positioning, suction, adjunctive airways, foreign body removal.
b. Breathing
Use bag-valve mask ventilation, with/without cricoid pressure.
Endotracheal intubation: suction, oxygen, equipment, medication, monitors.
Cricothyriodotomy: for a complete upper airway obstruction only, when unable to orotracheally intubate.
c. Circulation
Chest compressions for patients in cardiac arrest, profound tachycardia / bradycardia (adequately hydrated
child) without a palpable pulse.
Gain intravascular access. Use quickest, largest, most accessible site.
Intraosseous access for asystolic or severely compromised.
Expand intravascular volume with 20ml/kg normal saline or Ringers Lactate
Treat arrhythmias.
d. Drugs
Give 100% oxygen to all patients
Give 10% Dextrose @ 5ml/kg for documented or suspected hypoglycaemia.
Other common resuscitation medications
Adrenaline: Use for asystole, profound bradycardia, pulseless ventricular tachycardia (VT),
ventricular fibrillation (VF), hypotension due to myocardial dysfunction.
Standard dosage:-Adrenaline (1:10000) first dose 0.1ml/kg IV or IO
Subsequent doses: 0.1ml/kg IV or IO repeat 3-5min (or 10 × 15:2 CPR cycles )
Contraindication:-Hypertension.
Main side effects:-Tachycardia, arrhythmias.
Atropine: symptomatic or vagally mediated bradycardia @ 0.02mg/kg (min 0.1mg), Q20min
Lidocaine: VT, VF frequent PVCs @ 1mg/kg Q5-10min
Naloxone: suspected opiate overdose @ 0.1mg/kg Q15 – 30min
Sodium bicarbonate: severe metabolic acidosis (pH ≤ 7.2) or prolong CPA.@ 1mEq/kg over 15-30min
Adenosine: supraventricular tachycardia (SVT) @ 0.05 – 0.25mg/kg increase by 0.05mg/kg
Q2min up to 0.25mg/kg (or 12mg)
Antibiotics: suspected infection
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
3
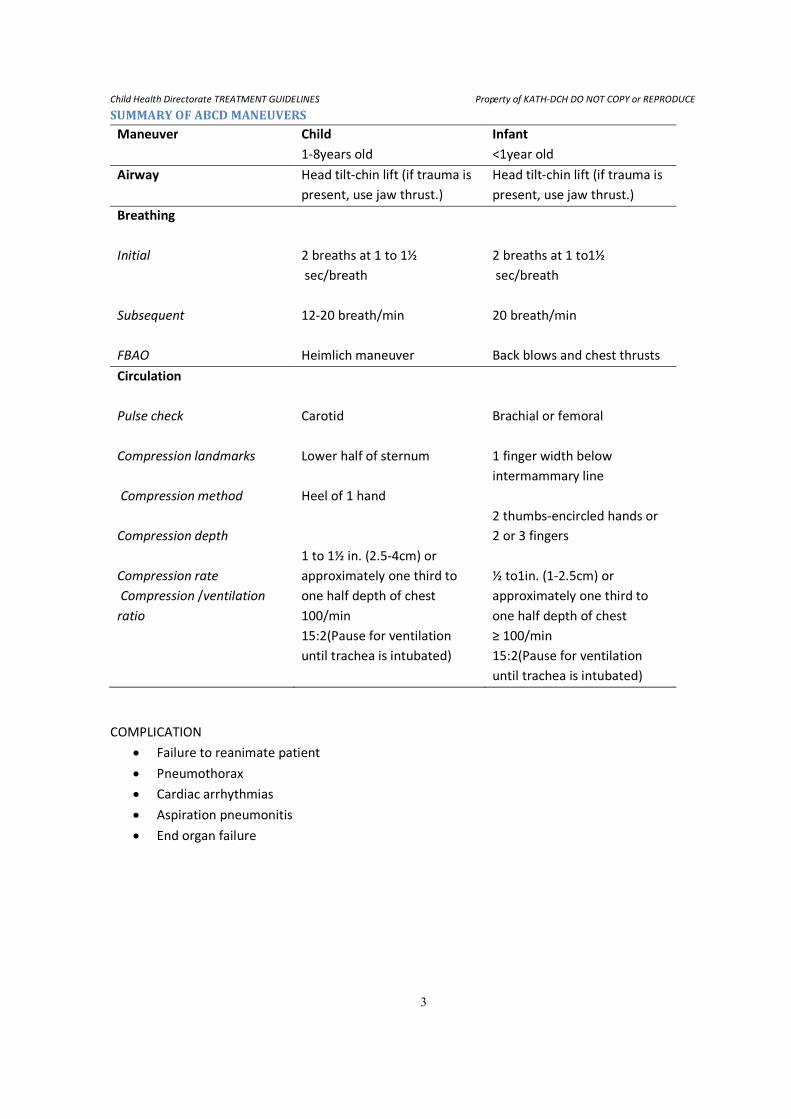
SUMMARY OF ABCD MANEUVERS
Maneuver Child
1-8years old
Infant
<1year old
Airway Head tilt-chin lift (if trauma is
present, use jaw thrust.)
Head tilt-chin lift (if trauma is
present, use jaw thrust.)
Breathing
Initial
Subsequent
FBAO
2 breaths at 1 to 1½
sec/breath
12-20 breath/min
Heimlich maneuver
2 breaths at 1 to1½
sec/breath
20 breath/min
Back blows and chest thrusts
Circulation
Pulse check
Compression landmarks
Compression method
Compression depth
Compression rate
Compression /ventilation
ratio
Carotid
Lower half of sternum
Heel of 1 hand
1 to 1½ in. (2.5-4cm) or
approximately one third to
one half depth of chest
100/min
15:2(Pause for ventilation
until trachea is intubated)
Brachial or femoral
1 finger width below
intermammary line
2 thumbs-encircled hands or
2 or 3 fingers
½ to1in. (1-2.5cm) or
approximately one third to
one half depth of chest
≥ 100/min
15:2(Pause for ventilation
until trachea is intubated)
COMPLICATION
• Failure to reanimate patient
• Pneumothorax
• Cardiac arrhythmias
• Aspiration pneumonitis
• End organ failure
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
4
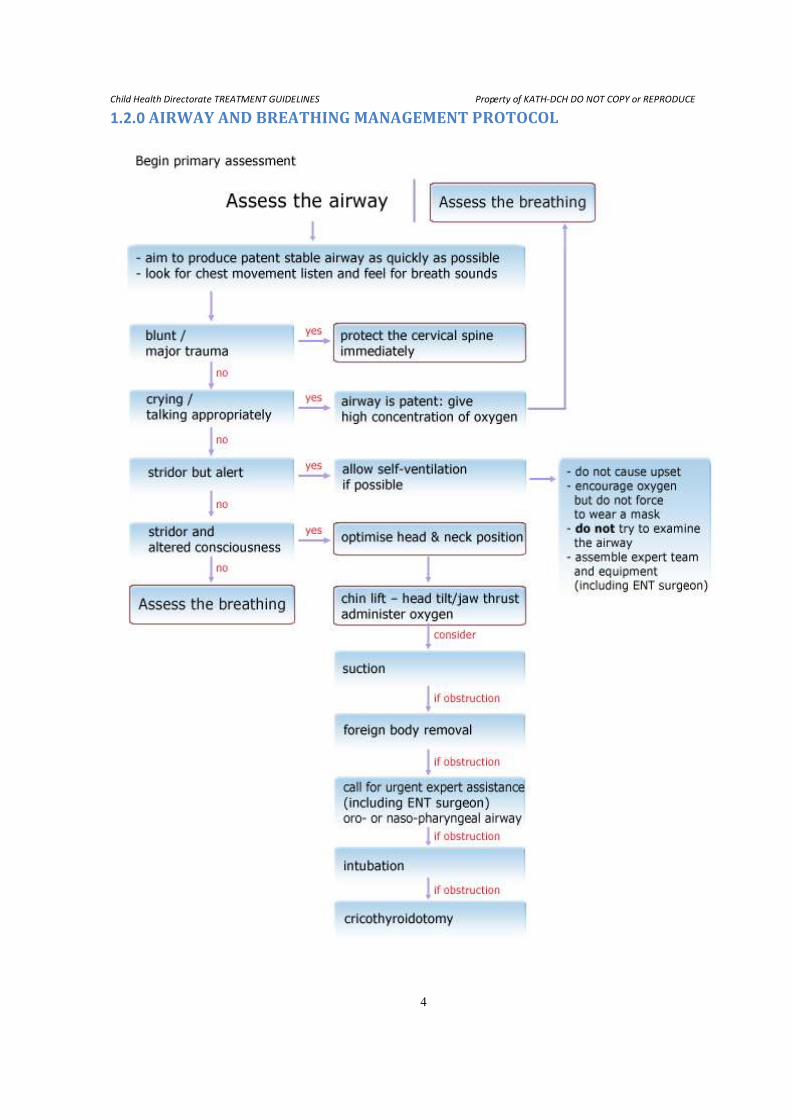
1.2.0 AIRWAY AND BREATHING MANAGEMENT PROTOCOL
Child Health Directorate TREATMENT GUIDELINES
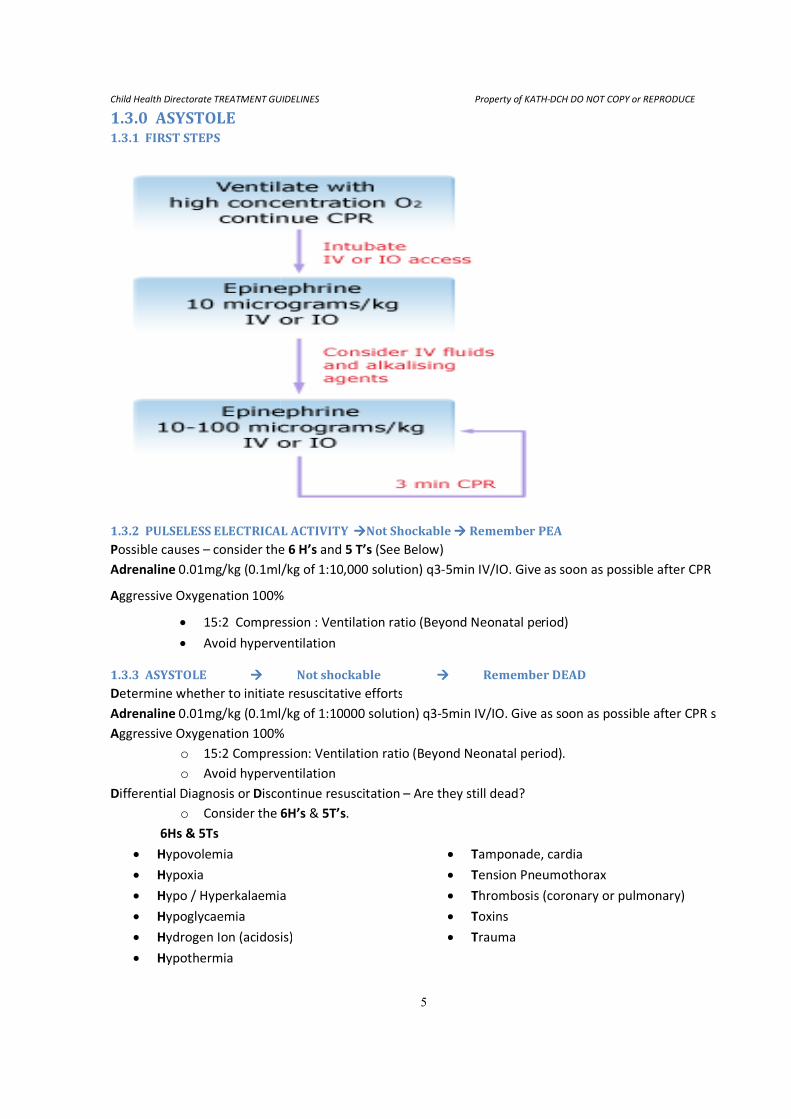
1.3.0 ASYSTOLE 1.3.1 FIRST STEPS
1.3.2 PULSELESS ELECTRICAL ACTIVITY Possible causes – consider the
Adrenaline 0.01mg/kg (0.1ml/kg of 1:10
Aggressive Oxygenation 100%
• 15:2 Compression : Ventilation ratio (Beyond Neonatal period)
• Avoid hyperventilation
1.3.3 ASYSTOLE ���� Determine whether to initiate resuscitative efforts
Adrenaline 0.01mg/kg (0.1ml/kg of 1:10
Aggressive Oxygenation 100%
o 15:2 Compression
o Avoid hyperventilation
Differential Diagnosis or Discontinue resuscitation
o Consider the 6
6Hs & 5Ts
• Hypovolemia
• Hypoxia
• Hypo / Hyperkalaemia
• Hypoglycaemia
• Hydrogen Ion (acidosis)
• Hypothermia
TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
5
ELECTRICAL ACTIVITY ����Not Shockable ���� Remember PEAconsider the 6 H’s and 5 T’s (See Below)
0.01mg/kg (0.1ml/kg of 1:10,000 solution) q3-5min IV/IO. Give as soon as possible after CPR
100%
Compression : Ventilation ratio (Beyond Neonatal period)
Avoid hyperventilation
Not shockable ���� Remember DEADetermine whether to initiate resuscitative efforts
0.01mg/kg (0.1ml/kg of 1:10000 solution) q3-5min IV/IO. Give as s
ggressive Oxygenation 100%
15:2 Compression: Ventilation ratio (Beyond Neonatal period)
Avoid hyperventilation
iscontinue resuscitation – Are they still dead?
6H’s & 5T’s.
• Tamponade, cardia
• Tension Pneumothorax
ypo / Hyperkalaemia • Thrombosis (coronary or pulmonary)
• Toxins
ydrogen Ion (acidosis) • Trauma
DCH DO NOT COPY or REPRODUCE
Remember PEA
as soon as possible after CPR
Compression : Ventilation ratio (Beyond Neonatal period)
Remember DEAD
5min IV/IO. Give as soon as possible after CPR s
(Beyond Neonatal period).
amponade, cardia
ension Pneumothorax
hrombosis (coronary or pulmonary)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
6
WHEN TO STOP RESUSCITATION
Resuscitation efforts are unlikely to be successful and can be discontinued if there is no return of
spontaneous circulation at any time after three ‘rounds’ of medication despite optimal resuscitation efforts-
usually 30 minutes of cumulative life support, and in the absence of recurring or refractory VF/VT.
Exceptions are patients with a history of poisoning or a primary hypothermic insult in whom prolonged
attempts may occasionally be successful. Prolonged external cardiac compressions provided that central
(femoral arterial) pulses can be felt, may (has) successfully resuscitated children with tricyclic
antidepressant overdoses. Seek expert help from a toxicologist or paediatric intensivist.
BRAIN DEATH
1. Patient must be normothermic and free from sedative or anticonvulsant drugs
2. Patients on mechanical ventilation must be re-examined at least 12 -24 hours after the following
clinical features first noticed
Clinical examination criteria
• Unresponsive to noxious stimuli (trigeminal distribution)
• Fixed dilated pupils
• Absent corneal reflex
• Absent spontaneous eye movements
• Absent oculocephalic (doll’s eye) and/or oculovestibular (caloric) reflex
• Absent cough to deep tracheal stimulation
• Absent suck, gag and rooting reflexes
• Absent spontaneous respiratory effort with PaCo2 > 50mmHg
Auxiliary tests
1. EEG
2. Cerebral blood flow study
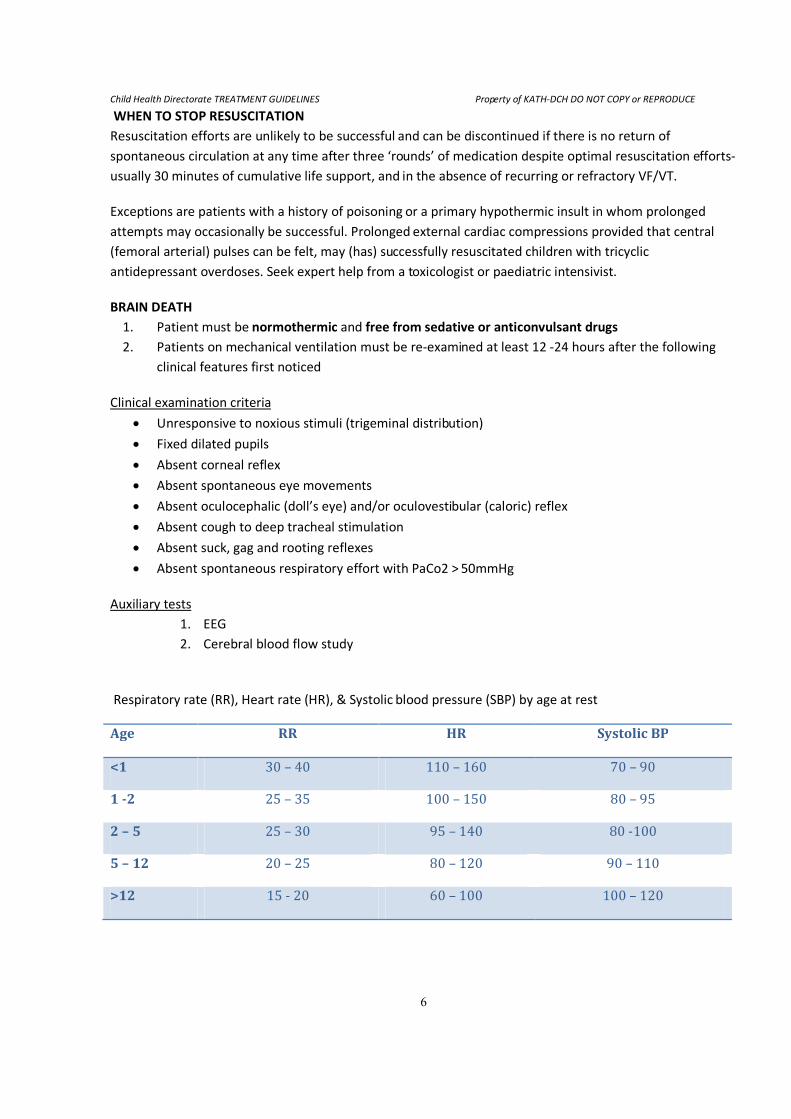
Respiratory rate (RR), Heart rate (HR), & Systolic blood pressure (SBP) by age at rest
Age RR HR Systolic BP
<1 30 – 40 110 – 160 70 – 90
1 -2 25 – 35 100 – 150 80 – 95
2 – 5 25 – 30 95 – 140 80 -100
5 – 12 20 – 25 80 – 120 90 – 110
>12 15 - 20 60 – 100 100 – 120
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
7
1.2.0 ANAPHYLAXIS 1. DEFINITION
Clinical syndrome of allergy or immediate generalized or systemic hypersensitivity to a foreign substance
characterized by rapidly developing, life threatening
• Airway, and/or
• Breathing, and/or
• Circulatory problems
• Usually with skin and/or mucosal changes.
Anaphylaxis commonly presents as one or more of the following:
• Anaphylactic shock
• Angioneurotic oedema
• Bronchoconstriction
• Urticaria
2. COMMON CAUSES
• Drug, vaccines and sera
• Blood /blood product transfusions
• Insect stings
• Food sensitivity
• Skin testing
• Desensitization
3. CLINICAL FEATURES
• Light headedness
• Paraesthesia and pruritus
• Sweating, flushing and palpitations
• Signs of respiratory distress – tachypnoea, apnoea, wheezing, recession, hyperinflation, choking,
stridor, respiratory arrest.
• Low peripheral vascular resistance leading to circulatory collapse and profound shock with
hypotension (SBP < 70 + 2[age in years]).
4. TREATMENT
• Adrenaline 1:1000
- Give IM @ following doses of 1:1000 [Repeat every 5 minutes if no better]
< 6 months 150 microgram (0.15ml)
6 months – 6years 150 microgram (0.15ml)
6 years – 12 years 300 microgram (0.30ml)
>12 years 500 microgram (0.50ml)
- OR May give 0.01ml/kg subcutaneously (or dilute to 1:10,000 and give IV / IO @ 0.1ml/kg)
• Airway
-Maintain a clear airway
-Ensure adequate oxygenation
-Laryngeal oedema may make endotracheal intubation necessary.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
8
• Bronchodilators for respiratory distress or wheezing
- Salbutamol nebulization Q20min × 3 (preferred).
Less than 6 years 2.5mg
6 years and above 5.0mg
(As second line treatment: Aminophylline intravenously @ 5mg/kg/30mins stat, then 1mg/kg/hr.
If patient has been on theophyllines then omit loading dose)
• IV Fluids
-Correct hypovolaemia due to massive exudation of intravascular fluids
-Give 0.9% Normal saline or Ringers Lactate (may give Colloids) 20ml/kg/5 -15min
- Monitor response and give further bolus as necessary
• Steroids
-Hydrocortisone IV @ 4mg/kg (max. dose 200mg) repeat 6hrly till oral therapy tolerated (24-48hrs)
< 6 months 25mg
6 months – 6 years 50mg
6 years – 12 years 100mg
>12 years 200mg
-Then oral Prednisolone 1-2mg/kg/day (to complete 2-5 days of steroids)
• Antihistamines
-Promethazine (Phenergan)
-0.5-1mg/kg (max. dose 50mg) IM stat or slow IV over 5 minutes.
-Chlorphenamine IM or Slow IV, repeat if required up to 4 times in 24 hours
< 6 months 0.25mg/Kg
6 months – 6 years 2.5mg
6 years – 12 years 5mg
>12 years 10mg
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
9
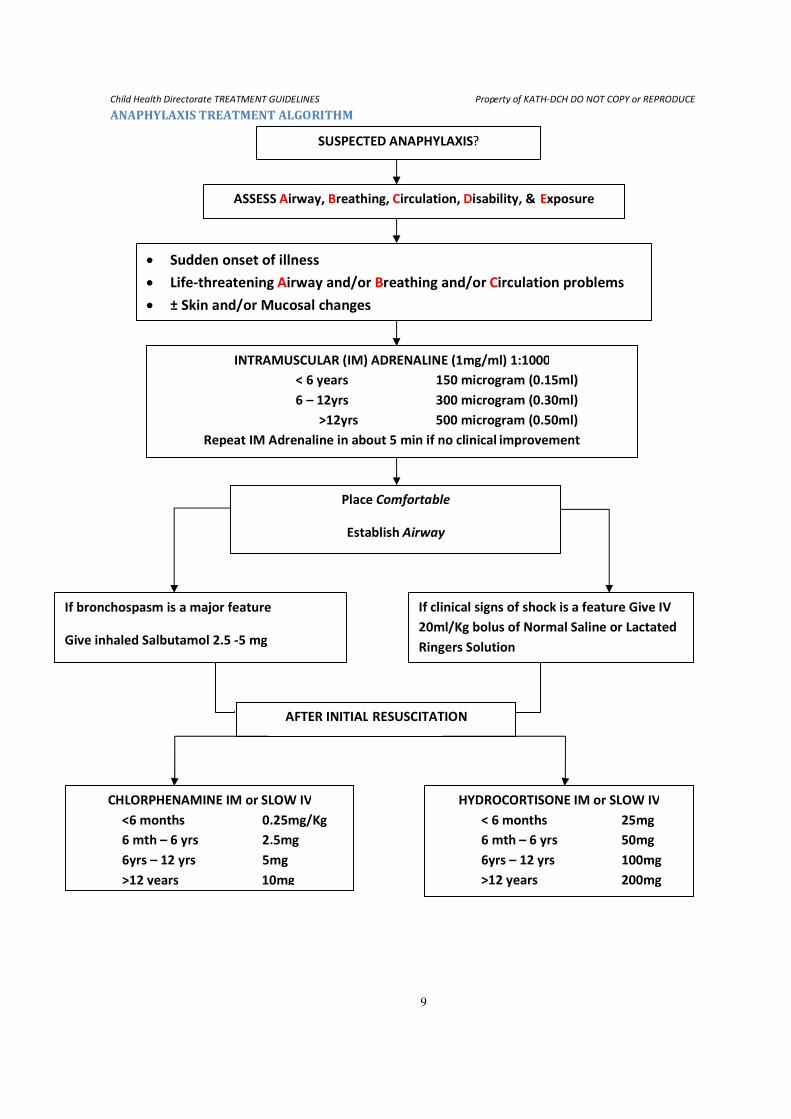
ANAPHYLAXIS TREATMENT ALGORITHM
SUSPECTED ANAPHYLAXIS?
ASSESS Airway, Breathing, Circulation, Disability, & Exposure
• Sudden onset of illness
• Life-threatening Airway and/or Breathing and/or Circulation problems
• ± Skin and/or Mucosal changes
INTRAMUSCULAR (IM) ADRENALINE (1mg/ml) 1:1000
< 6 years 150 microgram (0.15ml)
6 – 12yrs 300 microgram (0.30ml)
>12yrs 500 microgram (0.50ml)
Repeat IM Adrenaline in about 5 min if no clinical improvement
Place Comfortable
Establish Airway
If bronchospasm is a major feature
Give inhaled Salbutamol 2.5 -5 mg
If clinical signs of shock is a feature Give IV
20ml/Kg bolus of Normal Saline or Lactated
Ringers Solution
AFTER INITIAL RESUSCITATION
CHLORPHENAMINE IM or SLOW IV
<6 months 0.25mg/Kg
6 mth – 6 yrs 2.5mg
6yrs – 12 yrs 5mg
>12 years 10mg
HYDROCORTISONE IM or SLOW IV
< 6 months 25mg
6 mth – 6 yrs 50mg
6yrs – 12 yrs 100mg
>12 years 200mg
Child Health Directorate TREATMENT GUIDELINES
TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
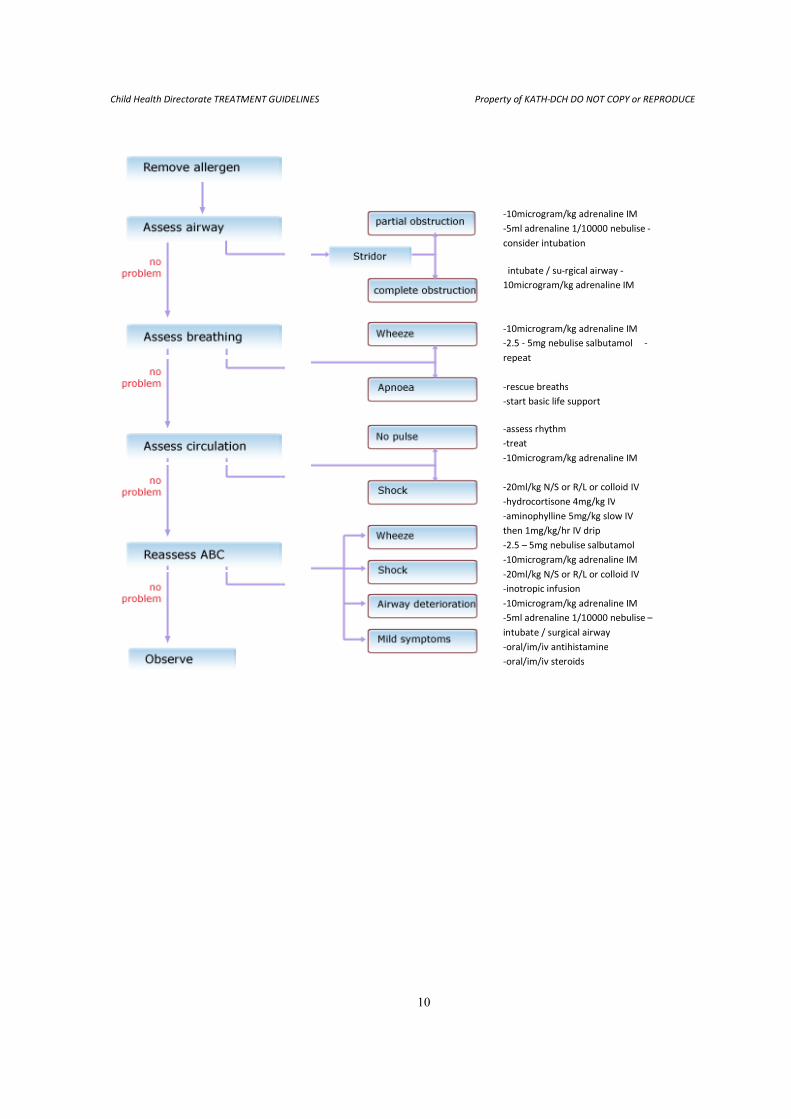
10
-10microgram/kg adrenaline IM
-5ml adrenaline 1/10000 nebulise
consider intubation
intubate / su
10microgram/kg adrenaline IM
-10microgram/kg adrenaline IM
-2.5 - 5mg nebulise
repeat
-rescue breaths
-start basic life support
-assess rhythm
-treat
-10microgram/kg adrenaline IM
-20ml/kg N/S or R/L or colloid IV
-hydrocortisone 4mg/kg IV
-aminophylline 5mg/kg slow IV
then 1mg/kg/hr IV drip
-2.5 – 5mg nebulise
-10microgram/kg adrenaline IM
-20ml/kg N/S or R/L or colloid IV
-inotropic infusion
-10microgram/kg adrenaline IM
-5ml adrenaline 1/10000 nebulise
intubate / surgical airway
-oral/im/iv antihistamine
-oral/im/iv steroids
DCH DO NOT COPY or REPRODUCE
10microgram/kg adrenaline IM
5ml adrenaline 1/10000 nebulise -
consider intubation
intubate / su-rgical airway -
10microgram/kg adrenaline IM
10microgram/kg adrenaline IM
5mg nebulise salbutamol -
rescue breaths
start basic life support
assess rhythm
10microgram/kg adrenaline IM
20ml/kg N/S or R/L or colloid IV
hydrocortisone 4mg/kg IV
aminophylline 5mg/kg slow IV
then 1mg/kg/hr IV drip
5mg nebulise salbutamol
10microgram/kg adrenaline IM
20ml/kg N/S or R/L or colloid IV
inotropic infusion
10microgram/kg adrenaline IM
5ml adrenaline 1/10000 nebulise –
intubate / surgical airway
oral/im/iv antihistamine
oral/im/iv steroids
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
11
2.0 NEUROLOGICAL DISORDERS 2.1.0 CONVULSIONS / SEIZURE DISORDERS
2.1.1 DEFINITIONS AND CLASSIFICATION 1. DEFINITIONS
Seizure – Sudden excessive discharge of neurons in parts of the brain manifested by involuntary motor,
sensory, autonomic or psychic phenomena, alone or in any combination often accompanied by alterations
or loss of consciousness.
Epilepsy – Spontaneous recurrent seizures, not related to fever or any acute cerebral insult.
Convulsion – Describes sudden and repeated abnormal movements and postures. It is the motor
manifestations of a seizure. It is usually but not always due to epilepsy.
Status Epilepticus – Prolonged or recurrent seizures lasting at least 30 minutes without the patient
regaining consciousness.
Epilepsy syndromes – Grouping of similar epileptic patients according to seizure type, EEG, age of onset,
familial episodes, prognosis, and other clinical signs.
2. INTERNATIONAL LEAGUE AGAINT EPILEPSY (ILAE) REVISED CLASSIFICATION OF SEIZURES
I. Partial seizures (seizures with focal onset)
A. Simple partial seizures (consciousness unimpaired)
1. with motor signs
2. with somatosensory or special sensory symptoms
3. with autonomic symptoms or signs
4. with psychic symptoms (higher cerebral functions)
B. Complex partial seizures (consciousness impaired)
1. starting as simple partial seizures
a. without automatism
b. with automatism
2. with impairement of consciousness at onset
a. without automatism
b. with automatism
C. Partial seizures evolving into secondarily generalized seizures
II. Generalized seizures
A. Absence seizures (brief lapse in awareness without postictal impairment)
• Typical absence • Atypical absence
B. Myoclonic seizures (brief repetitive symmetric muscle contractions)
C. Clonic seizures (rhythmic jerking; flexor spasm of extremities)
D. Tonic seizures (sustained muscle contraction)
E. Tonic-clonic seizures
F. Atonic seizures (abrupt loss of muscle tone)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
12
III. Unclassified Epileptic Seizures
These include all seizures that cannot be classified because of inadequate or incomplete data and
some that defy classification in hitherto described categories.
2.1.2 GENERAL AETIOLOGY OF CONVULSIVE DISORDERS 1. Congenital
• Idiopathic or genetic disorders (e.g. Juvenille Myoclonic Epilepsy)
• Neurocutanous disorders (Neurofibromatosis, Tuberous sclerosis)
• Metabolic disorders
• Congenital malformations of the CNS (e.g. vascular malformations)
2. Acquired
• Febrile convulsions
• Substance abuse/withdrawal (alcohol/drugs)
• Toxicity (drugs, poisons)
• Metabolic/electrolyte abnormalities (e.g., hypoglycemia, hypocalcemia)
• Perinatal brain injuries (birth asphyxias, intracranial hemorrhage)
• CNS infections (meningitis, encephalitis, cerebral malaria)
• Trauma (head injuries)
• Tumors
• Hypoxic/ ischemic stroke
• Systemic diseases (e.g. chronic renal failure, chronic liver disease, systemic hypertension,
etc.)
2.1.3 DIAGNOSIS The diagnoses is of epilepsy is a clinical one, based on history, physical and neurological examinations, and
supported where necessary by appropriate investigation such as electroencephalography, imaging studies
and special studies.
1. History
• Previous seizures
• Age of onset
• Frequency and duration of
• Description of ictal event
• Seizure type, e.g. Partial vs. Generalizad.
• Post-ictal phase
• Diurnal pattern
• Precipitating event e.g. fever, head injury, etc.
• Associated symptoms e.g. headache, incontinence, vomiting, etc.
• Any history of accidental drug/chemical ingestion
• Past history of birth/neonatal problems
• History of systemic illness e.g. SCD, DM, CRF, meningitis/encephalitis, neurocutaneous syndrome
etc.
• Developmental delay
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
13
• Family history
• Seizure diary
• Eye-witness account often reliable
2. Physical exam
• Rapid survey should include airway, breathing and circulation (ABC)
• If seizure is observed by examiner, details should be paid to seizure type, duration, associated signs
and symptoms etc
• Look for fever, signs of increased intracranial pressure (high BP, bradycardia, papilloedema)
• Look for any offending chemical agent and remove it
• Level of consciousness
• Detailed neurological examination
o dysmorphic features
o the stigmata of neurocutaneuous disorders (neurofibromatosis, Sturge-Weber)
o evidence of focal neurologic defect
o raised intracranial pressure
• Systemic physical exam should be tailored towards possible etiologic factors e.g. CRF,CNS infection,
HTN, Chronic Liver disease, trauma/head injury, genetic disorders, etc
3. Basic investigations
• Full blood count
• Random blood sugar (RBS)
• BUN, Creatinine, serum electrolytes (including Ca2+
, PO42+
, and Mg2+
)
• Liver function test
• Toxicology screen (if suspected from history/examination)
2.1.4 ACUTE MANAGEMENT OF SEIZURES / CONVULSIONS In practice any seizure lasting over 10 minutes should be treated as an EMERGENCY and the doctor
should not leave the patient until the seizures have been stopped.
1. AETIOLOGY:-
• Febrile convulsions
• Epilepsy (may be antiepileptic drug withdrawal)
• Acute encephalopathy (cerebral malaria, meningitis, hypertension)
• Cerebral ischaemia / trauma
• Metabolic (hypoglycaemia, uraemia, poisoning, hypo/hyper-natraeremia etc)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
14
2. INITIAL ASSESSMENT
History Examination/Investigation
Previous seizures Nature of convulsion: –
generalized or focal
Past medical history
birth/neonatal problems
meningitis/encephalitis Fever
neurological disorder
e.g. neurocutaneous syndrome
or neurodegenerative disorder
developmental delay
trauma Evidence of trauma
Recent head injury:
Accidental/Non-accidental Level of consciousness
-Ingestion of drugs Blood glucose ± electrolyte
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
15
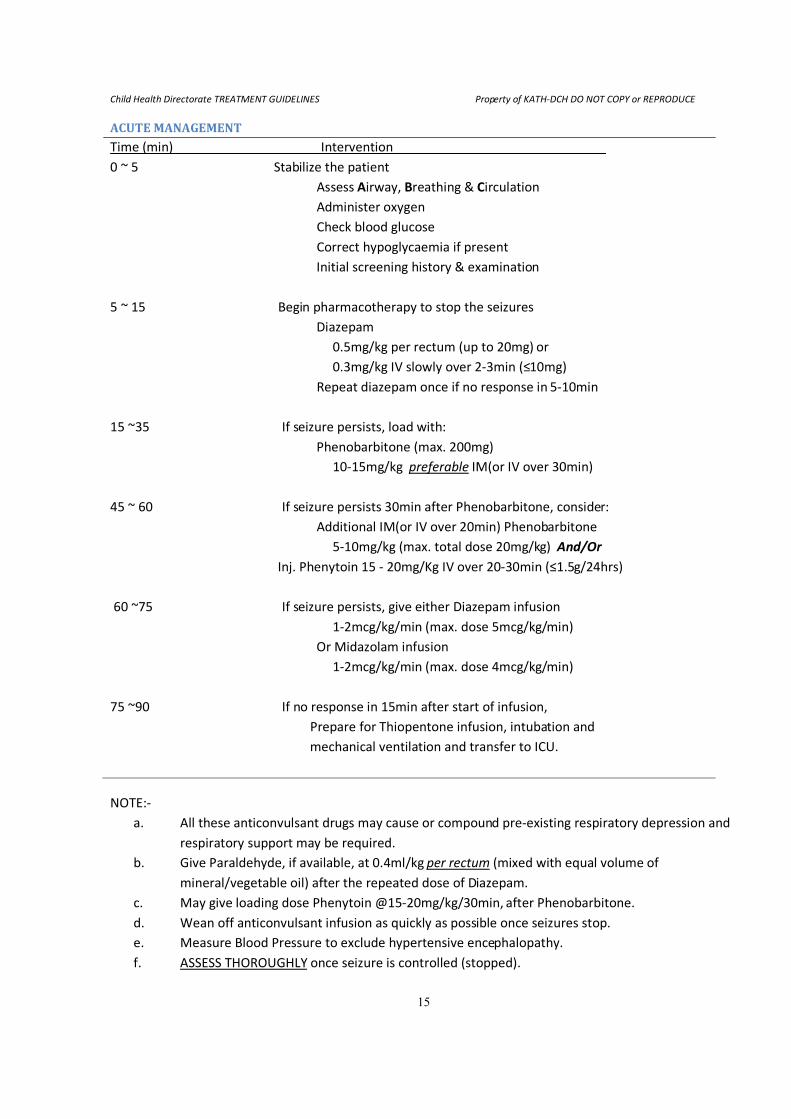
ACUTE MANAGEMENT
Time (min) Intervention______________________________
0 ~ 5 Stabilize the patient
Assess Airway, Breathing & Circulation
Administer oxygen
Check blood glucose
Correct hypoglycaemia if present
Initial screening history & examination
5 ~ 15 Begin pharmacotherapy to stop the seizures
Diazepam
0.5mg/kg per rectum (up to 20mg) or
0.3mg/kg IV slowly over 2-3min (≤10mg)
Repeat diazepam once if no response in 5-10min
15 ~35 If seizure persists, load with:
Phenobarbitone (max. 200mg)
10-15mg/kg preferable IM(or IV over 30min)
45 ~ 60 If seizure persists 30min after Phenobarbitone, consider:
Additional IM(or IV over 20min) Phenobarbitone
5-10mg/kg (max. total dose 20mg/kg) And/Or
Inj. Phenytoin 15 - 20mg/Kg IV over 20-30min (≤1.5g/24hrs)
60 ~75 If seizure persists, give either Diazepam infusion
1-2mcg/kg/min (max. dose 5mcg/kg/min)
Or Midazolam infusion
1-2mcg/kg/min (max. dose 4mcg/kg/min)
75 ~90 If no response in 15min after start of infusion,
Prepare for Thiopentone infusion, intubation and
mechanical ventilation and transfer to ICU.
NOTE:-
a. All these anticonvulsant drugs may cause or compound pre-existing respiratory depression and
respiratory support may be required.
b. Give Paraldehyde, if available, at 0.4ml/kg per rectum (mixed with equal volume of
mineral/vegetable oil) after the repeated dose of Diazepam.
c. May give loading dose Phenytoin @15-20mg/kg/30min, after Phenobarbitone.
d. Wean off anticonvulsant infusion as quickly as possible once seizures stop.
e. Measure Blood Pressure to exclude hypertensive encephalopathy.
f. ASSESS THOROUGHLY once seizure is controlled (stopped).
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
16
3. ONGOING MANAGEMENT:-
a. Monitor coma score, respiratory state, temperature, HR & BP(record in notes)
b. Control temperature with tepid sponge and regular antipyretics
c. Treat the underlying cause e.g. cerebral malaria, meningitis, encephalitis, electrolyte imbalance
etc.
d. Do not over hydrate.
e. If fits last >20min or recurrent, give maintenance long acting anticonvulsant e.g.
• Phenobarbitone 2.5mg/kg/dose Q12h.
• Phenytoin 5mg/kg/dose Q12h.
2.1.5 OTHER INVESTIGATIONS TO SUPPORT DIAGNOSIS OF EPILEPSY
a. Electroencephalography (EEG)
EEG, where available, is critical to the diagnosis of epilepsy. Methods of recording include:
• Routine
• Activated (Hyperventilation, Photic Stimulation)
• Sleep deprived
• 24-hr ambulatory
• Medication discontinued
• Placebo induction
• EEG video monitoring
• Electrode depth/type
Typical EEG findings in some epileptic syndromes are
• Simple partial seizures – focal sharp or slow waves (interictal), rhythmic discharge or often
normal (ictal)
• Complex partial seizures – sharp waves or spikes (interictal), focal or bilateral rhythmic
sharp waves (interictal)
• Tonic seizures – Flattening/high frequency discharge
• Atonic seizures – Slow spike-wave/flattening
• Tonic-clonic seizures – Variable, often obscured
• Absence Seizure – 3 Hz/sec spike waves (hyperventilation sensitive)
• Rolandic Seizure – Spikes in the Rolandic area ( centrotemporal region)
• Infantile spasms (West Syndrome) – Hypsarrhythmias (interictal)
• Juvenile myoclonic epilepsy – generalized polyspike-wave discharges
b. Neuroimaging (structural/anatomic) studies
• Computed tomography (CT) scan
• Magnetic Resonance Imaging (MRI)
Indication for imaging in children with epilepsy include
1. Seizures commencing first year of life
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
17
2. History or physical exam suggests an abnormality of CNS e.g. neurocutaneous
syndrome.
3. Developmental delay or regression
4. Persistent or localized slow-wave changes or spike wave foci suggesting a focal
lesion
5. Changes in seizure pattern
6. Refractory seizures may detect glioma
7. Child with previous normal scan but remains poorly controlled (no later than 12 –
18 months)
MRI in comparison to CT is a superior diagnostic tool in epilepsy. Better image resolution and
lack of “beam hardening artifacts” from surrounding bone, especially for structures in the
middle fossa (temporal lobes) make MRI a superior structural imaging modality for patients
with partial seizures. Specialized MRI sequences enable detection of small structural lesions in
patients with epilepsy
c. Special investigations (where available) include
• Positron emission tomography (PET)
• Single photon emission controlled tomography (SPECT)
• Magnetoencephalography (MEG)
• Intensive CCTV – EEG telemetry monitoring
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
18
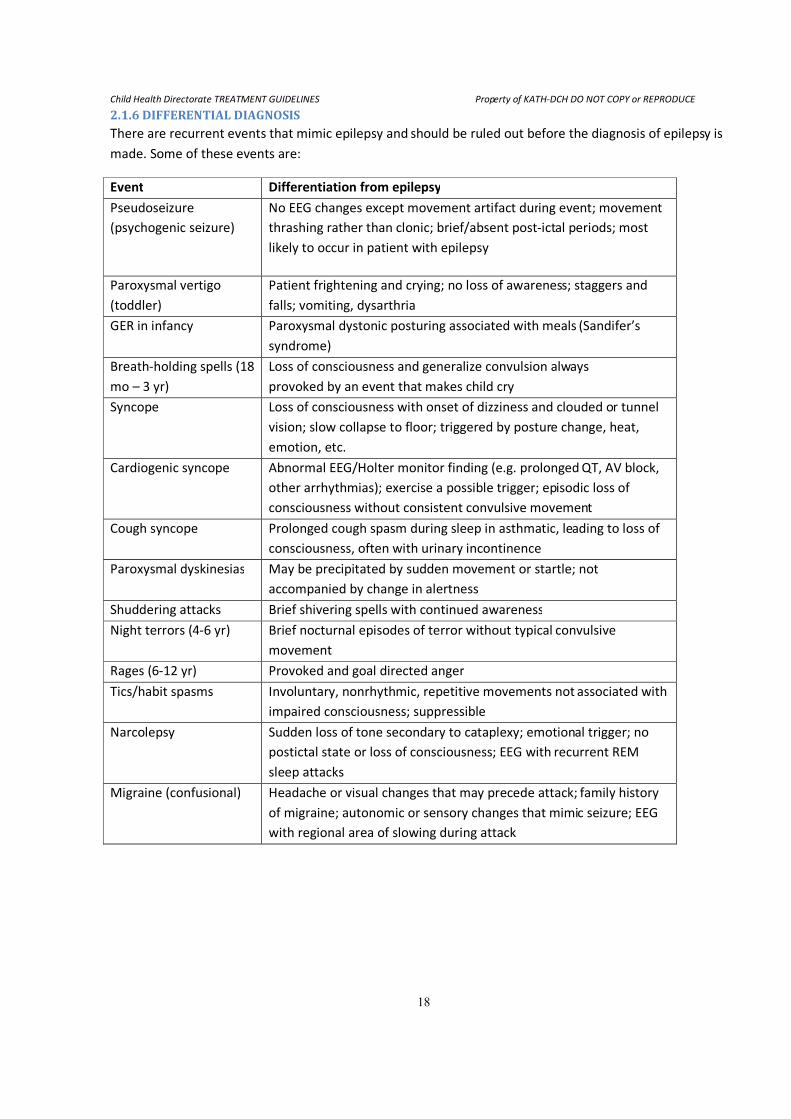
2.1.6 DIFFERENTIAL DIAGNOSIS There are recurrent events that mimic epilepsy and should be ruled out before the diagnosis of epilepsy is
made. Some of these events are:
Event Differentiation from epilepsy
Pseudoseizure
(psychogenic seizure)
No EEG changes except movement artifact during event; movement
thrashing rather than clonic; brief/absent post-ictal periods; most
likely to occur in patient with epilepsy
Paroxysmal vertigo
(toddler)
Patient frightening and crying; no loss of awareness; staggers and
falls; vomiting, dysarthria
GER in infancy Paroxysmal dystonic posturing associated with meals (Sandifer’s
syndrome)
Breath-holding spells (18
mo – 3 yr)
Loss of consciousness and generalize convulsion always
provoked by an event that makes child cry
Syncope Loss of consciousness with onset of dizziness and clouded or tunnel
vision; slow collapse to floor; triggered by posture change, heat,
emotion, etc.
Cardiogenic syncope Abnormal EEG/Holter monitor finding (e.g. prolonged QT, AV block,
other arrhythmias); exercise a possible trigger; episodic loss of
consciousness without consistent convulsive movement
Cough syncope Prolonged cough spasm during sleep in asthmatic, leading to loss of
consciousness, often with urinary incontinence
Paroxysmal dyskinesias May be precipitated by sudden movement or startle; not
accompanied by change in alertness
Shuddering attacks Brief shivering spells with continued awareness
Night terrors (4-6 yr) Brief nocturnal episodes of terror without typical convulsive
movement
Rages (6-12 yr) Provoked and goal directed anger
Tics/habit spasms Involuntary, nonrhythmic, repetitive movements not associated with
impaired consciousness; suppressible
Narcolepsy Sudden loss of tone secondary to cataplexy; emotional trigger; no
postictal state or loss of consciousness; EEG with recurrent REM
sleep attacks
Migraine (confusional) Headache or visual changes that may precede attack; family history
of migraine; autonomic or sensory changes that mimic seizure; EEG
with regional area of slowing during attack
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
19
2.1.7 ANTIEPILEPTIC DRUG (AED) THERAPY Principles of therapeutics
1. Be certain of the diagnosis
2. Decide whether to treat or not to treat
3. Select the best drug appropriate to both the seizure type and the patient
4. The main goal of treatment should be to achieve seizure control with least side effects
5. Start with low doses and gradually push the dose to clinical toxicity or seizure control
6. Use the least expensive AED (all things being equal, like efficacy)
7. Withdraw AEDs that are not effective
8. Prefer AEDs which can be taken od over bid, tid or qid dosing
9. Monotherapy is always preferred (never have a patient on more than 3 AEDs). Polypharmacy is
expensive, increases side effects and increases the complexity of adjusting AEDs in the refractory
patient.
10. Decide when to stop treatment
How to Start a New Drug
• Give clear instructions, preferable written
• Warn about side effects
• Often start bid dosing with night time dose
• Increase dose every 2 weeks
• Aim for about 2/3 of ‘max.’ target dose or lowest effective dose
• If possible continue max. dose for weeks before abandoning
• Avoid chopping and changing
• Beware of interactions
• Titrate dose over weeks
• Warn about problems during change over
• Push drug dose if necessary to:
• Effective dose
• Limits of tolerance
Traditional AEDs
• Carbamazepine • Sodium valproate • Phenytoin
• Phenobarbitone • Ethosuximide
Newer AEDs
• igabatrin • Felbamate • Levetiracetam
• Lamotrigine • Topiramate • Gabapetin
• Oxcarbazepine • Tiagabine • Zonisamide
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
20
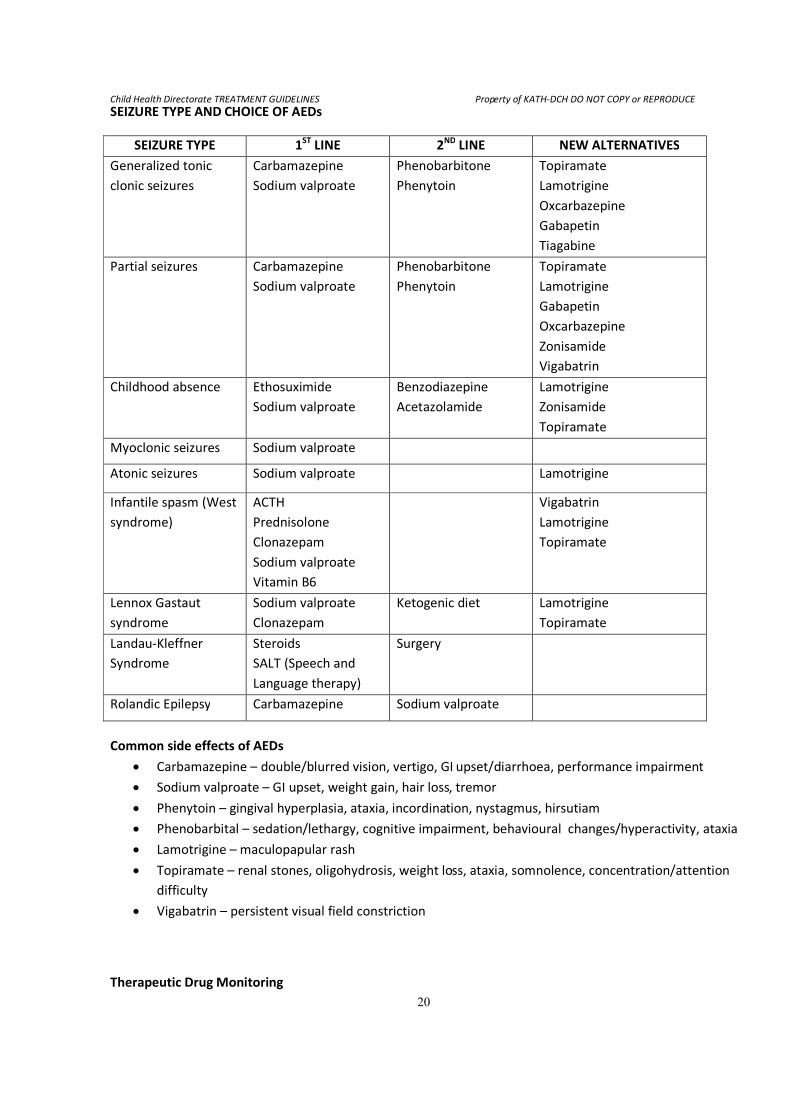
Common side effects of AEDs
• Carbamazepine – double/blurred vision, vertigo, GI upset/diarrhoea, performance impairment
• Sodium valproate – GI upset, weight gain, hair loss, tremor
• Phenytoin – gingival hyperplasia, ataxia, incordination, nystagmus, hirsutiam
• Phenobarbital – sedation/lethargy, cognitive impairment, behavioural changes/hyperactivity, ataxia
• Lamotrigine – maculopapular rash
• Topiramate – renal stones, oligohydrosis, weight loss, ataxia, somnolence, concentration/attention
difficulty
• Vigabatrin – persistent visual field constriction
Therapeutic Drug Monitoring
SEIZURE TYPE AND CHOICE OF AEDs
SEIZURE TYPE 1ST LINE 2ND LINE NEW ALTERNATIVES
Generalized tonic
clonic seizures
Carbamazepine
Sodium valproate
Phenobarbitone
Phenytoin
Topiramate
Lamotrigine
Oxcarbazepine
Gabapetin
Tiagabine
Partial seizures Carbamazepine
Sodium valproate
Phenobarbitone
Phenytoin
Topiramate
Lamotrigine
Gabapetin
Oxcarbazepine
Zonisamide
Vigabatrin
Childhood absence Ethosuximide
Sodium valproate
Benzodiazepine
Acetazolamide
Lamotrigine
Zonisamide
Topiramate
Myoclonic seizures Sodium valproate
Atonic seizures Sodium valproate Lamotrigine
Infantile spasm (West
syndrome)
ACTH
Prednisolone
Clonazepam
Sodium valproate
Vitamin B6
Vigabatrin
Lamotrigine
Topiramate
Lennox Gastaut
syndrome
Sodium valproate
Clonazepam
Ketogenic diet Lamotrigine
Topiramate
Landau-Kleffner
Syndrome
Steroids
SALT (Speech and
Language therapy)
Surgery
Rolandic Epilepsy Carbamazepine Sodium valproate
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
21
NB. "Routine" levels on controlled, nontoxic patients are not indicated
Check serum levels of AEDs only when necessary to assess:
1. Poor clinical control (compliance, metabolism)
2. Dose-related side effect
3. Drug or disease interaction
AED Idiosyncratic Reactions
• Rare
• Dose independent
• Unpredictable
• Usually appear in first 3-6 mo
• May recur
• Possibly life threatening, include the following:
o Stevens-Johnson
o Aplastic anaemia
o Hepatic failure
o Dermatitis/rash
o Pancreatitis
o Agranulocytosis
o Serum sickness
In the event of treatment failure, the following should be considered
1. Is the diagnosis of epilepsy certain?
2. Is the diagnosis of the type of epilepsy a correct one?
3. Are all episodes which are being recorded as seizures truly such?
4. Is compliance with treatment adequate?
5. Have appropriate drugs each been used in maximal doses?
6. Have appropriate combinations of drugs been tried?
7. Could the patient’s condition improve by having the number of drugs decreased or stopped?
8. Treatments other than anti- epileptic drugs
STOPPING ANTICONVULSANT THERAPY
• Withdraw gradually after a 2 year period of no seizures, preferably over a period of 4-6 months.
• Risk of relapse is 20% in children
KETOGENIC DIET
• High fat diet designed to mimic the metabolic effects of starvation
• Mechanism of seizure control is unknown
• Protein and Carbohydrate is restricted
• 80% of calorie supplied by fat
• Most effective in children aged between 2 – 5yrs
• Effective in refractory epilepsy
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
22
Side Effects:
o vomiting o acidosis o renal stones
o constipation o high serum cholesterol o growth restriction
2.1.8 SURGERY FOR EPILEPSY
• Temporal lobectomy • Hemispherectomy • Corpus Callostomy
2.1.9 PSYCHOLOGICAL MANAGEMENT
1. Prevent or reduce emotional stress
2. Counsel directly children over 8years
3. Orientate parents and family
4. Encourage normal mental and physical activities
5. Safety restrictions must be individualized
6. Contact sports (football, karate)must be avoided
7. Encourage supervised sports (basketball, swimming)
8. Most patients can drive a car at a legal age
9. Reduce constipation with high fibre diet
10. Should have a regular life style with drugs, food, rest, sleep
11. Children with refractory myoclonic and absences may be placed on modified high fat diet
12. Seizures appear to be associated with excessive ingestion of food or fluids
13. Recognition and management of associated learning, language, behavioral, neuromotor
disorders are important aspects of the comprehensive management of the patient with
epilepsy
2.1.10 OTHER PROBLEMS ASSOCIATED WITH EPILEPSY THAT NEED THE PHYSICIANS ATTENTION 1. Epilepsy and learning
• Children with uncomplicated epilepsy lag one year behind their peers (Yule 1980).
• They also have deficits of reading (severe in 20%), spelling and maths (Seidenberg et al 1986)
2. Epilepsy and psychosocial factors
• Stigmatization
• Parental anxiety
• Social isolation
3. Epilepsy and behaviour
• Behaviour problems in 50% attending neuroclinic
• Hyperactive, self injurious, mixed conduct/emotional disorder
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
23
2.1.11 INTEGRATED EPILEPSY SERVICE (MULTI-DISCIPLINARY)
• Paediatric neurologist • Support worker • Special needs teacher
• Nurse specialist • Psychologists • Neurosurgeon
• Neuro-psychiatrist
It is essential to adopt a multidisciplinary approach in the management of the child with epilepsy, while the
child remains under the care of a Paediatric Neurologist.
2.1.12 OUTCOME OF TREATMENT
• 2/3 of children with epilepsy will have seizures controlled with a single antiepileptic drug
• 2/3 of children with epilepsy are able to attend normal schools
• 10 years after diagnosis, 30% of patients with epilepsy will be without seizures and on no medication
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
24
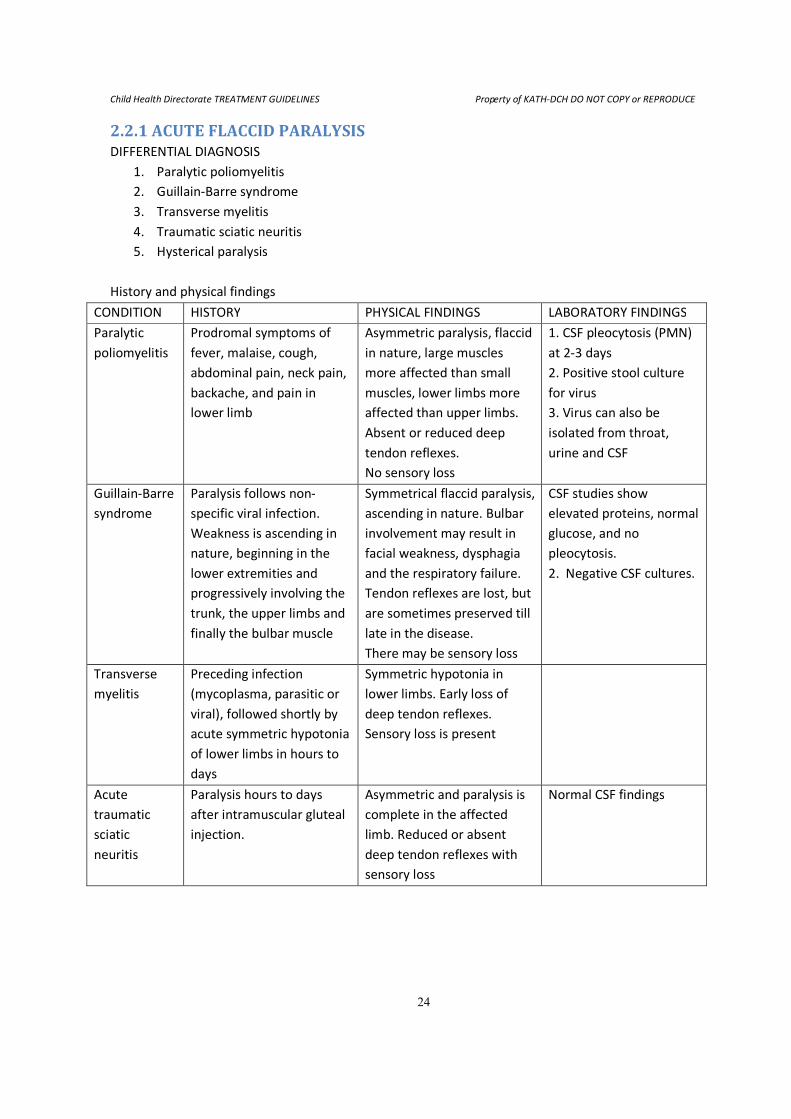
2.2.1 ACUTE FLACCID PARALYSIS DIFFERENTIAL DIAGNOSIS
1. Paralytic poliomyelitis
2. Guillain-Barre syndrome
3. Transverse myelitis
4. Traumatic sciatic neuritis
5. Hysterical paralysis
History and physical findings
CONDITION HISTORY PHYSICAL FINDINGS LABORATORY FINDINGS
Paralytic
poliomyelitis
Prodromal symptoms of
fever, malaise, cough,
abdominal pain, neck pain,
backache, and pain in
lower limb
Asymmetric paralysis, flaccid
in nature, large muscles
more affected than small
muscles, lower limbs more
affected than upper limbs.
Absent or reduced deep
tendon reflexes.
No sensory loss
1. CSF pleocytosis (PMN)
at 2-3 days
2. Positive stool culture
for virus
3. Virus can also be
isolated from throat,
urine and CSF
Guillain-Barre
syndrome
Paralysis follows non-
specific viral infection.
Weakness is ascending in
nature, beginning in the
lower extremities and
progressively involving the
trunk, the upper limbs and
finally the bulbar muscle
Symmetrical flaccid paralysis,
ascending in nature. Bulbar
involvement may result in
facial weakness, dysphagia
and the respiratory failure.
Tendon reflexes are lost, but
are sometimes preserved till
late in the disease.
There may be sensory loss
CSF studies show
elevated proteins, normal
glucose, and no
pleocytosis.
2. Negative CSF cultures.
Transverse
myelitis
Preceding infection
(mycoplasma, parasitic or
viral), followed shortly by
acute symmetric hypotonia
of lower limbs in hours to
days
Symmetric hypotonia in
lower limbs. Early loss of
deep tendon reflexes.
Sensory loss is present
Acute
traumatic
sciatic
neuritis
Paralysis hours to days
after intramuscular gluteal
injection.
Asymmetric and paralysis is
complete in the affected
limb. Reduced or absent
deep tendon reflexes with
sensory loss
Normal CSF findings
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
25
2.2.2 MANAGEMENT OF POLIOMYELITIS Acute Phase Management
1. Bed Rest – during the first week of admission or until fever resolves. Exercises would worsen
the extent & severity of paralysis. No invasive investigations at this time.
2. Analgesics & hot packs to relieve pain.
3. Keep the limbs in a neutral position & support with sand bags
4. Monitor closely for signs of worsening paralysis and bulbar involvement
5. I.C.U care and mechanical ventilation in cases of bulbar polio
Long Term Management
1. Physiotherapy
2. Use of special ambulatory devices
3. Surgery to correct deformities
2.2.3 MANAGEMENT OF GUILLAIN-BARRE SYNDROME 1. Admit
2. If ascending paralysis is slow in progression, simply observe patient for stabilization and
spontaneous remission without treatment
3. Treat rapidly progressive ascending paralysis with intravenous immunoglobulin.
Plasmapheresis, steroids and immunosuppressive drugs are alternatives.
4. Supportive care such as prevention of decubitus ulcers and treatment of secondary bacterial
infections are important.
5. Observe patient closely for respiratory muscle involvement
6. I.C.U care and mechanical ventilation in cases of bulbar involvement.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
26
2.3.0 ACUTE ENCEPHALOPATHY / NON TRAUMATIC COMA 1. COMMON CAUSES:-
Infection - malaria, meningitis, encephalitis etc
Epilepsy - convulsive or non convulsive
Vascular -hypertensive encephalopathy, intracranial haemorrhage etc
Toxic -drugs, poisons etc
Tumor -benign or malignancy
Metabolic -hypoglycaemia, hyperglycaemia, hepatic failure etc
Temperature regulation -hyperthermia, hypothermia
2. RAPID ASSESSMENT & STABILISATION ( NEUROLOGICAL ABC) :-
A -Airway Ensure there is an adequate airway, best protected by putting the
patient in the recovery position.
B -Breathing Ensure the patient is breathing sufficiently to provide adequate
Oxygenation (SaO2). Give oxygen, artificial respiration if needed.
C -Circulation Check for adequate circulation, with pulse, BP & cap. refill time.
D -Diabetes Check blood sugar - Dextrostix, BM sticks(true blood glucose if
possible) – if not available give 4-5ml/kg of 10% dextrose if the
altered consciousness could be due to hypoglycaemia.
-Drugs Consider overdose or poison.
E -Epilepsy Observe for seizures (lift the eye lids and look for tonic deviation
of the eyes or nystagmus) or stigmata, bitten tongue: stop/control
seizures.
F -Fever Check for fever, stiff neck, purpuric rash of meningococcal
meningitis, blood film malaria parasite for cerebral malaria.
G -Glasgow Assess coma score. Record sub scores (eyes/verbal/motor) as well
coma scale as total.
H -Herniation Is there evidence of conning or raised intracranial pressure?
LOOK for Evidence of Herniation
• Respiratory rate & pattern (e.g. Cheyne-Stokes, erratic respiration).
• Posture / Tone / Reflexes (include oculocephalic reflex & plantars).
• Motor response to pain, decorticate or decerebrate posturing.
• Cushing’s phenomenon (↑BP, ↓HR and slow irregular breathing).
• Papilloedema / Retinal haemorrhage / Cranial nerve palsies.
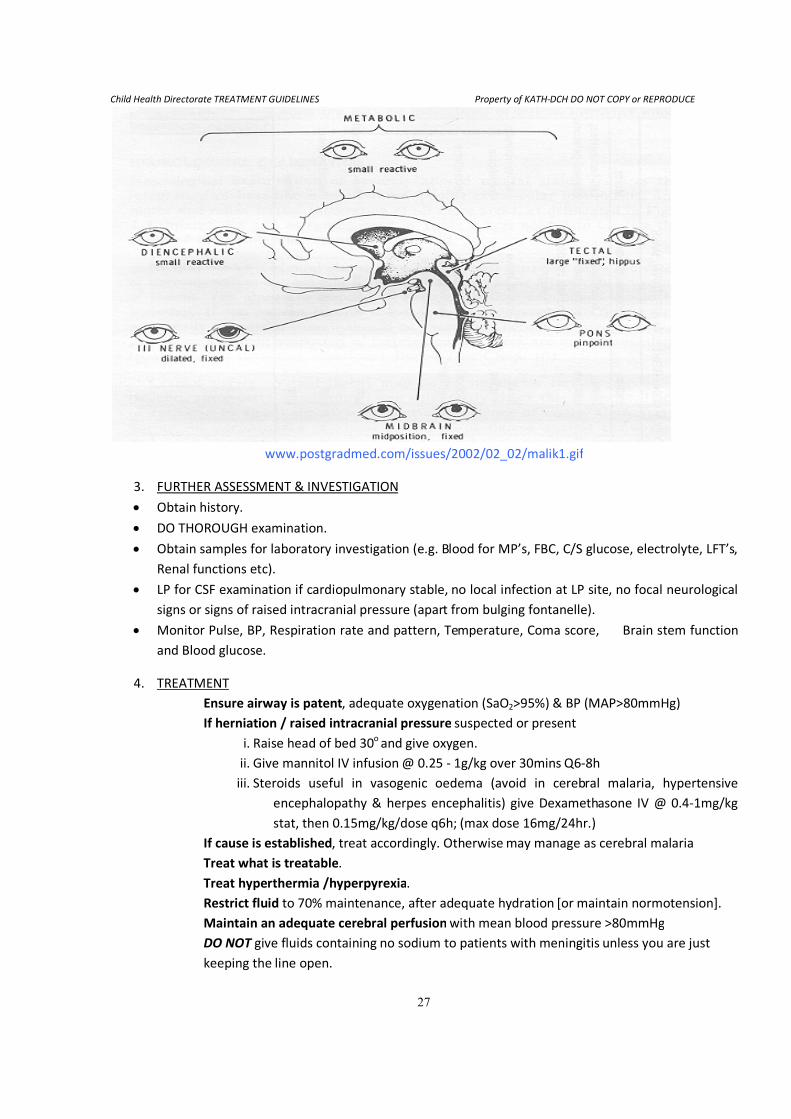
• Pupils size & response to light (including asymmetry)see below.
Child Health Directorate TREATMENT GUIDELINES
www.postgradmed.com/issues/2002/02_02/malik1.gif
3. FURTHER ASSESSMENT & INVESTIGATION
• Obtain history.
• DO THOROUGH examination.
• Obtain samples for laboratory investigation (e.g. Blood for MP’s, FBC, C/S glucose, electrolyte, LFT’s,
Renal functions etc).
• LP for CSF examination if cardiopulmonary stable,
signs or signs of raised intracranial pressure (apart from bulging fontanelle).
• Monitor Pulse, BP, Respiration rate and pattern, Temperature, Coma score, Brain stem function
and Blood glucose.
4. TREATMENT
Ensure airway is patent
If herniation / raised intracranial pressure
i. Raise head of bed 30
ii. Give mannitol IV infusion
iii. Steroids useful in vasogenic oedema (avoid in cerebral malaria, hypertensive
encephalopathy & herpes encephalitis) give Dexamethasone IV @
stat, then 0.15mg/kg/dose q6h;
If cause is established
Treat what is treatable
Treat hyperthermia /hyperpyrexia
Restrict fluid
Maintain an adequate cerebral perfusion
DO NOT give fluids containing
keeping the line open.
TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
27
www.postgradmed.com/issues/2002/02_02/malik1.gif
FURTHER ASSESSMENT & INVESTIGATION
DO THOROUGH examination.
Obtain samples for laboratory investigation (e.g. Blood for MP’s, FBC, C/S glucose, electrolyte, LFT’s,
LP for CSF examination if cardiopulmonary stable, no local infection at LP site
igns or signs of raised intracranial pressure (apart from bulging fontanelle).
Monitor Pulse, BP, Respiration rate and pattern, Temperature, Coma score, Brain stem function
Ensure airway is patent, adequate oxygenation (SaO2>95%) & BP (MAP>80mmHg)
If herniation / raised intracranial pressure suspected or present
Raise head of bed 30o
and give oxygen.
Give mannitol IV infusion @ 0.25 - 1g/kg over 30mins
Steroids useful in vasogenic oedema (avoid in cerebral malaria, hypertensive
encephalopathy & herpes encephalitis) give Dexamethasone IV @
stat, then 0.15mg/kg/dose q6h; (max dose 16mg/24hr.)
If cause is established, treat accordingly. Otherwise may manage as cerebral malaria
Treat what is treatable.
Treat hyperthermia /hyperpyrexia.
to 70% maintenance, after adequate hydration [
Maintain an adequate cerebral perfusion with mean blood pressure >80mmHg
give fluids containing no sodium to patients with meningitis
line open.
DCH DO NOT COPY or REPRODUCE
www.postgradmed.com/issues/2002/02_02/malik1.gif
Obtain samples for laboratory investigation (e.g. Blood for MP’s, FBC, C/S glucose, electrolyte, LFT’s,
no local infection at LP site, no focal neurological
igns or signs of raised intracranial pressure (apart from bulging fontanelle).
Monitor Pulse, BP, Respiration rate and pattern, Temperature, Coma score, Brain stem function
>95%) & BP (MAP>80mmHg)
present
1g/kg over 30mins Q6-8h
Steroids useful in vasogenic oedema (avoid in cerebral malaria, hypertensive
encephalopathy & herpes encephalitis) give Dexamethasone IV @ 0.4-1mg/kg
(max dose 16mg/24hr.)
may manage as cerebral malaria
[or maintain normotension].
with mean blood pressure >80mmHg
no sodium to patients with meningitis unless you are just
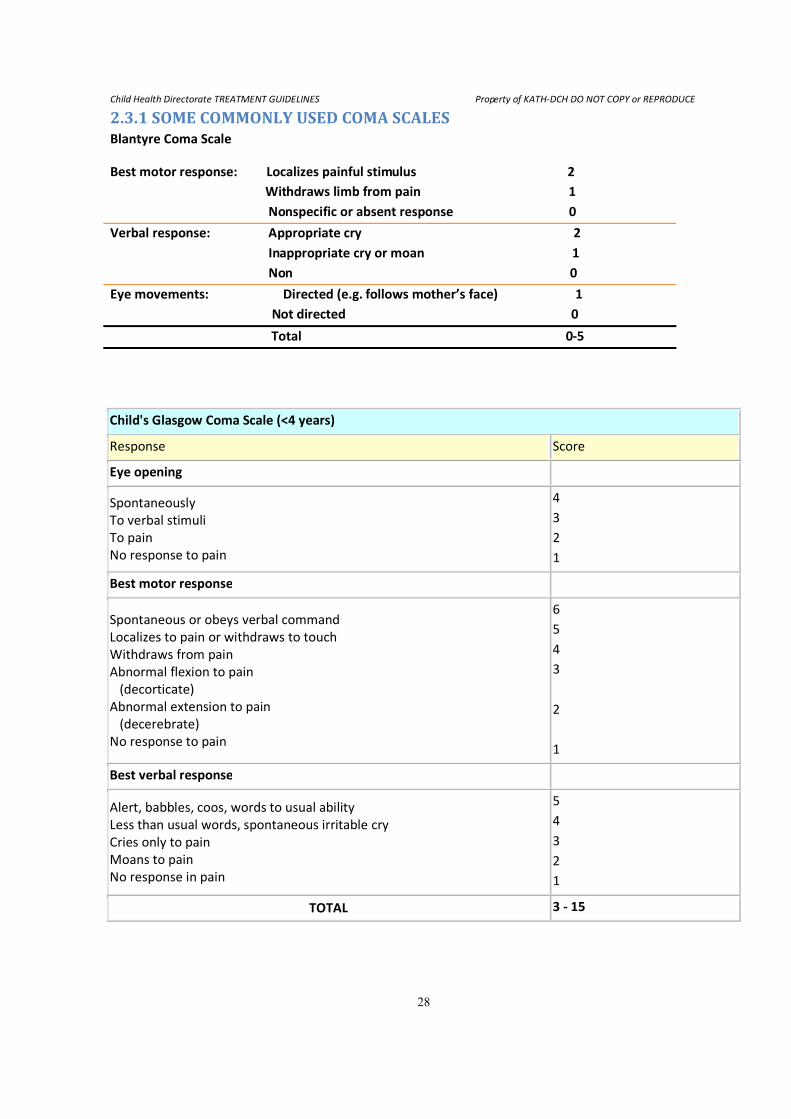
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
28
2.3.1 SOME COMMONLY USED COMA SCALES Blantyre Coma Scale
Best motor response: Localizes painful stimulus 2
Withdraws limb from pain 1
Nonspecific or absent response 0
Verbal response: Appropriate cry 2
Inappropriate cry or moan 1
Non 0
Eye movements: Directed (e.g. follows mother’s face) 1
Not directed 0
Total 0-5
Child's Glasgow Coma Scale (<4 years)
Response Score
Eye opening
Spontaneously
To verbal stimuli
To pain
No response to pain
4
3
2
1
Best motor response
Spontaneous or obeys verbal command
Localizes to pain or withdraws to touch
Withdraws from pain
Abnormal flexion to pain
(decorticate)
Abnormal extension to pain
(decerebrate)
No response to pain
6
5
4
3
2
1
Best verbal response
Alert, babbles, coos, words to usual ability
Less than usual words, spontaneous irritable cry
Cries only to pain
Moans to pain
No response in pain
5
4
3
2
1
TOTAL 3 - 15
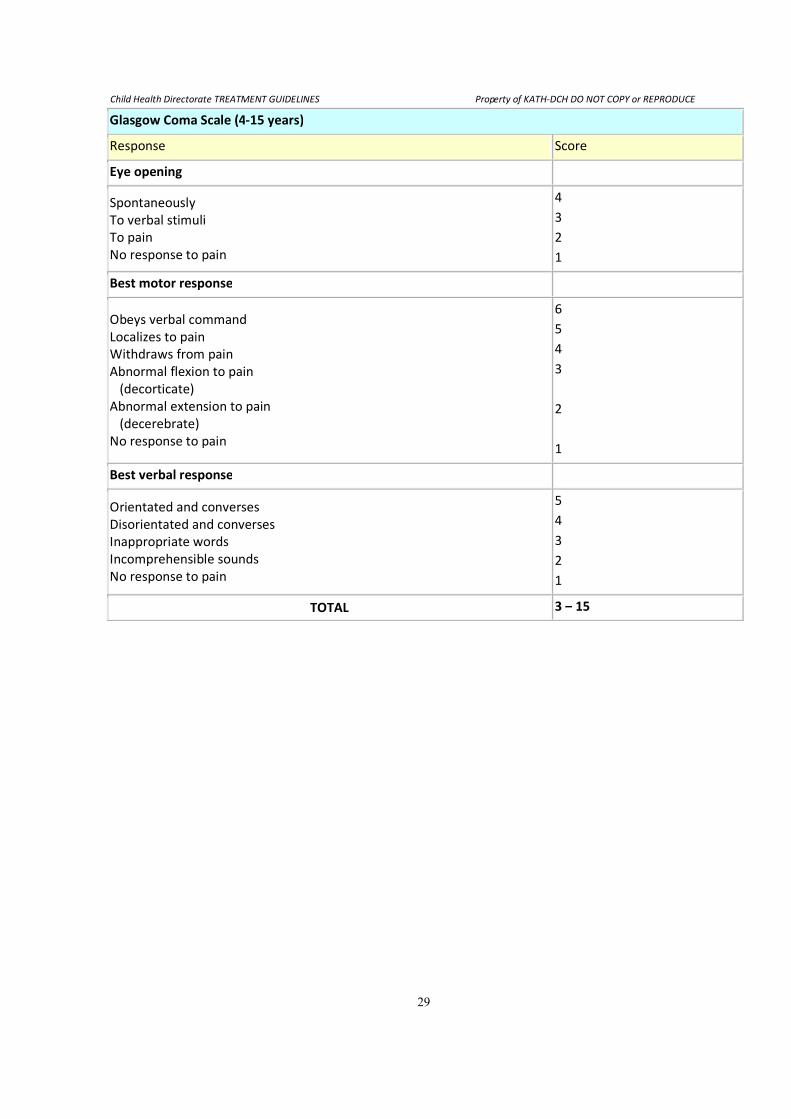
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
29
Glasgow Coma Scale (4-15 years)
Response Score
Eye opening
Spontaneously
To verbal stimuli
To pain
No response to pain
4
3
2
1
Best motor response
Obeys verbal command
Localizes to pain
Withdraws from pain
Abnormal flexion to pain
(decorticate)
Abnormal extension to pain
(decerebrate)
No response to pain
6
5
4
3
2
1
Best verbal response
Orientated and converses
Disorientated and converses
Inappropriate words
Incomprehensible sounds
No response to pain
5
4
3
2
1
TOTAL 3 – 15
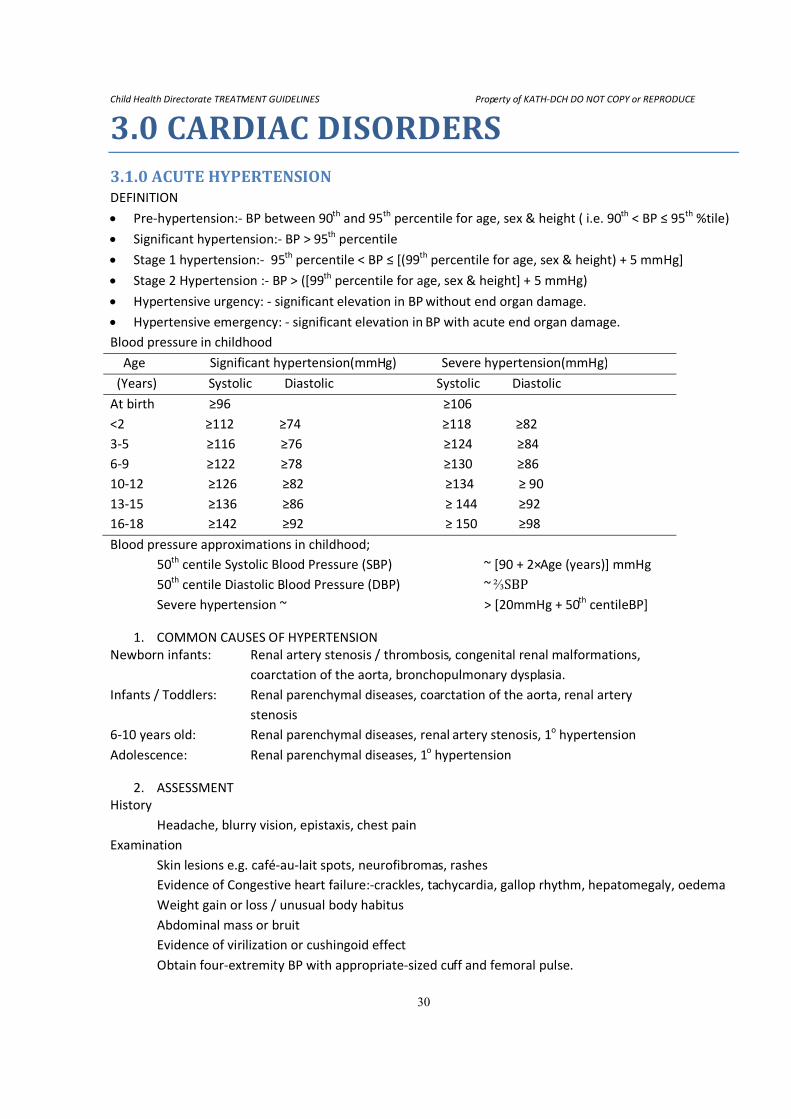
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
30
3.0 CARDIAC DISORDERS 3.1.0 ACUTE HYPERTENSION DEFINITION
• Pre-hypertension:- BP between 90th
and 95th
percentile for age, sex & height ( i.e. 90th
< BP ≤ 95th
%tile)
• Significant hypertension:- BP > 95th
percentile
• Stage 1 hypertension:- 95th
percentile < BP ≤ [(99th
percentile for age, sex & height) + 5 mmHg]
• Stage 2 Hypertension :- BP > ([99th
percentile for age, sex & height] + 5 mmHg)
• Hypertensive urgency: - significant elevation in BP without end organ damage.
• Hypertensive emergency: - significant elevation in BP with acute end organ damage.
Blood pressure in childhood
Age Significant hypertension(mmHg) Severe hypertension(mmHg)
(Years) Systolic Diastolic Systolic Diastolic
At birth ≥96 ≥106
<2 ≥112 ≥74 ≥118 ≥82
3-5 ≥116 ≥76 ≥124 ≥84
6-9 ≥122 ≥78 ≥130 ≥86
10-12 ≥126 ≥82 ≥134 ≥ 90
13-15 ≥136 ≥86 ≥ 144 ≥92
16-18 ≥142 ≥92 ≥ 150 ≥98
Blood pressure approximations in childhood;
50th centile Systolic Blood Pressure (SBP) ~ [90 + 2×Age (years)] mmHg
50th
centile Diastolic Blood Pressure (DBP) ~ ⅔SBP
Severe hypertension ~ > [20mmHg + 50th
centileBP]
1. COMMON CAUSES OF HYPERTENSION
Newborn infants: Renal artery stenosis / thrombosis, congenital renal malformations,
coarctation of the aorta, bronchopulmonary dysplasia.
Infants / Toddlers: Renal parenchymal diseases, coarctation of the aorta, renal artery
stenosis
6-10 years old: Renal parenchymal diseases, renal artery stenosis, 1o hypertension
Adolescence: Renal parenchymal diseases, 1o hypertension
2. ASSESSMENT
History
Headache, blurry vision, epistaxis, chest pain
Examination
Skin lesions e.g. café-au-lait spots, neurofibromas, rashes
Evidence of Congestive heart failure:-crackles, tachycardia, gallop rhythm, hepatomegaly, oedema
Weight gain or loss / unusual body habitus
Abdominal mass or bruit
Evidence of virilization or cushingoid effect
Obtain four-extremity BP with appropriate-sized cuff and femoral pulse.
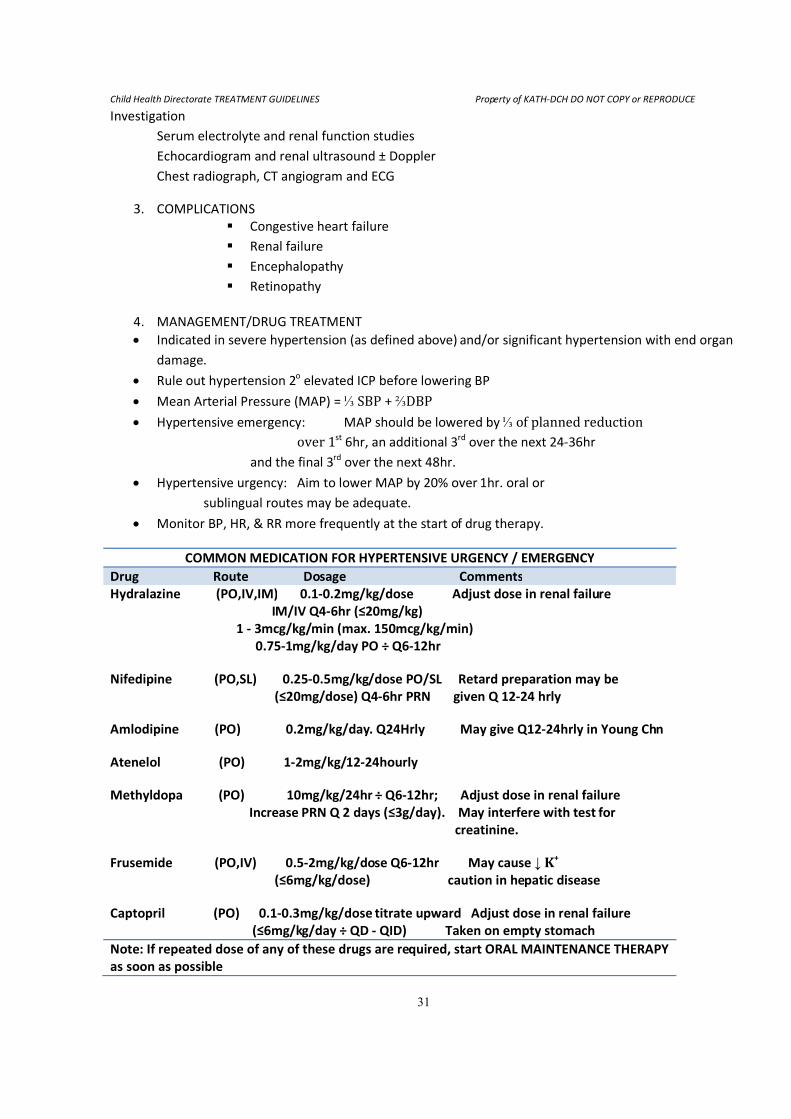
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
31
Investigation
Serum electrolyte and renal function studies
Echocardiogram and renal ultrasound ± Doppler
Chest radiograph, CT angiogram and ECG
3. COMPLICATIONS
� Congestive heart failure
� Renal failure
� Encephalopathy
� Retinopathy
4. MANAGEMENT/DRUG TREATMENT
• Indicated in severe hypertension (as defined above) and/or significant hypertension with end organ
damage.
• Rule out hypertension 2o elevated ICP before lowering BP
• Mean Arterial Pressure (MAP) = ⅓ SBP + ⅔DBP
• Hypertensive emergency: MAP should be lowered by ⅓ of planned reduction
over 1st 6hr, an additional 3rd over the next 24-36hr
and the final 3rd
over the next 48hr.
• Hypertensive urgency: Aim to lower MAP by 20% over 1hr. oral or
sublingual routes may be adequate.
• Monitor BP, HR, & RR more frequently at the start of drug therapy.
COMMON MEDICATION FOR HYPERTENSIVE URGENCY / EMERGENCY
Drug Route Dosage Comments
Hydralazine (PO,IV,IM) 0.1-0.2mg/kg/dose Adjust dose in renal failure
IM/IV Q4-6hr (≤20mg/kg)
1 - 3mcg/kg/min (max. 150mcg/kg/min)
0.75-1mg/kg/day PO ÷ Q6-12hr
Nifedipine (PO,SL) 0.25-0.5mg/kg/dose PO/SL Retard preparation may be
(≤20mg/dose) Q4-6hr PRN given Q 12-24 hrly
Amlodipine (PO) 0.2mg/kg/day. Q24Hrly May give Q12-24hrly in Young Chn
Atenelol (PO) 1-2mg/kg/12-24hourly
Methyldopa (PO) 10mg/kg/24hr ÷ Q6-12hr; Adjust dose in renal failure
Increase PRN Q 2 days (≤3g/day). May interfere with test for
creatinine.
Frusemide (PO,IV) 0.5-2mg/kg/dose Q6-12hr May cause ↓ K+
(≤6mg/kg/dose) caution in hepatic disease
Captopril (PO) 0.1-0.3mg/kg/dose titrate upward Adjust dose in renal failure
(≤6mg/kg/day ÷ QD - QID) Taken on empty stomach
Note: If repeated dose of any of these drugs are required, start ORAL MAINTENANCE THERAPY
as soon as possible
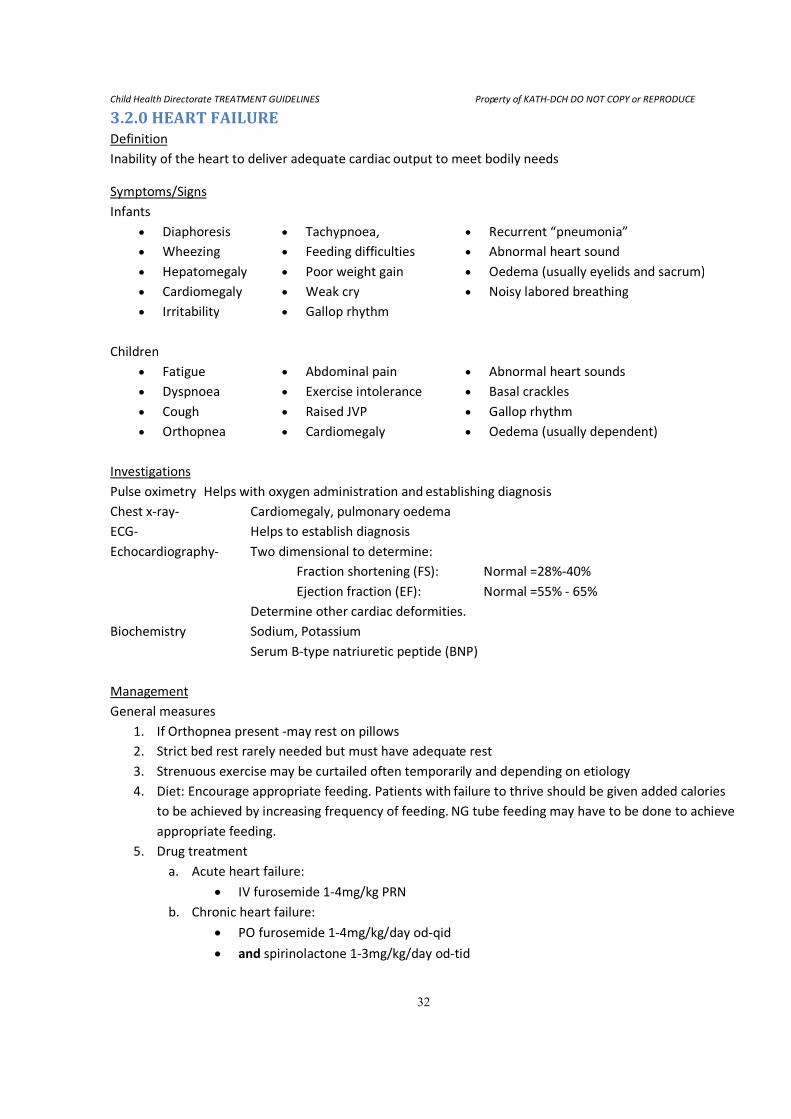
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
32
3.2.0 HEART FAILURE Definition
Inability of the heart to deliver adequate cardiac output to meet bodily needs
Symptoms/Signs
Infants
• Diaphoresis • Tachypnoea, • Recurrent “pneumonia”
• Wheezing • Feeding difficulties • Abnormal heart sound
• Hepatomegaly • Poor weight gain • Oedema (usually eyelids and sacrum)
• Cardiomegaly • Weak cry • Noisy labored breathing
• Irritability • Gallop rhythm
Children
• Fatigue • Abdominal pain • Abnormal heart sounds
• Dyspnoea • Exercise intolerance • Basal crackles
• Cough • Raised JVP • Gallop rhythm
• Orthopnea • Cardiomegaly • Oedema (usually dependent)
Investigations
Pulse oximetry Helps with oxygen administration and establishing diagnosis
Chest x-ray- Cardiomegaly, pulmonary oedema
ECG- Helps to establish diagnosis
Echocardiography- Two dimensional to determine:
Fraction shortening (FS): Normal =28%-40%
Ejection fraction (EF): Normal =55% - 65%
Determine other cardiac deformities.
Biochemistry Sodium, Potassium
Serum B-type natriuretic peptide (BNP)
Management
General measures
1. If Orthopnea present -may rest on pillows
2. Strict bed rest rarely needed but must have adequate rest
3. Strenuous exercise may be curtailed often temporarily and depending on etiology
4. Diet: Encourage appropriate feeding. Patients with failure to thrive should be given added calories
to be achieved by increasing frequency of feeding. NG tube feeding may have to be done to achieve
appropriate feeding.
5. Drug treatment
a. Acute heart failure:
• IV furosemide 1-4mg/kg PRN
b. Chronic heart failure:
• PO furosemide 1-4mg/kg/day od-qid
• and spirinolactone 1-3mg/kg/day od-tid
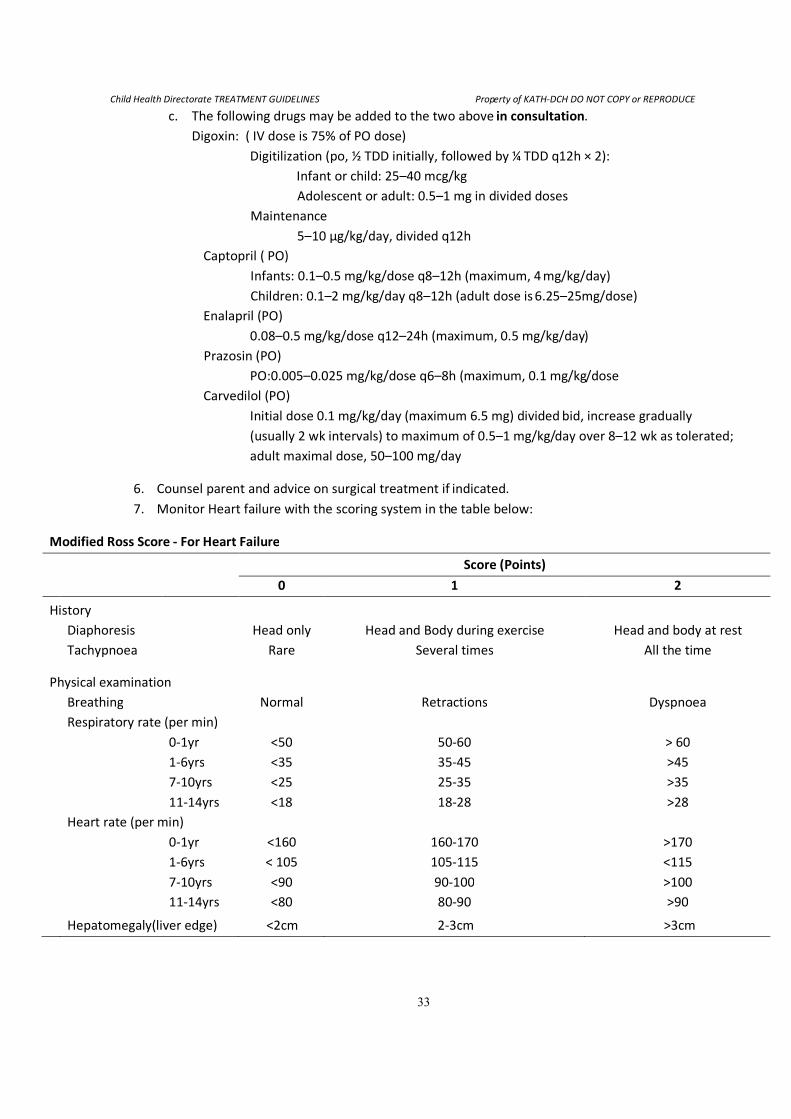
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
33
c. The following drugs may be added to the two above in consultation.
Digoxin: ( IV dose is 75% of PO dose)
Digitilization (po, ½ TDD initially, followed by ¼ TDD q12h × 2):
Infant or child: 25–40 mcg/kg
Adolescent or adult: 0.5–1 mg in divided doses
Maintenance
5–10 μg/kg/day, divided q12h
Captopril ( PO)
Infants: 0.1–0.5 mg/kg/dose q8–12h (maximum, 4 mg/kg/day)
Children: 0.1–2 mg/kg/day q8–12h (adult dose is 6.25–25mg/dose)
Enalapril (PO)
0.08–0.5 mg/kg/dose q12–24h (maximum, 0.5 mg/kg/day)
Prazosin (PO)
PO:0.005–0.025 mg/kg/dose q6–8h (maximum, 0.1 mg/kg/dose
Carvedilol (PO)
Initial dose 0.1 mg/kg/day (maximum 6.5 mg) divided bid, increase gradually
(usually 2 wk intervals) to maximum of 0.5–1 mg/kg/day over 8–12 wk as tolerated;
adult maximal dose, 50–100 mg/day
6. Counsel parent and advice on surgical treatment if indicated.
7. Monitor Heart failure with the scoring system in the table below:
Modified Ross Score - For Heart Failure
Score (Points)
0 1 2
History
Diaphoresis
Head only Head and Body during exercise Head and body at rest
Tachypnoea
Rare Several times All the time
Physical examination
Breathing
Normal Retractions Dyspnoea
Respiratory rate (per min)
0-1yr <50 50-60 > 60
1-6yrs <35 35-45 >45
7-10yrs <25 25-35 >35
11-14yrs <18 18-28 >28
Heart rate (per min)
0-1yr <160 160-170 >170
1-6yrs < 105 105-115 <115
7-10yrs <90 90-100 >100
11-14yrs <80 80-90 >90
Hepatomegaly(liver edge) <2cm 2-3cm >3cm
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
34
3.3.0 INFECTIVE ENDOCARDITIS (IE)
Definition:
Infection of the endocardium (+heart valves) by bacterial, viral, fungal and other microbes. Most often
caused by Streptcoccus viridians and staphylococcus aureus
Symptoms/signs
• Often History of congenital heart disease, rheumatic heart disease, surgery-dental, urinary tract,
intestinal, central venous catheter.
• Fever, chills, abdominal pain, myalgia, arthrigia, dyspnoea, malaise weight loss, night sweats.
• Tachycardia, Embolic phenomena (Roth spots, petechiae, splinter nail bed hemorrhages, Osler
nodes, CNS or ocular lesions), new r changing murmur, splenomagaly, arthritis, heart failure,
clubbing.
Modified duke’s criteria as a diagnostic tool
Two major or one major and three minor or five minor criteria is diagnostic of infective endocarditis.
1. Major criteria
• Positive blood cultures (two separate cultures for a usual pathogen, two or more for
less typical pathogens)
• Evidence of endocarditis on echocardiography (intracardiac mass on a valve or other
site, regurgitant flow near a prosthesis, abscess, partial dehiscence of prosthetic valves,
or new valve regurgitant flow)
2. Minor criteria
• Fever
• Predisposition – congenital heart disease, IV drug use, recent surgery, central catheter
use.
• Embolic vascular phenomenon - major arterial emboli, septic pulmonary infarcts,
mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, and Janeway
lesions
• Immunologic phenomena - glomerulonephritis, Osler's nodes, Roth spots , and
rheumatoid factor
• Microbiological evidence: positive blood culture but does not meet a major criterion as
noted in the major criteria
• Serological evidence of active infection with organism consistent with IE
• Echocardiographic findings: consistent with IE but do not meet a major criterion as
noted above
• Newly diagnosed clubbing
• Splenomegaly
• Splinter hemorrhages, and petechiae
• Elevated erythrocyte sedimentation rate
• Elevated C-reactive protein
• Presence of central non-feeding lines
• Presence of peripheral lines
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
35
Investigations:
• Blood C/S – three times preferably at the peak of the fever and before starting antibiotics
• FBC (Hb, WBC), C-reactive proteins, ESR,
• Urine R/E (hematuria)
• Chest X-ray (bilateral infiltrates)
• Echocardiography – vegetations, valve dysfunction
Management
• Start antibiotic as soon as possible
o Gentamycin: 5mg/kg/dose daily PLUS
o Penicillin: 300,000U/kg/day in 4-6 divided doses PLUS
o Flucloxacillin: 100mg/kg/day in 4 divided doses
• Further treatment based on antibiotic sensitivity
• Treat for at least 4 weeks (even if fever settles within a week)
• Treat heart failure as per the heart failure protocol
• Endocarditis prophylaxis
� Oral Amoxyl 40mg/kg at least 1hr before surgery OR
� IV/IM Ampicillin 50mg/kg 30mins before procedure OR
� Oral clindamycin 20mg/kg 1 hr before procedure OR
� Oral azithromycin 15mg/kg one hr before procedure
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
36
3.4.0 RHEUMATIC HEART DISEASE
Definition
This is inflammation of the endocardium and valves of the heart secondary to rheumatic fever. In
decreasing order the valves affected are mitral, aortic, tricuspid, and pulmonary valves.
Symptoms/signs
• Most cases are mild to moderate and usually are not symptomatic but patients often seen at KATH
are the severe ones
• Predominantly have signs of mitral regurgitation (MR), stenosis and mixed regurgitation and
stenosis
• Pansystolic murmur radiating to the axilla often present with MR.
• Mid-dastolic rumble indicates increased flow across mitral valve
• Mitral stenosis (MS) often present later in the disease and associated with a longer diastolic
murmur
• Other signs of heart failure described on page 32 may be present especially in severe disease
Investigations
• Chest x-ray: often shows cardiomegaly with mitralization of the left ventricle. Pulmonary artery
enlargement may also be seen
• ECG: p wave abnormalities (notched, tall) and features of left ventricular enlargement, arrhythmia.
• Echocardiography
Management
• In all cases
o Prophylaxis against rheumatic fever
a. IM Benzathine penicillin 1.2mu 3-4weekly for life or
b. Penicillin V 250mg bid for life or
c. Erythromycin 250mg bid for life
o Repeat echo every six months to one year
• MR - moderate to severe (often associated with symptoms)
o Prophylaxis against rheumatic heart disease
o Treat arrhythmia as indicated
o Endocarditis as indicated in the section on endocarditis
o Heart failure as indicated in the section on heart failure. Here predominantly ACE inhibitors
such as lisinopril and captopril are preferred.
o Surgical repair cand be sought but valve replacement shuld be delayed as long as possible if
well controlled by drugs alone till patients is 18yrs and older
• MS – moderate to severe
o Temporarily treat with decongestive drugs – diuretics
o Advice surgical repair/ balloon angioplasty as early as possible
• Aortic insufficiency –
o Often well tolerated so may require ACE inhibitors
o Valve replacement may be considered in severe case when patient is >18yrs
• Pulmonary and tricuspid valves diasese

Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
37
o Often responds to appropriate treatment of the left sided lession
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
38
3.5.0 TETRALOGY OF FALLOT (TOF) AND HYPERCYANOTIC (TET) SPELL Definition:
Cyanotic congenital heart disease characterized by
1. VSD
2. Right ventricular outflow tract obstruction
3. Right ventricular hypertrophy
4. Overriding aorta
Hypercyanotic spells is a sudden onset of paroxysmal hyperpnoea, irritability, increasing cyanosis and
decreased intensity for heart murmur in children often less than a year with TOF.
Signs/Symptoms
TOF: Dyspnoea on exertion, cyanosis (variable and often not present at birth), squatting, tachypnoea,
tachycardia, clubbing, polycythemia (plethora), ejection systolic murmur, stunting
tet spell: Tachypnoea, hyperpnoea, irritability, increasing cyanosis, unconsciousness, decreased intensity for
heart murmur, hemiparesis,
Investigation
N.B: not all cyanotic congenital heart diseases are Tetralogy of fallot!!
TOF:
1. Chest x-ray – typical “boot” shape
2. ECG – right axis deviation
3. Echocardiography – usually diagnostic
4. Full blood count - Hb, WBC
Tet spell: blood chemistry-pH, HCO3-,
Management
TOF stable state
1. Regular (6monthly reviews)
2. Iron 3mg/kg/day
3. May need to put infants with frequent tet spells on oral Propranolol
4. Appropriate feeding advice
5. Phlebotomy based only on Hemoglobin remains controversial so do not perform till patient has
signs of polycythemia.
TOF with tet spell
1. Place in knee chest position
2. Administer oxygen (has limited value so do not force it if infant combative)
3. IM/sc morphine 0.1-0.2mg/kg stat
The above usually aborts the attack but if persistent continue with the following
4. IV Propranolol 0.1-0.2mg/kg as slow IV push
5. Correct acidosis if present with 1mEq/kg IV.
Remember to discharge home on iron supplements!!
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
39
4.0 HAEMATOLOGICAL DISORDERS 4.1.0 SICKLE CELL DISEASE
Definitions
- Sickle cell disease: hemoglobinopathies characterized by the formation of sickled red cells in
response to deoxygenation
- Sickle cell anaemia: substitution of valine for glutamine in the 6th
amino acid position of the β chain.
- Others: HbSC, sickle-thalassemia combination.
- All sickle cell patients should be considered as immunocompromised host.
Therapy:
1. Stabilization: ABCs, treat shock, frequent reassessment
2. Hydration: Maintain adequate hydration, monitor volume status DO NOT over hydrate
3. Liberal pain control: relaxes patient, and enhances pulmonary toilet.
4. *Treat infection
• Antimalarial: consider local resistance & sensitivity pattern (e.g. Give Quinine or ACT)
• Antibiotics: must provide coverage for encapsulated organism
(e.g. Strept. pneumoniae, H. influenzae) & others like Staphylococcus, Salmonella
5. *Haemotransfusion: partial exchange/straight transfusion (see anaemia transfusion)
ASSOCIATED ACUTE ILLNESS:
GENERAL PRINCIPLES OF MANAGEMENT IN ACUTE EPISODES
o Make sure diagnosis of SCD has been confirmed by relevant laboratory findings
o Take cognizance of presence or otherwise of any long term complications of SCD e.g. Renal
Failure.
o Always do routine tests for established patients.
o Look for source of infection by doing Blood cultures, thick/thin film for MP’s, Urine R/E etc.
o Prescribe a curative antimalarial according to National Protocol
o Prescribe appropriate antibiotics if infection is present
o Relieve distress
o Aim to improve vascular blood flow by ensuring adequate hydration
o Aim to mobilize patient early
4.1.1 INFECTION (MALARIA/SEPSIS/PNEUMONIA/OSTEOMYELITIS/UTIS ETC) Clinical Assessment: fever and/or other signs/symptoms of infection
FBC + B/F for MP’s, ± blood & urine C/S
CXR, LP if indicated & no contraindication(s)
Management: ABC’s, freq. reassessment, hydration, analgesics ± antimalarial,
antibiotics, O2.
DO NOT delay antibiotics while waiting for C/S
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
40
Acute Osteomyelitis:
Most common organisms - Staphylococcus species
Salmonella species
Investigations:
1. Bone marrow culture an infection site – Needle aspiration
2. Blood culture/sensitivity
3. Stool culture/sensitivity
4. Rule out Koch’s disease
5. X-ray of affected bone – Changes seen about 10-14 days after onset
Treatment:
Initial therapy before culture and sensitivity results should cover both staphylococcus and samonella
species. Fair choice antibiotics include clindamycin, vancomycin for staphylococcus and
chloramphenicol for salmonella. Other useful antibiotics for salmonella include thrimethoprim-
sulfamethoxizole, aminoglycosides, 2nd
and 3rd
generation cephalosporins and ciprofloxacin in adults.
Duration of therapy – About 4 – 6 weeks
Parenteral antibiotics is necessary in the first 10 days
Hand Foot Syndrome:
Treatment
1. Analgesics
2. Hydration
3. Parental reassurance
Note – Early osteomyelitis can mimic this syndrome
� In the presence of fever, marked inflammation or no clinical improvement after 3 days –
Evaluate for osteomyelitis.
4.1.2 HYPERHEMOLYTIC CRISIS Clinical Assessment: ↑icterus, acute drop in Hb, haemoglobinuria FBC, RBCs indices, rectic count
Management: ABCs, O2, serial PCV & urine monitor
Treat infection, hydration ± transfusion
4.1.3 SPLENIC SEQUESTRATION (MASSIVE RBCS + PLASMA SEQUESTRATION IN SPLEEN)
Clinical Assessment: Acute drop in Hb > 2g/dl,anaemia, ↑ retic, ↓platelet Pallor, irritable, abd.
pain/distension, ↓ intravascular volume. FBC, RBCs indices, rectic count
Management: ABC’s, & freq. reassessment
Treat shock, hydration, ± haemotransfusion, analgesics, antimalarial & antibiotics
4.1.4 APLASTIC CRISIS (CESSATION OF ERYTHROPOIESIS) Clinical Assessment: Hx of URTI signs/symptoms, rapid ↓Hb, ↓retic, pallor, weak
FBC, RBCs indices, rectic count
Management: If stable, monitor closely; spontaneous resolution 1-2weeks
If unstable �ABCs, freq. assessment + top-up transfusions
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
41
4.1.5 VASO-OCCLUSIVE CRISIS Pain
Clinical Assessment: precipitants; (hypoxia, dehydration acidosis, infection) long bone or abd.
pain, dactylitis (6-12mths) R/o infection, acute abd. and osteomyelitis
Management:
The GOAL of therapy is to provide prompt pain relief.
o Hydration, analgesics & treat infection if present
Assess pain and categorize into:
Mild: Pain limited to a single joint or limb of bearable intensity and without any associated
symptoms/signs e.g. Fever, anaemia.
Should be treated on out-patient basis.
Moderate: Pain affecting multiple sites impairing normal activity without any associated symptoms
or signs.
Can be treated on outpatient basis except where social circumstances of the patient and good sense
indicate otherwise
Severe: Severe pain in single or multiple sites
1. With or without associated symptoms/signs
2. Abdominal crisis (pain)
3. Chest pain
4. Severe headache
Patient must be detained in the first instance (if recovery ward is available) and admitted if
symptoms have not subsided after 24-48 hours.
Mild – Moderate Painful Episodes:
o Try to identify the precipitating factor(s)
o Ascertain that the patient’s temperature is normal
o Investigate thoroughly – refer labs for established patients
o Encourage high oral fluid intake
o Start with simple analgesics- e.g. Paracetamol 10mg/kg every 4-6 hrs or Ibuprofen 5-
10mg/kg/dose every 6-8hrs.
Note: Alternating paracetamol and ibuprofen doses 3 hourly offers sustained pain relief
Moderate pain demands the use of higher NSAIDs e.g. Tramadol, Toradol or Codeine.
Ketorolac (Toradol) 1mg/kg load, followed by 0.5mg/kg every 6hrs
o Warm baths, massage and application of warm pads help relieve pain
o Give curative dose of antimalarial
o See patient within 3-5 days to assess and alter management if indicated.
Severe Pain
o Admit patient
o Do Numbers 1-4 under Mild to Moderate pain
o Give IV fluids (N/S or D). Total volume should not exceed 1.5X maintenance requirement
for 24hrs for the patient.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
42
o Give analgesic:
Start with a strong NSAID e.g.: Ketorolac (Toradol) - 1 mg/kg stat, followed by 0.5mg/kg
every 6 hours;
Morphine: Parenteral: 100mcg/kg 4 hourly
PO: 80-200mcg/kg 4 hourly
There should be no PRN regimen
Assess patient frequently- every hour
4.1.5.1 PRIAPISM
Clinical Assessment: painful erection, most often seen in adolescents
Management: hydration & analgesics, avoid over hydration, if 4-6hrs no resolution
�haemotransfusion & Urology consult
4.1.5.2 ACUTE CHEST SYNDROME (PNEUMONIA/INFARCT)
Clinical Assessment: cough, pleuritic chest pain, tachypnea, hypoxia, CXR (changes in lugs)
Management: ABCs, O2, hydration (1X maintenance volume), analgesics, antibiotics
Consider haemotransfusion, mycoplasma, & PTB
4.1.5.3 CVA
Clinical Assessment: headache, seizure, weakness, altered sensorium
Focal neurologic defecit
Must R/o meningitis, abscess, frontal bone infact
Management: ABCs, frequent reassessment, O2, hydration ± antibiotics,
haemotransfusion
Control seizure & ICP
4.1.6 INDICATIONS FOR BLOOD TRANSFUSION:
1. A need to improve oxygen-carrying capacity and transport. Transfusions should be
SIMPLE TRANSFUSION a. Anaemic patients with impending or overt high output cardiac failure, dyspnoea, postural
hypotension angina or cerebral dysfunction.
b. Acute splenic or hepatic sequestration crisis
c. Hb less than 5gm/dl and PCV less than 15%, associated erythroid hypoplasia or aplasia
2. A need to improve microvascular perfusion by decreasing the proportion of erythrocytes containing HbS. (Partial exchange transfusion)
a. Acute impending or suspected cerebro-vascular accidents, including transient
ischaemic attacks
b. Arterial hypoxia syndrome (“fat embolism”)
c. Acute progressive lung disease
d. Unresponsive acute Priapism
e. Eye surgery
4.1.7 CHRONIC COMPLICATIONS A. Leg Ulcers:
1. Always treat in collaboration with plastic surgeon
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
43
2. Search for other causes of leg ulcers such as varicose veins, diabetes mellitus and collagen
vascular diseases.
3. Radiography of the leg to rule out underlying bony infection
4. Wound swab for culture and sensitivity
5. Daily dressing
Failure to Heal:
1. Try chronic blood transfusions to raise Hb to 10mg/dl for a period of six months.
2. Try skin grafting
B. Aseptic Necrosis:
1. Always treat in collaboration with specialist Orthopaedic Surgeons
2. Radiograph in AP and frog-leg position.
3. In early case and in children in particular
- Avoidance of weight bearing not motion with the use of braces.
- Appliance of local hat and analgesics for up to 6 months
4. In individuals beyond adolescence and with severe aseptic necrosis, surgical replacement may
be considered.
C. Hypersplenism
Diagnosis: - Spleen 4cm or more below coastal margin
- Hb less that 6.5g/dl
- Reticulocyte count above 15
- Platelets count below 2000x109/L
- Observed on 2 occasions 6 months apart.
Treatment:
1. Chronic transfusion programmes
2. Splenectomy – preferable refer Surgeon
Equivocal Indication- no clear cut evidence whether transfusion is either useful or necessary.
a. Preparation for surgery requiring general anaesthesia
b. Intractable acute events
c. Before injection of contrast material
D. Chronic Transfusion:
This may be relevant for several chronic conditions related to sickle cell disease. In these cases the
proportion of normal cells circulating should be maintained above 70% by repeated simple
transfusion. Clear indication is for:
- Cerebral vascular occlusion (stroke)
Other less clear indications are:
- leg ulcers - chronic organ damage
- skin graft - pregnancy
- extreme diminution of performance status due to recurrent complications of SCD.
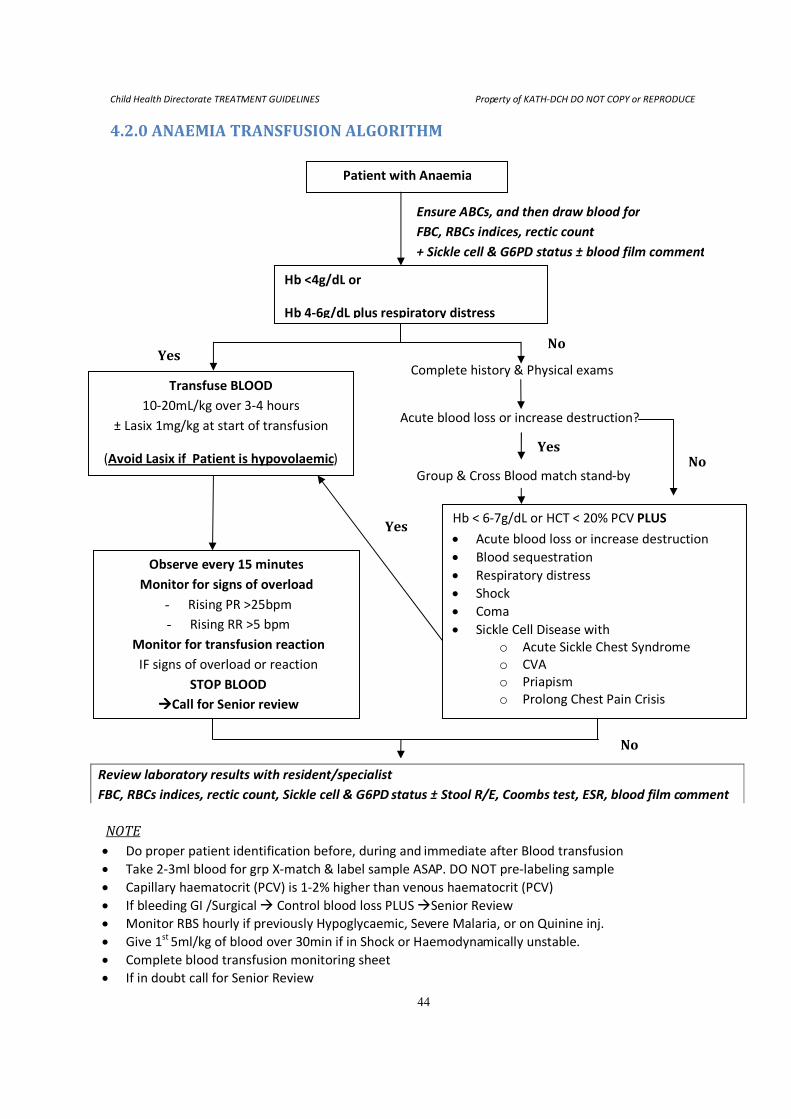
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
44
4.2.0 ANAEMIA TRANSFUSION ALGORITHM
Hb < 6-7g/dL or HCT < 20% PCV PLUS
• Acute blood loss or increase destruction
• Blood sequestration
• Respiratory distress
• Shock
• Coma
• Sickle Cell Disease with
o Acute Sickle Chest Syndrome
o CVA
o Priapism
o Prolong Chest Pain Crisis
Observe every 15 minutes
Monitor for signs of overload
- Rising PR >25bpm
- Rising RR >5 bpm
Monitor for transfusion reaction
IF signs of overload or reaction
STOP BLOOD
����Call for Senior review
Group & Cross Blood match stand-by
Acute blood loss or increase destruction?
Transfuse BLOOD
10-20mL/kg over 3-4 hours
± Lasix 1mg/kg at start of transfusion
(Avoid Lasix if Patient is hypovolaemic)
Complete history & Physical exams
Hb <4g/dL or
Hb 4-6g/dL plus respiratory distress
Ensure ABCs, and then draw blood for
FBC, RBCs indices, rectic count
+ Sickle cell & G6PD status ± blood film comment
Patient with Anaemia
Yes No
No Yes
Yes
No
Review laboratory results with resident/specialist
FBC, RBCs indices, rectic count, Sickle cell & G6PD status ± Stool R/E, Coombs test, ESR, blood film comment
NOTE
• Do proper patient identification before, during and immediate after Blood transfusion
• Take 2-3ml blood for grp X-match & label sample ASAP. DO NOT pre-labeling sample
• Capillary haematocrit (PCV) is 1-2% higher than venous haematocrit (PCV)
• If bleeding GI /Surgical � Control blood loss PLUS �Senior Review
• Monitor RBS hourly if previously Hypoglycaemic, Severe Malaria, or on Quinine inj.
• Give 1st
5ml/kg of blood over 30min if in Shock or Haemodynamically unstable.
• Complete blood transfusion monitoring sheet
• If in doubt call for Senior Review
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
45
5.0 INFECTIOUS DISEASES 5.1.0 MENINGITIS
1. DIAGNOSIS:
• Bacterial infection of the meninges = bacterial meningitis
• High index of suspicion as symptoms can be subtle, especially in infants.
• Symptoms may include headache, neck pains, neck stiffness, irritability etc.
• LP for CSF -Cellular CSF (>5 wbc) with/without positive culture
• Do Blood c/s if child not stable for an LP* (see below for contra-indications)
2. ORGANISM COMMONLY CAUSING BACTERIAL MENINGITIS Neonatal period E. coli and other Gram-negative organisms
Listeria monocytogenes, (rarely seen at KATH)
Group B streptococcus (rarely seen at KATH)
1 month - 6 years Neisseria meningitides (meningococcus)
Streptococcus pneumoniae(pneumococcus)
Haemophilus influenza
>6 years Neisseria meningitides (meningococcus)
Streptococcus pneumoniae(pneumococcus)
3. ASSESSMENT
History Examination Investigation
Fever Fever Blood glucose
Headache Purpuric rash FBC + MP’s
Photophobia Photophobia CSF c/s, Protein & glucose
Poor feeding / vomiting Convulsion Blood c/s
Irritability Neck stiffness/bulging fontanelle
Hypotonia Kernig / Brudzinski sign +ve
Drowsiness Irritable child
Coma Coma / Drowsy
*Contra-indications for lumbar puncture
I. Focal neurological signs II. Clinical signs of raised ICP (apart from bulging fontanelle)
III. Coagulopathy IV. Local infection at site of needle insertion
V. Cardiopulmonary
instability
VI. If it causes undue delay in the administration of antibiotics (+ve
culture still possible within 2hrs of antibiotic administration)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
46
4. TREATMENT / MANAGEMENT PRIORITIES:
Antibiotics
<1 month Penicillin + Gentamycin
(Second line: 3rd
generation cephalosporin e.g. cefotaxime or ceftriaxone)
>3 months Penicillin G & Chloramphenicol
(Second line: 3rd
generation cephalosporin e.g. certriaxone or cefotaxime)
Duration,
Pneumococcus ~10- 14days
Meningococcus ~5 - 7days
Haemophilus influenzae ~7 -10days
Other Gram-negative organisms ~ >21days
Steroids
• >1 month – 6 years old child, give Dexamethasone @ 0.6/kg/day in 3-4 divided doses (or
0.4mg/kg/dose Q12h) for 2-4 days.
• Start as soon as possible, preferable before 1st dose of antibiotics.
Fluids
• If in shock, resuscitate with 0.9% Normal saline or Ringers Lactate or Colloids.
• Correct / prevent hypoglycaemia.
• Restrict fluid to 70% maintenance, but not at the expense of adequate intravascular volume.
• DO NOT give fluids containing no sodium to patients with meningitis unless you are just keeping the
line open.
Cerebral monitoring
• Stop / control seizures with anticonvulsant (fever with tepid sponge & antipyretic)
• Monitor coma score, brainstem function for herniation, BP, HR, RR, Temp.(see neurology section)
Public health notification & antibiotic prophylaxis of contacts
Meningococcus:
Postexposure chemoprophylaxis
� Rifampicin:
o <1mth old 10mg/kg/day in 2 divided doses for 2 days
o >1mth old 20mg/kg/day in 2divided doses for 2 days
(max.1200mg/day)
� Ceftriaxone:
o 50-75mg/kg stat IM/IV
� Ciprofloxacin:
o 500-750mg stat for non-pregnant adult (i.e. >12yrs)
� Exposed persons-
o household, child care, and nursery school contacts
o Potential contact with oral secretions of infected patient.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
47
Haemophilus influenzae:
Postexposure chemoprophylaxis
� Rifampicin:
o <1mth old 10mg/kg PO daily for 4 days
o >1mth old 20mg/kg PO daily for 4 days (max.600mg/day)
� Ceftriaxone:
o 50-75mg/kg stat IM/IV
� Exposed persons
o <4yrs-household, child care, and nursery school contacts
o Potential contact with oral secretions of infected patient.
5. COMPLICATIONS
i) Local vasculitis
ii) Local cerebral infarction
iii) Subdural effusion
iv) Hydrocephalus
v) Cerebral abscess
6. DRUG DOSAGES FOR BACTERIAL MENINGITIS BEYOND THE NEONATAL PERIOD
DRUG DOSAGE
Penicillin G
Ampicillin
Chloramphenicol
Cefotaxime
Ceftriaxone
Ciprofloxacin
Cefuroxime
0.5 - 0.6mu /kg/day in 4-6 divided doses
150 -200mg/kg/day in 4 divided doses
100mg/kg/day in 4 divided doses
150-200mg/kg/day in 3-4divided doses
80 - 100mg/kg/day daily
30mg/kg/day in 2 divided doses
200 -240mg/kg/day in 3-4 divided doses
Meropenem 40mg/kg/dose Q8hrly
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
48
5.2.0 SEVERE MALARIA DEFINITION
Plasmodium falciparum malaria infection which is of immediate threat to life, it is a medical
emergency, and may present with;
• Confusion
• Prostration
• Coma
• Convulsions
• Severe anaemia
• Acute renal failure
• Hypoglycaemia
• Metabolic acidosis
• Acute Respiratory Distress Syndrome (non-cardiogenic pulmonary oedema)
• Respiratory distress
• Circulatory collapse, shock (algid malaria)
• Spontaneous bleeding and coagulopathy
• Hyperpyrexia
• Hepatic dysfunction (Jaundice)
• Hyperparasitaemia
• Malarial haemoglobinuria
5.2.1 CEREBRAL MALARIA
1. DIAGNOSIS:-
• Falciparum malaria evidence
• Unarousable coma. Blantyre coma score ≤ 2/5
• Rule out other causes of encephalopathy
2. ASSESSMENT
• Airway (maintain patent) or protect airway if actively convulsing
• Breathing, rate and depth of respiration
• Circulation, pulse rate and blood pressure
• Temperature
• Level of consciousness (Blantyre coma score)
• State of hydration
• Presence of aneamia (palmer / conjunctival pallor) or bleeding
• Investigation
a. Finger–prick blood glucose
b. Thick and thin films for malaria parasite
c. Haematocrit (PCV), ± lumbar puncture.
d. FBC (leucocytosis is not unusual in severe disease and does not necessarily imply an
associated bacterial infection.)
e. Blood culture in suspected septicaemia (e.g. algid malaria)
Assess deepness of coma with a coma scale familiar with other health staff (see examples in neurology
section)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
49
3. MANAGEMENT OF SEVERE MALARIA
• Maintain airway and oxygenation ± supplementary oxygen to keep SaO2>92%
• Maintain adequate hydration +Treat/Correct shock if present
• Exclude/ treat hypoglycaemia.
• Start 5 - 10% Dextrose containing fluid till able to tolerate enteric feeding.
• Start appropriate anti malarial immediately, preferable parenteral.
• Treat convulsions with anticonvulsants e.g. benzodiazepam, phenobarbitone, phenytoin
• Exclude other treatable causes of coma.
• Record fluid intake & output.
• Haemotransfuse screened fresh whole blood or packed cells for severe anaemia.
• Antibiotics for suspect Gram-negative septicaemia in children with shock, (i.e. algid malaria).
• Monitor & record vital signs brain stem function and level of consciousness.
• Manage complications appropriately
4. ANTIMALARIAL
A. QUININE (IM)
Indications: Cerebral malaria, Malaria with altered sensorium, other forms of severe malaria
• Give 20mg dichloride salt/kg (loading dose) then 10mg salt /kg Q8hrly for 24-48hrs, then Q12hrly
until the Patient can swallow, then oral quinine @10mg salt /kg Q8hrly to completed a 7-day
course of treatment or give complete course of an effective ACT.
• Give IM quinine in the anterior/anterior-lateral thigh (not in the buttocks).
• The loading dose of quinine should be divided between 2 sites, half the dose in each anterior
/anterior-lateral thigh
• Dilute quinine in normal saline to a concentration of 60 - 100mg salt /ml.
• May give Quinine as IV infusion in Dextrose @ < 3-5mg/kg/hr; Same dose as above
B. ARTERMISININ OR ARTERSUNATE INJECTION/SUPPOSITORY
• Injection Artesunate (IM/IV) 2.4mg/kg /dose
• Injection Artemeter (IM) 3.2mg/kg/dose
• Rectal Artesunate (PR) 5mg/kg/dose
• Dihydroartermisinin (IM/PR) 2mg/kg/dose
Give on 0hr, 12hr, 24hr then daily (i.e. Q12h for 24hrs, then Q24h)
a. till patient can take oral then give a complete course of oral ACT
b. for 7 completed days
C. ARTERMISININ COMBINATION THERAPY (ACT)
Indication: for uncomplicated malaria, continuation treatment after parenteral quinine.
a. Amodiaquine / Artesunate(PO)
• Oral Amodiaquine at 8-10mg/kg/day for 3 days PLUS Artersunate at 4-5mg/kg/day for 3days
b. Artemether/Lumefantrine 20/120mg (e.g. Coartem)
Dose schedule: 0hr repeat dose after 8hrs then Q12h for 2days
• 5 -15kg @ I tablet/dose • 15-25kg @ 2 tablets/dose
• 25-35kg @ 3 tablets/dose • >35kg @ 4 tablets/dose
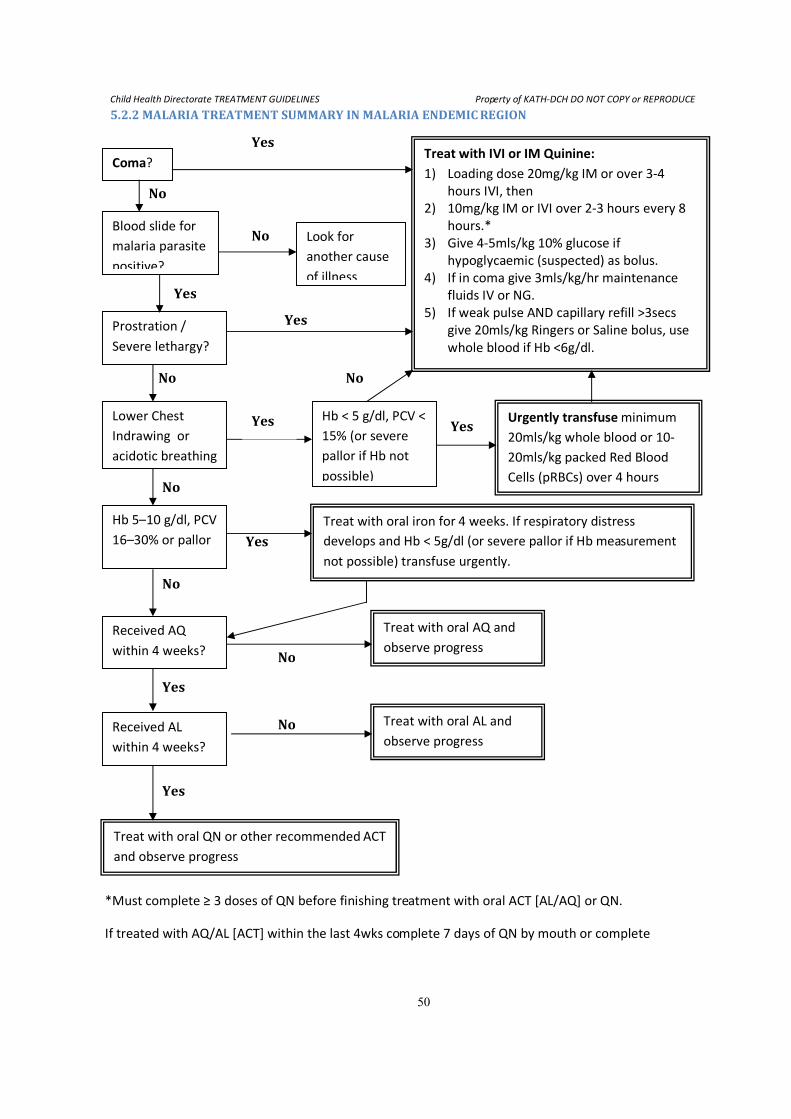
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
50
5.2.2 MALARIA TREATMENT SUMMARY IN MALARIA ENDEMIC REGION
Coma? Treat with IVI or IM Quinine:
1) Loading dose 20mg/kg IM or over 3-4
hours IVI, then
2) 10mg/kg IM or IVI over 2-3 hours every 8
hours.*
3) Give 4-5mls/kg 10% glucose if
hypoglycaemic (suspected) as bolus.
4) If in coma give 3mls/kg/hr maintenance
fluids IV or NG.
5) If weak pulse AND capillary refill >3secs
give 20mls/kg Ringers or Saline bolus, use
whole blood if Hb <6g/dl.
Blood slide for
malaria parasite
positive?
Look for
another cause
of illness
Prostration /
Severe lethargy?
Lower Chest
Indrawing or
acidotic breathing
Hb < 5 g/dl, PCV <
15% (or severe
pallor if Hb not
possible)
Urgently transfuse minimum
20mls/kg whole blood or 10-
20mls/kg packed Red Blood
Cells (pRBCs) over 4 hours
Hb 5–10 g/dl, PCV
16–30% or pallor
Treat with oral iron for 4 weeks. If respiratory distress
develops and Hb < 5g/dl (or severe pallor if Hb measurement
not possible) transfuse urgently.
Received AQ
within 4 weeks?
Treat with oral AQ and
observe progress
Received AL
within 4 weeks?
Treat with oral AL and
observe progress
Treat with oral QN or other recommended ACT
and observe progress
Yes
Yes
Yes
No
No
No
Yes
Yes
Yes
No
No
No
Yes
Yes
No No
*Must complete ≥ 3 doses of QN before finishing treatment with oral ACT [AL/AQ] or QN.
If treated with AQ/AL [ACT] within the last 4wks complete 7 days of QN by mouth or complete
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
51
5.3.0 TETANUS Definition
Acute spastic paralytic illness caused by tetanospasmin, an exotoxin (neurotoxin) produced by clostridium
tetani
Clinical features
Incubation period typically 2 – 14 days, but may be as long as several months after the injury, often
forgotten.
May present as
o localized tetanus or
o generalized tetanus.
Clinical features
o Main features are trismus ± other rigid muscles (spasms) with clear sensorium.
o Other features are fever, tachycardia
Localized tetanus
Painful spasm of the muscles adjacent to the wound site. This may precede generalized tetanus.
I. Cephalic tetanus:-
Involves the bulbular musculature on account of wounds on the head, nostrils, face or chronic otitis
media and may present as
o retracted eyelid,
o deviated gaze,
o trismus,
o spastic paralysis of the tongue / pharyngeal musculature
II. Generalized tetanus
Disturbance by sight, sound or touch may trigger sudden, severe tonic contraction of the muscles
with fist clenching, flexion and adduction of the arms hyperextension of the legs.
Differential Diagnosis
• Meningitis
• Dental or Para/Retro-pharyngeal abscess
• Rabies
• Acute encephalitis involving the brain stem
Management
• Eradication of Clostridium tetani
o Clean wounds, debride as needed
o Antibiotics for 10 – 14 days
Penicillin @ 0.2 - 0.3mu/kg/day ÷ 6hrly ± Metronidazole @ 30mg/kg/day ÷ 8hrly x 5days
Or Erythromycin, tetracycline (children≥ 8yrs) for penicillin allergy
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
52
• Immune therapy
Optimal doses not determined. Adults and children receive the same dose
a. Usual doses given after a test dose (for ATS), are either:
o Human tetanus Immune globulin (TIG) @ 5,000U – 6,000U intramuscularly OR
o Anti tetanus Serum (ATS) @ 50,000U – 100,000U. Give half IV and other half IM
b. Active immunization with 3 doses of Tetanus toxoid (Td) 0.5ml.
Separate syringes and separate site from ATS or TIG!
Give 2nd
dose 4-6weeks from 1st
dose and 3rd
dose 6-12 months from the 2nd
dose
• Control of spasms (Given in alternate regimens)
o Diazepam 0.05-0.2mg/kg SLOW IV or 0.3-0.5mg /kg PR (max. 10mg/dose) Q 4-6hrly
o Phenobarbitone 5 - 10mg/kg/8-12hrly IM
o Chlorpromazine 0.5mg/kg/ 6-8hrly IM
� May combine any two of the above or intravenous Midazolam infusion
� Caution: Beware and monitor for possible respiratory distress
Consider paralysing and mechanical ventilation if the above fail to control spasms
• Supportive care
Nurse meticulously in a quiet, secluded setting
Complications
• Aspiration
• Apnea
• Intramuscular haematoma
• Soft tissue injury
• Fracture
• Rhbdomyolsis � Myoglobinuria � Renal failure
• Cardiac arrhythmias
• Serum sickness
• Labile temperature
• Unstable blood pressure
Prevention
• Injury prevention
• Early and effective wound management(i.e. Cleaning and removal of foreign bodies)
• Use of sterile equipment or sharps
• Adequate tetanus prophylaxis for injuries
• Adequate infant and pregnant women immunization (i.e. Universal immunization)
• Adequate immunization for nursing mothers’ of children with neonatal tetanus
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
53
6.0 MALNUTRITION 6.1.0 DEFINITION AND GENERAL GUIDELINES
DEFINITION:
• Severe malnutrition (multiple nutrient deficiencies) is characterised by oedema or wasting, usually with
anorexia and infection
• Severe Acute Malnutrition (SAM) is defined as weight-for-height of < - 3 SD/ 70% Expected Weight OR
bilateral oedema in the presence of other signs of malnutrition/absence of other causes of oedema .
• Two clinical pictures are seen with much overlap (marasmus and kwashiorkor)
Both have severe hypoproteinaemia, hypokalaemia, hypomagnesaemia and hypogylycaemia, and
anaemia
CLASSIFICATION OF MALNUTRITION
Moderate malnutrition Severe malnutrition
Oedema No Yes (kwashiorkor)
Weight for height <-2 SD <-3 SD (marasmus)
Height for age <-2SD (moderate stunting) <-3SD (severe stunting)
CLINICAL MANAGEMENT
• All cases should have the PEM data (enclosed in patient’s folder) filled in whole by the attending
doctor (i.e. the admission data, laboratory data, and discharge/demise data).
• Weight and Height should always be re-checked on admission using the appropriate height
measuring device and Weight-for Height (Z-score) computed.
• Body weight should be measured and recorded every other day.
• The under-listed investigations should be done ROUTINELY for all cases:
I. Blood
• Full Blood Count (haematology) • Culture & Sensitivity
II. Urine
• Dipstick + microscopy • Culture & Sensitivity
III. Stool R/E
IV. Chest X-ray (with Radiologist’s report)
V. Provider initiated Counseling and Testing for HIV*
VI. ± Gastric Lavage (Discuss with senior resident/specialist)
VII. LFT
VIII. Other Investigations as may be necessary
• Acute complications must ALWAYS be looked for and treated appropriately (see overleaf)
*Counseling and testing for HIV should only be done when the patient has been well stabilized and parents
are in the best psychological state of the mind to undergo counseling. Results of the test must remain
PRIVATE AND CONFIDENTIAL and should only be released to the head nutritionist and/or consultant.
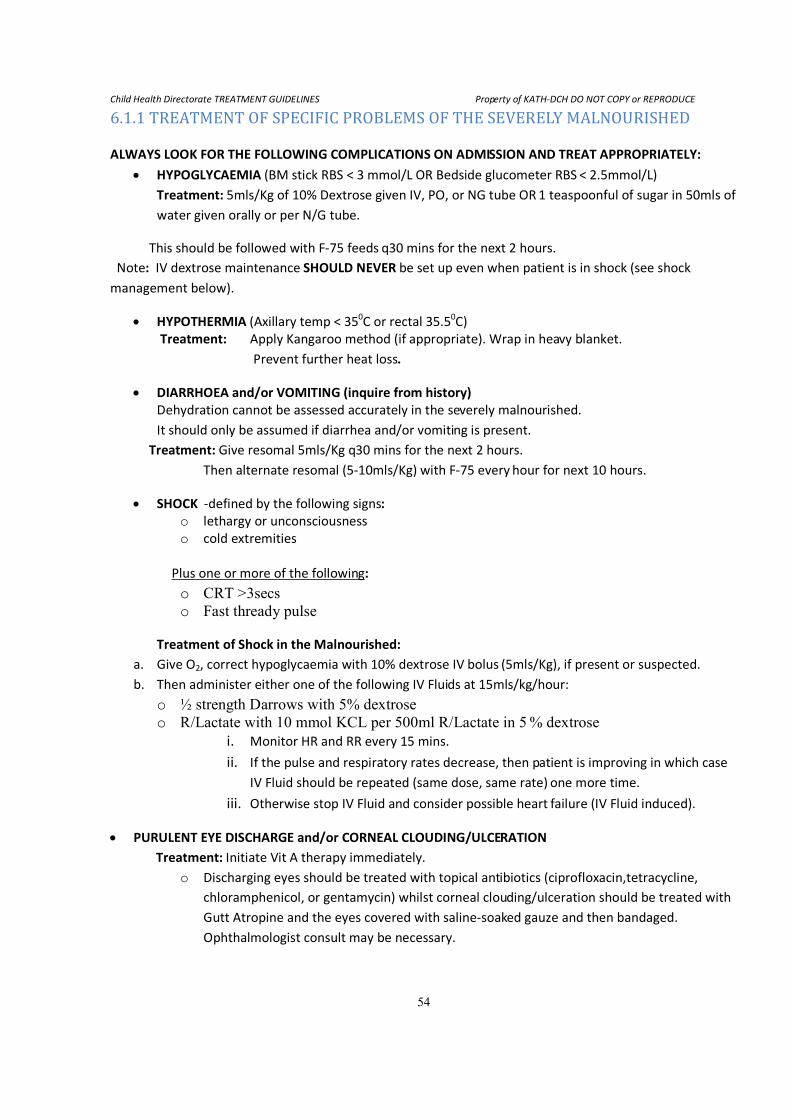
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
54
6.1.1 TREATMENT OF SPECIFIC PROBLEMS OF THE SEVERELY MALNOURISHED
ALWAYS LOOK FOR THE FOLLOWING COMPLICATIONS ON ADMISSION AND TREAT APPROPRIATELY:
• HYPOGLYCAEMIA (BM stick RBS < 3 mmol/L OR Bedside glucometer RBS < 2.5mmol/L)
Treatment: 5mls/Kg of 10% Dextrose given IV, PO, or NG tube OR 1 teaspoonful of sugar in 50mls of
water given orally or per N/G tube.
This should be followed with F-75 feeds q30 mins for the next 2 hours.
Note: IV dextrose maintenance SHOULD NEVER be set up even when patient is in shock (see shock
management below).
• HYPOTHERMIA (Axillary temp < 350C or rectal 35.5
0C)
Treatment: Apply Kangaroo method (if appropriate). Wrap in heavy blanket.
Prevent further heat loss.
• DIARRHOEA and/or VOMITING (inquire from history)
Dehydration cannot be assessed accurately in the severely malnourished.
It should only be assumed if diarrhea and/or vomiting is present.
Treatment: Give resomal 5mls/Kg q30 mins for the next 2 hours.
Then alternate resomal (5-10mls/Kg) with F-75 every hour for next 10 hours.
• SHOCK -defined by the following signs:
o lethargy or unconsciousness
o cold extremities
Plus one or more of the following:
o CRT >3secs
o Fast thready pulse
Treatment of Shock in the Malnourished:
a. Give O2, correct hypoglycaemia with 10% dextrose IV bolus (5mls/Kg), if present or suspected.
b. Then administer either one of the following IV Fluids at 15mls/kg/hour:
o ½ strength Darrows with 5% dextrose
o R/Lactate with 10 mmol KCL per 500ml R/Lactate in 5 % dextrose
i. Monitor HR and RR every 15 mins.
ii. If the pulse and respiratory rates decrease, then patient is improving in which case
IV Fluid should be repeated (same dose, same rate) one more time.
iii. Otherwise stop IV Fluid and consider possible heart failure (IV Fluid induced).
• PURULENT EYE DISCHARGE and/or CORNEAL CLOUDING/ULCERATION
Treatment: Initiate Vit A therapy immediately.
o Discharging eyes should be treated with topical antibiotics (ciprofloxacin,tetracycline,
chloramphenicol, or gentamycin) whilst corneal clouding/ulceration should be treated with
Gutt Atropine and the eyes covered with saline-soaked gauze and then bandaged.
Ophthalmologist consult may be necessary.
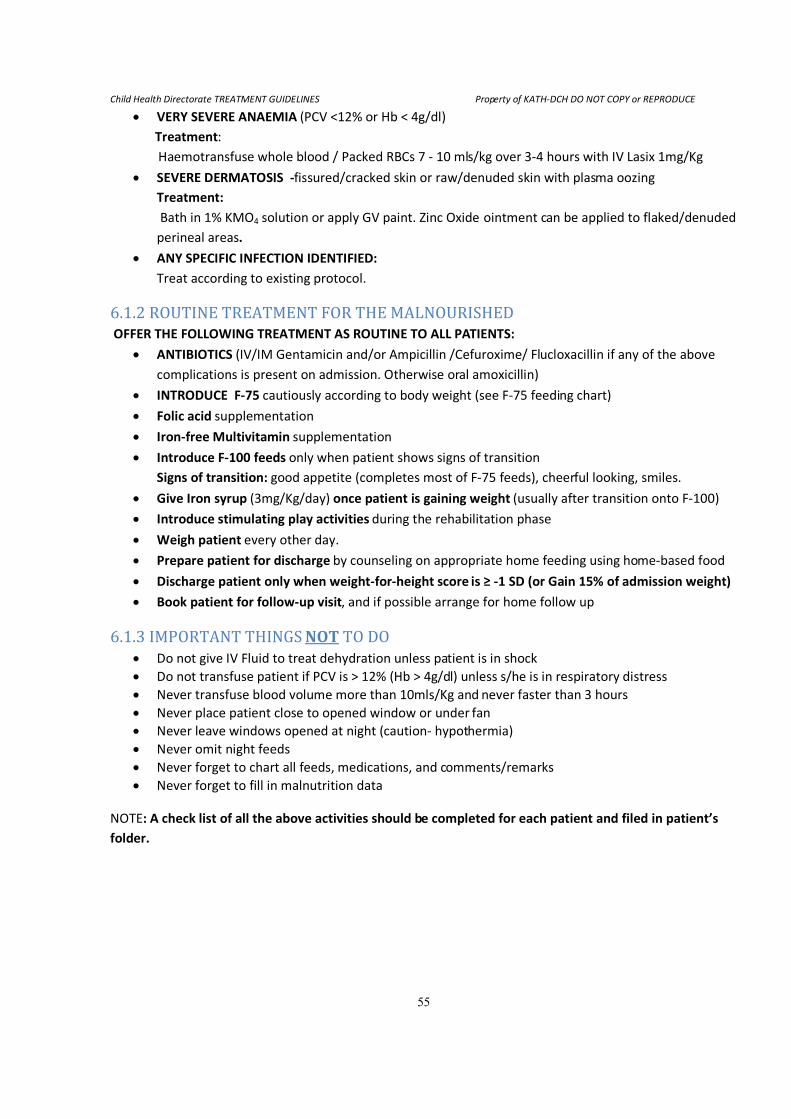
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
55
• VERY SEVERE ANAEMIA (PCV <12% or Hb < 4g/dl)
Treatment:
Haemotransfuse whole blood / Packed RBCs 7 - 10 mls/kg over 3-4 hours with IV Lasix 1mg/Kg
• SEVERE DERMATOSIS -fissured/cracked skin or raw/denuded skin with plasma oozing
Treatment:
Bath in 1% KMO4 solution or apply GV paint. Zinc Oxide ointment can be applied to flaked/denuded
perineal areas.
• ANY SPECIFIC INFECTION IDENTIFIED:
Treat according to existing protocol.
6.1.2 ROUTINE TREATMENT FOR THE MALNOURISHED
OFFER THE FOLLOWING TREATMENT AS ROUTINE TO ALL PATIENTS:
• ANTIBIOTICS (IV/IM Gentamicin and/or Ampicillin /Cefuroxime/ Flucloxacillin if any of the above
complications is present on admission. Otherwise oral amoxicillin)
• INTRODUCE F-75 cautiously according to body weight (see F-75 feeding chart)
• Folic acid supplementation
• Iron-free Multivitamin supplementation
• Introduce F-100 feeds only when patient shows signs of transition
Signs of transition: good appetite (completes most of F-75 feeds), cheerful looking, smiles.
• Give Iron syrup (3mg/Kg/day) once patient is gaining weight (usually after transition onto F-100)
• Introduce stimulating play activities during the rehabilitation phase
• Weigh patient every other day.
• Prepare patient for discharge by counseling on appropriate home feeding using home-based food
• Discharge patient only when weight-for-height score is ≥ -1 SD (or Gain 15% of admission weight)
• Book patient for follow-up visit, and if possible arrange for home follow up
6.1.3 IMPORTANT THINGS NOT TO DO
• Do not give IV Fluid to treat dehydration unless patient is in shock
• Do not transfuse patient if PCV is > 12% (Hb > 4g/dl) unless s/he is in respiratory distress
• Never transfuse blood volume more than 10mls/Kg and never faster than 3 hours
• Never place patient close to opened window or under fan
• Never leave windows opened at night (caution- hypothermia)
• Never omit night feeds
• Never forget to chart all feeds, medications, and comments/remarks
• Never forget to fill in malnutrition data
NOTE: A check list of all the above activities should be completed for each patient and filed in patient’s
folder.
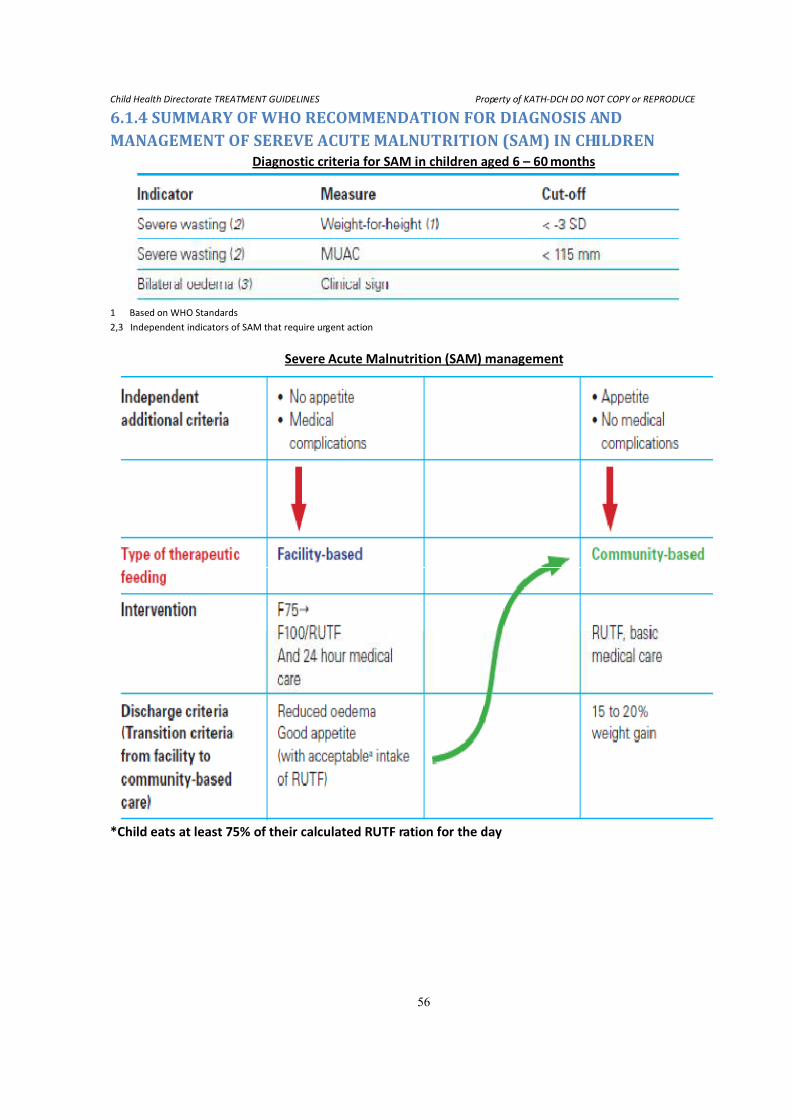
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
56
6.1.4 SUMMARY OF WHO RECOMMENDATION FOR DIAGNOSIS AND MANAGEMENT OF SEREVE ACUTE MALNUTRITION (SAM) IN CHILDREN
Diagnostic criteria for SAM in children aged 6 – 60 months
1 Based on WHO Standards
2,3 Independent indicators of SAM that require urgent action
Severe Acute Malnutrition (SAM) management
*Child eats at least 75% of their calculated RUTF ration for the day
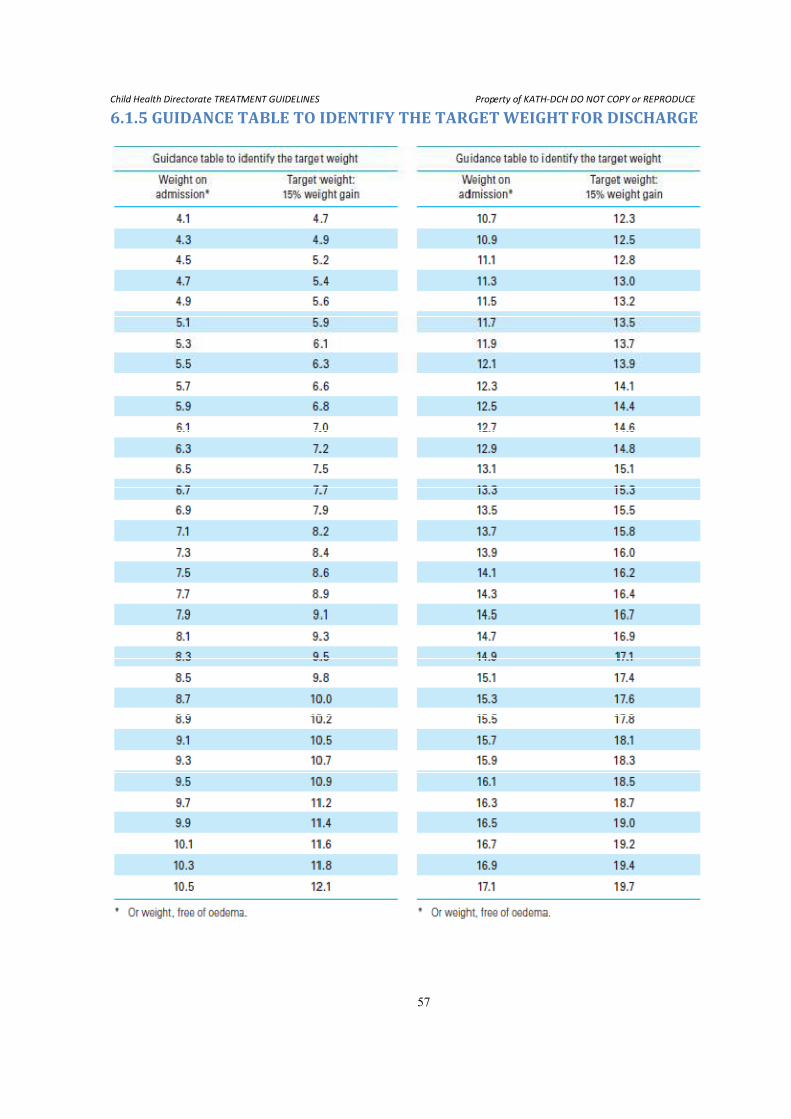
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
57
6.1.5 GUIDANCE TABLE TO IDENTIFY THE TARGET WEIGHT FOR DISCHARGE
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
58
7.0 NEONATAL DISORDERS
7.1.0 INTRODUCTION Birth asphyxia and neonatal seizures are among the most common problems encountered among neonates
in the Komfo Anokye Teaching Hospital.
Approximately 1 in 3 babies seen at the MBU may present with either condition or both.
7.1.1 NEONATAL RESUSCITATION
RISK FACTORS ASSOCIATED WITH THE NEED FOR RESUSCITATION Antepartum factors
o Diminished fetal activity o Maternal infection
o Age <16 or >35 years o Polyhydramnios
o No prenatal/antenatal care o Oligohydramnios
o Size-dates discrepancy o Previous fetal or neonatal death
o Post-term gestation o Anaemia or isoimmunisation
o Multiple gestation o Magnesium
o Pregnancy-induced hypertension o Maternal substance abuse
o Chronic hypertension o Fetal malformation
o Drug therapy: adrenergic blockers o Maternal diabetes
o Antepartum haemorrhage (APH) o Maternal cardiac, renal, pulmonary,
thyroid or neurologic disease
Intrapartum factors
o Fetal bradycardia / Fetal distress o Prolonged labour > 24 hours
o Emergency C/S o Prolapsed cord
o Forceps / Vacuum assisted delivery o Prolonged second stage of labour >2hours
o Breech or abnormal presentation o Non-reassuring heart rate patterns
o Use of general anaesthesia o Uterine tetany
o Premature labour o Meconium-stained amniotic fluid
o Precipitous labour o Chorioamnionitis
o Prolonged rupture of membranes ( > 18
hours before delivery)
o Narcotics administered to mother within 4
hours of delivery
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
59
A B C’s of RESUSCITATION
Airway – Position and clear – 30 seconds
� Place under the radiant heater
� Position by slightly extending the neck – ‘sniffing position’
� Place a rolled cloth/towel under the shoulders (if available)
� Suction mouth, then nose
Breathing - Stimulate to breath – 30 seconds
� Dry baby, change wet linen
� Reposition the head,
� Other ways to stimulate the baby are;
� Slapping or flicking the soles of the feet or
� Gently rub the back, trunk or extremities
� Give oxygen as necessary
� If not breathing, give positive pressure ventilation (PPV) with bag and mask (page 4,5)
� Oxygen saturation
Circulation – Assess heart rate and colour – 30 seconds
� Blue baby/cyanosis, give oxygen
� Acrocyanosis-( pink centrally but blue extremities), if breathing and SpO2 ≥ 88%, - No need
for oxygen
� HR <100bpm, give PPV
� HR <60bpm, give PPV and chest compressions (page 6,7)
� Oxygen saturation
Drugs - e.g. Adrenaline
� Cardiac stimulant
� Inotropic effect, increases the strength and rate of cardiac contractions
� Peripheral vasoconstriction, increasing blood flow to the heart and brain
Key point!
Evaluation is based primarily on the following three signs:
1. Respirations – increase in rate and depth after stimulation, good chest rise
2. Heart rate – should be > 100bpm
3. Colour – pink all over
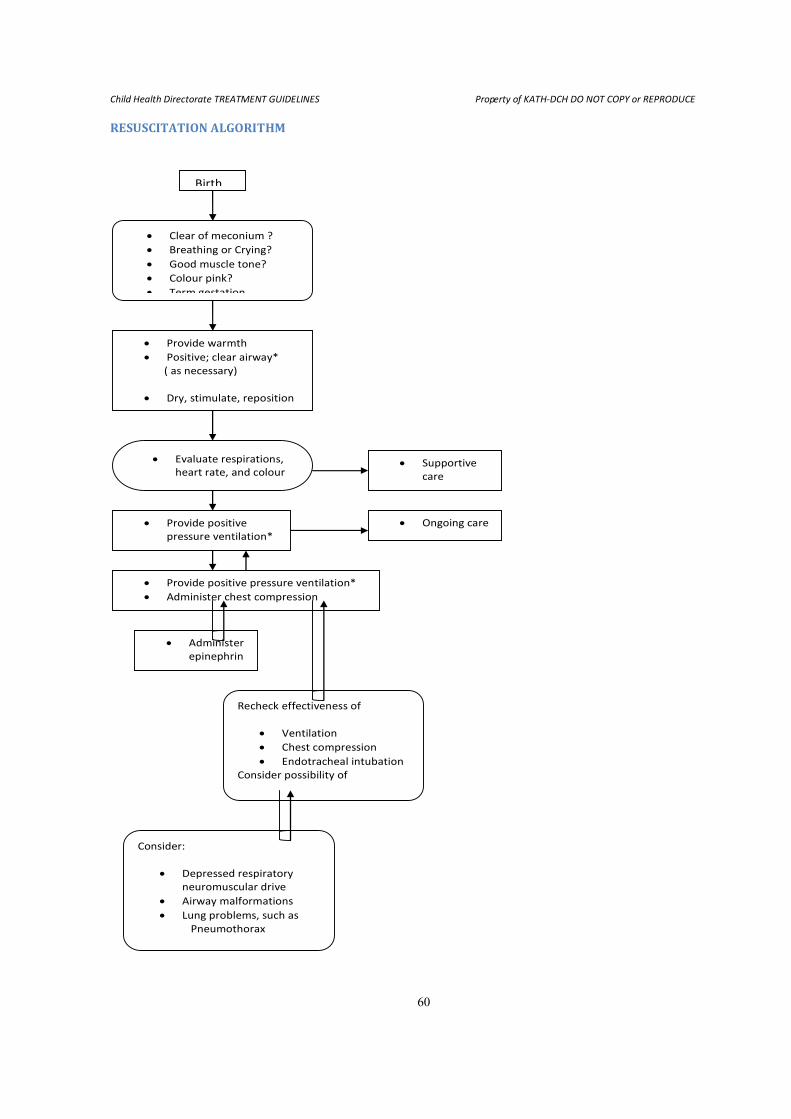
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
60
RESUSCITATION ALGORITHM
• Clear of meconium ?
• Breathing or Crying?
• Good muscle tone?
• Colour pink?
• Term gestation
• Provide warmth
• Positive; clear airway*
( as necessary)
• Dry, stimulate, reposition
• Give O2 (as necessary)
• Evaluate respirations,
heart rate, and colour
• Provide positive
pressure ventilation*
• Ongoing care
• Provide positive pressure ventilation*
• Administer chest compression
• Administer
epinephrin
e
Recheck effectiveness of
• Ventilation
• Chest compression
• Endotracheal intubation
Consider possibility of
Consider:
• Depressed respiratory
neuromuscular drive
• Airway malformations
• Lung problems, such as
Pneumothorax
• Supportive
care
Birth
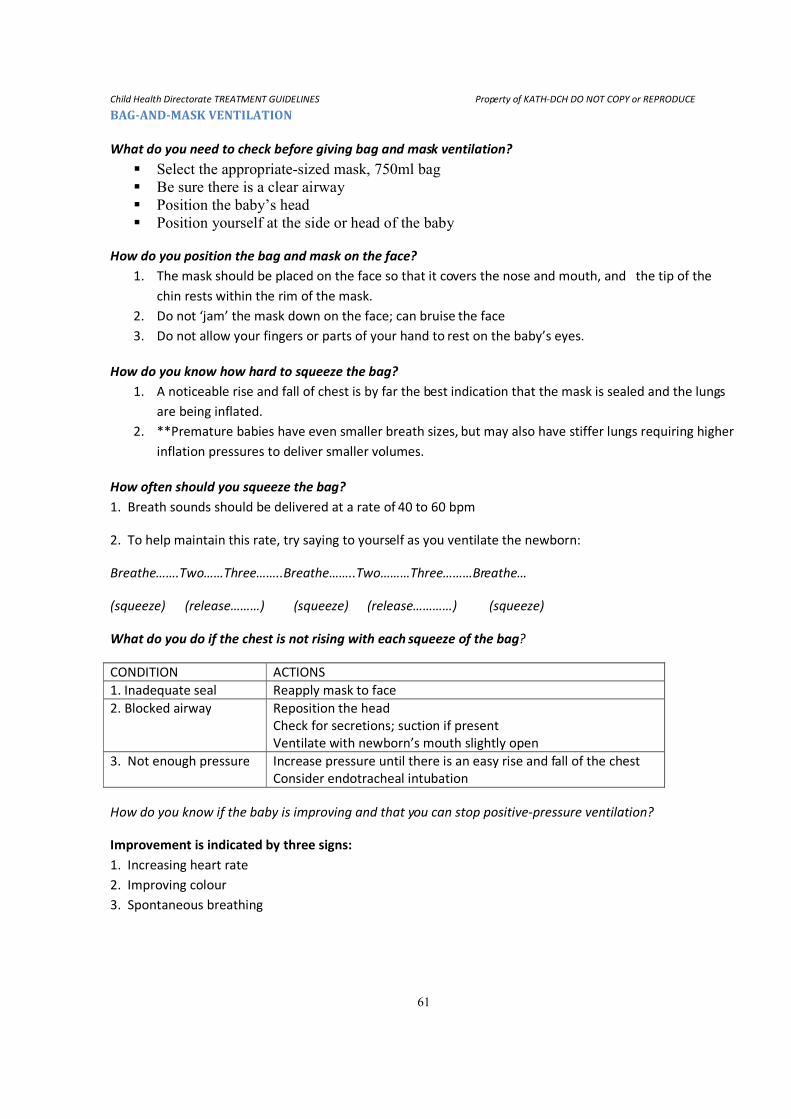
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
61
BAG-AND-MASK VENTILATION
What do you need to check before giving bag and mask ventilation?
� Select the appropriate-sized mask, 750ml bag
� Be sure there is a clear airway
� Position the baby’s head
� Position yourself at the side or head of the baby
How do you position the bag and mask on the face?
1. The mask should be placed on the face so that it covers the nose and mouth, and the tip of the
chin rests within the rim of the mask.
2. Do not ‘jam’ the mask down on the face; can bruise the face
3. Do not allow your fingers or parts of your hand to rest on the baby’s eyes.
How do you know how hard to squeeze the bag?
1. A noticeable rise and fall of chest is by far the best indication that the mask is sealed and the lungs
are being inflated.
2. **Premature babies have even smaller breath sizes, but may also have stiffer lungs requiring higher
inflation pressures to deliver smaller volumes.
How often should you squeeze the bag?
1. Breath sounds should be delivered at a rate of 40 to 60 bpm
2. To help maintain this rate, try saying to yourself as you ventilate the newborn:
Breathe…….Two……Three……..Breathe……..Two………Three………Breathe…
(squeeze) (release………) (squeeze) (release…………) (squeeze)
What do you do if the chest is not rising with each squeeze of the bag?
CONDITION ACTIONS
1. Inadequate seal Reapply mask to face
2. Blocked airway Reposition the head
Check for secretions; suction if present
Ventilate with newborn’s mouth slightly open
3. Not enough pressure Increase pressure until there is an easy rise and fall of the chest
Consider endotracheal intubation
How do you know if the baby is improving and that you can stop positive-pressure ventilation?
Improvement is indicated by three signs:
1. Increasing heart rate
2. Improving colour
3. Spontaneous breathing
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
62
Notes:
� Newborns requiring bag-and-mask ventilation for longer than several minutes, should have
an orogastric tube inserted, suction gastric contents, then leave it in place because:
� A stomach distended with gas puts pressure on the diaphragm, preventing full expansion of
the lungs.
� Gas in the stomach may cause regurgitation of gastric contents, which may then be aspirated
during bag-and-mask ventilation.
What do you do if the baby is not improving?
� Is chest movement adequate?
� Is the face-mask seal tight?
� Is the airway blocked because of improper head position or secretions in the nose, mouth, or
pharynx?
� Is the bag working properly?
� Is air in the stomach interfering with chest expansion?
� Is 100% oxygen being administered?
� Is the oxygen tubing attached to the bag and to the oxygen source?
� Is gas flowing through the flow meter?
� If you have checked all these factors and chest expansion is still not satisfactory, or you
don’t hear good breath sounds bilaterally, then insert an endotracheal tube at this time.
� Complications like pneumothorax may have occurred.
*NOTE*: Recent studies have suggested that babies can be successfully resuscitated with room air (21%
oxygen). However, the recommendation is for 100% oxygen when it is available.
CHEST COMPRESSIONS
What are chest compressions?
1. Sometimes referred to as external cardiac massage
2. Compress the heart against the spine
3. Increase the intrathoracic pressure
4. Circulate blood to the vital organs of the body
*NOTE*: The heart lies in the chest between the lower third of the sternum and the spine.
How do you position your hands on the chest to begin chest compressions?
1. Thumb technique
The two thumbs are used to depress the sternum, while the hands encircle the torso and the fingers
support the spine.
2. Two-finger technique
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
63
The tips of the middle finger and either the index finger or ring finger of one hand are used to compress the
sternum.
The other hand is used to support the baby’s back, unless the baby is on a very firm surface.
Where on the chest do you position your thumbs and fingers?
The lower third of the sternum, which lies between the xyphoid and a line drawn between the nipples.
When compressing the chest, only the two fingertips should rest on the chest.
With the thumb technique, you should apply pressure vertically to compress the heart.
How much pressure should you use to compress the chest?
Depress the sternum to a depth of approximately one-third of the anterior-posterior diameter of the chest,
then release the pressure to allow the heart to refill.
Do not lift your thumbs or fingers off the chest between compressions.
Provide enough pressure for compressions without damaging underlying organs.
How often do you compress the chest and coordinate with ventilation?
1. Three compressions to One ventilation
‘One-…and-…Two-…and- …Three-…and-…Breathe-…and-…One-…and-…’
2. It should come to at least 30 breaths and 90 compressions per minute.
When do you stop chest compressions?
If the heart rate >60bpm, then discontinue chest compressions but continue positive-pressure ventilation,
at a rate of 40 to 60bpm.
What do you do if the baby is not improving?
You should continue to ask yourself the following questions-
� Is chest movement adequate? (Have you considered or performed endotracheal intubation)
� Is 100% oxygen being given?
� Is the depth of chest compression approximately one-third of the diameter of the chest?
� Are the chest compressions and ventilation being well coordinated?
If the heart rate remains <60bpm, then give Adrenaline – medications; page
ENDOTRACHEAL INTUBATION
When is endotracheal intubation required?
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
64
If there is meconium and the baby is not vigorous – depressed respirations, muscle tone, or heart rate, you
will need to intubate the trachea as the very first step, before any other resuscitation measures are started.
If positive-pressure ventilation by bag and mask is not resulting in good chest rise
If the need for positive-pressure ventilation lasts beyond a few minutes, you may decide to intubate simply
to improve the efficacy and ease of assisted ventilation.
If chest compressions are necessary, intubating may facilitate coordination of chest compressions and
ventilation
Can be used as a route to administer Adrenaline
How do you prepare the endotracheal tube for use?
Select the appropriate-sized tube.
Tube Size (mm) Weight Gestational Age
(inside diameter) (g) (wks)
2.5 Below 1,000 Below 28
3.0 1,000 – 2,000 28 – 34
3.5 2,000 – 3,000 34 – 38
3.5 – 4.0 Above 3,000 Above 38
Ideal tube length 13 – 15cm
How do you prepare the laryngoscope and additional supplies?
� Select blade and attach to handle
� No. 0 for preterm newborns
� No. 1 for term newborns
� Check light
� Prepare suction equipment
� Prepare resuscitation bag and mask
� Turn on oxygen
� Get stethoscope
� Cut tape or prepare stabilizer
How should you position the newborn to make intubation easiest?
Use the same position as for bag-and-mask ventilation i.e. the “sniffing” position
How do you hold the laryngoscope?
• First turn on the laryngoscope light
• Hold the laryngoscope in your left hand, between your thumb and first two or three fingers,
with the blade pointing away from you.
How do you visualize the glottis and insert the tube?
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
65
1. Stabilize the babies head with your right hand – sniffing position.
( Free-flow oxygen should be delivered throughout the procedure )
2. Slide the laryngoscope blade over the right side of the tongue, pushing the tongue to the left
side of the mouth
3. Advance the blade until the tip lies in the vallecula, just beyond the base of the tongue. You
may need to use your right index finger to open the babies mouth.
4. Lift the blade slightly, thus lifting the tongue out of the way to expose the pharyngeal area.
5. Do not elevate the tip of the blade by using a rocking motion and pulling the handle toward
you.
6. Look for landmarks: the epiglottis at the top, the glottic opening below, and the vocal cords
appearing as vertical stripes on each side of the glottis or as an inverted letter “V”
7. Insert the tube with your right hand
8. The vocal cord guide – the black marking close to the end of the tube, should be at the level
of the cords. * If the cords are together wait for them to open*
9. Stabilize the tube with one hand, and remove the laryngoscope with the other.
How do you check to be sure that the tube is in the trachea?
• If the tube is positioned correctly, you should observe:
• A rise in the chest with each breath
• Breath sounds over both lung fields, but decreased or absent over the stomach
• No gastric distension with ventilation
• Vapour condensing on the inside of the tube during exhalation
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
66
7.2.0 BIRTH ASPHYXIA Clinical Definition/Criteria:
Age:
• By definition, this disease is seen in the newborn period.
• Most neonates are term at birth.
• In most cases, the disease manifests at birth or within a few hours after birth.
History:
• Persistence of an Apgar score of 0-3 for longer than 5 minutes
• Neonatal neurologic sequelae (eg, seizures, coma, hypotonia)
• Multiple organ involvement (eg, of the kidney, lungs, liver, heart, intestines)
• Maternal History – e.g. Prolonged labour, C/S , Meconium stained liquor,etc
• Profound metabolic or mixed acidemia (pH <7.00) in an umbilical artery blood sample, if
obtained
Physical examination:
Clinical manifestations and course vary depending on Hypoxic Ischaemic Encephalopathy (HIE)
severity.
Mild HIE / Aspyhxia
• Hyperalert :- appearance of hunger, yet not feeding well; together with a wide-eyed gaze, but
failure to fixate.
• Irritability, or excessive crying or sleepiness, may be observed.
• By 3-4 days of life, the CNS examination findings become normal.
Moderate HIE / Asphyxia
• The infant is lethargic, with significant hypotonia and diminished deep tendon reflexes.
• Seizures may occur within the first 24 hours of life.
• Full recovery within 1-2 weeks is possible and is associated with a better long-term outcome.
• An initial period of well-being may be followed by sudden deterioration, suggesting reperfusion
injury; during this period, seizure intensity might increase.
Severe HIE / Asphyxia
• Stupor or coma is typical. The infant may not respond to any physical stimulus.
• Breathing may be irregular, and the infant often requires ventilatory support.
• Generalized hypotonia and depressed deep tendon reflexes are common.
• Seizures occur early and often and may be initially resistant to conventional treatments.
• The seizures are usually generalized, and their frequency may increase during the 2-3 days after
onset, correlating with the phase of reperfusion injury.
• The fontanelle may bulge, suggesting increasing cerebral edema.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
67
Infants who survive severe HIE
• The level of alertness improves by days 4-5 of life.
• Hypotonia and feeding difficulties persist, requiring tube feeding for weeks to months
Lab investigations:
• No specific test excludes or confirms a diagnosis of HIE.
• The diagnosis is based on the history and physical examination.
• Choice of tests depends on the evolution of symptoms.
• As with any other disease, test results should be interpreted in conjunction with clinical history and
the findings of physical examination.
Management of Birth Asphyxia:
• Effective Resuscitation
• General supportive care
o Keep warm:- under the radiant heater or in the incubator
o Oxygen:- if blue or Oxygen saturation < 88%
o Correct hypoglycaemia (i.e. RBS ≤ 2.2mmol/L ) by giving 5ml/kg body weight of 10% Dextrose
IV, continued with maintenance IV 10% Dextrose
o Feeding / Fluid Therapy - depending on gestational age, weight, and severity of asphyxia
Mild HIE/Asphyxia:
- Can start with NG tube or Cup feeds (e.g. EBM), based on weight for the 1st
24hours, then
continue with breastfeeding as soon as baby is able to suck.
Moderate and Severe Asphyxia/HIE:
- In the first 2-3days of life, restrict intravenous fluids to two thirds of the daily requirement
for gestational age/weight.
- Restrict to nothing by mouth (NPO) during the first 3days of life or until the general level of
alertness and consciousness improves.
- When infants begin to improve, urinary output increases, and fluid administration must be
adjusted to daily maintenance.
- If there are no seizures, the baby can then be started on NG tube feeds 2-3hrly, and if
tolerating feeds well, can later be put on cup feeds – EBM depending on the weight.
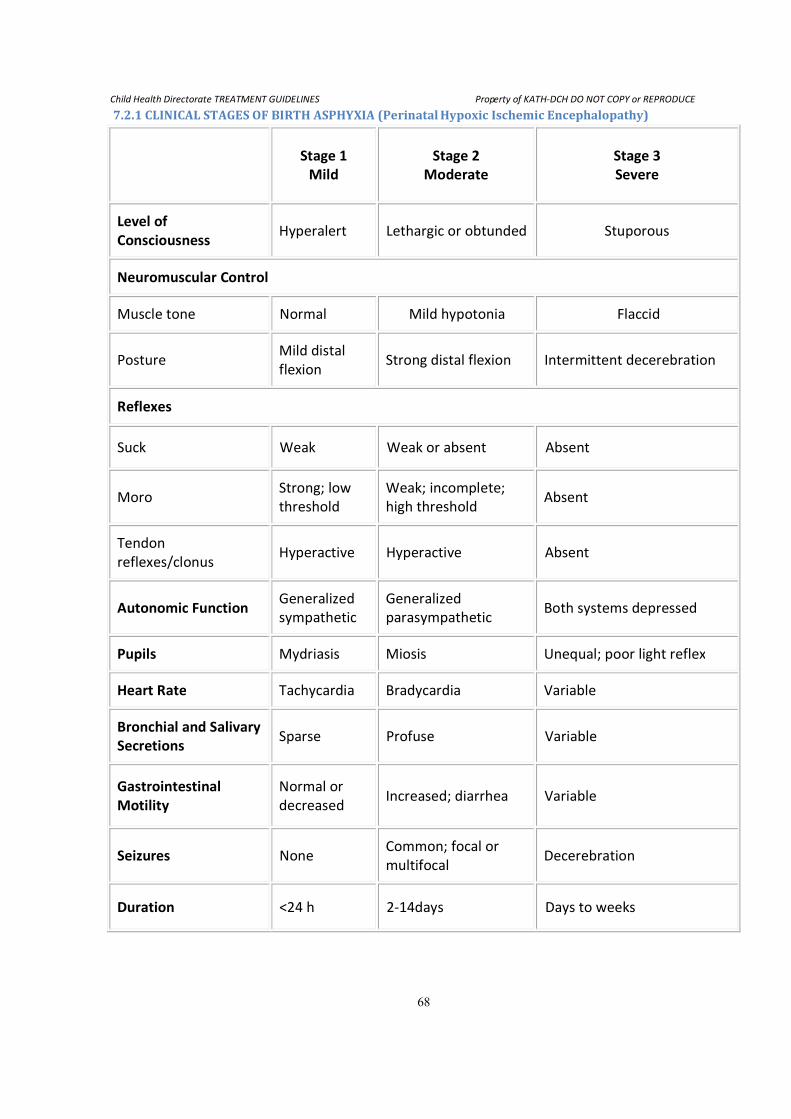
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
68
7.2.1 CLINICAL STAGES OF BIRTH ASPHYXIA (Perinatal Hypoxic Ischemic Encephalopathy)
Stage 1
Mild
Stage 2
Moderate
Stage 3
Severe
Level of
Consciousness Hyperalert Lethargic or obtunded Stuporous
Neuromuscular Control
Muscle tone Normal Mild hypotonia Flaccid
Posture Mild distal
flexion Strong distal flexion Intermittent decerebration
Reflexes
Suck Weak Weak or absent Absent
Moro Strong; low
threshold
Weak; incomplete;
high threshold Absent
Tendon
reflexes/clonus Hyperactive Hyperactive Absent
Autonomic Function Generalized
sympathetic
Generalized
parasympathetic Both systems depressed
Pupils Mydriasis Miosis Unequal; poor light reflex
Heart Rate Tachycardia Bradycardia Variable
Bronchial and Salivary
Secretions Sparse Profuse Variable
Gastrointestinal
Motility
Normal or
decreased Increased; diarrhea Variable
Seizures None Common; focal or
multifocal Decerebration
Duration <24 h 2-14days Days to weeks
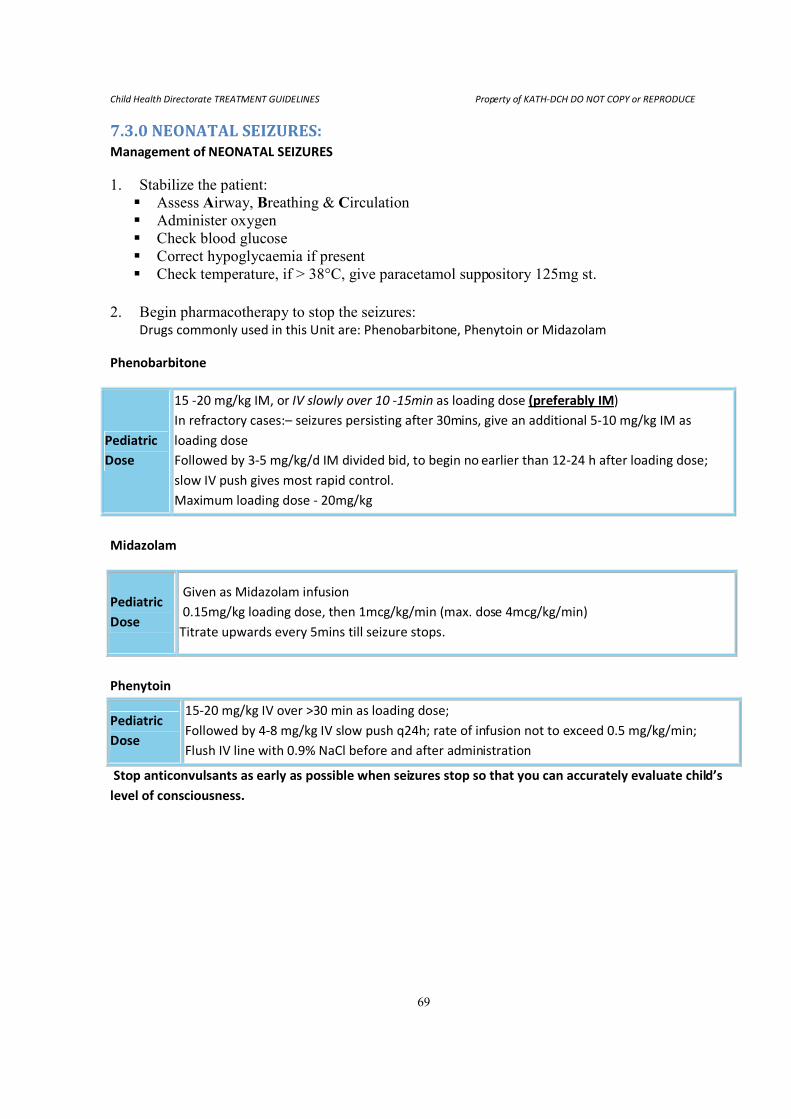
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
69
7.3.0 NEONATAL SEIZURES: Management of NEONATAL SEIZURES
1. Stabilize the patient:
� Assess Airway, Breathing & Circulation
� Administer oxygen
� Check blood glucose
� Correct hypoglycaemia if present
� Check temperature, if > 38°C, give paracetamol suppository 125mg st.
2. Begin pharmacotherapy to stop the seizures: Drugs commonly used in this Unit are: Phenobarbitone, Phenytoin or Midazolam
Phenobarbitone
Midazolam
Pediatric
Dose
Given as Midazolam infusion
0.15mg/kg loading dose, then 1mcg/kg/min (max. dose 4mcg/kg/min)
Titrate upwards every 5mins till seizure stops.
Phenytoin
Stop anticonvulsants as early as possible when seizures stop so that you can accurately evaluate child’s
level of consciousness.
Pediatric
Dose
15 -20 mg/kg IM, or IV slowly over 10 -15min as loading dose (preferably IM)
In refractory cases:– seizures persisting after 30mins, give an additional 5-10 mg/kg IM as
loading dose
Followed by 3-5 mg/kg/d IM divided bid, to begin no earlier than 12-24 h after loading dose;
slow IV push gives most rapid control.
Maximum loading dose - 20mg/kg
Pediatric
Dose
15-20 mg/kg IV over >30 min as loading dose;
Followed by 4-8 mg/kg IV slow push q24h; rate of infusion not to exceed 0.5 mg/kg/min;
Flush IV line with 0.9% NaCl before and after administration
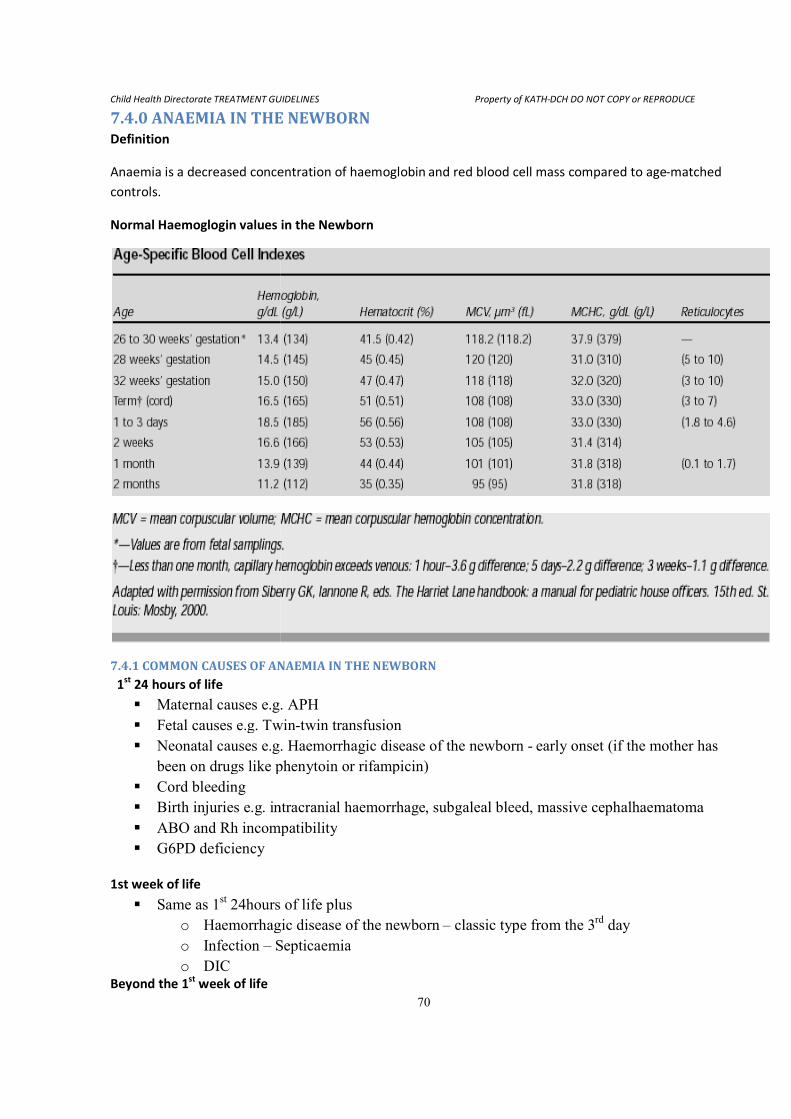
Child Health Directorate TREATMENT GUIDELINES
7.4.0 ANAEMIA IN THE NEWBORNDefinition
Anaemia is a decreased concentration of haemoglobin and red blood cell mass compared to age
controls.
Normal Haemoglogin values in the Newborn
7.4.1 COMMON CAUSES OF ANAEMIA IN THE NEWBORN
1st
24 hours of life
� Maternal causes e.g. APH
� Fetal causes e.g. Twin
� Neonatal causes e.g.
been on drugs like phenytoin or rifampicin)
� Cord bleeding
� Birth injuries e.g. intracranial haemorrhage
� ABO and Rh incompatibility
� G6PD deficiency
1st week of life
� Same as 1st 24hours of life plus
o Haemorrhagic disease of the newborn
o Infection – Septicaemia
o DIC Beyond the 1
st week of life
TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
70
ANAEMIA IN THE NEWBORN
Anaemia is a decreased concentration of haemoglobin and red blood cell mass compared to age
Normal Haemoglogin values in the Newborn
ANAEMIA IN THE NEWBORN
g. APH
g. Twin-twin transfusion
g. Haemorrhagic disease of the newborn - early onset (if the mother has
been on drugs like phenytoin or rifampicin)
ntracranial haemorrhage, subgaleal bleed, massive cephalhaematoma
ABO and Rh incompatibility
24hours of life plus
Haemorrhagic disease of the newborn – classic type from the 3
Septicaemia
DCH DO NOT COPY or REPRODUCE
Anaemia is a decreased concentration of haemoglobin and red blood cell mass compared to age-matched
early onset (if the mother has
, subgaleal bleed, massive cephalhaematoma
classic type from the 3rd
day
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
71
� Haemorrhagic disease of the newborn – late onset, usually due to liver disease
� G6PD deficiency
� Infection eg malaria usually after 4weeks of life, and septicaemia
7.4.2 CLINICAL FEATURES OF ANAEMIA IN THE NEWBORN Key questions in the history:
Ask about:
� Maternal history of bleeding
� History of bleeding in other siblings
� Home delivery – Vit K not given
� Vacuum extraction done or failed vacuum
� Neonatal jaundice in other siblings
� Herbal medication given – G6PD deficiency
� Presence of fever, etc
Symptoms
� Poor feeding
� Difficulty in breathing/tachypnoea
� Vomiting
� Irritability
� Lethargy
� Failure to gain weight
Signs
� Pallor
� Weak pulses
� Cold extremities
� Decreased capillary refill time
� Hypotension
� Tachypnoea
� Tachycardia
� Apnoea
� Obvious bleeding eg. From the cord, mouth, nostrils etc
� Abdominal distension from intra-abdominal bleeding
� Increasing head size, pitting oedema on the forehead and behind the ears - subgaleal bleed
� Jaundice
� Hepatosplenomegaly
� Fever
Investigations
� Urgent PCV
� Complete blood count, film comment,
� Malaria parasites – age > 1month
� Reticulocyte count
� Blood grouping and cross-matching
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
72
If jaundice is present include:-
� Grouping and cross-matching against the mother’s blood, Rhesus factor
� Direct antibody test (Coombs)
� Serum bilirubin - SBR
� G6PD screen
� Blood C/S
7.4.3 MANAGEMENT
� FIRST STOP BLEEDING*
o If in shock from blood loss, give 10ml/kg of Normal Saline over 30mins while
arranging for blood, and monitor RR, HR, CRT, peripheries, and passage of urine. If
Normal Saline is not available give Ringers Lactate.
Transfusion guidelines:
WHAT TO GIVE
- Whole blood (Fresh if possible ) or Packed RBC’s – 20ml/kg/day – given over 4hours.
- Whole blood should be given for anaemia due to blood loss, and packed cells for haemolysis.
- In acute haemorrhage, a bolus of whole blood 5ml/kg can be given over 30mins.
- Give I.V. lasix 1mg/kg st, if cause of anaemia is not due to blood loss.
WHEN TO TRANSFUSE
- Do not transfuse for phlebotomy losses alone.
- Do not transfuse for hematocrit alone, unless the hematocrit level is less than 40% in the 1st
24hrs
of life, and 30% within the 1st
week of life.
- Transfuse for shock associated with acute blood loss.
- Transfuse (beyond the 1st
week of life) for hematocrit levels less than 35% in the following
situations:
Infant with severe pulmonary disease; CHECK oxygen saturation
Infant in whom anemia may be contributing to congestive heart failure
In the following situations, (beyond the 1st week of life) transfuse for a hematocrit level that is 25-30% or
less if:
The patient has significant apnoea and bradycardia
The patient has persistent tachycardia or tachypnoea without other explanation for 24 hours.
Weight gain of patient is deemed unacceptable without other explanation such as known increases
in metabolic demands or known losses in metabolic demands (malabsorption).
The patient is scheduled for surgery; transfuse in consultation with the surgery team.
Iron therapy
Anaemia (refer to drug dosages) without symptoms, clinically stable, give 3-5mg/kg/day. Monitor Hb/PCV
levels
All preterms are to be given iron on discharge – mothers should be counseled to start administering iron at
6 weeks/40days
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
73
- Discuss with Resident/Specialist
Indications for Antimalarials:
� If malaria parasite is present
� After blood transfusion/exchange transfusion
� Baby >4wks with fever and anaemia
Antibiotics: where indicated
IM/IV Vitamin K 1-2mg/kg st, then, 1mg/kg after 24hrs if still bleeding. Max. 10mg/day
NOTE: Discuss with Resident/Specialist before any transfusion
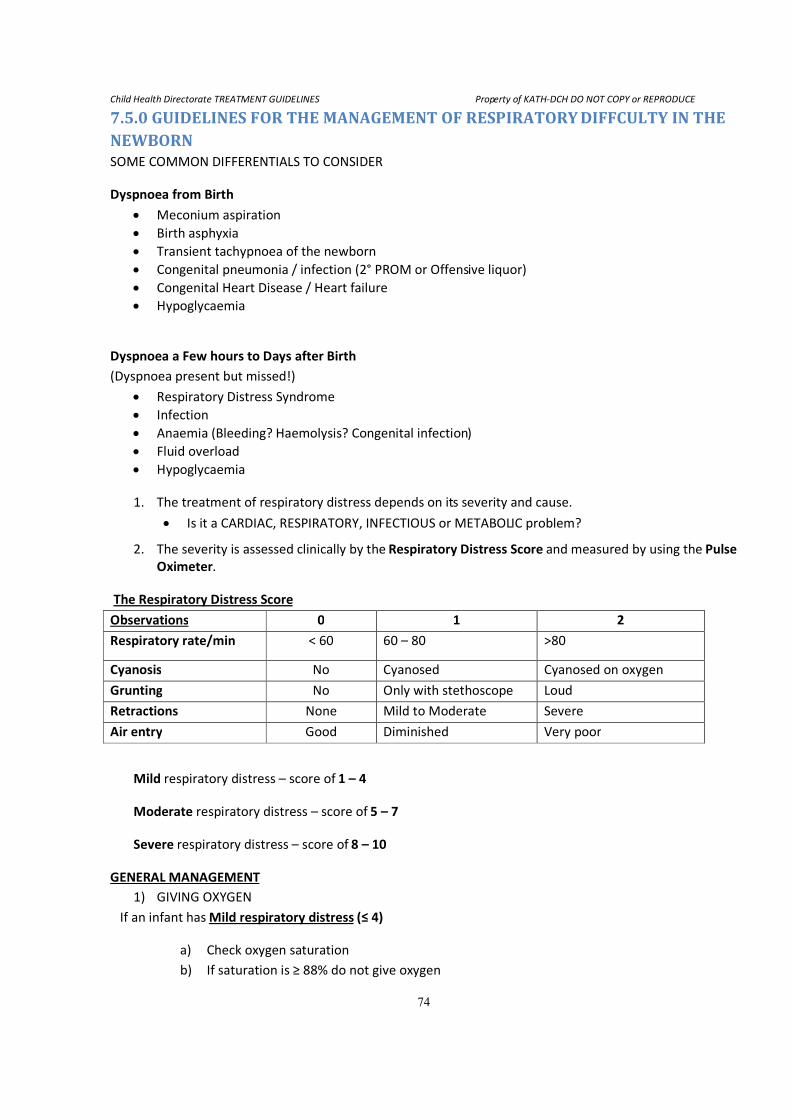
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
74
7.5.0 GUIDELINES FOR THE MANAGEMENT OF RESPIRATORY DIFFCULTY IN THE NEWBORN SOME COMMON DIFFERENTIALS TO CONSIDER
Dyspnoea from Birth
• Meconium aspiration
• Birth asphyxia
• Transient tachypnoea of the newborn
• Congenital pneumonia / infection (2° PROM or Offensive liquor)
• Congenital Heart Disease / Heart failure
• Hypoglycaemia
Dyspnoea a Few hours to Days after Birth
(Dyspnoea present but missed!)
• Respiratory Distress Syndrome
• Infection
• Anaemia (Bleeding? Haemolysis? Congenital infection)
• Fluid overload
• Hypoglycaemia
1. The treatment of respiratory distress depends on its severity and cause.
• Is it a CARDIAC, RESPIRATORY, INFECTIOUS or METABOLIC problem?
2. The severity is assessed clinically by the Respiratory Distress Score and measured by using the Pulse
Oximeter.
The Respiratory Distress Score
Observations 0 1 2
Respiratory rate/min < 60 60 – 80 >80
Cyanosis No Cyanosed Cyanosed on oxygen
Grunting No Only with stethoscope Loud
Retractions None Mild to Moderate Severe
Air entry Good Diminished Very poor
Mild respiratory distress – score of 1 – 4
Moderate respiratory distress – score of 5 – 7
Severe respiratory distress – score of 8 – 10
GENERAL MANAGEMENT
1) GIVING OXYGEN
If an infant has Mild respiratory distress (≤ 4)
a) Check oxygen saturation
b) If saturation is ≥ 88% do not give oxygen
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
75
c) If saturation is < 88%, or pulse oximetry is not available, give oxygen by nasal catheter with
a flow of 0.5 to 1L/min
If an infant is cyanosed or has moderate to
Severe respiratory distress (> 4)
a) Check the oxygen saturation
b) Increase oxygen flow till the saturation is ≥ 88%
c) Use the oxihood or oxygen face mask, if you have to give an oxygen flow of >2L/min
d) If there is no oxihood or face mask, use double nasal catheters
If apnoeic or RR ≤ 20/min, resuscitate with bag and mask, and if HR <60bpm perform chest
compressions.
2) CORRECT HYPOGLYCAEMIA and SHOCK
3) GIVE ANTIBIOTICS
4) FEEDING/IV FLUIDS
a) Amount will depend on the baby’s weight and age
b) In severe respiratory distress, give IV fluids cautiously (Rule out heart failure!!!)
c) In mild to moderate respiratory distress, give tube feeds (EBM)
d) In mild respiratory distress, mother can breastfeed if there is NO grunting, indrawing or
cyanosis.
e) Feeding tube should be inserted through the mouth rather than the nose
f) Give slow, small and frequent feeds to prevent reflux, distension and aspiration
g) Encourage mother to breastfeed as soon the baby is stable.
5) MONITOR and CHART – Respiratory Distress Score, Oxygen Saturation and Capillary Refill Time hourly
and Blood Sugar 3hourly.
7.6.0 FEEDING PROTOCOL FOR BABIES ADMITTED TO THE MOTHER BABY UNIT, THE IDEAL WHICH WE AIM FOR IS EXCLUSVE BREASTFEEDING FOR EVERY BABY ON THE UNIT. EVERY EFFORT
MUST BE MADE BY ALL STAFF OF THE UNIT TO ACHIEVE THIS, WHERE POSSIBLE.
GENERAL PRINCIPLES TO BE FOLLOWED
1. Artificial feeds are to be handled like drugs. They should only be given when prescribed by the
doctor on duty or with permission from the Nurse in charge. They should only be given for medical
reasons.(see below)
2. A baby who has started breast feeding should never be given artificial feeds until after the mother
has been to feed, if necessary.
3. A baby who is on a functioning IV line with glucose in it should never be given artificial feeds as
there is no immediate risk of hypoglycaemia.
4. Every effort should be made to call mothers OR to take the baby to mother to breastfeed rather
than giving the baby artificial feeds only because the mother is late in coming.
5. Artificial feeds should never be given to babies with birth asphyxia unless there is no functioning IV
line, to reduce the risk of necrotizing enterocolitis.
6. Ward doctors must, as part of daily ward rounds, review the baby’s feeding chart and as much as
possible find out from the mother independently, how feeding is going, in order to make the
necessary changes in the baby’s feeding schedule.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
76
7. It is the duty of all health care staff on the unit to identify mothers with breast feeding problems
and help them to overcome them.
8. In order not to send wrong messages, artificial feeds must not be prepared in full view of the
mothers. All talks to mothers must enforce exclusive breast feeding and where mothers are being
counseled about artificial feeding, this must be done with as much discretion as possible.
EXAMPLES OF COMMON AND ACCEPTABLE MEDICAL REASONS FOR GIVING A BABY ARTIFICIAL FEEDS
1. A baby with a high risk of hypoglycaemia (e.g. a premature baby, a baby of a diabetic mother or a
very growth retarded baby) in whom there is no functioning IV line and in whom the mother is
either not available or in whom it is judged that there is insufficient breast milk to prevent
hypoglycaemia from occurring.
NB A healthy term or near term baby is not at risk of developing hypoglycaemia just because
feeding is delayed for an hour or so – HUNGER is not the same as hypoglycaemia.
2. The baby of an HIV positive mother (or any other mother!) who has made an informed choice not to
breast feed. This information must be adequately communicated to the ward staff. (In the case of
the HIV Positive mother, artificial feeds should never be started until the mother’s decision on
feeding is known. This to avoid mixing of breast feeding and artificial feed which is believed to carry
a high risk of transmitting HIV to the baby.)
3. Where the mother is dead, or where the mother has abandoned the baby or has a psychiatric
disorder where it is considered that the baby is at risk of being harmed by the mother.
SOME COMMON, NON MEDICAL AND UNACCEPTABLE REASONS FOR GIVING ARTIFICIAL FEEDS e.g.
1. The mother hasn’t come. (Send for her!)
2. The baby is too big.
3. The stomach “looks flat”
4. The baby is crying after being fed.
5. The baby “looks hungry”.
In all these cases the solution is to give more breast milk and only if this fails should artificial feeds be
considered.
SOME SITUATIONS WHERE ORAL FEEDS SHOULD USUALLY BE WITHHELD
1. Moderate and severe birth asphyxia, (to reduce the risk of Necrotising Enterocolitis).
2. Any neonate who is very ill immediately after birth, or a preterm baby less than 30 weeks. In both
these cases however breast feeding should start as soon as the baby is stable.
3. In suspected intestinal obstruction.
4. In any baby who is going for General Anaesthesia who has been made nil per os.
5. The baby of an HIV positive mother whose feeding choice is not yet known by the ward staff.
6. A baby who on a previous feed has not tolerated oral feeding. (E.g. turned blue or had an apnoeic
attack.)
7. Any neonate with a Respiratory rate >80 breaths per minute or has other signs of severe respiratory
distress.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
77
8. A baby who is about to have an exchange blood transfusion. (A baby whose bilirubin is being
monitored in whom a decision concerning exchange transfusion has not been taken should be fed.
However feeds should be stopped as soon as the decision to do the procedure is made).
9. A baby who has an umbilical vein catheter should not be fed until the catheter has been removed.
VOLUMES OF FEED TO GIVE
- DAY 1 (i.e. the 1st
24 hour period) - 60ML PER KG PER DAY
- DAY 2 (i.e. the 2nd
24 hour period) - 90ML PER KG PER DAY
- DAY 3 (i.e. the 3rd
24 hour period) - 120 ML PER KG PER DAY
- DAY 4 (i.e. the 4th
24 hour period) - 150 ML PER KG PER DAY
- DAY 5 AND BEYOND:
o For TERM babies, give 150 ML PER KG PER DAY, unless otherwise prescribed.
o For PRETERM AND LOW BIRTH WEIGHT BABIES, GIVE 180 MLS PER KG PER DAY OR MORE IF
THEY WILL TOLERATE IT
� For very small babies, feeds can be given two hourly or even hourly if they cannot tolerate larger
volumes three hourly.
� Where the baby cannot suck, feeds should be given by NG tube or cup depending on the gestational age
and condition of the baby.
� All babies must have a feeding chart which is filled daily.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
78
7.7.0 GUIDELINES FOR THE MANAGEMENT OF NEONATAL JAUNDICE Neonatal jaundice is a common condition which doctors are often called upon to manage. Decisions as to
which management option to choose are based on what YOU consider to be the baby’s risk of developing
kernicterus. This can sometimes be confusing. Below are some guidelines to help you decide how to
manage the baby. In some cases, the decision is straight forward and easy to take. In others, it is not so
simple. Always be prepared to consult when you are not sure what to do.
FIRST DECIDE WHETHER THE JAUNDICED BABY HAS ANY SIGNS OF KERNICTERUS.
Some of the things to look for include the following :
• Does he have poor feeding? - Remember to ask whether the baby is feeding AS WELL AS he was the
day before?
• Has he become irritable? – is he crying more than usual? Is he sleeping poorly? Is he taking longer
than usual to attach to the breast because of fussing or crying?
• Has he become lethargic? – Is he sleeping more than usual or feeding poorly? Does he have little
movement?
• Are there seizures? Are there any abnormal looking movements?
IF THE ANSWER TO ANY OF THESE IS YES, THE BABY MAY BE DEVELOPING KERNICTERUS.
PREPARE HIM FOR AN EXCHANGE TRANSFUSION. (AFTER PERFORMING ALL EMERGENCY PROCEDURES
SUCH AS CORRECTING HYPOGLYCAEMIA, ETC.)
7.7.1 PREPARATION FOR AN EXCHANGE BLOOD TRANSFUSION.
1. While taking blood for culture, G6PD etc, take a specimen from the baby and one from the mother
also for grouping and cross matching. In filling the request form, make sure the lab knows the
request is for an exchange and not a simple transfusion so that you get the right group of blood.
Request for 160mls/kg of blood
2. Set an IV line to rehydrate the baby and treat/prevent hypoglycaemia. Keep the baby nil per os until
after the exchange. If you are conversant with passing an umbilical vein catheter you may go ahead
and do so.
3. Put the baby under phototherapy.
4. Discuss the decision with a senior colleague if ANY doubt exists.
If the answer to all the above questions is no (i.e. you assess the baby as having no signs of kernicterus,)
decide whether there is a risk of this baby developing kernicterus.
Some factors that will put a baby at risk of developing kernicterus include the following:
1. Serum bilirubin of 400µ/1 in a term baby, or 10 x the gestational age in a preterm baby.
2. A previous history of a jaundiced baby who was hospitalized or severely affected (or even
unexplained neonatal deaths, as the mother may not have observed the jaundice.)
3. Jaundice noticed before the baby was 48 hrs old
4. Age less than 72 hours.
5. Child deeply jaundiced, especially if this involves the whole body including the feet.
6. Prematurity
7. Co-existing illness such as birth asphyxia or injury sepsis, meningitis etc.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
79
IF THE CHILD HAS ANY OF THESE HE MAY BE AT RISK OF DEVELOPING KERNICTERUS. PREPARE AS IF YOU
ARE GOING TO EXCHANGE HIM AND DISCUSS WITH A SENIOR COLLEAGUE.
If you decide that there is no sign of kernicterus and there is no risk of the baby developing kernicterus, take
all necessary samples to the lab. Usually this will include a blood culture, a full blood count and blood film
for malaria parasites. Always check for G6PD deficiency.
Put the baby under phototherapy and give IV fluids if necessary. Give all other treatments as necessary.
Though many babies admitted for jaundice will need sepsis treatment, this should NOT be a routine.
7.7.2 PERFORMING THE EXCHANGE BLOOD TRANSFUSION (EBT)
You should have observed at least one exchange blood transfusion and should have been supervised to do
at least one, before attempting to do one on your own. You should therefore be familiar with the basic set
of the procedure. Below however are a few points to note.
1. Remember that rehydration and phototherapy may have reduced the bilirubin to a level where EBT
is no longer indicated, especially in borderline cases. As much as possible, especially where the SBR
was not checked in the last hour, recheck before starting.
2. An EBT is a hazardous procedure. Every effort should be made to maintain cleanliness and sterility,
especially when passing the UVC. Once passed, the UVC should be secured to prevent the need for
re- passage and its attendant increased risk of infection and thromboembolism.
3. The baby must be kept warm and carefully monitored during the procedure. If the heart rate or
respiratory rates become deranged, slow down and allow the baby to recover.
4. Aim to do the procedure over two hours to allow the bilirubin in the tissue to equilibrate with that
in the blood.
5. Remember to keep mixing the blood in the bag to prevent anaemia at the end of the exchange. This
is especially important as the adult blood used for the exchange will usually have an Hb well below
the expected value for a baby.
6. At the end of the exchange
a. Remove the UVC slowly.
b. Cover the cord with sterile gauze.
c. Give the baby Vitamin K (treatment dose), and anti malarial and antibiotics if indicated
d. Check the Serum Bilirubin to provide a baseline for subsequent monitoring.
e. Maintain IV dextrose, keep the baby nil per os and continue to monitor until at least two
hour after the exchange.
f. Where the baby is very young (usually < about 4 days), the bilirubin may rise such that
another exchange is needed. Always check again within 6 hours of completing the
procedure. Conversely, there is rarely the need to go on monitoring bilirubin once the
baby is 7 complete days old.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
80
7.8.0 GUIDELINES TO THE MANAGEMENT OF THE HIV EXPOSED BABY Diagnosis
The Delivery Head Ticket may have the number 279 written on it, indicating that the mother has the
infection.
Antiretroviral (ARV) prophylaxis
1. Give a single dose of Nevirapine susp. 2mg/kg within 48hrs of delivery PLUS one week course of
a. Syr Zidovudine 4mg/kg bd
PLUS
Syr Lamivudine 2mg/kg bd
BUT
2. If the mother has had less than 4 weeks of ARV prophylaxis, then
a. Give the baby a 6 week course of Zidovudine and Lamivudine.
3. Collect the drugs from the dispensary (FREE).
4. Document all the drugs given in the patient’s folder or weighing card, and in the 279/PMTCT
records book on the ward.
Feeding options
• DO NOT give artificial feeds if the mother has not opted for it.
• Find out what feeding option the mother has chosen.
o ? Exclusive breastfeeding
OR
o ? Artificial feeds
• If the mother has opted to breastfeed:
o Support her
o Ask any of the doctors/nurses who have been trained in PMTCT to counsel the mother on
how to minimize risk of infection to the baby.
• If the mother has opted not to breastfeed but to give artificial feeds
o Support her
o Ask any of the doctors/nurses trained in PMTCT to counsel mother on AFASS.
• If the mother has not made any informed choice or you do not have any information on the
mother’s feeding choice, then
o Admit and give IV fluids till the mother has been counseled
o Get in touch with the mother as soon as possible
1. IDENTIFY and TREAT any other problems
Follow-up
• The baby should be seen at the HIV clinic at 6 weeks of age.
• If there are any problems before 6 weeks of age, the baby should be brought to the hospital.
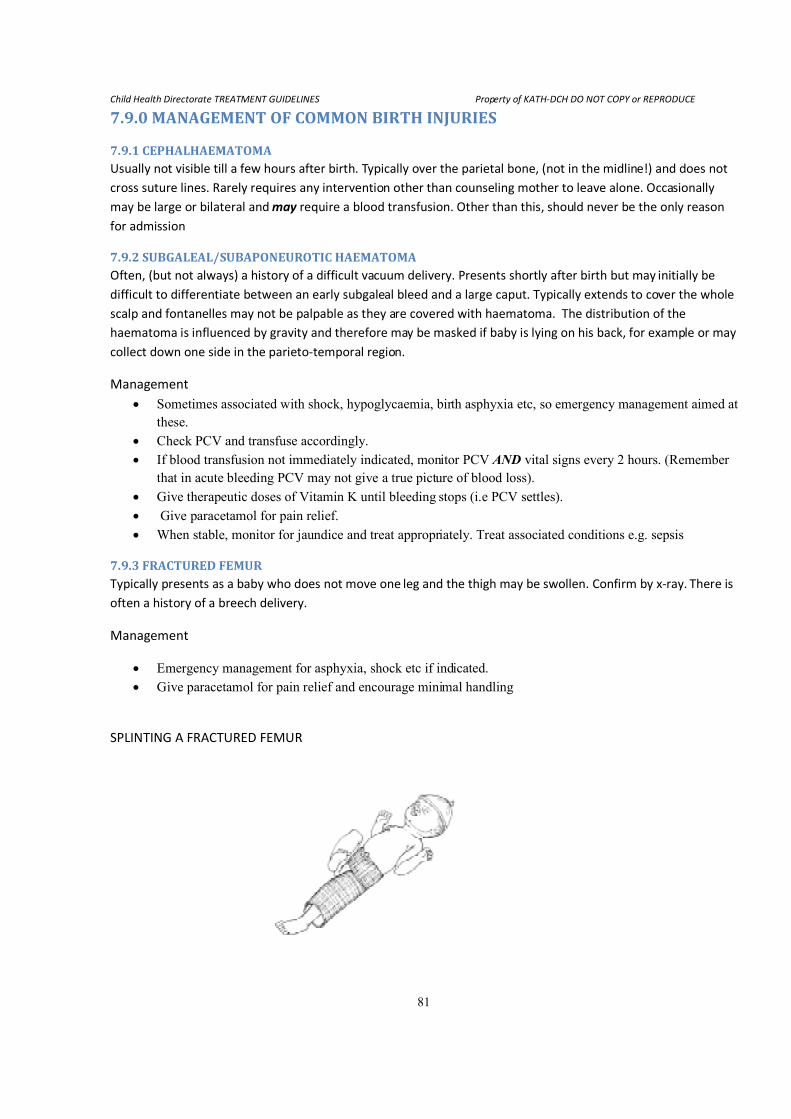
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
81
7.9.0 MANAGEMENT OF COMMON BIRTH INJURIES
7.9.1 CEPHALHAEMATOMA Usually not visible till a few hours after birth. Typically over the parietal bone, (not in the midline!) and does not
cross suture lines. Rarely requires any intervention other than counseling mother to leave alone. Occasionally
may be large or bilateral and may require a blood transfusion. Other than this, should never be the only reason
for admission
7.9.2 SUBGALEAL/SUBAPONEUROTIC HAEMATOMA Often, (but not always) a history of a difficult vacuum delivery. Presents shortly after birth but may initially be
difficult to differentiate between an early subgaleal bleed and a large caput. Typically extends to cover the whole
scalp and fontanelles may not be palpable as they are covered with haematoma. The distribution of the
haematoma is influenced by gravity and therefore may be masked if baby is lying on his back, for example or may
collect down one side in the parieto-temporal region.
Management
• Sometimes associated with shock, hypoglycaemia, birth asphyxia etc, so emergency management aimed at
these.
• Check PCV and transfuse accordingly.
• If blood transfusion not immediately indicated, monitor PCV A�D vital signs every 2 hours. (Remember
that in acute bleeding PCV may not give a true picture of blood loss).
• Give therapeutic doses of Vitamin K until bleeding stops (i.e PCV settles).
• Give paracetamol for pain relief.
• When stable, monitor for jaundice and treat appropriately. Treat associated conditions e.g. sepsis
7.9.3 FRACTURED FEMUR Typically presents as a baby who does not move one leg and the thigh may be swollen. Confirm by x-ray. There is
often a history of a breech delivery.
Management
• Emergency management for asphyxia, shock etc if indicated.
• Give paracetamol for pain relief and encourage minimal handling
SPLINTING A FRACTURED FEMUR
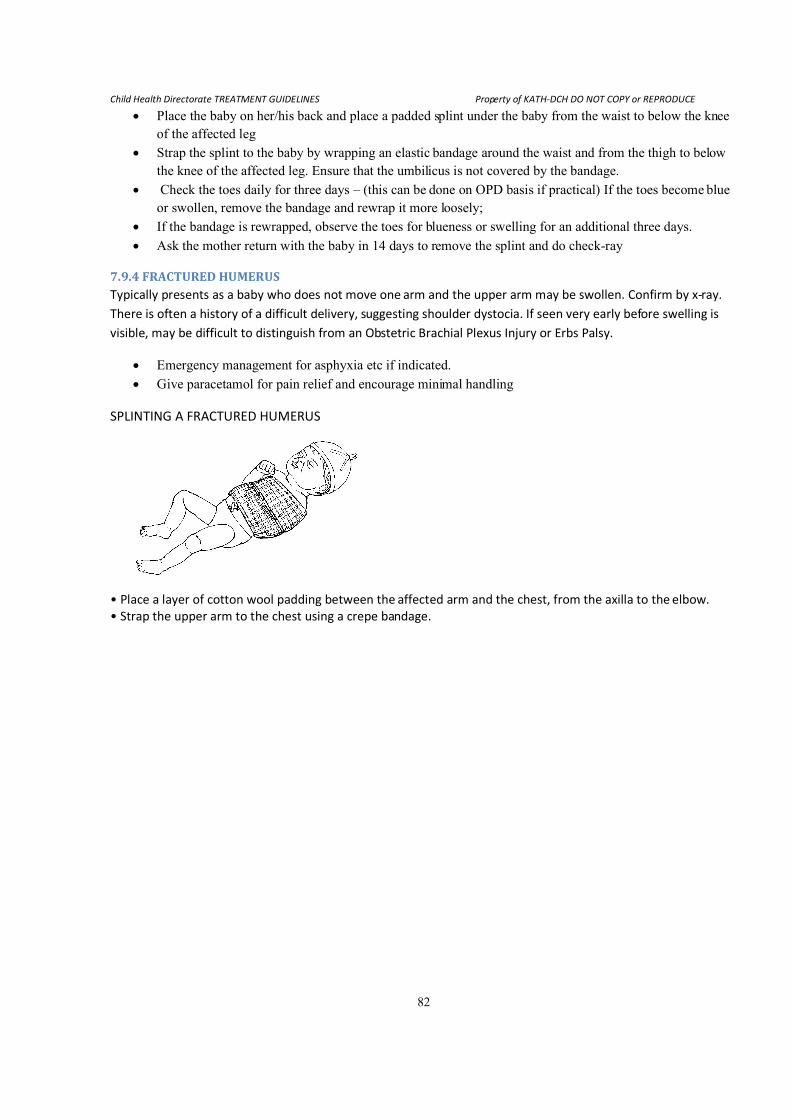
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
82
• Place the baby on her/his back and place a padded splint under the baby from the waist to below the knee
of the affected leg
• Strap the splint to the baby by wrapping an elastic bandage around the waist and from the thigh to below
the knee of the affected leg. Ensure that the umbilicus is not covered by the bandage.
• Check the toes daily for three days – (this can be done on OPD basis if practical) If the toes become blue
or swollen, remove the bandage and rewrap it more loosely;
• If the bandage is rewrapped, observe the toes for blueness or swelling for an additional three days.
• Ask the mother return with the baby in 14 days to remove the splint and do check-ray
7.9.4 FRACTURED HUMERUS Typically presents as a baby who does not move one arm and the upper arm may be swollen. Confirm by x-ray.
There is often a history of a difficult delivery, suggesting shoulder dystocia. If seen very early before swelling is
visible, may be difficult to distinguish from an Obstetric Brachial Plexus Injury or Erbs Palsy.
• Emergency management for asphyxia etc if indicated.
• Give paracetamol for pain relief and encourage minimal handling
SPLINTING A FRACTURED HUMERUS
• Place a layer of cotton wool padding between the affected arm and the chest, from the axilla to the elbow.
• Strap the upper arm to the chest using a crepe bandage.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
83
7.10.0 MANAGEMENT OF NEONATAL TETANUS (NNT) Suspect tetanus in a previously well neonate with inability to feed and spasms, which are provoked or
aggravated by stimulation. There is often no history of the mother having had anti tetanus immunization
during pregnancy, and there may be a history of poor cord care.
7.10.1 AIMS OF MANAGEMENT
o RESUSCITATION (Airways, Breathing and Circulation, Treat Hypoglycaemia)
o MAXIMUM SPASM CONTROL WITH MINIMUM RESPIRATORY DEPRESSION
o IDENTIFICATION AND TREATMENT OF ALL ONGOING INFECTION
o MAINTENANCE OF HYDRATION AND NUTRITION
7.10.2 SPECIFIC STEPS TO TAKE
• Resuscitate and stabilise, check for and treat hypoglycaemia
• Take bloods as for neonatal sepsis and do LP if not contraindicated and if possible give the
following drugs
o Broad spectrum antibiotics as for sepsis/meningitis
o Antitetanus serum 5000 units (or Human tetanus immunoglobulin im, single dose of
500 units – preferable if available)
o Chlorpromazine IM/NGT 7.5mg every 8 hrs plus
o Phenobarbitone IM/NGT 30mg stat then 7.5mg every 12 hours
o Diazepam IM/NGT 2mg every 3-6 hrs PRN
• Control fever appropriately
• Pay attention to keeping the cord clean on a daily basis
• Maintain a policy of minimal handling (no bathing!)
• Keep well hydrated by NG tube feeding of breast milk, and IV fluids.
• Adequate immunization for nursing mothers’ of children with neonatal tetanus
MONITOR BREATHING AND SPASMS, AND GRADUALLY REDUCE THE SEDATION AS THE SPASMS DECREASE
IN FRQUENCY AND INTENSITY. THIS MAY TAKE AS LONG AS TWO WEEKS BUT MAY BE MUCH SHORTER.
WHEN SPASMS STOP, ENCOURAGE MOTHER TO KEEP PUTTING THE BABY TO BREAST.
NB!!!
� Risk factors for NNT are risk factors for neonatal sepsis, cord sepsis and meningitis, hence
the need to identify these other infections and treat them appropriately. It is common to see a
baby being treated for NNT, with the source of the infection, often the cord, remaining
unclean and badly infected and thus maintaining the infection.
� Use of oral sedatives, (crushed tablets down an NG tube) cuts the cost of sedatives by 90%,
and should be used as soon as possible, usually after about the first day of treatment. Passage
of the NG tube should be done under sedation with diazepam, with an ambu bag ready at
hand as it may provoke severe prolonged spasms and consequent apnoea. Once passed, the
NG tube must be firmly taped to avoid the need for re passage.
� Sedatives must be written up on a separate sedation chart to avoid confusion. They should be
evenly spaced to provide regular, smooth and sustained sedation.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
84
7.11.0 KANGAROO MOTHER CARE (KMC) 1. All staff should learn, teach and encourage mothers to practice KMC
2. All mothers should know the benefits of KMC and how to practice KMC
3. Preterm and Low birth babies in stable condition should be placed in KMC position for at least 4
hours in the morning - 8am to 12noon, and 4 hours in the afternoon - 2pm to 6pm.
4. All nurses and other staff should support mothers practicing KMC and allow them to keep their
babies in KMC position for as long as they can.
5. KMC babies should be weighed on alternate days, head circumference and length measured
weekly
6. Monitor temperature 4 hourly
7. Babies can be discharged if feeding well (breastmilk) and gaining weight, and if baby is said to be
well to go home according to the doctor, and mother confident to practice KMC at home
8. Before discharge, the grandmother, father or a relative should be involved in KMC of the baby and
provide support to the mother at home
9. Follow up should be continued until the baby weighs more than 2.5kg
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
85
7.12.0 ANTIBIOTIC PROTOCOL FOR BABIES ADMITTED TO MBU
1. Take BLOOD and CSF for culture before starting antibiotics
2. See the drug dosages chart for the antibiotic dosages
3. Duration of treatment for Staph. aureus and Gram negative sepsis is 14 – 21 days: parentheral
for at least 7 days
4. Duration of treatment for Coagulase neg. staph sepsis – 7 days
First line antibiotics for Sepsis
• Cefuroxime and Gentamicin
Second line antibiotics for Sepsis
• Cefotaxime or Ceftazidime or Ceftriaxone
Avoid Ceftriaxone in first week of life
First line antibiotics for Cord Sepsis /Cellulitis /Abscess
• Flucloxacillin and Gentamicin
First line antibiotics for Meningitis
• Crystalline Penicillin and Gentamicin
Second line antibiotics for Meningitis
• Ceftriaxone or Cefotaxime or Ceftazidime
First line antibiotics for Osteomyelitis/Septic Arthritis
• Flucloxacillin & Gentamicin (at least 14 days parentheral, total duration of treatment is 6 weeks)
Second line antibiotics for Osteomyelitis/Septic Arthritis
• Clindamycin
CHANGING FROM FIRST LINE TO SECOND LINE
1. Should not be based on culture results alone
2. When patient is clinically not improving eg. temperature spiking or unstable temperature, feeing
poorly, respiratory difficulty etc,
a) Change after 48hrs of antibiotic treatment
b) Change antibiotics based on culture
c) But if culture not yet ready, change to second line
3. Always consult a senior colleague when changing
4. If patient has been on adequate frist line antibiotics before admission, start with second line
5. For all re-admissions who need antibiotics, start with second line
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
86
8.0 FLUID & METABOLIC DISORDERS 8.1.0 DIABETIC HYPERGLYCEMIC CRISIS/COMA
1. RAPID ASSESSMENT
i) Vomiting, drowsiness, polyuria, polydipsia, abdominal pains, weight loss etc.
ii) Dehydration (-10%) Listlessness, deep rapid breathing, Ketotic (‘fruity’) breath shock, coma
iii) Significant hyperglycemia, usually > 17mmol/L
2. Diagnosis of DKA
i) Hyperglycemia (glucose > 11.1mmol/dl)
ii) Acidosis (pH < 7.25 or bicarbonate <17)
iii) Ketosis (serum or urine)
3. MANAGEMENT
i) Airway, Breathing, & Circulation
ii) 100% O2 to patients with cyanosis/shock or SaO2 <90%
iii) Start IV fluid, insulin, & Potassium as below
iv) Pass an N-G tube to drain gastric contents in comatose patients.
v) Accurately assess urine output.
vi) Suspect cerebral edema if there is a set back after 2-24hrs and treat with mannitol.
vii) Find precipitating cause and treat appropriately.
viii) Maintain a flow chart of patient’s clinical data
FLUID
i. Start intravenous fluid (N/S or R/L) at once to run at 10-20ml/kg/hr (i.e. 0.35ml/kg/min for
1st
hr ± plasma/Haemaccel 10ml/kg IV if shocked).
ii. If no urine is passed, continue IV bolus for 2nd
(±3rd
) hours as well
iii. Calculate fluid requirement for 24hrs. (i.e. maintenance fluid + 10% deficit/ dehydration )
a. Give 1.5 times maintenance for 36-48hrs or
b. Decrease infusion rate to 10ml/kg/hr for next 6-7 hrs.
i. Give the remaining fluid requirement over the subsequent 16 hrs.
iv. Change IVF to 5% Dextrose /saline when blood glucose ≤11mmol/L.
INSULIN
i. Start insulin after first hour of NS/LR bolus/rapid infusion is completed.
ii. Start low dose insulin regimen
a) Soluble insulin @ O.1u/kg/hr as IV infusion with a syringe pump,
b) May give first dose IV then subsequent doses IM/IV (e.g. 0.2u/kg/2hrs IM )
b) Reduce insulin dose to 0.05u/kg/hr if child < 5 years or glucose falls more than 4
mmol/L/hr.
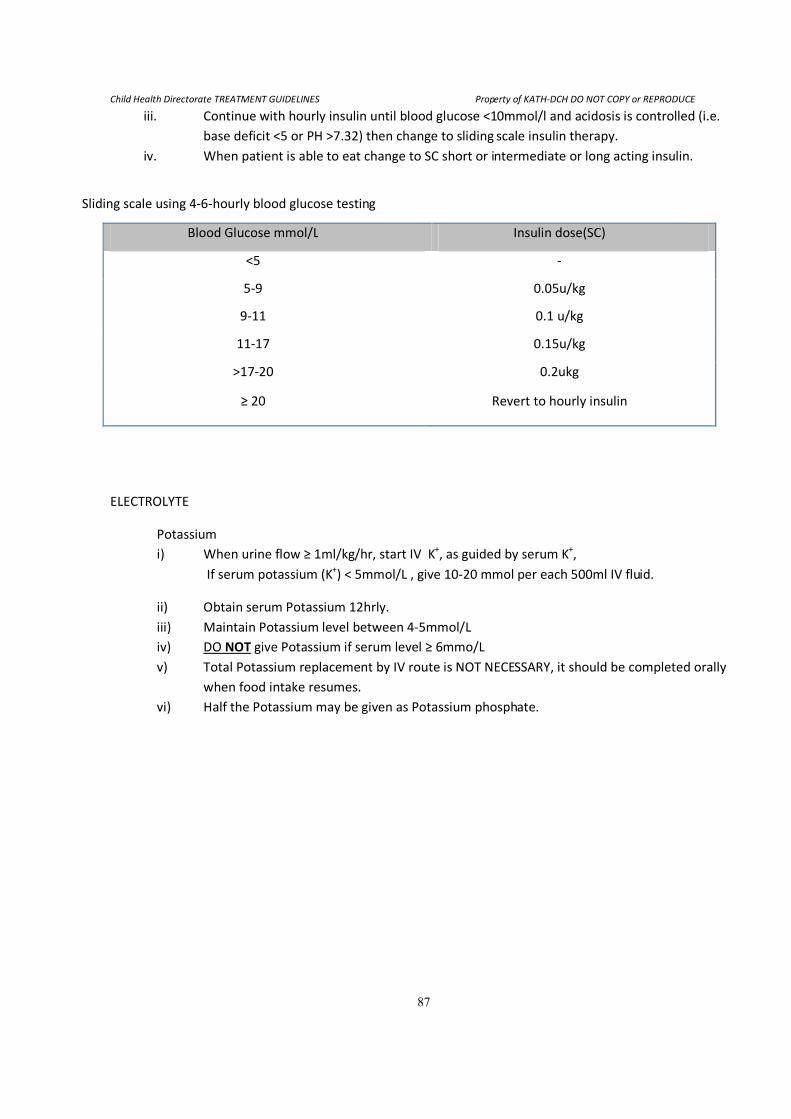
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
87
iii. Continue with hourly insulin until blood glucose <10mmol/l and acidosis is controlled (i.e.
base deficit <5 or PH >7.32) then change to sliding scale insulin therapy.
iv. When patient is able to eat change to SC short or intermediate or long acting insulin.
Sliding scale using 4-6-hourly blood glucose testing
Blood Glucose mmol/L Insulin dose(SC)
<5 -
5-9 0.05u/kg
9-11 0.1 u/kg
11-17 0.15u/kg
>17-20 0.2ukg
≥ 20 Revert to hourly insulin
ELECTROLYTE
Potassium
i) When urine flow ≥ 1ml/kg/hr, start IV K+, as guided by serum K
+,
If serum potassium (K+) < 5mmol/L , give 10-20 mmol per each 500ml IV fluid.
ii) Obtain serum Potassium 12hrly.
iii) Maintain Potassium level between 4-5mmol/L
iv) DO NOT give Potassium if serum level ≥ 6mmo/L
v) Total Potassium replacement by IV route is NOT NECESSARY, it should be completed orally
when food intake resumes.
vi) Half the Potassium may be given as Potassium phosphate.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
88
9.0 ONCOLOGICAL DISORDERS
9.1.0 METABOLIC AND ONCOLOGIC EMERGENCIES
9.1.1 TUMOUR LYSIS SYNDROME This syndrome occur primary in patients with high tumour burden, bulky B-cell or T-cell leukemias or
lymphomas, and can occur in standard-risk acute lymphoblastic leukemia (ALL)
The rapid lysis of blasts (tumor cells) causes a massive release of intracellular contents, particularly
potassium, phosphorus, and nucleic acids resulting in;
a. Hyperkalemia
b. Hyperuricaemia
c. Hyperphosphatemia (accompanied by compensatory hypocalcemia)
Complications
Cardiac arrhythmias
Renal failure
Seizures
Coma
Disseminated intravascular coagulation (DIC)
Death
Management
Administer
Hydration(K+ free), at 2 times maintenance to keep urine specific gravity <1.010.
allopurinol,100mg/m2/dose Q8hr (or10mg/kg/day) PO. May load with 300mg/m
2
alkalinization, may give NaHCO3 100mg/kg/day PO Q6-8hrly to keep urine
pH 7.0-7.5. Stop alkalinization if urine pH > 7.5
Strictly monitor urine output, specific gravity and pH (keep urine output >3ml/kg/hr)
Manage metabolic derangement appropriately:
Hyperkalemia (K+>6.0mmol/L)
Do not administer K until tumor lysis is controlled.
Use the following measures to drive K into cells:
Provide hydration and alkalinization.
Nebulize with salbutamol 5mg (2.5mg if <8yr old) Q3-4hrly
Insulin 0.1/kg/hr with glucose 0.5g/kg/hr. Monitor glucose hourly.
10% Calcium gluconate (with onset of ECG changes) 1ml/kg/dose over 5mins.
Consider dialysis if these measures are not successful.
Hypocalcaemia (Ca2+
< 0.75mmol/L)
Hypocalcaemia is compensatory to hyperphosphatemia (Ca2+
× PO42-
<60)
Only treat symptomatic hypocalcaemia (e.g. Tetany).
Give 10% Calcium gluconate at 0.5ml/kg/dose over 5mins. May repeat after 0.5hr
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
89
Hyperphosphatemia
Restrict dietary phosphate
Give Al(OH)3 150mg/kg/day PO ÷ 4-6hrly, use with caution in renal failure.
Or Calcium Carbonate (up to 5 tablets 8hrly)
N/saline at 20ml/kg over hr and IV mannitol (use only if renal function is normal)
Consider dialysis, if poor renal function.
Prevention
With 1st
course of therapy.
1. Commence allopurinol 24-48 hours before treatment.
2. Prehydrate for 24hours . Do not use fluids containing K. Volume to be given is 3L/m2. Unless
there is renal failure with oliguria, in which case fluid input must be appropriate.
3. May need to alkalinise the urine with IV NaHCO3 at 3 mmol/kg/day.
4. Strict input/output chart.
Monitor the serum electrolytes and uric acid level.
9.1.2 FEBRILE NEUTROPENIA
Definition
• Absolute Neutrophil count <1.0 x 109/L and
• Temperature ≥ 38oC for two hours should be treated as an infection.
Infections caused by both gram negative and gram positive organisms.
Investigations
• FBC, Blood Film for mps,
• Culture blood, urine, stool (± CSF if indicated); swabs of lesions, throat swabs
• Chest x-rays
• Abdominal Ultrasound Scan, at least.
Management
Choice of antibiotics-
1st
line � Ampicillin / Co-Amoxiclav and Gentamycin,
2nd
line�Cefuroxime/Ceftazidime / Ceftriaxone and Amikacin/ Ciproflocaxin,
Meropenem
• Remember to give antimalarial treatment.
• If fever persists over 48hours, add anti-staphylococcus –e.g. Flucloxacillin, but preferably
vancomycin if available.
• If fever persists further, consider adding antifungal. The most common fungal infection is candida.
• May have to treat possible atypical pneumonia if respiratory symptoms e.g. consider pneumocystis.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
90
9.2.0 BASIC INVESTIGATIONS FOR ALL ONCOLOGY PATIENTS General
• FBC [Hb, RBCs indices, WBCs total and differential, Platelet] + rectic count ± film comment
• Renal function test:- Na, K, Cl, urea, creatinine, cholesterol, Ca, Mg, inorg PO4
• Liver function test
• Uric acid, LDH
• Chest x –ray
• Abdominal Ultrasound Scan
• Stool R/E
• Fine needle aspirate/ biopsy
o Contact pathologists so that reports are obtained within 3 -5 days.
Other laboratory investigations
• HIV screen
• Bone marrow aspirate
• Lumber puncture for CSF (when giving first IT dose)
o cytology or
o may send for cell type and count (to microbiology) if cytology not possible.
• Etc etc depending on differential diagnosis.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
91
9.3.0 RETINOBLASTOMA Investigations
• FBC[Hb, RBCs, WBCs total and differential, Platelet] + rectic count ± film comment
• Renal function test, Blood Urea and electrolyte
• Chest x –ray
• Abdominal Ultrasound Scan
• Head CT scan
• Tumor aspirate/ biopsy
• CSF for cytology.
• Refer for ophthalmologist assessment if not already done.
Management
Surgery + Neojuvant/Adjuvant chemotherapy ± Adjuvant radiotherapy
Many of the cases seen here are advanced and require enucleation followed by chemotherapy within two
weeks of surgery or chemotherapy reduction and then enucleation (usually after two courses of chemo)
followed by further chemotherapy.
If thickened optic nerve on CT scan and /or tumour found at excised optic nerve end then will require
adjunctive radiotherapy.
Six courses of chemotherapy required at 3 weeks interval (check neutrophils count)
• IV vincristine 1.5mg/m2 bolus
• Etoposide 300mg/m2 in 100 ml N/S over 1 hr
• Carboplatin 600mg/m2 in 100mls 5% dextrose over one hour.
o Or Cyclophosphamide 800mg/m2 in 100mls fluid over 30 mins
o Carboplatin preferred if can afford this in place of Cyclophosphamide use;
• IT methotrexate and IV vincristine weekly for first 6 weeks.
If bone marrow involvement, ensure it is free (repeat BM) before doing the radiotherapy.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
92
9.4.0 RHABDOMYOSARCOMA Investigations
• FBC[Hb, RBCs, WBCs total and differential, Platelet] + rectic count ± film comment
• Renal function test, Blood Urea and electrolyte
• Chest x –ray
• Abdominal Ultrasound Scan
• Tumor aspirate/ biopsy
Management
Management includes chemotherapy and may require adjunctive surgery to remove residual tumour or
radiotherapy.
TREATMENT
Give at three week interval for a total of 9 courses (27 weeks);
• vincristine 1.5mg/m2 bolus
• Actinomycin D 1.5mg/m2 bolus
• cyclophosphamide 800mg/m2
in 100ml fluid over 30 minutes
• weekly iv vincristine 1.5mg/m2 (for the first 6 weeks)
Re-assess after first three full courses of treatment;
• If tumour response is over 50% reduction in size then continue for the nine courses.
• If tumour response is poor, < 50% reduction, then discuss with consultant and will add further
chemo-agents-e.g. etoposide, carboplatin, doxorubicin in combination.
After six courses, then residual tumour is removed surgically or adjunctive radiotherapy given.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
93
9.5.0 BURKITT’S LYMPHOMA Clinical features
• typical jaw tumor with dental anarchy,
• abdominal mass(es) with a highly suggestive ultrasound result (single or multiple homogenous
round masses without capsule
Investigations
• FBC[Hb, RBCs, WBCs total and differential, Platelet] + rectic count ± film comment
• Renal function test, Blood Urea and electrolyte
• LDH and Uric acid
• Chest x –ray
• Abdominal Ultrasound Scan
• Tumor aspirate/ biopsy
Staging
Stage 1 - Single solitary extra-abdominal site
R - Intra-abdominal, more than 90% of tumor resected
Stage 2 -Multiple extra-abdominal tumors
Stage 3 -Intra-abdominal tumor
Stage 4 -Intra-abdominal plus one or more extra-abdominal sites
Management
General supportive care
• Ensure good oral hygiene
• Note and treat every fever suspicious of neutropenia
• Note and treat every pain suspicious of relapse
• Ensure frequent voiding (even at night) during treatment with cyclophosphamide to prevent
hemorrhagic cystitis
Treatment divided into Pre-phase and Induction.
The Induction treatment is given in several cycles (minimum 6, or until remission plus 2 cycles).
Clinical follow-up for patients in Remission (treatment completed and tumor not detectable) for at
least one year to detect Relapse.
Preparation for Pre-phase: 24hours before prephase, the patient should be given
• Fluids @ 2 - 2.5L/m2 for 24 hrs
• Allopurinol @ 10-20mg/kg in 2-3 doses [for the 1st 5 days]
• Analgesics if indicated.
Pre-phase
Allopurinol [continue from preparation phase above]
Cyclophosphomade (PO/IV) @ 200mg/m2 daily for 5 days
Induction
Before each cycle of chemotherapy FBC should be done:
• If HB<7g/dl hemotransfuse before giving i.v. cyclophosphamide/vincristine.
• If total WBC < 3.0 x 109/L and patient not ill, give amoxicillin for 5 days and defer
chemotherapy until total WBC ≥ 3.0 x 109/L
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
94
• If platelets < 70 x 109/L defer i.t. methotrexate until platelets ≥ 70 x 10
9/L
� first course of chemotherapy for all stages
1. IV Cyclophospamide (CTX) 1200mg/m2 OR 40mg/kg over 30mins in 100ml fluid (N/S)
• Dose may be given as two half doses; 600mg/m2 each, 48 hrs apart in cases with very
bulky diseases.
2. IT methotrexate(see below for dosages)
• If no CNS disease give IT methotrexate stat only
• if CNS disease, then give extra
i. IT methotrexate daily x 4 days and tabs folinic acid 15mg tds x 5 days
ii. If no folinic acid then give IT cytarabine 30mg daily x 4 days.
• Continue with post-hydration for at least 48 hrs after last dose of CTX.
IT methotrexate dosage by age: –
<1yr= 6 mg 1- 2yr = 8mg
2-3yr = 10mg ≥3yr = 12.5mg
May use midazolam sedation or ketamine
Second and subsequent courses (two weekly intervals)
Check FBC and ensure absolute neutrophils count > 1.0 x 109/L before giving chemotherapy.
Stage 1 and 2
• IV Cyclophosphamide 1200mg/m2 over 30 minutes
• IT Methotrxate 12.5mg (see dosage if younger than three years)
Give a total of three courses (no pre or post IV fluid hydration required but ensure child tolerating about
2.5L/m2 and there is no vomiting)
STAGES 3 and 4 (combination chemotherapy required)
• IV Cyclophosphamide 700mg/m2 in 100mls fluid over 30 mins
• IT Methotrxate 12.5mg (see dosage if younger than three years)
• IV Vincristine 1.5mg/m2 bolus
• IV Doxorubicin (Adriamycin) 30mg/m2 in 250mls over 6 hrs.
*IV metoclopromide 100 micrograms/kg 30 mins before chemo, may repeat after 6 hrs.
Repeat this at two weekly intervals alternating with;
• IV Vincristine 1.5mg/m2 bolus
• IV Cytarabine (cyctosine arabinoside) 400mg/m2 in 500mls over 24hrs.
• IT Methotrexate 12.5mg (see dosage if younger than three years)
• IV Cyclophosphamide 700mg/m2 in 100mls fluid over 30 mins
These courses will be given for a total of 4-6 courses (no hydration fluid required)
IT methotrexate is given for only the first three courses.
Relapsed Burkitt’s lymphoma: combination chemotherapy as above.
May use high dose methotrexate iv in some cases- consultant to decide.
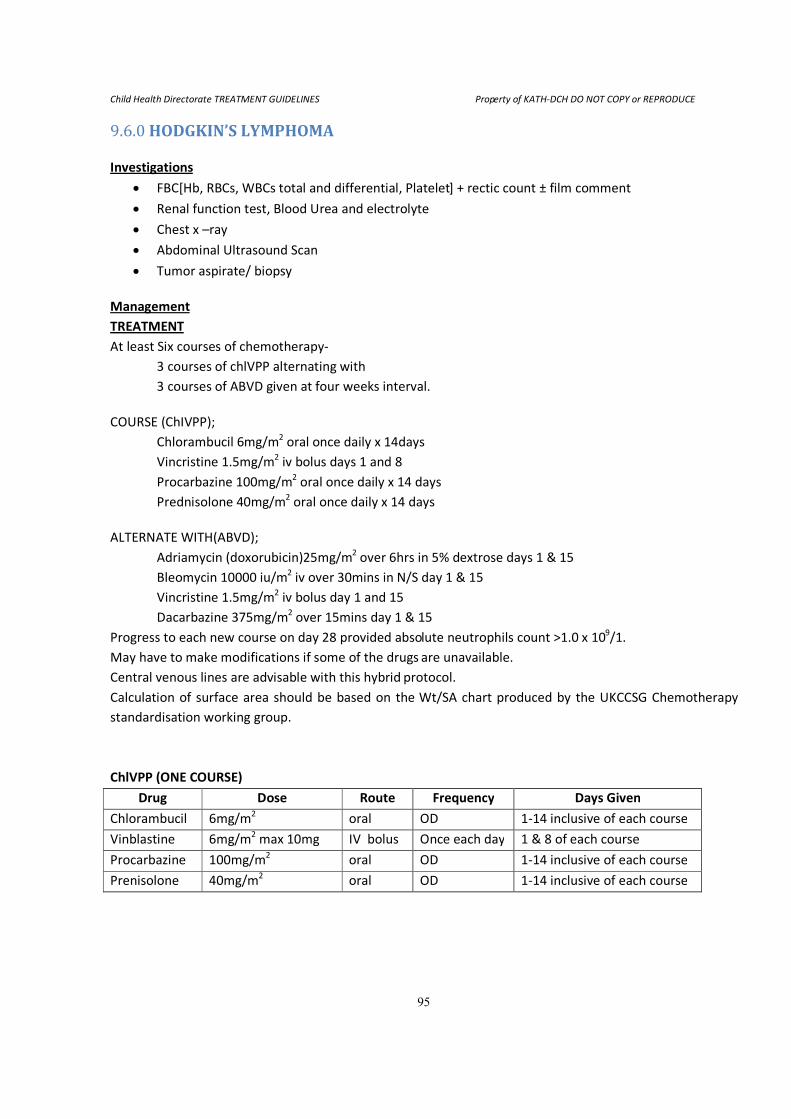
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
95
9.6.0 HODGKIN’S LYMPHOMA
Investigations
• FBC[Hb, RBCs, WBCs total and differential, Platelet] + rectic count ± film comment
• Renal function test, Blood Urea and electrolyte
• Chest x –ray
• Abdominal Ultrasound Scan
• Tumor aspirate/ biopsy
Management
TREATMENT
At least Six courses of chemotherapy-
3 courses of chlVPP alternating with
3 courses of ABVD given at four weeks interval.
COURSE (ChIVPP);
Chlorambucil 6mg/m2 oral once daily x 14days
Vincristine 1.5mg/m2 iv bolus days 1 and 8
Procarbazine 100mg/m2 oral once daily x 14 days
Prednisolone 40mg/m2 oral once daily x 14 days
ALTERNATE WITH(ABVD);
Adriamycin (doxorubicin)25mg/m2 over 6hrs in 5% dextrose days 1 & 15
Bleomycin 10000 iu/m2 iv over 30mins in N/S day 1 & 15
Vincristine 1.5mg/m2 iv bolus day 1 and 15
Dacarbazine 375mg/m2 over 15mins day 1 & 15
Progress to each new course on day 28 provided absolute neutrophils count >1.0 x 109/1.
May have to make modifications if some of the drugs are unavailable.
Central venous lines are advisable with this hybrid protocol.
Calculation of surface area should be based on the Wt/SA chart produced by the UKCCSG Chemotherapy
standardisation working group.
ChlVPP (ONE COURSE)
Drug Dose Route Frequency Days Given
Chlorambucil 6mg/m2
oral OD 1-14 inclusive of each course
Vinblastine 6mg/m2 max 10mg IV bolus Once each day 1 & 8 of each course
Procarbazine 100mg/m2
oral OD 1-14 inclusive of each course
Prenisolone 40mg/m2 oral OD 1-14 inclusive of each course
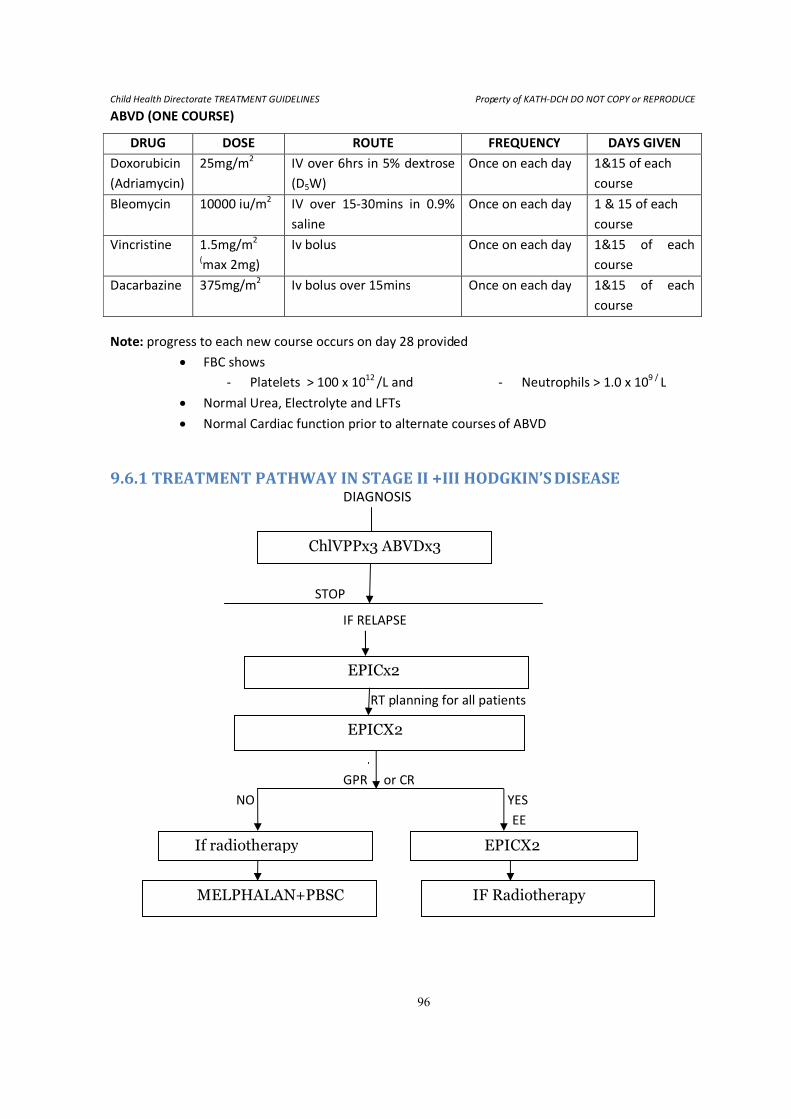
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
96
ABVD (ONE COURSE)
DRUG DOSE ROUTE FREQUENCY DAYS GIVEN
Doxorubicin
(Adriamycin)
25mg/m2 IV over 6hrs in 5% dextrose
(D5W)
Once on each day 1&15 of each
course
Bleomycin 10000 iu/m2
IV over 15-30mins in 0.9%
saline
Once on each day 1 & 15 of each
course
Vincristine 1.5mg/m2
(max 2mg)
Iv bolus Once on each day 1&15 of each
course
Dacarbazine 375mg/m2 Iv bolus over 15mins Once on each day 1&15 of each
course
Note: progress to each new course occurs on day 28 provided
• FBC shows
- Platelets > 100 x 1012
/L and - Neutrophils > 1.0 x 109 /
L
• Normal Urea, Electrolyte and LFTs
• Normal Cardiac function prior to alternate courses of ABVD
9.6.1 TREATMENT PATHWAY IN STAGE II +III HODGKIN’S DISEASE DIAGNOSIS
STOP
IF RELAPSE
RT planning for all patients
EEEEP
GPR or CR
NO YES
EE
ChlVPPx3 ABVDx3
EPICx2
EPICX2
If radiotherapy EPICX2
IF Radiotherapy MELPHALAN+PBSC
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
97
9.7.0 WILM’S TUMOUR
Investigations
• FBC[Hb, RBCs, WBCs total and differential, Platelet] + rectic count ± film comment
• Renal function test, Blood Urea and electrolyte
• Chest x –ray
• Abdominal Ultrasound Scan
• Tumor aspirate/ biopsy
o Contact pathologists so that reports are obtained within 3 -5 da
Management
AFTER investigations and fine needle aspirate, management is by paediatric surgery/urology. Treatment
consists of pre-operative chemotherapy, surgical removal of tumour/ kidney, post operative chemotherapy
and may require adjunctive radiotherapy.
Vincristine @ 1.5mg/m2 bolus weekly x 4 weeks
Actinomycin D @ 1.5mg/m2 bolus at week one and week three.
Note: doses for patients <12kg is reduced to two thirds calculated dose.
Surgery at week 5 – 6
Post operative chemotherapy given once peristalsis is established following surgery and within 21 days of
last pre-operative chemotherapy.
Duration of post-operative chemotherapy is 27 weeks.
Post operative chemotherapy:
Vincristine @1.5mg/m2 weekly for 8 weeks and then at 3 weekly intervals
i.e. weeks 11, 14, 17, 20, 23, 26.
Actinomycin D @ 1.5mg/m2 bolus weeks 2, 5, 8, 11, 14, 17, 20, 23 and 26
Based on risk assessment some high risk cases will require other drugs and radiotherapy --> consultant to
decide: Drugs include cyclophosphamide, doxorubicin, etoposide, carboplatin.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
98
9.8.0 PAEDIATRIC ACUTE LYMPHOBLASTIC LEUKAEMIA (ALL)
Investigations
• FBC[Hb, RBCs, WBCs total and differential, Platelet] + rectic count ± film comment
• Renal function test, Blood Urea and electrolyte
• Chest x –ray
• Abdominal Ultrasound Scan
• Tumor aspirate/ biopsy
o Contact pathologists so that reports are obtained within 3 -5 days.
Management
• Cytotoxic drugs are calculated by body surface area (BSA)
• BSA (M₂) = Square root of [Height (m) x Weight (kg) /3600) or use chart to convert from kg.
• Treatment is given as pre-treatment phase, followed by regimen A or B induction phase, followed by
maintenance.
• Regimen A induction for patients age<10yrs and highest recorded total WBC count <50 x10 9/L.
• Regimen B induction for patients age ≥ 10yrs and/or highest recorded total WCC >50 x10 9/L.
9.8.1 PRE-TREATMENT PHASE
• Commence as soon as diagnosis confirmed either by blood film or bone marrow aspirate review by
haematologist.
• For patients with clinic suspicion of CNS disease see notes at end of protocol
• Hydration is commenced – maximal oral fluids, supplemented for 48hrs with 2-2.5L/m2/24hrs iv.
• Allopurinol is commenced – 10-20mg/kg/day po in 2 divided doses for 7 days
• Prednisolone 2mg/kg po daily in the morning.
o If WCC≥80x109/L the pre-treatment phase continues for 7days
o If WCC<80x109/L the pre-treatment phase continues for 2 days
• Once pre-treatment phase completed patient commences day 1 of induction with regimen A or B
depending on their highest recorded WCC and age as above.
9.8.2 REGIMEN A INDUCTION
• Prednisolone 2mg/kg po in the morning day 1-28, then 1.5mg/kg for 2 days, 1mg/kg for 2 days,
0.5mg/kg for 2 days, then stop.
• Vincristine 1.5mg/m 2 (max dose 2mg) iv day 1, 8, 15, 22, 29)
• Intrathecal Methotrexate dose by age:
o <2yrs=7.5mg, 2yrs=10mg, ≥3yrs = 12.5mg
o Day 9, 16 and 23 (see intrathecal notes)
• Cotrimoxazole by BSA on day of vincristine and following days (Day 1,2,8,9,15,16,22,23,29,30)
o 0.5-0.75 m2 =240mgbd,
o 0.76-1.0m2
=360mg bd,
o >1.0m2
= 480mg bd
• Folic Acid 5mg PO daily day 1-30
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
99
Reviews during regimen A induction:
1. Patient can be discharged once diagnosis confirmed and iv fluids discontinued if they are
afebrile, well enough to be managed at home and parents understand the drug regimen and
plan for review. Parents must also understand indications for returning for earlier review.
2. Check FBC on day 30 to see if ready to progress to maintenance (neutrophil count more than
0.75x109/L and platelet count > 75x10
9/L). If counts too low request blood film review by
haematologist �?needs BM aspirate or ?non-responder/relapse.
9.8.3 REGIMEN B INDUCTION
• Prednisolone 2mg/kg po in the morning day 1-28, then 1.5mg/kg for 2 days, 1mg/kg for 2 days,
0.5mg/kg for 2 days, then stop
• Vincristine 1.5mg/m2
(max dose 2mg) iv day 1,8, 15,22, 29
• Doxorubicin 25mg/m2
iv day 8 and 22
• Cyclophosphamide 750mg/m2
iv day 29 and 36
• 6-mercaptopurine 75mg/m2
po daily day 30 onwards irrespective of blood counts. Do not take milk
simultaneously
• Intrathecal Methotrexate dose by age: ,2yrs =7.5mg, 2yrs=10mg, 3yrs or more = 12.5mg day 9,16,23,
and 30 (see intrathecal notes)
• Cotrimoxazole by BSA on day of vincristine and following day (Day 1,2,8,9,15,16,22,23,29,30)
o 0.5.-75 m2
=240mg BD, 0.76-1.0m2 =360mg BD, >1.0m
2 =480mg BD
• Folic Acid 5mg po daily on day 1-30
Reviews during regimen B induction:
1. Patient can be discharged once diagnosis confirmed and iv fluids discontinued if they are
afebrile, well enough to be managed at home and parents understand the drug regimen and
plan for review. Parents must also understand indications for returning for earlier review.
2. Check FBC on day 43 to see if ready to progress to maintenance (neutrophil count more than
0.75x109/1 and platelet count >75x109/1). If counts too low adjust dose of 6-mercaptopurine
as below and repeat FBC on day 50. If count still too low omit 6mercaptopurine and request
FBC with blood film review by haematologist on day 57 � ?needs BM aspirate - ?non-
responder/relapse.
9.8.4 MAINTENANCE
1. Commence once induction completed, PLUS Neutrophil count > 0.75x109/L and PLT > 75x10
9/L.
2. Should be continued for 48 weeks in four cycles of 12 weeks (84days)
• Intrathecal Methotrexate dose by age:
<2yrs = 7.5mg, 2-3yrs = 10mg, ≥3yrs = 12.5mg day 1
• 6-mercaptopurine 75mg/m2
po daily day 1-84 (see below re dose adjustment). Do not take milk
simultaneously
• Oral Methotrexate 20mg/m2
po weekly day 8, 15, 22, 29, 36, 43, 50, 57, 64, 71, 78
(weekly, but omit on day of intrathecal metehotrexate) (see below re dose adjustment)
• Vincristine 1.5mg/m2 (max dose 2mg) iv day 15, 43, 71 (ie week 3,7, 11)
• Prednisolone 2mg/kg po day 15-19, 43-47, 71-75 (ie for 5 days week 3,7,11)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
100
Clinic visits during maintenance:
Patient should attend for FBC on the day prior to intrathecal methotrexate and attend with the results to be
checked prior to drug administration platelet count must be >50x109/L and patient’s card.
The IV vincristine and PO Prednisolone are then given.
Notes:
6-mereaptopurine and oral methodtrexate dose adjustment during maintenance
The doses should be adjusted to maintain the neutrophil count between 0.75 and 1.5x109/1 and platelets
between 75 -150x109/L.
If the neutrophil count falls to 0.5 - 0.75x109/L halve the dose of 6-mercaptopurine and oral methotrexate.
Check FBC weekly and restart the 6-mercaptopurine (75mg/m2 po daily) and oral methotrexate (20mg/m
2
po weekly) when the neutrophil count is > 0.75x109/L.
If the platelet count falls to between 50 -75x109/L halve the dose of 6-mercaptopurine and oral
methotrexate.
If the platelet count falls to < 50x109/L. STOP the 6-mercaptopurine and oral methotrexate. Check FBC
weekly and restart the 6-mercaptopurine (75mg/m2 po daily) and oral methotrexate (20mg/m
2 po weekly)
when the platelet count is >75x109/L.
If both the platelet and neutophil counts fall, adjust dose according to which has the biggest drop and
ensure that both rise with dose adjustment.
Intrathecal Methotrexate
It is imperative that vincristine is NOT given via the intrathecal route.
In order to avoid this occurring intravenous vincristine should NOT be given on the same day as intrathecal
methotrexate.
The only drugs that can be given by the intrathecal routs are methotrexate, hydrocortisone and cytosine.
10 drops of CSF should be collected into a sterile container and taken to the haematology lab for a slide to
be made and a white cell count done. If the CSF WCC is >0.1x109/L and RCC<1x10
9/L discuss with
haematologist �?CNS involvement/relapse.
Who should be admitted to the ward
1. Patients that are neutropenic (neutrophil count<1.0x109/L) and febrile (Temp. > 38
OC) should be
assessed and admitted to the ward for broad spectrum antibiotics as per the neutropenic sepsis
regimen.
2. Patients that are too unwell to be managed at home e.g. Diarrhea or vomiting requiring intravenous
fluids, hypoxia, severe uncontrolled pain.
3. Patients with clinical evidence of CNS disease at presentation (neurological deficit) and patients who
have blasts in their CSF
o These patients should be treated as per regimen B unless too unwell to treat (at the
discretion of the specialist)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
101
Relapse and Non-Responders
These patients should be given palliative treatment only eg dexamethasone (discuss with the specialist)
Considerations for the future
Asparaginase could be added to the regimen if it becomes more readily available locally small doses of iv
cytosine could be added to regimen B induction if this becomes more readily available locally.
General Rules
• Patients are enrolled into the treatment programme through a specialist.
• Pre-phase helps to reduce the risk of tumour lysis syndrome. If cyclophosphamide tabs cannot be
swallowed, pre-phase can be given i.v.
• Laboratory investigations before treatment (minimum) includes Hb, WBC and platelets (renal
function and electrolytes are not necessary in my opinion – urinary output is more important);
LDH is not a necessary parameter – only if it is high before starting treatment, then it may be
able to monitor remission and relapse)
• X-rays are usually not helpful and in classical presentation not needed should be indicated by
specialists;
• Ultrasound of abdomen in all cases desirable
Pre-phase and first cycle of induction is given as in-patient treatment
Subsequent cycles can be given as out-patient treatment.
On each visit
History of fever, pain, mouth sores, appetite, weight loss, skin/joint problems, activity
O/E temperature, weight, pallor, inspection mucous membranes and skin for infections,
Lab: FBC (Hb, WBC, Platelets) + MPs
Reasons to defer treatment:
• If HB below 7g/dl – defer cycle for 5 days but give oral dexamethasone (O.6mg/kg in 2-4 doses
• If platelets below 100ml defer intrathecal methotrexate (without delaying the next i.v cycle)
• If malaria positive, but not ill – treat malaria and give chemotherapy
• If malaria positive, but very ill – treat malaria first and discuss with specialist (child may be ill
because of the tumour!!)
• If fever for no obvious reasons – treat with antibiotics and discuss with senior.
When to discuss a patient
• When tumour increases during treatment
• When patient ill
• When fever without explanation
• When any reason to defer treatment persists more than one week (do not forget – it is the tumour
that kills the patient!!!)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
102
6-mercaptopurine and request FBC with film FAO haematologist on day 27�? Needs BM aspirate - ?non-
responder/relapse.
Maintenance
Commence once induction completed and neutrophil count > 0.75x109/L and platelet count more than
75x109/L
Should be continued for 48 weeks in four cycles of 12 weeks (84 days)
Intrathecal Methotrexate dose by age:
<2yrs=7.5mg
2yrs=10mg,
≥3yrs =12.5mg day 1
6-mercaptopurine 75mg/m2 po daily day 1-84 (see below for dose adjustment) [Do not take milk
simultaneously]
Oral Methotrexate 20mg/m2
po weekly day 8,15,22, 29, 36, 43, 50, 57, 64,71, 78
(weekly, but omit on day of intrathecal methotrexate) (see below re dose adjustment
Vincristine 1.5mg/m2 (max dose 2mg) IV day 15, 43, 71 (i.e. week 3, 7, 11)
Prednisolone 2mg/kg po day 15-19, 43-47, 71-75 (i.e. for 5 days in weeks 3, 7, 11)
Clinic visits during maintenance:
Patient should attend for review on days 15, 43, and 71(i.e. 4 weekly). They should have FBC checked the
day before. The patient and FBC result should be reviewed (fro side effects of treatment and possible signs
of relapse especially). Dose adjustments should be made to the oral methotrexate and 6-mercaptopurine
doses (see below) and documented in the patient’s card. The iv vincristine and po Prednisolone are then
given.
Notes:
6-mercaptopurine and oral methotrexate dose adjustment during maintenance
The doses should be adjusted to maintain the neutrophil count between 0.75 and 1.5x109/1 and platelets
between 75 and 150x109/1.
If the neutrophil count falls to between 0.5 and 0.75x109/L. HALVE the dose of 6-mercaptopurine and oral
methotrexate.
If the neutrophil count falls to <0.5x109/L. STOP the 6-mercaptopurine and oral methotrexate. Check FBC
weekly and restart the 6-mmercaptopurine (75mg/m2 po daily) and oral methotrexate (20mg/m
2 po weekly)
when the neutrophil count is >0.75x109/L.
If the platelet count falls to between 50 and 75x109/L. HALVE the dose of 6-mercaptopurine and oral
methotrexate.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
103
If the platelet count falls to <50x109/L. STOP the 6-mercaptopurine and oral methotrexate. Check FBC
weekly and restart the 6-mercaptopurine (75mg/m2 po daily) and oral methotrexate (20mg/m
2 po weekly)
when the platelet count is .75x109/1.
If both the platelet and neutrophil counts fall dose adjust according to which has the biggest drop and
ensure the both rise with dose adjustment.
Intrathecal Methotrexate
It is imperative that vincristine is NOT given via the intrathecal route. In order to avoid this occurring
intravenous vincristine should not be given on the same day as intrathecal methotrexate.
The only drugs that can be given by the intrathecal route are methotrexate, hydrocortisone and cytosine.
10drops of CSF should be collected into a sterile container and taken to the haematology lab for a slide to
be made and a white cell count done. If the CSF WCC is > 0.1x109/L and RCC >1.0x10
9/L discuss with
haematologist ?CNS involvement /relapse.
Who should be admitted to the ward?
• Patients that are neutropenic (neutrophil count < 1.0x109/L) and febrile (Temp. 38
0C) should be
assessed and admitted to the ward for broad spectrum antibiotics as per the neutropenic sepsis
regimen
• Patients that are too unwell to be managed at home e.g. diarrhea or vomiting requiring intravenous
fluids, hypoxia, and severe uncontrolled pain.
• Patients with clinic evidence of CNS disease at presentation (neurological deficit) and patients who
have blasts in their CSF
These patients should be treated as per regimen B unless too unwell to treat (at the discretion of the
specialist)
Relapse and Non-Responders
These patients should be given palliative treatment only e.g. dexamethasone (discuss with the specialist)
Considerations for the future
Asparaginase could be added to the regimen if it becomes more readily available locally small doses of iv
cytosine could be added to regimen B induction if this becomes more readily available locally
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
104
9.9.0 SOME COMMON DRUGS USED IN PAEDIATRIC ONCOLOGY PATIENTS • IV Cyclophosphamide dose over 30mins in 100mls fluid(N/S)
• IV vincristine dose bolus
• IV Etoposide dose in 100ml N/S over one hour
• IV Doxorubicin (Adriamycin) dose in 250mls over 6 hrs.
• IV Carboplatin dose in 150ml 5% dextrose over one hour.
• IV Actinomycin D dose bolus
• IV Bleomycin dose over 30 mins in N/S
• IV Dacarbazine bolus over 15mins
• IT Methotrexate is age dependent:
<1yr= 6 mg
1-< 2yr = 8mg
2-< 3yr = 10mg
>3yr = 12.5mg
NOTE
• Vincristine maximum dose 2mg
• Actinomycin D maximum dose 2mg
• Infants under 1 year and children with weight < 10kg give two thirds of calculated doses of
chemotherapy.
• Do not give actinomycin D/doxorubicin within two weeks of radiotherapy.
EXTRAVASATION OF DRUGS
• Vincristine, Actinomycin D, doxorubicin.
• Local injection of hydrocortisone- infiltrate of site as much as possible.
• For vincristine, immediate application of warm compress will increase circulation and encourage
absorption of drug from tissues to blood stream.
• After one hour, a cold compress may relieve swelling and inflammation.
• Early application of ice pack for other drugs.
• Where skin damage is extensive, early referral to plastic surgeon.
Antiemetic
• IV Metoclopromide 100 micrograms/kg 30 mins before chemotherapy, may repeat after 6hrs.
• IV/ oral dexamethasone 1-4mg 8 hourly.
• IV Granisetron 40 mcg/kg before chemotherapy.
Sedation
• IV Midazolam 100mcg/kg but doses up to 300mcg/kg may be used.
Analgesia
Mild pain- -paracetamol
Moderate pain -dihydrocodeine ± paracetamol
Severe pain - oral morphine
Opiates may cause constipation so consider stool softeners.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
105
10.0 PAEDIATRIC EMERGENCIES 10.1.0 HYPOGLYCAEMIA
1. DEFINITION
Surrogate marker for harmfully low levels of energy in the central nervous system.
Blood glucose ≤2.0mmol/L (serum/plasma glucose ≤2.5mmol/L) or BM stix ≤ 3.0mmol/L
2. COMMON CAUSES
Metabolic
Ketotic hypoglycaemia –after short period of starvation in young children
Infections
Severe malaria
Septicaemia in young children/severe malnutrition
Liver disease
Reye syndrome
Acute liver failure
Hepatic failure/dysfunction
Inborn errors of metabolism
Glycogen storage disorders
Galactosaemia
Hereditary fructose intolerance
Poisoning
Alcohol
Aspirin
Hormonal
Hormone excess
Insulin -administered insulin in diabetes or poisoning
-Drug (e.g. Quinine) induced
-Insulinoma
-Beckwith syndrome
Hormone deficiency
Growth hormone -Growth hormone deficiency
ACTH -Panhypopituitarism
Cortisol -Addison disease
-Congenital adrenal hyperplasia
Miscellaneous:
Malaria
Diarrhea
Malnutrition
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
106
3. CLINICAL FEATURES
• Sweating
• Pallor
• CNS signs of irritability, headache, seizures and coma
4. DIAGNOSIS / ASSESSMENT
• High index of suspicion as symptoms can be subtle
• Do blood glucose in any child who:
-appears seriously ill
-has a prolong seizures
-has altered sensorium
5. TREATMENT / MANAGEMENT
a. BOLUS
• 5ml/kg IV bolus of 10% Dextrose over 5 – 10 minutes ( or mini bolus of 2ml/Kg for Neonates)
• Rapid bolus of 5ml/kg of 10% Dextrose or
o 2ml/kg of 25% Dextrose may be given per rectum (as retain enema) or
o per gastric tube (if able to tolerate enteric feeding).
• If child is conscious, give 50ml 10% sugar solution or start feeding immediately.
b. CONTINUOUS INFUSION
• 10% (5-12.5%) Dextrose containing fluid at maintenance rate (or rate of 4-8mg/kg/min)
• Repeat blood sugar every 30mins until blood sugar is stable, then continue blood sugar monitoring
at less frequent interval till patient is stable
• Keep blood sugar between 4-12mmol/L.
• If blood sugar is < 4mmol/L, repeat a bolus (or mini-bolus 2ml/Kg) of glucose and review infusion
rate. DO NOT over infuse (i.e. Avoid fluid overload).
• Oral / gastric tube feeding should be commenced as soon as child is able to tolerate oral feeds or
tube feeding.
*INTRAMUSCULAR (IM) THERAPY (use only in place of bolus dextrose)
Glucagon @ 0.03/kg IM/SC stat (max. dose 1mg)
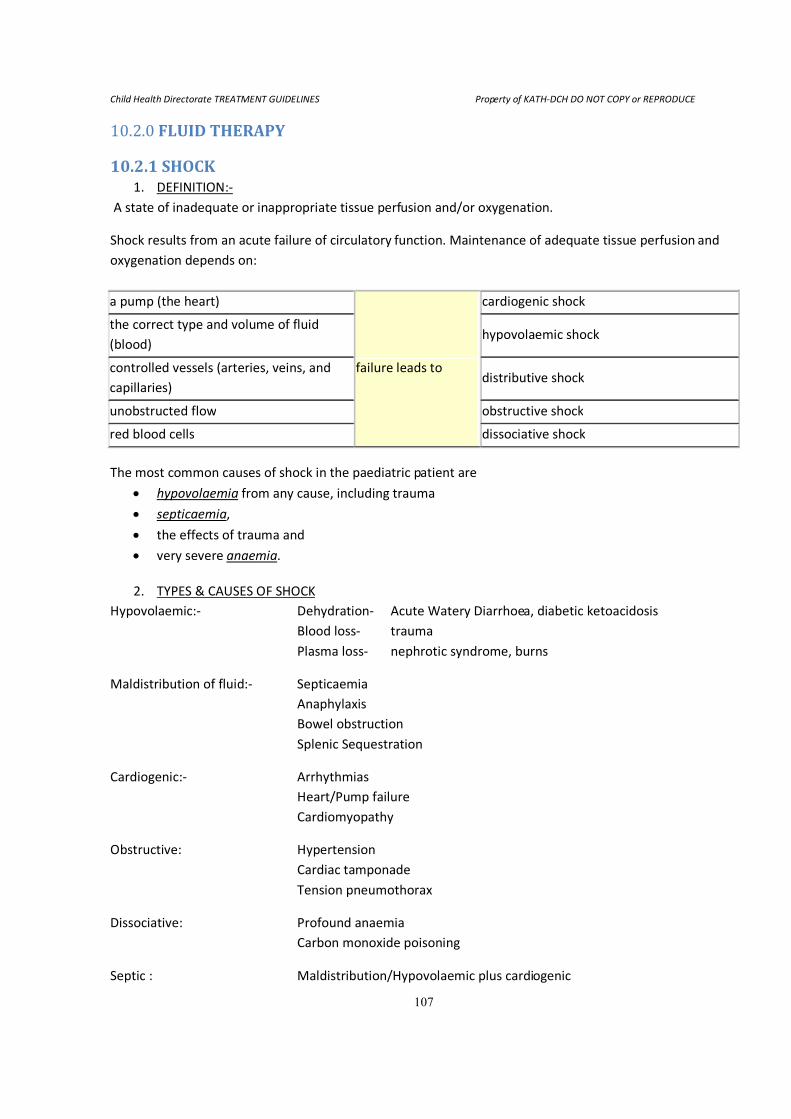
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
107
10.2.0 FLUID THERAPY
10.2.1 SHOCK 1. DEFINITION:-
A state of inadequate or inappropriate tissue perfusion and/or oxygenation.
Shock results from an acute failure of circulatory function. Maintenance of adequate tissue perfusion and
oxygenation depends on:
a pump (the heart)
failure leads to
cardiogenic shock
the correct type and volume of fluid
(blood) hypovolaemic shock
controlled vessels (arteries, veins, and
capillaries) distributive shock
unobstructed flow obstructive shock
red blood cells dissociative shock
The most common causes of shock in the paediatric patient are
• hypovolaemia from any cause, including trauma
• septicaemia,
• the effects of trauma and
• very severe anaemia.
2. TYPES & CAUSES OF SHOCK
Hypovolaemic:- Dehydration- Acute Watery Diarrhoea, diabetic ketoacidosis
Blood loss- trauma
Plasma loss- nephrotic syndrome, burns
Maldistribution of fluid:- Septicaemia
Anaphylaxis
Bowel obstruction
Splenic Sequestration
Cardiogenic:- Arrhythmias
Heart/Pump failure
Cardiomyopathy
Obstructive: Hypertension
Cardiac tamponade
Tension pneumothorax
Dissociative: Profound anaemia
Carbon monoxide poisoning
Septic : Maldistribution/Hypovolaemic plus cardiogenic
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
108
3. CLINICAL SIGNS:-
Early (compensated) Late (decompensated)
Tachycardia Acidotic (Kussmaul) breathing
Tachypnoea Hypotension (SBP < [70+2[age in yrs]])
Decreased skin turgor Confusion/depressed consciousness
Delayed capillary refill (>4secs) Absent urine output
Mottled pale, cold skin
Core-peripheral temperature gap (>4oC)
Decreased urinary output
Diagnostic pointers
• A history of vomiting and/or diarrhoea points to fluid loss either externally (eg gastroenteritis) or
into the abdomen (e.g. volvulus, intussuception, early stages of gastroenteritis)
• Fever or a rash points to septicaemia
• Urticaria, angio-neurotic oedema or a history of allergen exposure points to anaphylaxis
• Cyanosis unresponsive to oxygen or signs of heart failure in a baby under 4 weeks points to duct-
dependent congenital heart disease
• Signs of heart failure in an older infant or child may points to severe anaemia (usually with severe
pallor) or cardiomyopathy
• A history of sickle cell disease or diarrhoeal illness and low haemoglobin points to acute haemolysis
• A history of major trauma points to blood loss, and more rarely, tension pneumothorax,
haemothorax, cardiac tamponade or spinal cord transection
• Severe tachycardia or signs of heart failure point to an arrhythmia or to a cardiomyopathy
• A history of polyuria, sighing, respirations and a very high blood glucose points to diabetes (see
Diabetic ketoacidosis)
• A history of drug ingestion points to poisoning
4. MANAGEMENT PRIORITIES:-
• Fluid resuscitation (key element to the successful treatment of shock)
• Ensure adequate Airway and Breathing. Give O2, support ventilation if needed.
• Rapid restoration of the intravascular circulating volume is most critical.
• Start 20ml/kg of 0.9%Normal Saline / Ringers Lactate over ≤20mins (may modify if myocardial
dysfunction likely).
• Reassess. If no improvement, repeat 0.9%Normal Saline / Ringers Lactate @ 10ml/kg in ≤10-15mins
(up to max. 60ml/kg), there after consider inotropes with further fluid therapy
• Reassess. If replacement requires >40ml/kg or if acute blood loss, consider haemacell, plasma (FFP),
or red blood cells (packed or whole) @10ml/kg.
• If cardiogenic etiology is suspected, fluid resuscitation may worsen clinical status.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
109
10.2.2 NORMAL MAINTENNANCE FLUIDS i) Age <6 months - 100 -120ml/kg/day.
ii) Age >6 months -for first 10kg, 100ml/kg/day
-for next 10kg, 50ml/kg/day
-every additional weight >20kg, 20ml/kg/day
Electrolyte mmol/100ml of water
Sodium Na+
Potassium K+
Chloride Cl-
3
2
2
e.g. 25kg girl would need (10 ×100ml)+(10 ×50ml)+(5 × 20) = 1700ml/day of fluid
(17×3)mmol of Na+ = 51mmol of Na
+/day
(17×2)mmol of K+
= 34mmol of K+/day
(17×2)mmol of Cl-
= 34mmol of Cl-/day
TYPES OF FLUIDS:-
a. Crystalloid solutions
• Half strength Darrow’s solution in 2.5-5% Dextrose
Frequently used for rehydration & maintenance in infants & the malnourished.
• Ringers lactate solution
Used for rehydration & volume expansion.
• 0.9% Normal saline solution
Used for rehydration & volume expansion.
• 5-10% Dextrose in 0.9% Normal saline solution.
Used as maintenance solution.
• 2.5-10% Dextrose in Ringers lactate solution.
Used frequently for rehydration & as maintenance solution
10% dextrose in 1/5 strength Normal Saline (0.18% Saline)
b. Colloid solutions-( Haemaccel, Albumin,Plasma etc.)
Used for volume expansion
c. Blood
• Packed cells (pRBC’s)
Used for chronic anaemia
• Whole blood
Used for hypovolaemic shock due to haemorrhage or sequestration
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
110
NOTE:
• DO NOT give fluids containing no sodium to patients with meningitis unless you are just keeping the
line open.
• REMEMBER to restrict to 70% maintenance in meningitis after correction of intravascular volume
deficit.
• NEVER give only Dextrose for more than 24hrs. Change to, or alternate with crystalloid.
FAST REHYDRATION
Give rehydration requirement over 4-6hrs followed by the day’s maintenance given over the next 20hrs
Fast rehydration is most appropriate if child is in shock.
Fast rehydration is contra-indicated in:-
Severe malnutrition
Hypernatraemia
Hyperosmolar state (e.g. hyperglycaemic crisis/coma)
SLOW REHYDRATION
Add rehydration requirement to child’s maintenance for 24-36hrs and give the total amount of fluid
gradually over 24-36hrs.
Slow rehydration is most suitable in:-
Severe malnutrition
Hypernatraemia
Hyperosmolar state (e.g. hyperglycaemic crisis/coma)
NOTE:
• In either fast or slow rehydration, correct shock with fast/bolus IV fluid @ 15-20ml/kg over 10-20mins
[preferably ≤ 30mins] (15ml /kg over 60mins for the SEVERELY malnourished child).
• May repeat IV bolus @ 10ml/kg in ≤ 15 min (15ml/kg/60min in PEM) till peripheral pulse palpable (or up
to 60 – 80ml/kg).
• Consider inotropes in septic shock( after adequate hydration) or Cardiogenic shock
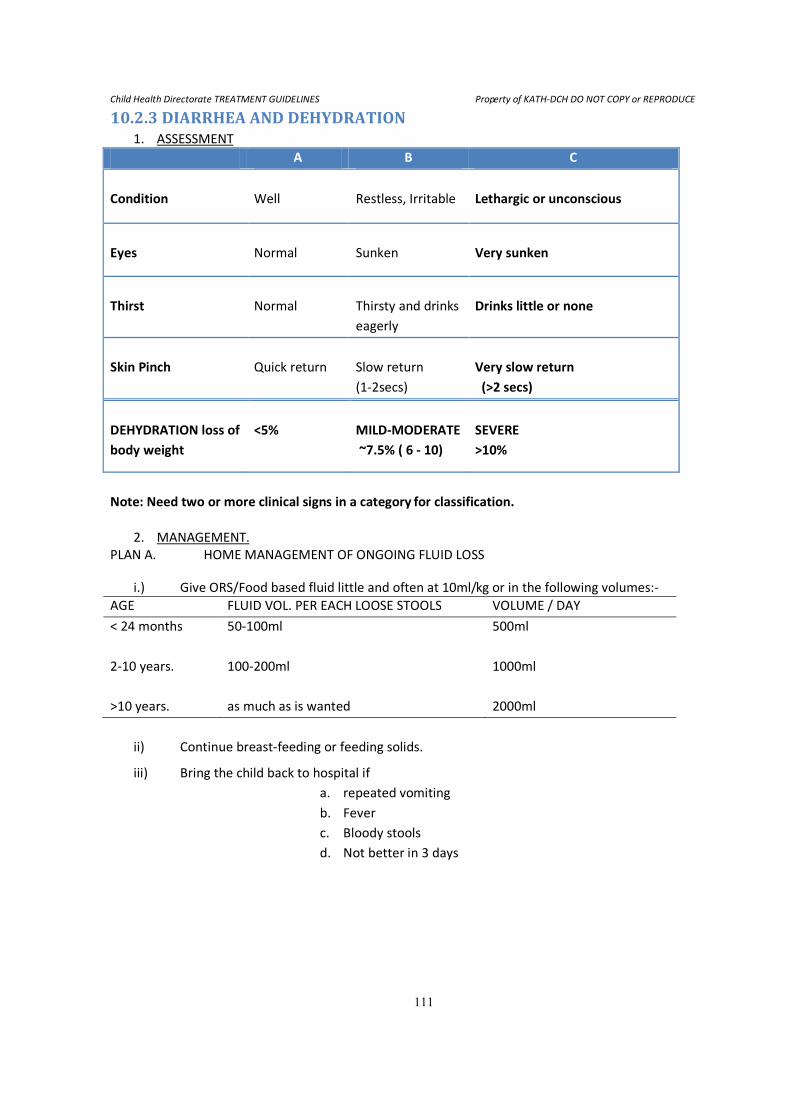
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
111
10.2.3 DIARRHEA AND DEHYDRATION 1. ASSESSMENT
A B C
Condition
Well
Restless, Irritable
Lethargic or unconscious
Eyes
Normal
Sunken
Very sunken
Thirst
Normal
Thirsty and drinks
eagerly
Drinks little or none
Skin Pinch
Quick return
Slow return
(1-2secs)
Very slow return
(>2 secs)
DEHYDRATION loss of
body weight
<5%
MILD-MODERATE
~7.5% ( 6 - 10)
SEVERE
>10%
Note: Need two or more clinical signs in a category for classification.
2. MANAGEMENT.
PLAN A. HOME MANAGEMENT OF ONGOING FLUID LOSS
i.) Give ORS/Food based fluid little and often at 10ml/kg or in the following volumes:-
AGE FLUID VOL. PER EACH LOOSE STOOLS VOLUME / DAY
< 24 months
2-10 years.
>10 years.
50-100ml
100-200ml
as much as is wanted
500ml
1000ml
2000ml
ii) Continue breast-feeding or feeding solids.
iii) Bring the child back to hospital if
a. repeated vomiting
b. Fever
c. Bloody stools
d. Not better in 3 days
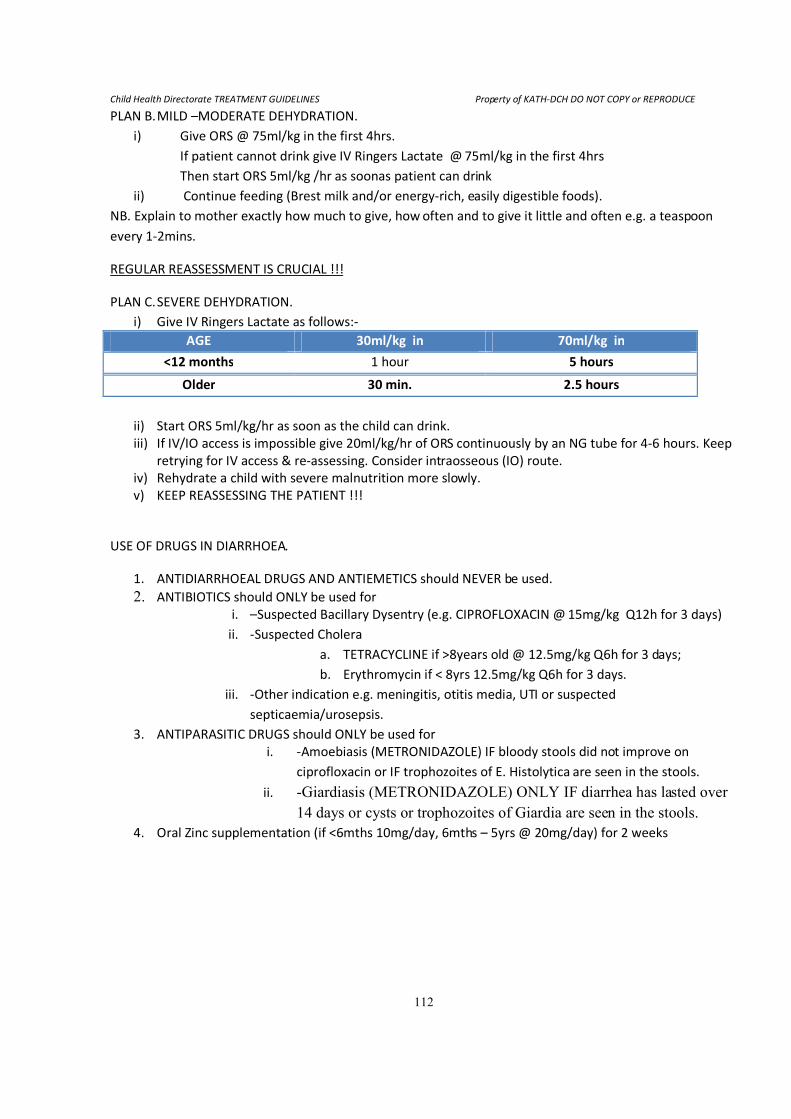
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
112
PLAN B. MILD –MODERATE DEHYDRATION.
i) Give ORS @ 75ml/kg in the first 4hrs.
If patient cannot drink give IV Ringers Lactate @ 75ml/kg in the first 4hrs
Then start ORS 5ml/kg /hr as soonas patient can drink
ii) Continue feeding (Brest milk and/or energy-rich, easily digestible foods).
NB. Explain to mother exactly how much to give, how often and to give it little and often e.g. a teaspoon
every 1-2mins.
REGULAR REASSESSMENT IS CRUCIAL !!!
PLAN C. SEVERE DEHYDRATION.
i) Give IV Ringers Lactate as follows:-
AGE 30ml/kg in 70ml/kg in
<12 months 1 hour 5 hours
Older 30 min. 2.5 hours
ii) Start ORS 5ml/kg/hr as soon as the child can drink.
iii) If IV/IO access is impossible give 20ml/kg/hr of ORS continuously by an NG tube for 4-6 hours. Keep
retrying for IV access & re-assessing. Consider intraosseous (IO) route.
iv) Rehydrate a child with severe malnutrition more slowly.
v) KEEP REASSESSING THE PATIENT !!!
USE OF DRUGS IN DIARRHOEA.
1. ANTIDIARRHOEAL DRUGS AND ANTIEMETICS should NEVER be used.
2. ANTIBIOTICS should ONLY be used for i. –Suspected Bacillary Dysentry (e.g. CIPROFLOXACIN @ 15mg/kg Q12h for 3 days)
ii. -Suspected Cholera
a. TETRACYCLINE if >8years old @ 12.5mg/kg Q6h for 3 days;
b. Erythromycin if < 8yrs 12.5mg/kg Q6h for 3 days.
iii. -Other indication e.g. meningitis, otitis media, UTI or suspected
septicaemia/urosepsis.
3. ANTIPARASITIC DRUGS should ONLY be used for
i. -Amoebiasis (METRONIDAZOLE) IF bloody stools did not improve on
ciprofloxacin or IF trophozoites of E. Histolytica are seen in the stools.
ii. -Giardiasis (METRONIDAZOLE) ONLY IF diarrhea has lasted over
14 days or cysts or trophozoites of Giardia are seen in the stools.
4. Oral Zinc supplementation (if <6mths 10mg/day, 6mths – 5yrs @ 20mg/day) for 2 weeks
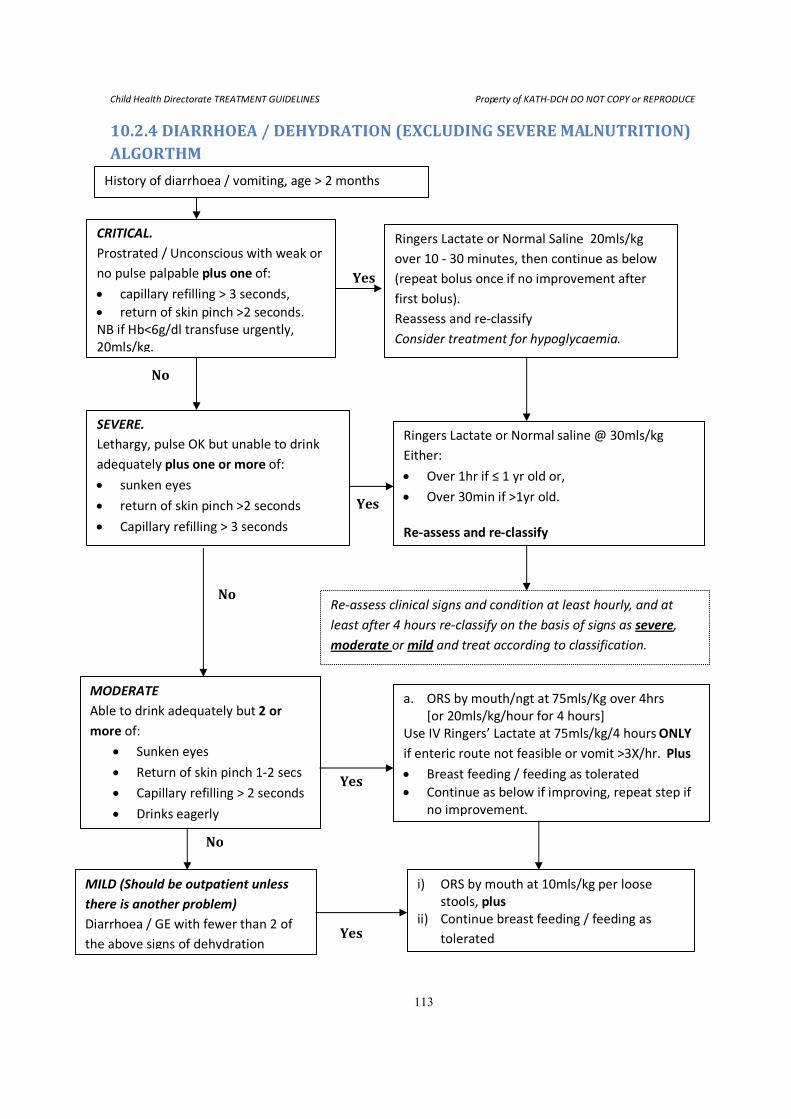
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
113
10.2.4 DIARRHOEA / DEHYDRATION (EXCLUDING SEVERE MALNUTRITION) ALGORTHM
History of diarrhoea / vomiting, age > 2 months
CRITICAL.
Prostrated / Unconscious with weak or
no pulse palpable plus one of:
• capillary refilling > 3 seconds,
• return of skin pinch >2 seconds.
NB if Hb<6g/dl transfuse urgently,
20mls/kg.
Ringers Lactate or Normal Saline 20mls/kg
over 10 - 30 minutes, then continue as below
(repeat bolus once if no improvement after
first bolus).
Reassess and re-classify
Consider treatment for hypoglycaemia.
SEVERE.
Lethargy, pulse OK but unable to drink
adequately plus one or more of:
• sunken eyes
• return of skin pinch >2 seconds
• Capillary refilling > 3 seconds
Ringers Lactate or Normal saline @ 30mls/kg
Either:
• Over 1hr if ≤ 1 yr old or,
• Over 30min if >1yr old.
Re-assess and re-classify
Re-assess clinical signs and condition at least hourly, and at
least after 4 hours re-classify on the basis of signs as severe,
moderate or mild and treat according to classification.
MODERATE
Able to drink adequately but 2 or
more of:
• Sunken eyes
• Return of skin pinch 1-2 secs
• Capillary refilling > 2 seconds
• Drinks eagerly
a. ORS by mouth/ngt at 75mls/Kg over 4hrs
[or 20mls/kg/hour for 4 hours]
Use IV Ringers’ Lactate at 75mls/kg/4 hours ONLY
if enteric route not feasible or vomit >3X/hr. Plus
• Breast feeding / feeding as tolerated
• Continue as below if improving, repeat step if
no improvement.
MILD (Should be outpatient unless
there is another problem)
Diarrhoea / GE with fewer than 2 of
the above signs of dehydration
i) ORS by mouth at 10mls/kg per loose
stools, plus
ii) Continue breast feeding / feeding as
tolerated Yes
Yes
No
Yes
No
Yes
No
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
114
11.0 RENAL DISORDERS 11.1.0 GENERAL GUIDE FOR ALL RENAL CASES
• Efforts should be made to arrive at a definitive diagnosis irrespective of the Referring/Admitting
diagnosis.
• All cases should have the renal data (enclosed in patient’s folder) filled in whole by the attending
doctor (i.e. the admission data, laboratory data, and discharge data).
• BP should always be re-checked on admission using the appropriate cuff size and must be “plotted”
on the appropriate BP centile chart for height, age, and sex.
• Body weight should be measured every other day.
• Urine output should be measured daily over 24 hours and recorded in mls/kg/hour.
• All cases should have a repeat dipstick urinalysis on the bedside by the attending doctor (at booking
to the ward/unit)
• All cases should have culture of an appropriately collected urine sample done on admission.
• The under-listed investigations should be done ROUTINELY for all cases:
I. Blood
• Full Blood Count (haematology)
• Chemistry – BUE, Creatinine, Albumin & Total Protein, Cholesterol,
Ca2+
, Phosphorus, and Alkaline Phosphatase
II. Urine
• Dipstick + microscopy
• C/S
III. Stool R/E
IV. Ultrasonography scan of Kidneys and urinary tract
V. Other Investigations as may be necessary
• All cases should have their GFR estimated using the Schwartz formula for children:
GFR(ml/min/1.73m2) = K X height (cm)
Serum Creatinine (µmol/L)
Where K is:
40 for neonates and infants younger than 1 yr,
49 for children 1 – 12 years
49 for adolescent females, 13 – 21 years
60 for adolescent males, 13 – 21 years
Minimum urine output: >1ml/Kg/hour in children
>2ml/Kg/hour in infants
• Appropriate dietary advice should be given in all cases (see overleaf)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
115
11.2.0 DIETARY ADVICE FOR RENAL CASE
A) For all cases in Renal Failure:
• Avoid Potassium-rich food like banana, coconut, and tomatoes
• Avoid Phosphorus-rich diet like milk, and diary products
• Limit 24-hour fluid intake (water and all other drinks including fluid diet) to insensible loss
(500 mls/m2 ) + Previous day’s output
• Protein intake should not exceed 2g/kg/day
• Promote high Caloric-diet
• Avoid nephrotoxic drugs like Gentamycin
• Adjust doses of all drugs as appropriate
• Prescribe low salt diet
• Do Renal function test weekly (urea, creatinine and electrolytes, including serum calcium
and phosphate levels)
B) For Grossly edematous patients including Nephrotic Syndrome:
• Limit fluid intake to insensible loss (500 mls/m2) + Previous day’s output
• Prescribe low salt diet
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
116
11.3.0 NEPHRITIC SYNDROME (ACUTE GLOMERULONEPHRITIS)
11.3.1 CLINICAL DEFINITION/CRITERIA Definition
For the purpose of this protocol, acute nephritic syndrome shall be defined by acute onset of any
combination of:
1. haematuria (pink or brownish urine)
2. oliguria
3. oedema
4. hypertension
5. azotaemia
6. red cells and red cell cast and/or granular cast on urine microscopy
7. moderate proteinuria
Common causes include:
• postinfectious (Strep & Staph)
• IgA nephropthy
• Henoch-Scholein syndrome
• Membranous proliferative
• SLE
• ANCA and anti-glomerular basement membrane disease
All cases should be assumed to be of postinfectious aetiology unless proven otherwise
11.3.2 MANAGEMENT GUIDELINES FOR NEPHRITIC SYNDROME (AGN)
.Routine laboratory tests
1. Urine dipstick for protein, blood, leucocyte & nitrite
2. Urine microscopy, C & S
3. Full blood count
4. Blood chemistry (Na, K, Cl, urea, creatinine, albumin, total protein, cholesterol, Ca, Mg, inorg PO4)
5. HBsAg
6. VDRL
7. HIV (only after counselling)
8. CXR for any evidence of cardiomegaly and pulmonary oedema
Other laboratory tests e.g. ANA, anti-dsDNA, ANCA, anti GBM may be requested on selected cases
Management Principles
• Control hypertension with appropriate anti-hypertensives, preferably amlodipine (5mg or 10 mg)
• Give diuretics (frusemide) to control the fluid overload
• Reinforce dietary management (see above)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
117
Management
1. Daily weight
2. Daily fluid intake versus output chart
3. Strict fluid balance (intake to strictly match previous day’s output + insensible loss –use 300ml/m2)
4. Strict salt restriction including all known salt-rich food
5. Amoxycillin 15mg/kg/dose 8 hourly for 5-7 days
6. Lasix 1mg/kg/dose 8-24 hourly. IV lasix 2-4mg/kg slowly over 5-10 mins if in pulmonary oedema
7. Dialysis (see indications below)
Indications for dialysis
1. Hyperkalaemia not responding to medical treatment
2. Pulmonary oedema unresponsive high dose IV lasix
3. Rapidly Progressive Renal Functional Impairment
4. Anuria not responding to high dose IV lasix
11.3.3 COMPLICATIONS & THEIR MANAGEMENT
1. Stage 2 Hypertension (BP > [99th percentile for age, sex & height + 5 mmHg])
Note: Stage 1 hypertension usually can be controlled on diuretics alone
• Amlodipine 0.2mg/kg/day. For younger children who are fast metabolisers, the dose could be
given 12 hourly
• Atenelol 1-2mg/kg/12-24hourly
• Continue diuretic
2. Hypertensive encephalopathy
• IV labetalol (continuos IV infusion @ 0.5mg/kg/hr, adjusted interval > 15min; max 3mg/kg/hr) or
IV hydrallazine 0.1-0.2mg/kg q30mins-60mins. These should be titrated to achieve a gradual
and gentle fall in BP by 1/3 in the 1st 24 hrs, 1/3 in the next 24 hrs and 1/3 in the final 24 hours
• IV Lasix 1-2mg/kg
• IV mannitol 0.25-0.5mg/kg over 30 mins
• Commence oral antihypertensives as soon as stable to take. Preferably use short acting drugs
like Nifedipine
3. Pulmonary oedema
• Confirm with urgent CXR
• Prop up and give O2
• IV Lasix (high dose) 4-5mg/kg slowly over5-10mins
• Acute dialysis
4. Congestive cardiac failure
• Manage as per Pulmonary oedema
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
118
5. Hyperkalaemia
• Put on cardiac monitor to see ECG changes
• Commence nebulised salbutamol 5mg 2-hourly whilst serial levels of potassium are determined
• Kayexalate 0.5-1g 6-hourly (per rectum or orally)
• Soluble insulin in 10% Dextrose to run at 1units of insulin/5g of dextrose over 1 hour whilst RBS
is checked frequently.
• Dialysis if the above Rx fail
6. Rapidly Progressive Renal Functional Impairment
• Defined by escalating levels of BUN, Cr ± decreasing urine output
• All cases should undergo emergency renal biopsy
• Commence IV methyl prednisolone 10mg/kg/day x 5
• Consider dialysis
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
119
11.4.0 NEPHROTIC SYNDROME
11.4.1 CLINICAL DEFINITION/CRITERIA FOR NEPHROTIC SYNDROME: Definition
In this protocol, nephrotic syndrome (NS) shall be defined as triad of
• Urinary protein of 3+ or more on dipstick, or protein/creatinine ratio of >0.2 (g/l/mmol/l) of early
morning urine
• Hypoalbuminaemia of < 25g/l
• Clinical oedema
Hypercholesterolaemia is invariably present but not needed for diagnosis
11.4.2 MANAGEMENT GUIDELINES FOR NEPHROTIC SYNDROME
Routine laboratory tests
The following tests should be done in ALL confirmed cases of NS
1. Blood chemistry (Na, K, Cl, urea, creatinine, albumin, total protein, cholesterol, Ca, Mg, inorg PO4)
2. Full blood count + PCV
3. EMU protein/creatinine ratio
4. Urine electrolytes + fractional excretion of sodium
5. Urine dipstick for leucocyte & nitrite. If either or both is +ve, do urine C&S
6. Blood for HBsAg
7. Blood for VDRL
8. HIV (only after counselling)
9. CXR for any evidence of PTB
10. Mantoux test
11. Stool for strongyloides and other parasites
Other laboratory tests e.g. ANA, anti-dsDNA, ASO & anti-DNASe titres may be requested on selected cases
Management
A) Adjunctive/Supportive therapy
1. Daily weight
2. daily fluid output chart
3. If urine output is low from history or from output chart, then limit fluid intake to match previous
day’s output + insensible losses (300-500ml/m2)
4. Low salt diet
5. Amiloride (alone or as combined tablet with thiazide e.g moduretic) ± lasix if grossly oedematous.
Hypovolaemia should always be ruled out before starting diuretics. Discontinue all diuretics with
complete resolution of oedema
6. Pen V prophylaxis if grossly oedematous
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
120
7. Albumin infusion (1g/kg/day) or plasma (10ml/kg/day) may be prescribed for very severe oedema
to run for 3-4 hours. Either should be given with IV lasix 1mg/kg half-way into infusion. Repeat at
end of infusion.
Note: ACEI & statins should NOT be prescribed routinely for acute cases.
They should be reserved for chronic nephrotics (see definition below) and SRNS.
B) Corticosteroids
Steroid shall be the cornerstone of treatment for all cases of confirmed nephrotics but their use is NEVER an
emergency. They should only be started after the diagnosis has been confirmed and all potential infections
have been ruled out (see under routine laboratory tests). Also, make sure that blood pressure is normalised
with antihypertensives before commencing on steroids.
Induction of remission
Prednisolone 60mg/m2/day for 28 days per os.
In overtly oedematous cases in which absorption from GI may be suspect , IV methylprednisolone
10mg/kg/day may be given for the initial 3 days.
If proteinuric at end of 28 days, declare as steroid resistant and prepare for renal biopsy (see subsequent
treatment below).
Steroid sensitive
If steroid responsive/sensitive (i.e. –ve or trace proteinuria on dipstick for 3 consecutive days within the first
28 days of steroids), document time duration at which response occurred. However, for the purpose of this
protocol, all steroid responsive cases should continue the high dose prednisolone (60mg/m2/day) for 6
complete weeks.
Maintainance of remission
Prednisolone 40mg/kg/day on alternate days for 6 complete weeks, then taper over 2 weeks by 25%
decrement every 3rd
day.
The above treatment protocol shall apply to all steroid sensitive cases who relapse for the first 2 instances.
STEROID RESISTANT NEPHROTIC SYNDROME (SRNS)
For the purpose of this protocol, steroid resistance shall be defined as 1+ or more of dipstick proteinuria
after 28 days of 60mg/m2/day of prednisolone.
For all such cases, the following actions should be taken:
1. Quantify proteinuria by EMU protein/creatinine ration. This will differentiate partial response
(pro/creat of < 0.2) from incomplete response (pro/creat of > 0.2)
2. Arrange for renal biopsy (see pre-biopsy preparation below)
3. Continue high dose prednisolone (60mg/m2/day) while waiting for histology report.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
121
For all SRNS, high dose prednisolone (60mg/m2/day) may be continued for 12 weeks after which
40mg/M2
given on alternate days for another 12 weeks may be given. Thereafter, wean off
prednisolone over 2 weeks (decrease by 25% each 3rd
day) and reinforce adjunctive therapy.
4. Adjunctive therapy shall be reinforced and shall consists of the following:
• Low salt diet
• Amiloride (alone or as combined tablet with thiazide e.g moduretic) if grossly oedematous.
Discontinue all diuretics with complete resolution of oedema
• Pen V prophylaxis if grossly oedematous
• Albumin infusion (1g/kg/day) or plasma (10ml/kg/day) may be prescribed for very severe
oedema to run for 3-4 hours. Either should be given with IV lasix 1mg/kg half-way into infusion.
Repeat at end of infusion.
• ACEI ± ARB
• Statin
• Blood pressure control
• Adequate nutrition
• Aspirin (for mesangial proliferative, membranous and membranous proliferative –see below)
Further immunosuppressive therapy will to be guided by biopsy report as follows:
1. Minimal change
Continue high dose prednisolone for 6 complete weeks.
Responsive to 6 weeks steroid
If responds at end of 6 weeks, declare as late steroid resistance and give maintenance prednisolone
40mg/m2/day for 12 complete weeks and wean off over 2 weeks.
No response after 6 weeks steroid: give cyclophosphamide
If no response at end of 6 weeks, start 2nd
line agent –cyclophosphamide –for 3 months. Continued the
steroid while on the cyclophosphamide.
Responds to cyclophosphamide
If response to cyclophosphamide, give maintenance prednisolone 40mg/m2/alternate day for another 12
weeks and then wean off over 2 weeks.
No response to cyclophosphamide; give cyclosporin
Give 3rd
line agent –cyclosporin – for 1–2 years. At this juncture, side effects of steroid may be problematic.
If so, the dose of prednisolone may be decreased to 40mg/m2/day while on cyclosporin.
Responds to cyclosporin
If responds to cyclosporin, wean off steroids and continue cyclosporine for 1-2 yrs.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
122
No response to cyclosporin
Declare treatment resistant. Stop all immunosuppressants and emphasise adjunctive therapy.
Prepare for another biopsy.
Mesangial proliferative
Treat as steroid resistant minimal change but add aspirin to adjunctive therapy
2. Focal segmental glomerulosclerosis
Continue high dose prednisolone 60mg/m2/day for 3 complete months and maintenance dose
40mg/m2/alternate day for another 3 months.
No response to 6 months prednisolone
Give cyclophosphamide for 3 months. Here, the steroid dose should be tapered to low tolerable dose on
alternate days.
No response to cyclophosmamide
Give cyclosporin for 2 years. If responds to cyclosporin, wean off steroids and continue cyclosporin
Prepare for renal biopsy after 2 years on cyclosporin
3. Membranoproliferative/Mesangiocapillary
1. Adjunctive therapy as cornerstone of treatment
2. Aspirin
3. Prednisolone on alternate days for 2 years ± cytotoxics
4. Membranous
Always rule out secondary causes in children (e.g. HBV, syphilis, SLE, drug exposure like gold & Hg).
1. High rate of spontaneous remission in the 1st
12 months
2. Adjunctive therapy cornerstone in treatment
3. Aspirin.
4. Statins.
5. ACEI, ARB to control proteinuria
6. Immunosuppressants are reserved for caes that manifest nephrotic proteinuria. NEVER give
steroids alone!
• Medrol 10mg/kg/day on day 1-3 followed by prednisone to complete 1st month. Alternate
monthly with cyclophosphamide for total of 6 months of combination therapy
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
123
11.4.3 SECONDARY CAUSES OF NEPHROTIC SYNDROME All should undergo renal biopsy
HIV associated nephrotic syndrome
1. ARVs shall be cornerstone of treatment
2. Adjunctive therapy
Hepatitis B Virus associated nephrotic syndrome
1. No immunosuppresives unless rapidly progressive glomerulonephritis. Risk of converting stable
chronic persistent hepatitis to chronic active hepatitis if immunosuppressant are given without prior
antiviral therapy.
2. Adjunctive therapy shall be cornerstone of therapy
3. Antiviral therapy (Interferon α, lamivudine, tenofovir) if affordable.
Watch renal function closely if tenofovir is given due to potential nephrotoxicity.
Syphillis
• Pen G for 14 days
• Adjunctive therapy
• Look for contact and treat also
SLE (+ve ANA & anti-dsDNA) associated nephrotic syndrome (i.e. WHO class V)
1. Remission shall be induced as follows:
• IV medrol 10mg/kg/day x 3 to be followed by prednisolone 1mg/kg/day x 4 weeks, then
prednisolone 0.75mg/kg/day x 4 weeks. Thereafter, taper prednisolone (if disease is well controlled)
for long-term therapy
• IV cyclophosphamide 500-1000mg/m2 monthly x 6
2. Maintenance therapy shall consist of:
• Azathioprine 2mg/kg/day in the long-term till in remission for at least 1 year
• Low dose prednisolone 0.5mg/kg/alternate days to control extra renal disease
3. Extra renal disease (musculoskeletal, skin, serosa) shall be controlled with NSAIDs, chloroquine and
the low dose prednisolone.
4. Aspirin shall be given if anticardiolipin/antiphospholipid positive
Note: Disease activity shall be monitored both by clinical symptoms/signs and laboratory tests.
Laboratory tests:
1. Urine dipstick and microscopy
2. ESR
3. Anti nuclear antibody (ANA) and anti double strand DNA titres
Exacerbation of disease activity shall be treated with pulse medrol and high dose prednisolone ± IV
cyclophosphamide
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
124
11.4.4 COMPLICATIONS OF NEPHROTIC SYNDROME & THEIR MANAGEMENT 1. Hypovalaemia
Suspect if:
• complaint of abdominal pain without tenderness
• history of diarrhoea and/or vomiting
• oliguria
• urine Na <10mmol/L or FENa < 1%
2. Spontaneous bacterial peritonitis
• Do blood and peritoneal fluid C&S
• Start IV Penicillin + Gentamycin x 7 days
3. Cellulitis
• Do pus swab if there are open discharging wound
• Start on Co-Amoxiclav for 7 days OR IV Cefuroxime if too ill.
4. Venous thrombosis
• Suspect if asymmetrical limb swelling, gross haematuria in “pur”nephritic (Renal vein
thrombosis)
• Confirm with Doppler ultrasound scan
• Treat with heparin and subsequently warfarin
Definitions in Nephrosis
• Remission- urine albustix –ve or trace for 3 consecutive days
• Relapse –urine albustix ≥ 2+ (± oedema)having achieved remission previously
• Frequently relapsing -2 or more relapse in the 1st
6mths after presentation or 4 relapses
within any 12 mths period
• Steroid dependant –relapse whilst on steroid therapy or within 14 days of
discontinuation of steroid
• Steroid resistant –failure of proteinuria to resolve ff 28 days of Pred at dose of
60mg/m2/day
• Congenital Nephrotic –NS occuring in 1st
3 months of life
• Infantile Nephrotic –NS occuring b/n 3 mths -1 yr of life
Treatment of Relapse
• For infrequent relapses (≤ 2X in 6 mths or < 4 in a yr)) the same regimen as for the initial
presentation is recommended.
• For frequent relapses (>2X within 6 mths of initial response or > 4x within any 12
months period), low dose steroid (0.5mg Pred/kg/alt day) should be given for 3-6mths.
• For those who relapse while on alternate day steroid Or within 2 wks of cessation of steroid
(steroid dependent), the lowest dose of prednisolone at which remission is sustained should be
used.
• Ketrax (levamisole) 2.5 mg/kg/alt days may be given for 4-12 mths.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
125
Indications for renal biopsy
• Age <12 months or > 12 years
• SRNS
• Atypical features
• Initial macroscopic hematuria at any age (in the absence of infectn or renal vein thrombosis)
• Evidence of vasculitis
• Persistentent HPT
• Persistent impaired renal function
• Low C3
• Hepatitis B or C serology, HIV
Protocol for Performing Renal biopsy
1. Book with the sonographer (Radiologist)
2. Do baseline KUB USS. A small shrunken kidney is not biopsyable.
3. Obtain inform consent from Parents/Guardians
4. Do FBC, Coagulation screen (PT, PTT, INR), BUE, Cr)
5. Maintain normotension
6. Keep patient nil per os overnight
7. Do blood grouping and cross match and safe
8. Obtain IV line access
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
126
11.5.0 URINARY TRACT INFECTION Definition: bacteriological diagnosis based on culture of a single bacterial species of appropriate colony
count from appropriately collected urine;
• for suprapubic aspiration (SPA), any amount of bacteria count or growth
• for mid stream urine (MSU) or clean catch, colony count of >100,000/ml urine
• for catheterised urine sample, colony count of > 10,000/ml
• Lower bacterial counts (1000/ml) may be accepted if prior antibiotic intake. Always state clearly on the laboratory request form the type of urine sample and antibiotic history.
Non-bacterial pathogens e.g fungus (candida) and virus may be considered significant particularly for the
immunocompromised.
Bagged urine collection is not suitable. It may only be used for screening purposes.
Clinical suspicion: Suspect UTI in any child with the following:
• fever in the infant and young child in whom symptoms may be non-specific
• any child with urine dipstick positive for leucocyte and/or nitrite, or pus cells >10/HPF on
microscopy
• dysuria, frequency of micturation, loin pain, 20 enuresis, offensive urine.
Classification:
• lower tract infection (cystitis) and upper tract infection (pyelonephritis).
• Pyelonephritis represents the most severe form and carries the risk of renal scaring. It is
often not possible to localize the site of the infection. Cystitis is often associated with only low grade fever whilst pyelonephritis is often associated with
temperatures > 390C.
Treatment
For children with severe symptoms or in whom pyelonephritis is suspected, treatment should be
commenced straight away once urine sample has been collected preferably with IV antibiotics.
For less severe symptoms, antibiotics can wait till after culture and sensitivity results.
Choice of antibiotics:
Parenteral antibiotics:
• gentamycin 7.5mg/kg OD
• ciprofloxacin 10mg/kg 12hrly
• 2nd
/3rd
generation cephalosporin e.g.
o 30-50mg/kg cefuroxime BD or
o 50mg/kg ceftriaxone OD
• Co-amoxiclav 15mg/kg/dose of amoxil TDS
Oral antibiotics:
• ciprofloxacin 15mg/kg BD
• Co-amoxiclav 15mg/kg of amox BD
• cefuroxime 10mg/kg BD
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
127
Note: co-trimoxazole and amoxicillin are ineffective therapies for UTI in this locality*
Duration of therapy: 5-7 days for cystitis. 7-14 days for pyelonephritis.
All children should have follow up urine C/S done at least 48hrs after completing antimicrobial therapy to
document cure.
Antibiotic prophylaxis: This may be considered for newborns and young infants with culture-proven UTI
who are yet to have radiological evaluation to rule out underlying structural abnormalities. It should be
considered for all children with proven underlying urinary tract abnormalities.
Choice of prophylaxis:
• cefuroxime (for newborns) 5mg/kg BD
• nitofurantoin (1mg/kg nocte)
• nalidixic acid(7.5mg/kg BD)
Radiological investigations
For this protocol, all children with culture-proven UTI should have radiological investigation to rule out
underlying structural abnormality or renal scarring as follows:
• kidney, ureter and bladder (KUB) ultrasound request –ALL CASES
• micturiting cystourethrogram (MCUG)-done only after UTI has been cured:
o for all children under 2 years
o for all boys
o for all cases abnormality on ultrasound
• IVU –for all cases of suspected Pelvicoureteric junction obstruction or renal scaring. Nuclear
imaging is the ideal test and may be requested for at other institution. Other radiological investigations may be discussed with the Nephrologist or Radiologist.
*Antwi et al. Urine dipstick as a screening test for urinary tract infection. Ann Trop Paediatr 2008; 28:117-
122
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
128
11.6.0 ACUTE RENAL FAILURE Definition
In this protocol, ARF shall be defined as
• An elevated serum creatinine greater than the acceptable range of normal for age in the setting of
risk factor for acute kidney injury (see below) in a patient with known normal renal function for the
preceding 3 months
OR
• ≥ 1.5-fold rise (50% ↑) in serum creatinine or an absolute ↑in serum creatinine of ≥ 26.4 μmol/l
from known baseline value occurring within 48 hours.
OR
• a sudden decreased in urine output of < 0.5ml/kg/hour for any duration > 6 hours.
For any patient with known chronic kidney disease, the occurrence of any one of the above shall be defined
as acute-on-chronic renal failure. Efforts should thus be made to identify any remediable event (e.g.
infection, urinary tract obstruction & dehydration) that precipitated such failure.
The following serum creatinine values shall be used:
• Newborns(1st
7 days of life)..................27-88 μmol/l
• Infant…………………………..…....................18-35 μmol/l
• Child……………………………….....................27-62 μmol/l
• Adolescent………………………....................44-88 μmol/l
Acute Renal failure is POTENTIALLY REVERSIBLE if intervention is instituted early. Every effort should
therefore be made in getting input from the Paediatric Nephrologist whilst primary intervention is
instituted by the attending Clinician.
Evaluation
A. History Any event that is known to potentially cause kidney injury should be clearly identified and noted. These
include:
Pre-renal events
1. Volume loss e.g. from diarrhoea & vomiting, haemorrhage, burns, 3rd
spacing
2. Hypotension from any cause
3. Sepsis
4. Decreased renal perfusion e.g. from shock including Algid malaria
5. Vasoconstriction from radiographic contrast
Renal events
1. Hypoxia
2. Nephrotoxic agents including drugs like gentamycin
3. Muscle injury or intravascular haemolysis (passage of dark urine)
4. Sepsis
5. Glomerulonephritis
6. Pyelonephritis and other causes of tubule-interstitial nephritis
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
129
7. Haemolytic Uraemic syndrome
8. Tumour infiltrate
Post-renal events
1. Poor urine stream e.g. dribbling of urine
2. Difficulty in voiding
3. History of kidney stones (colicky pain in the flank ±bloody urine)
B. Physical findings
1. Determine volume status (volume deficit e.g cold extremities, weak pulse, ↓CRT, ↓skin turgor for
pre-renal ARF; volume overload e.g. engorged neck veins, oedema in the absence of hypovolaemia
for post-renal ARF)
2. Blood pressure (hypotension for pre-renal ARF, hypertension for renal ARF)
3. Palpable kidneys or palpable bladder (post-renal ARF)
C. Investigations
1. Urine dipsticks
2. Urine microscopy, C&S
3. Urine electrolytes + fractional excretion of sodium (FENa).
4. Blood chemistry (Na, K, Cl, urea, creatinine, albumin, total protein, cholesterol, Ca, Mg, inorg PO4)
5. Blood gas
6. Full blood count
7. KUB ultrasound
Other tests should be determined by suspected diagnosis e.g. Urine calcium/creatinine ratio for suspected
hypercalciuria
Useful discriminatory tests between Pre-reanal ARF and Intrinsic ARF
Parameter Pre-renal Intrinsic ARF
History Volume loss +ve Volume loss –ve (or very long duration)
Volume status ↓ N or↑
BP ↓ or paradoxically ↑ N or ↑
Urine-Na < 10mmol/l > 20mmol/l
FE-Na < 1% > 1%
Fluid challenge +ve response No response
BUN/Scr > 20:1 < 20:1
Urine microscopy Normal or non-specific findings Granular/tubular cell cast/red cell cast
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
130
FENa(%) = Urine Sodium X Serum Creatinine X100
Urine Creatinine X Serum Sodium
Management
General Principles
• Establish the cause of the ARF as much as possible
• For all suspected post-renal causes, URGENT KUB ultrasound should be requested
• Avoid on-going kidney injury with nephrotoxins like gentamycin and NSAIDs
• Look for acute complications (see below) and treat
Steps in Management:
1. Pass indwelling catheter for strict urine output monitoring (measure in ml/kg/hour). Catheter will
also relieve obstruction in post-renal causes
2. Fluid challenge with N/Saline 20ml/kg infused over 30 min – 1 hour for all cases of suspected pre-
renal cause in the absence of obvious volume overload. Fluid bolus may be repeated x 2.
In the absence of obvious fluid overload, try fluid challange if not sure of cause of ARF.
Monitoring should, however, be done for iatrogenic pulmonary oedema (increasing breathlessness, new
onset basal crackles, new onset facial oedema and/or hepatomegaly, ↑RR, ↑HR)
3. If hypovolaemic despite fluid resuscitation, give ionotropes (dopamine, dobutamine or
norAdrenaline/Adrenaline) to maintain normal BP
4. Fluid restriction in established intrinsic ARF. if oliguric give insensible loss [400ml/m2/day] +
previous day’s output. If markedly hypervolemic and anuric, total fluid restriction
5. Fluid replacement if polyuric particularly after relief of obstruction in post-renal ARF or following
recovery in ATN
6. Diuretic challange for persistent oligo-anuria despite adequate fluid resuscitation. Lasix 2mg/kg I.V.
stat. A second dose of 5mg/kg may be given slowly over 5-10 mins if no satisfactory response.
Alternatively, lasix infusion 0.5-1mgkg/hr may be given ± aminophylline infusion 0.7mg/kg to run for
6 hours. New infusion should be prepared every 6 hours.
Complications of ARF and their Management
1. Hyperkalaemia (See also under Nephritic syndrome)
• Put on cardiac monitor to see ECG changes
• Stabilise myocardial with Ca gluconate 10% (0.5ml/kg IV over 10 min)
• Commence salbutamol nebulisation 5mg 2-hourly (2.5mg if < 5yrs) whilst serial levels of potassium
are determined
• Kayexalate 0.5-1g 6-hourly (per rectum or orally)
• Soluble insulin in 10% Dextrose to run at 1units of insulin/5g of dextrose over 1 hour whilst RBS is
checked frequently.
• NaHCO3 1 mmol/kg/day but be careful with associated ↑ in intratravascular volume
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
131
• Dialysis if the above treatment measures fail
Supporting measures in treatment of Hyperkalaemia
• Avoid K-rich diet
• Avoid drugs that cause hyperK+
2. Pulmonary oedema
• Confirm with urgent CXR
• Prop up and give O2
• IV Lasix (high dose) 4-5mg/kg slowly over5-10mins
• Acute dialysis invariably
3. Hypocalcaemia/Hyperphosphataemia
• If symptomatic hypocalcaemia (tetany or convulsion), then give IV Ca gluconate
• Phosphate binders per oral with food e.g. CaCO3, Al(OH)3
4. Metabolic acidosis
• Treat with NaHCO3
5. Hypertensive encephalopathy (See also under Nephritic syndrome)
• IV labetalol (continuos infusion) or IV hydrallazine 0.1-0.2mg/kg q30mins-60mins. These should
be titrated to achieve a gradual and gentle fall in BP by 1/3 in the 1st
24 hours, 1/3 in the next 24
hours and 1/3 in the final 24 hours
• IV Lasix 1-2mg/kg
• IV mannitol 0.25-0.5mg/kg over 30 mins
• Commence oral antihypertensives as soon as stable to take. Preferably use short acting drugs
like Nifedipine
6. Hyponatraemia
• Restrict all plain water intake
• If symptomatic, treat with IV 3% NaCl
Indications for dialysis in ARF
• Failure of conservative Management
• Pulmonary oedema unresponsive to diuretics
• Hyperkalaemia not controlled by conservative treatment
• Severe metabolic acidosis
• Oligo-anuria
• Uraemic pericarditis
• Multisystem failure
• Severe hyponatraemia
• To make room for volume therapy (e.g. Transfusion, TPN) in the oligo-anuric patient
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
132
11.7.0 CHRONIC RENAL FAILURE/CHRONIC KIDNEY DISEASE
Definitions
1. Chronic kidney disease (CKD)
Any kidney injury that last > 3 months. Such injury may be defined by structural or functional abnormalities
as follows:
o ↑ serum urea & creatinine
o Proteinuria ± haematuria
o Abnormal renal imaging.
o Abnormality on kidney biopsy.
2. Chronic renal failure (CRF)
Irreversible lost of renal function with a resulting decrease in GFR and a slowly creeping serum creating.
CRF occurs on the background of chronic kidney injury, leading to loss of functional renal mass →small
shrunken kidneys.
Since the kidneys maintain a large functional reserve, the renal damage must exceed 50% of the nephron
population for CRF to develop. In CRF, there is significant impairment of the synthetic function →anaemia,
and Renal Osteodystrophy (ROD) .
Classification/Staging of CKD
In this protocol, all children with CKD shall have GFR estimated by the Swart formula and staged according
to the National Kidney Foundation Disease Outcome Quality Initiative (K/DOQI) guidelines as follows:
Swart formula:
Estimated GFR (eGFR)
= height (cm) x K
Serum creatinine (μmol/l)
Where K = 40 for children < 1 year
49 for all children 1-12 yrs old
49 for adolescent females 13-21 yrs
60 for adolescent males 13-21 yrs
NKF-K/DOQI classification of chronic kidney disease (CKD)
Stage of CKD GFR(ml/min/1.73m2) Description
1 ≥ 90 Kidney damage with normal or increased GFR
2 60-89 Kidney damage with mild reduction of GFR
3 30-59 Moderate reduction of GFR
4 15-29 Severe reduction of GFR
5 < 15 End stage renal failure
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
133
Clinical suspicion
Suspect CRF in any child with renal failure who has any of the following:
• growth failure
• anaemia (usually normocytic normochromic)
• hypertension
• rickets
Investigations
The following investigations shall be done for all children with CRF
1. Ultrasound of the Kidneys, ureters, and bladder (KUB)
2. Blood urea, creatinine, electrolytes, Ca2+, Mg2+, PO4-, albumin, total proteins, cholesterol, alkaline
phosphatise, liver transaminases (ALT & AST).
3. Urine dipstick, microscopy and C/S
4. Serum parathyroid hormones
5. Blood gases
6. Full blood count
Other investigations may be determined by individual cases.
Treatment
Rx focuses on measures aimed at slowing progression of CKD to ESRFand shall consist of the following:
• Reduce proteinuria with ACEIs & angiotensin receptor blocker e.g losartan. Beware of side effect of
hyperkalaemia.
• Control hypertension with antihypertensives. Aim for BP < 90th centile for age & sex
• Control fluid overload with fluid restriction and high dose lasix (up to 5mg/kg may be given BD-TDS)
± metolazone.
• Control lipidaemia with statins especially chronic nephrotics. Statins also have anti-inflammatory
effects that help to reduce chronic glomerular inflammation.
• Control ROD with PO4 binders (e.g. CaCO3) given with every meal & calcitriol/1α vit D3 0.25μg-
1μg/day
• Control acidosis with NaHCO3 50-100 mmol/kg/day in 2-4 divided doses (titrate against blood pH)
• Manage anaemia with Inj. erythropoeitin (20-50U/kg subcut 2-3x/week) & haematinics
• Manage hyperkalaemia with kayaxelate 0.5-1g/kg QID. Lasix and metolazone may also help to
control hyperkalaemia.
• Ensure adequate nutrition to allow for growt. Up to 2g/kg protein per day may be given. The
support of nutritionist may be needed here.
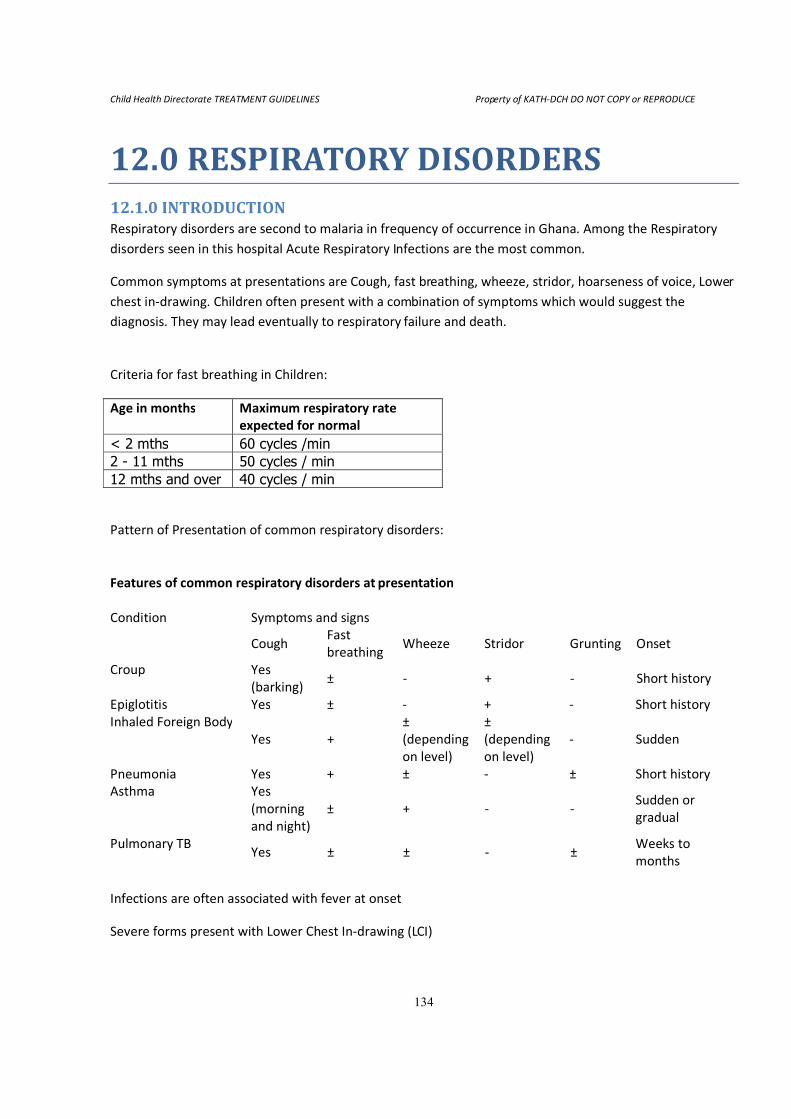
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
134
12.0 RESPIRATORY DISORDERS 12.1.0 INTRODUCTION Respiratory disorders are second to malaria in frequency of occurrence in Ghana. Among the Respiratory
disorders seen in this hospital Acute Respiratory Infections are the most common.
Common symptoms at presentations are Cough, fast breathing, wheeze, stridor, hoarseness of voice, Lower
chest in-drawing. Children often present with a combination of symptoms which would suggest the
diagnosis. They may lead eventually to respiratory failure and death.
Criteria for fast breathing in Children:
Age in months Maximum respiratory rate
expected for normal
< 2 mths 60 cycles /min 2 - 11 mths 50 cycles / min
12 mths and over 40 cycles / min
Pattern of Presentation of common respiratory disorders:
Features of common respiratory disorders at presentation
Condition Symptoms and signs
Cough
Fast
breathing Wheeze Stridor Grunting Onset
Croup Yes
(barking) ± - + - Short history
Epiglotitis Yes ± - + - Short history
Inhaled Foreign Body
Yes +
±
(depending
on level)
±
(depending
on level)
- Sudden
Pneumonia Yes + ± - ± Short history
Asthma Yes
(morning
and night)
± + - - Sudden or
gradual
Pulmonary TB Yes ± ± - ±
Weeks to
months
Infections are often associated with fever at onset
Severe forms present with Lower Chest In-drawing (LCI)
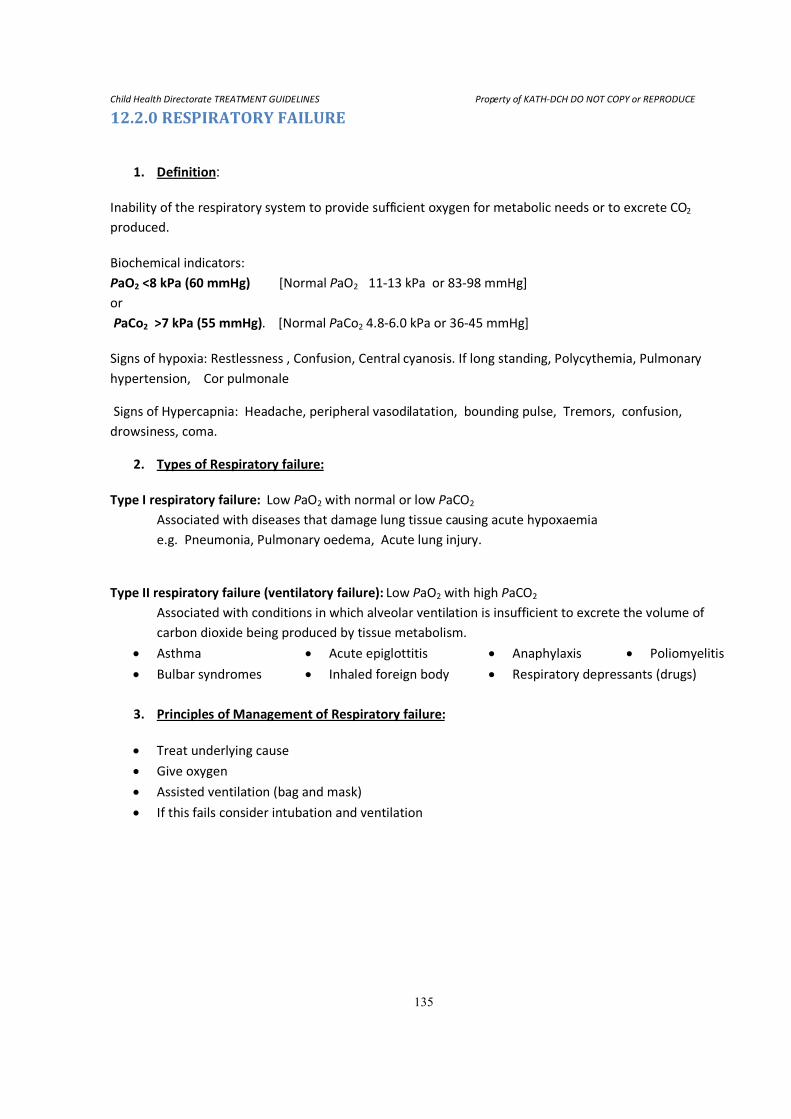
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
135
12.2.0 RESPIRATORY FAILURE
1. Definition:
Inability of the respiratory system to provide sufficient oxygen for metabolic needs or to excrete CO2
produced.
Biochemical indicators:
PaO2 <8 kPa (60 mmHg) [Normal PaO2 11-13 kPa or 83-98 mmHg]
or
PaCo2 >7 kPa (55 mmHg). [Normal PaCo2 4.8-6.0 kPa or 36-45 mmHg]
Signs of hypoxia: Restlessness , Confusion, Central cyanosis. If long standing, Polycythemia, Pulmonary
hypertension, Cor pulmonale
Signs of Hypercapnia: Headache, peripheral vasodilatation, bounding pulse, Tremors, confusion,
drowsiness, coma.
2. Types of Respiratory failure:
Type I respiratory failure: Low PaO2 with normal or low PaCO2
Associated with diseases that damage lung tissue causing acute hypoxaemia
e.g. Pneumonia, Pulmonary oedema, Acute lung injury.
Type II respiratory failure (ventilatory failure): Low PaO2 with high PaCO2
Associated with conditions in which alveolar ventilation is insufficient to excrete the volume of
carbon dioxide being produced by tissue metabolism.
• Asthma • Acute epiglottitis • Anaphylaxis • Poliomyelitis
• Bulbar syndromes • Inhaled foreign body • Respiratory depressants (drugs)
3. Principles of Management of Respiratory failure:
• Treat underlying cause
• Give oxygen
• Assisted ventilation (bag and mask)
• If this fails consider intubation and ventilation
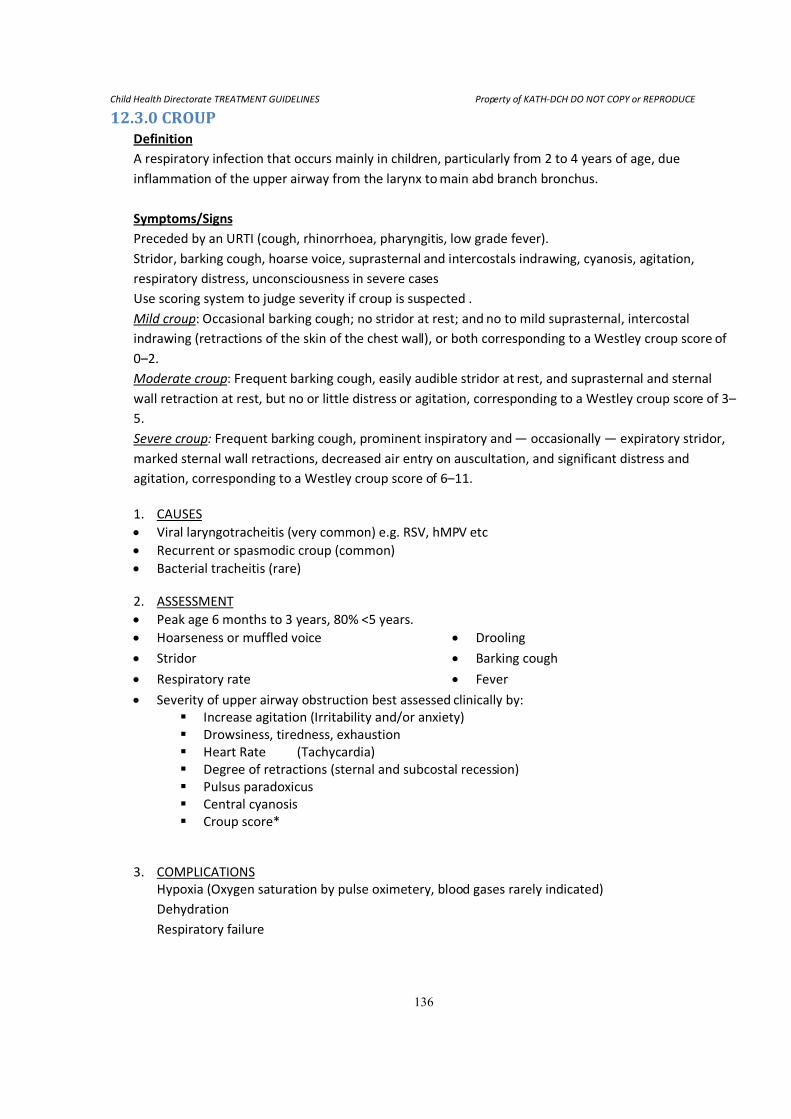
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
136
12.3.0 CROUP Definition
A respiratory infection that occurs mainly in children, particularly from 2 to 4 years of age, due
inflammation of the upper airway from the larynx to main abd branch bronchus.
Symptoms/Signs
Preceded by an URTI (cough, rhinorrhoea, pharyngitis, low grade fever).
Stridor, barking cough, hoarse voice, suprasternal and intercostals indrawing, cyanosis, agitation,
respiratory distress, unconsciousness in severe cases
Use scoring system to judge severity if croup is suspected .
Mild croup: Occasional barking cough; no stridor at rest; and no to mild suprasternal, intercostal
indrawing (retractions of the skin of the chest wall), or both corresponding to a Westley croup score of
0–2.
Moderate croup: Frequent barking cough, easily audible stridor at rest, and suprasternal and sternal
wall retraction at rest, but no or little distress or agitation, corresponding to a Westley croup score of 3–
5.
Severe croup: Frequent barking cough, prominent inspiratory and — occasionally — expiratory stridor,
marked sternal wall retractions, decreased air entry on auscultation, and significant distress and
agitation, corresponding to a Westley croup score of 6–11.
1. CAUSES
• Viral laryngotracheitis (very common) e.g. RSV, hMPV etc
• Recurrent or spasmodic croup (common)
• Bacterial tracheitis (rare)
2. ASSESSMENT
• Peak age 6 months to 3 years, 80% <5 years.
• Hoarseness or muffled voice • Drooling
• Stridor • Barking cough
• Respiratory rate • Fever
• Severity of upper airway obstruction best assessed clinically by:
� Increase agitation (Irritability and/or anxiety)
� Drowsiness, tiredness, exhaustion
� Heart Rate (Tachycardia)
� Degree of retractions (sternal and subcostal recession)
� Pulsus paradoxicus
� Central cyanosis
� Croup score*
3. COMPLICATIONS
Hypoxia (Oxygen saturation by pulse oximetery, blood gases rarely indicated)
Dehydration
Respiratory failure
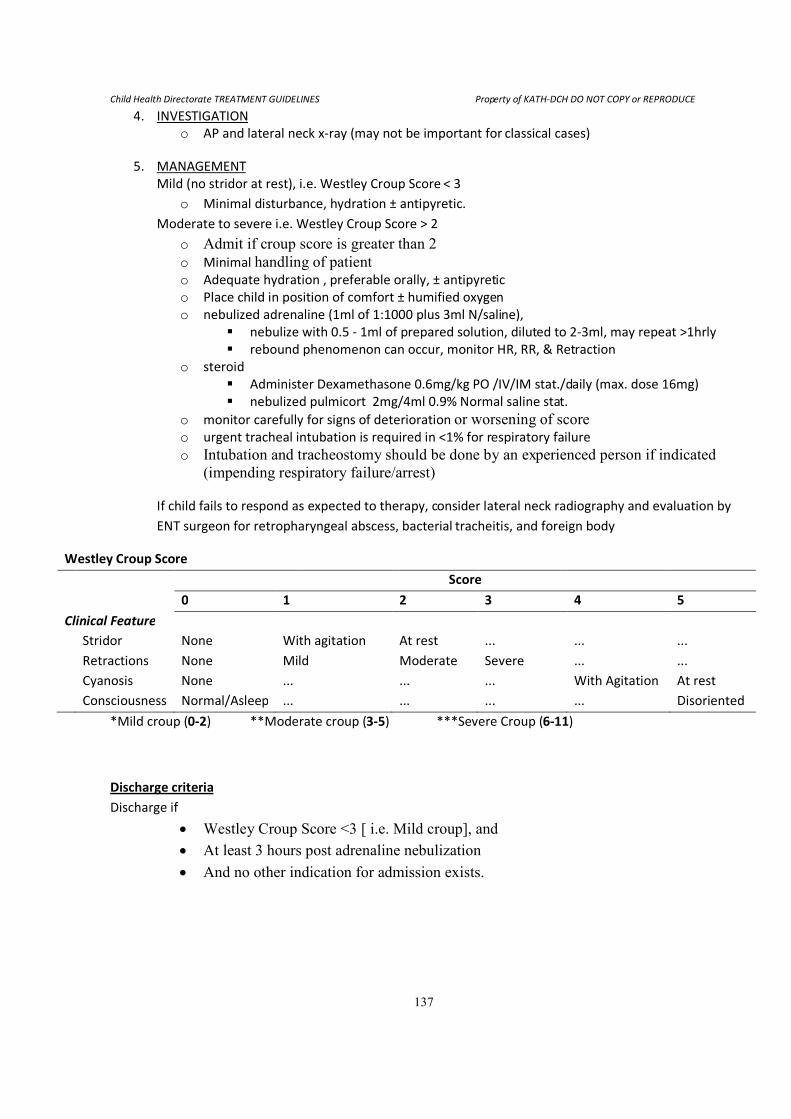
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
137
4. INVESTIGATION
o AP and lateral neck x-ray (may not be important for classical cases)
5. MANAGEMENT
Mild (no stridor at rest), i.e. Westley Croup Score < 3
o Minimal disturbance, hydration ± antipyretic.
Moderate to severe i.e. Westley Croup Score > 2
o Admit if croup score is greater than 2
o Minimal handling of patient o Adequate hydration , preferable orally, ± antipyretic
o Place child in position of comfort ± humified oxygen
o nebulized adrenaline (1ml of 1:1000 plus 3ml N/saline),
� nebulize with 0.5 - 1ml of prepared solution, diluted to 2-3ml, may repeat >1hrly
� rebound phenomenon can occur, monitor HR, RR, & Retraction
o steroid
� Administer Dexamethasone 0.6mg/kg PO /IV/IM stat./daily (max. dose 16mg)
� nebulized pulmicort 2mg/4ml 0.9% Normal saline stat.
o monitor carefully for signs of deterioration or worsening of score
o urgent tracheal intubation is required in <1% for respiratory failure
o Intubation and tracheostomy should be done by an experienced person if indicated
(impending respiratory failure/arrest)
If child fails to respond as expected to therapy, consider lateral neck radiography and evaluation by
ENT surgeon for retropharyngeal abscess, bacterial tracheitis, and foreign body
Westley Croup Score
Score
0 1 2 3 4 5
Clinical Feature
Stridor None With agitation At rest ... ... ...
Retractions None Mild Moderate Severe ... ...
Cyanosis None ... ... ... With Agitation At rest
Consciousness Normal/Asleep ... ... ... ... Disoriented
*Mild croup (0-2) **Moderate croup (3-5) ***Severe Croup (6-11)
Discharge criteria
Discharge if
• Westley Croup Score <3 [ i.e. Mild croup], and
• At least 3 hours post adrenaline nebulization
• And no other indication for admission exists.
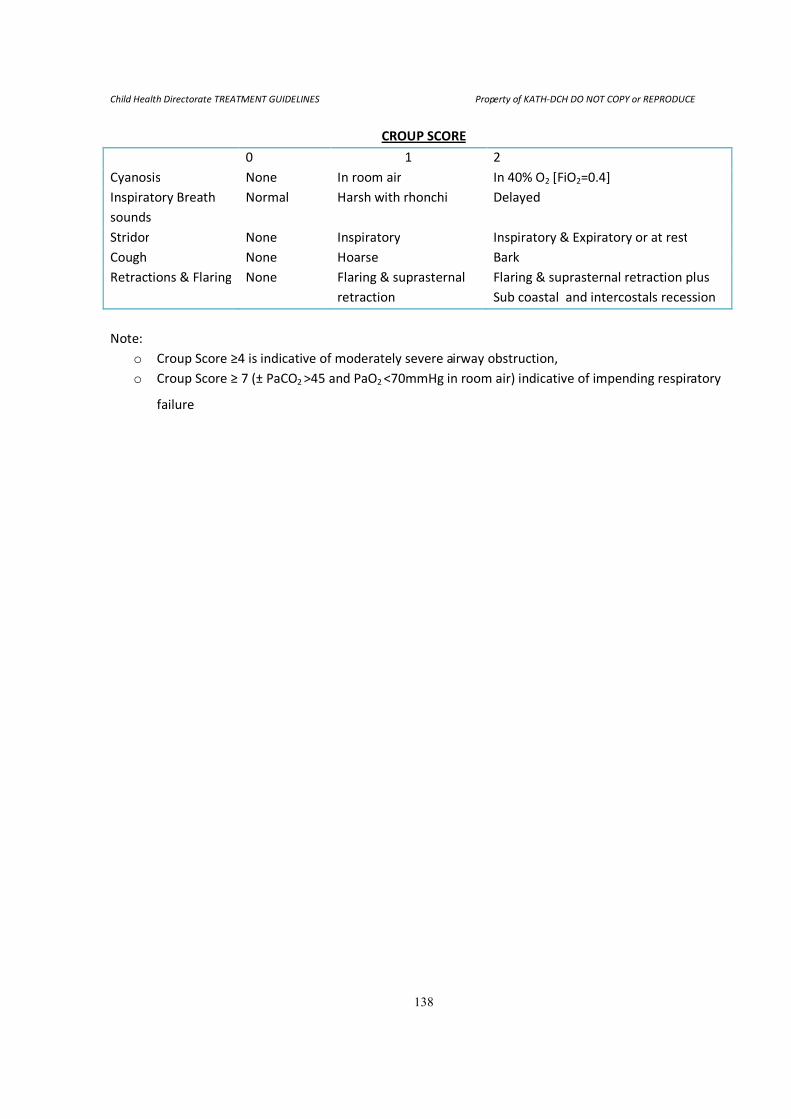
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
138
CROUP SCORE
0 1 2
Cyanosis None In room air In 40% O2 [FiO2=0.4]
Inspiratory Breath
sounds
Normal Harsh with rhonchi Delayed
Stridor None Inspiratory Inspiratory & Expiratory or at rest
Cough None Hoarse Bark
Retractions & Flaring None Flaring & suprasternal
retraction
Flaring & suprasternal retraction plus
Sub coastal and intercostals recession
Note:
o Croup Score ≥4 is indicative of moderately severe airway obstruction,
o Croup Score ≥ 7 (± PaCO2 >45 and PaO2 <70mmHg in room air) indicative of impending respiratory
failure
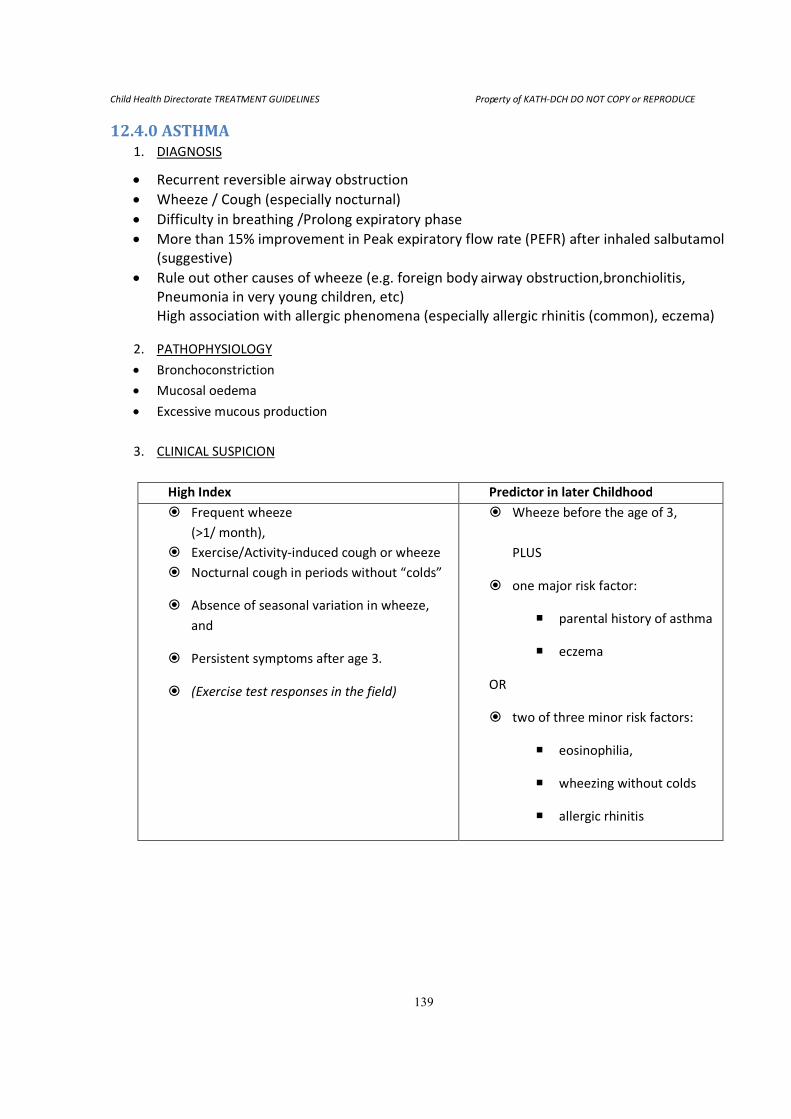
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
139
12.4.0 ASTHMA 1. DIAGNOSIS
• Recurrent reversible airway obstruction
• Wheeze / Cough (especially nocturnal)
• Difficulty in breathing /Prolong expiratory phase
• More than 15% improvement in Peak expiratory flow rate (PEFR) after inhaled salbutamol
(suggestive)
• Rule out other causes of wheeze (e.g. foreign body airway obstruction,bronchiolitis,
Pneumonia in very young children, etc)
High association with allergic phenomena (especially allergic rhinitis (common), eczema)
2. PATHOPHYSIOLOGY
• Bronchoconstriction
• Mucosal oedema
• Excessive mucous production
3. CLINICAL SUSPICION
High Index Predictor in later Childhood
� Frequent wheeze
(>1/ month),
� Exercise/Activity-induced cough or wheeze
� Nocturnal cough in periods without “colds”
� Absence of seasonal variation in wheeze,
and
� Persistent symptoms after age 3.
� (Exercise test responses in the field)
� Wheeze before the age of 3,
PLUS
� one major risk factor:
� parental history of asthma
� eczema
OR
� two of three minor risk factors:
� eosinophilia,
� wheezing without colds
� allergic rhinitis
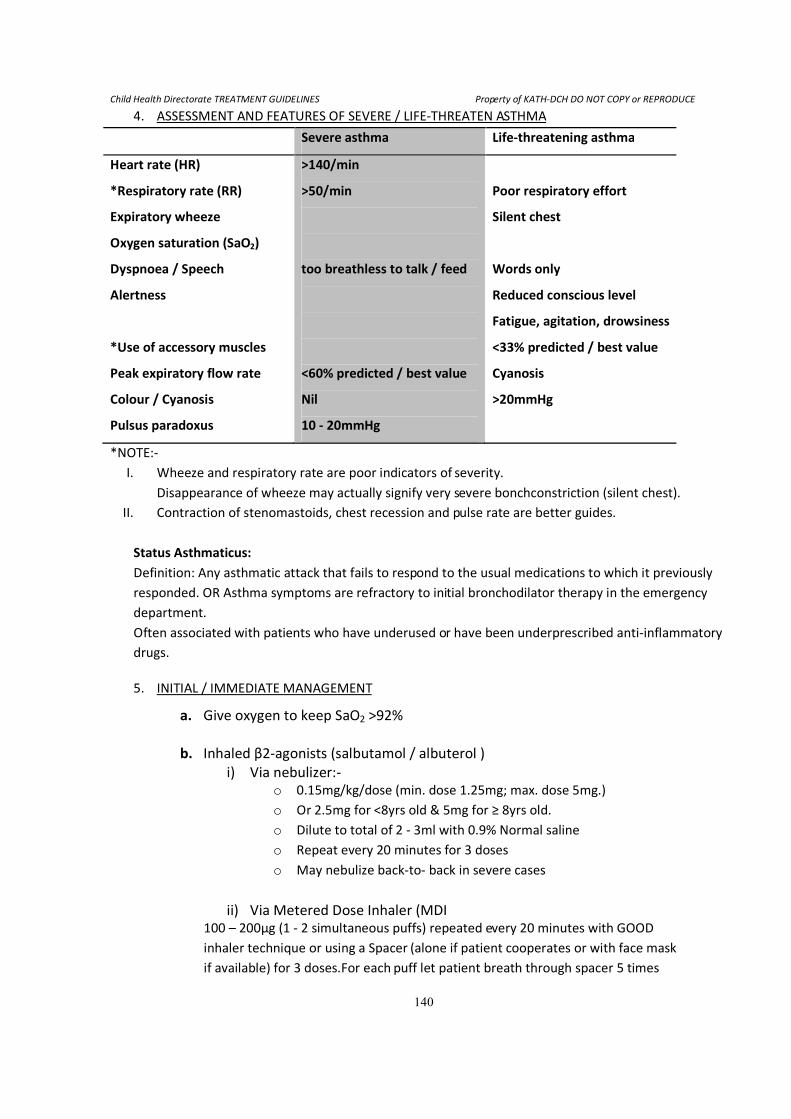
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
140
4. ASSESSMENT AND FEATURES OF SEVERE / LIFE-THREATEN ASTHMA
Severe asthma Life-threatening asthma
Heart rate (HR)
*Respiratory rate (RR)
Expiratory wheeze
Oxygen saturation (SaO2)
Dyspnoea / Speech
Alertness
*Use of accessory muscles
Peak expiratory flow rate
Colour / Cyanosis
Pulsus paradoxus
>140/min
>50/min
too breathless to talk / feed
<60% predicted / best value
Nil
10 - 20mmHg
Poor respiratory effort
Silent chest
Words only
Reduced conscious level
Fatigue, agitation, drowsiness
<33% predicted / best value
Cyanosis
>20mmHg
*NOTE:-
I. Wheeze and respiratory rate are poor indicators of severity.
Disappearance of wheeze may actually signify very severe bonchconstriction (silent chest).
II. Contraction of stenomastoids, chest recession and pulse rate are better guides.
Status Asthmaticus:
Definition: Any asthmatic attack that fails to respond to the usual medications to which it previously
responded. OR Asthma symptoms are refractory to initial bronchodilator therapy in the emergency
department.
Often associated with patients who have underused or have been underprescribed anti-inflammatory
drugs.
5. INITIAL / IMMEDIATE MANAGEMENT
a. Give oxygen to keep SaO2 >92%
b. Inhaled β2-agonists (salbutamol / albuterol )
i) Via nebulizer:-
o 0.15mg/kg/dose (min. dose 1.25mg; max. dose 5mg.)
o Or 2.5mg for <8yrs old & 5mg for ≥ 8yrs old.
o Dilute to total of 2 - 3ml with 0.9% Normal saline
o Repeat every 20 minutes for 3 doses
o May nebulize back-to- back in severe cases
ii) Via Metered Dose Inhaler (MDI
100 – 200μg (1 - 2 simultaneous puffs) repeated every 20 minutes with GOOD
inhaler technique or using a Spacer (alone if patient cooperates or with face mask
if available) for 3 doses.For each puff let patient breath through spacer 5 times
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
141
before the next puff is administered.
Most patients respond within 1 hour of treatment.
iii) Ipratropium 0.25 mg (or 2% solution) via nebulizer:
Ipratropium is synergistic with β2-agonists and should be administered with
salbutamol every 4-6 hours if available.
Note: Children appear to have more cholinergic receptors than adults and therefore are
more responsive to parasympathetic stimulation.
c. Start corticosteroids simultaneously with inhaled β2-agonists
Orally:
o Prednisolone /Methylprednisolone @1 -2mg/kg/day for 3 -5days OR
o Dexamethasone phosphate (decadron) @ 0.6mg/kg/day for ≤ 3days
Parentarely till oral tolerated:
IV Methylprednisolone 2mg/kg stat, then 0.5mg/kg/dose 6hrly OR
IM Dexamethasone 0.4mg/kg/dose BD (max. dose 16mg/day) OR
IV Hydrocortisone 4mg/kg/dose 6hrly
d. Intravenous Magnesium Sulfate in dose of 40–75 mg/kg (typical dose 50mg/Kg, maximum
of 2g per dose) disolved in 30–50 ml normal saline, infused over about 20 - 30 minutes could
be helpful for severe exacerbations not responding to conventional therapy.
6. CRITERIA FOR ADMISSION
If after nebulized bronchodilator therapy, child
• Has not responded adequately clinically
• Is exhausted
• Still has a marked reduction in the predicted (or usual) peak flow rate
• Has a reduced SaO2 <90%
• Has status asthmaticus
o CXR is indicated ONLY if there is severe dyspnoea or unusual features (e.g. asymmetry chest
signs suggestive of pneumothorax, lobar collapse) or signs of chest infection.
o Blood gases indicated ONLY in life-threatening or refractory cases.
Respiratory failure and death may be precipitated by fatigued respiratory muscles. Hence, patients not
responding to treatment would require transfer to ICU for intubation and ventilatory support while
inhaled /parenteral bronchodilators and parenteral corticosteroids are administered.
7. SUBSEQUENT ACUTE MANAGEMENT
• Continue with oxygen
• Check hydration status and Rehydrate and/or maintain hydration
• Continue nebulization therapy 1- 4hrly and space interval as tolerated.
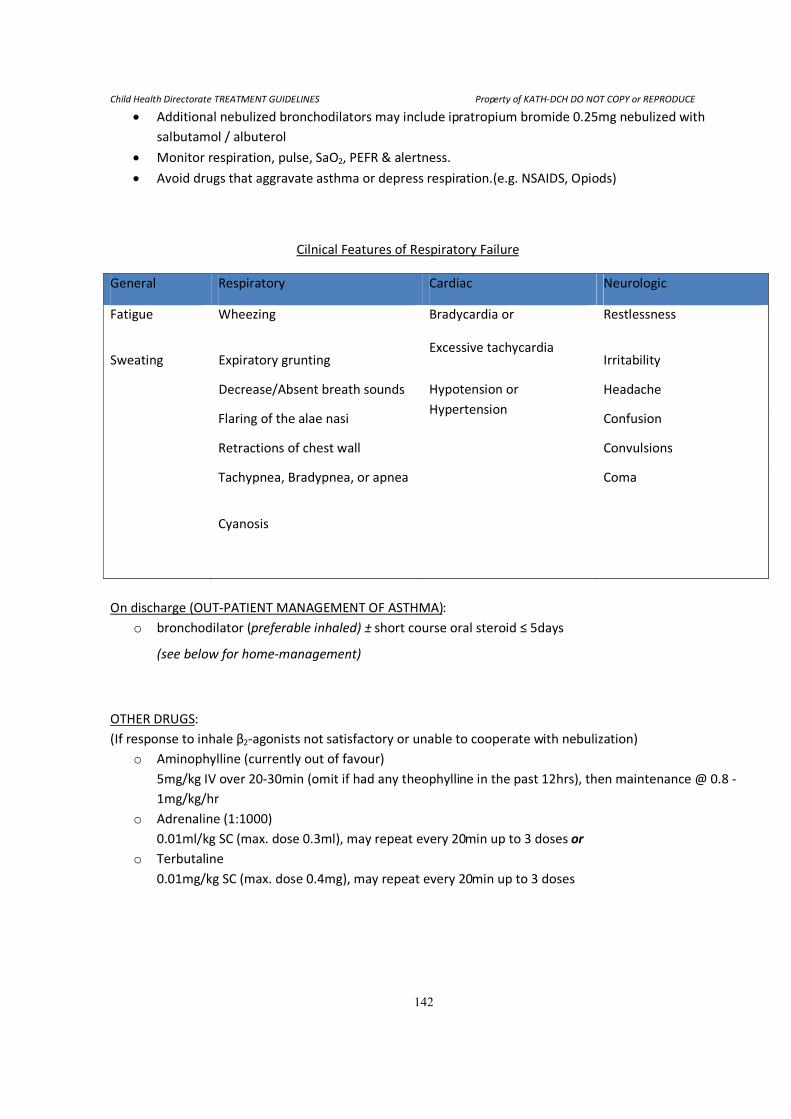
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
142
• Additional nebulized bronchodilators may include ipratropium bromide 0.25mg nebulized with
salbutamol / albuterol
• Monitor respiration, pulse, SaO2, PEFR & alertness.
• Avoid drugs that aggravate asthma or depress respiration.(e.g. NSAIDS, Opiods)
Cilnical Features of Respiratory Failure
General Respiratory Cardiac Neurologic
Fatigue Wheezing Bradycardia or
Excessive tachycardia
Restlessness
Sweating Expiratory grunting Irritability
Decrease/Absent breath sounds Hypotension or
Hypertension
Headache
Flaring of the alae nasi Confusion
Retractions of chest wall Convulsions
Tachypnea, Bradypnea, or apnea Coma
Cyanosis
On discharge (OUT-PATIENT MANAGEMENT OF ASTHMA):
o bronchodilator (preferable inhaled) ± short course oral steroid ≤ 5days
(see below for home-management)
OTHER DRUGS:
(If response to inhale β2-agonists not satisfactory or unable to cooperate with nebulization)
o Aminophylline (currently out of favour)
5mg/kg IV over 20-30min (omit if had any theophylline in the past 12hrs), then maintenance @ 0.8 -
1mg/kg/hr
o Adrenaline (1:1000)
0.01ml/kg SC (max. dose 0.3ml), may repeat every 20min up to 3 doses or
o Terbutaline
0.01mg/kg SC (max. dose 0.4mg), may repeat every 20min up to 3 doses
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
143
(HOME/OUT-PATIENT MANAGEMENT OF ASTHMA):
o Prevention of attacks/hospitalizations: Review periodically and treat:
Use PEFRs to monitor progress
Very occasional symptoms (once in several months):
Give short course (3-5 days) oral steroids with attacks
Inhaled bronchodilator as required
Frequent symptoms (more than one episode per month)
Daily Inhaled corticosteroids with bronchodilators
Adjust dose according to severity - The ultimate goal is to achieve a totally asthma-free status
Identify and counsel against precipitating factors
Note:
- Poor technique of using medications or adherence is often a cause of failed response to treatment
-Early intiation of steroids is useful in prevention severe attacks
-Exclude helminthiasis before administering high doses of steroids
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
144
12.5.0 APPROACH TO PNEUMONIAS Introduction
• Commonly presents as acute onset of illness with cough, sometimes following acute
upper respiratory Illness (AURI).
• Common features:
o Fever,
o Tachypnoea (fast breathing),
o Respiratory distress (Lower Chest In-drawing),
o Grunting
• Evidence of area of consolidation on CXR (but not always)
• Dullness, crepitations
• Referred pain to abdomen suggests usually Right or Left lower lobe involvement
• Presence of neck stiffness suggests Right upper lobe pneumonia
• Abdominal distention may occur
• Diagnosis not always easy: from mild febrile illness to peripheral circulatory collapse
with respiratory failure.
• Lateral and AP X-rays are important for confirming diagnosis
• Blood cultures are recommended for
o Severely ill
o Immunocompromised
o The malnourished
o Patients with other focus/foci of infection(s)
• Sputum miscroscopy and culture useful if possible
• Right Upper lobe pneumonias usually occur in first year of life from aspiration
• Main Risk factors:
o Malnutrition,
o Low Birth Weight,
o Measles,
o Crowding,
o Smoke.
Aetiology: Common causes:
� In developing:
◦ Strept pneumoniae (pneumococcus): 30-50% cases
◦ H. influenza (10-30% cases, more commonly in children <4 year)
◦ There may be others that are less well known
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
145
� In young infants in developed countries:
◦ Group B strept.,
◦ Chlamydia trachomatis,
◦ Listeria monocytogenes,
◦ Strept faecalis,
◦ Enteric gram negative bacilli - E. coli,
◦ Klebsiella spp.
Treatment:
1st year:
� Streptococcal, Staphylococcal, E. coli � chloramphenicol/ benzyl pen/ fluclox + gent (as first line)
� Chlamydia trachealis � Erythromycin/Azithromycin
� PS: Chlamydia pneumonia � dramatic X-ray changes in infants who are not that ill.
Beyond 1st year:
� Pneumococcus (over 90%) � Amoxicillin /Co-AmoxiClav/Cefuroxime/
Co-trimoxazole if Pneumocystis jeroveci infection is suspected in the immune compromised
� Remember Chlamydia, TB as important differentials
Any of these organisms may cause pneumonia in the malnourished or immunesuppressed, hence
appropriate treatment.
Oral treatment:
Amoxicillin,Co- AmoxiClav/Cefuroxime
Parenterral treatment:
Penicillin G, Co-AmoxiClav/Cefuroxime
Second line: Third generation cephalosporins
Choice of antibiotics ideally based on suspected organisms. For example, appropriate gram-negative
coverage should be considered in the immunocompromised.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
146
Special notes
� Common complications:
Pleural effusions – with pneumococcal infections
� Empyemas, pneumothorax – commonly with with staphylococcal infections
� Suspect immunosuppression if there is a history of more than 2 episodes of pneumonia in one year
Notes during management:
� Amoxicillin can effectively be given at 90mg/kg in 2 divided doses orally for 5 – 7 days, especially for
all patients who do not require admission.
� Although septicaemic illness does not always occur it is helpful to do a blood culture at booking for
all hospitalized cases to facilitate choices for second line treatment, should the need arise.
� Useful second line drugs:
Cefotaxime, Clindamycin, Azithromycin.
� Need for hydration and nutritional support (look for and manage dehydration)
� Effects of underlying/associated problems, e.g. measles, FB, AIDS, TB, etc
� NB: Coughing + poor peripheral perfusion, rapid pulse, High resp. rate, cardiomegaly, Hepato-
(spleno)megaly is suggestive of Heart failure
12.6.0 ATYPICAL PNEUMONIAS Definition:
Pneumonia caused by non-bacterial pathogens, typically Mycoplasma pneumoniae, Pneumocystis jeroveci,
viruses. Commonly associated with mild (progressive) symptoms (fever, cough) with chest X-rays that look
much worse than clinical picture would suggest.
• Exclude TB
• Always rule out immunosuppression in such cases.
• Consider Erythromycin/Azithromycin or Co-trimoxazole for treatment in such cases depending on
history and other clinical parameters.
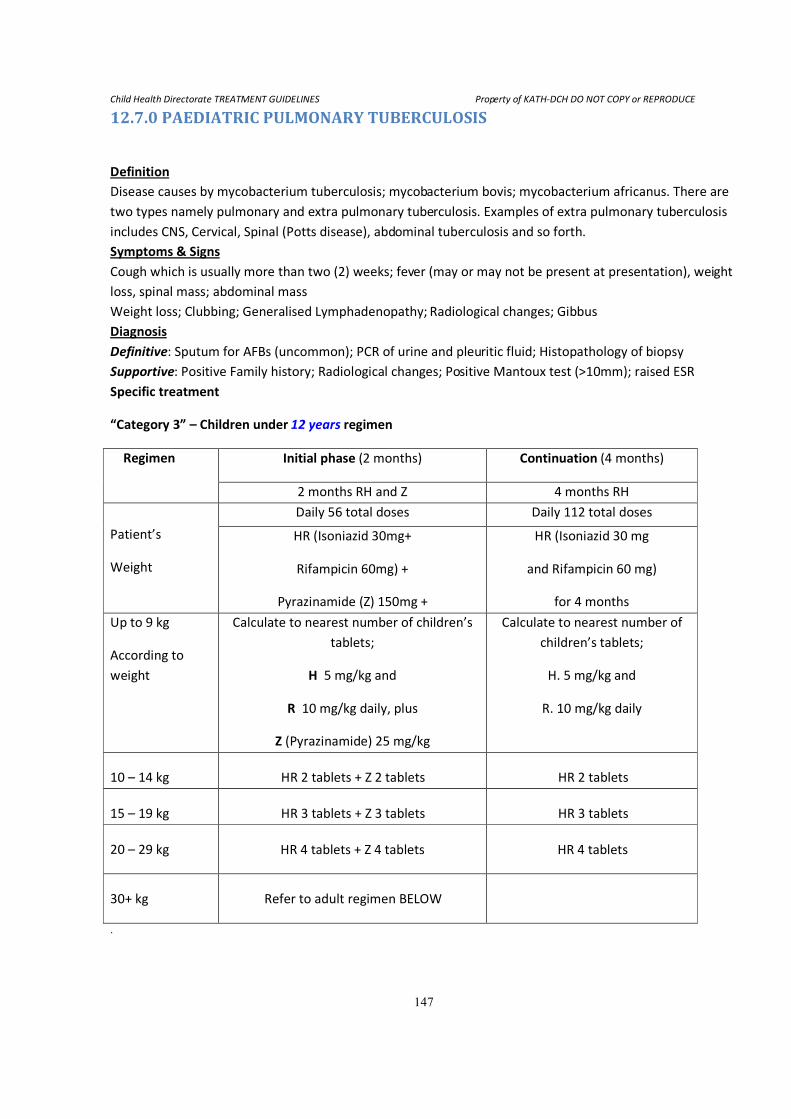
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
147
12.7.0 PAEDIATRIC PULMONARY TUBERCULOSIS
Definition
Disease causes by mycobacterium tuberculosis; mycobacterium bovis; mycobacterium africanus. There are
two types namely pulmonary and extra pulmonary tuberculosis. Examples of extra pulmonary tuberculosis
includes CNS, Cervical, Spinal (Potts disease), abdominal tuberculosis and so forth.
Symptoms & Signs
Cough which is usually more than two (2) weeks; fever (may or may not be present at presentation), weight
loss, spinal mass; abdominal mass
Weight loss; Clubbing; Generalised Lymphadenopathy; Radiological changes; Gibbus
Diagnosis
Definitive: Sputum for AFBs (uncommon); PCR of urine and pleuritic fluid; Histopathology of biopsy
Supportive: Positive Family history; Radiological changes; Positive Mantoux test (>10mm); raised ESR
Specific treatment
“Category 3” – Children under 12 years regimen
Regimen Initial phase (2 months) Continuation (4 months)
2 months RH and Z 4 months RH
Patient’s
Weight
Daily 56 total doses Daily 112 total doses
HR (Isoniazid 30mg+
Rifampicin 60mg) +
Pyrazinamide (Z) 150mg +
HR (Isoniazid 30 mg
and Rifampicin 60 mg)
for 4 months
Up to 9 kg
According to
weight
Calculate to nearest number of children’s
tablets;
H 5 mg/kg and
R 10 mg/kg daily, plus
Z (Pyrazinamide) 25 mg/kg
Calculate to nearest number of
children’s tablets;
H. 5 mg/kg and
R. 10 mg/kg daily
10 – 14 kg HR 2 tablets + Z 2 tablets HR 2 tablets
15 – 19 kg HR 3 tablets + Z 3 tablets HR 3 tablets
20 – 29 kg HR 4 tablets + Z 4 tablets HR 4 tablets
30+ kg Refer to adult regimen BELOW
.
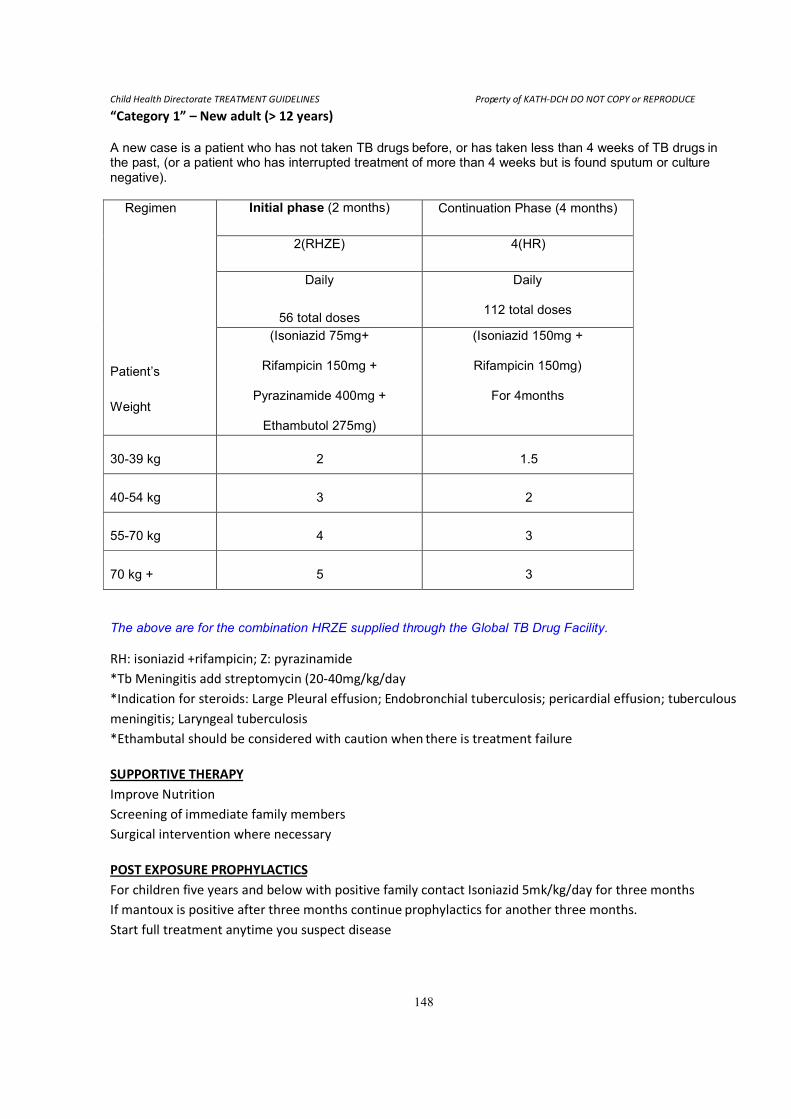
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
148
“Category 1” – New adult (> 12 years)
A new case is a patient who has not taken TB drugs before, or has taken less than 4 weeks of TB drugs in the past, (or a patient who has interrupted treatment of more than 4 weeks but is found sputum or culture negative).
Regimen
Patient’s
Weight
Initial phase (2 months) Continuation Phase (4 months)
2(RHZE) 4(HR)
Daily
56 total doses
Daily
112 total doses
(Isoniazid 75mg+
Rifampicin 150mg +
Pyrazinamide 400mg +
Ethambutol 275mg)
(Isoniazid 150mg +
Rifampicin 150mg)
For 4months
30-39 kg 2 1.5
40-54 kg 3 2
55-70 kg 4 3
70 kg + 5 3
The above are for the combination HRZE supplied through the Global TB Drug Facility.
RH: isoniazid +rifampicin; Z: pyrazinamide
*Tb Meningitis add streptomycin (20-40mg/kg/day
*Indication for steroids: Large Pleural effusion; Endobronchial tuberculosis; pericardial effusion; tuberculous
meningitis; Laryngeal tuberculosis
*Ethambutal should be considered with caution when there is treatment failure
SUPPORTIVE THERAPY
Improve Nutrition
Screening of immediate family members
Surgical intervention where necessary
POST EXPOSURE PROPHYLACTICS
For children five years and below with positive family contact Isoniazid 5mk/kg/day for three months
If mantoux is positive after three months continue prophylactics for another three months.
Start full treatment anytime you suspect disease
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
149
13.0 MISCELLANEOUS DISORDERS
13.1.0 SNAKE BITES Venomous snakes constitute approximately <15% of species of snakes known to exist.
13.1.1 RECOGNITION OF VENOMOUS SNAKES
• Cytotoxic (local tissue destruction).
Viperidae (e.g. Puff adder, Gaboon viper)
-flat, arrow-shaped head
-short and stout body
-often lie in ‘Z’ position
• Neurotoxic (neuromuscular paralysis)
Elapidae (e.g. Mamba, Cobra)
-head continuous with body
-slender and agile
-hooded neck; spits
• Haemotoxic (bleeding diathesis)
Colubrids and some vipers (e.g. carpet viper-Echis carinatus)
-very large eyes
-slender body
-ragged deep wound
• Cardiotoxic(cardiac arrhythmias, hypotension etc)
-Viperidae
• Myotoxic (systemic rhabdomyolysis)
-Hydrophiidae
13.1.2 CLINICAL FEATURES
Local pain and fang marks are very variable and of no help in diagnosis.
a. Neurotoxicity
• Typically, symptoms develop within 1-2 hours
• Contraction of frontalis muscle (puckered forehead)
• Extra-ocular muscles paralysis (e.g. opthalmoplegia, ptosis, blurred vision)
• hyperacusis, hypersalivation, congested conjuctiva, circum-oral numbness
• More serious late signs include dysphagia,dysphonia, and paralysis of muscles of deglutition and
respiration
NB. The paralysed tongue (inability to protrude ) may obstruct the upper airway.
b. Haemotoxic (Procoagulant and haemorrhagin )
• Persistent bleeding from fang mark, venopuncture site or new scarification marks
• Spontaneous bleeding (e.g. gingival sulci, haematuria, intraperitoneal, GI tract)
• Severe headache, meningism suggestive of Subarachnoid Haemorrhage
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
150
• Convulsion, hemiplegia and coma suggestive of intracranial haemorrhage
• Shock and pulmonary oedema from haemorrhage and /or carpillary leakage.
c. Cytotoxic
• -Blisters, tender swelling spreads from site of bite
• -Early tender enlargement of lymph nodes draining the bitten site.
• -Tensely swollen limbs are at risk of compartment syndrome
d. Myotoxicity
• -Muscle pain and stiffness with trismus
• -Respiratory muscle paralysis
• -Myoglobinuria and hyperkalaemia
e. Cardiotoxicity
• Cardiac arrhymias, ECG abnormalities and hypotension
• Responds rapidly to intravenous antivenom
13.1.3 MANAGEMENT
i) general measures to support vital functions (including Airway, Breathing & IV fluids)
ii) the site should be cleansed and then left strictly alone
iii) Sedatives are required if the patient is apprehensive
iv) Lab. Investigation:
o Look for evidence of blood in urine, stool & vomitus
o FBC (neutrophil >20,000/mm3,thrombocytopenia in severe envenoming)
o Incoagulable blood (leave 2-5mls of blood in dry glass: failure to clot in 20min)
o Raised CPK, AST, BUN in severe envenoming
o Do BUN, creatinine, serum K+ in ALL oliguric patients
o CXR for suspected pulmonary oedema
v) Appropriate antitetanus prophylaxis
vi) Treat / prevent secondary infection (e.g. using Penicillin & metronidazole)
vii) Antivenom if indicated* (see below)
13.1.4 INDICATION FOR ANTIVENOM
• Severe local envenoming:
-swelling involving more than half the bitten limb or develop extensive blistering
• Systemic envenoming:
-Neurotoxicity -Haemotoxicity (see above)
-Impaired consciousness -Cardiotoxicity (cardiac arrhythmias, abnormal ECG, hypotension)
-Myotoxicity (Rhabdomyolysis� stiff and tender muscles, trismus, myoglobinuria)
• Local envenoming however small it may be plus
-vomiting in the absence of emetic mixture (herbal or orthodox) ingestion
-neutrophil leucocytosis
-elevated serum enzymes (CPK & AST)
-haemoconcerntration (elevated PCV)
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
151
-uraemia
-oliguria ( urine output <0.5ml/kg/hour )
• Confirmed case of elapid (cobra, mamba):
-do not wait for symptoms
-evidence of fang penetration and snake must definitely have been an elapid.
13.1.5 ADMINISTRATION OF ANTIVENOM
• As soon as possible when ever indicated
• The dosage is the same for adults and children; antivenom is for treating the amount of venom
and not size of patient.
• IV route preferable to IM
• Dosage
• 40ml in 200ml Normal saline IV stat, for adder/viper bite
• 60-80ml in 200ml Normal saline IV stat, for elapid (neurotoxin) bite
• Run few drops initially as “Test dose” for serum sensitivity and look out for reaction, if no
reaction then whole drip in 1hr.
• Repeat dose of antivenom if signs & symptoms of envenoming persist after 1st
dose;
-persistence of cardiopulmonary signs > 30min after 1st
dose
-persistence of incoaguable blood > 6hrs after 1st
dose
• Have drugs to counter anaphylaxis drawn up prior to giving antivenom (i.e. adrenaline,
antihistamine, corticosteroid )
• Dilute 1 amp antivenom in 9 parts water for rinsing of venom from eyes (e.g. cobra)
• Use specific antivenom for sea-snake or boomslang bites
NOTE:-
a) Fixed dilated pupils with paralysis may occur in cobra and mamba bites
b) The carpet viper (Echis carinatus) accounts for more snake bite morbidity and mortality than any
other species; and in Northern Ghana the same species is responsible for 86 bites per 100,000
populations with 28% mortality.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
152
13.2.0 POISONING IN CHILDREN Poisoning in children may be:
• Accidental -the vast majority, especially <5years
• Non-accidental -as a form of child abuse in children over 6 years
• Deliberate self-poisoning -in older children
• Iatrogenic
A. ASSESSMENT
a. History
• High index of suspicion:
o Abrupt onset of symptoms
o Inconsistent history
o Previous history of ingestion
o Consider possibility of poisoning in any child with unexplained coma, seizures, or affective
disorder
• Identification of toxins with details of ingestion
o Type and time of ingestion/exposure and maximum possible quantity of toxin
ingested/exposed.
• Consider other causes of coma in the unconscious child e.g. trauma, seizures, CNS infection
Potential toxicity in accidental poisoning in children
Toxicity Medicine Household products
Low Oral contraceptives Chalk & crayons
Most antibiotics washing powder
Intermediate Paracetamol elixir Bleach, disinfectants,
Salbutamol window cleaners
High Alcoholic drinks, iron Acids, alkalis, petroleum distillates
Salicylate, digoxin organophosphorus insecticides
Tricyclic antidepressants
B. EXAMINATION
Neuromuscular: Ataxia Delirium/psychosis; Convulsions/seizures
Vital signs: Pulse; Respiration; Blood pressure; Temperature
Neuromuscular: Ataxia Delirium/Psychosis; Convulsions/Seizures; Paralysis; Coma
Ophthalmologic : Pupil size; Nystagmus
Skin: Jaundice; Cyanosis; Urticaria; Hot dry; Flushing
Breath odors: Alcohol; Garlic; Acetone; Coal gas
Gastrointestinal tract: Ileus; Violet emesis; Urinary retention
C. MANAGEMENT
Priorities
I. Resuscitation; maintain the airway, breathing, and circulation.
II. Determine the type and severity of ingestion; utilizing the history, physical examination &
laboratory analysis
III. Prevent further toxicity by removing the toxin or decreasing its absorption
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
153
IV. Enhance the elimination of the drug and its metabolites
i) Continue assessment of vital signs
ii) Administer an antidote if possible
iii) Rule out attempted suicide or child abuse
The comatose child
i) Maintain adequacy of airway and ventilation
ii) Start an intravenous line, give 10% dextrose containing fluid @ 5ml/kg for documented or
suspected hypoglycaemia. If effective continue fluid at maintenance rate.
iii) Give naxolone 0.1mg/kg for documented or suspected opiate over dose.
iv) Poor perfusion or circulatory compromise should be treated with IV infusion of 10ml/kg of
normal saline or Ringer’s lactate, repeated prn till child’s condition stable (≤60ml/kg).
v) Obtain samples for toxicology (i.e. urine, blood, gastric aspirate)
Surface decontamination
Remove clothing and wash skin with soap and water
Wash eyes with water or normal saline
Gastrointestinal decontamination
Note: Airway protection is of prime importance in gastrointestinal (GI) decontamination procedures.
Insertion of cuffed endotracheal tube is important in patients with altered sensorium or depressed gag
reflex, especially in those undergoing gastric lavage.
Activated charcoal
1g/kg body weight (or 10g / g ingested drug) PO or NG tube (≤50g).
contraindications
i. increased risk of aspiration e.g. Ileus, intestinal obstruction, hydrocarbons,
absent gag reflex.
ii. Alcohols, iron, caustics, lithium, electrolyte solutions, boric acid.
Gastric lavage
Indications: gastric lavage with large-bore tube may be useful in a life-threatening
ingestion and/or obtunded who arrive soon (≤90mins.)
Contraindications: caustic or hydrocarbon ingestions, co-ingestion of sharps.
Ipecac (Not recommended for use in hospital set up)
6 - 12month-old: 10ml followed by 10ml/kg water
1 - 5 years old: 15ml followed by 120ml water
>5 years old: 30ml followed by 200-300ml water
Contraindication: Coma, Convulsions, Caustics, and hydroCarbon
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
154
Cathartics (Avoid in children < 4years)
70% sorbitol solution at 1-2ml/kg
Magnesium citrate at 4-6ml/kg (max. 200ml)
Magnesium sulphate at 250mg/kg
Whole bowel irrigation
Polyethylene glycol solution @ 500ml/hr for 4-6hrs. Start slowly.
Dosage for adolescent is 1L/hr for 4-6hrs.
Effective and method of choice for symptomatic iron toxicity
Enhanced elimination
pH alteration to enhance excretion of weak acids and bases.
Sodium bicarbonate for alkalinization of urine (e.g. salicylates )
Ammonium chloride for acidification of urine, limited value.
Haemodialysis
Specific antidotes or therapy
Available for only a limited number of poisons.
e.g. N-acetylctsteine for acetaminophen (paracetamol).
Social assessment
To prevent further poisoning or accidents.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
155
13.3.0 SPECIFIC POISONING
13.3.1 HYDROCARBONS
Agents : Gasoline, kerosene, lubricating oils, mineral oil
Benzene, turpentine, toluene, camphor
Carbon tetrachloride, methylene chloride, trichloroethane.
Assessment
Pulmonary: tachypnea, dyspnea, tachycardia, cyanosis, grunting, cough.
CNS: lethargy, seizures, coma.
Hepatic toxicity: Acute liver failure
Cardiac toxicity: Arrhythmias.
Management
a.) Decontamination
i) Avoid emesis or lavage because of the risk of aspiration
ii) Avoid charcoal unless there is co-ingestion. It does not bind aliphatics and
will increase the risk of aspiration.
iii) If toxic amount ingested or contains potentially toxic substance, consider
INTUBATION WITH A CUFFED EndoTrachealTube followed by lavage.
b.) If patient seen within 2hr, consider single dose of liquid paraffin
to decrease absorption. Give 10-15ml stat orally.
c.) Treat pnuemonitis with oxygen.
• Routine use of antibiotics and steroids not warranted.
• Add antibiotics only with aspiration or suspected superimposed bacterial
infection.
d.) Observe patient for at least 6 hours.
i) If asymptomatic for 6hrs and CXR is normal, discharge.
ii) If symptomatic within 6hrs, admit.
iii) If asymptomatic but abnormal CXR, observe further.
iv) Lung complication may be delayed 12 hrs.
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
156
13.3.2 CAUSTIC INGESTIONS Agents:
Strong acids
Alkalis (e.g. hair relaxers, drain/oven cleaners, detergent crystals ) Have the
potential for airway swelling or esophageal perforation, even if no symptoms initially or no
oropharyngeal burns.
Assessment
Drooling, persistent salivation, vomiting (often with blood or tissue) stridor, dyspnea,
aphonia, hoarseness, chest pain, abdominal pain.
Management
a) Ipecac or lavage is contraindicated
b) Asymptomatic
ingested GI irritants but non caustic substance (e.g. household bleach) and
demonstrate good oral intake. Give oral fluids as a diluent (10-15ml/kg of
water, milk, etc.). may be followed as outpatients.
c) Symptomatic
i) Stabilize airway
ii) Maintain NPO. Do not pass NG tube BLINDLY
iii) Obtain IV access and start IV fluids
iv) Obtain FBC, GXM, CXR
v) Obtain surgical consultation; prepare for endoscopy.
vi) Consider IV steroid, though controversial; (hydrocortisone at
4mg/kg q6hrly or dexamethasone at 0.4mg/kg/12hrly or
methylprednisolone at 2mg/kg/day divided Q6-8hr )
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
157
13.3.3 IRON POISONING Assessment
1st
stage GI toxicity (30min ~ 6hrs):
Nausea, vomiting, diarrhea, abdominal pain, hematemesis, and malena. Rarely
shock, seiziures,and coma
2nd
stage Latent period (6 ~ 24 hours):
Improvement and sometimes resolution of clinical symptoms.
3rd
stage Systemic toxicity (6 ~ 48 hours) :
Shock ,seizures, cyanosis, lerthargy, coma, hypoglycaemia, metabolic acidosis,
coagulopathy associated with hepatic dysfunction and/or renal failure, and
death.
4th
stage Late complications (4 ~ 8 weeks):
Stricture formation with pyloric or antral stenosis.
Management
i) Determine amount of iron ingested. Abdominal X-ray may be helpful as most
iron tablets are radio-opaque.
ii) If dose of elemental iron < 20mg/kg, no treatment is needed.
iii) For elemental iron 20 – 60mg/kg or ingestion of unknown amount, consider
gastric emptying & give 60ml milk after. If remain asymptomatic in first 6hrs, no
further treatment.
iv) Consider gastric lavage if dose ingested >60mg/kg and/or presence of large
amount of tablets on radiograph. If iron tablets still present in stomach despite
lavage begin whole bowel irrigation, especially if abdominal. X-ray reveals iron
tablets distal to the pylorus.
v) Supportive care is the most important therapy. IV fluids, avoid hypovolemic
shock / acidemia. Maintain urine output >2ml/kg/hr.
vi) Give deferoxamine IV at 15mg/kg/hr via continuous infusion in all cases of
serious poisoning (i.e. presence of significant clinical symptoms, positive abd. X-
ray with significant number of tablets.) up to a total of 80mg/kg/24h. Leave 5g
in 50ml water in the stomach after gastric lavage. Beware of hypotension!!!
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
158
13.3.4 PESTICIDES Common agents
Carbamates e.g. Carbaryl
Organophosphates e.g. Malathion, dimefox, diazirion, TEPP etc.
Organochloride e.g. DDT, benzene hexachloride, lindane etc.
Assessments
• Muscarinic:
Salivation, Lacrimation, Urination, Defecation, gastric Cramping, Emesis (SLUDGE);
brochorrhea, miosis.
• Nicotinic:
Muscle fasciculations, tremor, weakness.
• Central Nervous System (CNS):
Aagitation, seizures, coma.
Treatment
• Decontamination
a. Remove clothing and wash skin with soap and water
b. Gastric lavage if poison swallowed
c. Avoid milk or oils as they enhance absorption
• Aims to support respiration and circulation, to treat acetylcholinesterase inhibition,
control/treat seizures and to prevent hypoglycaemia.
a. Atropine(causes tachycardia, pupils dilatation, reduces bronchorrhea) 0.025mg/kg (min.
dose 0.1mg & max. dose 1mg) Q15min till fully atropinized
b. Pralidoxime (reverse & prevents fasciculations,neuropathy& weakness 20-40mg/kg,
Q6hrly for 24-48hrs.
c. Control seizures with pharmacotherapy e.g. Diazepam.
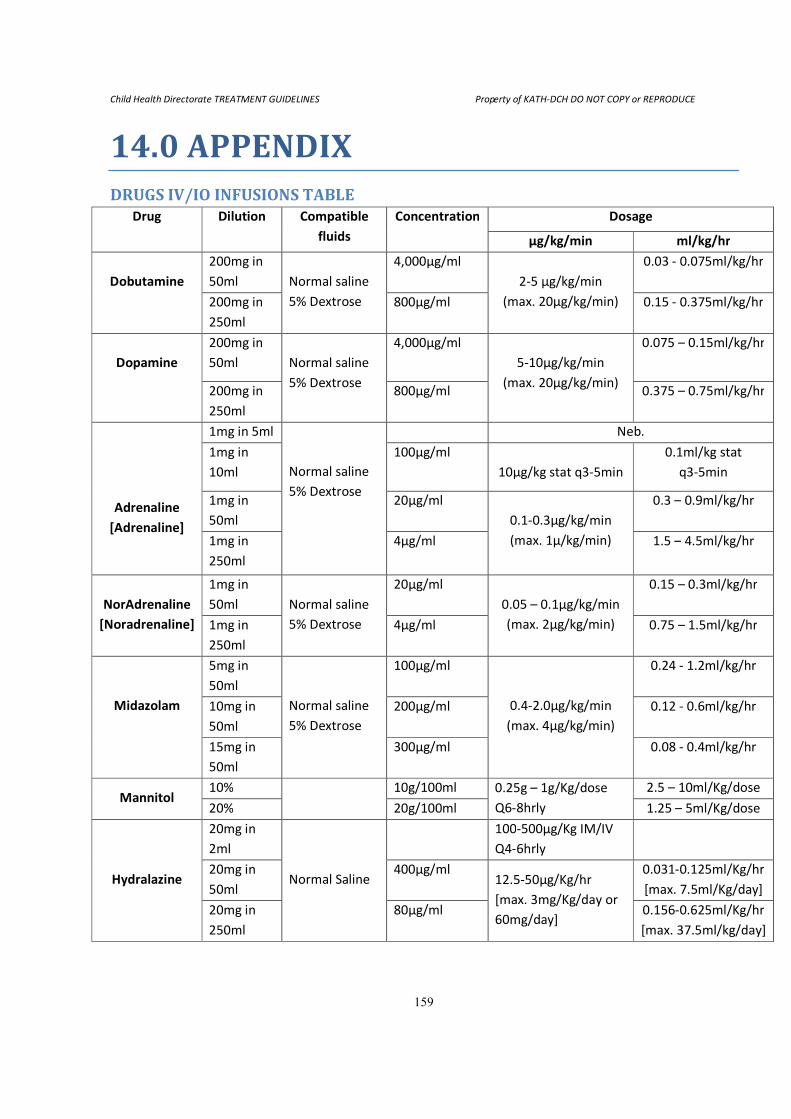
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
159
14.0 APPENDIX DRUGS IV/IO INFUSIONS TABLE
Drug Dilution Compatible
fluids
Concentration Dosage
µg/kg/min ml/kg/hr
Dobutamine
200mg in
50ml
Normal saline
5% Dextrose
4,000µg/ml
2-5 µg/kg/min
(max. 20µg/kg/min)
0.03 - 0.075ml/kg/hr
200mg in
250ml
800µg/ml 0.15 - 0.375ml/kg/hr
Dopamine
200mg in
50ml
Normal saline
5% Dextrose
4,000µg/ml
5-10µg/kg/min
(max. 20µg/kg/min)
0.075 – 0.15ml/kg/hr
200mg in
250ml
800µg/ml 0.375 – 0.75ml/kg/hr
Adrenaline
[Adrenaline]
1mg in 5ml
Normal saline
5% Dextrose
Neb.
1mg in
10ml
100µg/ml
10µg/kg stat q3-5min
0.1ml/kg stat
q3-5min
1mg in
50ml
20µg/ml
0.1-0.3µg/kg/min
(max. 1μ/kg/min)
0.3 – 0.9ml/kg/hr
1mg in
250ml
4µg/ml 1.5 – 4.5ml/kg/hr
NorAdrenaline
[Noradrenaline]
1mg in
50ml
Normal saline
5% Dextrose
20µg/ml
0.05 – 0.1μg/kg/min
(max. 2μg/kg/min)
0.15 – 0.3ml/kg/hr
1mg in
250ml
4µg/ml 0.75 – 1.5ml/kg/hr
Midazolam
5mg in
50ml
Normal saline
5% Dextrose
100µg/ml
0.4-2.0µg/kg/min
(max. 4µg/kg/min)
0.24 - 1.2ml/kg/hr
10mg in
50ml
200µg/ml 0.12 - 0.6ml/kg/hr
15mg in
50ml
300µg/ml 0.08 - 0.4ml/kg/hr
Mannitol 10% 10g/100ml 0.25g – 1g/Kg/dose
Q6-8hrly
2.5 – 10ml/Kg/dose
20% 20g/100ml 1.25 – 5ml/Kg/dose
Hydralazine
20mg in
2ml
Normal Saline
100-500µg/Kg IM/IV
Q4-6hrly
20mg in
50ml
400µg/ml 12.5-50µg/Kg/hr
[max. 3mg/Kg/day or
60mg/day]
0.031-0.125ml/Kg/hr
[max. 7.5ml/Kg/day]
20mg in
250ml
80µg/ml 0.156-0.625ml/Kg/hr
[max. 37.5ml/kg/day]
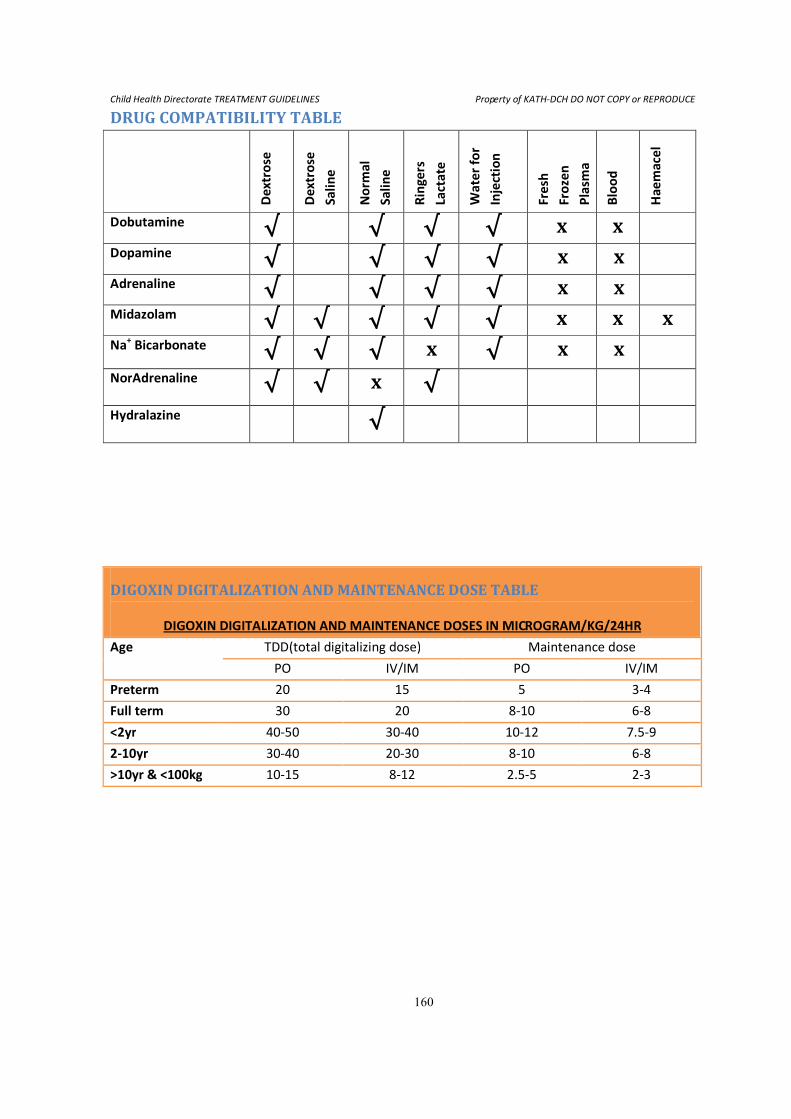
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
160
DRUG COMPATIBILITY TABLE
De
xtr
ose
De
xtr
ose
Sa
lin
e
No
rma
l
Sa
lin
e
Rin
ge
rs
Lact
ate
Wa
ter
for
Inje
ctio
n
Fre
sh
Fro
zen
Pla
sma
Blo
od
Ha
em
ace
l
Dobutamine √ √ √ √ x x Dopamine √ √ √ √ x x Adrenaline √ √ √ √ x x Midazolam √ √ √ √ √ x x x Na
+ Bicarbonate √ √ √ x √ x x
NorAdrenaline √ √ x √
Hydralazine √
DIGOXIN DIGITALIZATION AND MAINTENANCE DOSE TABLE
DIGOXIN DIGITALIZATION AND MAINTENANCE DOSES IN MICROGRAM/KG/24HR
Age TDD(total digitalizing dose) Maintenance dose
PO IV/IM PO IV/IM
Preterm 20 15 5 3-4
Full term 30 20 8-10 6-8
<2yr 40-50 30-40 10-12 7.5-9
2-10yr 30-40 20-30 8-10 6-8
>10yr & <100kg 10-15 8-12 2.5-5 2-3
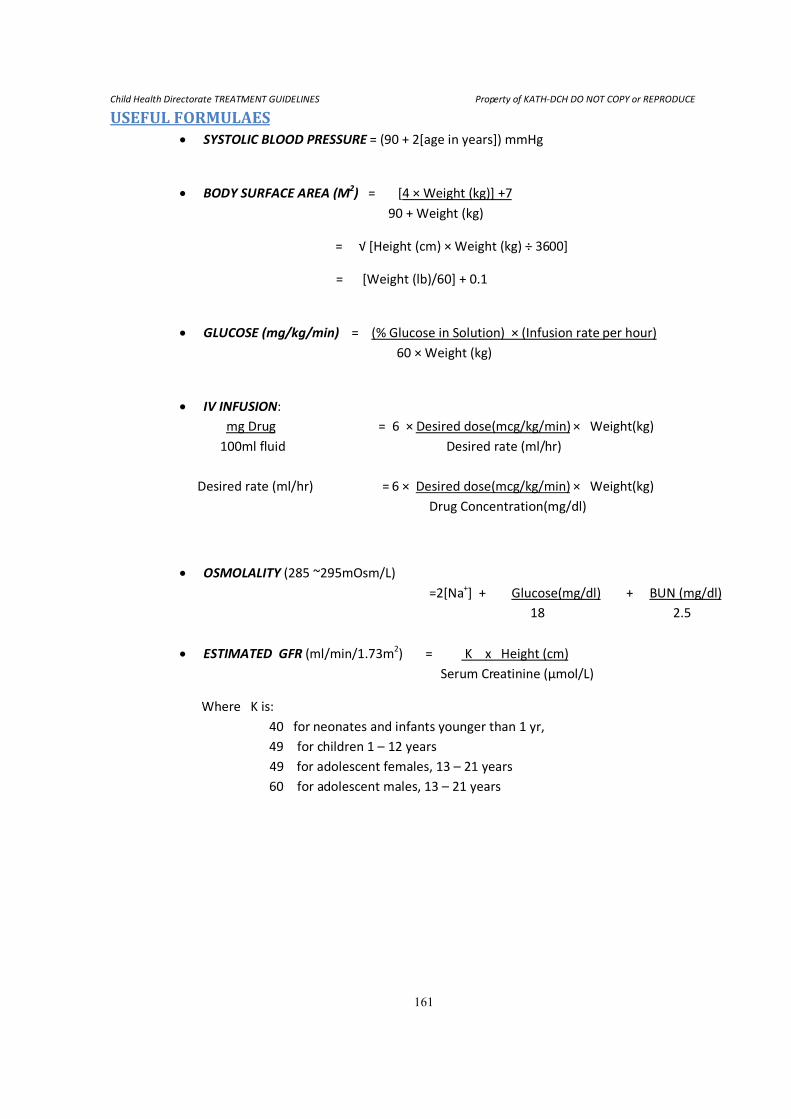
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
161
USEFUL FORMULAES • SYSTOLIC BLOOD PRESSURE = (90 + 2[age in years]) mmHg
• BODY SURFACE AREA (M2) = [4 × Weight (kg)] +7
90 + Weight (kg)
= √ [Height (cm) × Weight (kg) ÷ 3600]
= [Weight (lb)/60] + 0.1
• GLUCOSE (mg/kg/min) = (% Glucose in Solution) × (Infusion rate per hour)
60 × Weight (kg)
• IV INFUSION:
mg Drug = 6 × Desired dose(mcg/kg/min) × Weight(kg)
100ml fluid Desired rate (ml/hr)
Desired rate (ml/hr) = 6 × Desired dose(mcg/kg/min) × Weight(kg)
Drug Concentration(mg/dl)
• OSMOLALITY (285 ~295mOsm/L)
=2[Na+] + Glucose(mg/dl) + BUN (mg/dl)
18 2.5
• ESTIMATED GFR (ml/min/1.73m2) = K x Height (cm)
Serum Creatinine (µmol/L)
Where K is:
40 for neonates and infants younger than 1 yr,
49 for children 1 – 12 years
49 for adolescent females, 13 – 21 years
60 for adolescent males, 13 – 21 years
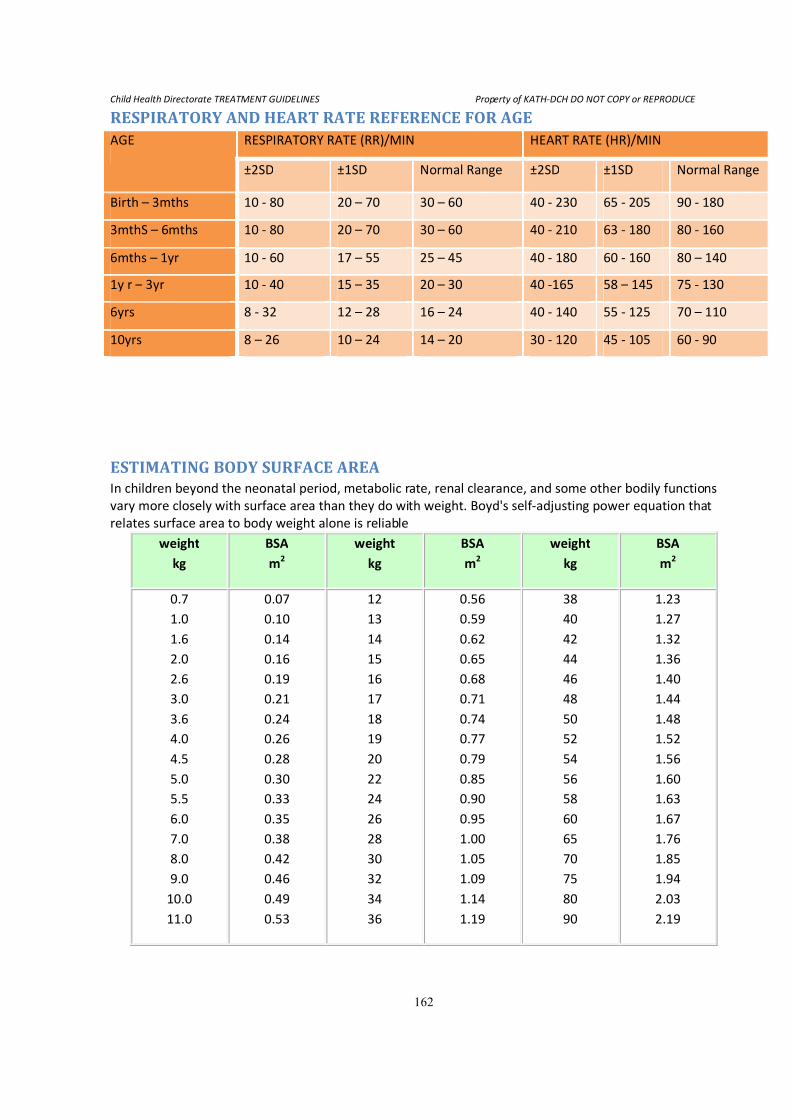
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
162
RESPIRATORY AND HEART RATE REFERENCE FOR AGE AGE RESPIRATORY RATE (RR)/MIN HEART RATE (HR)/MIN
±2SD ±1SD Normal Range ±2SD ±1SD Normal Range
Birth – 3mths 10 - 80 20 – 70 30 – 60 40 - 230 65 - 205 90 - 180
3mthS – 6mths 10 - 80 20 – 70 30 – 60 40 - 210 63 - 180 80 - 160
6mths – 1yr 10 - 60 17 – 55 25 – 45 40 - 180 60 - 160 80 – 140
1y r – 3yr 10 - 40 15 – 35 20 – 30 40 -165 58 – 145 75 - 130
6yrs 8 - 32 12 – 28 16 – 24 40 - 140 55 - 125 70 – 110
10yrs 8 – 26 10 – 24 14 – 20 30 - 120 45 - 105 60 - 90
ESTIMATING BODY SURFACE AREA In children beyond the neonatal period, metabolic rate, renal clearance, and some other bodily functions
vary more closely with surface area than they do with weight. Boyd's self-adjusting power equation that
relates surface area to body weight alone is reliable
weight
kg
BSA
m2
weight
kg
BSA
m2
weight
kg
BSA
m2
0.7
1.0
1.6
2.0
2.6
3.0
3.6
4.0
4.5
5.0
5.5
6.0
7.0
8.0
9.0
10.0
11.0
0.07
0.10
0.14
0.16
0.19
0.21
0.24
0.26
0.28
0.30
0.33
0.35
0.38
0.42
0.46
0.49
0.53
12
13
14
15
16
17
18
19
20
22
24
26
28
30
32
34
36
0.56
0.59
0.62
0.65
0.68
0.71
0.74
0.77
0.79
0.85
0.90
0.95
1.00
1.05
1.09
1.14
1.19
38
40
42
44
46
48
50
52
54
56
58
60
65
70
75
80
90
1.23
1.27
1.32
1.36
1.40
1.44
1.48
1.52
1.56
1.60
1.63
1.67
1.76
1.85
1.94
2.03
2.19
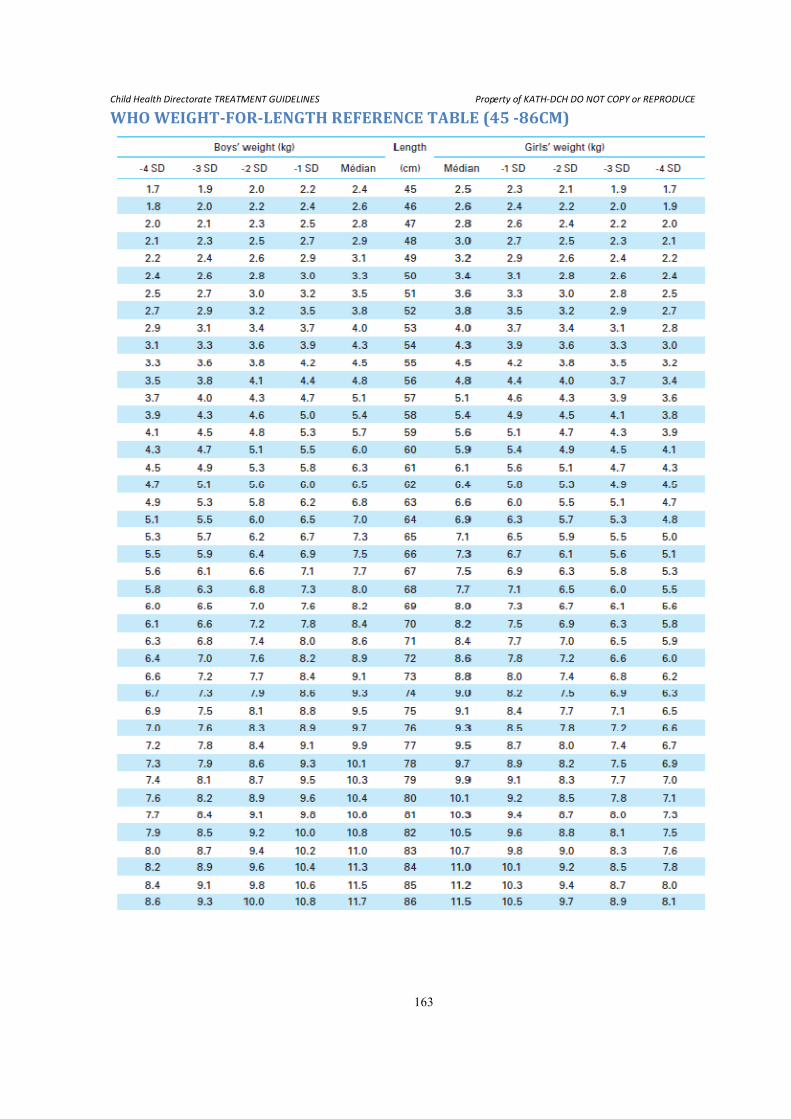
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
163
WHO WEIGHT-FOR-LENGTH REFERENCE TABLE (45 -86CM)
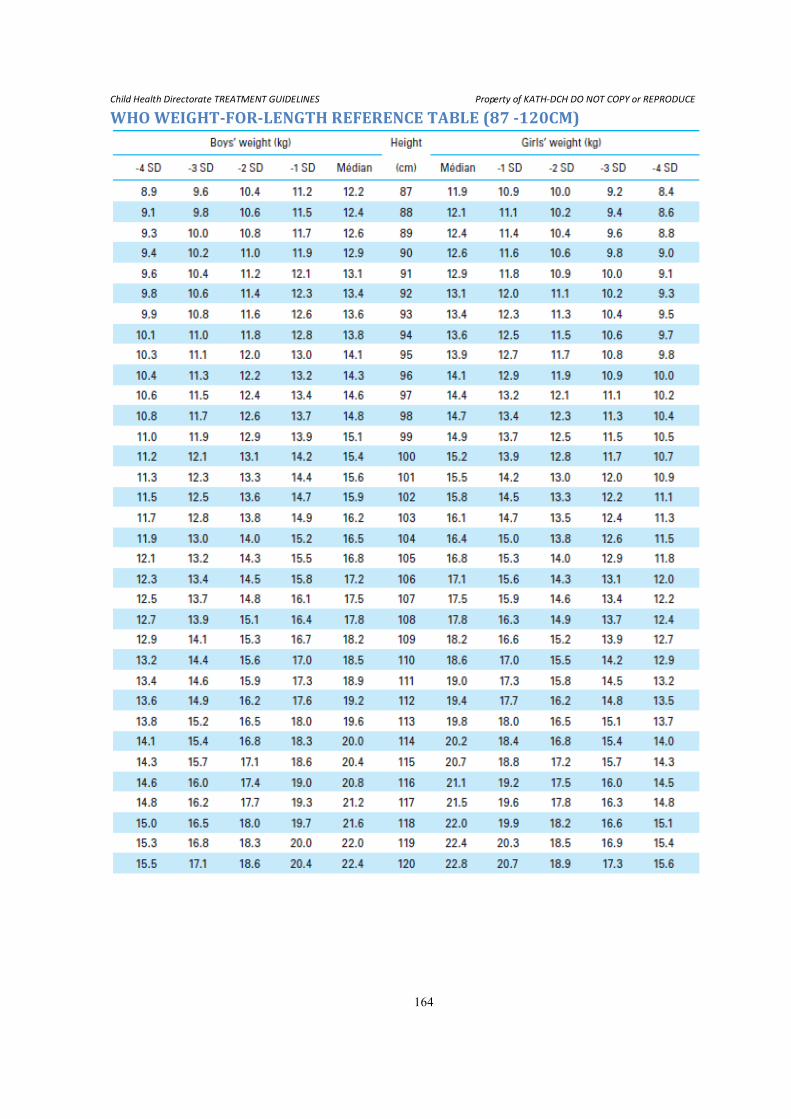
Child Health Directorate TREATMENT GUIDELINES Property of KATH-DCH DO NOT COPY or REPRODUCE
164
WHO WEIGHT-FOR-LENGTH REFERENCE TABLE (87 -120CM)