jpet/2003/055616 revised pparγ agonist provides superior
TRANSCRIPT

JPET/2003/055616 REVISED
PPARγ agonist provides superior renal protection vs. angiotensin converting
enzyme inhibition in a rat model of type 2 diabetes with obesity
by
Chris Baylis, Elke-Astrid Atzpodien, Gary Freshour, and Kevin Engels
Department of Physiology
West Virginia University
Morgantown, WV (C.B., G.F., and K.E.)
and
F. Hoffmann-La –Roche AG
Basel, Switzerland (E-A.A.)
Copyright 2003 by the American Society for Pharmacology and Experimental Therapeutics.
JPET Fast Forward. Published on October 14, 2003 as DOI:10.1124/jpet.103.055616This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
Running Head: PPARγ agonists protect the kidney better than ACEI
Address correspondence to: Chris Baylis, Ph.D.,
Professor of Physiology, POB 9229,
West Virginia University Health Sciences Ctr.
1 Medical Center Drive, Morgantown, WV 26506-9229, USA.
Tel: 304 293 1499. fax: 304 293 3973 email: [email protected]
Number of text pages = 14
Number of tables = 1
Number of Figures = 6
Number of References = 37
Number of words in the Abstract = 228
Number of words in the Introduction = 323
Number of words in the Discussion = 933
Abbreviations:
ACEI angiotensin converting enzyme inhibitors
AT1 angiotensin type 1
BP systemic blood pressure
DN diabetic nephropathy (DN)
ESRD end stage renal disease (ESRD)
GFR glomerular filtration rate
PGC glomerular blood pressure
PPAR γ peroxisome proliferator-activated receptor γ
ΠA colloid osmotic pressure of the plasma).
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
ABSTRACT:
The inbred obese Zucker (ZDF/Gmi, fa/fa) rat develops severe hyperglycemia
and also exhibits severe renal disease. In this study we compared the relative benefits
of long term treatment with angiotensin converting enzyme inhibition (ACEI) to a PPARγ
agonist. Four groups of obese inbred Zucker rats were studied over a 6 month
observation period; untreated animals, rats treated with ACEI alone, rats treated with
PPARγ agonist alone and rats treated with a combination of ACEI and PPARγ agonist.
PPARγ agonist treatment normalized plasma glucose and led to massive increases in
body weight. Both ACEI and PPARγ agonist were effective in reducing the proteinuria
and glomerular and tubular kidney damage. However, the PPARγ agonist exerted
superior renal protection when compared to ACEI, in this model of spontaneously
occurring chronic renal disease (CRD) in the diabetic, obese inbred Zucker rat. Of note,
although ACEI lowered BP, there was no difference in glomerular blood pressure in any
group at the end of the study. The GFR was improved by ACEI with a borderline effect
of PPARγ agonist alone. A mild additive protection on GFR and tubulointerstitial
damage was seen with the combination. Based on the literature it is likely that the
superior protection by PPARγ agonist vs. glomerular and tubular damage as well as
proteinuria extends beyond glycemic and lipidemic control and also reflects direct,
protective intrarenal actions of the PPARγ agonists.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
Diabetic nephropathy (DN) eventually develops in ~ 30% of patients with both
type 1 and type 2 diabetes, and once present will progress in many of these individuals
to end stage renal disease (ESRD). Because of the rapidly increasing prevalence of
type 2 diabetes, this is leading to a massive increase in the incidence of ESRD in the
US and elsewhere (Ritz 1999). Blockade of the angiotensin system is currently the
standard treatment for slowing progression of renal disease in diabetic nephropathy
(DN) (Hollenberg 2002), although this has no inherent beneficial effect on the diabetes.
Where angiotensin converting enzyme inhibitors (ACEI) were first used, these are now
being replaced, or supplemented with angiotensin type 1 (AT1) receptor blockers.
Nevertheless, the incidence of DN in type 2 diabetes continues to increase (Ritz 1999).
In recent years it has also become evident that prolonged tight glycemic control
slows down progression of DN in type 1 diabetics (DCCT 1995) and some (but not all)
studies suggest that good metabolic control is protective to DN in type 2 diabetes (Di
Landro et al 1998). The recent development of the peroxisome proliferator-activated
receptor γ (PPAR γ) agonists has provided a novel means of improved glycemic control.
These drugs (the thiazolidinediones) enhance sensitivity of the peripheral insulin
receptor to glucose in type 2 diabetes, leading to reduced plasma glucose and insulin
levels and reductions in glycosylated Hb. These drugs also exert a beneficial effect on
the lipid profile, are antihypertensive and inhibit collagen type 1 production by the
glomerular mesangial cells ( Rosak 2002; Guan and Breyer 2001).
The present study was conducted to test the relative benefit of long term (6
month) ACEI vs. PPAR γ agonist therapy as well as in combination, in a rat model of
severe type 2 diabetes, the inbred obese Zucker (ZDF/Gmi, fa/fa) rat. When untreated
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
these rats develop marked kidney damage compared to their lean littermates (Vora et
al., 1996; Baylis 2001).
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
METHODS:
Studies were conducted on 30 inbred obese male Zucker (ZDF/Gmi, fa/fa) rats
purchased from Genetic Models, Inc., Indianapolis, at age 5 weeks. Baseline
measurements of blood glucose and urinary protein excretion (see below) were made at
6 weeks of age and at 8 weeks of age rats were randomized to one of the following 4
groups and followed for 6 months: 1). Controls (n=9), 2). Rats treated with PPAR γ
agonist rosiglitazone (Rosi, oral; 3mg/Kg/d) (n=6), 3). Rats treated with ACE inhibitor
cilazapril (Cil, oral 10mg/kg/d) (n=9), 4). Rats treated with both drugs (n=6). For the two
different drugs, submaximally effective doses were selected based on their specific
pharmacologic effects (reduction of insulin
resistance for PPARγ agonist; antihypertensive effect for ACEI).
One Rosi treated and 2 control rats died during the 6 month observation period and
were not included in any analysis. Body weight and water intakes were measured every
48 hours and the drug concentration adjusted according to water consumption, to give a
constant dose of drug.
All rats were allowed water and were fed Purina 5008 diet ad lib, to maintain a
hyperglycemic state in the obese rats. Eight hour urine collections were made at
monthly intervals and urine frozen for later analysis. Tail vein blood samples were
taken at 2 monthly intervals during the study for analysis of blood glucose and BUN.
After 6 months observation, rats were prepared for terminal acute micropuncture studies
for measurement of glomerular blood pressure and renal hemodynamics. Anesthesia
was induced with ip Inactin; for the grossly obese rats treated with Rosi, an induction
dose of 180mg/kg BW was given followed by frequent iv supplementation (40mg/kg), as
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
needed. Controls and Cil alone treated rats received the regular ip induction dose of
120mg/kg with iv supplementation at 20mg/kg, as required. Both jugular veins were
catheterized, one for iv Inactin and one for an infusion of 0.9% NaCl (~0.5% BW) + 3H-
inulin (2 µC/ml) and PAH (0.5g/100ml) was infused at 50µl/kg BW via T piece. Before
starting the NaCl/ inulin/ PAH infusion, an arterial cannula was placed in the right carotid
artery and a 0.2ml blood sample was removed for later estimation of plasma creatinine.
Then the trachea was cannulated, the abdomen opened by a ventral midline incision
and the urinary bladder was catheterized. The perirenal fat was gently cleared from the
left kidney and the kidney was stabilized for micropuncture as described previously
(Deng and Baylis 1995). Paraffin wax blocks were inserted into 5-12 midproximal
tubule segments on the kidney surface, so that stop-flow pressure (Psf) could be
measured proximal to the block.
After an initial bolus and 40 min infusion (~2ml/h) of a solution of 0.9% NaCl
containing 3H-inulin and PAH (PAH concentration in the infusate was varied according
to the group so that plasma PAH was always below 4mg/dl), 2 timed 15 –20 min urine
collections were made with midpoint arterial blood samples (0.2ml). During whole
kidney clearance periods, measurements were made of Psf and free flow proximal
tubule pressure. Then the rat was sacrificed and the kidneys, heart, liver and pancreas
were removed and fixed in 10% buffered formalin for at least 24h for later histologic and
immunohistologic analysis (kidneys only). Measurement of urine creatinine was by
Sigma kits # 555. Blood glucose was measured by Sigma’s glucose Trinder reagent
(Trinder 1969). PAH was analyzed colorimetrically, 3H-inulin activity was determined by
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
scintillation counting and plasma protein concentration by refractometer, as described
previously (Deng and Baylis 1995; Smith et al., 1945).
For histology and immunohistochemistry, kidneys were trimmed, processed and
embedded in Paraplast. Kidney sections (2-3 µm thick) were cut and stained with
hematoxylin and eosin (HE) or periodic acid Schiff reagent (PAS). Immunostaining for
expression of CD 68 using the monoclonal antibody Ki-M6 specific for
monocytes/macrophages (BMA T-1005, 1:100 dilution, Biomedicals AG, Switzerland)
(Parwaresch et al., 1986) was performed on kidney sections of 4 animals each per
treatment group. An avidin biotin peroxidase complex technique was applied according
to the manufacturer’s specifications (ready-to-use detection kits and an automated slide
stainer, Ventana Medical System, Strasbourg, France). Renal changes were scored on
a scale of 1+ to 4+ (1+ = minimal, 2+ = slight, 3+ = moderate, 4+ = marked to massive)
as adapted from Zbinden (1976). Tubulointerstitial changes were defined as tubular
degeneration, regeneration and/or atrophy, tubular dilation, hyaline casts, interstitial
inflammatory infiltrates or fibrosis. In addition, for quantification of glomerular sclerosis,
kidney sections (5 µm thick) were cut and stained with PAS as described by us earlier
(Deng and Baylis 1995). Glomerular sclerosis was defined as segmental or global
increases in glomerular matrix, accumulation of hyaline material, and loss of local
capillary organization. All data are given as mean ±SE. Statistical significance was
assumed when p<0.05, using one- and two way ANOVA and Wilcoxon Rank sum test
for quantitative assessment of glomerular injury. All other pathology findings were
expressed as “summary incidence of grading” for each finding.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
RESULTS
As shown in Figure 1 blood glucose was normal in obese rats at 6-8 weeks of
age (time 0) but rose markedly in untreated animals and reached a stable elevated level
by age 14 –16 weeks (month 2). A similar profile was seen in the rats treated with ACEI
whereas blood glucose remained normal in both groups of rats receiving PPARγ
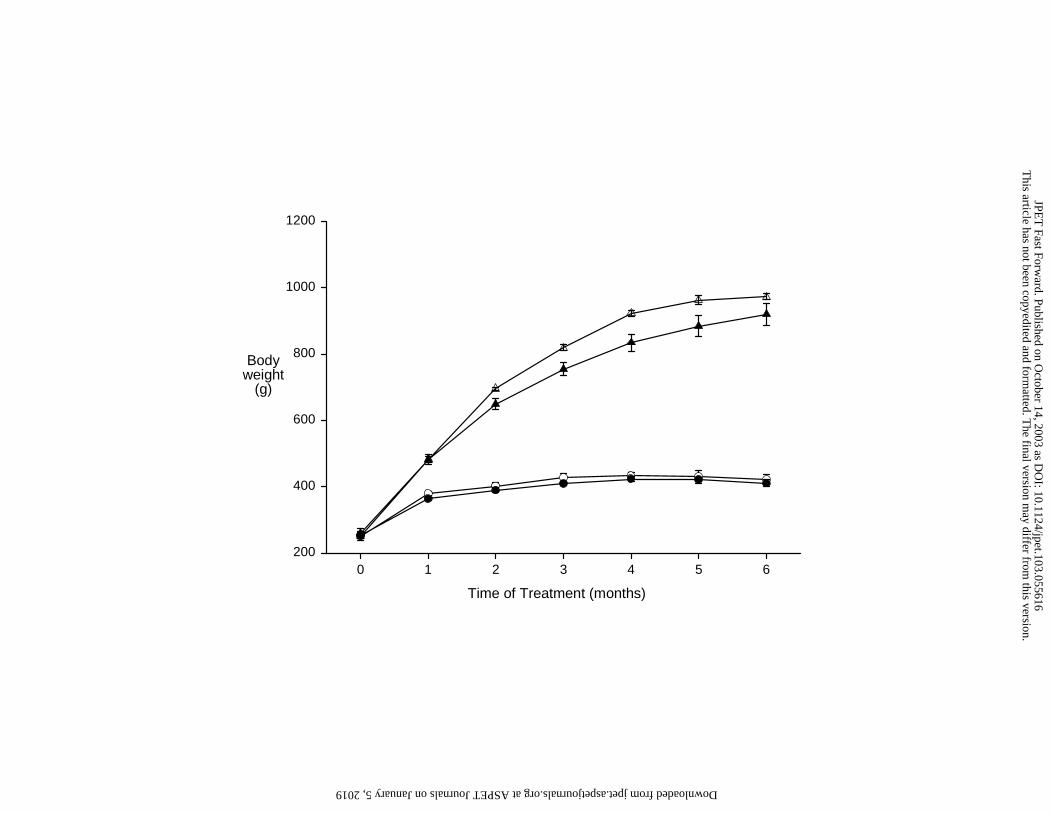
agonist. All PPARγ agonist treated rats were massively obese and body weight
increased profoundly over the 6 month treatment period (Figure 2) in some cases
exceeding 1kg prior to sacrifice. In contrast, the untreated rats and rats given ACEI
alone, showed only moderate weight gain with age. We did not evaluate body
composition but the 24h urinary creatinine excretion gives an index of skeletal muscle
mass. The absolute values were similar in all 4 groups but when factored for body
weight creatinine excretion was significantly higher in untreated or ACEI treated rats
(33.1±3.5 and 29.1±1.6 mg/24h/kgBW) vs. those given PPARγ agonist alone or in
combination (11.8±2.3 and 13.4±2.4; p vs. untreated <0.001 for both), suggesting
greatly increased % of adipose tissue in the PPARγ agonist treated animals.
Unfortunately the high, variable levels of plasma lipids prevented meaningful plasma
creatinine measurements.
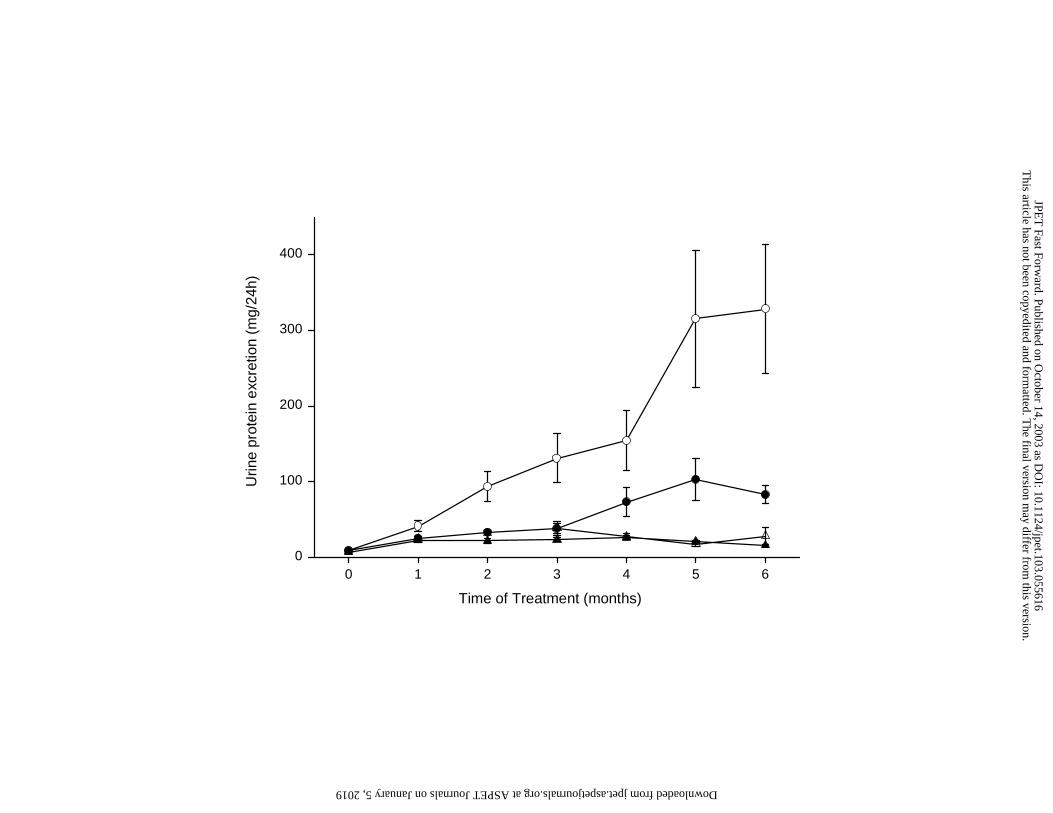
The total urine protein excretion rose markedly in the untreated rats, reflecting
development of progressive kidney damage (Figure 3) and was significantly higher
(p<0.05) than all other groups at 6 months of observation. The ACEI was effective in
reducing urinary protein excretion although significant proteinuria (p<0.01 vs. both
PPAR Groups) was still evident after 6 months treatment. In contrast, rats given PPARγ
agonist (either +/- ACEI), developed no proteinuria over the entire treatment period.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
Histologic evaluation of the kidneys revealed pronounced glomerular sclerosis in
untreated rats with some level of injury in 26±1 % of glomeruli. Rats receiving ACEI
alone had less damage (17±1 %; p<0.05 vs. control) but this was still greater than in
either of the PPARγ agonist treated groups (PPARγ agonist alone, 9±1 % damaged
glomeruli; p<0.01 vs. ACEI alone, and PPARγ agonist + ACEI, 10±1 %; p<0.01 vs. ACEI
alone). Figure 4 shows that in addition to a higher % of the total glomeruli being
affected by damage, the grade of injury is also greater in the untreated rats, with
significantly more 3+ and 4+ damage vs. ACEI alone (p<0.05), who in turn have more
2+, 3+ and 4+ injury (p<0.05) than either PPARγ agonist treated group.
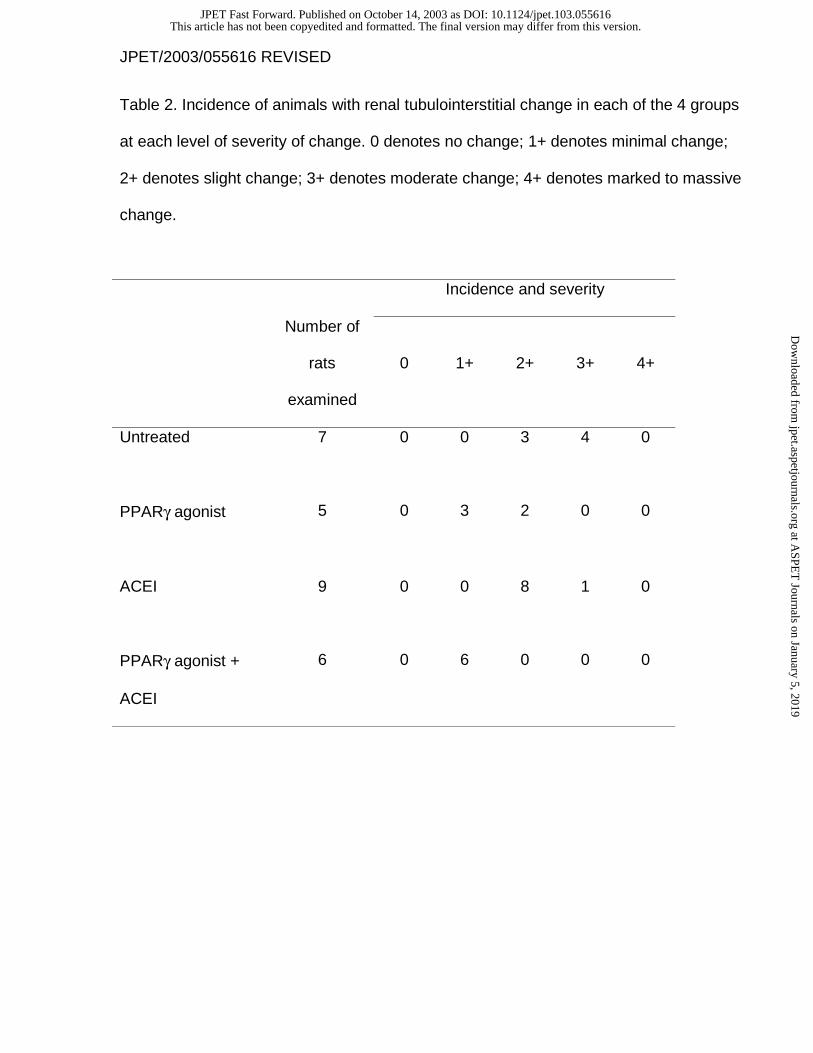
In untreated rats, in addition to pronounced glomerular sclerosis, moderate
tubulointerstitial changes were observed. These consisted of tubular atrophy,
degeneration and regeneration, tubular dilation, hyaline casts, and interstitial
mononuclear cell infiltrates and fibrosis. Slight epithelial cell vacuolation was observed
in distal tubules. These vacuolated cells appeared as swollen, clear cells with prominent
cell boundaries and condensed nuclei. (Figure 5, panel A). Treatment with either
PPARγ agonist or ACEI alone or with a combination of both drugs clearly reduced the
development of renal lesions (Figure 5, panels B-D). In addition to the drug-induced
reduction in the incidence and severity of glomerular sclerosis, associated
tubulointerstitial changes were improved in parallel. The tubulointerstitial protection was
greater in rats receiving a combination of PPARγ agonist and ACEI than in animals
given PPARγ alone, and was the least pronounced in animals receiving ACEI alone.
Treatment with PPARγ agonist alone or in combination with ACEI completely inhibited
development of tubular epithelial cell vacuolation. In contrast, treatment with ACEI alone
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
had no impact on the incidence and severity of tubular epithelial cell vacuolation. The
incidence of cells expressing CD 68 within the glomeruli using the
monocyte/macrophage marker Ki M6 (Parwaresch et al., 1986) was slight in untreated
rats, minimal in rats given PPARγ agonist alone or ACEI alone, and absent in rats
receiving the combination of ACEI and PPARγ agonist. Hyperplasia of the
juxtaglomerular apparatus (JGA) was minimal in rats given ACEI as reported by others
(Owen and Molon-Noblot 1998) and was marked in rats receiving the combination of
ACEI and PPARγ agonist, with the change extending along afferent arterioles to affect
interlobular arteries. The reason for this greater severity of hyperplasia of the JGA in
the combination group is unknown. Pelvic dilation was present in untreated rats and in
all drug-treated groups to a similar extent.
The data given in Table 1 were derived from the acute study conducted at the
end of the 6 month treatment period. Arterial Hct was lower in both groups of rats
receiving PPARγ agonist than in untreated or ACEI treated rats and since the PPAR γ
agonists are reported to produce fluid retention (Lebovitz 2002), this may account for
the lower Hct although there were no differences in plasma protein concentration or the
colloid osmotic pressure of the plasma (ΠA). Untreated rats had elevated systemic BP
but normal glomerular BP (PGC) while ACEI alone or with PPARγ agonist lowered
systemic BP without altering PGC, which remained normal. The group receiving PPARγ
agonist alone had an elevated BP similar to untreated rats and PGC was also similar to
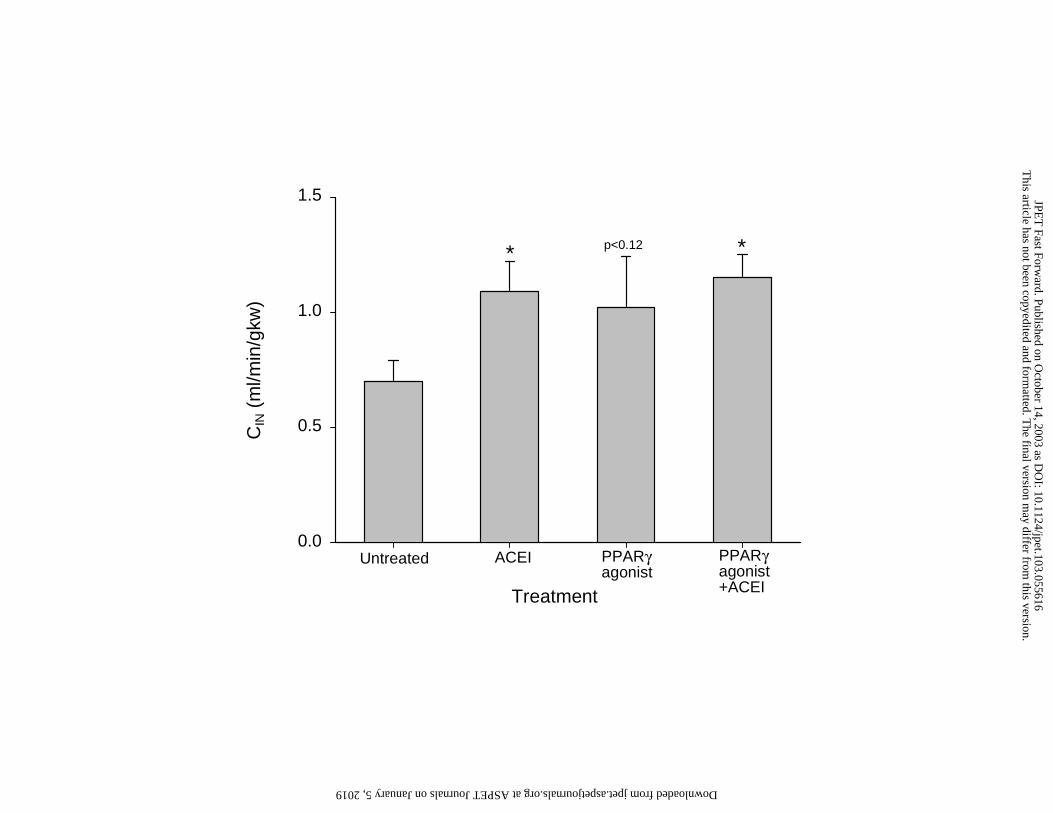
other groups. The inulin clearance was lowest in untreated rats and GFR significantly
improved in rats given ACEI alone or with PPARγ agonist. There was a borderline
improvement with PPARγ agonist alone (Figure 6).
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
DISCUSSION
There was a clear benefit in treatment with either the PPARγ agonist or ACEI in
reducing the structural and functional changes in the kidney in this rat model of obesity
and type 2 diabetes. The main finding of the present study was that PPARγ agonist
gave better protection vs. ACEI on both proteinuria (p<0.005) and glomerular sclerosis
(p<0.02) in association with improved metabolic control. There was an additive
protection against tubulointerstitial damage and macrophage/ monocyte infiltration, a
borderline improvement of GFR and no additional benefit on proteinuria and glomerular
sclerosis when the PPARγ agonist was combined with ACEI vs. PPARγ agonist alone.
The inbred obese Zucker (ZDF/Gmi fa/fa) rat fed the Purina 5008 diet develops severe
diabetes and extensive kidney damage. However, the renal damage does not exhibit all
the characteristics of diabetic nephropathy. In remaining intact glomeruli there is no
evidence of mesangial expansion or thickening of the glomerular basement membrane
and the lesions seen were more indicative of focal segmental glomerular sclerosis
(Baylis 2001). In addition, this inbred strain of Zucker rats has a genetic predisposition
to develop hydronephrosis, seen to an equal extent in both obese and lean rats (Vora et
al., 1996; Baylis 2001). However, most likely the majority of the renal injury in the
obese inbred Zucker rats is due to the metabolic disturbances, since the present study
demonstrates that chronic treatment with PPARγ agonist prevents the proteinuria and
structural damage.
Given the wide range of actions of the PPARγ agonists there are a number of
possible mechanisms for the superior renal protection seen here. The glycemic control
is undoubtedly a factor since hyperglycemia exerts multiple damaging actions on the
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
kidney (Phillips et al., 1995; West 2000; Larkins and Dunlop 1992; Brownlee et al.,
1988) and good glycemic control is renoprotective in clinical studies in diabetics (DCCT
1995; Di Landro et al., 1998). The vacuoles seen in the renal distal tubular epithelial
cells of untreated rats were probably the result of abnormal accumulation of glycogen
(resembling Armanni-Ebstein lesion) widely seen in renal tubules of diabetics. PPARγ
agonist treatment completely eradicated these reflecting the normalization of blood
glucose (Wehner 1998). Furthermore, experimentally induced hyperglycemia (with
streptozotocin) in normoglycemic, hyperinsulinemic outbred Zucker rats, causes early
glomerular hypertrophy (Park and Meyer 1995), a key event in progression of CRD
(Daniels and Hostetter 1990). Indeed, glomerular hypertrophy is reported as an early
pathological event in obese Zucker fa/fa and ZDF rats (Coimbra et al., 2000; Hoshi et
al., 2002).
In addition to the hyperglycemia, the untreated obese Zucker rats exhibit severe
hyperlipidemia and dyslipidemia, with LDL cholesterol and triglycerides at 20X that seen
in leans (Baylis 2001). Hyperlipidemia is one likely stimulus underlying progressive
podocyte damage and subsequent glomerular sclerosis in fa/fa rats (Coimbra et al.,
2000). Although not measured in the present study, the lipid lowering actions of the
PPARγ agonist (Rosak 2002; Guan and Breyer 2001) likely contributed to the improved
protection compared to rats treated with ACEI alone. In the outbred Zucker rat that is
not frankly hyperglycemic, chronic treatment with lipid lowering agents affords
considerable protection (Kasiske et al., 1992).
Systemic hypertension is another risk factor for development of kidney disease
and BP was elevated in the untreated inbred obese Zucker rats in the present study. Of
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
note, however, the glomerular blood pressure (PGC) was not elevated and although rats
receiving ACEI alone exhibited a significant fall in BP, PGC was not lowered.
Furthermore, the rats receiving PPARγ agonist alone showed no change in either BP or
PGC despite the fact that these animals enjoyed superior renoprotection vs. those given
ACEI alone. These findings suggest that glomerular hypertension was not an important
contributory factor in this model of renal disease.
Several groups have reported that the thiazolidinediones protect the kidney in rat
models of type 1 and type 2 diabetes (Fujii et al., 1997; Buckinham et al., 1998;
McCarthy et al., 2000). In addition to the improved metabolic control it is possible that
PPARγ agonists have more direct beneficial actions on the kidney since constitutively
expressed PPARγ are found in glomeruli, particularly mesangial cells (Guan et al., 2001;
Asano et al., 2000; Nicholas et al., 2001) and PPARγ agonists reduce type I collagen
synthesis in cultured glomerular mesangial cells (Routh et al., 2002; Zheng et al., 2002).
In addition to directly inhibiting glomerular collagen synthesis, PPARγ agonist may also
act indirectly, via its anti-inflammatory action. Glomerular sclerosis positively correlates
with the occurrence of interstitial and glomerular monocytes/ macrophages and
activated mesangial cells (Young et al., 1995; Nikolic-Paterson et al., 1994; Lavaud et
al., 1996). In the present study, the incidence of cells expressing CD 68 within the
glomeruli (determined with the monocyte/macrophage marker Ki-M6), is blunted with
either the ACEI or PPARγ agonist alone, and was absent in rats given PPARγ agonist in
combination with ACEI. Thus both PPARγ agonists and ACEI might act via inhibition of
recruitment or activation of these cells. In fact, PPARγ agonists are protective in the
non-diabetic, 5/6th renal ablation model of glomerulosclerosis (Ma et al., 2001) and exert
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
direct anti-inflammatory and antiproliferative actions on the circulation (Ishibashi et al.,
2002), suggesting that the renal protective actions extend beyond improvement of the
metabolic profile.
Overall, long-term administration of the PPARγ agonist was found to be
powerfully protective in the complex model of CRD seen in the inbred obese Zucker rat.
One disadvantage of the PPARγ agonists is that they potently stimulate adipocyte
formation (Rosak 2002; Guan and Breyer 2001) leading to massive obesity. Of note,
however, this obesity is not, in itself, damaging to the kidneys, since rats in the present
study that received PPARγ agonist were massively obese without kidney damage. In
fact the PPARγ agonist treated rats seemed “healthy” despite massive obesity.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
ACKNOWLEDGEMENTS. The excellent technical assistance of Lennie Samsell and
Agnes Klumpp is gratefully acknowledged.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
REFERENCES
Asano T, Wakisaka M, Yoshinari M, Iino K, Sonoki K, Iwase M and Fujishima M (2000)
Peroxisome proliferator-activated receptor gamma1 (PPARgamma1) expresses in rat
mesangial cells and PPARgamma agonists modulate its differentiation. Biochim
Biophys Acta 1497:148-154.
Baylis C (2001) Inbred Zucker obese rats: A model of type II diabetic nephropathy (DN).
J Am Soc Nephrol 12:831A.
Brownlee M, Cerami A and Vlassara H (1988) Advanced glycosylation end products in
tissue and the biochemical basis of diabetic complications. N Engl J Med 318:1315-
1321.
Buckingham RE, Al Barazanji KA, Toseland CD, Slaughter M, Connor SC, West A,
Bond B, Turner NC and Clapham JC (1998) Peroxisome proliferator-activated receptor-
gamma agonist, rosiglitazone, protects against nephropathy and pancreatic islet
abnormalities in Zucker fatty rats. Diabet 47:1326-1334.
Coimbra TM, Janssen U, Grone HJ, Ostendorf T, Kunter U, Schmidt H, Brabant G and
Floege J (2000) Early events leading to renal injury in obese Zucker (fatty) rats with type
II diabetes. Kidney Int 57:167-182.
Daniels BS and Hostetter TH (1990) Adverse effects of growth in the glomerular
microcirculation. Am J Physiol 258:F1409-F1416.
Deng A and Baylis C (1995) Glomerular hemodynamic responses to pregnancy in rats
with severe reduction of renal mass. Kidney Int 48:39-44.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
Di Landro D, Catalano C, Lambertini D, Bordin V, Fabbian F, Naso A and Romagnoli
GF (1998) The effect of metabolic control on development and progression of diabetic
nephropathy. Nephrol Dial Transplant 13 Suppl 8:35-43.
Fujii M, Takemura R, Yamaguchi M, Hasegawa G, Shigeta H, Nakano K and Kondo M
(1997) Troglitazone (CS-045) ameliorates albuminuria in streptozotocin-induced
diabetic rats. Metab 46:981-983.
Guan Y and Breyer MD (2001) Peroxisome proliferator-activated receptors (PPARs):
Novel therapeutic targets in renal disease. Kidney Int 60:14-30.
Guan Y, Zhang Y, Schneider A, Davis L, Breyer RM and Breyer MD (2001) Peroxisome
proliferator-activated receptor-gamma activity is associated with renal microvasculature.
Am J Physiol Renal Physiol 281:F1036-F1046.
Hollenberg NK (2002) AT(1)-receptor blockade and the kidney: Importance of non-ACE
pathways in health and disease. J Hum Hypertens 16 Suppl 3:S59-S63.
Hoshi S, Shu Y, Yoshida F, Inagaki T, Sonoda J, Watanabe T, Nomoto K and Nagata M
(2002) Podocyte injury promotes progressive nephropathy in Zucker diabetic fatty rats.
Lab Invest 82:25-35.
Ishibashi M, Egashira K, Hiasa K, Inoue S, Ni W, Zhao Q, Usui M, Kitamoto S, Ichiki T
and Takeshita A (2002) Anti-inflammatory and antiarteriosclerotic effects of
pioglitazone. Hypertens 40:687-693.
Kasiske BL, O'Donnell MP and Keane WF (1992) The Zucker rat model of obesity,
insulin resistance, hyperlipidemia, and renal injury. Hypertens 19:I110-I115.
Larkins RG and Dunlop ME (1992) The link between hyperglycaemia and diabetic
nephropathy. Diabetologia 35:499-504.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
Lavaud S, Michel O, Sassy-Prigent C, Heudes D, Bazin R, Bariety J and Chevalier J
(1996) Early influx of glomerular macrophages precedes glomerulosclerosis in the
obese Zucker rat model. J Am Soc Nephrol 7:2604-2615.
Lebovitz HE (2002) Differentiating members of the thiazolidinedione class: a focus on
safety. Diabetes Metab Res Rev 18 Suppl 2:S23-S29.
Ma LJ, Marcantoni C, Linton MF, Fazio S and Fogo AB (2001) Peroxisome proliferator-
activated receptor-gamma agonist troglitazone protects against nondiabetic
glomerulosclerosis in rats. Kidney Int 59:1899-1910.
McCarthy KJ, Routh RE, Shaw W, Walsh K, Welbourne TC and Johnson JH (2000)
Troglitazone halts diabetic glomerulosclerosis by blockade of mesangial expansion.
Kidney Int 58:2341-2350.
Nicholas SB, Kawano Y, Wakino S, Collins AR and Hsueh WA (2001) Expression and
function of peroxisome proliferator-activated receptor- gamma in mesangial cells.
Hypertens 37:722-727.
Nikolic-Paterson DJ, Lan HY, Hill PA and Atkins RC (1994) Macrophages in renal injury.
Kidney Int Suppl 45:S79-S82.
Owen RA and Molon-Noblot S (1998) Juxtaglomerular cell hyperplasia induced
laboratory animals, in Monographs on pathology of laboratory animals urinary system
(Jones TC, Hard GC and Mohr U eds)
Park SK and Meyer TW (1995) The effect of hyperglycemia on glomerular function in
obese Zucker rats. J Lab Clin Med 125:501-507.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
Parwaresch MR, Radzun HJ, Kreipe H, Hansmann ML and Barth J (1986)
Monocyte/macrophage-reactive monoclonal antibody Ki-M6 recognizes an
intracytoplasmic antigen. Am J Pathol 125:141-151.
Phillips AO, Steadman R, Topley N and Williams JD (1995) Elevated D-glucose
concentrations modulate TGF-beta 1 synthesis by human cultured renal proximal
tubular cells. The permissive role of platelet-derived growth factor. Am J Pathol
147:362-374.
Ritz E (1999) Nephropathy in type 2 diabetes. J Intern Med 245:111-126.
Rosak C (2002) The pathophysiologic basis of efficacy and clinical experience with the
new oral antidiabetic agents. J Diabetes Complications 16:123-132.
Routh RE, Johnson JH and McCarthy KJ (2002) Troglitazone suppresses the secretion
of type I collagen by mesangial cells in vitro. Kidney Int 61:1365-1376.
Smith HW, Finkelstein N, Aliminosa L, Crawford B and Graber M ((1945) The renal
clearances of substituted hippuric acid derivatives and other aromatic acids in dog and
man. J Clin Invest 42:388-404.
The Diabetes Control and Complications (DCCT) Research Group (1995) Effect of
intensive therapy on the development and progression of diabetic nephropathy in the
diabetes control and complications trial. Kidney Int 47:1703-1720.
Trinder P (1969) Determination of blood glucose using 4-amino phenazone as oxygen
acceptor. J Clin Pathol 22:246.
Vora JP, Zimsen SM, Houghton DC and Anderson S (1996) Evolution of metabolic and
renal changes in the ZDF/Drt-fa rat model of type II diabetes. J Am Soc Nephrol 7:113-
117.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
Wehner H (1998) Effect of Experimental diabetes mellitus, kidney, rat, in Monographs
on pathology of laboratory animals urinary system (Jones TC, Hard GC and Mohr U
eds) pp 283-289, Springer & Heidelberg, Berlin.
West IC (2000) Radicals and oxidative stress in diabetes. Diabet Med 17:171-180.
Young BA, Johnson RJ, Alpers CE, Eng E, Gordon K, Floege J, Couser WG and Seidel
K (1995) Cellular events in the evolution of experimental diabetic nephropathy. Kidney
Int 47:935-944.
Zheng F, Fornoni A, Elliot SJ, Guan Y, Breyer MD, Striker LJ and Striker GE (2002)
Upregulation of type I collagen by TGF-beta in mesangial cells is blocked by
PPARgamma activation. Am J Physiol Renal Physiol 282:F639-F648.
Zbinden G. (1976) The role of pathology in toxicity testing. In: Progress in toxicology.
Special topics. Volume 2, pp. 8-18 Springer-Verlag Berlin, Heidelberg, New York, Tokyo
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
FOOTNOTES
These studies were supported by funds from F. Hoffmann-La Roche AG, Basel, Switzerland.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
Table 1. Data obtained during micropuncture of inbred obese male Zucker
(ZDF/Gmi, fa/fa) studied at ~ 8months of age after 6 months of no treatment,
angiotensin converting enzyme inhibition (ACEI), peroxisome proliferator-
activated receptor γ agonist (PPARγ) alone or in combination with ACEI.
* denotes a significant difference (p<0.05) vs. untreated rats.
Hct vol/dl CA, g/dl ΠA, mmHg BP, mmHg PGC,
mmHg
Untreated 48±1 5.6±0.2 18±1 144±2 55±4
+ACEI 50±1 5.7±0.3 19±1 120±4* 49±1
+PPARγ 43±1* 6.1±0.3 21±2 130±5 53±3
+PPARγ/ACEI 41±1* 6.2±0.1* 21±1 100±8* 52±4
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
Table 2. Incidence of animals with renal tubulointerstitial change in each of the 4 groups
at each level of severity of change. 0 denotes no change; 1+ denotes minimal change;
2+ denotes slight change; 3+ denotes moderate change; 4+ denotes marked to massive
change.
Incidence and severity
Number of
rats
examined
0
1+
2+
3+
4+
Untreated
7 0 0 3 4 0
PPARγ agonist
5 0 3 2 0 0
ACEI
9 0 0 8 1 0
PPARγ agonist +
ACEI
6 0 6 0 0 0
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from
JPET/2003/055616 REVISED
FIGURE LEGENDS
Figure 1.
The plasma glucose (mg/dl) at 6-8 weeks of age (prior to initiation of treatment) and
over the 6 month observation period in untreated (open circles), ACEI treated (closed
circles), PPARγ agonist treated (open triangles) and PPARγ agonist + ACEI treated
(closed triangles) rats.
Figure 2.
The body weight (g) at 6-8 weeks of age (prior to initiation of treatment) and over the 6
month observation period in untreated (open circles), ACEI treated (closed circles),
PPARγ agonist treated (open triangles) and PPARγ agonist + ACEI treated (closed
triangles) rats.
Figure 3
The total urinary protein excretion (mg/24h) at 6-8 weeks of age (prior to initiation of
treatment) and over the 6 month observation period in untreated (open circles), ACEI
treated (closed circles), PPARγ agonist treated (open triangles) and PPARγ agonist +
ACEI treated (closed triangles) rats.
Figure 4.
The % of damaged glomeruli in each of the 4 groups at each level of severity of
damage. 1+ denotes less that 25% of the glomerulus damaged; 2+ denotes 26-50%
damage, 3+ denotes 51-75% damage, 4+ denotes 76-100% damage.
Figure 5.
Renal cortex of obese ZDF fa/fa rats, Hematoxylin and Eosin staining, Bar=200µm. A:
untreated rat showing tubular atrophy, tubular dilation, hyaline casts, interstitial fibrosis
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

JPET/2003/055616 REVISED
and inflammatory infiltrates, and glomerular sclerosis. B: PPARγ agonist treated rat,
normal morphology. C: ACEI treated rat, focal tubular degeneration and regeneration,
tubular dilation with hyaline casts, glomerular sclerosis, and hyperplasia of
juxtaglomerular apparatus. D: combination treatment of PPARγ agonist and ACEI:
normal morphology except for hyperplasia of juxtaglomerular apparatus.
Figure 6.
The glomerular filtration rate, factored for kidney weight, measured from the inulin
clearance (CIN, ml/min/gKW) after the 6 month observation period in each group.
* denotes p<0.05 vs. untreated Zucker rats.
This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from

Time of Treatment (months)
0 2 4 6
Plasmaglucosemg/dL
0
100
200
300
400
500
600
700
Untreated
ACEI
PPARγagonist +ACEI
PPARγagonist
This article has not been copyedited and form
atted. The final version m
ay differ from this version.
JPET
Fast Forward. Published on O
ctober 14, 2003 as DO
I: 10.1124/jpet.103.055616 at ASPET Journals on January 5, 2019 jpet.aspetjournals.org Downloaded from
Time of Treatment (months)
0 1 2 3 4 5 6
Bodyweight
(g)
200
400
600
800
1000
1200
This article has not been copyedited and form
atted. The final version m
ay differ from this version.
JPET
Fast Forward. Published on O
ctober 14, 2003 as DO
I: 10.1124/jpet.103.055616 at ASPET Journals on January 5, 2019 jpet.aspetjournals.org Downloaded from
Time of Treatment (months)
0 1 2 3 4 5 6
Urin
e pr
otei
n ex
cret
ion
(mg/
24h)
0
100
200
300
400
This article has not been copyedited and form
atted. The final version m
ay differ from this version.
JPET
Fast Forward. Published on O
ctober 14, 2003 as DO
I: 10.1124/jpet.103.055616 at ASPET Journals on January 5, 2019 jpet.aspetjournals.org Downloaded from

Untreated
0
2
4
6
8
10
12
ACEI
0
2
4
6
8
10
12
PPARγagonist
0
2
4
6
8
10
12
PPARγagonist+ACEI
Level of sclerosis
1+ 2+ 3+ 4+
Affe
cted
glo
mer
uli (
%)
0
2
4
6
8
10
12
This article has not been copyedited and form
atted. The final version m
ay differ from this version.
JPET
Fast Forward. Published on O
ctober 14, 2003 as DO
I: 10.1124/jpet.103.055616 at ASPET Journals on January 5, 2019 jpet.aspetjournals.org Downloaded from

A B
C D
Figure 5
This article has not been copyedited and form
atted. The final version m
ay differ from this version.
JPET
Fast Forward. Published on O
ctober 14, 2003 as DO
I: 10.1124/jpet.103.055616 at ASPET Journals on January 5, 2019 jpet.aspetjournals.org Downloaded from
Treatment
CIN
(m
l/min
/gkw
)
0.0
0.5
1.0
1.5
* *p<0.12
Untreated ACEI PPARγagonist
PPARγagonist+ACEI
This article has not been copyedited and form
atted. The final version m
ay differ from this version.
JPET
Fast Forward. Published on O
ctober 14, 2003 as DO
I: 10.1124/jpet.103.055616 at ASPET Journals on January 5, 2019 jpet.aspetjournals.org Downloaded from

This article has not been copyedited and formatted. The final version may differ from this version.JPET Fast Forward. Published on October 14, 2003 as DOI: 10.1124/jpet.103.055616
at ASPE
T Journals on January 5, 2019
jpet.aspetjournals.orgD
ownloaded from