journal of parenteral and enteral nutrition safety... · 2 journal of parenteral and enteral...
TRANSCRIPT
http://pen.sagepub.com/Nutrition
Journal of Parenteral and Enteral
http://pen.sagepub.com/content/early/2013/11/19/0148607113511992The online version of this article can be found at:
DOI: 10.1177/0148607113511992
published online 26 November 2013JPEN J Parenter Enteral NutrNeal, Gordon Sacks, David S. Seres and Patricia Worthington
Phil Ayers, Stephen Adams, Joseph Boullata, Jane Gervasio, Beverly Holcombe, Michael D. Kraft, Neil Marshall, AntoinetteA.S.P.E.N. Parenteral Nutrition Safety Consensus Recommendations
Published by:
http://www.sagepublications.com
On behalf of:
The American Society for Parenteral & Enteral Nutrition
can be found at:Journal of Parenteral and Enteral NutritionAdditional services and information for
http://pen.sagepub.com/cgi/alertsEmail Alerts:
http://pen.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Nov 26, 2013OnlineFirst Version of Record >>
by guest on January 9, 2014pen.sagepub.comDownloaded from by guest on January 9, 2014pen.sagepub.comDownloaded from

Journal of Parenteral and EnteralNutritionVolume XX Number X Month 2013 1 –38© 2013 American Societyfor Parenteral and Enteral NutritionDOI: 10.1177/0148607113511992jpen.sagepub.comhosted at online.sagepub.com
Clinical Recommendations
Table of Contents
Introduction 1Prescribing and Communicating the Parenteral Nutrition Order 3Parenteral Nutrition Order Review and Verification Process 10Compounding 23Parenteral Nutrition Administration 28Conclusion 38
Introduction
Parenteral nutrition (PN) serves as an important therapeutic modality that is used in adults, children, and infants for a variety of indications. The appropriate use of this complex therapy aims to maximize clinical benefit while minimizing the poten-tial risk for adverse events. Despite being classified and acknowledged as a high-alert medication,1 only 58% of organi-zations have precautions in place to prevent errors and patient harm associated with PN.2 Complications can occur as a result of the therapy and as the result of the PN process. These recom-mendations are based on practices that are generally accepted to minimize errors with PN therapy. However, the broad range of healthcare settings in which PN administration occurs—from
critical care to home care—raises the potential for disparities to exist in the knowledge and skills of the healthcare professionals responsible for PN prescribing, review, compounding, and administration. Regardless of the setting or the number of patients treated in a given facility, the classification of PN as a high-alert medication requires healthcare organizations to develop evidence-based policies and procedures related to PN.
511992 PENXXX10.1177/0148607113511992Journal of Parenteral and Enteral NutritionAyers et alresearch-article2013
From 1Baptist Health Systems, Department of Pharmacy, Jackson, Mississippi; 2Vitaline Infusion Pharmacy Services, Geisinger Medical Center, Danville, Pennsylvania; 3University of Pennsylvania, School of Nursing, Philadelphia; 4Butler University College of Pharmacy and Health Science, Indianapolis, Indiana; 5American Society for Parenteral and Enteral Nutrition, Silver Spring, Maryland; 6University of Michigan Health System, Department of Pharmacy Services, Ann Arbor; 7Walgreens Infusion Services, Sun Valley, California; 8Infusion Pharmacy, Cleveland Clinic at Home, Independence, Ohio; 9Department of Pharmacy Practice, Harrison School of Pharmacy, Auburn University, Auburn, Alabama; 10Division of Preventive Medicine and Nutrition, New York Presbyterian Hospital–Columbia University Medical Center, New York; 11Thomas Jefferson University Hospital, Philadelphia, Pennsylvania.
Received for publication October 3, 2013; accepted for publication October 3, 2013.
Corresponding Author:Peggi Guenter, A.S.P.E.N., Silver Spring, MD, USA. E-mail: [email protected].
A.S.P.E.N. Parenteral Nutrition Safety Consensus Recommendations
Phil Ayers, PharmD, BCNSP, FASHP-Chairperson1; Stephen Adams, MS, RPh, BCNSP2; Joseph Boullata, PharmD, RPh, BCNSP3; Jane Gervasio, PharmD, BCNSP, FCCP4; Beverly Holcombe, PharmD, BCNSP, FASHP5; Michael D. Kraft, PharmD, BCNSP6; Neil Marshall, RN, BSN, CRNI, CNSC7; Antoinette Neal, RN, CRNI, CNSC, VA-BC8; Gordon Sacks, PharmD, BCNSP, FCCP9; David S. Seres, MD, ScM, PNS10; Patricia Worthington, MSN, RN, CNSC11
AbstractParenteral nutrition (PN) serves as an important therapeutic modality that is used in adults, children, and infants for a variety of indications. The appropriate use of this complex therapy aims to maximize clinical benefit while minimizing the potential risks for adverse events. Complications can occur as a result of the therapy and as the result of the PN process. These consensus recommendations are based on practices that are generally accepted to minimize errors with PN therapy, categorized in the areas of PN prescribing, order review and verification, compounding, and administration. These recommendations should be used in conjunction with other A.S.P.E.N. publications, and researchers should consider studying the questions brought forth in this document. (JPEN J Parenter Enteral Nutr. XXXX;xx:xx-xx)
Keywordsparenteral nutrition; nutrition; parenteral formulas/compounding; safety
by guest on January 9, 2014pen.sagepub.comDownloaded from

2 Journal of Parenteral and Enteral Nutrition XX(X)
Conceptually, the American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) recommends use of the standardized process, which includes clinicians with expertise in the area of nutrition support.3
During the past few years, many circumstances and inci-dents have threatened the safety of patients receiving PN as an important therapy. In light of the need to revise A.S.P.E.N.’s Safe Practices for Parenteral Nutrition guidelines and to pub-licly address the safety of PN prescribing, compounding, and delivery, A.S.P.E.N. leaders hosted a multiorganizational safety summit on September 23, 2011. This summit brought together 46 key stakeholders to identify processes to improve the safety of prescribing, preparing, and delivering PN to patients across a variety of healthcare settings.4 Findings from this summit guided the A.S.P.E.N. PN Safety Task Force to develop safety consensus recommendations.
In an attempt to answer as many questions about PN safety as possible, this Task Force, in partnership with the A.S.P.E.N. Clinical Practice Guidelines Editorial Board PN workgroup, developed many clinical questions still unanswered in existing documents. The workgroups were divided into two segments, each responsible for specific tasks. The first group developed questions that could be answered with a high level of confi-dence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) process (the process by which the A.S.P.E.N. Clinical Guidelines are developed).5 The second group developed questions for which the level of evidence in the literature did not support any GRADE-level recommendations, meaning that consensus recommendations would depend on expert opinion. This paper addresses clinical concerns that impact PN safety for which current literature does not provide GRADE-level evidence and provides consen-sus recommendations for safe PN practice and future research based on expert opinion. These recommendations are not clini-cal guidelines as defined by A.S.P.E.N.6 The need to deliver practice information to clinicians, even when it is of a consen-sus nature from practice experts, remains an important role of A.S.P.E.N. Redundancies were deliberately built into this doc-ument between sections for users who may only view individ-ual sections based on their practice area. Reviewers of this paper included the A.S.P.E.N. Clinical Practice Committee, Dietetics Practice, Medical Practice, Nutrition Support Nurses, and Pharmacy Practice Sections, as well as clinical content experts outside of the organization. This document was also reviewed and approved by the A.S.P.E.N. Board of Directors. The questions to be answered with the Clinical Practice Guidelines GRADE process, listed in Appendix 1, will be addressed by a separate workgroup and published separately. This document should be used in conjunction with those guidelines.
Similar to A.S.P.E.N.’s Standards of Practice documents, the following terminology is used with each recommendation
to indicate the level of evidence and strength of consensus reached for each statement.
“Shall”: Indicates that the recommendation is to be fol-lowed strictly.
“Should”: Indicates that among several possibilities, one is particularly suitable, without mentioning or excluding others, or that a certain course of action is preferred, but not necessarily required.
“May”: Indicates a course of action that is permissible within the limits of recommended practice.
The recommendations within this document are intended for discussion and adoption over time by organizations and indi-vidual professionals involved in the routine care of patients requiring PN. These recommendations are not intended to supersede the judgment of the healthcare professional based on the circumstances of the individual patient. Although the substantial focus of these recommendations is on institutional settings, many of the safety issues exist across other patient-care settings. Concerns that are unique to home care are also addressed where appropriate. In every clinical set-ting, it is the responsibility of the prescriber, pharmacist, nurse, dietitian, and nutrition support team to recognize and report all PN-related medication errors, whether or not they reach the patient. This allows the medication safety officer/committee to review and address these events periodically with the commit-tee or individuals having oversight of PN.
References
1. Institute for Safe Medication Practices. ISMP’s list of high-alert medi-cations, 2012. http://www.ismp.org/Tools/highalertmedications.pdf. Accessed May 2012.
2. Institute for Safe Medication Practices. Results of ISMP survey on high alert medications. ISMP Medication Safety Alert! 2012;7(3):1-4.
3. Kochevar M, Guenter P, Holcombe B, Malone A, Mirtallo J; A.S.P.E.N. Board of Directors and Task Force on Parenteral Nutrition Standardization. A.S.P.E.N. statement on parenteral nutrition standardization. JPEN J Parenter Enteral Nutr. 2007;31:441-448.
4. Mirtallo JM, Guenter P. Introduction and goals of the A.S.P.E.N. paren-teral nutrition safety summit. JPEN J Parenter Enteral Nutr. 2012;36:7S-9S.
5. Druyan ME, Compher C, Boullata JI, et al; A.S.P.E.N. Board of Directors. Clinical guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients: applying the GRADE system to develop-ment of A.S.P.E.N. clinical guidelines. JPEN J Parenter Enteral Nutr. 2012;36:77-80.
6. American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors and Clinical Practice Committee. Definition of terms, style, and conventions used in A.S.P.E.N. Board of Directors—approved documents May 2012. http://nutritioncare.org/Professional_Resources/Guidelines_and_Standards/Guidelines/2012_Definitions_of_Terms,_Style,_and_Conventions_Used_in_A_S_P_E_N__Board_of_Directors-Approved_Documents/ Accessed November 25, 2012.
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 3
Prescribing and Communicating the Parenteral Nutrition Order
Background
PN is a complex prescription therapy associated with signifi-cant adverse effects. Deaths have occurred when safe practice guidelines were not followed.1 Appropriate and safe prescrib-ing and ordering of PN is a critical first step and an essential component of the PN use process. The safe prescribing of PN requires a thorough knowledge of protein and energy require-ments, macronutrients, micronutrients, fluid homeostasis, and acid-base balance. The prescriber shall be well versed in the appropriate indications for PN, basics in sterility and infection control, as well as vascular access devices (peripheral and cen-tral) and their associated complications. Safe prescribing of PN begins with PN-specific interdisciplinary education and insti-tutional policies focused on writing clear PN orders. Furthermore, there shall be clear means of communication among physicians, physician extenders/mid-level providers (eg, nurse practitioners, physician assistants), dietitians, phar-macists, and nurses involved in this process. This section pro-vides guidance and suggestions for healthcare institutions to adopt in order to promote safe prescribing of PN. Many of these recommendations have been adapted from literature of another high-alert therapy: cancer chemotherapy.2-4
Question: Prescribing 1–2 (P1–P2)
(P1) Does a standardized process for PN prescribing increase clarity and reduce PN-related errors? (P2) What are the essen-tial elements of a PN order that minimize errors?
Recommendations
1. Healthcare organizations shall use a standardized pro-cess for PN management, and this process shall include clinicians with expertise in the area of nutrition sup-port, preferably from multiple disciplines.5,6
a. Healthcare organizations shall develop written policies and procedures for all aspects of PN therapy in the manner described in the A.S.P.E.N. Safe Practices for Parenteral Nutrition.1
b. The patient and caregivers shall be informed of the risks and benefits associated with PN.
c. A comprehensive PN education program and competency assessment shall be developed for healthcare professionals who are involved in the care of patients receiving PN therapy, and competency should be assessed at least annually.4
d. Healthcare organizations shall have a written policy addressing credentials, training, and com-petency certification(s) required of clinicians who prescribe PN.4
2. The primary healthcare team, in collaboration with nutrition support professionals, shall evaluate, clearly define, and accurately document the patient’s medical problem(s) and indication(s) for PN.a. The patient shall have an appropriate indication
for PN therapy based on published guidelines and evidence for the use of PN, which shall be documented in the medical record.1
b. The healthcare team shall confirm that the patient has appropriate intravenous (IV) access for PN prior to prescribing PN therapy.1
c. The indication(s) for PN and appropriate IV access shall be included on the PN order (see section 4 and Table 1).1
3. The primary healthcare team, in collaboration with nutrition support professionals, shall specify and docu-ment the therapeutic goal(s) of PN therapy.a. Appropriate energy and protein goals shall be
determined for the patient’s condition based on published guidelines and evidence.1
b. Appropriate parameters and frequency of mon-itoring shall be determined for the patient’s condition to assess efficacy, detect and prevent complications, evaluate changes, and document outcomes.1
c. Appropriate monitoring parameters for PN shall include fluid requirements, serum electro-lyte concentrations, serum glucose concentra-tions, hepatic function, renal function, serum triglyceride concentrations, and signs or symp-toms of vascular access device complications.1
d. Therapeutic goals should be established for PN, including end points, response to treatment, and treatment failure.
4. PN shall be prescribed using a standardized PN order format and review process applicable to patients of every age and disease state within a healthcare organization.1,6
a. Standardized electronic PN orders (eg, a com-puterized prescriber order entry [CPOE] system) should be used to prescribe PN for all patients.1,7-9 Handwritten orders to prescribe PN should be avoided due to potential for error. Verbal and tele-phone orders for PN should be avoided.
b. Clinical decision support should be available within electronic PN orders to alert and pre-vent prescribers from ordering doses of mac-ronutrients, micronutrients, and/or medications that exceed recommended/safe clinical limits or that exceed limits of compatibility (eg, hard limits when maximum concentrations have been exceeded).1,7,8
c. When a CPOE system is not available, PN should be prescribed using a standardized order
by guest on January 9, 2014pen.sagepub.comDownloaded from
4 Journal of Parenteral and Enteral Nutrition XX(X)
template as an editable electronic document in order to avoid handwritten orders.
d. PN order templates shall be designed so they are clear and easily understood by all healthcare professionals involved in the care of patients receiving PN.1
e. Table 1 lists components that shall be included on the PN order.1,4
f. All PN order templates should include the required components listed in the sequence in Table 1. This sequence should match the PN labels as well. See Figure 1 and Figure 2 for PN Order Templates.
g. In the event of a product shortage, PN com-ponent conservation and allocation strategies should include the A.S.P.E.N. parenteral nutri-tion shortage considerations for multivitamins, trace elements, IV fat emulsions (IVFE), amino acids, electrolyte/minerals, and cysteine,10-15 and the PN order format should be updated accordingly. Multivitamins shall be prescribed daily in PN admixtures. When multivitamin products are not available, thiamine, ascorbic acid, pyridoxine, and folic acid should be pre-scribed daily.10
h. All PN ingredients shall be ordered in amounts per day (eg, for adult patients) or amounts per kilogram per day (eg, pediatric and neonatal patients) rather than in amounts per liter, per-cent concentration, or volume.1 Amount per day refers to macronutrients in grams per day, and micronutrients in mEq, mmol, mcg, or mg per day. Electrolytes shall be ordered as the com-plete salt form rather than the individual ion.1 Each individual macronutrient and micronutri-ent ordered shall be listed with its correspond-ing dose.1 If available, the total ion amounts and concentrations may be reported or displayed to the prescriber within the PN order.
i. The PN order template in CPOE systems should display current patient monitoring values and their date and time of entry to include param-eters such as laboratory values, temperature, weight, etc.
j. The PN order template should contain the full generic name for each ingredient.1,4 Proprietary names should only be used when multiple products exist and/or when the proprietary name may assist in identifying unique proper-ties of the specific dosage form (eg, inherent electrolytes in amino acid formulations, fatty acids in IVFE).4 Any abbreviations shall follow The Joint Commission standards on abbrevia-tions.4,16 Abbreviations on the Institute for Safe
Medication Practices (ISMP) list of error-prone abbreviations, symbols, and dose designations shall not be used.17
k. The PN order should include related orders for routine care, laboratory tests, and relevant mon-itoring parameters.1
l. Prescribing a PN formulation that includes non-nutrient medications should be avoided. When no other reasonable alternatives exist, non-nutrient medications shall only be included on the PN order if data support compatibility/stability.1
m. Healthcare organizations should develop poli-cies and/or protocols to allow modification of PN orders when potential incompatibilities may exist (eg, incompatibilities associated with cal-cium and phosphate salts, adjustment of IVFE dosing when it is not expected to be stable as a total nutrient admixture [TNA] [ordering IVFE separately or adjusting IVFE dosing such that the daily dose achieves minimum concentration for stability]).1 All PN order modifications shall be communicated to the healthcare team and documented in the medical record. PN orders shall be signed by a licensed prescriber who has been credentialed by the healthcare organiza-tion to prescribe PN.4
n. PN orders should be prescribed with a time lim-itation to allow for appropriate patient evalua-tion at predetermined intervals based on clinical status and required level of care.1-4
o. For optimal safety, PN orders should be pre-scribed and transmitted when supported by properly trained personnel who regularly per-form this task. This is usually done during day-time hours.18
5. Institutions shall create a home PN order template/for-mat that provides a safe plan for multiple days of ther-apy. The prescription for home PN therapy should be written in a format that specifically reflects trends in laboratory values and previous days of PN therapy. An institutional daily PN order format should not be used as a home PN prescription.
6. The most appropriate nutrition modality, in collabora-tion with nutrition support professionals, should be prescribed for the patient. Healthcare organizations should determine the most appropriate types of PN formulation(s) for their patient population(s) (eg, stan-dardized compounded, standardized commercial [pre-mixed] PN products, or customized compounded PN admixtures) or methods of delivery (eg, dextrose/amino acid vs total nutrient admixtures) and should develop criteria for each formulation that will be used in their patients.19
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 5
Rationale
PN is a complex prescription therapy with many potential safety concerns. The World Health Organization (WHO) advo-cates a systematic approach to prescribing in order to improve quality and minimize errors.2 Pollock and colleagues described considering drug costs and using computer technology when prescribing medications.3 These approaches provide an excel-lent template for the clinician prescribing PN. The A.S.P.E.N. Safe Practices for PN document describes the benefits of using a standardized PN ordering process and recommends compo-nents that should be included on a PN order template (manda-tory, strongly recommended, and worthy of consideration).1 Like PN, chemotherapy is a class of complex prescription medications with critical safety concerns. The American Society of Clinical Oncology and Oncology Nursing Society developed Chemotherapy Administration Safety Standards in the outpatient setting in 2009,20 with revisions to expand these to the inpatient setting in 2011.4 The concepts in these safety standards are consistent with the A.S.P.E.N. Safe Practices for PN. We recommend that healthcare organizations and clini-cians adopt these standards and guidelines when creating poli-cies for ordering/prescribing PN.1-4
Standardized order formats for PN incorporating prescriber guidelines can provide education that can lead to reduced pre-scribing errors, improved efficiency/productivity, and ulti-mately reduced costs and waste.1 In addition, adopting a standardized PN order format designed with ingredients listed in the same sequence may improve consistency, and clarifying orders decreases the risk of errors when patients transition care from one setting to another. The Agency for Healthcare Research and Quality recently reported on a meaningful reduc-tion in errors (from 9 to 4 per 1000 PN orders) at a children’s hospital that adopted a standardized ordering and administra-tion process for PN.6 Other observations included a reduced need for pharmacists to correct orders, a more efficient order-ing and administration process, earlier delivery and adminis-tration, and an associated increase in staff satisfaction.6
The use of electronic or computerized PN orders can also improve efficiency and safety and reduce errors. Maat and col-leagues demonstrated a significant 16% time reduction for sim-ple and a 60% time reduction for complex calculations related to PN prescribing in neonates when using a CPOE system with basic clinical decision support.7 Brown and colleagues com-pleted a retrospective cross-sectional study evaluating the impact of an interactive computerized PN worksheet on PN–prescribing
Table 1. Required Components for PN Orders and Preferred Sequence.
Components for the PN Order
Patient Information Patient identifiers (patient name, medical record number or other unique identifiers, birth date/age, patient location)Patient location (home address for home PN patients)Allergies and reactions Height and dosing weight (metric) Diagnosis(es)/indication(s) for PN Vascular access device/location Administration date/timePN Ingredients (should match PN label) Amino acids Dextrose IVFE Sodium phosphate Sodium chloride Sodium acetate Potassium phosphate Potassium chloride Potassium acetate Magnesium sulfate or magnesium chloride Calcium gluconate Multivitamins Trace elements Additives (eg, cysteine, regular insulin) as clinically appropriate and compatible
PN Instructions Total volume, infusion rate, start and stop times, cycle information Prescriber and contact information
by guest on January 9, 2014pen.sagepub.comDownloaded from

6 Journal of Parenteral and Enteral Nutrition XX(X)
errors. The worksheet was developed using commonly available spreadsheet software (ie, not part of an integrated CPOE sys-tem), but still required separate entry and transcription of the PN order. While use of the worksheet was associated with a reduc-tion in the prescribing error rate, all of the errors that did occur were attributed to transcription or data entry mistakes.9 Shamliyan and colleagues completed a review of studies to examine the association between computerization of physician orders and prescribing medication orders.8 Computerized orders were associated with a 43% reduction in dosing errors, 37.5% reduction in adverse drug events, and 66% reduction in total pre-scribing errors in adults.8 Of the studies included in this review, 80% reported a significant reduction in total prescribing errors.8 While these data are not specific to PN therapy, they do highlight the benefits of CPOE on the medication use process and associ-ated errors and adverse drug events.
The ISMP reported a case of a 16-year-old boy who received a PN order in which the ingredients were ordered in amounts per kg, but the PN admixture was prepared in amounts per day.21 This resulted in infusion of a hypo-osmolar PN admix-ture (138 mOsm/L) with very low doses of nutrients (eg, pro-tein and dextrose both at 1 g/d rather than 1 g/kg/d) for almost an entire day before it was identified (no adverse effects were incurred by the patient). There were multiple failures across the entire medication use process in this scenario. For example, the PN order template in the CPOE system did not match the template in the pharmacy system/Automated Compounding Device (ACD). Further, there was a lack of clinical decision support and automated warnings in both the CPOE PN order template and the ACD, a lack of redundancies in the process, and multiple points of transcription. ISMP provided several safe practice recommendations21:
Patient Information
Patient name______________Medical record number___________________ Birthdate/age
______ Patient location____________________ Allergies________________________
Height and dosing weight: Ht: ____cm Dosing Wt: ______kg
Diagnosis(es)/Indication(s) for PN______________________________
Vascular access device/location CVC type____________________ Location________________
Administration date/time
Base Formula Amount/day
Amino acids g
Dextrose g
IV Fat emulsion g
Electrolytes
Sodium phosphate mmol
Sodium chloride mEq
Sodium acetate mEq
Potassium phosphate mmol
Potassium chloride mEq
Potassium acetate mEq
Magnesium sulfate mEq
Calcium gluconate mEq
Vitamins, Trace Elements, Additives
Multi-component vitamins mL
Multi-component Trace elements mL
Other Additives (eg, individual vitamins or trace elements, cysteine, regular insulin) as clinically appropriate
and compatible
PN Instructions
Total volume________mL Infusion rate______mL/hr , start and stop times__________
Cycle information
Prescriber and contact information______________________________
Figure 1. Parenteral Nutrition Order Template: Adult Patient.
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 7
•• Match prescribing and pharmacy templates•• Build, test, and heed automated warnings•• Heighten suspicions of errors•• Carry out effective redundancies•• Provide clear labeling (and the label should always
match the PN order template in the PN order form/CPOE system and the ACD)
•• Educate and validate competency•• Eliminate transcription of PN orders
Despite the potential advantages of CPOE, use of CPOE with respect to PN orders appears to be limited. A 2011 survey of PN practices noted that a CPOE system was used for PN orders in only 33% of the surveyed organizations.22 Most recently, Radley et al conducted a systematic review of the literature and derived a summary estimate of the effect of CPOE using a random effects meta-analytic technique. Their pooled analysis revealed that implementing CPOE was associated with a 48% (95% CI,
41%–55%) reduction in medication error rates. They further estimated that as many as 104 million medication errors could be averted annually if all hospitals fully adopted CPOE to process all medication orders.23 To the best of our knowledge, only one large commercial Health Information System–Electronic Medical Record/CPOE system provides even rudimentary PN calculation or decision support capability.
Question: Prescribing 3 (P3)
(P3) What improvements in the physical environment would promote safe PN ordering and use?
Recommendations
Institutions shall meet the following requirements for the physi-cal environment as described in The United States Pharmacopeial Convention, USP General Chapter <1066>:
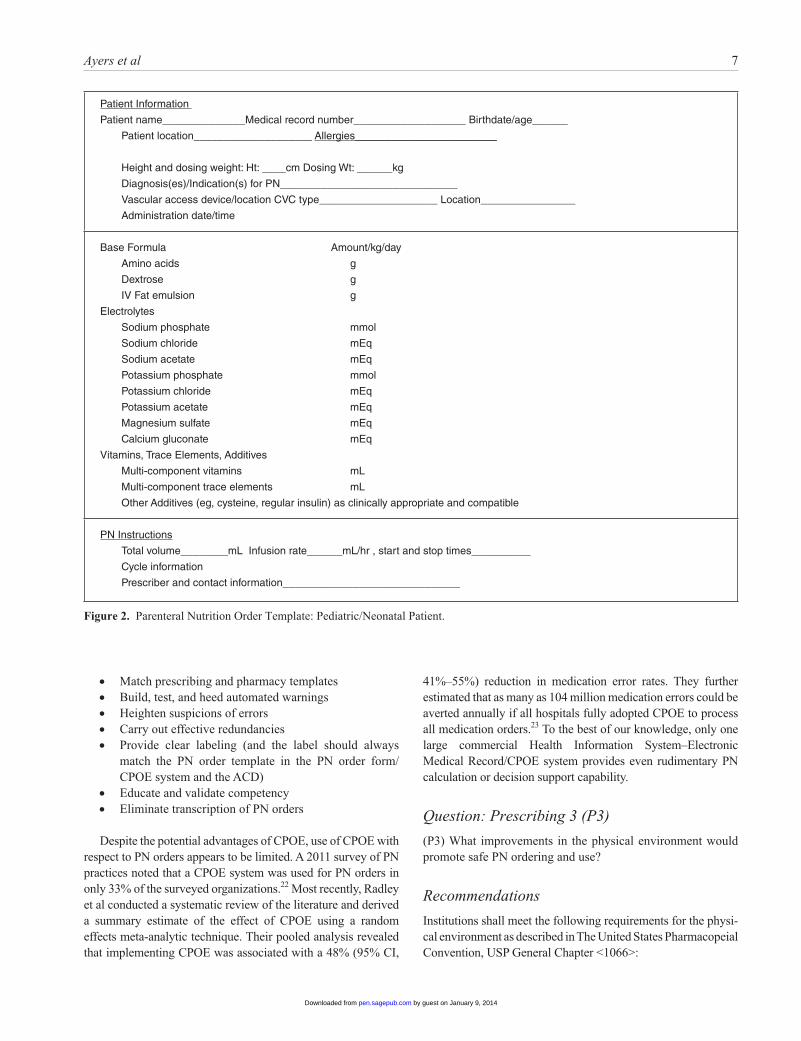
Figure 2. Parenteral Nutrition Order Template: Pediatric/Neonatal Patient.
Patient Information
Patient name______________Medical record number___________________ Birthdate/age______
Patient location____________________ Allergies________________________
Height and dosing weight: Ht: ____cm Dosing Wt: ______kg
Diagnosis(es)/Indication(s) for PN______________________________
Vascular access device/location CVC type____________________ Location________________
Administration date/time
Base Formula Amount/kg/day
Amino acids g
Dextrose g
IV Fat emulsion g
Electrolytes
Sodium phosphate mmol
Sodium chloride mEq
Sodium acetate mEq
Potassium phosphate mmol
Potassium chloride mEq
Potassium acetate mEq
Magnesium sulfate mEq
Calcium gluconate mEq
Vitamins, Trace Elements, Additives
Multi-component vitamins mL
Multi-component trace elements mL
Other Additives (eg, cysteine, regular insulin) as clinically appropriate and compatible
PN Instructions
Total volume________mL Infusion rate______mL/hr , start and stop times__________
Cycle information
Prescriber and contact information______________________________
by guest on January 9, 2014pen.sagepub.comDownloaded from

8 Journal of Parenteral and Enteral Nutrition XX(X)
1. Illumination: USP <1066> recommends the following lighting levels for healthcare settings24: Computer order entry 1000 Lux Handwritten order processing 1000 Lux Sterile compounding and preparation 1000–1500
Lux Medication preparation area 1000 Lux Medication administration work area 1000 Lux
2. Interruptions and distractions: The 2008 USP MEDMARX Data Reports noted distractions rank high (approximately 45%) as contributing to medica-tion errors in hospitals and health systems.25
3. Sound and noise: The standard for sound levels for medication safety zones is set at 50 decibels A-weighted for sound (dBA), the level of conversation.24
4. Physical design and organization of work space: The design of the workplace environment can influence the effectiveness of the prescriber to perform tasks.24 USP <1066> promotes ergonomic design of the workplace environment. Factors such as counter height, height of supplies, drawer lighting, and work clutter are noted to influence efficiency as well as safety.
5. Medication safety zones: Defined as a critical area where medications are prescribed, orders are entered into a computer or transcribed onto paper documents, and where medications are prepared, dispensed, or administered.24
Rationale
The process of ordering/prescribing PN is very complex and requires an environment that promotes safety. According to the United States Pharmacopeia (USP), the work environment has been identified as one of the most common reported factors known to contribute to medication errors.24 In October 2010, The United States Pharmacopeial Convention published an official bulletin titled Physical Environments That Promote Safe Medication Use, General Chapter <1066>. This chapter focuses on the characteristics of the physical environment that are essential to promoting accurate medication use.24 These guidelines provide an excellent resource to promote safe pre-scribing for the nutrition support clinicians to incorporate into their practice.
Question: Prescribing 4 (P4)
(P4) How often should the PN prescription be reordered after the initial order?
1. An institution-specific or organization-specific policy should be created to dictate the duration of a PN order.
2. When reordering PN, each PN component should be reordered in its entirety, including full generic names and doses.
3. Patients with newly initiated PN should be monitored and have their orders reviewed more frequently.
4. The reordering process should be structured to require accountability for reviewing the orders, laboratory findings, and patient’s condition. Simple processes (eg, a single-step “renew order” button) that lack this accountability should not be used. The following are categories for patients and examples for their corre-sponding monitoring frequencies:a. Patients who are new to PN should be monitored
daily until stable (more frequently if clinically significant metabolic abnormalities are found or patient is at risk for refeeding syndrome).
b. Patients in an unstable clinical condition (eg, acutely ill, critically ill, recovering from criti-cal illness, recent surgery) should be monitored daily until stable (more frequently if clinically significant abnormalities are observed).
c. Stable patients in the hospital with no required changes in formulation for 1 week should be monitored every 2 to 7 days.
d. Stable patients in a hospital, long-term care, or home setting with no changes in formula-tion for more than 1 week should be monitored every 1 to 4 weeks or longer in select clinically stable patients.
Rationale
There are no known studies that examine whether the duration of a PN order or the frequency with which such orders are renewed impacts outcomes or safety measures. However, the collaborative multidisciplinary care approach and application of safe practices guidelines have repeatedly proven to reduce com-plications, costs, and inappropriate use of PN.26 It is reasonable to assume that patients newly initiated on PN, especially those with preexisting electrolyte abnormalities or at risk for refeeding syndrome or with unstable clinical status (such as those newly critically ill or postoperative patients), will require more fre-quent monitoring. Similarly, patients who have been stable for some time may need less frequent monitoring. Policies regard-ing the frequency of PN order renewals improve monitoring practices. Protocols for ordering PN may be designed such that laboratory values must be entered or acknowledged prior to sub-mitting the order as is common in home infusion practice. Published guidelines and literature on prescribing should be adopted and reinforced and each healthcare organization shall include clinicians with expertise in the area of nutrition support, preferably from multiple disciplines in the prescribing process.5,6
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 9
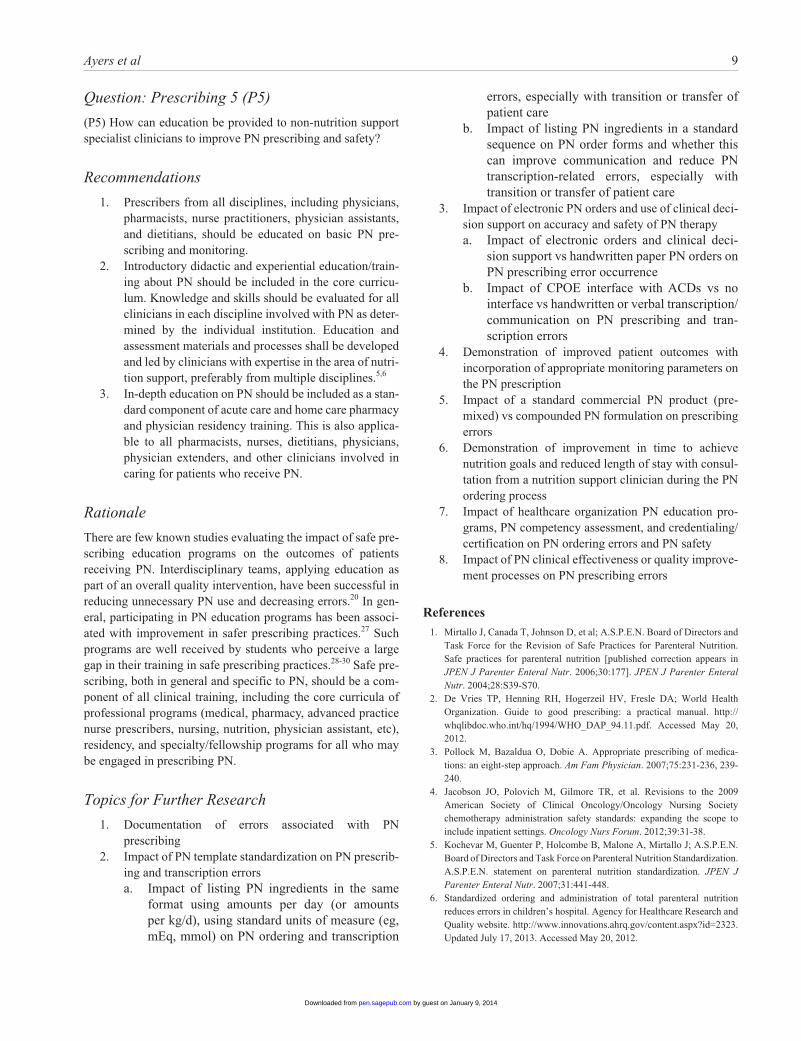
Question: Prescribing 5 (P5)
(P5) How can education be provided to non-nutrition support specialist clinicians to improve PN prescribing and safety?
Recommendations
1. Prescribers from all disciplines, including physicians, pharmacists, nurse practitioners, physician assistants, and dietitians, should be educated on basic PN pre-scribing and monitoring.
2. Introductory didactic and experiential education/train-ing about PN should be included in the core curricu-lum. Knowledge and skills should be evaluated for all clinicians in each discipline involved with PN as deter-mined by the individual institution. Education and assessment materials and processes shall be developed and led by clinicians with expertise in the area of nutri-tion support, preferably from multiple disciplines.5,6
3. In-depth education on PN should be included as a stan-dard component of acute care and home care pharmacy and physician residency training. This is also applica-ble to all pharmacists, nurses, dietitians, physicians, physician extenders, and other clinicians involved in caring for patients who receive PN.
Rationale
There are few known studies evaluating the impact of safe pre-scribing education programs on the outcomes of patients receiving PN. Interdisciplinary teams, applying education as part of an overall quality intervention, have been successful in reducing unnecessary PN use and decreasing errors.20 In gen-eral, participating in PN education programs has been associ-ated with improvement in safer prescribing practices.27 Such programs are well received by students who perceive a large gap in their training in safe prescribing practices.28-30 Safe pre-scribing, both in general and specific to PN, should be a com-ponent of all clinical training, including the core curricula of professional programs (medical, pharmacy, advanced practice nurse prescribers, nursing, nutrition, physician assistant, etc), residency, and specialty/fellowship programs for all who may be engaged in prescribing PN.
Topics for Further Research
1. Documentation of errors associated with PN prescribing
2. Impact of PN template standardization on PN prescrib-ing and transcription errorsa. Impact of listing PN ingredients in the same
format using amounts per day (or amounts per kg/d), using standard units of measure (eg, mEq, mmol) on PN ordering and transcription
errors, especially with transition or transfer of patient care
b. Impact of listing PN ingredients in a standard sequence on PN order forms and whether this can improve communication and reduce PN transcription-related errors, especially with transition or transfer of patient care
3. Impact of electronic PN orders and use of clinical deci-sion support on accuracy and safety of PN therapya. Impact of electronic orders and clinical deci-
sion support vs handwritten paper PN orders on PN prescribing error occurrence
b. Impact of CPOE interface with ACDs vs no interface vs handwritten or verbal transcription/communication on PN prescribing and tran-scription errors
4. Demonstration of improved patient outcomes with incorporation of appropriate monitoring parameters on the PN prescription
5. Impact of a standard commercial PN product (pre-mixed) vs compounded PN formulation on prescribing errors
6. Demonstration of improvement in time to achieve nutrition goals and reduced length of stay with consul-tation from a nutrition support clinician during the PN ordering process
7. Impact of healthcare organization PN education pro-grams, PN competency assessment, and credentialing/certification on PN ordering errors and PN safety
8. Impact of PN clinical effectiveness or quality improve-ment processes on PN prescribing errors
References
1. Mirtallo J, Canada T, Johnson D, et al; A.S.P.E.N. Board of Directors and Task Force for the Revision of Safe Practices for Parenteral Nutrition. Safe practices for parenteral nutrition [published correction appears in JPEN J Parenter Enteral Nutr. 2006;30:177]. JPEN J Parenter Enteral Nutr. 2004;28:S39-S70.
2. De Vries TP, Henning RH, Hogerzeil HV, Fresle DA; World Health Organization. Guide to good prescribing: a practical manual. http://whqlibdoc.who.int/hq/1994/WHO_DAP_94.11.pdf. Accessed May 20, 2012.
3. Pollock M, Bazaldua O, Dobie A. Appropriate prescribing of medica-tions: an eight-step approach. Am Fam Physician. 2007;75:231-236, 239- 240.
4. Jacobson JO, Polovich M, Gilmore TR, et al. Revisions to the 2009 American Society of Clinical Oncology/Oncology Nursing Society chemotherapy administration safety standards: expanding the scope to include inpatient settings. Oncology Nurs Forum. 2012;39:31-38.
5. Kochevar M, Guenter P, Holcombe B, Malone A, Mirtallo J; A.S.P.E.N. Board of Directors and Task Force on Parenteral Nutrition Standardization. A.S.P.E.N. statement on parenteral nutrition standardization. JPEN J Parenter Enteral Nutr. 2007;31:441-448.
6. Standardized ordering and administration of total parenteral nutrition reduces errors in children’s hospital. Agency for Healthcare Research and Quality website. http://www.innovations.ahrq.gov/content.aspx?id=2323. Updated July 17, 2013. Accessed May 20, 2012.
by guest on January 9, 2014pen.sagepub.comDownloaded from

10 Journal of Parenteral and Enteral Nutrition XX(X)
7. Maat B, Rademaker Carin MA, Oostveen MI, et al. The effect of a com-puterized prescribing and calculating system on hypo- and hyperglyce-mias and on prescribing time efficiency in neonatal intensive care patients. JPEN J Parenter Enteral Nutr. 2013;37:85-91.
8. Shamliyan TA, Duval S, Du J, Kane RL. Just what the doctor ordered: review of the evidence of the impact of computerized physician order entry on medication errors. Health Serv Res. 2008;43:32-53.
9. Brown CL, Garrison NA, Hutchinson AA. Error reduction when prescrib-ing neonatal parenteral nutrition. Am J Perinatol. 2007;24:417-427.
10. Information to use in the event of an intravenous multivitamin shortage—May 2012: information to use in the event of adult IV multivitamin short-age. American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/lcontent.aspx?id=5346. Accessed August 5, 2013.
11. Information to use in the event of an intravenous amino acids shortage—October 2010. American Society for Parenteral and Enteral Nutrition web-site. http://www.nutritioncare.org/Index.aspx?id=5646. Accessed August 5, 2013.
12. Information to use in the event of an intravenous fat emulsion shortage—June 2010. American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/Professional_Resources/Information_to_Use_in_the_Event_of_an_Intravenous_Fat_Emulsion_Shortage/. Accessed August 5, 2013.
13. Parenteral nutrition trace element product shortage considerations (5-19-2011). American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/News/Parenteral_Nutrition_Trace_Element_Product_Shortage_Considerations/. Accessed August 5, 2013.
14. Parenteral nutrition cysteine product shortage considerations: September, 2011. American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/Professional_Resources/Guidelines_and_Standards/Guidelines/PN_Cysteine_Product_Shortage_Considerations/. Accessed August 5, 2013.
15. Holcombe B, Andris DA, Brooks G, Houston DR, Plogsted SW. Parenteral nutrition electrolyte/mineral product shortage considerations. JPEN J Parenter Enteral Nutr. 2011;35:434-436.
16. The Joint Commission. Official “Do Not Use” abbreviations list. Information Management Standard IM 02.02.01.
17. Institute for Safe Medication Practices. List of error-prone abbreviations, symbols, and dose designations. http://www.ismp.org/tools/errorproneab-breviations.pdf. Accessed September 21, 2012.
18. Institute for Safe Medication Practices. Fatal 1,000-fold overdoses can occur, particularly in neonates, by transposing mcg and mg. ISMP Medication Safety Alert! September 6, 2007. http://www.ismp.org/Newsletters/acutecare/articles/20070906.asp. Accessed June 2012.
19. Gervasio J. Compounding vs. standard commercial parenteral nutrition product: pros and cons. JPEN J Parenter Enteral Nutr. 2012;36:40S-41S.
20. Jacobson JO, Polovich M, McNiff KK, et al. American Society of Clinical Oncology/Oncology Nursing Society chemotherapy administration safety standards. Oncology Nurs Forum. 2009;36:651-658.
21. Institute for Safe Medication Practices. Mismatched prescribing and phar-macy templates for parenteral nutrition (PN) lead to data entry errors. ISMP Medication Safety Alert! June 28, 2012;17(13).
22. Boullata J, Guenter P, Mirtallo J. A parenteral nutrition use survey with a gap analysis. JPEN J Parenter Enteral Nutr. 2013;37:212-222.
23. Radley DC, Wasserman MR, Olsho LEW, et al. Reduction in medication errors in hospitals due to adoption of computerized provider order entry systems. J Am Med Inform Assoc. 2013;20:470-476.
24. USP Chapter <1066> Physical Environments That Promote Safe Medication Use. 2010. The United States Pharmacopeial Convention.
25. Hicks RW, Becker SC, and Cousins DD, eds. USP MEDMARX Data Report: A Report on the Relationship of Drug Names and Medication Errors in Response to the Institute of Medicine’s Call for Action. Rockville, MD: Center for Advancement of Patient Safety, U.S. Pharmacopeia; 2008.
26. Boitano M, Bojak S, McCloskey S, McCaul DS, McDonough M. Improving the safety and effectiveness of parenteral nutrition: results of a quality improvement collaboration. Nutr Clin Pract. 2010;25:663-671.
27. Scobie SD, Lawson M, Cavell G, Taylor K, Jackson SH, Roberts TE. Meeting the challenge of prescribing and administering medicines safely: structured teaching and assessment for final year medical students. Med Educ. 2003;37:434-437.
28. Naritoku DK, Faingold CL. Development of a therapeutics curriculum to enhance knowledge of fourth-year medical students about clinical uses and adverse effects of drugs. Teach Learn Med. 2009;21:148-152.
29. Tobaiqy M, McLay J, Ross S. Foundation year 1 doctors and clinical pharmacology and therapeutics teaching: a retrospective view in light of experience. Br J Clin Pharmacol. 2007;64:363-372.
30. Garbutt JM, Highstein G, Jeffe DB, Dunagan WC, Fraser VJ. Safe medi-cation prescribing: training and experience of medical students and hous-estaff at a large teaching hospital. Acad Med. 2005;80:594-599.
Parenteral Nutrition Order Review and Verification Process
Background
PN is a highly complicated therapy administered to patients in hospitals and alternative sites including the home and long-term care facilities. PN formulations may contain more than 40 ingredients, including amino acids, dextrose, IVFE, electro-lytes, vitamins, trace elements, insulin, and other medications. PN is considered a high-alert medication because significant patient harm may occur when this therapy is used in error.1,2 A critical step in the PN process is a pharmacist’s review and verification of PN orders. Breaches in the review and verifica-tion processes have resulted in errors and patient harm.1 Healthcare organizations have the opportunity to improve the safety of PN therapy by optimizing technology for prescribing PN and transmitting PN order information as well as standard-izing the PN review and verification processes.
Question: Verification 1 (V1)
(V1) What are the essential components or attributes for safely transmitting PN orders to pharmacists for review and verification?
Recommendations
1. PN should be prescribed using a CPOE system that is fully integrated with an automated compounding device (ACD).3 “Fully integrated” is described to mean that the order entered into the CPOE system is trans-mitted electronically to the ACD without requiring reentry of any data and any modifications to an order are electronically transmitted back to the CPOE system for physician approval and signature.
2. When PN formulations are outsourced to a third-party vendor for compounding, PN orders should be pre-scribed using a CPOE system and electronically trans-mitted to the vendor to avoid transcription errors.
3. In the absence of a fully integrated system, PN should be prescribed using a standardized order template as an
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 11
editable electronic document in order to avoid hand-written orders.
4. Verbal and telephone orders for PN should be avoided except for pharmacist to prescriber communication to modify or clarify the order.
5. PN order data should be in a standardized format, including standardized sequence of ingredients, stan-dard units, standard formulas, and formulation options1 as described above in the Questions (P1–P2).
6. If transcription into the ACD is required, the output of the PN order data should be formatted to support direct entry into the ACD without requiring reordering of the ingredients, manual calculations of amounts, or unit-of-measure conversions.
7. Data should only be manually transcribed from the PN order into the ACD when absolutely necessary. Transcribed data should always be double-checked by independent processes to monitor accuracy.4 Multiple manual transcriptions of PN order data should be avoided.
8. PN orders should be prescribed, transmitted, and com-pounded when supported by properly trained person-nel who regularly perform this task.5 This is usually during the daytime hours.
9. Vendors and application architects for CPOE systems should place priority on developing pathways for pre-scribing PN that support the prescriber with appropri-ate clinical decision support (as previously described), enforce standards of practice, and communicate directly with ACDs.
10. Application vendors and application architects for CPOE systems should collaborate with ACD manufac-turers to develop fully integrated systems.
11. Application vendors and application architects for CPOE systems should collaborate with ACD manufac-turers and outsourcing pharmacies to develop fully integrated systems.
Rationale
Few healthcare organizations currently use a CPOE system for prescribing PN formulations that is fully integrated with an ACD. While some healthcare organizations use a CPOE sys-tem for prescribing PN, the majority continue to use paper order forms to prescribe PN, including handwritten orders.6-8 Outsourcing pharmacies receive PN data in a variety of for-mats, including handwritten forms, which are commonly trans-mitted to the pharmacy. This may necessitate unit-of-measure conversion calculations, data manipulation, and transcription, which may result in errors. Editable electronic documents allow prescribers to complete orders and avoid the risks associ-ated with handwritten orders.9,10 The lack of integration of the PN order with an ACD requires the manual entry of PN order data, which may lead to transcription errors.11 A recent survey of PN practices reported that more than half of PN orders are
transcribed by a pharmacist from handwritten orders or a printed label or requisition.8 Two recent reports from the ISMP describe transcription errors. One was the death of a 6-week-old infant who received a dose of sodium 600 times the pre-scribed amount.12 The second report describes a PN order data entry error in which nutrients were entered into an incorrect PN template, resulting in a patient receiving a hypotonic PN for-mulation.13 Sacks et al also described a PN system in which PN order data were transcribed from a handwritten order into a hospital pharmacy computer and then reentered into the ACD, thereby increasing the risk for transcription errors.11 If the PN process requires transcriptions, limiting the number of times data are entered from one system to another will decrease the risk of data entry errors. PN errors associated with incorrect calculations or converting units of measure have been reported and may result in patient harm. The ISMP reported the death of a neonate who received PN that included zinc at a dose 1000 times the prescribed amount. This error was the result of a cal-culation error in converting mcg/100 mL to mcg/kg/d.5
There are numerous CPOE vendors but few offer templates for prescribing PN that are user-friendly, allow institution-spe-cific customization, or interface with an ACD. Although the number of orders for PN is a small percentage of the total num-ber of medications prescribed, it is one of the most complex and complicated therapies provided by pharmacies. A CPOE system that is fully integrated with an ACD improves the safety of the PN process.13
Question: Verification 2 (V2)
(V2) What improvements in the PN review and verification processes will enhance the safety of PN therapy?
Recommendations
1. Healthcare organizations shall have a written policy and procedure for pharmacists to review and verify PN orders.
2. The review and verification of PN orders should be conducted in an environment without distractions.
3. PN orders shall be reviewed by a knowledgeable and skilled pharmacist to assess that the order is clear and complete.
4. The PN order shall include the following elements:a. Complete patient identifiers (patient name,
medical record number or other unique identi-fiers, patient location)
b. Birth date and/or agec. Allergies and associated reactionsd. Height and dosing weight in metric unitse. Diagnosis/diagnosesf. Indication(s) for PNg. Administration route/vascular access device
(peripheral vs central)h. Contact information for prescriber
by guest on January 9, 2014pen.sagepub.comDownloaded from
12 Journal of Parenteral and Enteral Nutrition XX(X)
i. Date and time order submittedj. Administration date and timek. Volume and infusion ratel. Infusion schedule (continuous or cyclic)m. Type of formulation (dextrose/amino acids
with separate infusion of IVFE or total nutrient admixture)
n. All PN ingredients shall be ordered as follows:
1. Ingredients ordered as amounts per day (for adult patients) or amounts per kilogram per day (for pediatric and neonatal patients) rather than in amounts per liter, percent concentra-tion, or volume.1 “Amount per day” refers to macronutrients in grams per day and micronu-trients in mEq, mmol, mcg, or mg per day.
2. Electrolytes shall be ordered as the complete salt form rather than the individual ion.
3. The PN order should contain the full generic name for each ingredient.1,14 Brand names should only be used when multiple products exist and/or when the brand name may assist in identifying unique properties of the specific dosage form (eg, inherent electrolytes in amino acid formulations, fatty acids in IVFE).14
4. All abbreviations shall follow The Joint Commission standards on abbreviations.14,15 Abbreviations on the ISMP’s list of error-prone abbreviations, symbols, and dose desig-nations shall not be used.16
o. A dose for each macronutrientp. A dose for each electrolyteq. A dose for vitamins, including multivita-
mins and/or individual vitamin entities. Multivitamins shall be included daily in PN formulations1,17
r. A dose for trace elements, including multicom-ponents and/or individual trace element entities
s. A dose for each non-nutrient medication (eg, insulin)
5. PN orders shall undergo a clinical review to assess appropriateness and shall include the following elements:a. Indication is consistent with published guide-
lines.b. Calculated osmolarity of the PN formulation is
appropriate for the route of administration/vas-cular access device (peripheral vs central).1
c. Each additive macronutrient, micronutri-ent, non-nutrient medication (eg, insulin) is evaluated to confirm that the dose is clinically appropriate for the patient’s nutrition needs, metabolic status, organ function, allergies, con-
comitant interventions, and other indices, and to confirm that the dose is consistent with insti-tutional practice standards.
d. The formulation is compared with the previ-ous day’s PN formulation, if any, to assess for substantial additions, deletions, increases, or decreases in dosages of macronutrients, micro-nutrients, or medications (eg, insulin).
e. When laboratory data are available, updated laboratory values that have been reported since the order was submitted should be reviewed for significant changes and, if present, the appro-priateness of additive dosing should be reevalu-ated.
6. PN orders shall undergo a formulation safety review that includes the following elements:a. All ingredients are evaluated for compatibility
with each other. Calcium-phosphate precipita-tion risk should be assessed according to insti-tutional policies and procedures.
b. PN formulation is evaluated for expected sta-bility from the time of preparation until the time that administration of the PN is complete. For example, emulsion stability of a total nutrient admixture should be evaluated.
7. Healthcare organizations shall develop policies and/or protocols to clarify PN orders when doses are outside normal ranges or potential incompatibilities may exist (eg, adjusting calcium and phosphate doses to avoid the risk of calcium-phosphate precipitation, adjusting the IVFE dose when it is not expected to be stable as a TNA [ordering IVFE separately or adjusting IVFE dosage such that the daily dose achieves minimum concentration for stability]).
8. Modifications to the prescriber’s original PN order shall be communicated to the licensed prescriber (or their designee) and documented in the patient’s medi-cal record in a manner that is auditable.
9. All PN orders that require transcription of order data should undergo an independent double-check4 process prior to compounding the PN formulation. The double-check shall be documented and auditable.
10. All PN orders requiring calculations or conversion of units of measure should undergo an independent dou-ble-check4 process prior to compounding the PN for-mulation. All double-checks shall be documented and auditable.
11. Recommendations for pharmacy review of PN orders apply whether the pharmacist reviewing the PN order is on site or at a remote location from the prescriber. The time dedicated for the pharmacist(s) to review PN orders should be based on the average number of PN orders and the estimated time to review, clarify, and/or modify a PN order at an organization.
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 13
12. PN orders that are completed in a hospital but out-sourced to a third-party pharmacy for compounding and PN orders submitted to home infusion pharmacies should undergo the same standardized pharmacy review and verification process prior to transmission to the pharmacy for compounding.
13. Institutions shall create a home PN order process that provides a safe plan for multiple days of therapy. The prescription for home PN therapy should be written in a format that specifically reflects trends in laboratory values and previous days of PN therapy. An institu-tional daily PN order format should not be used as a home PN prescription.
14. Pharmacies have the same responsibility of maintain-ing the PN orders in their records as with other medica-tion orders.
15. The healthcare organization shall develop criteria to evaluate and identify pharmacists who are competent to review and verify PN orders.a. Pharmacists responsible for the review and
verification of PN orders should have com-pleted specialty residency training and/or be certified as a Board Certified Nutrition Support Pharmacist (BCNSP) by the Board of Pharmacy Specialties (BPS).
b. In the absence of pharmacists with specialty resi-dency training or BCNSP certification, the orga-nization should have methods to identify and evaluate pharmacists competent to review and verify PN orders such as the certification pro-gram offered by the National Board of Nutrition Support Certification (NBNSC) until such time that a pharmacist with specialty residency train-ing or BCNSP certification is available.
c. In the absence of pharmacists with specialty residency training or BCNSP certification, the organization should provide formal training pro-grams or an opportunity to participate in formal training programs to increase knowledge and skills in nutrition support and with a goal of becoming certified in nutrition support. Training should focus on evaluating dosage of macronu-trients and micronutrients as well as prescribing non-nutrient medications (eg, insulin) and their compatibilities and stabilities in PN.
16. Pharmacists who review and verify PN orders should demonstrate competency at least annually.
17. Quality improvement programs should be in place to report, track, and analyze errors associated with the PN order review and verification process.
Rationale
The review of medication orders, including PN orders, involves many steps in which the pharmacist evaluates the order for
safety, efficacy, and appropriateness. These processes require knowledge of PN therapy and formulations; critical thinking and decision making by the pharmacist is crucial, and appropri-ate allotment of time is necessary.2,18 Before any PN formula-tion is compounded, the PN order is reviewed and verified. Standardizing these processes satisfies that all elements are included and the order is complete. The review and verification of PN orders includes both a clinical review and a pharmaceuti-cal review. The verification is conducted to check that the PN order is complete and that the appropriate vascular access is in place for new patients beginning PN.2 Additionally, the clinical review evaluates the appropriateness of the dose of each macro-nutrient and micronutrient as well as non-nutrient medications in the PN formulation. A pharmaceutical review of PN orders is also conducted to determine if the prescribed components are compatible and if the PN formulation is expected to be stable.2
A recent survey of PN practices reported that most institu-tions (60.2%) dedicate 0.6 full-time equivalent or more phar-macists to verify and review PN orders. However, 23.1% did not have any dedicated pharmacist time for these tasks. When a pharmacist is involved, most conduct both a clinical and pharmaceutical review of PN orders. The 2012 survey by the American Society of Health-System Pharmacists of pharmacy practice in hospitals reports that 11.1% of hospital pharmacies have pharmacists responsible for monitoring patients receiving PN therapy.19
The complexity of PN orders necessitates special knowl-edge and skills to adequately review PN orders. Special train-ing programs focusing on all aspects of the review process, especially the total daily dose of PN components, will improve the review process and heighten the pharmacist’s awareness and ability to identify errors.12 Identification of errors in turn requires follow-up and/or clarification with the prescriber. In the recent survey of PN practices conducted by Boullata et al, the reasons for PN order clarification included illegible orders, doses outside normal ranges, incompatible additives, and incorrect PN volume or infusion rate.8 Errors and patient harm have also occurred when pharmacists misinterpreted informa-tion on the PN label when patients transferred from one health-care setting to another (eg, home to hospital).1 Failure to follow and be judicious with the verification and review processes have resulted in adverse events.1,5,12,13 Certification in nutrition support validates an individual’s qualifications and level of knowledge to practice in this area.20 BPS criteria for recogni-tion states that the area of specialization shall be one for which specifically trained practitioners are needed to fulfill the responsibilities of the pharmacy profession in improving the health and welfare of the public, which are responsibilities that may not otherwise be fulfilled effectively. Nutrition support pharmacy practice fulfills that criteria.20 In one paper, staff obtained certification in nutrition support and targeted indi-viduals with specialty certification when recruiting for new staff. This resulted in a substantial increase in knowledge and ability of pharmacists to manage the associated complexities of PN.21
by guest on January 9, 2014pen.sagepub.comDownloaded from
14 Journal of Parenteral and Enteral Nutrition XX(X)
Question: Verification 3 (V3)
(V3) What are the steps healthcare organizations can take to improve the PN label and labeling system?
Recommendations
1. Healthcare organizations shall have a policy and pro-cedure/protocol for standardized labeling of PN formulations.
2. Elements of the PN label include1: (see Figure 3 and Figure 4)a. Two patient identifiers (eg, name, medical
record number, date of birth)b. Patient location or addressc. Dosing weight in metric unitsd. Administration date and timee. Beyond-use date and timef. Route of administration (central vs peripheral
vascular access)g. Prescribed volume and overfill volumeh. Infusion rate expressed in mL/hi. Duration of the infusion (continuous vs cyclic)j. Size of in-line filter (1.2 or 0.22 micron)k. Complete name of all ingredientsl. Barcodem. All ingredients shall be listed in the same
sequence and same units of measure as PN order. All PN ingredients shall be ordered in amounts
per day (for adult patients) or amounts per kilogram per day (for pediatric and neonatal patients) rather than in amounts per liter, per-cent concentration, or volume. “Amount per day” refers to macronutrients in grams per day and micronutrients in mEq, mmol, mcg, or mg per day.
Electrolytes shall be ordered as the complete salt form rather than the individual ion. Each individual macronutrient and micronutrient ordered shall be listed with its corresponding dose.
For home or alternative site PN labels, a list of patient/caregiver additives shall be included; these additives shall be easily identified and differentiated from the other PN components. Techniques to identify patient additives include highlighting or an asterisk to identify the addi-tives that are added just prior to administration.
3. Name of institution or pharmacy4. Institution or pharmacy contact information, including
telephone number
5. Auxiliary labels may be used to express individual elec-trolytes as mEq and the phosphorus content as mmol per day. The label may also include information on the amount of energy provided by each macronutrient or electrolytes intrinsic to the amino acids product.
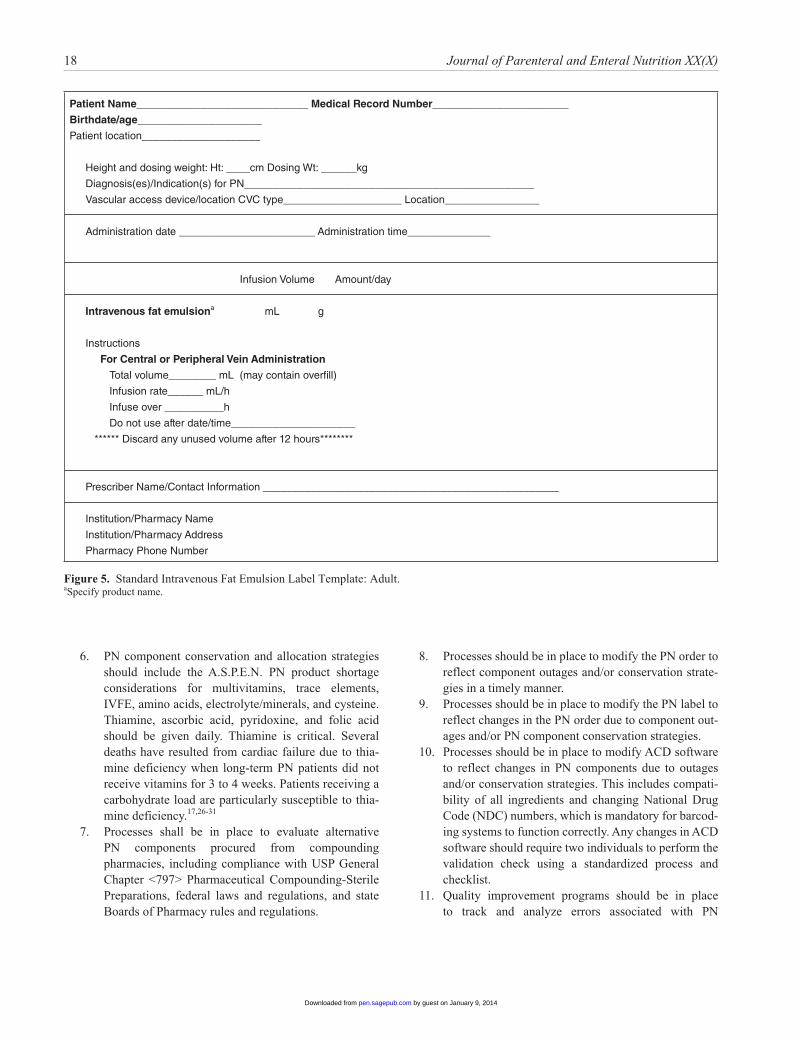
6. If IVFEs are infused separately (vs TNA), the essential elements of the IVFE label are: (see Figure 5 and Figure 6)a. Two patient identifiers (name, medical record
number, date of birth)b. Patient location or addressc. Dosing weightd. Administration date and timee. Route of administration (central vs peripheral
access)f. Prescribed amount of IVFE and volume
required to deliver that amountg. Infusion rate expressed in mL/hh. Duration of the infusion (not longer than 12
hours)i. Complete name of the IVFE, even though label
placed on original manufacturer containerj. Beyond-use date and timek. Name of institution or pharmacyl. Institution or pharmacy telephone number
7. Labels for home PN formulations should be consistent with USP General Chapter <17>.22 (See Figure 7)a. Organize the prescription label in a patient-cen-
tered manner.● Organized in a manner that best reflects how
most patients seek out and understand medical information
● Includes only the most important patient infor-mation needed for safe and effective understanding
b. Emphasize instructions and other information important to the patient.● Prominently display information that is critical
for patient’s safe and effective use of therapy● At the top of the label, specify the patient’s
name, drug name (spelling out full generic and brand name), and strength/dose. Include explicitly clear directions for use in simple language
● Directions should follow a standard format so the patient can expect that each element will be in the same regimented order each time the medication is received
c. Simplify language● Language on the label should be clear, simpli-
fied, concise, and familiar, and should be used in a standardized manner. Only common terms and sentences should be used.
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 15
● Use simplified, standardized sentences that have been developed to promote ease of under-standing the instructions correctly.
d. Give explicit instructions● Do not use alphabetic characters for numbers.● Use standardized directions.● List which PN ingredients must be added by
the patient/caregiver.● Ambiguous directions such as “take as
directed” should be avoided unless clear and unambiguous supplemental instructions and counseling are provided.
e. Include purpose for use of PN using clear, sim-ple terms such as “for nutrition supplementa-tion” or “to provide nutrition”
f. Limit auxiliary information● Auxiliary information should be evidence
based in simple explicit language that is mini-mized to avoid distracting patients with nones-sential information.
● Information should be presented in a standard-ized manner and critical for patient under-standing and safe medication use.
● Use only icons for which adequate evidence suggests improved patient understanding about correct use of medication.
g. Address limited English proficiency● Whenever possible, the directions for use
should be provided in the patient’s preferred language, otherwise there is risk of misinter-pretation of instructions with limited English proficiency, which could lead to medication errors.
● Whenever possible, the directions for use should also appear in English to facilitate counseling.
● Medication names shall be in English so that emergency personnel and other intermediaries can have quick access to the information.
● Translations of prescription labels should be produced using a high-quality translation process.
h. Improve readability● Labels should be designed and formatted so
that they are easy to read.● Optimize typography using:
● high-contrast print● simple uncondensed familiar fonts with
space within letters and between letters● sentence case with initial capital followed
by lowercase words● large font size for critical information● adequate white space between lines of text
● white space to distinguish sections on the label such as directions for use vs pharmacy information
● horizontal text only● never truncate or abbreviate critical
information● highlighting, bolding, and other typographi-
cal cues should preserve readability and should emphasize patient-centric informa-tion or information that facilitates adherence
● limit the number of colors used for highlighting
● address visual impairment
Rationale
PN formulations are complex mixtures with multiple ingredi-ents. The pharmacy-generated label is a critical tool used to compare the PN ingredients and administration information against the PN order. Standardized pharmacy labels for PN for-mulations provide information in a clear, uniform, and organized manner, and improves the verification processes for pharma-cists.1 Additionally, the label serves as a final check for those administering the PN, including nurses or patients/caregivers.13 Listing ingredients in a uniform sequence and units of measure removes the need for calculations and reduces the risk of misin-terpretation. The misinterpretation of a PN label resulted in a child receiving an overdose of iron dextran and experiencing subsequent liver toxicity from iron overload.23 The lack of stan-dardization has created confusion, especially when patients are transferred from one healthcare environment to another.24
Question: Verification 4 (V4)
(V4) What processes can healthcare organizations implement to improve the safety of PN therapy during shortages of PN components?
Recommendations
1. Healthcare organizations (including vendors and home infusion providers) shall have a process to com-municate PN component shortages and outages to pre-scribers and staff who participate in providing PN therapy.25
2. Healthcare organizations shall develop and approve written PN component substitution protocols to be used in the event of a PN component shortage or outage.25
3. Healthcare organizations shall develop and approve written protocols for PN component substitution and/or conservation strategies to be used in the event of a PN component shortage or outage.25
by guest on January 9, 2014pen.sagepub.comDownloaded from
16 Journal of Parenteral and Enteral Nutrition XX(X)
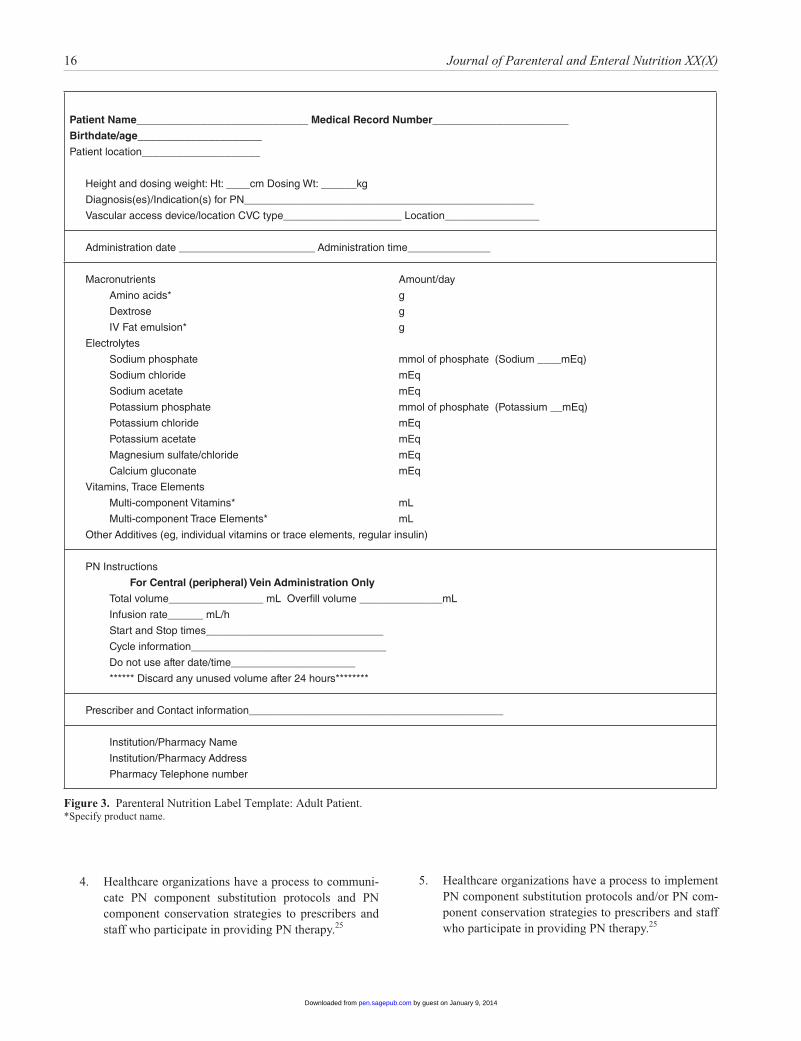
Figure 3. Parenteral Nutrition Label Template: Adult Patient.*Specify product name.
Patient Name_____________________________ Medical Record Number_______________________
Birthdate/age_____________________
Patient location____________________
Height and dosing weight: Ht: ____cm Dosing Wt: ______kg
Diagnosis(es)/Indication(s) for PN_________________________________________________
Vascular access device/location CVC type____________________ Location________________
Administration date _______________________ Administration time______________
Macronutrients Amount/day
Amino acids* g
Dextrose g
IV Fat emulsion* g
Electrolytes
Sodium phosphate mmol of phosphate (Sodium ____mEq)
Sodium chloride mEq
Sodium acetate mEq
Potassium phosphate mmol of phosphate (Potassium __mEq)
Potassium chloride mEq
Potassium acetate mEq
Magnesium sulfate/chloride mEq
Calcium gluconate mEq
Vitamins, Trace Elements
Multi-component Vitamins* mL
Multi-component Trace Elements* mL
Other Additives (eg, individual vitamins or trace elements, regular insulin)
PN Instructions
For Central (peripheral) Vein Administration Only
Total volume________________ mL Overfill volume ______________mL
Infusion rate______ mL/h
Start and Stop times______________________________
Cycle information_________________________________
Do not use after date/time_____________________
****** Discard any unused volume after 24 hours********
Prescriber and Contact information___________________________________________
Institution/Pharmacy Name
Institution/Pharmacy Address
Pharmacy Telephone number
4. Healthcare organizations have a process to communi-cate PN component substitution protocols and PN component conservation strategies to prescribers and staff who participate in providing PN therapy.25
5. Healthcare organizations have a process to implement PN component substitution protocols and/or PN com-ponent conservation strategies to prescribers and staff who participate in providing PN therapy.25
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 17
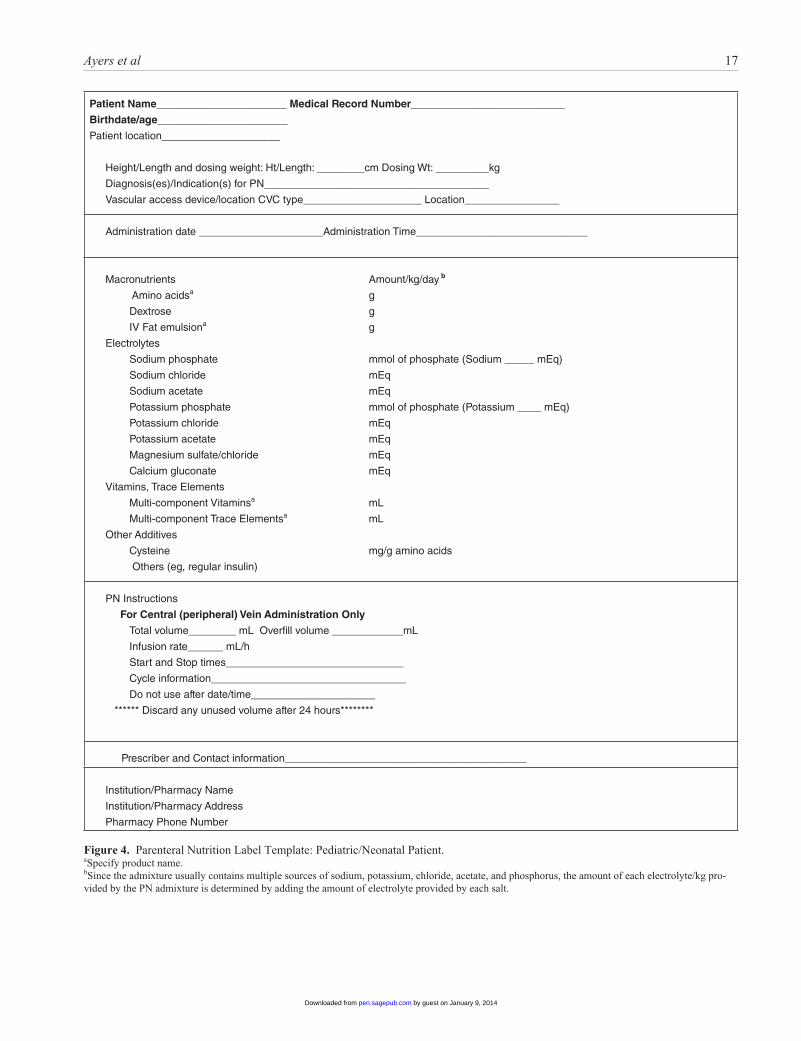
Figure 4. Parenteral Nutrition Label Template: Pediatric/Neonatal Patient.aSpecify product name.bSince the admixture usually contains multiple sources of sodium, potassium, chloride, acetate, and phosphorus, the amount of each electrolyte/kg pro-vided by the PN admixture is determined by adding the amount of electrolyte provided by each salt.
Patient Name______________________ Medical Record Number__________________________
Birthdate/age______________________
Patient location____________________
Height/Length and dosing weight: Ht/Length: ________cm Dosing Wt: _________kg
Diagnosis(es)/Indication(s) for PN______________________________________
Vascular access device/location CVC type____________________ Location________________
Administration date _____________________Administration Time_____________________________
Macronutrients Amount/kg/day b
Amino acidsa g
Dextrose g
IV Fat emulsiona g
Electrolytes
Sodium phosphate mmol of phosphate (Sodium _____ mEq)
Sodium chloride mEq
Sodium acetate mEq
Potassium phosphate mmol of phosphate (Potassium ____ mEq)
Potassium chloride mEq
Potassium acetate mEq
Magnesium sulfate/chloride mEq
Calcium gluconate mEq
Vitamins, Trace Elements
Multi-component Vitaminsa mL
Multi-component Trace Elementsa mL
Other Additives
Cysteine mg/g amino acids
Others (eg, regular insulin)
PN Instructions
For Central (peripheral) Vein Administration Only
Total volume________ mL Overfill volume ____________mL
Infusion rate______ mL/h
Start and Stop times______________________________
Cycle information_________________________________
Do not use after date/time_____________________
****** Discard any unused volume after 24 hours********
Prescriber and Contact information___________________________________________
Institution/Pharmacy Name
Institution/Pharmacy Address
Pharmacy Phone Number
by guest on January 9, 2014pen.sagepub.comDownloaded from
18 Journal of Parenteral and Enteral Nutrition XX(X)
Patient Name_____________________________ Medical Record Number_______________________
Birthdate/age_____________________
Patient location____________________
Height and dosing weight: Ht: ____cm Dosing Wt: ______kg
Diagnosis(es)/Indication(s) for PN_________________________________________________
Vascular access device/location CVC type____________________ Location________________
Administration date _______________________ Administration time______________
Infusion Volume Amount/day
Intravenous fat emulsiona mL g
Instructions
For Central or Peripheral Vein Administration
Total volume________ mL (may contain overfill)
Infusion rate______ mL/h
Infuse over __________h
Do not use after date/time_____________________
****** Discard any unused volume after 12 hours********
Prescriber Name/Contact Information __________________________________________________
Institution/Pharmacy Name
Institution/Pharmacy Address
Pharmacy Phone Number
Figure 5. Standard Intravenous Fat Emulsion Label Template: Adult.aSpecify product name.
6. PN component conservation and allocation strategies should include the A.S.P.E.N. PN product shortage considerations for multivitamins, trace elements, IVFE, amino acids, electrolyte/minerals, and cysteine. Thiamine, ascorbic acid, pyridoxine, and folic acid should be given daily. Thiamine is critical. Several deaths have resulted from cardiac failure due to thia-mine deficiency when long-term PN patients did not receive vitamins for 3 to 4 weeks. Patients receiving a carbohydrate load are particularly susceptible to thia-mine deficiency.17,26-31
7. Processes shall be in place to evaluate alternative PN components procured from compounding pharmacies, including compliance with USP General Chapter <797> Pharmaceutical Compounding-Sterile Preparations, federal laws and regulations, and state Boards of Pharmacy rules and regulations.
8. Processes should be in place to modify the PN order to reflect component outages and/or conservation strate-gies in a timely manner.
9. Processes should be in place to modify the PN label to reflect changes in the PN order due to component out-ages and/or PN component conservation strategies.
10. Processes should be in place to modify ACD software to reflect changes in PN components due to outages and/or conservation strategies. This includes compati-bility of all ingredients and changing National Drug Code (NDC) numbers, which is mandatory for barcod-ing systems to function correctly. Any changes in ACD software should require two individuals to perform the validation check using a standardized process and checklist.
11. Quality improvement programs should be in place to track and analyze errors associated with PN
by guest on January 9, 2014pen.sagepub.comDownloaded from
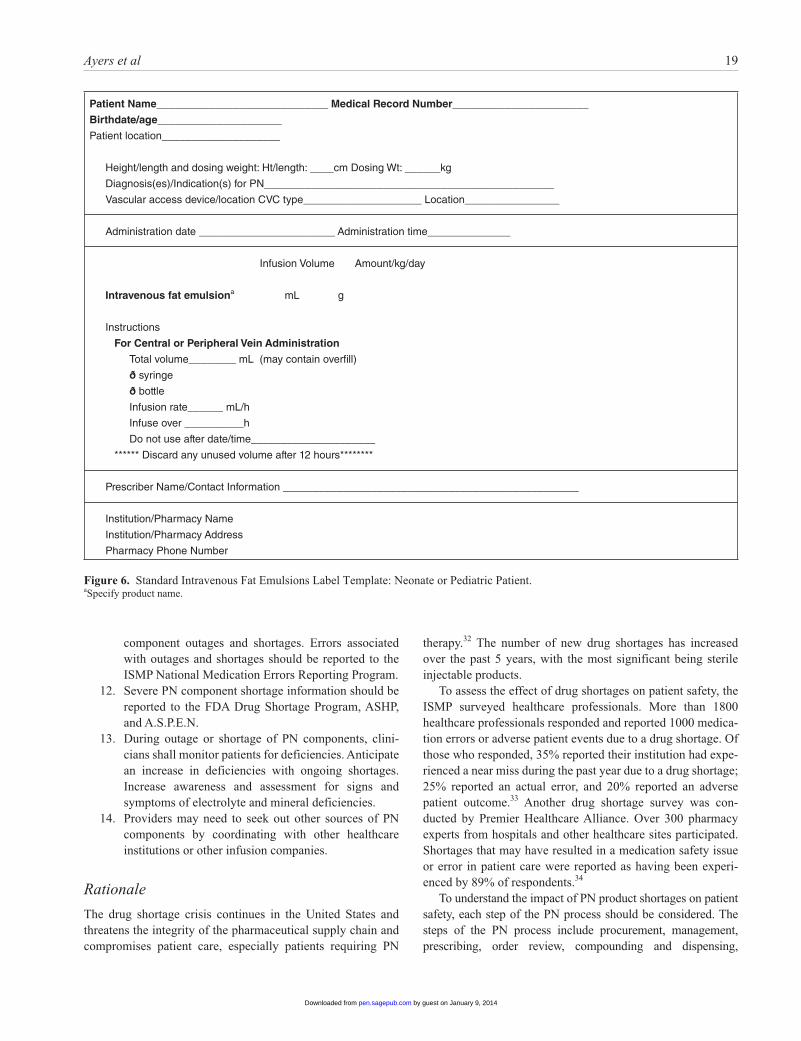
Ayers et al 19
Patient Name_____________________________ Medical Record Number_______________________
Birthdate/age_____________________
Patient location____________________
Height/length and dosing weight: Ht/length: ____cm Dosing Wt: ______kg
Diagnosis(es)/Indication(s) for PN_________________________________________________
Vascular access device/location CVC type____________________ Location________________
Administration date _______________________ Administration time______________
Infusion Volume Amount/kg/day
Intravenous fat emulsiona mL g
Instructions
For Central or Peripheral Vein Administration
Total volume________ mL (may contain overfill)
ð syringe
ð bottle
Infusion rate______ mL/h
Infuse over __________h
Do not use after date/time_____________________
****** Discard any unused volume after 12 hours********
Prescriber Name/Contact Information __________________________________________________
Institution/Pharmacy Name
Institution/Pharmacy Address
Pharmacy Phone Number
Figure 6. Standard Intravenous Fat Emulsions Label Template: Neonate or Pediatric Patient.aSpecify product name.
component outages and shortages. Errors associated with outages and shortages should be reported to the ISMP National Medication Errors Reporting Program.
12. Severe PN component shortage information should be reported to the FDA Drug Shortage Program, ASHP, and A.S.P.E.N.
13. During outage or shortage of PN components, clini-cians shall monitor patients for deficiencies. Anticipate an increase in deficiencies with ongoing shortages. Increase awareness and assessment for signs and symptoms of electrolyte and mineral deficiencies.
14. Providers may need to seek out other sources of PN components by coordinating with other healthcare institutions or other infusion companies.
Rationale
The drug shortage crisis continues in the United States and threatens the integrity of the pharmaceutical supply chain and compromises patient care, especially patients requiring PN
therapy.32 The number of new drug shortages has increased over the past 5 years, with the most significant being sterile injectable products.
To assess the effect of drug shortages on patient safety, the ISMP surveyed healthcare professionals. More than 1800 healthcare professionals responded and reported 1000 medica-tion errors or adverse patient events due to a drug shortage. Of those who responded, 35% reported their institution had expe-rienced a near miss during the past year due to a drug shortage; 25% reported an actual error, and 20% reported an adverse patient outcome.33 Another drug shortage survey was con-ducted by Premier Healthcare Alliance. Over 300 pharmacy experts from hospitals and other healthcare sites participated. Shortages that may have resulted in a medication safety issue or error in patient care were reported as having been experi-enced by 89% of respondents.34
To understand the impact of PN product shortages on patient safety, each step of the PN process should be considered. The steps of the PN process include procurement, management, prescribing, order review, compounding and dispensing,
by guest on January 9, 2014pen.sagepub.comDownloaded from
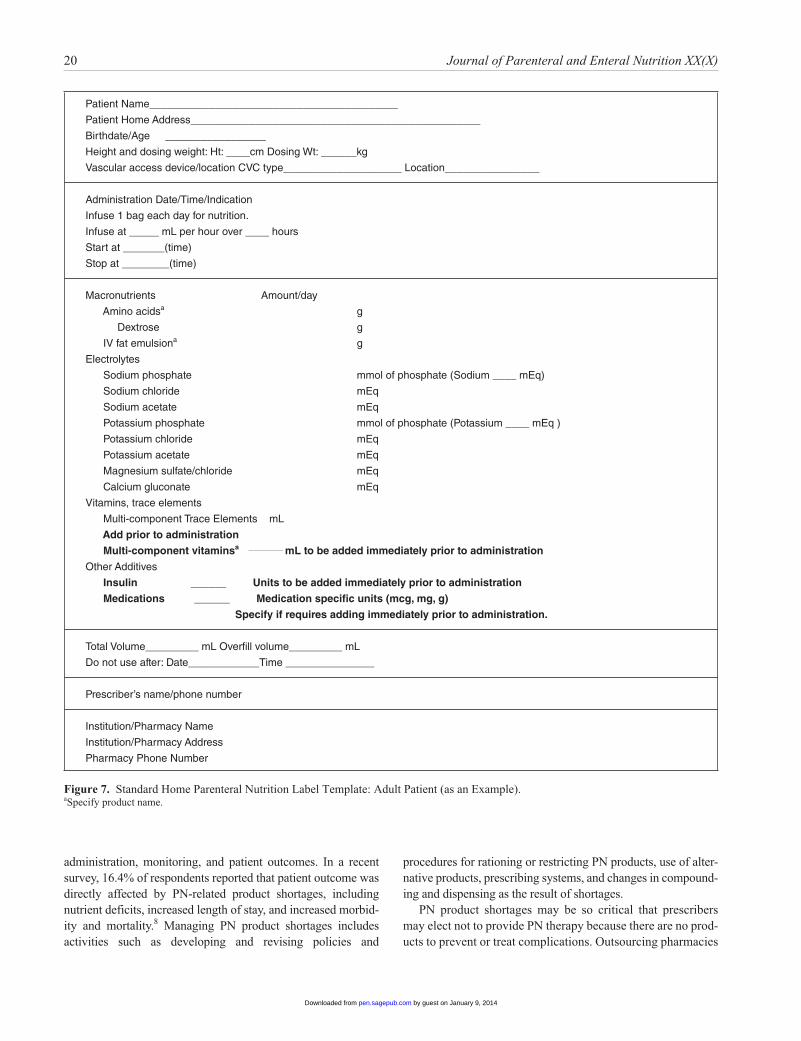
20 Journal of Parenteral and Enteral Nutrition XX(X)
Figure 7. Standard Home Parenteral Nutrition Label Template: Adult Patient (as an Example).aSpecify product name.
administration, monitoring, and patient outcomes. In a recent survey, 16.4% of respondents reported that patient outcome was directly affected by PN-related product shortages, including nutrient deficits, increased length of stay, and increased morbid-ity and mortality.8 Managing PN product shortages includes activities such as developing and revising policies and
procedures for rationing or restricting PN products, use of alter-native products, prescribing systems, and changes in compound-ing and dispensing as the result of shortages.
PN product shortages may be so critical that prescribers may elect not to provide PN therapy because there are no prod-ucts to prevent or treat complications. Outsourcing pharmacies
Patient Name__________________________________________
Patient Home Address_________________________________________________
Birthdate/Age _________________
Height and dosing weight: Ht: ____cm Dosing Wt: ______kg
Vascular access device/location CVC type____________________ Location________________
Administration Date/Time/Indication
Infuse 1 bag each day for nutrition.
Infuse at _____ mL per hour over ____ hours
Start at _______(time)
Stop at ________(time)
Macronutrients Amount/day
Amino acidsa g
Dextrose g
IV fat emulsiona g
Electrolytes
Sodium phosphate mmol of phosphate (Sodium ____ mEq)
Sodium chloride mEq
Sodium acetate mEq
Potassium phosphate mmol of phosphate (Potassium ____ mEq )
Potassium chloride mEq
Potassium acetate mEq
Magnesium sulfate/chloride mEq
Calcium gluconate mEq
Vitamins, trace elements
Multi-component Trace Elements mL
Add prior to administration
Multi-component vitaminsa _________ mL to be added immediately prior to administration
Other Additives
Insulin ______ Units to be added immediately prior to administration
Medications ______ Medication specific units (mcg, mg, g)
Specify if requires adding immediately prior to administration.
Total Volume_________ mL Overfill volume_________ mL
Do not use after: Date____________Time _______________
Prescriber’s name/phone number
Institution/Pharmacy Name
Institution/Pharmacy Address
Pharmacy Phone Number
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 21
may dictate to customers PN product conservation strategies. Although this is severe, the PN product shortages have resulted in prescribing suboptimal therapy due to shortages or rationing of products. The prescribing step is affected as prescribers find it difficult to keep up with shortages, alternative products, rationing, restrictions, and so on. Furthermore, the prescribing process is constantly changing, and prescribers may use work-arounds to circumvent safety checks. Lastly, an increase in the number of prescribing errors has been associated with shortages.31
Many of the same safety concerns have been identified in the PN order review step. Pharmacists who perform this step have difficulty staying current with shortages, alternative prod-ucts, and rationing. There has been an increase in the number of PN orders that require clarification or those with prescribing errors.
The compounding and dispensing steps are associated with numerous patient safety issues resulting from PN product shortages. As with other aspects of the PN process, those responsible for compounding and dispensing find it difficult and stressful trying to keep up with the many shortages. During a shortage, alternative products that are unfamiliar or are simi-lar in appearance to other products may be substituted. This may lead to errors. Furthermore, PN may be compounded using alternative products such as calcium chloride or magne-sium chloride, for which there are insufficient stability and compatibility data or known unfavorable differences. Frequent changes in PN products or the size of the source containers necessitate a change in the configuration of ACD, increasing the potential for error. Some products cannot be configured for the ACD, requiring a manual addition to a PN formulation. Frequent changes in products, alternative products, ordering process, and ACD configuration may result in PN orders and PN bag labels that do not match. This creates significant con-cerns for those responsible for the administration of the PN admixture.
The PN product shortages affect the administration of PN whether administered by a nurse, patient, or caregiver. Just like others involved in the PN process, it is difficult and stressful to keep current with the shortages. As noted above, the PN order and PN bag labels may not match as the result of changes in the compounding process. With some shortages, patients may require supplemental electrolyte or mineral infusions when the alternative product cannot be added to the PN formulation due to stability or compatibility concerns. Increasing the number of times the patient’s intravascular device is accessed may increase the risk of catheter-related bloodstream infections.29 A recent study of PN practices reported the consequences of PN product shortages. Of the pharmacists responding, more than two-thirds reported that valuable time is consumed in develop-ing contingencies. Additionally, 70.3% of respondents indi-cated that shortages interfere with the ability to meet patients’ micronutrient needs, and almost half reported that shortages interfere with ability to meet macronutrient needs.8
The lack of a PN component increases the risk of a defi-ciency of that nutrient or complications. Shortages have been associated with patient harm. Anemia and leukopenia due to copper deficiency has been reported in an adult patient receiv-ing PN without trace elements for 4 months.35 Clinicians must have a heightened awareness of potential deficiencies and monitor for the deficiencies or associated complications.
The shortages pose safety risks throughout the entire PN process, from procurement to patient outcomes. Providing PN therapy during product shortages requires vigilance and con-tinuous assessment of the entire PN process to optimize patient care quality and avoid patient harm.
Topics for Future Research
1. Demonstration of decrease in PN errors when CPOE systems are fully integrated with ACDs.
2. Demonstration of decrease in PN errors with elimina-tion of handwritten paper PN orders and use of editable electronic orders or CPOE systems for prescribing PN.
3. Documentation of PN errors associated with PN verifi-cation process.
4. Documentation of PN errors associated with the clini-cal and pharmaceutical reviews of PN orders.
5. Documentation of PN errors associated with transcrip-tion of PN data from the order to an ACD.
6. Impact of PN order standardization on PN data tran-scription errors.
7. Demonstration of PN error reduction with implemen-tation of standardized review and verification of PN orders.
8. Demonstration of a reduction in PN errors with imple-mentation of a standardized checklist for the verifica-tion and review of PN orders.
9. Impact of a fully integrated electronic system for pre-scribing PN and data into an ACD.a. Demonstration of medication error reductionb. Demonstration of improved patient safetyc. Demonstration of decreased costs
10. Documentation of PN errors associated with PN order calculations.
11. Documentation of PN errors associated with misinter-pretation of PN bag labeling.
12. Demonstration of PN error reduction with standard-ized PN labeling.
13. Development and implementation of a standardized home PN label that is consistent with the A.S.P.E.N. Safe Practices for PN and USP General Chapter <17>.
14. Evaluation of patient understanding and satisfaction with PN labeling that is consistent with the A.S.P.E.N. Safe Practices for PN and USP General Chapter <17>.
15. Demonstration of reduction in PN errors when PN orders are reviewed by a pharmacist with specialty residency training and/or BCNSP certification.
by guest on January 9, 2014pen.sagepub.comDownloaded from
22 Journal of Parenteral and Enteral Nutrition XX(X)
16. Report of successful PN formal training programs for pharmacists and pharmacy technicians.
17. Demonstration of PN error reduction with PN formal training programs for pharmacists and pharmacy technicians.
18. Compatibility of PN components, including macronu-trients, micronutrients, and non-nutrient medications.
19. Determination of maximum osmolarity of PN formula-tions for administration via peripheral veins.
20. Impact of PN product shortages on patient outcomes.
References
1. Mirtallo J, Canada T, Johnson D, et al; A.S.P.E.N. Board of Directors and Task Force for the Revision of Safe Practices for Parenteral Nutrition. Safe practices for parenteral nutrition [published correction appears in JPEN J Parenter Enteral Nutr. 2006;30:177]. JPEN J Parenter Enteral Nutr. 2004;28:S39-S70.
2. Boullata JI. Overview of the parenteral nutrition use process. JPEN J Parenter Enteral Nutr. 2012;36:10S-13S.
3. Institute for Safe Medication Practices. Mismatched prescribing and phar-macy templates for parenteral nutrition (PN) lead to data entry errors. ISMP Medication Safety Alert! June 28, 2012. Accessed November 25, 2012.
4. Institute for Safe Medication Practices. Independent double-checks: undervalued and misused. ISMP Medication Safety Alert! June 13, 2013. Accessed June 2, 2013.
5. Institute for Safe Medication Practices. 1,000-Fold overdoses can occur, particularly in neonates, by transposing mcg and mg. ISMP Medication Safety Alert! September 6, 2007. Accessed November 25, 2012.
6. O’Neal BC, Schneider PJ, Pedersen CA, Mirtallo JM. Compliance with safe practices for preparing parenteral nutrition formulations. Am J Health-Syst Pharm. 2002;59:264-269.
7. Seres D, Sacks GS, Pedersen CA, et al. Parenteral nutrition safe practices: results of the 2003 American Society for Parenteral and Enteral Nutrition survey. JPEN J Parenter Enteral Nutr. 2006;30:259-265.
8. Boullata J, Guenter P, Mirtallo J. A parenteral nutrition use survey with a gap analysis. JPEN J Parenter Enteral Nutr. 2012;13:212-222.
9. Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293:1197-1203.
10. Shamliyan TA, Duval S, Du J, Kane RL. Just what the doctor ordered: review of the evidence of the impact of computerized physician order entry on medication errors. HSR Health Serv Res. 2008;43:32-53.
11. Sacks GS, Rough S, Kudsk KA. Frequency and severity of harm of medi-cation errors related to the parenteral nutrition process in a large university teaching hospital. Pharmacotherapy. 2009;29:966-974.
12. Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. JAMA. 2005;293:1197-1120.
13. Institute for Safe Medication Practices. Another tragic parenteral nutri-tion compounding error. ISMP Medication Safety Alert! April 21, 2011. Accessed November 25, 2012.
14. Institute for Safe Medication Practices. Mismatched prescribing and phar-macy templates for parenteral nutrition (PN) lead to data entry errors. ISMP Medication Safety Alert! June 28 2012. Accessed November 25, 2012.
15. Jacobson JO, Polovich M, Gilmore TR, et al. Revisions to the 2009 American Society of Clinical Oncology/Oncology Nursing Society Chemotherapy Administration Safety Standards: expanding the Scope to Include Inpatient Settings. Oncology Nurs Forum. 2012;39:31-38.
16. The Joint Commission. Official “Do Not Use” abbreviations list. Information Management Standard IM 02.02.01.
17. Institute for Safe Medication Practices. List of error-prone abbreviations, symbols, and dose designations. http://www.ismp.org/tools/errorproneab-breviations.pdf. Accessed January7, 2013.
18. Information to use in the event of an intravenous multivitamin shortage—May 2012: information to use in the event of adult IV multivitamin short-age. American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/lcontent.aspx?id=5346. Accessed January 6, 2013.
19. Meyer LD, Raymond CB, Rodrigue CM. Development and evaluation of a checklist for medication order review by pharmacists. Can J Hosp Pharm. 2011;64:199-206.
20. Pedersen CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: monitoring and patient educa-tion—2012. Am J Health-Syst Pharm. 2013;70:787-803.
21. Durfee SM. Pharmacist specialty certification. JPEN J Parenter Enteral Nutr. 2012;36(2)(suppl):51S-52S.
22. Boitano M, Bojak S, McCloskey S, McCaul DS, McDonough M. Improving the safety and effectiveness of parenteral nutrition: results of a quality improvement collaboration. Nutr Clin Pract. 2010;25:663-671.
23. USP General Chapter <17> Prescription Container Labeling. 2012. The United States Pharmacopeial Convention.
24. Iron overdose due to miscommunication of TPN order: error alert. Pharmacy Today. September 1995.
25. Carey LC, Haffey M. Incident: home TPN formula order misinterpreted after hospital admission. Home Care Highlights. Spring 1995:7.
26. The Joint Commission. Medication Management Standard MM. 02.01. 2012.
27. Information to use in the event of an intravenous amino acids shortage. American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/Index.aspx?id=5646. Accessed January 6, 2013.
28. Information to use in the event of an intravenous fat emulsion shortage—June 2010. American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/Professional_Resources/Information_to_Use_in_the_Event_of_an_Intravenous_Fat_Emulsion_Shortage/. Accessed January 6, 2013.
29. Parenteral nutrition trace element product shortage considerations (5-19-2011). American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/News/Parenteral_Nutrition_Trace_Element_Product_Shortage_Considerations/. Accessed January 6, 2013.
30. Holcombe B, Andris DA, Brooks G, Houston DR, Plogsted SW. Parenteral nutrition electrolyte/mineral product shortage considerations. JPEN J Parenter Enteral Nutr. 2011;35:434-436.
31. Parenteral nutrition cysteine product shortage considerations—September, 2011. American Society for Parenteral and Enteral Nutrition website. http://www.nutritioncare.org/Professional_Resources/Guidelines_and_Standards/Guidelines/PN_Cysteine_Product_Shortage_Considerations/. Accessed January 6, 2013.
32. Holcombe B. Parenteral nutrition product shortages: impact on safety. JPEN J Parenter Enteral Nutr. 2012;36:44S-47S.
33. Institute for Safe Medical Practices. Drug shortages: national survey reveals high level of frustration, low level of safety. ISMP Medication Safety Alert! 2010;15(19):1-4. http://www.ismp.org/newsletters/acutec-are/articles/20100923.asp. Accessed September 2, 2012.
34. Cherici C, Frazier J, Feldman M, et al. Navigating drug shortages in American healthcare: a premier healthcare alliance analysis. Premier drug shortage white paper. http://www.premierinc.com/about/news/11-mar/drug-shortage-white-paper-3-28-11.pdf. Accessed September 4, 2012.
35. Pramyothin P, Kim DW, Young LS, Wichansawakun S, Apovian CM. Anemia and leukopenia in a long-term parenteral nutrition patient during a shortage of parenteral trace element products in the United States. JPEN J Parenter Enteral Nutr. 2013;37:425-429.
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 23
Compounding
Background
Recent PN errors caused by a knowledge deficit, lack of train-ing, insufficient competency, and poor proficiency with ACDs are areas of significant concern. Additionally, a lack of compe-tency-based educational curriculum in schools of pharmacy or pharmacy technician training programs may contribute to PN errors. Very few suitable studies exist that characterize the for-malized training of pharmacy students or technicians in the preparation of sterile products and admixtures. Available data suggest that when pharmacy students are formally taught asep-tic technique skills with direct observation and assessment of parenteral compounding procedures, microbial contamination rates related to medium-risk level compounding (eg, PN com-pounding) decreased significantly from baseline toward the end of the 16-week course.1 Several recommendations pertain-ing to the knowledge and competency of staff involved in the preparation of compounded sterile products were developed at the recent ISMP Sterile Preparation Compounding Safety Summit.2 Surveys of pharmacists at the beginning of postgrad-uate training programs demonstrated that first-year pharmacy residents reported minimal experience (median = 2) on a scale from 1 to 5 (5, most experience and 1, no experience) with PN evaluations and IV admixtures. This suggests that there are educational deficits in current pharmacist training related to areas important for institutional or homecare pharmacy prac-tice.3 Observational data from practicing hospital pharmacists and pharmacy technicians revealed that compounding error rates were 37% when PN formulations were manually com-pounded and 22% when prepared with an ACD. Errors included touch contamination, incorrect calculations performed by tech-nicians, and bypassing the built-in safety check systems on ACDs.4
Question: Compounding 1–2 (C1–C2)
(C1) What compounding errors have been caused by deficits in knowledge, lack of training, competency, and proficiency?(C2) What compounding errors have been caused by a lack of standardized educational curriculum in schools of pharmacy or pharmacy technician programs?
Recommendations
1. Schools of pharmacy in the United States shall develop curricula that address proper aseptic technique and USP Chapter <797> for making compounded sterile preparations (CSPs).
2. Pharmacy technicians shall be certified by the Pharmacy Technician Certification Board if they are involved in the making of CSPs, including PN.
3. Healthcare organizations shall provide a broad orienta-tion with an in-depth training program focusing on CSPs for all staff members supervising or participating in the
preparation process. An ongoing competency assess-ment program shall be included in the training as well.
4. Healthcare organizations shall require annual compe-tency evaluations of pharmacists and pharmacy techni-cians involved in preparation of CSPs. This should include:a. Calculationsb. Compounding base solutionsc. Preparing dilutions or aliquotsd. Aseptic technique manipulationse. Using technology (ie, ACD) for preparationf. Anticipating incompatibilities (calcium, phos-
phate)5. Organizations should develop a strategic plan for
implementation of automation and technology for the sterile products service.
6. Pharmacists and pharmacy technicians shall be profi-cient in the proper use of technology (ie, ACD) when used for preparation of CSPs.
7. State Boards of Pharmacy should create a specific license and licensing requirements for infusion phar-macies and compounding pharmacies.
8. State Boards of Pharmacy should provide an in-depth training program focusing on CSPs for all State Board inspectors. An ongoing competency assessment pro-gram should be included in the training as well.
Rationale
The lack of standardized training emphasizing foundational concepts behind sterile compounding and aseptic technique is startling in today’s professional programs educating both phar-macists and pharmacy technicians. Over the past 5 years, numerous reports of serious morbidity and mortality have appeared in the lay press due to a lack of training in aseptic technique with preparation of sterile products. The most recent tragic events have surrounded a rare outbreak of fungal menin-gitis that was traced to several lots of the injectable glucocorti-coid methylprednisolone acetate compounded by the New England Compounding Center. Although these sterile injec-tions were intended for back and joint pain, a lack of sterile compounding competency has sickened hundreds of patients and killed dozens.5 Even more relevant are the 9 deaths that occurred in Alabama during the preparation of amino acids under high-risk conditions and an error in sterile compounding technique. It is incumbent on pharmacists to check that all people involved in the oversight and preparation of CSPs obtain appropriate training and be evaluated on a regular basis through a competency assessment. Pharmacists would receive education in the physicochemical principles of pharmacy and practice experiences as part of a pharmacy school curriculum. Technicians would receive education in the operations of ACD hardware and software with varied practice experiences as part of the curriculum. Board certification for those involved in CSPs could guarantee a basic minimum requirement in lieu of
by guest on January 9, 2014pen.sagepub.comDownloaded from

24 Journal of Parenteral and Enteral Nutrition XX(X)
formalized training as part of a curriculum. The criteria required for nutrition support pharmacy board certification would suggest that these individuals are better prepared to allow fewer errors, although no data are available to support this contention. Anecdotal data would suggest that pharmacists and pharmacy technicians with specific education and many hours of hands-on experience are in the best position to be involved with PN compounding. In the workplace, pharma-cists and technicians should participate in a comprehensive orientation and training program with an ongoing competency assessment plan.2 This plan would evaluate all aspects of ster-ile compounding from calculations to the proper use of technology.
Question: Compounding 3 (C3)
(C3) How can organizations avoid PN errors by implementing soft and hard limits on an ACD?
Recommendations
1. Organizations shall implement specific computerized soft limits and hard (catastrophic) limits for PN ingre-dients based upon pharmacists’ review that are consis-tent with the needs of their patient population.
2. Access to the ACD database is limited to select indi-viduals qualified to manage and maintain this activity and all changes are traceable. Pharmacists and techni-cians shall be educated on interpretation and limita-tions of calcium-phosphate compatibility curves in the software.
3. Weight-based warning limits for doses shall be devel-oped by clinicians with the assistance of the vendors. As an alternative, organizations may develop and use their own weight-based warning limits.
4. Only pharmacists shall be allowed to override alerts. An independent double-check process should be com-pleted by another pharmacy staff member, ideally another pharmacist.2
5. Healthcare organizations should check that all unre-solved ACD alerts encountered during the PN order entry process should be presented to the person review-ing the order entry so they can also view and respond to the alerts.
6. Healthcare organizations shall reinforce the impor-tance of reacting to the ACD alerts and documenting all interventions.
7. Healthcare organizations should review available reports detailing the frequency of overrides as well as the frequency of overrides for specific PN components.
Rationale
Limits can be placed on the doses of each PN component to optimize safety within the compounding process. These limits
can be automated within the PN order-prescribing, reviewing, and/or compounding process. The term “hard limits” refers to alerts that indicate that a component is outside a determined safe range and shall not be exceeded; these are also referred to as “catastrophic” given patient outcomes if exceeded.2 “Soft limits” refer to alerts that indicate an unusual dose that requires further evaluation. Once addressed, any alert that is overridden or any dosing that is revised will require documentation of the rationale. Compared with manual methods, the software appli-cation available with ACDs should lead to improved com-pounding accuracy, enforcement of proper compounding sequence, and a reduction in opportunities for human touch contamination. However, preparing PN admixtures with an ACD is not an error-free process. Error rates in compounding complex preparations such as PN admixtures have been reported to be 22% when automated in part and 37% when manually prepared.6 Organizations may improve the safety of using PN compounding systems by requiring that all doses being compounded pass through an order entry/clinical deci-sion support system and by ensuring that those systems’ clini-cal decision support features are properly enabled and configured. Transcription of PN order data from an order-cal-culating software package into a compounding device should be avoided. In a recent survey on PN use, Boullata et al found that dose limit warnings were active in only two-thirds of orga-nizations that used ACDs for preparing PN formulations.7 ISMP Medication Safety Alerts from 2007 and 2011 described incidents in which adverse outcomes resulted, in part, from the absence of dose limit warnings.8,9 In both instances, infants received lethal doses of a micronutrient (zinc in one case, sodium in the other) when a manual order entry error was either not detected by the existing dose limits or dose limit alerts were not active. After reviewing the incidents, ISMP made a number of safe practice recommendations. Among these was the recommendation to install, test, and maximize automated dose-limit warnings in the pharmacy computer sys-tem and the ACD order entry system, particularly for high-alert medications such as PN and its ingredients. Further, ISMP rec-ommends that each organization develop weight-based dosing limits applicable to their patient populations, as ACD vendor-established “catastrophic” limits may still allow entry of a potentially fatal dose into the software without issuing a warning.8,9
The ASHP guidelines on the safe use of ACDs for the prep-aration of PN admixtures state that the pharmacy department should develop a monitoring and surveillance plan that pro-motes safe and efficacious use of the device at all times.10 This plan should include a review of dose-limit alerts and overrides, utilizing the reporting capabilities of the ACD or pharmacy computer system.
DeBoer and Maddox described a review of smart pump data after implementation throughout the Sanford USD Medical Center.11 Three to six months of smart pump data were col-lected for each unit and an analysis of edit variance detail and override variance detail was performed. After the initial review
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 25
was completed, data were analyzed for medications included in the ISMP high-alert medication list. Work practices were evaluated and revised with the goal of encouraging fewer edits and overrides. In a similar fashion, data from the ACD or phar-macy computer system should be regularly reviewed in the assessment of trends and other long-term measures of performance.
Question: Compounding 4 (C4)
(C4) What role does United States Pharmacopeia (USP) Chapter <797> play in preventing PN errors?
Recommendations
1. Healthcare organizations shall comply with USP Chapter <797> standards.12
2. Outsourcing should be considered as an alternative to in-house compounding when the healthcare organiza-tion does not possess the technological resources or staffing to prepare PN admixtures according to USP Chapter <797>. The decision to outsource should require that the pharmacy outsourcing PN production exercise due diligence to monitor that the outsourcer also operates within USP <797> guidelines.
3. Standardized, commercially available PN products may be viable options to manually compounded sterile PN products when compliance with USP Chapter <797> and accepted guidelines from patient safety organizations is not feasible.
4. Healthcare organizations shall have policies and proce-dures that address using multichamber, standardized, commercial PN products within their formulary.
5. Healthcare organizations shall have well-defined poli-cies and procedures that guide the preparation of PN admixtures.
6. Healthcare organizations must identify standardized workflow processes that include quality control, pro-cess change control, and documentation practices. These standardized operating procedures should encompass the entire compounding process from order entry to verification of the final labeled product.
7. Healthcare organizations should develop a strategic plan to include technology/automation for sterile com-pounding and consider using IV workflow software.2
8. When an ACD is used to prepare PN admixtures, poli-cies and procedures shall be developed that address performance requirements and responsibilities, control of the ACD in daily operations, safety and efficacy fea-tures, quality assurance monitoring and documenta-tion, storage and inventory, education and training, and device variability and maintenance.
9. Privileges to make changes in the ACD database shall be restricted to a limited number of pharmacy staff who are well trained in both the theory and the mechan-ics of this process.2
10. Customized order entry templates created by organiza-tions should have a documented standard review pro-cess by qualified staff person that includes review and testing of the clinical decision support that is expected to alert the pharmacist to significant warnings. The use of a checklist or sign-off sheet shall be required and two staff members, including at least one pharmacist, shall sign off on or validate the template.2
11. The additive sequence in compounding shall be opti-mized and validated as a safe and efficacious method. Manufacturers of ACDs shall provide an additive sequence that promotes the safety of the compounding device. This compounding sequence should be reviewed with the manufacturer of the PN products used by the organization.13
12. The use of a checklist or signoff sheet shall be required when adding new products, including new and alterna-tive generics, changes in vial size or concentration, and when making other modifications to the ACD database (eg, changes in privileges, changes in data require-ments). Two staff members shall be required to sign off on or validate changes. (This process would not apply to inputting a new lot number for a product already in the database.)2
13. Barcode verification shall be used to verify product identity during ACD setup and replacement of ingredients.2
14. An independent double-check process for the initial daily ACD setup shall be performed by two staff mem-bers using a printed checklist. Verbal affirmation should take place to validate placement of all additives and base solutions, including name, concentration, and container size.2 When the vendor of the compounding system describes a validated system for proper setup, that system should be followed.
15. Tubing set(s) shall be traced from the source container to the port where it is attached during the initial daily ACD setup and with each change in the source container.2
16. If multiple containers of a single additive are used dur-ing the preparation of a single CSP, all empty contain-ers shall be presented to the pharmacist and verified as part of the final check process prior to dispensing the final CSP.2
17. When an ACD is used, it should deliver all ingredients. Manual compounding should only be used:a. If the volume of a PN component to be mixed is
less than the ACD can accurately deliver.b. If there is an interaction between a PN compo-
nent and a component of the ACD (eg, insulin and tubing).
c. If there is a chemical interaction between PN components that cannot be mitigated by sequencing the addition of ingredients.
d. During a shortage of a specific PN component, manual compounding can be a consideration as part of conservation efforts.
by guest on January 9, 2014pen.sagepub.comDownloaded from

26 Journal of Parenteral and Enteral Nutrition XX(X)
18. Verification of manual additives should include inspec-tion of the actual vials and syringes that contain the additives.9 Proxy methods of verification (eg, syringe pullback) shall not be used.2
19. If the manual method is being used, the process should be standardized to promote safety and efficacy.13 The use of a checklist or sign-off sheet shall be incorpo-rated into the manual process.
20. PN orders should be prescribed, transmitted, and com-pounded when supported by properly trained person-nel who regularly perform this task.9 This is usually during the daytime hours.
21. In facilities that care for adult, pediatric, and neonatal patients, the preparation of CSPs for each population shall be separated by time or location. Separation strat-egies can include the use of different colored bins for assembling products to be prepared.2
22. At least three verification processes should occur in the pharmacy: (1) after initial order entry of PN, (2) before manually injecting additives into the PN, and (3) once the PN has been compounded.9 In-process or end-product testing requires that the PN prepara-tion be held pending results. It may be better to fully automate and validate the entire PN compounding process to prevent errors from being made in the first place.
23. Organizations should develop a drug conservation pol-icy that addresses the handling and disposition of PN components (while maintaining their integrity and ste-rility) that may be in short supply due to market condi-tions, as these shortages can affect workflow conditions.
24. The physical environment in which PN compounding takes place should be assessed in terms of lighting, interruptions and distractions, sound and noise, ergo-nomics, and medication safety zone. USP General Chapter <1066> describes optimal physical environ-ment standards that promote safe medication use throughout the medication-use process.14 Any defi-ciencies should be addressed following organizational chain of command.
25. Once a standardized process for compounding PN has been implemented, organizations should review and revise the process on an annual basis along with a review of personnel compounding behavior.
26. Operation of the compounding process must be rou-tinely observed for procedural compliance and correc-tive action must be taken immediately if noncompliance is observed.
Rationale
An ASHP national survey of pharmacy practice in hospital set-tings published in 2012 found that overall, 65% of hospital
pharmacy departments reported having a United States Pharmacopeia (USP) Chapter <797> compliant cleanroom.15 Having a USP Chapter <797> compliant cleanroom differed significantly by hospital size, with more than 87.5% of the largest hospitals (600 or more staffed beds) having a compliant cleanroom, compared with 48.1% of hospital pharmacy depart-ments in hospitals with fewer than 50 beds. Commercially available PN multichamber bags were used by 36% of hospi-tals as the predominant form of PN formulation. ACDs were used by 20.4% of hospitals, followed by gravity methods (17.4%) and outsourcing compounding activities (14.6%); 11.6% of hospitals did not prepare PN formulations. The method of preparing PN differed significantly by hospital size. Larger hospitals most commonly used ACDs or outsourced preparations. Hospitals with fewer than 50 staffed beds most commonly used commercially available dextrose/amino acid formulations or TNA did not prepare any PN admixtures or used gravity methods to prepare PN.15
Organizations should refer to a number of available guide-lines and articles regarding standardization of the PN com-pounding process (see Table 2). Organizations compounding PN admixtures must have well-defined policies and procedures to guide each step of preparation and shall comply with stan-dards set forth in USP Chapter <797>.2 Compounding PN “as usual” is no longer acceptable if it does not comply fully with USP Chapter <797>.18 Error rates in compounding complex preparations such as PN admixtures have been reported to be 22% when automated in part and 37% when manually pre-pared.6 Error rates of 24% in PN preparation were identified in a prospective observational study.19 Compounding errors that result in an unexpected patient event occur in 30% of hospi-tals.6 The USP chapter that describes the compounding of ster-ile preparations provides minimum practice and quality standards based on current scientific information and best ster-ile compounding practices.12 Organizations that are unable to comply with USP Chapter <797> and accepted guidelines from patient safety organizations should consider alternative compounding options such as outsourcing or standardized commercially available PN products.
Policies that require prescribers to order PN daily before a specified deadline should be established and enforced to maxi-mize the safety with which these admixtures are prepared and dispensed. Pharmacy staff should be aware of all patients who are receiving PN and check if orders have not been received by the established deadline. PN ingredients considered to be very small volumes that staff manually prepare, check, and inject require verification, including inspection of the vials and syringes containing such additives. Verification of manual additives should include inspection of the actual vials and syringes that contain the additives. Proxy methods of verifica-tion such as the syringe pull-back method of verification should not be used in the preparation of PN and other high-alert CSPs and shall not be used without the presence of the actual original source containers (medication and diluent).2
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 27
Table 2. Documents Discussing the Standardization of the Parenteral Nutrition Preparation Process.
Source Title Publisher Publication Year Reference Number
USP Chapter <797> – “The objective of this chapter is to describe conditions and practices to prevent harm, including death, to patients that could result from the following: (1) microbial contamination (nonsterility), (2) excessive bacterial endotoxins, (3) variability in the intended strength of correct ingredients that exceeds either monograph limits for official articles (see ‘official’ and ‘article’ in the General Notices and Requirements) or 10% for nonofficial articles, (4) unintended chemical and physical contaminants, and (5) incorrect types and qualities of ingredients in Compounded Sterile Preparations (CSPs).”
USP 2006 12
ISMP Sterile Preparation Compounding Safety Summit Proceedings
ISMP 2013 2
A.S.P.E.N. Statement on Parenteral Nutrition Standardization A.S.P.E.N. 2007 16ASHP guidelines on the safe use of automated-compounding
devices for the preparation of parenteral nutrition admixtures.
ASHP 2000 10
Safe Practices for Parenteral Nutrition A.S.P.E.N. 2004 13Compounded vs standardized commercial parenteral nutrition
products: A.S.P.E.N. Parenteral Nutrition Safety SummitA.S.P.E.N. 2012 17
ASHP, American Society of Health-Systems Pharmacists; A.S.P.E.N., American Society for Parenteral and Enteral Nutrition; ISMP, Institute for Safe Medication Practices.
Independent double-checks should be incorporated into the compounding process. At least three verification processes should occur in the pharmacy: (1) after initial order entry of PN, (2) before manually injecting additives into the PN, and (3) once the PN has been compounded. Each step in the verifi-cation process should require a pharmacist to compare the actual prescriber’s order to the printed labels, and the printed labels to the additives and final product, as appropriate. Verification of manual additives should include inspection of the actual vials and syringes that contain the additives. The final verification of the compounded PN should include a com-prehensive review of the PN order, the label on the product and the compounding work label, and a visual inspection of the CSP. Quality control checks and verification of replacement components on the compounder either manually or via barcod-ing should also be required, as should an independent double-check of any calculations.9
PN multichamber bags, which are designed to reduce the risk for instability or precipitation, are available. These multi-chamber bags separate components of the PN formulation with a bar or seal until just prior to activation and administration. The contents of the chambers should be mixed and any addi-tives introduced by pharmacy staff prior to dispensing the for-mulation. However, if these products are used in home care, patients and/or caregivers shall be provided with thorough training regarding the procedure for properly mixing the prod-uct before use. In addition, the containers should be accompa-nied by auxiliary labels alerting users to the need to mix the product prior to administration.
Organizations should review and revise the PN compound-ing process on an annual basis. A number of analytical methods have been applied to another high-risk complex compounding process, such as the preparation of chemotherapy. Bonan et al describe a multidisciplinary team’s application of the Hazard Analysis and Critical Control Points method to preparation of anticancer drugs.20 The team identified 11 critical points. Monitoring, control measures, and corrective actions were identified for each risk. Over a 10-month period, 16,647 che-motherapy preparations were compounded with 1157 noncon-formities for the 11 critical control points. These included 693 compounding sheet errors and 131 analytical nonconformities. Aboumatar et al reported the outcomes of application of Lean Sigma solutions to the chemotherapy preparation process.21 Once mistake-proofing interventions were introduced via workspace redesign, process redesign, and developing stan-dard operating procedures for pharmacy staff, reported medi-cation errors reaching patients causing an increase in patient monitoring decreased and the number of reported near misses increased. These improvements would be welcomed in the PN use process.
Topics for Further Research
1. The impact of the educational level and training of sterile compounding personnel on PN compounding error rates.
2. The impact of State Boards of Pharmacy inspections on PN compounding error rates.
by guest on January 9, 2014pen.sagepub.comDownloaded from
28 Journal of Parenteral and Enteral Nutrition XX(X)
3. Impact of the sequence for adding macronutrients, micronutrients, and non-nutrient medications on PN stability and compounding error rates.
4. Impact of multichamber PN admixtures (commercially available vs customized compounded) on stability, including risk of precipitation.
5. The impact of standardized, commercial PN products vs customized compounded PN admixtures on infec-tions, stability, and preparation errors.
References
1. Isanhart CM, McCall KL, Kretschmer D, Grimes BA. Parenterals labo-ratory course to reduce microbial contamination rates in media fill tests performed by pharmacy students. Am J Pharm Edu. 2008;72(2):27.
2. Rich DS, Fricker MP, Cohen MR, Levine SR. Guidelines for the safe preparation of sterile compounds: results of the ISMP sterile preparation compounding safety summit of October 2011. Hosp Pharm. 2013;48:282-294, 301.
3. Garris K, Wellein MG, Wessell A, Ragucci D, Blair MM. First-year resi-dency candidates' experience in various areas of pharmacy practice. Am J Pharm Edu. 2008;72(1):6.
4. Flynn EA, Pearson RE, Barker KN. Observational study of accuracy in compounding I.V. admixtures at five hospitals. Am J Health Syst Pharm. 1997;54:904-912.
5. Outterson K. .Regulating compounding pharmacies after NECC. N Engl J Med. 2012;367:1969-1972.
6. Flynn EA, Pearson RE, Barker K. Observational study of accuracy in compounding IV admixtures in five hospitals. Am J Health-Syst Pharm. 1997;54(8):904-912.
7. Boullata JI, Guenter P, Mirtallo JM. A parenteral nutrition use survey with gap analysis. JPEN J Parenter Enteral Nutr. 2013;37:212-222.
8. Institute for Safe Medication Practices, Medication Safety Alert, April 21, 2011. Safety Brief: Parenteral Nutrition deaths tied to drug short-age. http://www.ismp.org/newsletters/acutecare/articles/20110421.asp. Accessed June 2012.
9. Institute for Safe Medication Practices, Medication Safety Alert, September 6, 2007. Fatal 1,000-fold overdoses can occur, particularly in neonates, by transposing mcg and mg. http://www.ismp.org/Newsletters/acutecare/articles/20070906.asp. Accessed June 2012.
10. American Society of Health-System Pharmacists. ASHP guidelines on the safe use of automated compounding devices for the preparation of paren-teral nutrition admixtures. Am J Health-Syst Pharm. 2000;57:1343-1348.
11. DeBoer E, Maddox M. Advancing Medication Safety with Smart Pump Data. May 2011. http://www.pppmag.com/article_print.php?articleid=898. Accessed May 2012.
12. United States Pharmacopeia. USP chapter <797>; Pharmaceutical Compounding–Sterile Preparations. United States Pharmacopeial Convention, Inc. 2006.
13. Mirtallo J, Canada T, Johnson D, et al. Safe practices for parenteral nutri-tion [published correction appears in JPEN J Parenter Enteral Nutr. 2006;30:177]. JPEN J Parenter Enteral Nutr. 2004:28:S39-S70.
14. United States Pharmacopeial Convention. Chapter <1066> Physical Environments That Promote Safe Medication Use. The United States Pharmacopeial Convention. 2010.
15. Pedersen CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: dispensing and administra-tion—2011. Am J Health-Syst Pharm. 2012;69:768-852.
16. Kochevar M, Guenter P, Holcombe B, Malone A, Mirtallo JM. A.S.P.E.N. statement on parenteral nutrition standardization. JPEN J Parenter Enteral Nutr. 2007;31:441-448.
17. Gervasio J. Compounding vs. standardized commercial parenteral nutri-tion product: pros and cons. JPEN J Parenter Enteral Nutr. 2012;36:40S-41S.
18. Kastango ES. Compounding USP <797>: inspection, regulation, and oversight of sterile compounding pharmacies. JPEN J Parenter Enteral Nutr. 2012;36:38S-39S.
19. Sacks GS, Rough S, Kudsk KA. Frequency and severity of harm of medi-cation errors related to the parenteral nutrition process in a large university teaching hospital. Pharmacotherapy. 2009;29(8):966-974.
20. Bonan B, Martelli N, Berhoune M, et al. The application of hazard analy-sis and critical control points and risk management in the preparation of anti-cancer drugs. Int J Qual Health Care. 2009;21:44-50.
21. Aboumatar HJ, Winner l, Davis R, et al. Applying Lean Sigma solutions to mistake-proof the chemotherapy preparation process. Joint Comm J Qual Pat Safety. 2010;36:79-86.
Parenteral Nutrition Administration
Background
Because PN administration errors occur at the point of patient contact, mistakes in this phase of the medication delivery pro-cess are less likely than other types of PN errors to be inter-cepted and more likely to cause harm. In addition, the broad range of healthcare settings in which PN administration takes place—from critical care to home care—raises the potential for disparities to exist in the technology, equipment, and knowl-edge and skills of the nursing staff and caregivers responsible for PN administration. Although once uncommon, PN is administered with increasing frequency in long-term care and skilled nursing facilities. Regardless of the setting or the num-ber of patients receiving the therapy in a given facility, the clas-sification of PN as a high-alert medication requires healthcare organizations to develop evidence-based policies and proce-dures designed to promote safe PN administration and to vali-date the competence of those responsible for delivering this complex form of IV therapy.
Question: Administration 1 (A1)
(A1) What system-based measures can organizations imple-ment to enhance the safety of PN administration?
Recommendations
1. Written policies and procedures shall be developed to standardize nursing practices for the administration of PN throughout the organization.
2. Education and competency assessment shall be pro-vided to newly hired nurses and patients or caregivers who are responsible for PN administration.
3. Healthcare organizations should conduct ongoing vali-dation of competency in PN administration based on changes in practice related to PN administration, results of medication error monitoring, and/or the
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 29
vulnerability of the patient population (eg, high acuity patients, including neonates and the critically ill).
4. Healthcare organizations that provide nursing services related to home infusion shall establish mechanisms for periodic reassessment of knowledge and techniques used by patient or caregivers for home PN.
5. Interdisciplinary quality improvement programs shall incorporate analysis of medication errors associated with PN administration and knowledge of errors that occur in other institutions.
6. Safeguards shall be implemented to address specific problem areas as indicated by analysis of PN adminis-tration errors.
7. An interdisciplinary process should be employed for selecting and evaluating equipment and technological aids, such as smart pumps and barcoding to reduce errors in PN administration.
8. Healthcare organizations shall develop policies and procedures that address extravasation of PN formulations.
9. Acute care facilities should establish a policy that pro-hibits the use of a PN formulation prepared for admin-istration at home or in subacute or long-term care facilities.
10. Protocols for safe operation of infusion pumps shall stipulate rules regarding alarm silencing, modification, and disabling.
11. Healthcare organizations should purchase infusion pumps with capacity to reduce errors due to incorrect programming. Whenever possible, infusion pumps should be standardized throughout the organization.
Rationale
Data pertaining to the incidence of errors related to PN admin-istration are scarce. A recent survey revealed that 44% of orga-nizations do not track PN-related medication errors and do not know where in the process errors may be occurring.1 The lit-erature does provide some insight into the scope of the prob-lem. In particular, the frequency with which case reports of PN-related errors involve neonatal and pediatric patients sug-gests that this population may be most vulnerable to PN admin-istration errors.2
One prospective observational study of errors associated with PN found that 35% of PN-related errors occurred during the administration process.3 In a similar audit of 18,588 PN days in a tertiary pediatric hospital, administration-related errors accounted for 30% of all PN errors.4 In addition, data gathered over a 5-year period from a national medication error–reporting program revealed 266 errors associated with IVFE in neonatal intensive care units, 93.2% of which occurred in the administration phase.5,6 Another report of quality improvement data from a single 39-bed unit caring for neo-nates to young adults indicated that in one 6-month period, PN and IVFE errors accounted for 25% of all medication errors.7
Standardized Procedures and Competency Validation. Failure to follow established procedures plays a prominent role in PN administration errors.2 While human factors frequently con-tribute to PN errors, organizational efforts to strengthen the safety of PN administration must extend beyond a focus on individual performance and center on identifying system-based approaches to reduce errors.8,9 Fundamental to this process is the development and articulation of nursing policies and proce-dures for PN administration that standardize nursing practices based on published clinical guidelines.2,5,10 These policies and procedures shall be reviewed and revised on a regular basis. Table 3 provides an outline of essential components of nursing procedures for safe PN administration.
Healthcare organizations, regardless of setting (acute care to home care), shall conduct ongoing education of nurses and patients or caregivers and establish mechanisms to validate competence in PN administration. At a minimum, competency validation should occur in the following circumstances: as part of orientation for newly hired nurses, when a change in proto-col or procedure takes place, with the introduction of new equipment or technology, and when quality improvement mon-itoring or other data sources reveal a gap in skills or knowledge related to PN administration.11 Home infusion nursing care providers shall establish processes for periodic reassessment of knowledge and techniques used by patients or caregivers in the delivery of PN in the home.12 Studies of educational initiatives aimed at reducing intravenous medication errors have not con-sistently produced the desired impact on error rates.13 The opti-mal strategy (simulation, case scenarios, observation, etc) for providing continuing education aimed at reducing medication errors remains unclear, emphasizing the importance of using a variety of educational strategies and maintaining vigilance in evaluating their effectiveness.
Policies and procedures related to PN administration should address management of extravasation of PN formulations into perivascular or subcutaneous tissues.14-18 Although most often associated with peripheral vein infusions, PN extravasation can occur with all types of vascular access devices (VADs).11,17 A number of factors influence the extent of tissue damage, including pH, osmolarity, electrolyte content, and duration of tissue exposure.17 No controlled trials are available for the management of PN extravasations, but consensus-based rec-ommendations include stopping the infusion, aspiration of residual fluid, elevation of the limb, and application of cold therapy.11,17 Treatment with hyaluronidase has also been described for extravasations of PN and hypertonic dextrose.17,19 Education for nursing staff and nutrition support clinicians should include ongoing assessment of the vascular access site and appropriate interventions in the event of an extravasation.
Organizations must also develop policies pertaining to the administration of PN formulations brought in from home or from another facility. The inability to verify the stability and sterility of the formulation—as required by The Joint Commission standards—raises serious safety concerns.20 The lack of medical and pharmacy review can potentially lead to
by guest on January 9, 2014pen.sagepub.comDownloaded from
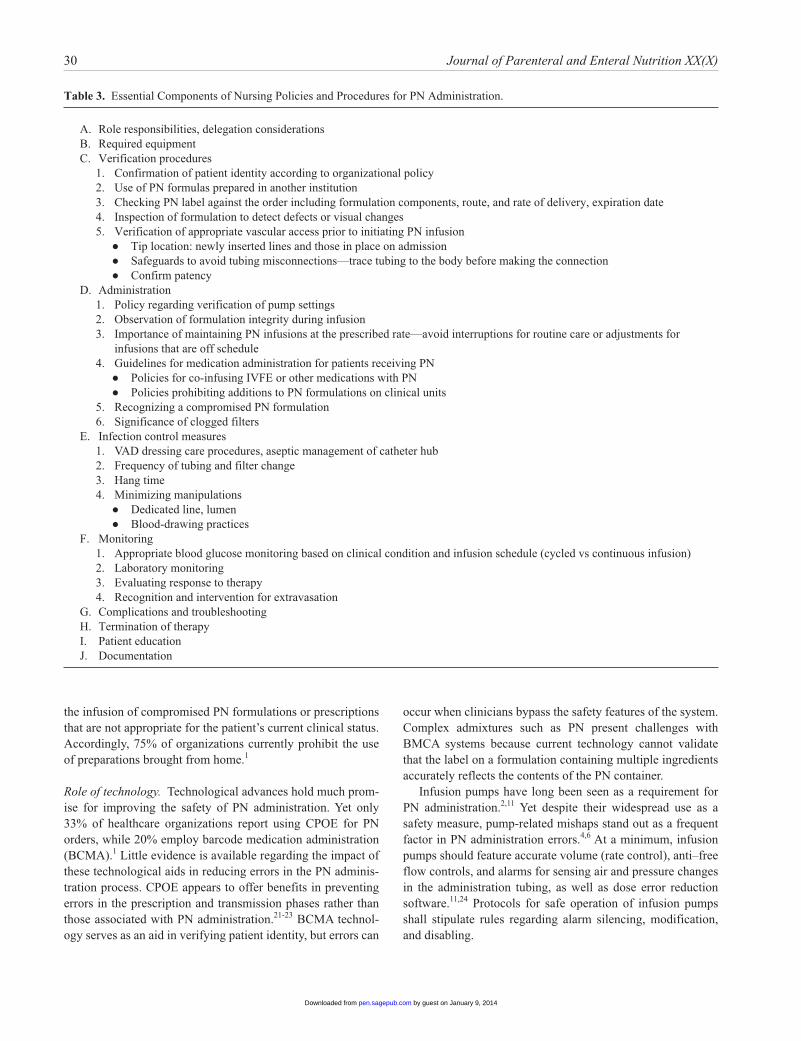
30 Journal of Parenteral and Enteral Nutrition XX(X)
the infusion of compromised PN formulations or prescriptions that are not appropriate for the patient’s current clinical status. Accordingly, 75% of organizations currently prohibit the use of preparations brought from home.1
Role of technology. Technological advances hold much prom-ise for improving the safety of PN administration. Yet only 33% of healthcare organizations report using CPOE for PN orders, while 20% employ barcode medication administration (BCMA).1 Little evidence is available regarding the impact of these technological aids in reducing errors in the PN adminis-tration process. CPOE appears to offer benefits in preventing errors in the prescription and transmission phases rather than those associated with PN administration.21-23 BCMA technol-ogy serves as an aid in verifying patient identity, but errors can
occur when clinicians bypass the safety features of the system. Complex admixtures such as PN present challenges with BMCA systems because current technology cannot validate that the label on a formulation containing multiple ingredients accurately reflects the contents of the PN container.
Infusion pumps have long been seen as a requirement for PN administration.2,11 Yet despite their widespread use as a safety measure, pump-related mishaps stand out as a frequent factor in PN administration errors.4,6 At a minimum, infusion pumps should feature accurate volume (rate control), anti–free flow controls, and alarms for sensing air and pressure changes in the administration tubing, as well as dose error reduction software.11,24 Protocols for safe operation of infusion pumps shall stipulate rules regarding alarm silencing, modification, and disabling.
Table 3. Essential Components of Nursing Policies and Procedures for PN Administration.
A. Role responsibilities, delegation considerationsB. Required equipmentC. Verification procedures
1. Confirmation of patient identity according to organizational policy2. Use of PN formulas prepared in another institution3. Checking PN label against the order including formulation components, route, and rate of delivery, expiration date4. Inspection of formulation to detect defects or visual changes5. Verification of appropriate vascular access prior to initiating PN infusion
● Tip location: newly inserted lines and those in place on admission● Safeguards to avoid tubing misconnections—trace tubing to the body before making the connection● Confirm patency
D. Administration1. Policy regarding verification of pump settings2. Observation of formulation integrity during infusion3. Importance of maintaining PN infusions at the prescribed rate—avoid interruptions for routine care or adjustments for
infusions that are off schedule4. Guidelines for medication administration for patients receiving PN
● Policies for co-infusing IVFE or other medications with PN● Policies prohibiting additions to PN formulations on clinical units
5. Recognizing a compromised PN formulation6. Significance of clogged filters
E. Infection control measures1. VAD dressing care procedures, aseptic management of catheter hub2. Frequency of tubing and filter change3. Hang time4. Minimizing manipulations
● Dedicated line, lumen● Blood-drawing practices
F. Monitoring1. Appropriate blood glucose monitoring based on clinical condition and infusion schedule (cycled vs continuous infusion)2. Laboratory monitoring3. Evaluating response to therapy4. Recognition and intervention for extravasation
G. Complications and troubleshootingH. Termination of therapyI. Patient educationJ. Documentation
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 31
In recent years, infusion pumps equipped with software designed to detect potential errors (“smart pumps”) have become available, although conflicting information exists regarding the use of these devices. A recent gap analysis that specifically addressed current PN practices found that smart pumps are available in 29% of responding facilities.1 On the other hand, a survey of hospital-based pharmacies reported a usage rate of 77% for these devices.22 Smart pumps provide a safeguard against programming errors and capture data that can support quality improvement programs.25 When used properly, smart pumps reduce the potential for error, but this pump technology is not foolproof. If a smart pump drug library is bypassed or is used incorrectly or the infusion rate and vol-ume are manually entered, a dose error can occur. One case study, for example, reported an incident in which a PN infusion was administered at 10 times the prescribed rate for 2 hours when a soft limit alert was bypassed.26 The advantages of smart pumps can be offset by the complexity of programming the pumps and maintaining a current drug library. To have a mean-ingful impact on patient safety, smart pumps must be integrated with BCMA and CPOE systems as well as hospital and phar-macy information systems.21 A comprehensive organizational commitment to the technology of smart pumps is essential to the successful deployment in clinical areas.25,27 Organizations should purchase infusion pumps with capacity to reduce errors due to incorrect programming. Whenever possible, infusion pumps should be standardized throughout the organization to promote user familiarity with the operation of the device.28
Quality improvement. A critical step in efforts to improve the safety of PN is the implementation of quality improvement programs designed to track and analyze errors associated with PN administration.8 However, only 39.9% of organizations report having an ongoing quality improvement process for PN.1 Proactive and reactive methodologies, failure mode effects analysis, root cause analysis, and the Plan-Do-Study-Act (PDSA) model should all serve as the framework for iden-tifying high occurrence or high impact errors, closing practice gaps, and engendering continuous process improvement.29,30 Multifaceted interdisciplinary approaches must foster a culture of safety, clarify problem areas, involve key stakeholders, test change strategies, and maintain channels of communication. These key concepts are most effective in bringing about and sustaining behavior change.29
As noted earlier, smart pumps can serve as a valuable source of quality improvement data that allows organizations to track practices related to PN administration and identify interven-tions that address safety breaches.25 However, without a reli-able wireless network, data retrieval can be labor intensive.25,27,31,32
Question: Administration 2 (A2)
(A2) What strategies can prevent errors in the verification phase of PN administration?
Recommendations
1. The verification process of PN administration should be presented in a bundle format, which uses a set of evidence-based interventions for a defined patient pop-ulation or care setting.
2. Nurses, caregivers, and patients shall visually inspect the integrity of the PN container and formulation before spiking the container.
3. The PN label shall be verified against the original pre-scriber order. No verbal orders shall be accepted.a. Check the patient identifiers, product name,
route of administration (central vs peripheral), designated initiation time, infusion rate, and beyond-use date and time.
b. Match all components listed on the label of the formulation to the PN order.
4. A printed copy of the PN prescription shall be provided to home PN consumers initially and with each formu-lation change to allow this verification step.
5. Patient identity shall be confirmed using two identifi-ers according to organizational policy.
6. The administration tubing shall be traced to the point of origin in the body at the initiation of the infusion and at all handoffs.
7. An independent double-check process and verification of infusion pump settings should be performed by a second clinician before beginning the PN infusion and documented in the medical record.
Rationale
PN administration errors often stem from failure to adhere to the verification steps of PN administration, which parallel the “five rights” of medication safety that all nurses learn: right patient, right drug, right dose, right route, and right time.9,11 Policies and procedures for PN administration should avoid broad directives to “check the label” but instead provide clear procedural guid-ance for each step in the verification process. This verification process should be presented in a bundle format, which uses a set of evidence-based interventions for a defined patient population or care setting. As with other bundles used in healthcare, all components of the verification process must be implemented together to achieve improvements in care.33
Adherence to the “five rights” is not sufficient in preventing medication errors. Although human factors frequently contrib-ute to errors, healthcare organizations have a responsibility to create an infrastructure that supports safe practice and reduces the potential for error.8,9 This includes educating staff about the proper use and effectiveness of double-checks and creating procedures for reporting errors, near misses, and barriers to safe practice in a nonpunitive environment.8,9
Verification procedures. PN formulations often resemble other products used in clinical care, such as bladder irrigation fluids,
by guest on January 9, 2014pen.sagepub.comDownloaded from

32 Journal of Parenteral and Enteral Nutrition XX(X)
enteral formula, human breast milk, and cardioplegia solu-tions, posing the risk for wrong-product or wrong-route errors. Practices related to the delivery and storage of these items can mitigate the likelihood of such errors, but the importance of the verification process as the final step before the point of patient contact cannot be overstated.
Nursing education for PN administration shall include infor-mation regarding management of potentially compromised or unstable PN formulations. This includes inspection of PN for-mulations prior to initiating the infusion and at regular intervals during the infusion. Any formulation that displays evidence of precipitants, particulate matter, or an unstable formulation shall be returned to the pharmacy for further investigation.34
Other examples of lapses in the verification process include PN administration to the wrong patient by the wrong route—infusing a central formulation via peripheral vein or through an incorrect tubing connection—or at the wrong rate.2 The nurse or caregiver should be provided access to the complete original PN order to facilitate verification of all elements of the order (ie, patient identifiers, nutrient dosing, infusion rate, etc).1
Mistakes involving incorrect infusion rates are among the most common errors reported. Often, these errors are related to mistakes in programming a single infusion pump, but the risk for rate errors appears to increase when IVFE and dextrose/amino acid components are administered as separate infu-sions.2,3,6 Errors involving incorrect infusion rates pose the greatest risk for patient harm due to the potential for causing life-threatening metabolic disturbances such as hyperglycemia or fat overload syndrome.
Tubing misconnections. Inadvertent catheter tubing miscon-nections have been recognized as a serious problem in health-care. Although the administration of enteral feeding through intravenous devices has been associated with the most serious injuries, accidental connections between intravenous tubing and other systems that rely on Luer connectors have been reported, including epidural, intracranial, intrathecal, and tra-cheal tubing systems.35,36 Because tubing used to administer PN must be changed every 24 hours, the potential for a miscon-nection occurs at more frequent intervals than with conven-tional intravenous fluids. Clear labeling on PN containers, tubing, and pump channels can reduce the risk of inadvertent misconnections.32,37 However, the single most important risk reduction strategy is to trace all tubing back to its origin before connecting devices or infusions and to recheck connections and trace all patient tubes and catheters to their sources at the start of each shift and upon the patient’s arrival to a new setting or unit as part of the hand-off process.38,39
Independent double-checks. Reports of PN-related errors often recommend implementation of independent double-checks at critical phases of PN administration, such as order verification or programming the infusion rate into the
pump.2,3,6,7,32 To be effective, an independent double-check must involve two clinicians separately checking the infusion settings in accordance with the prescriber’s order, alone and apart from each other, then comparing results.40 Although dou-ble-checks serve as a valuable safety mechanism if performed correctly, the process may require up to 20 minutes of addi-tional nursing time.40 Other barriers include a lack of clarity regarding the procedure for double-checking and a culture that does not fully support peer review.41 Furthermore, excessive use of double-checks can dilute the effectiveness of this safety mechanism.40,42 Independent double-checks should not be implemented to address problems that could be corrected through system redesign.40 Nevertheless, organizations that have identified errors in conjunction with a specific component of the PN verification process, such as order verification, patient identification, or pump programming, should imple-ment double-checks strategically to avert potentially harmful errors. For optimal effectiveness, independent double-checks should be used in conjunction with other error reduction strate-gies and system changes aimed at reducing the risk of medica-tion errors.40 The use of computer-generated checklists with PN infusion instructions has been suggested as a way to guide verification procedures without increasing workload demands, but this approach requires further study.5,43
Question: Administration 3 (A3)
What practices maintain patient safety during the infusion of PN?
Recommendations
1. PN shall be administered by or under the supervision of trained, competent personnel.
2. Organizations shall establish evidence-based policies to guide the selection, insertion, care, and maintenance of VADs used to administer PN.
3. PN protocols shall include measures to reduce contam-ination through manipulation of the catheter hub.
4. VADs used for PN administration should not be used to obtain blood samples for laboratory tests unless no peripheral access is available.
5. PN infusions shall be infused through a filter appropri-ate for the type of formulation.
6. An occluded filter shall never be removed in response to occlusion alarms, thus allowing the unfiltered for-mulation to continue to infuse.
7. Administration tubing should be attached to PN con-tainers immediately prior to use.
8. Administration tubing and filters shall be changed with each new PN container (every 24 hours for TNAs and dextrose/amino acid formulations; 12 hours for IVFE infused separately).
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 33
9. For prolonged infusions of IVFE (20–24 hours), the daily dose should be divided into 2 parts, with a new container and tubing every 12 hours.
10. Policies regarding PN multichamber bags should be developed using a multidisciplinary approach.
11. The PN infusion shall be maintained at the prescribed rate:a. Correct pump settings shall be verified at regu-
lar intervals and at each hand-off.b. The PN infusion rate shall not be adjusted if the
infusion is off schedule.c. The rate of PN shall not be increased in response
to changes in fluid needs; additional hydration should be provided as a separate infusion.
d. The PN should not be interrupted for routine care or patient transport for diagnostic studies.
e. Organizations shall develop policies regarding PN infusion and appropriate metabolic moni-toring during surgery.
12. The timing and frequency for blood glucose monitor-ing shall be based on clinical status and performed in a manner appropriate for the PN infusion schedule (cycled vs continuous).
13. Caution shall be used when administering subcutane-ous insulin coverage prior to a scheduled interruption of the PN infusion.
14. In acute care acute settings (including long-term acute care), no additions should be made to PN formulations outside the compounding pharmacy; in home settings, additions to PN formulations should be limited in num-ber and be made as close as possible to initiating the infusion.
15. In long-term care facilities and in home care, education should be provided and caregiver competency regard-ing proper technique for the addition of prescribed additives to PN formulations should be verified.
16. Co-infusion of medications through PN lines shall require a review of compatibility and stability data by a pharmacist.
17. PN should be discontinued prior to transfer to another facility.
18. The administration of PN and the patient’s tolerance shall be documented in the medical record.
Rationale
Nursing care during PN infusion centers on administering the infusion as prescribed, preventing complications, monitoring metabolic stability, assessing progress toward therapeutic goals, and documenting patient response to therapy. This pro-cess includes safe and effective management of all medical devices and equipment used in the delivery of PN, safe admin-istration of medications in conjunction with PN therapy, and optimal care of vascular access devices.
Medical devices and equipment. Vascular access: Reliable vascular access is essential for safe and effective delivery of PN. A wide array of VADs are available, but some are better suited to PN delivery than others. Factors that influence the selection of a VAD for PN include the patient’s medical condi-tion, need for concomitant intravenous medication(s), the anticipated duration of PN therapy, and the setting in which PN is administered.11 In all care settings, the patient’s views should also play a role in the decision-making process for VAD selection.
Despite their essential role in PN administration, VADs are a leading cause of serious adverse complications related to PN therapy, in particular, central line–associated bloodstream infection (CLABSI). PN is an independent risk factor for CLABSI, requiring organizations to be especially vigilant in establishing policies to guide the selection, insertion, and care of these devices.44 In recent years, widespread implementation of a bundle of evidence-based guidelines for insertion and maintenance of VADs has achieved substantial reductions in the CLABSI rates.45 In addition to addressing VAD insertion and site care, PN protocols shall also include measures aimed at reducing contamination that occurs through manipulation of the catheter hub. Some organizations maintain policies requir-ing a dedicated line or lumen for PN administration, although studies have not yielded consistent results regarding the effi-cacy of this practice.46
Many organizational protocols for care of VADs discourage blood sampling from central lines as part of an overall effort to reduce manipulation and subsequent contamination of the catheter hub. For similar reasons, The Joint Commission has highlighted the use of VADs for blood sampling as a “practice to avoid.”47 One recent study of home PN recipients found an increased risk for CLABSI in patients who routinely had blood drawn from a VAD, leading these authors to conclude that PN catheters should not be used for obtaining blood samples unless no peripheral access is available.46 The elevated risk for CLABSI that is associated with PN administration warrants a multifaceted approach to CLABSI prevention that targets all pathways for VAD infection.
The use of VADs for blood withdrawal not only increases the risk for microbial contamination of the line and hub, but samples drawn incorrectly from a VAD during PN infusion can also lead to spurious laboratory values. Binkley et al first drew attention to the danger of this phenomenon in a report of a 10-month quality assurance study.48 More recently, a year-long prospective cohort study in an academic medical center found 63 incidents of spurious blood work in 34 PN recipients.49 In both cases, investigators recount incidents of patient harm—typically hypoglycemia or hypokalemia—that resulted from unnecessary medical intervention for falsely elevated labora-tory values.
Filters: In-line filters are required for PN administration to reduce the potential for patient harm due to particulates, micro-precipitates, microorganisms, and air emboli.50 These devices
by guest on January 9, 2014pen.sagepub.comDownloaded from

34 Journal of Parenteral and Enteral Nutrition XX(X)
should be placed as close to the patient as possible on the administration system. A 0.22-micron filter is recommended for a dextrose/amino acids formulation; a 1.2-micron filter is used for a TNA formulation. Because nurses must deal with the problem of pump alarms at the point of care, nursing compe-tencies for PN administration shall include appropriate actions and troubleshooting in response to high-pressure alarms or an occluded filter. This education shall emphasize that a filter that becomes occluded during PN administration should raise sus-picions that the incorrect filter size has been used or that a pre-cipitate or particulate is present in the formulation. When an occluded filter triggers pump alarms, the PN infusion shall be stopped. Before resuming PN, a pharmacist should review the PN formulation to determine if incompatibility issues are the cause of the problem and to identify actions to prevent further occurrences.
Filters are manufactured for single patient use and should be changed according to the manufacturer’s guidelines. The typical maximum use interval for PN filters is 24 hours. Due to the potential for contamination and subsequent release of endotoxin, filters should not be primed with PN fluid in advance—in the compounding pharmacy, for example. Instead, the filter should be filled with fluid immediately before initiat-ing the infusion.
Administration tubing and containers: PN formulations should be provided in a single daily bag, with the exception of IVFE that is administered as a separate infusion. The PN admixture should be kept refrigerated and protected from light exposure between the times it is dispensed until just before infusion. Exposure of PN formulations to ambient light gener-ates peroxides and other degradation products, potentially con-tributing to oxidant stress. Concern regarding the clinical impact of this phenomenon has led to recommendations that PN be shielded from light, especially for neonates.51 However, studies have failed to demonstrate clear clinical benefits of shielding PN formulations from light. Partial light protection offers no clinical benefit. To reduce PN degradation, the con-tainer and tubing must be protected from light at all points from compounding through administration.52 Further research is required to determine if complete photoprotection of PN for-mulations can lead to improved clinical outcomes.
The administration tubing should be attached to the PN container, using sterile technique, immediately prior to initiat-ing the infusion. Although there may be workflow advantages to spiking the container and priming tubing in advance, no studies have examined the safety of this practice. Infection control guidelines for non-nutrition intravenous fluids stipulate that the infusion begin within 1 hour of inserting the tubing spike into the container.53 The issue of whether the risk of con-tamination could be reduced by spiking the PN container in an ISO Class 5 environment or higher remains unknown.
IVFE administered separately shall be appropriately labeled and administered in keeping with the organization’s policies and procedures for minimum/maximum hang times. PN con-tainers and administration sets shall be free of the plasticizer
di-2-ethylhexyl phthalate (DEHP) to prevent DEHP contami-nation of TNA formulations and IVFE that are infused sepa-rately.2,11 Guidelines for the frequency of tubing changes for PN formulations often make a distinction between admixtures that contain IVFE (every 24 hours) and those that contain only dextrose and amino acids (no more frequently than 96 hours).11,44 However, these recommendations overlook the potential for contamination of the filter on all types of PN for-mulations. Therefore, administration sets and filters should be changed with each new PN container. For continuous infu-sions, this interval will typically be every 24 hours; cycled PN will require tubing and filter changes based on the hours of the infusion. Administration sets used for IVFE infused separately shall also be changed with each new infusion (hang time 12 hours). In cases in which a prolonged IVFE infusion is desir-able to promote tolerance, the daily fat emulsion dose should be divided into 2 parts, with a new container and tubing used every 12 hours.54,55
Multichamber PN bags are available, which are designed to reduce the risk for instability or precipitation. These multi-chamber bags separate components of the PN formulation with a bar or seal until just prior to administration. The contents of the chambers should be mixed and additives introduced by pharmacy staff prior to dispensing the formulation.56 However, if these products are used in home care, patients and/or care-givers shall be provided with thorough training regarding the procedure for properly mixing the product before use. In addi-tion, the containers should be accompanied by auxiliary labels alerting users to the need to mix the product prior to administration.57
Infusion practices. PN infusions should be administered according to the prescribed rate via an infusion pump. Nurses shall verify the correct rate when the PN infusion is initiated, at regular intervals during the infusion, and at hand-offs.58 Sched-uled changes in the prescribed administration rate should be based on patient tolerance and metabolic stability. In acute care settings, PN is commonly infused continuously over 24 hours. However, a schedule in which the PN is cycled to infuse over 10 to 14 hours (based on patient tolerance) can offer physio-logic and psychological benefits to patients in selected circum-stances.59,60 The conversion from a continuous to a cycled administration period typically takes place by reducing the infusion time by 4 to 6 hours each day until the infusion time has been compressed to the target duration. However, one recent study suggests that cycling PN to 12 hours can be accomplished in one step.61 A report documenting a high inci-dence of adverse events associated with PN cycling under-scores the importance of close patient monitoring during the transition to cycled PN.60 At each stage, the healthcare team must assess tolerance of the cyclic infusion before advancing to the next step.
Hyperglycemia, edema, or symptoms of fluid intolerance signal the need for a more cautious approach to cyclic infusion. Adult patients tolerate abrupt discontinuation of PN without
by guest on January 9, 2014pen.sagepub.comDownloaded from

Ayers et al 35
experiencing rebound hypoglycemia.62 However, a 30- to 60-minute taper-down period is customarily used with ambula-tory PN infusion pumps that perform this function automati-cally.63 On the other hand, pediatric patients younger than 2 or 3 years old are prone to developing hypoglycemia with abrupt discontinuation of PN and therefore require more gradual taper-down procedures in conjunction with cycling.59,60 During the transition to a cycled PN regimen, on-cycle and off-cycle glucose monitoring should take place daily. Once patient toler-ance to cycled PN is established, less frequent glucose moni-toring may be acceptable, especially in stable home PN patients.64
When transitioning to cyclic PN, dosing regimens for insu-lin should be tailored to avoid abnormal fluctuations in blood glucose levels. In patients for whom PN is the sole source of nutrition, giving subcutaneous correctional dose insulin in the final phase of the cycle could lead to hypoglycemia when the PN infusion is discontinued. On the other hand, when PN for-mulations contain large doses of insulin, patients may require intermediate or long-acting insulin to prevent hyperglycemia after the PN stops.
Unscheduled interruptions in the infusion should be avoided because they may contribute to metabolic disturbances and suboptimal nutrient delivery. PN administration should not be interrupted for medication administration.4 PN should be dis-continued prior to discharge or transport to another facility. As noted earlier, a taper-down period is a gradual reduction in the PN rate. Adult patients do not require a taper; however, a taper period for pediatric patients receiving PN prevents rebound hypoglycemia.
The risks of metabolic complications, particularly those related to glycemic control, have raised questions regarding the safety of continuing PN during operative procedures. However, no studies have adequately examined this issue. One survey of pediatric anesthesiologists revealed a high degree of variability in the clinical management of blood glucose levels in patients receiving PN during anesthesia.65 As with other areas of PN administration, healthcare organizations should develop clear and consistent policies that address intraopera-tive PN infusion. When the PN infusion is continued during surgery, the prescribed infusion rate should be maintained, with close monitoring of blood glucose levels and insulin administration as needed to maintain glycemic control. The use of PN infusions for fluid resuscitation shall be avoided.
Medication administration. Historically, PN formulations were viewed as convenient vehicles for delivery of medications such as heparin, insulin, and histamine (H
2) receptor antagonists.
However, a better understanding of factors that impact the stabil-ity of PN formulations and the potential for drug-nutrient inter-actions warrants a more conservative approach to medication administration with PN formulations. The mixture of medica-tions in PN preparations is being addressed more specifically in A.S.P.E.N.’s forthcoming parenteral nutrition clinical guide-lines, which are to be published in the near future.
Incompatibility reactions range from discoloration, degradation of nutrients or medication, and formation of precipitates, to loss of emulsion integrity in TNA formulations. The greatest risk for incompatibility exists with medications that are added directly to the PN formulation due to the prolonged time of contact between the medication and PN components with direct admixtures.66 Standardized commercial PN products that require further addi-tives prior to patient administration should be prepared in the pharmacy under aseptic conditions. Therefore, in acute care set-tings, policies shall be implemented that prohibit the addition of medication outside the compounding pharmacy. However, in home care settings, stability considerations often require that medication, such as multivitamin preparations or insulin, be added to PN formulations prior to initiating the infusion. In this case, the addition of medication should take place as close to the beginning of the infusion as possible. Patient and caregiver training in the proper technique for adding medication to PN formulations shall be documented. The additions should be made as close to the beginning of the infusion as possible to reduce the potential for harm should touch contamination occur during this process.
As noted earlier, the optimal way to administer PN is through an IV line (one lumen of a multilumen VAD) reserved solely for that purpose. However, maintaining a dedicated line for PN administration may be impractical or impossible in patients who receive multiple IV medications or have limited vascular access.2 Pharmacists must conduct a comprehensive review of stability and compatibility data from the literature and manufacturer of intravenous nutrients before a medication is administered in a PN formulation.
As with all high-alert medications, PN should be adminis-tered as a primary infusion.37 Co-infusion of medication through the same tubing used for PN should also be avoided if possible. Compatibility information should be derived for PN that closely matches the formulation in question. Medication administration policies should explicitly detail safe practices with regard to medication administration in conjunction with PN.
Documentation. Organizational policies and procedures shall define documentation practices related to PN administration in accordance with legal and regulatory requirements. This should include, but is not limited to, initiation and discontinu-ing times of the infusion, rate, route of administration, results of capillary glucose monitoring and laboratory tests, condition of the VAD, patient’s response to therapy, progress toward therapeutic goals, and patient education provided.
Topics for Further Research
1. Identification of the optimal use of independent clini-cian double-checks in critical aspects of the PN admin-istration process.
2. Identification of educational strategies that are most effective in developing and validating competence in PN administration procedures.
by guest on January 9, 2014pen.sagepub.comDownloaded from
36 Journal of Parenteral and Enteral Nutrition XX(X)
3. Demonstration of PN error reduction with routine assessment of competence in PN administration procedures.
4. Identification of environmental and human factors that contribute to PN administration errors.
5. Identification of strategies to mitigate the risk of PN administration errors.
6. Evaluation of the optimal approach for managing PN during surgery.
7. Impact on infection rates and accuracy of laboratory tests with the use of vascular access devices to obtain blood samples for laboratory tests.
8. Clarification of the appropriate use of filters with IVFE administration.
9. Evaluation of using checklists for PN administration in reducing PN-related errors.
References
1. Boullata J, Guenter P, Mirtallo J. A parenteral nutrition survey with gap-analysis. JPEN J Parenter Enteral Nutr. 2013;37(2):212-222.
2. Mirtallo J, Canada T, Johnson D, et al; Task Force for the Revision of Safe Practices for Parenteral Nutrition. Safe practices for parenteral nutrition. JPEN J Parenter Enteral Nutr. 2004;28:S39-S70.
3. Sacks GS, Rough S, Kudsk KA. Frequency and severity of harm of medi-cation errors related to the parenteral nutrition process in a large university teaching hospital. Pharmacotherapy. 2009;29(8):966-974.
4. Narula P, Hartigan D, Puntis JWL. The frequency and significance of errors related to parenteral nutrition in children. Proc Nutr Soc. 2010;69(OCE7):E556.
5. Chuo J, Lambert G, Hicks RW. Intralipid medication errors in the neonatal intensive care unit. J Qual Patient Saf. 2007;33:104-111.
6. Hicks RW, Becker SC, Chuo J. A summary of NICU fat emulsion medi-cation errors and nursing services: data from MEDMARX. Adv Neonatal Care. 2007;7:299-310.
7. Colevas AH, Rempe B. Nurse sensitive indicators: integral to the Magnet™ journey. Am Nurse Today. 2011;6:39-41.
8. Sacks GS. Safety surrounding parenteral nutrition systems. JPEN J Parenter Enteral Nutr. 2012;36:20S-22S.
9. Institute for Safe Medication Practices. The five rights cannot stand alone. ISMP Medication Safety Alert! Nurse Adviser-Err. 2004;2(11).
10. Boitano M, Bojak S, McCloskey S, McCaul DS, McDonough M. Improving the safety and effectiveness of parenteral nutrition: results of a quality improvement collaboration. Nutr Clin Pract. 2010;25(6):663-671.
11. Infusion Nursing Society. Infusion nurses standards of practice. J Infusion Nurs. 2011;34:S1-S110.
12. Winkler M, Hagen E, Albina J. Home nutrition support. In: Muller CM, ed. The A.S.P.E.N. Adult Nutrition Support Core Curriculum. 2nd ed. Silver Spring, MD: American Society for Parenteral and Enteral Nutrition; 2012:639-655.
13. Hughes RG, Blegen MA. Medication administration safety. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. AHRQ Publication No. 08-0043. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
14. Gil ME, Mateu J. Treatment of extravasation from parenteral nutrition solution. Ann Pharmacother. 1998;32:51-55.
15. Kumar RJ, Pegg SP, Kimble RM. Management of extravasation injuries. ANZ J Surg. 2001;71:285-289.
16. Wilkens CE, Emmerson AJB. Extravasation injuries on regional neonatal units. Arch Dis Child Fetal Neonatal Ed. 2004;89:F274-F275.
17. Doellman D, Hadaway L, Bowe-Geddes LA, et al. Infiltration and extrav-asation. J Infusion Nurs. 2009;32:203-211.
18. Benedetta B, Andres C. Extravasation of peripherally administered paren-teral nutrition. N Engl J Med. 2011;364:e20.
19. Weigand R, Brown J. Hyaluronidase for the management of dextrose extravasation. Am J Emerg Med. 2010;28(2):257.e1-2.
20. Joint Commission. Standard MM.03.01.05. In: Comprehensive Medication Manual for Hospital: The Official Handbook, Update 2 (CAMH). Oakbrook Terrace, IL: Joint Commission Resources; September 2011.
21. Husch M, Sullivan C, Rooney D, et al. Insights from the sharp end of intravenous medication errors: implications for infusion pump technol-ogy. Qual Saf Health Care. 2005;14:80-86.
22. Pederson CA, Schneider PJ, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: monitoring and patient educa-tion—2012. Am J Health-Syst Pharm. 2013;70:787-797.
23. Hilmas E, Peoples JD. Parenteral nutrition prescribing process using com-puterized prescriber order entry: opportunities to improve safety. JPEN J Parenter Enteral Nutr. 2012;36:32S-35S.
24. ECRI Institute. General purpose infusion pumps. Health Devices. 2007. https://www.ecri.org/Documents/Infusion_Pumps_Evaluation.pdf. Accessed June 20, 2012.
25. Institute for Safe Medication Practices. Proceedings from the ISMP Summit on the Use of Smart Infusion Pumps: Guidelines for Safe Implementation and Use. 2009. ismp.org/Tools/guidelines/smartpumps/default.asp. Accessed June 1, 2012.
26. Cummings K, McGowan R. “Smart” infusion pumps are selectively intel-ligent. Nursing. 2011;41:58-59.
27. AAMI Foundation/HTSI. Safety innovations: best practice recom-mendations for infusion pump–information network integration. 2012. http://www.aami.org/htsi/SI_Series/Infusion_Pump_White_Paper.pdf. Accessed September 4, 2012.
28. ECRI Institute. Deep dive identifies treasures to prevent medication errors. PSO Monthly Brief. May 2012. https://www.ecri.org/Email Resources/PSO_Monthly_Brief/PSO_Brief_May12.pdf. Accessed June 24, 2012.
29. Hughes RG. Tools and strategies for quality improvement and patient safety. In: Hughes RG, ed. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. AHRQ Publication No. 08-0043. Rockville, MD: Agency for Healthcare Research and Quality; March 2008.
30. Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. 2nd ed. San Francisco, CA: Jossey-Bass; 2009.
31. Trbovich P, Easty A. Safety innovations: smart pump implementa-tion: a guide for healthcare institutions. 2012. AAMI Foundation HTSI. http://www.aami.org/htsi/SI_Series/Smart_Pump_Implementation.pdf. Accessed September 5, 2012.
32. Food and Drug Administration. Infusion pump risk reduction strate-gies for clinicians. April 2010. http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/GeneralHospitalDevicesandSupplies/InfusionPumps/ucm205406.htm. Accessed June 22, 2012.
33. Resar R, Griffin FA, Haraden C, Nolan TW. Using Care Bundles to Improve Health Care Quality. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement; 2012.
34. Rollins CJ. Total nutrient admixtures: stability issues and their impact on nursing practice. J Intravenous Nurs. 1997;20(6):299-303.
35. The Joint Commission on Accreditation of Healthcare Organizations. Tubing misconnections—a persistent and deadly occurrence. Sentinel Event Alert. 2006;36:1-3.
36. Pennsylvania Patient Safety Advisory. Tubing misconnections: making the connection to patient safety. Pa Patient Saf Advis. 2010;7:41-45.
37. AAMI Foundation/HTSI. Safety innovations: nine recommendations to prevent multiple line infusion medication errors. http://www.aami.org/htsi/SI_Series/Nine_Recommendations_Multiple_Line_Infusion.pdf. Accessed September 4, 2012.
38. Guenter P, Hicks RW, Simmons D, et al. Enteral feeding misconnec-tions: a consortium position statement. Jt Comm J Qual Patient Saf. 2008;34:285-292.
by guest on January 9, 2014pen.sagepub.comDownloaded from
Ayers et al 37
39. Simmons D, Symes L, Guenter P, Graves K. Tubing misconnections: nor-malization of deviance. Nutr Clin Pract. 2011;26:286-293.
40. ISMP. Independent double checks: undervalued and misused: selective use of this strategy can play an important role in medication safety. ISMP Medication Safety Alert! June 13, 2013. http://www.ismp.org/newsletters/acutecare/issue.asp?dt=20130613. Accessed June 26, 2013.
41. Dickinson A, McCall E, Twomey B, James N. Paediatric nurses’ under-standing of the process and procedure of double-checking medications. JCN J Clin Nurs. 2010;19:728-735.
42. Grissinger M. The virtue of independent double-checks: they really are worth your time. P & T. 2006;31:492.
43. AHRQ Health Care Innovations Exchange. Standardized ordering and administration of total parenteral nutrition reduces errors in children’s hospital. www.innovations.ahrq.gov/content.aspx?id=2323. Updated May 2011. Accessed June 2, 2012.
44. O’Grady NP, Alexander M, Burns LA, et al. Guidelines for the preven-tion of intravascular catheter-related infection, 2011. Centers for Disease Control and Prevention website. http://www.cdc.gov/hipac/pdf/guide-lines/bse-guidelines-2011.pdf. Accessed June 24, 2012.
45. Institute for Healthcare Improvement. Implement the central line bundle. http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Changes/ImplementCentralLineBundle.htm. Accessed June 24, 2012.
46. Buchman AL, Opilla M, Kwasny M, Diamantidis TG, Okamoto R. Risk factors for the development of catheter-related bloodstream infection in patients receiving home parenteral nutrition [published online June 6, 2013]. JPEN J Parenter Enteral Nutr.
47. The Joint Commission. Preventing Central Line–Associated Bloodstream Infections: A Global Challenge, a Global Perspective. Oak Brook, IL: Joint Commission Resources; May 2012. http://www.PreventingCLABSIs.pdf. Accessed June 12, 2012.
48. Binkley JE, Mills B, Roy MA, Diaz JJ, Jensen GL. Spurious laboratory values from improper sampling of blood containing parenteral nutrition. Nutr Clin Pract. 2004;19:540-541.
49. Fairholm L, Saqui O, Baun M, Yeung M, Fernandes G, Allard JP. Monitoring parenteral nutrition in hospitalized patients: issues related to spurious bloodwork. Nutr Clin Pract. 2011;26:700-707.
50. Food and Drug Administration. Safety alert: hazards of precipitation with parenteral nutrition. Am J Hosp Pharm. 1994;51:1427-1428.
51. Hoff DS, Michaelson AS. Effects of light exposure on total parenteral nutrition and its implications in the neonatal population. J Pediatr Pharmacol Ther. 2009;14(3):132-143.
52. Sherlock R, Chessex P. Shielding parenteral nutrition from light: does the available evidence support a randomized controlled trial? Pediatrics. 2009;123(6):1529-1533.
53. Dolan SA, Felizardo G, Barnes S, et al. APIC position paper: safe injec-tion, infusion and medication vial practices in healthcare. Am J Infect Control. 2010;38:167-172.
54. Committee on Nutrition, American Academy of Pediatrics; Kleinman RE, ed. Pediatric Nutrition Handbook. 6th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2004.
55. Koletzko E, Goulet O, Hunt J, Krihn K, Shamir R. Guidelines on pae-diatric parenteral nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), sup-ported by the European Society of Pediatric Research (ESPR). J Pediatr Gastroenterol Nutr. 2005;31:S1-S87.
56. Institute for Safe Medication Practices. Pharmacist supervision is critical for proper preparation of Clinimix multichamber bags. ISMP Medication Safety Alert! Nurse Adviser-Err. 2011;9(4).
57. Cohen MR. Safe practices for compounding of parenteral nutrition. JPEN J Parenter Enteral Nutr. 2012;36:14S-19S.
58. Institute for Safe Medication Practices. Lack of standard dosing methods contribute to IV errors. ISMP Medication Safety Alert! Nurse Adviser-Err. 2007;12(17):1-3.
59. Stout SM, Cober MP. Metabolic effects of cyclic parenteral nutrition infu-sion in adults and children. Nutr Clin Pract. 2010;25:277-281.
60. Suryadevara S, Celestin J, DeChicco R, et al. Type and prevalence of adverse events during the parenteral nutrition cycling process in patients being prepared for discharge. Nutr Clin Pract. 2012;27:268-273.
61. Austhof SI, DeChicco R, Corrigan ML, et al. Cycling parenteral nutrition from 24 hours to 12 hours in 1 step is safe in patients requiring long-term therapy [published online January 2013]. JPEN J Parenter Enteral Nutr. Abstract Data Supplement.
62. Krzywda EA, Andris DA, Whipple JR, et al. Glucose response to abrupt discontinuation of total parenteral nutrition. JPEN J Parenter Enteral Nutr. 1993;17:64-67.
63. Newton AF, DeLegge MH. Home initiation of parenteral nutrition. Nutr Clin Pract. 2007;22:57-64.
64. Norman JL, Crill CM. Optimizing the transition to home parenteral nutri-tion in pediatric patients. Nutr Clin Pract. 2011;26:273-285.
65. Ayers J, Graves SA. Perioperative management of total parenteral nutri-tion, glucose containing solutions, and intraoperative glucose monitor-ing in paediatric patients: a survey of clinical practice. Paediatr Anesth. 2001;11:41-44.
66. Barber JR, Sacks GS. Parenteral nutrition formulations. In: Muller CM, ed. The A.S.P.E.N. Adult Nutrition Support Core Curriculum. 2nd ed. Silver Spring, MD: American Society for Parenteral and Enteral Nutrition; 2012:245-264.
Appendix 1. A.S.P.E.N. Clinical Guidelines Questions for Safe Practice Parenteral Nutrition Ordering, Order Review, Compounding, and Labeling/Dispensing.
Question
1. Does education of prescribers improve PN ordering?2. What is the maximum safe osmolarity of a PN admixture intended for peripheral vein administration?3. What are the appropriate calcium intake and the calcium-phosphate ratios for optimal neonatal bone mineralization in PN therapy?4. What are the clinical advantages/disadvantages of premixed PN formulations compared with traditional/customized PN
formulations?5. What are the clinical/cost advantages/disadvantages of 2-in-1 compared with 3-in-1 PN admixtures?6. What macronutrient dosing limits provide for the most stable 3-in-1 admixtures?7 What are the most appropriate recommendations for maximizing calcium (gluconate) and (Na- or K-) phosphate compatibility in PN
admixtures?8. What micronutrient contamination is present from parenteral stock solutions currently used to compound PN admixtures?9. Should the PN admixture be used as a vehicle for non-nutrient medication delivery?10. Should heparin be included in the PN admixture to reduce the risk of central vein thrombosis?11. What data support a methodology for the repackaging of intravenous fat emulsion (IVFE) into smaller patient-specific volumes?12. What beyond-use date should be used for a. IVFE dispensed for separate infusion in the original container, and b. repackaged intravenous fat emulsion (IVFE)?
by guest on January 9, 2014pen.sagepub.comDownloaded from

38 Journal of Parenteral and Enteral Nutrition XX(X)
Conclusion
PN serves as an important therapeutic modality used in adults, children, and infants for a variety of indications. The appropriate use of this complex therapy aims to maxi-mize clinical benefit while minimizing the potential risks for adverse events. Complications can occur as a result of the therapy, as well as the result of the PN formulation pro-cess. These consensus recommendations are based on prac-tices generally accepted to minimize errors with PN therapy
and categorized in the areas of PN prescribing, order review and verification, compounding, and administration. These recommendations should be used in conjunction with other A.S.P.E.N. publications, and researchers should consider studying the questions brought forth in this document.
Author Note
Companion Clinical Guidelines, titled “Parenteral Nutrition Ordering, Order Review, Compounding, and Labeling Dispensing,” are expected to be published in Winter 2014.
by guest on January 9, 2014pen.sagepub.comDownloaded from
http://pen.sagepub.com/Nutrition
Journal of Parenteral and Enteral
http://pen.sagepub.com/content/36/2_suppl/14SThe online version of this article can be found at:
DOI: 10.1177/0148607111435332
2012 36: 14SJPEN J Parenter Enteral NutrMichael R. Cohen
Safe Practices for Compounding of Parenteral Nutrition
Published by:
http://www.sagepublications.com
On behalf of:
The American Society for Parenteral & Enteral Nutrition
can be found at:Journal of Parenteral and Enteral NutritionAdditional services and information for
http://pen.sagepub.com/cgi/alertsEmail Alerts:
http://pen.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Mar 1, 2012Version of Record >>
by Karrie Derenski on April 1, 2013pen.sagepub.comDownloaded from

PN Safety Summit Report
Journal of Parenteral and Enteral NutritionVolume 36 Supplement 2March 2012 14S-19S© 2012 American Society for Parenteral and Enteral NutritionDOI: 10.1177/0148607111435332http://jpen.sagepub.comhosted athttp://online.sagepub.com
Errors during pharmacy preparation of parenteral products and admixtures have been reported to the Institute for Safe Medica-tion Practices (ISMP) over the years. As early as the 1990s, observational studies on the accuracy of preparing small- and large-volume injectables, chemotherapy solutions, and paren-teral nutrition (PN) showed a mean error rate of 9%, meaning almost 1 in 10 preparations were prepared incorrectly and then dispensed.1 Error rates for complex solutions such as PN were especially high—37% for manual preparation and 22% for preparations that were partly automated. More recently, a 2009 State of Pharmacy Compounding Survey showed that 30% of hospitals have experienced a patient event involving a com-pounding error in the past 5 years.2
Recently, several high-profile intravenous (IV) admixture error cases have received media attention, several of which specifically related to PN compounding, engendering a deci-sion by the American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) to conduct a PN safety summit. In prep-aration for the meeting, a review of past error reports submit-ted to the ISMP National Medication Errors Reporting Program (ISMP MERP) was conducted to describe some of the com-monly reported contributing factors. Although the causes of these errors are numerous and varied, examples of pharmacy PN preparation errors follow.
Wrong Dextrose Concentration
A serious issue in the early years of PN compounding was confusion between 5% dextrose large-volume parenteral con-tainers and 50% or 70% dextrose, mainly due to similar pack-aging. In some cases, mix-ups were also reported between amino acid and dextrose solutions. In one case, a patient erro-neously received 70% dextrose instead of 10% amino acids. In another, a fold in the bag made a 7 look like a 1, contributing to a mix-up between 70% and 10% dextrose. The error was discovered the following morning when the 70% dextrose bag was noticed on the pharmacy’s automated IV compounder. Fortunately, practitioner recognition of these problems, as well as labeling and packaging improvements by large-volume
parenteral solution manufacturers, has helped to reduce these types of incidents. In addition, incorporation of refractometer testing and a final check of the actual total bag weight com-pared with a calculated expected weight has also resulted in fewer such reports to the ISMP.
Other PN Product Mix-ups
Mix-ups between 250-mL containers of 5% dextrose and potassium chloride concentrate have occurred, suggesting that potassium additive solutions must be carefully stored and con-trolled while in use. The ISMP frequently receives reports about mix-ups between small-volume and large-volume par-enteral products such as heparin sodium and magnesium sul-fate, potassium phosphate and magnesium sulfate, and many others. Best practice dictates that every organization have at least 1 individual who regularly reviews ISMP reports to iden-tify potential problems at their location. Often problems can be avoided by working with group purchasing organizations to modify purchasing contracts when, for example, 2 different products are known to look nearly identical to one another.
Whenever possible, have a pharmacist pull the necessary products prior to compounding of the preparation and place them in a bin to give to technicians. Technicians should then verify the products and, if they do not match what is expected, ask questions before preparation. Optimally, either bar coding should be used with an automated compounder, or an indepen-dent check of ingredients should be made by the pharmacist before product is prepared if bar coding is not used. Ensure that
From the Institute for Safe Medication Practices, Horsham, Pennsylvania.
Financial disclosure: none declared. The A.S.P.E.N. Parenteral Nutrition Safety Summit was made possible through the sponsorship of Baxter International, Inc.
Received for publication December 2, 2011; accepted for publication December 5, 2011.
Corresponding Author: Michael R. Cohen, Safe Medication Practices, Horsham, PA; e-mail: [email protected].
Safe Practices for Compounding of Parenteral Nutrition
Michael R. Cohen, RPh, MS, ScD, FASHP
AbstractSafe practices for sterile compounding are essential to preventing errors, particularly with parenteral nutrition (PN). This article reports several areas of errors in PN processes and provides recommendations for error prevention. (JPEN J Parenter Enteral Nutr. 2012;36:14S-19S)
Keywordselectrolytes/acid-base; outcomes research/quality; parenteral formulas/compounding; parenteral nutrition
by Karrie Derenski on April 1, 2013pen.sagepub.comDownloaded from

Safe Practices for Compounding of Parenteral Nutrition / Cohen 15S
preparations are discarded if there are any doubts, even if minor, about the compounding and storage of the preparation.
Catheter Misconnections
Luer connector systems, common to many healthcare cathe-ters, tubes, administration sets, extension sets, and syringes, have been at the heart of many catheter/tubing misconnec-tions. At the center of one of the most commonly reported problems is the fact that some manufactured enteral catheters still have end connectors that only accept parenteral adminis-tration sets and syringes. Then, even if a liquid medication is prepared in an oral syringe, the medication must be transferred to a parenteral syringe for administration via this type of enteral tube connector, risking the accidental administration of the drug via a parenteral line. In addition, lines have been jury-rigged to make an incompatible fitting work.
Breast milk has been given intravenously to neonates and bladder irrigation solutions of amphotericin B (yellow in color) have been confused with PN solutions with vitamins and given intravenously. Likewise, PN solutions with vitamins have been administered via Foley catheters. Also, IV administration sets have been spiked into enteral nutrition containers, resulting in enteral nutrition solutions administered intravenously.
Catheter/tubing misconnections are a serious problem in healthcare. The International Organization for Standardization (ISO) has been working with the Association for the Advancement for Medical Instrumentation (AAMI) on a stan-dard (ISO/IEC/FDIS 80369-1, “Small-bore connectors for liq-uids and gases in healthcare applications”) that will result in making various healthcare catheter fittings and associated tub-ing sets or syringes incompatible with one another.
It is important for organizations to perform a risk assessment to identify the various types of catheters and fittings now in use, identify the possibility for misconnections, assess the potential severity of misconnections, and address process changes that need to be made. For example, 2 easy-to-implement risk reduction strategies common to most types of catheter/tubing misconnections include (1) always tracing the port and tubing back to its insertion site to verify the correct access/route of administration and (2) never attempting to force or jury-rig a connection that does not fit easily and securely into an access port.
Issues Related to Drug Shortages
A national shortage of common electrolyte solutions, vitamins, and trace elements in certain strengths and sizes has forced many pharmacists to replace their standard injectable solutions with a different product. These products, sizes, or concentra-tions that have been in short supply include concentrated sodium chloride 14.6% and 23.4%; potassium phosphate injection; potassium acetate injection; zinc chloride injection; selenium, calcium gluconate injection; and calcium chloride
injection. As a result, it has become critically important to fol-low a formal verification process, not only for purchasing alternative products and making inventory adjustments but also for ensuring that necessary changes are made within com-puter software that drives various medication use systems, such as IV compounders and computer order entry systems, smart pumps, and any other affected technology.
At issue with automated IV compounders is that the National Drug Code (NDC) number in the compounder soft-ware tags the specific concentration of the listed electrolyte. However, there is no interface for communication with the pharmacy order entry system where NDC numbers are updated when product changes occur. Thus, if the compounder soft-ware is not changed manually to reflect the new product and NDC number, bar-coding systems will not properly detect a difference between the software and the product being scanned for use with the compounder.
Pharmacists must ensure that a workable, standard process exists and is well understood by practitioners for making these adjustments with all due care. Omitting this important step could easily result in a serious error. Require that 2 individuals perform the validation check of these database modifications using a standardized process and checklist. Start by having 1 staff member make the change to the database and prepare the checklist. Then have this same individual read the changes aloud from the checklist while a pharmacy supervisor or sec-ond designated individual confirms the changes. The checklist should be countersigned by a pharmacy supervisor after the change has been validated. This checklist would not be required for the addition of lot numbers and expiration dates, as is required as part of the routine production process.
In addition, shortages have sometimes led to compounding of sterile preparations by sterile IV compounding pharmacies when manufacturers have been unable to supply. However, a lack of governmental oversight for USP chapter <797> com-pliance in many states, as well as confusion over which of these pharmacies are regulated by the U.S. Food and Drug Administration (FDA) as manufacturers and thus required to follow current good manufacturing processes, has led to a dearth of information about which of these compounding phar-macies provide an appropriate level of safety for the prepara-tions they provide. In some cases, quality control compliance has been compromised, resulting in inadvertent contamination of solutions. For example, the Alabama Department of Public Health (ADPH) reported an ongoing investigation of an out-break of Serratia marcescens bacteremia associated with con-taminated PN bags in 6 Alabama hospitals. An investigation by the ADPH and the Centers for Disease Control and Prevention (CDC) led to the discovery that because of a shortage of cer-tain commercial amino acid solutions, a compounding phar-macy prepared batches of solutions from nonsterile powders of amino acids. Sterilization of the solutions ultimately failed, resulting in cases of S marcescens bacteremia in 19 patients, 9 of which resulted in fatalities.
by Karrie Derenski on April 1, 2013pen.sagepub.comDownloaded from

16S Journal of Parenteral and Enteral Nutrition 36(Suppl 2)
The ISMP has called upon the FDA to work collaboratively with the state boards of pharmacy to provide them with the necessary support and training to survey compounding phar-macies for compliance with USP Chapter <797>.3 Furthermore, we believe compounding pharmacies that distribute sizable quantities (to be defined by the FDA) of preparations, as well as those operating interstate, should be registered with the FDA and subject to periodic inspections. We also encourage the FDA to move forward with plans to publish guidance on Good Pharmacy Compounding Practices for Sterile Drug Products and the Outsourcer Pharmacy Operations Compliance Policy Guide (www.ismp.org/sc?k=ucm079647) to clearly articulate requirements for registration with the FDA, periodic inspections, support available to the state boards of pharmacy, and expectations regarding the state boards’ role in regulating compounding pharmacies.
As a result of drug shortages, sometimes pharmacists advise a switch to oral forms of drugs. This was the case during a recent shortage of parenteral multiple vitamins. In such cases, patient medication administration records should be monitored to ensure that patients are actually receiving the oral replace-ment. Sometimes, because of taste or gastrointestinal (GI) issues, or because oral medications may not be considered as important as injectables, doses are left unadministered.
Failure to Incorporate IV Compounder Catastrophic LimitsNot all automated compounders have the inherent software capability to establish catastrophic limits to ensure an inadver-tent catastrophic amount of electrolyte is not delivered. Even when limits can be set, it may still be possible for an entry to be made without a hard stop if the PN order is entered into a non-PN patient-type template that the user can create without dose limits. Another possibility is if an adult application of the software was purposely used to enter the neonatal PN where the limits set are far too high for the infant. Patient safety dic-tates that pharmacies preparing PN solutions with electrolytes should install, test, and maximize automated dose limit warn-ings in the pharmacy computer system and automated com-pounders, particularly for high-alert medications such as PN and its products.
Insulin Mix-ups With Heparin
Several incidents have been reported where mix-ups between heparin and insulin were at issue. In one case, a bag of PN contained insulin instead of heparin. A blood glucose level of 17 mg/dL was reported for a premature baby in the neonatal intensive care unit (NICU), 6 hours after a PN infusion had been started. Despite multiple bolus doses of dextrose and an infusion of dextrose 20% in sodium chloride 0.45%, the hypo-glycemia did not completely resolve until discontinuing the PN. Although the infant survived, the baby’s long-term well-being
had not been assessed at the time of the report. Insulin has been accidentally added to infant PN in other cases known to the ISMP, each with fatal outcomes. In addition, a 1991 ISMP article describes cases of severe hypoglycemia after one phar-macist added 200 units of insulin instead of heparin to PN and another added 1000 units of insulin instead of heparin to PN.4 Also, in other cases in our database, 2 patients, neither of whom was diabetic, died after being injected with insulin instead of heparin during a vascular catheter flush procedure. And in yet still other reports, a nurse flushed a patient’s central line catheter with insulin instead of heparin, and another erro-neously transcribed a verbal order to resume an insulin drip as “resume heparin drip.”5
The most common factors associated with these mix-ups seem to be (1) similar packaging of insulin and heparin in 10-mL vials and placement of insulin and heparin vials, both typically used each shift/day, next to each other on a counter or under a pharmacy IV admixture hood and (2) mental slips leading to confusion between heparin and insulin, especially because both drugs are dosed in units. Some implanted cathe-ters are flushed with 100 units per mL of heparin, and insulin is commonly available in a concentration of 100 units per mL. Perhaps the risk of a mental slip is growing, as insulin infu-sions are more commonly used in recent years.
To prevent confusion between heparin and insulin vials during drug preparation, do not keep insulin and heparin vials alongside one another on top of counters or drug carts or under the laminar flow IV admixture hood in the pharmacy. Many organizations do not allow insulin near the location where PN is being prepared, as they add all insulin separately. Some organizations have worked to eliminate heparin as a PN addi-tive, thus removing the potential for confusion with insulin.
Dangerous Abbreviations and Dose DesignationsErrors have happened commonly with insulin and heparin when the word unit is abbreviated with a U. The U can easily be con-fused as a 0, a 7, or even cc when scripted. And U can look like a 0 even when typed. Similarly, when international unit is abbrevi-ated IU, it has been seen as IV, resulting in some oral liquids being injected directly into the venous system. Neither of these abbre-viations should ever be used under any circumstances as it has been responsible for fatalities and brain injuries due to insulin overdose or bleeding events due to heparin overdose.
Compounding errors due to leading zeros and trailing zeros are also frequently reported, and some have been associated with catastrophic results due to 10-fold overdoses when, for example, a decimal point is not seen when a number is less than 1 (eg, .2 mg may be seen as 2 mg) or when a trailing zero is used (1.0 seen as 10). For obvious reasons, all practitioners must take this issue very seriously. A complete list of danger-ous abbreviations can be found at http://www.ismp.org/ Tools/errorproneabbreviations.pdf. Also, ISMP guidelines for
by Karrie Derenski on April 1, 2013pen.sagepub.comDownloaded from

Safe Practices for Compounding of Parenteral Nutrition / Cohen 17S
Communication of Medication Orders can be found here: http://www.ismp.org/newsletters/acutecare/articles/20030220.asp. You should also refer to The Joint Commission’s “Do Not Use” list: http://www.jointcommission.org/assets/1/18/Official_Do% 20Not%20Use_List_%206_10.pdf.
Ineffective or Nonexistent Systems for Independent ChecksThe ISMP is aware of fatal errors that reached patients because of IV admixture errors that were not detected during the checking process. In some of these cases, the operator’s work has gone unchecked. Whether PN is set up and prepared by a pharmacist or pharmacy technician is not what matters. What matters is that there is a method available to ensure sufficient quality control checks are made and documented 100% of the time.
Checks performed after manual IV admixture preparation often involve the “syringe pullback” method, particularly if the checking pharmacist is not consistently available in the IV clean room. To check each product added to a PN solution or chemotherapy bag, for example, the empty syringe used for each drug or electrolyte is left alongside the item with its plunger pulled back to the volume that was added.
Although the “syringe pullback” checking process is stan-dard in many hospitals and even mentioned in USP Chapter <797>, it is less than ideal because the check is made after preparation and is based on the preparer’s memory of how much product was added to the bag. Proper placement of the syringe next to the used product can also be problematic, par-ticularly if the checking area is small and/or crowded. Situations have occurred in which empty syringes were placed alongside the wrong drug vial or the plunger was drawn back to an incorrect volume. If checking pharmacists noticed incon-sistencies, they have occasionally assumed them to be errors in matching the syringe with the correct vial or pulling back the plunger to the correct volume, not actual errors during the admixture process.
To minimize these situations, a standardized commercially available PN product (such as “premixed” solutions) or an out-sourced PN preparation could be used when clinically appro-priate. When pharmacy admixture is required, at a minimum, preparations with high-alert medications (eg, chemotherapy, PN, electrolytes, neonatal/pediatric infusions) should employ an independent check of the vials, prepared syringes, and con-tainer labels (drug and diluent) prior to adding it to the solution.
Given that IV production errors can result in serious medi-cation errors, where affordable, new IV robotic preparation systems and commercially available workflow management systems are highly welcomed technologies. These systems use robotics or barcode scanning with video technology or digital images to reduce the risk of error. Stored digital images in workflow management systems allow visibility of the actual
drug and amount drawn into the syringe prior to addition to the IV bag. They can also be employed in a way that lets pharma-cists complete essential checks when outside of the IV admix-ture area or even from a remote location.
Establish a standard operating procedure for how pharma-cists should verify preparations compounded in the IV room. For additives checked before mixing (superior checking pro-cess, recommended when mixing high-alert medications), ensure that the process allows the pharmacist to clearly verify the source of the additive visually (eg, vial, ampul, stock bot-tle) and the measured amount. For additives checked after mix-ing (inferior checking process, which involves containers placed alongside empty syringes with plungers pulled back to the volume measured [not recommended]), ensure that the method allows the pharmacist to make reasonable assumptions regarding the products and amounts added to base solutions.
In either situation, it is also important to include verifica-tion of the base solution and any premixed dilutions used to make the final preparation, as with neonatal/pediatric prepara-tions, where a product is first diluted and then used as a stock bottle during daily preparations. It is also critical to require the checking pharmacist to verify the label and final preparation via comparison with the original order. The automated tech-nologies mentioned above can make safer verification pro-cesses within reach of most hospitals.
Place each compounded preparation and associated sup-plies into a single bin/basket for checking, one at a time. Avoid bins/baskets with multiple compartments. Do not leave prod-ucts on open counters for checking, even if they are well sepa-rated. Establish a system to communicate when compounded preparations are ready for checking, monitor the workflow, and provide assistance when necessary to avoid a backlog of preparations awaiting verification. Some hospitals use differ-ent-colored bins to signify steps in the process (eg, red bin for final preparations ready to be checked) or categories of solu-tions (ie, neonatal, pediatric, adult). Ensure the checking area is uncluttered, of sufficient size, and well lighted.
Dual-Chambered Bag Systems
On the market is a PN multichamber bag system with 1 cham-ber containing dextrose and the other chamber containing amino acids. A seal that separates the 2 chambers must be broken to mix the contents of both chambers together prior to dispensing. IV fat emulsion and electrolytes, vitamins, and trace elements are added as appropriate. There is also a similar product with electrolytes, and this can help to reduce medica-tion preparation errors by lowering the risk of compounding calculations and minimizing the number of preparation steps. However, the ISMP has published previous reports where nurses or pharmacy staff have failed to activate or mix together the multichamber bags of PN solutions.6 The ISMP recommends that, wherever possible, these products not remain available in an automated dispensing cabinet or other
by Karrie Derenski on April 1, 2013pen.sagepub.comDownloaded from

18S Journal of Parenteral and Enteral Nutrition 36(Suppl 2)
floor stock systems and other areas outside the pharmacy. Mixing should always be done prior to dispensing.
In hospitals without 24-hour service, PN should not be started after pharmacy hours, and dextrose alternatives should be available to provide replacement solution in emergencies until pharmacy service is available. Should an unusual circum-stance exist, where product must be stored outside the phar-macy, they need to be accompanied by auxiliary labels (eg, “Mix Properly Prior to Administration”) and have instructions for mixing. The label could be applied to the overwrap near the port that will be spiked with tubing, to remind staff to mix the 2 chambers before administration. The manufacturer provides educational resources on its Web site (www.clinimix.com/pop-ups/video.jsp) that illustrate the multichamber bag technology and offer step-by-step bag activation training.
Insulin and Tuberculin Syringe Measurement ErrorsThe ISMP has received multiple error reports involving improper use of syringes to prepare insulin doses. These errors have been made by nurses, pharmacists, physicians, physician assistants, and so on. For example, when 7 units of insulin were needed, 0.7 mL (or 70 units with U-100 insulin) was drawn into a tuberculin syringe. In a recent article on insulin dosing mix, we described multiple cases where healthcare personnel were unfamiliar with proper use of the dose scale on insulin syringes, resulting in multiple over-doses and fatalities.7 Human error (eg, mental slips, lapses, forgetfulness) associated with insulin dose measurement is at issue.
With insulin, it must not be assumed that all healthcare practitioners are knowledgeable and skilled with measuring doses, preparing insulin infusions, and recognizing doses that exceed safe limits. Education regarding the concentration of insulin products, the differences between insulin syringes and other parenteral syringes, how to measure doses, recognition of safe dosage ranges, and how to administer the drug should be provided to all who might prepare PN solutions or adminis-ter insulin. Restrict insulin preparation and administration to those who have demonstrated competency. As always, require an independent double-check of all doses before dispensing and administering IV insulin.
Special Handling of Electrolyte Additives
Sending additives to the nursing unit or the patient’s home in syringes has posed some safety problems. In one incident, a poorly trained patient was sent syringes of potassium chlo-ride to add to her son’s home PN upon detection of hypoka-lemia. Sadly, the mother injected the drug directly into the patient’s venous line, killing him almost instantly. Sending syringes for addition at home is a perilous practice for many reasons, not the least of which is the potential for misuse by
caregivers who are not properly trained. Newly prepared solutions are a safer option.
Adding certain drugs to hanging IV containers can also present problems. With potassium chloride in particular, the additive may layer in the bottom of the IV bag close to the exit port. Thus, when infusion is resumed, a bolus of potassium chloride is inadvertently administered. Many nurses are not aware of this. Again, additives should not be added to PN solu-tions except under proper conditions in the pharmacy.
Order Entry Errors
Electrolytes in PN have been entered into the computer incor-rectly. Often the basis for PN preparation in the IV compound-ing area is a label printed by the person inputting PN orders. However, no one else is actually making a second check of what was typed in by the order entry pharmacist. Thus, only one person actually has read the order, interpreted it, and entered it, and the other person is working off of that informa-tion. A second independent check is necessary, but a way to communicate the original scanned or electronic order must be available so that IV room staff do not need to leave their area. Standard label formats that list ingredients in the same order as PN order sets add efficiency and safety to the order entry process.
Accidental Mix-ups Between Dosage Units
Use of incorrect dosage units during ordering, order transcrip-tion, and/or labeling has been a routine cause for catastrophic errors. One example is an incident where an infant received a lethal dose of zinc stemming from an error that occurred dur-ing the order entry and compounding of a PN solution. The PN was prescribed for a preterm infant born at 26 weeks’ gesta-tion. On the day of the event, the physician’s order included directions to add zinc in a concentration measured as mcg/100 mL. Because the automated compounder used for PN required entry of zinc in a mcg/kg dose, the pharmacist converted the mcg/100-mL dose to a mcg/kg dose. She performed this calcu-lation correctly but accidentally entered the zinc dose in the pharmacy computer in mg, not mcg. This resulted in a final concentration in terms of mg/100 mL—a 1000-fold overdose.8
Another pharmacist checked the work and preparation labels that were printed for compounding of the PN, but she did not notice the mcg to mg error. A pharmacy technician pre-pared the PN, replenishing the compounder syringe that con-tained zinc 11 times while preparing the solution, which required dozens of vials of zinc sulfate. The pharmacy com-puter order entry system and the automated compounder used to mix the PN did not alert the pharmacist that a 1000-fold overdose had been entered into the systems for the zinc addi-tive. Upon discovery of the error, the infant received edetate calcium disodium (also referred to as calcium EDTA), which had been compounded by an external pharmacy, but the
by Karrie Derenski on April 1, 2013pen.sagepub.comDownloaded from

Safe Practices for Compounding of Parenteral Nutrition / Cohen 19S
chelation therapy was unsuccessful, and the infant died. The coroner listed cardiac failure caused by zinc intoxication as the cause of death.
To best prevent incidents like this, the method of ordering PN solutions for neonates, pediatric patients, and adults should be standardized so that each prescribed product and strength matches the dosing templates used for entering the orders into the computer system and automated compounder. Use pre-printed forms or standard order sets that list typical products and prompt the correct dosing method. On the rare occasions that calculations are necessary, require 2 clinicians to calculate the dose independently and compare their answers for verification.
This error happened at night when the PN was ordered. Policies that require prescribers to order PN daily during the day shift should be established and enforced to maximize safety with which these solutions are prepared and dispensed. Pharmacy staff should be aware of patients who are receiving PN and check if orders have not been received by the estab-lished time.
Continually emphasize to staff to complete a full review of the patient’s medications any time there is a need to use more than a few dosage containers (whether it be tablets, capsules, vials, ampuls, etc) to prepare or administer a single dose of any medication. In this case, use of 11 vials should have signaled that a catastrophic event may have been in process.
Safe Storage of Supplies
Separate the storage of concentrated bulk solutions, particu-larly concentrated electrolytes, amino acids, and dextrose, from all other products that are directly dispensed to a patient care unit. Among admixture supplies, also sequester sterile water for injection to reduce the risk of inadvertent use. When possible, employ small-volume vials of concentrated electro-lytes for manual IV additives so that bulk bottles cannot be inadvertently used as base solutions or introduced back into the production line. In fact, it would be safest to use a vial size closest to the dose required to prepare the final preparation for any drug used in manual sterile compounding.
Error Reporting
Errors with PN or enteral nutrition (EN) should be reported to the ISMP MERP so that others may learn from near
misses or actual PN-related errors. Although PN and EN are not traditionally thought of as medications, they are thera-pies that are prescribed, dispensed, and administered similar to medications. Administration also involves infusion devices that may be used in error. A.S.P.E.N. recommends that errors such as the ones described here be reported to the ISMP MERP. A special Web site location has been estab-lished for this purpose at www.nutritioncare.org/safety. The ISMP is a federally designated patient safety organization (PSO) that extends privilege and confidentiality protection for patient safety work product (information collected and created during the reporting and analysis of patient safety events).
Conclusion
Errors have occurred with PN ordering, transcribing, and com-pounding processes. Safe and standardized practices using organizational and regulatory guidelines must be used, and errors that do occur must be reported.
References
1. Flynn EA, Pearson RE, Barker K. Observational study of accuracy in compounding i.v. admixtures at five hospitals. Am J Health Syst Pharm. 1997;54(8):904-912.
2. Pharmacy Purchasing & Products. State of pharmacy compounding 2009: survey findings. Pharm Purchasing Products. 2009;6(4):4-20.
3. TPN-related deaths call for FDA guidance and pharmacy board oversight of USP Chapter <797>. April 11, 2011. http://www.ismp.org/Newsletters/acutecare/archives/Apr11.asp
4. Cohen MR. Insulin overdoses that originated in the pharmacy IV admix-ture area. Hosp Pharm. 1991;26:998-999.
5. Action needed to prevent dangerous heparin-insulin confusion. ISMP Medication Safety Alert! May 3, 2007. http://www.ismp.org/Newsletters/acutecare/articles/20070503.asp
6. Institute for Safe Medication Practices (ISMP). Mixing multi-chamber bags of CLINIMIX (amino acid and dextrose) or CLINIMIX E (amino acid and dextrose with electrolytes) ISMP Quarterly Action Agenda. http://www.ismp.org/Newsletters/acutecare/articles/ActionAgenda1102.doc. Accessed November 19, 2011.
7. Institute for Safe Medication Practices (ISMP). Misadministration of IV insulin associated with dose measurement and hyperkalemia treatment. ISMP Medication Safety Alert! August 11, 2011. http://www.ismp.org/Newsletters/acutecare/archives/Aug11.asp
8. Institute for Safe Medication Practices (ISMP). Fatal 1,000-fold overdoses can occur, particularly in neonates, by transposing mcg and mg. ISMP Medication Safety Alert! September 6, 2009. http://www.ismp.org/news-letters/acutecare/articles/20070906.asp
by Karrie Derenski on April 1, 2013pen.sagepub.comDownloaded from

Safe Practices forParenteral Nutrition
Task Force for the Revision of SafePractices for Parenteral Nutrition:
Jay Mirtallo, MS, RPh, BCNSP, Chair,Todd Canada, PharmD, BCNSP,
Deborah Johnson, MS, RN,Vanessa Kumpf, PharmD, BCNSP,
Craig Petersen, RD, CNSD,Gordon Sacks, PharmD, BCNSP,
David Seres, MD, CNSP, andPeggi Guenter, PhD, RN, CNSN
Approved by A.S.P.E.N. Board ofDirectors July 21, 2004
Supplement to
An international journal of nutrition and metabolic support
JOURNAL OF PARENTERALAND ENTERAL NUTRITION
VOLUME 28, NUMBER 6, SUPPLEMENT
NOVEMBER–DECEMBER 2004
Special Report
Safe Practices for Parenteral Nutrition
Task Force for the Revision of Safe Practices for Parenteral Nutrition: Jay Mirtallo, MS, RPh, BCNSP, Chair,Todd Canada, PharmD, BCNSP, Deborah Johnson, MS, RN, Vanessa Kumpf, PharmD, BCNSP,
Craig Petersen, RD, CNSD, Gordon Sacks, PharmD, BCNSP, David Seres, MD, CNSP, andPeggi Guenter, PhD, RN, CNSN
APPROVED BY A.S.P.E.N. BOARD OF DIRECTORS JULY 21, 2004
NOTICE: These A.S.P.E.N. Practice Guidelines for SafePractices for Parenteral Nutrition are based upon generalconclusions of health professionals who, in developing suchguidelines, have balanced potential benefits to be derivedfrom a particular mode of providing parenteral nutritionfeeding formulations. The underlying judgment regardingthe propriety for any specific practice guideline or procedureshall be made by the attending health professional in light ofall the circumstances presented by the individual patient andthe needs and resources particular to the locality. Theseguidelines are not a substitute for the exercise of such judg-ment by the health professional, but rather are a tool to beused by the health professional in the exercise of such judg-ment. These guidelines are voluntary and should not bedeemed inclusive of all proper methods of care or exclusive ofmethods of care reasonably directed toward obtaining thesame result.
TABLE OF CONTENTS
Preface .....................................................................S40I. Introduction..................................................S42
II. Ordering Parenteral NutritionBackground...................................................S43Mandatory for Inclusion............................S44
Overall Design: Clarity of the OrderingForm ...........................................................S44Specific Components ..............................S45
Table II. Determining the Estimated Osmo-larity of PN Formulations .........................S45Strongly Recommended for Inclusion....S46Worthy of Consideration for Inclusion ....S46Adult PN Order Template .........................S46Figure 1. Physician Orders: ParenteralNutrition-Adult.............................................S47Practice Guidelines.....................................S48
Special Considerations ..........................S48III. Labeling Parenteral Nutrition Formulations
Background .............................................................S48PN Label Template ...............................................S49Practice Guidelines ..............................................S51
Special Considerations...................................S52Standard Label Templates..............S50, S51, S52
IV. Nutrient RequirementsNutrient Requirements: Adults................S53Nutrient Requirements: Pediatrics.........S55
Aluminum contamination .....................S56Practice Guidelines.....................................S56
Special Considerations ..........................S57V. Sterile Compounding of Parenteral Nutri-
tion FormulationsScreening the PN Order
Background ..............................................S57Practice Guidelines ................................S58
Special Considerations .......................S58PN Compounding
Background ..............................................S58Practice Guidelines ................................S60
Quality Assurance of the CompoundingProcess
Background ..............................................S60Gravimetric Analysis .............................S60Chemical Analysis...................................S60Refractometric Analysis........................S60In-Process Testing ..................................S60Practice Guidelines ................................S61
Special Considerations ......................S67VI. Stability and Compatibility of Parenteral
Nutrition FormulationsPN Stability...................................................S61PN Compatibility .........................................S62
Medication Administration with PN....S63Insulin Use with PN...........................S64
Practice Guidelines.....................................S64VII. Parenteral Nutrition Administration
Venous Access Selection, Care and Assess-ment ................................................................S65Medical Equipment for PN Administration
Filters.........................................................S66Infusion Pumps and AdministrationSets .............................................................S66
Administration Issues Related to PN Solu-tion Properties .............................................S67
Patient Response to PN Administra-tion ..............................................................S68
Received for publication, July 1, 2004.Accepted for publication, July 31, 2004.Correspondence: Jay M. Mirtallo, RPh, BCNSP, 2921 BraumillerRoad, Delaware, OH 43015. Electronic mail may be sent to [email protected].
0148-6071/04/2806-0S39$03.00/0 Vol. 28, No. 6JOURNAL OF PARENTERAL AND ENTERAL NUTRITION Printed in U.S.A.Copyright © 2004 by the American Society for Parenteral and Enteral Nutrition
S39
IVFE infusion in hypertriglyceridemicpatients ......................................................S68
Use of PN Prepared by Another Facility ...S68Practice Guidelines.....................................S69
GLOSSARY OF TERMS
Automated Compounding Device: A device usedin the preparation of parenteral nutrition. It auto-mates the transfer of dextrose, amino acids, fat emul-sion, and sterile water, as well as small volumeinjectables, such as electrolytes and minerals to thefinal PN container. The device is driven by computersoftware.
Beyond-use Date: The date established by health-care professionals from the published literature ormanufacturer-specific recommendations beyond whichthe pharmacy-prepared product should not be used.
Compatibility: The ability to combine 2 or morechemical products such that the physical integrity ofthe products is not altered. Incompatibility refers toconcentration-dependent precipitation or acid-basereactions that result in physical alteration of the prod-ucts when combined together.
Computerized Prescriber Order Entry (CPOE):A prescription ordering system where the prescriberenters orders directly into a computer.
DEHP: Di (2-ethylhexyl) phthalate, a plasticizerused in various intravenous administration sets orplastic infusion bags.
Dosing Weight: The weight used by the clinician indetermining nutrient doses. Dependent on institu-tional or professional preference, the dosing weightmay be the actual, ideal or adjusted body weight of theindividual.
Drug-nutrient Interaction: An event that occurswhen nutrient availability is altered by a medication,or when a drug effect is altered or an adverse reactioncaused by the intake of nutrients.
Dual-chamber Bags: A bag designed to promoteextended stability of a PN formulation by separatingthe IVFE from the rest of the formulation. It consists of2 chambers separated by a seal or tubing that isclamped. At the time of administration, the seal orclamp is opened to allow the contents of both chambersto mix and create a TNA.
Expiration Date: The date established from scien-tific studies to meet FDA regulatory requirements forcommercially manufactured products beyond whichthe product should not be used.
Hang Time: The period of time beginning with theflow of a fluid through an administration set and cath-eter or feeding tube and ending with the completion ofthe infusion.
Institute of Safe Medication Practices (ISMP):A nonprofit organization that works closely withhealthcare practitioners and institutions, regulatoryagencies, professional organizations and the pharma-ceutical industry to provide education about adversedrug events and their prevention. The Institute pro-vides an independent review of medication errors thathave been voluntarily submitted by practitioners to anational Medication Errors Reporting Program
(MERP) operated by the United States Pharmacopeia(USP).
Intravenous Fat Emulsion (IVFE): An intrave-nous oil-in-water emulsion of oil(s), egg phosphatidesand glycerin. The term should be used in preference tolipids.
MEDMARX: The internet-based medication errorreporting program operated by the U.S. Pharmacopeiathat complements quality improvement activities atthe local and national level. MEDMARX is availablethrough subscription service only.
Osmolarity: The number of osmotically active par-ticles in a solution, expressed as milliosmoles per literof solution. The osmolarity of a PN formulation needsto be considered, when determining whether that solu-tion can be administered through a peripheral vein.
Parenteral Nutrition: Nutrients provided in-travenously.
Central: Parenteral nutrition delivered into a highflow vein, usually the superior vena cava adjacent tothe right atrium.Peripheral: Parenteral nutrition delivered into aperipheral vein, usually of the hand or forearm.Percent Concentration (weight/volume): A
standardized unit of concentration determined by theamount of drug or nutrient within a given volume,whereby 1% (w/v) is equivalent to 1 g of drug or nutri-ent per 100 mL of volume.
Stability: The extent to which a product retains,within specified limits, and throughout its period ofstorage and use (i.e., its shelf-life), the same propertiesand characteristics that it possessed at the time of itsmanufacture.
Total Nutrient Admixture (TNA): A parenteralnutrition formulation containing IVFE as well as theother components of PN (carbohydrate, amino acids,vitamins, minerals, trace elements, water and otheradditives) in a single container.
Medication Error Reporting Program (MERP):U.S. Pharmacopeia’s spontaneous reporting programfor medication errors that is operated in cooperationwith the Institute for Safe Medication Practices for useby any healthcare professional or interested party.
Venous Access Devices (VAD): Catheters placeddirectly into the venous system for infusion therapyand/or phlebotomy.
PREFACE
The members of the American Society for Parenteraland Enteral Nutrition (A.S.P.E.N.) are health care pro-fessionals representing the fields of medicine, nursing,pharmacy, and dietetics. A.S.P.E.N.’s mission is toserve as the preeminent, interdisciplinary nutritionsociety dedicated to patient-centered, clinical practiceworldwide through advocacy, education, and researchin specialized nutrition support.
Patients may be treated with parenteral nutrition(PN) in any of several care settings including hospitals,long-term care or rehabilitation facilities, or at home.Because patients transfer from one health care envi-ronment to another, it is the opinion of the A.S.P.E.N.Board of Directors that the practice guidelines in the
S40 MIRTALLO ET AL Vol. 28, No. 6

“Safe Practices for Parenteral Nutrition” are the stan-dard of practice for the provision of PN in all health-care settings.
The original ‘Safe Practice’ document was specific toPN and the practice of pharmacy.1 The objective of thisrevision is to deal with PN in a comprehensive mannerrealizing the interdisciplinary nature of this therapy. Anew section is added that addresses the ‘ordering ofparenteral nutrition’. The nutrient range section isexpanded to provide dosage recommendations that gobeyond normal requirements and include componentsnot addressed in the initial guidelines (e.g., iron andthe potential for developing an essential fatty aciddeficiency). Further, the PN filtration section is re-named and expanded into: “Administration of paren-teral nutrition”. This section includes hang time forintravenous fat emulsion (IVFE) and PN, formulareview prior to administration as well as institutionaluse of PN brought from home or sent with the patienton transfer from another facility.
Unfortunately, practice for some of these latter areashave little, if any, published evidence to support goodpractice. As such, the Task Force conducted the 2003Survey of PN Practices. This provided an overview ofthe variance and consistency of current practices. Thesurvey was organized in the following sections: demo-graphics, writing PN orders, computer order entry ofPN orders and problems with PN orders. There were667 responses, mostly from hospitals (85%), with die-titians (55%) and pharmacists (32%) being the predom-inant professionals responding to the questionnaire. Inthe home health care environment, responses werefrom pharmacists (76%) and dietitians (17%). Theaverage daily census for organizations responding was100 patients. Most organizations used a once dailynutrient infusion system (76%). The number of adultPN patients per day was from 0–20 for 85% of respond-ers. However, 4.9% of responders reported more than40 adult PN patients per day. For organizations thathad neonate and pediatric patients, the number of PNpatients per day was 0–5 for both.
Over half (54%) of responders had a performanceimprovement program that monitored the appropriateuse of PN, accuracy of PN orders, metabolic complica-tions and catheter and infectious complications. Phy-sicians and nurses selected these categories more fre-quently than pharmacists and dietitians. Qualitycontrol of PN compounding and PN costs were notmonitored as frequently (�50%).
It was noted that physicians were the professionalgroup responsible for writing PN orders. However,there was also significant involvement by dietitians aswell as pharmacists. It is noteworthy that nurse prac-titioners and physician assistants were also involvedwith writing PN orders. Oversight of writing the PNorder was performed predominantly by the pharmacistwith significant involvement by a nutrition supportservice, medical staff committee and nutrition and die-tetics department. For PN components, the base for-mula was ordered in terms of percent final concentra-tion (47%) or as the percent of stock solution (31%).There is no consistent method of ordering PN electro-lytes. Phosphorus is usually ordered as millimoles
(mmol) of phosphorus or as both mmol of phosphorusand milliequivalents (mEq) of associated cation. Elec-trolytes as components of the amino acid formulationwere not usually considered when writing PN orders(71%). Multiple electrolyte formulations were used in62% of organizations, according to the summary ofresponses, but only 46% of the time according to thepharmacist response (in this case, the pharmacistresponse should be more accurate). In 62% of respond-ers, the pharmacist adjusts the chloride and acetatecontent of the PN formulation. Trace elements areordered as a standard volume (87%) with only someorganizations adjusting the content based on thepatient’s clinical condition (22%). Standard orderforms are used by 87% of responders of which 96% arefor adults and 40–42% are for pediatric and neonatalpatients. Home infusion services are the outlier in thisgroup where standard order forms are used in only32% of organizations. Standard orders for laboratorytests and patient care orders are used in only 54% ofcases. Data for the hang time or maximal infusion rateof IVFE were more difficult to interpret since a write-inanswer was required. The maximum hang time for atotal nutrient admixture (TNA) was 24 hours andintermittent, separate IVFE infusion of 12 hours.Responses to minimum hang time (related to maximalinfusion rates) were not consistent.
Only 29% of organizations used a computerized pre-scriber order entry (CPOE) system for PN orders. Ofthese, 88% used it for adults and 54% and 58% used itfor pediatric and neonatal patients. The majority ofpharmacies (88%) used an automated compoundingdevice. Order input to the automated compoundingdevice was done by the pharmacist 84% of the time dueto a lack of an interface with the CPOE system. Only15% of organizations outsourced PN formulations. Ofthose that did, a pharmacist at the organizationreviewed the order where the order originated (95%)prior to it being sent to the compounding pharmacy.
Problems with PN orders were queried in the follow-ing manner; number of PN orders written per day,percent of orders requiring clarification, reasons ordersneeded to be clarified, frequency of errors in PN ther-apy, categories of PN adverse events and severity ofadverse events. Most (55%) organizations deal with0–10 PN orders per day while 15% had more than 30orders per day. These orders need to be clarified �25%of the time for 88% of responders and �10% of the timefor 61% of responders. The most frequent reasonsorders need to be clarified are macronutrient content,illegible orders, incompatibility, nutrient dose outsidethe normal range, infusion rate not prescribed andincorrect PN volume. Seldom, if ever, were orders clar-ified for a pharmacy compounding error. The highestranked reason, very often (5% of responders) was illeg-ible orders. The frequency of reported errors per monthfor PN was low (none in 26%, 1–5 in 60% and 6–10 in10% of responders). These events were related to elec-trolytes (69%), dextrose (31%), insulin (31%), aminoacids, vitamins and IVFE (15% and 26%). Of theseerrors, 55% of responders related them to errors inordering PN in the category of 1–25%, 12% in the26–50% category, 8% in the 51–75% category and 17%
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S41
in the 76–100% category. For adverse events that hadoccurred in the last 2 years, 44% of responders werenot aware of any events, 64% of the events required notreatment or just an increase in monitoring. Only 10%responded that none of these events occurred. Of inter-est are the reports by a few responders of harm, tem-porary (13%, N � 61 responders) or permanent (2%,N � 7 responders), near-death (3%, N�16 responders)or death (2%, N �7 responders). Whether hospitalsallowed PN formulations compounded by organizationsother than their own was queried and results weremixed (43% - Yes, 58% - No).
Realizing that the original Safe Practice guidelinesare not consistently implemented,2 the Task Forceused this information to identify practices pertinent tothe revision of the Safe Practice guidelines. The surveyresults presented in this document are those findingspertinent to the development of the guideline. A morein-depth and complete analysis of the 2003 Survey ofPN Practices will be conducted and reported by theTask Force within the next year. This snapshot ofcurrent practices and expert opinion or consensus pro-vided by both external and internal reviews was com-piled into the current Safe Practices.
Guidelines will be presented in a format similar tothe A.S.P.E.N. Guidelines for the Use of Parenteral andEnteral Nutrition in Adult and Pediatric Patient.3
“Safe Practices for Parenteral Nutrition” is organizedinto seven sections.● Introduction● Ordering parenteral nutrition● Labeling parenteral nutrition formulations● Nutrient requirements● Sterile compounding of parenteral nutrition for-
mulations● Stability and compatibility of parenteral nutrition
formulations● Parenteral nutrition administration
Each section includes an introduction to the practicearea addressed, with examples where clinical data(including patient harm) support the need for practiceguidelines to ensure patient safety; specific practiceguidelines based on consensus of the Task Force mem-bers; summary of areas requiring special consider-ation; and a list of supporting references.
The members of the Task Force for the Revision ofSafe Practices for Parenteral Nutrition are as follows:
Chairman:Jay Mirtallo, MS, RPh, BCNSPThe Ohio State University Medical CenterColumbus, Ohio
Todd Canada, PharmD, BCNSPThe University of Texas, MD Anderson Cancer
CenterHouston, Texas
Deborah Johnson, MS, RNMeriter HospitalMadison, WI
Vanessa Kumpf, PharmD, BCNSPNutrishare, IncElk Grove, CA
Craig Petersen, RD, CNSDUniversity of California Davis Medical CenterSacramento, CA
Gordon Sacks, PharmD, BCNSPUniversity of WisconsinMadison, WI
David Seres, MD, CNSPAlbert Einstein College of MedicineNew York, NY
Peggi Guenter PhD, RN, CNSNA.S.P.E.N.Silver Spring, MD
This document was internally reviewed by theA.S.P.E.N. Standards Committee as well as the Die-tetic, Nursing, Medical, and Pharmacy Practice Sec-tions and approved by the A.S.P.E.N. Board of Direc-tors after external review by individuals and otherassociations of health care professionals. A.S.P.E.N.recognizes that the practice guidelines will have broadramifications in changing clinical practice in manyhealth care settings for pharmacists, physicians,nurses, dietitians, and technical support personnel. Itis hoped that these guidelines will be accepted andused to prevent future patient harm, and will serve asa catalyst for future research.
REFERENCES
1. National Advisory Group on Standards and Practice Guidelinesfor Parenteral Nutrition: Safe practices for parenteral nutritionformulations. JPEN J Parenter Enteral Nutr. 1998;22:49–66.
2. O’Neal BC, Schneider PJ, Pedersen CA, Mirtallo JM. Compli-ance with safe practices for preparing parenteral nutrition for-mulations. Am J Health-Syst Pharm. 2002;59:264–269.
3. A.S.P.E.N. Board of Directors and The Clinical Guidelines TaskForce. Guidelines for the use of parenteral and enteral nutritionin adult and pediatric patients. JPEN J Parenter Enteral Nutr.2002;26 (Suppl):1SA–138SA. (Errata:2002;26:144).
SECTION I: INTRODUCTION
Over the past four decades, parenteral nutrition(PN) has become an important primary (e.g., intestinalfailure) and adjunctive therapy in a variety of diseasestates. Parenteral nutrition refers to all PN formula-tions; total nutrient admixtures (TNA) are PN formu-lations that include intravenous fat emulsions (IVFE);and 2 in 1 formulations are PN formulations that donot include IVFE. PN benefits patients having signifi-cant disruption in gastrointestinal (GI) functionbecoming a lifeline for those who have a permanentloss of the GI tract such as patients with GI fistulas orshort bowel syndrome. New knowledge and technologyhave improved patient selection for PN therapy.Refinement of PN will continue to make it a usefultherapy in the management of patients with dysfunc-tional GI tracts. However, PN formulations are
S42 MIRTALLO ET AL Vol. 28, No. 6

extremely complex admixtures containing 40 or morecomponents including amino acids, dextrose, fat emul-sions, water, electrolytes, trace elements, and vita-mins. Each of these components is a regulated pre-scription drug product. Serious harm and death haveoccurred from improperly prepared and administeredPN formulations. With a potential for significant ben-efit to many patients, its complexity warrants an effec-tive process of ordering, preparation, administrationand monitoring to assure a quality outcome from ther-apy. Early PN programs focused on minimizing thefrequency, severity, and type of complications thatcould result from this therapy. The interdisciplinaryapproach was found to improve efficacy, reduce com-plications, and facilitate efficient, cost-effective PNtherapy. Despite the highly successful use of PN formany years, the following adverse events demonstratethe types of PN errors that can result in serious harmand even death:● Two deaths related to errors in PN compounding led
to a Safety Alert being issued by the U.S. Food andDrug Administration (FDA).1 Autopsy of the patientsinvolved found diffuse microvascular pulmonaryemboli. There were also at least two other cases ofrespiratory distress occurring in patients at the sameinstitution. These patients had received total nutri-ent admixtures (TNA) thought to contain a precipi-tate of calcium phosphate that resulted fromimproper admixture practices in the pharmacy.
● Hospital personnel misinterpreted the dextrose con-tent on the label of a PN formulation used in homecare, which resulted in a pediatric patient’s death.2
The home care label read: “300 mL of 50% dextrose.”The hospital pharmacy interpreted this as a finalconcentration of dextrose 50% (up to twice the con-centration typically used in PN therapy). The patientdied after 2 days of receiving infusion of the incorrectformula.
● Two other fatal incidents have been reported involv-ing pharmacy-compounding operations for pediatricdextrose solutions.3 One infant was overdosed withdextrose when the PN was prepared with aminoacids and two bags of 50% dextrose in place of onebag of 50% dextrose and one bag of sterile water. Theother infant was underdosed with dextrose whilereceiving a 1.75% final concentration of dextrosesolution rather than a 17.5% concentration.
● Another PN formulation was compounded with nodextrose, resulting in irreversible brain damagewhen administered to a neonate.4
● An incident involving the misinterpretation of a labelresulted in iron overload and liver toxicity in a childreceiving PN with iron dextran.5 In this case, the PNlabel read, “iron dextran 1 mL,” the intention beingto use a 1-mg/mL concentration prediluted by thepharmacy. However, the solution containing theundiluted, 50-mg/mL concentration was used in com-pounding and resulted in a 50-fold error in the doseadministered.
● Four children were infected, two of whom died as aresult of receiving contaminated PN admixtures.6
Enterobacter cloacae was cultured from disposable
tubing that was used in the automated compoundingof these PN admixtures.
● A 2-year old child receiving home PN died after anexcessively high level of potassium was identified inthe PN formulation. The most likely explanation pro-vided for the death was human error in the manualpreparation of the PN formulation.7
● Two premature infants developed extreme magne-sium toxicity while receiving PN that was the resultof an automated PN compounder malfunction.8
PN has the potential for serious adverse eventsinvolving many PN components as well as systembreakdowns. Analysis of data reported to the UnitedStates Pharmacopeia Medication Error Reporting Pro-gram (MERP), presented in cooperation with theISMP, and the MEDMARX medication error databasesuggests that PN events are low in frequency but havethe capacity to cause patient harm. Errors were relatedto wrong drug preparation, improper dose, labeling andproblems with automated compounding devices. ThePN components most commonly associated with errorswere electrolytes, concurrent drug therapy, insulin anddextrose.9 It is unclear what proportion of actual PN-associated errors are actually reported to the USP.
The information provided in the ‘Safe Practices forParenteral Nutrition’ document provides guidelinesalong with supporting evidence to foster quality PNtherapy. The intent is for the principles provided in thedocument to become incorporated into healthcare orga-nization practice for the purpose of minimizing the riskof PN. The complexity of this therapy cannot be under-stated. There is good evidence in support of practicesthat favor positive patient outcomes.
REFERENCES
1. Food and Drug Administration. Safety Alert: Hazards of precip-itation associated with parenteral nutrition. Am J Hosp Pharm.1994;51:1427–1428.
2. Carey LC, Haffey M. Incident: Home TPN formula order misin-terpreted after hospital admission. Home Care Highlights. 1995;(spring):7.
3. Cobel MR. Compounding pediatric dextrose solutions. Medica-tion error alert. ASHP Newsletter. 1995;(Aug):3.
4. Gebbart F. Test hyperal solutions? Florida mom says yes. HospPharm Report. 1992;(Feb):35.
5. Iron overdose due to miscommunication of TPN order. Erroralert. Pharmacy Today. 1995;(Sep).
6. Two children die after receiving infected TPN solutions. PharmJ. 1994;(Aug):3. 2.
7. www.hopkinsmedicine.org/Press_releases/2003/12_19_03.html.8. Ali A, Walentik C, Mantych GJ, Sadiq HF, Keenan WJ, Noguchi
A. Iatrogenic acute hypermagnesemia after total parenteralnutrition infusion mimicking septic shock syndrome: two casereports. Pediatrics. 2003;112(1 Pt 1):e70–e72.
9. The U.S. Pharmacopeia Center for the Advancement of PatientSafety medication error reporting programs—MEDMARXSM andthe Medication Errors Reporting Program.
SECTION II: ORDERING PARENTERALNUTRITION
BACKGROUND
As reported in the introduction to this document,life-threatening errors continue to occur in the prepa-ration and delivery of PN admixtures to patients.Many of the errors that occur are related to the order-
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S43
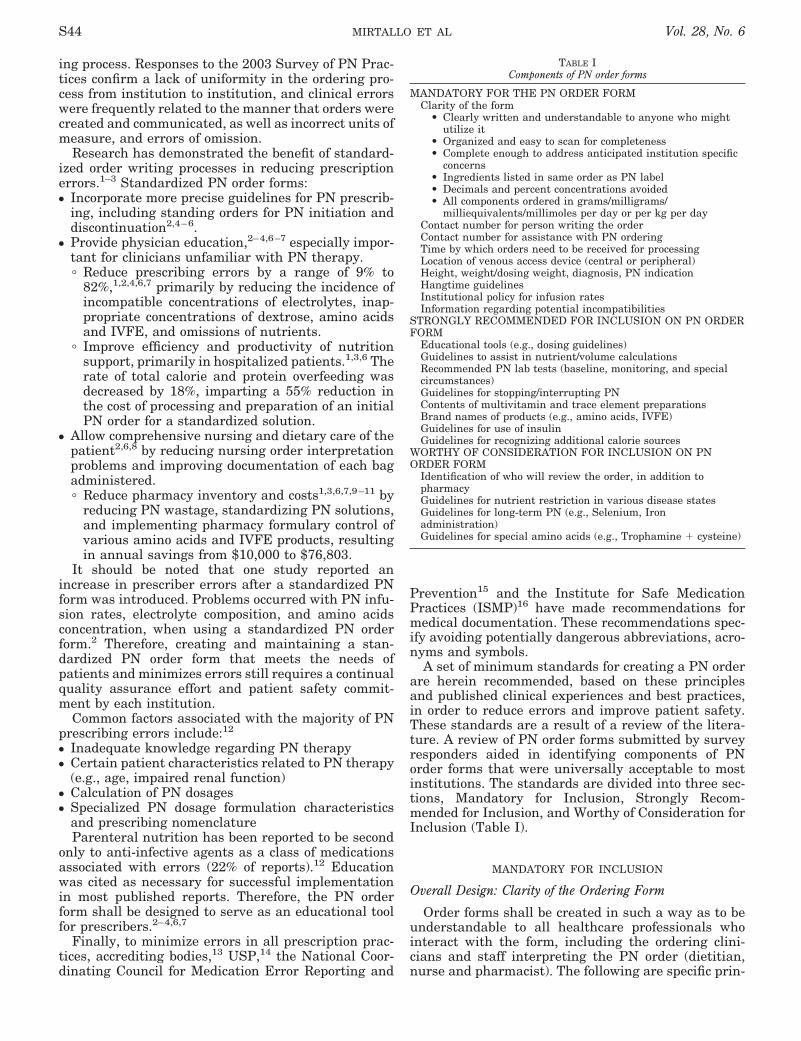
ing process. Responses to the 2003 Survey of PN Prac-tices confirm a lack of uniformity in the ordering pro-cess from institution to institution, and clinical errorswere frequently related to the manner that orders werecreated and communicated, as well as incorrect units ofmeasure, and errors of omission.
Research has demonstrated the benefit of standard-ized order writing processes in reducing prescriptionerrors.1–3 Standardized PN order forms:● Incorporate more precise guidelines for PN prescrib-
ing, including standing orders for PN initiation anddiscontinuation2,4–6.
● Provide physician education,2–4,6–7 especially impor-tant for clinicians unfamiliar with PN therapy.� Reduce prescribing errors by a range of 9% to
82%,1,2,4,6,7 primarily by reducing the incidence ofincompatible concentrations of electrolytes, inap-propriate concentrations of dextrose, amino acidsand IVFE, and omissions of nutrients.
� Improve efficiency and productivity of nutritionsupport, primarily in hospitalized patients.1,3,6 Therate of total calorie and protein overfeeding wasdecreased by 18%, imparting a 55% reduction inthe cost of processing and preparation of an initialPN order for a standardized solution.
● Allow comprehensive nursing and dietary care of thepatient2,6,8 by reducing nursing order interpretationproblems and improving documentation of each bagadministered.� Reduce pharmacy inventory and costs1,3,6,7,9–11 by
reducing PN wastage, standardizing PN solutions,and implementing pharmacy formulary control ofvarious amino acids and IVFE products, resultingin annual savings from $10,000 to $76,803.
It should be noted that one study reported anincrease in prescriber errors after a standardized PNform was introduced. Problems occurred with PN infu-sion rates, electrolyte composition, and amino acidsconcentration, when using a standardized PN orderform.2 Therefore, creating and maintaining a stan-dardized PN order form that meets the needs ofpatients and minimizes errors still requires a continualquality assurance effort and patient safety commit-ment by each institution.
Common factors associated with the majority of PNprescribing errors include:12
● Inadequate knowledge regarding PN therapy● Certain patient characteristics related to PN therapy
(e.g., age, impaired renal function)● Calculation of PN dosages● Specialized PN dosage formulation characteristics
and prescribing nomenclatureParenteral nutrition has been reported to be second
only to anti-infective agents as a class of medicationsassociated with errors (22% of reports).12 Educationwas cited as necessary for successful implementationin most published reports. Therefore, the PN orderform shall be designed to serve as an educational toolfor prescribers.2–4,6,7
Finally, to minimize errors in all prescription prac-tices, accrediting bodies,13 USP,14 the National Coor-dinating Council for Medication Error Reporting and
Prevention15 and the Institute for Safe MedicationPractices (ISMP)16 have made recommendations formedical documentation. These recommendations spec-ify avoiding potentially dangerous abbreviations, acro-nyms and symbols.
A set of minimum standards for creating a PN orderare herein recommended, based on these principlesand published clinical experiences and best practices,in order to reduce errors and improve patient safety.These standards are a result of a review of the litera-ture. A review of PN order forms submitted by surveyresponders aided in identifying components of PNorder forms that were universally acceptable to mostinstitutions. The standards are divided into three sec-tions, Mandatory for Inclusion, Strongly Recom-mended for Inclusion, and Worthy of Consideration forInclusion (Table I).
MANDATORY FOR INCLUSION
Overall Design: Clarity of the Ordering Form
Order forms shall be created in such a way as to beunderstandable to all healthcare professionals whointeract with the form, including the ordering clini-cians and staff interpreting the PN order (dietitian,nurse and pharmacist). The following are specific prin-
TABLE IComponents of PN order forms
MANDATORY FOR THE PN ORDER FORMClarity of the form
• Clearly written and understandable to anyone who mightutilize it
• Organized and easy to scan for completeness• Complete enough to address anticipated institution specific
concerns• Ingredients listed in same order as PN label• Decimals and percent concentrations avoided• All components ordered in grams/milligrams/
milliequivalents/millimoles per day or per kg per dayContact number for person writing the orderContact number for assistance with PN orderingTime by which orders need to be received for processingLocation of venous access device (central or peripheral)Height, weight/dosing weight, diagnosis, PN indicationHangtime guidelinesInstitutional policy for infusion ratesInformation regarding potential incompatibilities
STRONGLY RECOMMENDED FOR INCLUSION ON PN ORDERFORM
Educational tools (e.g., dosing guidelines)Guidelines to assist in nutrient/volume calculationsRecommended PN lab tests (baseline, monitoring, and specialcircumstances)Guidelines for stopping/interrupting PNContents of multivitamin and trace element preparationsBrand names of products (e.g., amino acids, IVFE)Guidelines for use of insulinGuidelines for recognizing additional calorie sources
WORTHY OF CONSIDERATION FOR INCLUSION ON PNORDER FORM
Identification of who will review the order, in addition topharmacyGuidelines for nutrient restriction in various disease statesGuidelines for long-term PN (e.g., Selenium, Ironadministration)Guidelines for special amino acids (e.g., Trophamine � cysteine)
S44 MIRTALLO ET AL Vol. 28, No. 6

ciples recommended to promote order form clarity:Organization. The form shall be organized in a sim-
ple manner. All nutrients in PN, as well as final vol-ume, and infusion duration, shall be clearly identifiedon the form. Final volume shall be the sum of allcomponents of the PN solution, including IVFE in aTNA. The process of entering specific components onthe order should follow an obvious visual pathway,making it easy to scan for completeness.
Institutional policies. The form shall contain enoughinformation to address anticipated institutional poli-cies and procedures. Institution-specific concerns shallbe incorporated into the order form as written instruc-tions. For example, institutional policies may specifythat certain clinical requirements be met, such as spe-cific diagnoses or the completion of baseline laboratorytests, before PN is prepared by the pharmacy.
Continuity. The PN order form shall list all compo-nents in the same format (e.g. amount per day and inthe neonatal or pediatric patient, both amount/day andamount/kg/day) and sequence as the PN label(described in Section III). In keeping with labelingguidelines, electrolytes shall be ordered as the quantityof associated salt to be added to the PN formulation.This will facilitate the verification of the PN contentsagainst the PN order.
Writing the order. The use of a standardized PNorder form will reduce the need for prescriber hand-written items, thus, potentially reducing misinterpre-tation.6 However, adequate space for clear handwritingshall be provided where needed. The use of decimalsand trailing zeroes shall be avoided whenever possible.Orders containing unclear handwriting, or other incor-rect or confusing marks, shall not be compounded untilthe pharmacy has clarified these with the cliniciangenerating the order.
Units of measure. The form shall be designed usingstandard units of measure (e.g. protein in grams,potassium in mEq, and phosphate in mmol) for dosingPN components. Review of sample PN order formssubmitted to the Task Force found doses of macronu-trients expressed in different units on the same orderform (e.g., dextrose in calories, protein in grams and fatas volume of a specific concentration). The use of per-cent concentration in PN orders is not recommended,to avoid confusion.17 Misinterpretation of orders usingpercent concentration has led to patient harm anddeath.18
Specific Components
The following are items considered to be mandatoryfor inclusion on the PN form. They include both data tobe collected on the form, as well as information thatmust be communicated to the clinician ordering thePN. It is assumed that areas for ordering the necessarycomponents of the PN (dextrose, protein, IVFE, elec-trolytes, vitamins, minerals, etc) will be incorporatedinto the form.● For the purpose of clarifying unclear or inappropri-
ate orders, the PN order form shall provide contactinformation for the person writing the PN order.There shall also be a space on the form for the contact
information of institutional resources, such as indi-vidual consultants or a nutrition support service.
● The order form shall specify the time by which PNorders need to be submitted for pharmacy processing.The specified deadline should be chosen by the insti-tution to assure adequate time for a comprehensiveorder review, safe compounding, and scheduleddelivery of the PN formulation. There shall also be astandardized hang time specific to each institution.The preparation and hang time of each PN solutionthat is not refrigerated should not exceed 30 hoursdue to stability concerns.19 Additionally, all compo-nents of the PN order form shall be completed intheir entirety when reordering for an existingpatient. Each institution shall dictate the frequencyof PN reordering (e.g., daily).
● The PN order form shall contain the location of thevenous access device, in order to assure that venousaccess is appropriate for the osmolarity (Table II) ofthe ordered PN formulation. A checkbox on the orderform may be used to denote whether the catheter tiplies in a peripheral or central venous position, andwhether position has been confirmed by x-ray forcentral venous catheters.
● The order form shall contain fields for patient height,dosing weight, and PN indication. Knowledge ofpatient dosing weight is vital in assessing nutrientneeds and identifying nutrient dosing errors, espe-cially in the pediatric population, where total nutri-ent dosing varies dramatically based upon weight.
● Institutional policy for maximum or minimum nutri-ent hang times (and corresponding infusion rates),maximum dextrose infusion rate or IVFE infusionrate, or maximum allowable hang time for separatelyinfused IVFE, if 2-in-1 solutions are utilized, shall beindicated on the order form. Written infusioninstructions for either 24-hour or cycled PN mustcomply with institutional policies.
● The PN order form shall contain a general statementwarning of the potential for PN formulation incom-patibilities. Calcium and phosphorus compatibilityshall be specifically addressed, as it is common forprescribed concentrations of these nutrients toexceed PN solubility limits, which may result inpatient harm or death from calcium phosphate pre-cipitates instigating diffuse microvascular pulmo-nary emboli.20
TABLE IIDetermining the estimated osmolarity of PN formulations*
PN Component mOsmExample, 1 L volume
PN Content mOsm/L
Dextrose 5 per gram 170 g 850Amino Acids 10 per gram 60 g 600Fat Emulsion, 20% 0.71 per gram
(product dependent)20 g 14
Electrolytes 1 per mEq 243 mEq 243Total � 1707
*Based on approximations of the osmolarity of the PN componentsand used as an estimate only.
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S45
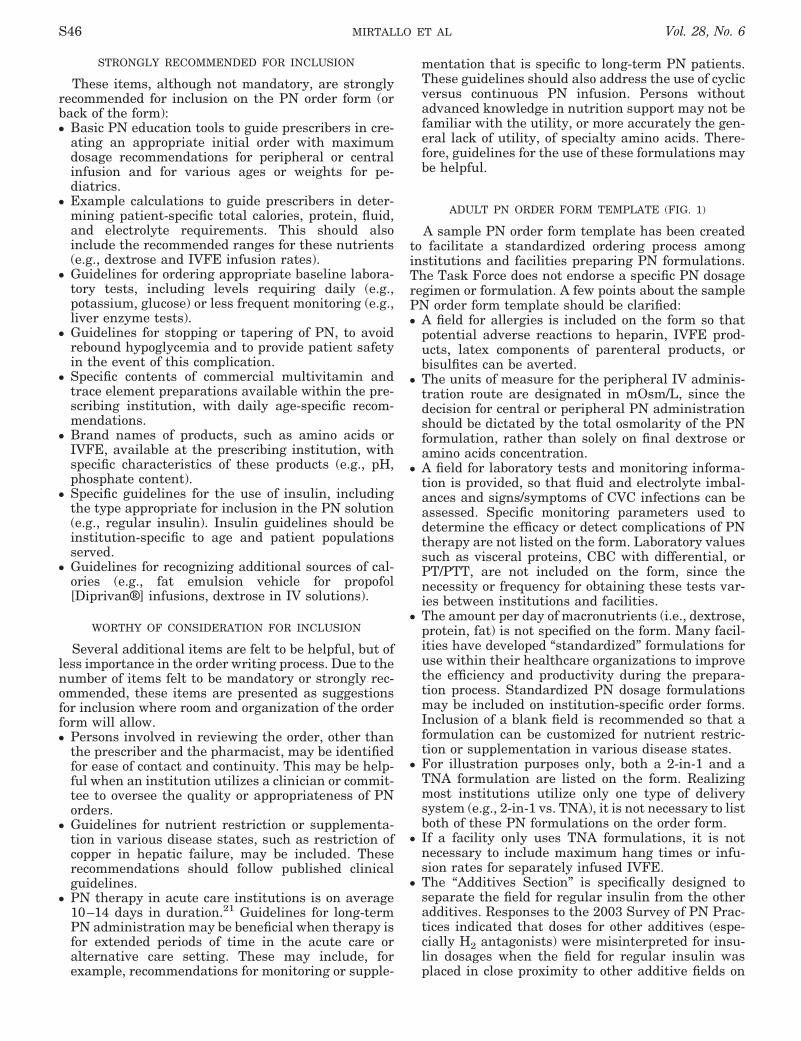
STRONGLY RECOMMENDED FOR INCLUSION
These items, although not mandatory, are stronglyrecommended for inclusion on the PN order form (orback of the form):● Basic PN education tools to guide prescribers in cre-
ating an appropriate initial order with maximumdosage recommendations for peripheral or centralinfusion and for various ages or weights for pe-diatrics.
● Example calculations to guide prescribers in deter-mining patient-specific total calories, protein, fluid,and electrolyte requirements. This should alsoinclude the recommended ranges for these nutrients(e.g., dextrose and IVFE infusion rates).
● Guidelines for ordering appropriate baseline labora-tory tests, including levels requiring daily (e.g.,potassium, glucose) or less frequent monitoring (e.g.,liver enzyme tests).
● Guidelines for stopping or tapering of PN, to avoidrebound hypoglycemia and to provide patient safetyin the event of this complication.
● Specific contents of commercial multivitamin andtrace element preparations available within the pre-scribing institution, with daily age-specific recom-mendations.
● Brand names of products, such as amino acids orIVFE, available at the prescribing institution, withspecific characteristics of these products (e.g., pH,phosphate content).
● Specific guidelines for the use of insulin, includingthe type appropriate for inclusion in the PN solution(e.g., regular insulin). Insulin guidelines should beinstitution-specific to age and patient populationsserved.
● Guidelines for recognizing additional sources of cal-ories (e.g., fat emulsion vehicle for propofol[Diprivan®] infusions, dextrose in IV solutions).
WORTHY OF CONSIDERATION FOR INCLUSION
Several additional items are felt to be helpful, but ofless importance in the order writing process. Due to thenumber of items felt to be mandatory or strongly rec-ommended, these items are presented as suggestionsfor inclusion where room and organization of the orderform will allow.● Persons involved in reviewing the order, other than
the prescriber and the pharmacist, may be identifiedfor ease of contact and continuity. This may be help-ful when an institution utilizes a clinician or commit-tee to oversee the quality or appropriateness of PNorders.
● Guidelines for nutrient restriction or supplementa-tion in various disease states, such as restriction ofcopper in hepatic failure, may be included. Theserecommendations should follow published clinicalguidelines.
● PN therapy in acute care institutions is on average10–14 days in duration.21 Guidelines for long-termPN administration may be beneficial when therapy isfor extended periods of time in the acute care oralternative care setting. These may include, forexample, recommendations for monitoring or supple-
mentation that is specific to long-term PN patients.These guidelines should also address the use of cyclicversus continuous PN infusion. Persons withoutadvanced knowledge in nutrition support may not befamiliar with the utility, or more accurately the gen-eral lack of utility, of specialty amino acids. There-fore, guidelines for the use of these formulations maybe helpful.
ADULT PN ORDER FORM TEMPLATE (FIG. 1)
A sample PN order form template has been createdto facilitate a standardized ordering process amonginstitutions and facilities preparing PN formulations.The Task Force does not endorse a specific PN dosageregimen or formulation. A few points about the samplePN order form template should be clarified:● A field for allergies is included on the form so that
potential adverse reactions to heparin, IVFE prod-ucts, latex components of parenteral products, orbisulfites can be averted.
● The units of measure for the peripheral IV adminis-tration route are designated in mOsm/L, since thedecision for central or peripheral PN administrationshould be dictated by the total osmolarity of the PNformulation, rather than solely on final dextrose oramino acids concentration.
● A field for laboratory tests and monitoring informa-tion is provided, so that fluid and electrolyte imbal-ances and signs/symptoms of CVC infections can beassessed. Specific monitoring parameters used todetermine the efficacy or detect complications of PNtherapy are not listed on the form. Laboratory valuessuch as visceral proteins, CBC with differential, orPT/PTT, are not included on the form, since thenecessity or frequency for obtaining these tests var-ies between institutions and facilities.
● The amount per day of macronutrients (i.e., dextrose,protein, fat) is not specified on the form. Many facil-ities have developed “standardized” formulations foruse within their healthcare organizations to improvethe efficiency and productivity during the prepara-tion process. Standardized PN dosage formulationsmay be included on institution-specific order forms.Inclusion of a blank field is recommended so that aformulation can be customized for nutrient restric-tion or supplementation in various disease states.
● For illustration purposes only, both a 2-in-1 and aTNA formulation are listed on the form. Realizingmost institutions utilize only one type of deliverysystem (e.g., 2-in-1 vs. TNA), it is not necessary to listboth of these PN formulations on the order form.
● If a facility only uses TNA formulations, it is notnecessary to include maximum hang times or infu-sion rates for separately infused IVFE.
● The “Additives Section” is specifically designed toseparate the field for regular insulin from the otheradditives. Responses to the 2003 Survey of PN Prac-tices indicated that doses for other additives (espe-cially H2 antagonists) were misinterpreted for insu-lin dosages when the field for regular insulin wasplaced in close proximity to other additive fields on
S46 MIRTALLO ET AL Vol. 28, No. 6
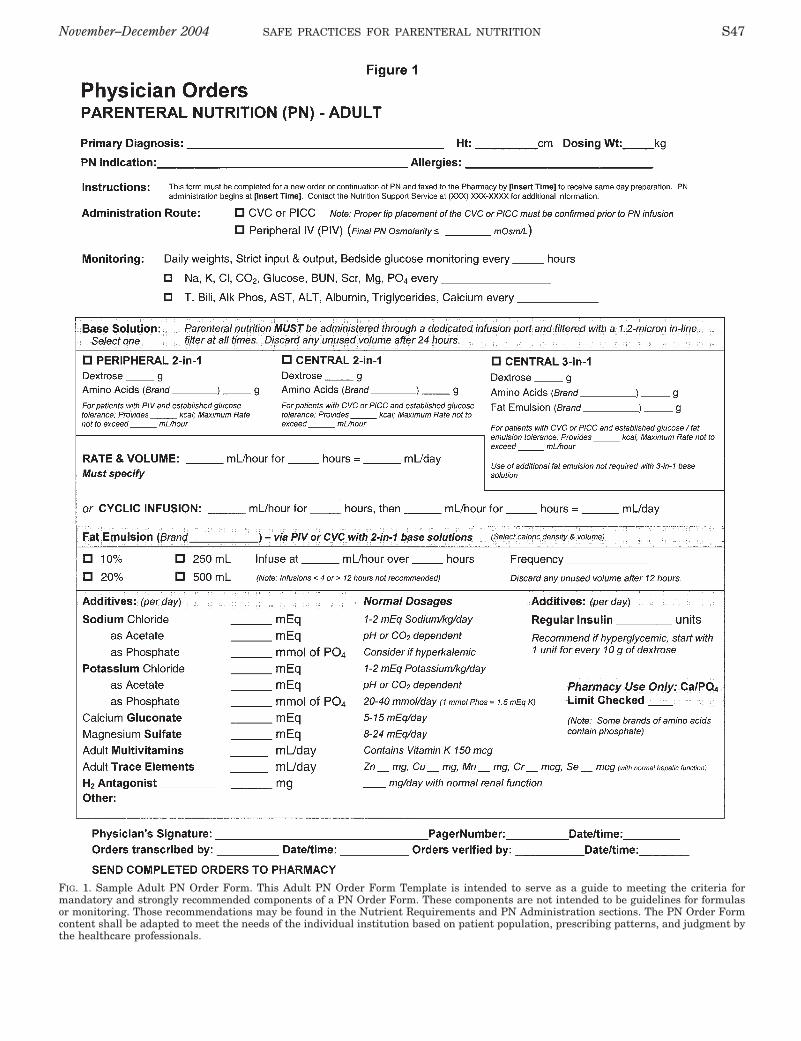
FIG. 1. Sample Adult PN Order Form. This Adult PN Order Form Template is intended to serve as a guide to meeting the criteria formandatory and strongly recommended components of a PN Order Form. These components are not intended to be guidelines for formulasor monitoring. Those recommendations may be found in the Nutrient Requirements and PN Administration sections. The PN Order Formcontent shall be adapted to meet the needs of the individual institution based on patient population, prescribing patterns, and judgment bythe healthcare professionals.
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S47
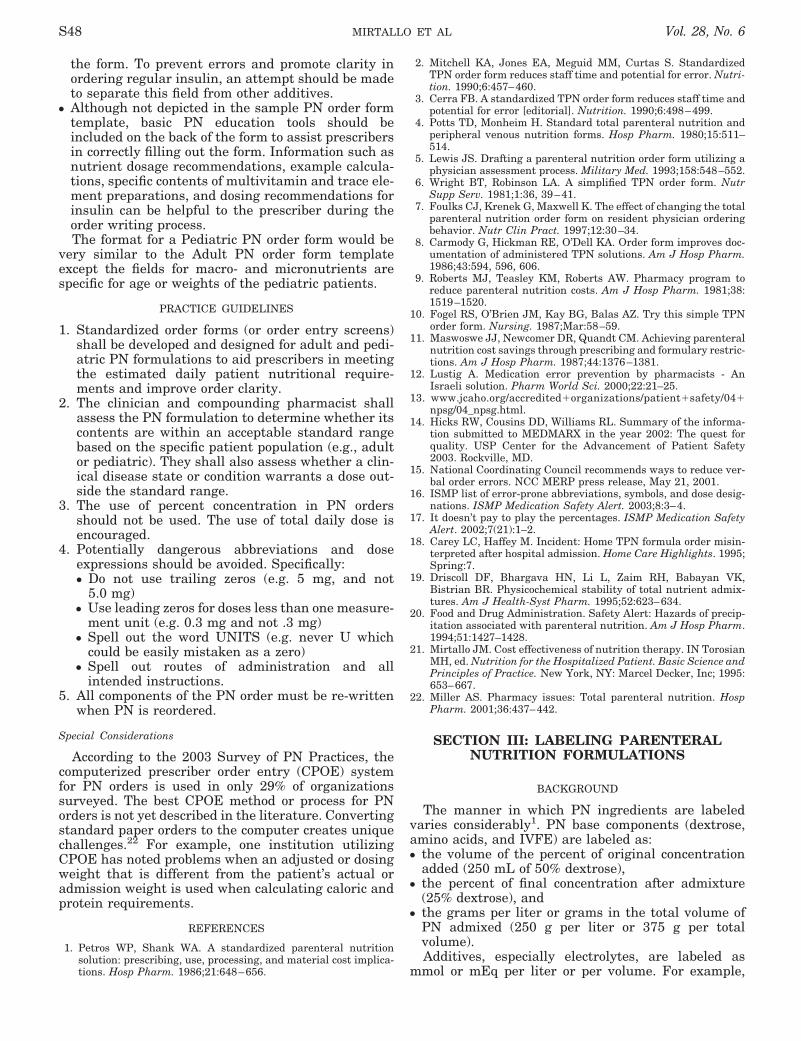
the form. To prevent errors and promote clarity inordering regular insulin, an attempt should be madeto separate this field from other additives.
● Although not depicted in the sample PN order formtemplate, basic PN education tools should beincluded on the back of the form to assist prescribersin correctly filling out the form. Information such asnutrient dosage recommendations, example calcula-tions, specific contents of multivitamin and trace ele-ment preparations, and dosing recommendations forinsulin can be helpful to the prescriber during theorder writing process.The format for a Pediatric PN order form would be
very similar to the Adult PN order form templateexcept the fields for macro- and micronutrients arespecific for age or weights of the pediatric patients.
PRACTICE GUIDELINES
1. Standardized order forms (or order entry screens)shall be developed and designed for adult and pedi-atric PN formulations to aid prescribers in meetingthe estimated daily patient nutritional require-ments and improve order clarity.
2. The clinician and compounding pharmacist shallassess the PN formulation to determine whether itscontents are within an acceptable standard rangebased on the specific patient population (e.g., adultor pediatric). They shall also assess whether a clin-ical disease state or condition warrants a dose out-side the standard range.
3. The use of percent concentration in PN ordersshould not be used. The use of total daily dose isencouraged.
4. Potentially dangerous abbreviations and doseexpressions should be avoided. Specifically:● Do not use trailing zeros (e.g. 5 mg, and not
5.0 mg)● Use leading zeros for doses less than one measure-
ment unit (e.g. 0.3 mg and not .3 mg)● Spell out the word UNITS (e.g. never U which
could be easily mistaken as a zero)● Spell out routes of administration and all
intended instructions.5. All components of the PN order must be re-written
when PN is reordered.
Special Considerations
According to the 2003 Survey of PN Practices, thecomputerized prescriber order entry (CPOE) systemfor PN orders is used in only 29% of organizationssurveyed. The best CPOE method or process for PNorders is not yet described in the literature. Convertingstandard paper orders to the computer creates uniquechallenges.22 For example, one institution utilizingCPOE has noted problems when an adjusted or dosingweight that is different from the patient’s actual oradmission weight is used when calculating caloric andprotein requirements.
REFERENCES
1. Petros WP, Shank WA. A standardized parenteral nutritionsolution: prescribing, use, processing, and material cost implica-tions. Hosp Pharm. 1986;21:648–656.
2. Mitchell KA, Jones EA, Meguid MM, Curtas S. StandardizedTPN order form reduces staff time and potential for error. Nutri-tion. 1990;6:457–460.
3. Cerra FB. A standardized TPN order form reduces staff time andpotential for error [editorial]. Nutrition. 1990;6:498–499.
4. Potts TD, Monheim H. Standard total parenteral nutrition andperipheral venous nutrition forms. Hosp Pharm. 1980;15:511–514.
5. Lewis JS. Drafting a parenteral nutrition order form utilizing aphysician assessment process. Military Med. 1993;158:548–552.
6. Wright BT, Robinson LA. A simplified TPN order form. NutrSupp Serv. 1981;1:36, 39–41.
7. Foulks CJ, Krenek G, Maxwell K. The effect of changing the totalparenteral nutrition order form on resident physician orderingbehavior. Nutr Clin Pract. 1997;12:30–34.
8. Carmody G, Hickman RE, O’Dell KA. Order form improves doc-umentation of administered TPN solutions. Am J Hosp Pharm.1986;43:594, 596, 606.
9. Roberts MJ, Teasley KM, Roberts AW. Pharmacy program toreduce parenteral nutrition costs. Am J Hosp Pharm. 1981;38:1519–1520.
10. Fogel RS, O’Brien JM, Kay BG, Balas AZ. Try this simple TPNorder form. Nursing. 1987;Mar:58–59.
11. Maswoswe JJ, Newcomer DR, Quandt CM. Achieving parenteralnutrition cost savings through prescribing and formulary restric-tions. Am J Hosp Pharm. 1987;44:1376–1381.
12. Lustig A. Medication error prevention by pharmacists - AnIsraeli solution. Pharm World Sci. 2000;22:21–25.
13. www.jcaho.org/accredited�organizations/patient�safety/04�npsg/04_npsg.html.
14. Hicks RW, Cousins DD, Williams RL. Summary of the informa-tion submitted to MEDMARX in the year 2002: The quest forquality. USP Center for the Advancement of Patient Safety2003. Rockville, MD.
15. National Coordinating Council recommends ways to reduce ver-bal order errors. NCC MERP press release, May 21, 2001.
16. ISMP list of error-prone abbreviations, symbols, and dose desig-nations. ISMP Medication Safety Alert. 2003;8:3–4.
17. It doesn’t pay to play the percentages. ISMP Medication SafetyAlert. 2002;7(21):1–2.
18. Carey LC, Haffey M. Incident: Home TPN formula order misin-terpreted after hospital admission. Home Care Highlights. 1995;Spring:7.
19. Driscoll DF, Bhargava HN, Li L, Zaim RH, Babayan VK,Bistrian BR. Physicochemical stability of total nutrient admix-tures. Am J Health-Syst Pharm. 1995;52:623–634.
20. Food and Drug Administration. Safety Alert: Hazards of precip-itation associated with parenteral nutrition. Am J Hosp Pharm.1994;51:1427–1428.
21. Mirtallo JM. Cost effectiveness of nutrition therapy. IN TorosianMH, ed. Nutrition for the Hospitalized Patient. Basic Science andPrinciples of Practice. New York, NY: Marcel Decker, Inc; 1995:653–667.
22. Miller AS. Pharmacy issues: Total parenteral nutrition. HospPharm. 2001;36:437–442.
SECTION III: LABELING PARENTERALNUTRITION FORMULATIONS
BACKGROUND
The manner in which PN ingredients are labeledvaries considerably1. PN base components (dextrose,amino acids, and IVFE) are labeled as:● the volume of the percent of original concentration
added (250 mL of 50% dextrose),● the percent of final concentration after admixture
(25% dextrose), and● the grams per liter or grams in the total volume of
PN admixed (250 g per liter or 375 g per totalvolume).Additives, especially electrolytes, are labeled as
mmol or mEq per liter or per volume. For example,
S48 MIRTALLO ET AL Vol. 28, No. 6

sodium chloride (NaCl) in a dose of 80 mEq/L admixedin a PN with a volume of 2 liters may be labeled asfollows:● NaCl 80 mEq/L● NaCl 160 mEq per total volume● Na 80 mEq/L, Cl 80 mEq/L● Na 160 mEq and Cl 160 mEq per total volume.
This lack of standardization causes a great deal ofconfusion when patients are transferred betweenhealthcare environments. As such, an essential compo-nent of a patient transfer between healthcare environ-ments is a pharmacist-to-pharmacist interaction toresolve potential problems with transfer of the pre-scription. Misinterpretation of a PN label that led to apatient death2 exemplifies what may occur if this inter-action does not occur. To avoid misinterpretation, thelabels for PN formulations should be standardized. AllPN labels in any health care environment shall expressclearly and accurately what the patient is receiving atany time.
Each method of labeling has distinct advantages anddisadvantages. The use of the percent of original dex-trose or amino acid concentration is specific for theproduct used by the pharmacy in compounding the PNformulation. However, interpretation of this labelrequires knowledge of pharmaceutical calculations inorder to determine the nutrient value of the PN formu-lation. This involves training professionals in severalhealth care disciplines to determine the nutrient valueof the PN admixture being administered. Using thepercent of final concentration of dextrose, amino acids,or IVFE still requires calculations to determine thecaloric value or dose being administered, but it is tra-ditionally the most accepted type of label because it isconsistent with the label of the original commercialproducts as shipped from the manufacturer. To mini-mize calculation errors and provide a label more con-sistent with dispensing a PN formulation as a nutrient,some programs have used grams of base componentsper liter. This simplifies the conversion of the nutrientsto calorie and gram doses being provided, but still mustbe converted to daily doses. This label also supportsthose programs that only compound PN formulationsin liter quantities so that prescriptions may be writtenas quantity per liter and thus consistent with the addi-tive as it appears on the label.
Finally, grams per total volume, with use of a24-hour nutrient infusion system is most consistentwith that of a nutrient label, requiring the least num-ber of calculations to determine the calorie or gramdose per day. It also supports the most cost-effectivesystem of PN compounding and delivery, which is the24-hour nutrient infusion system.3 This system hasbeen determined to decrease PN wastage and to reducepersonnel time in compounding and administering PN.Conceptually, this system is successful when acuteelectrolyte disorders are managed separately from thePN, until the time that electrolyte changes in the PNgo into effect. This system also requires the use ofautomated compounding devices, which have beenshown to be more accurate and faster than gravity-fillPN admixture systems.
PN LABEL TEMPLATE
The sample PN label templates provide a format tostandardize labels for adult, pediatric and neonatalpatients. A supplemental label template for IVFE isalso provided for those instances when IVFEs areadministered separate from the PN admixture. Due tothe complex nature of the label, there are severalpoints that should be clarified:● The amount per day is the only column required on
the adult label, but some programs accustomed toamounts per liter may supplement the label by add-ing a second column reflecting quantity per liter inparenthesis. The components are labeled as amountper day to facilitate review of the order for appropri-ate nutrient doses. However, certain additivesexpressed as quantity per liter in parenthesis on thePN label template, may be useful to the clinician indetermining whether the PN may be infused viaperipheral or central vein. It is also useful to thepharmacist in determining electrolyte compatibilitysince these are reported by concentration rather thanamount. Those familiar with ordering PN electro-lytes (similar to other intravenous fluids) as mEq/L,will be able to interpret the mEq/L electrolyte con-tent easier if provided in this format on the PN label.Finally, many programs order additives asquantity/liter. Labeling as such allows for the finalcheck of the PN by the nurse versus the physician’sorder, prior to its administration. This final check toconfirm that the PN content is the same as the phy-sician’s order is an essential component of the PNsystem. In the neonatal and pediatric patient, it iscommon to order PN components in amount/kg.Therefore, the PN label for these patients shall alsoexpress components as amount/kg/day, in addition toamount/day. The label can be further supplementedby an additional column expressing components asamount/liter or amount/100 ml in parenthesis, forthose who are accustomed to ordering in this format.Care should be taken in developing a label that isclear and concise and of a size that fits neatly on thePN admixture. Accordingly, some may choose to dis-pense the PN with a supplemental form providingthese optional details that may also be used for doc-umenting PN administration in the patient’s chart.
● The PN label specifies the route of administration.● The administration date and time and beyond-use
date and time are expressed clearly on the label. Theadministration date and time, as the term denotes, isthe date and time the PN is scheduled to be admin-istered to the patient. This may be the same day thatit was compounded and is different from the date andtime of admixture, which should be included on thecompounding worksheet but is not necessary on thelabel.
● The dosing weight is provided so that anyone evalu-ating the contents of the label may determine if thedoses of nutrients are appropriate. Dosing weightrefers to the weight used in calculating nutrient doses.
● The inorganic phosphorus content is provided as both
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S49
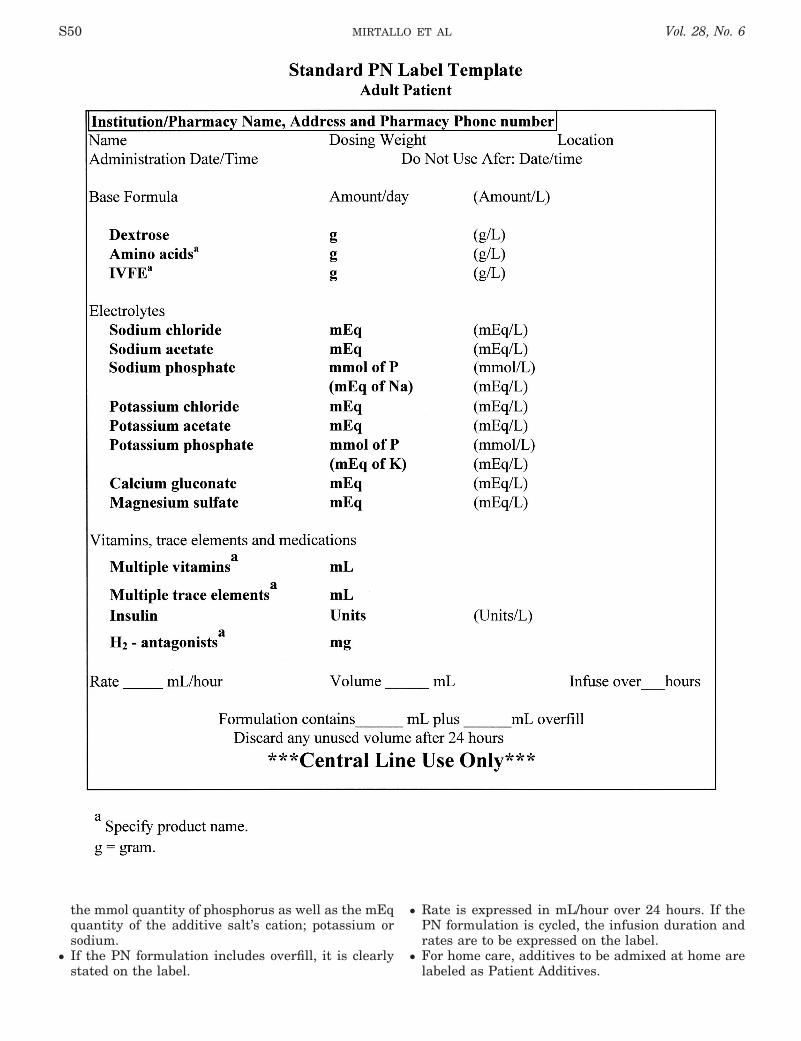
the mmol quantity of phosphorus as well as the mEqquantity of the additive salt’s cation; potassium orsodium.
● If the PN formulation includes overfill, it is clearlystated on the label.
● Rate is expressed in mL/hour over 24 hours. If thePN formulation is cycled, the infusion duration andrates are to be expressed on the label.
● For home care, additives to be admixed at home arelabeled as Patient Additives.
S50 MIRTALLO ET AL Vol. 28, No. 6
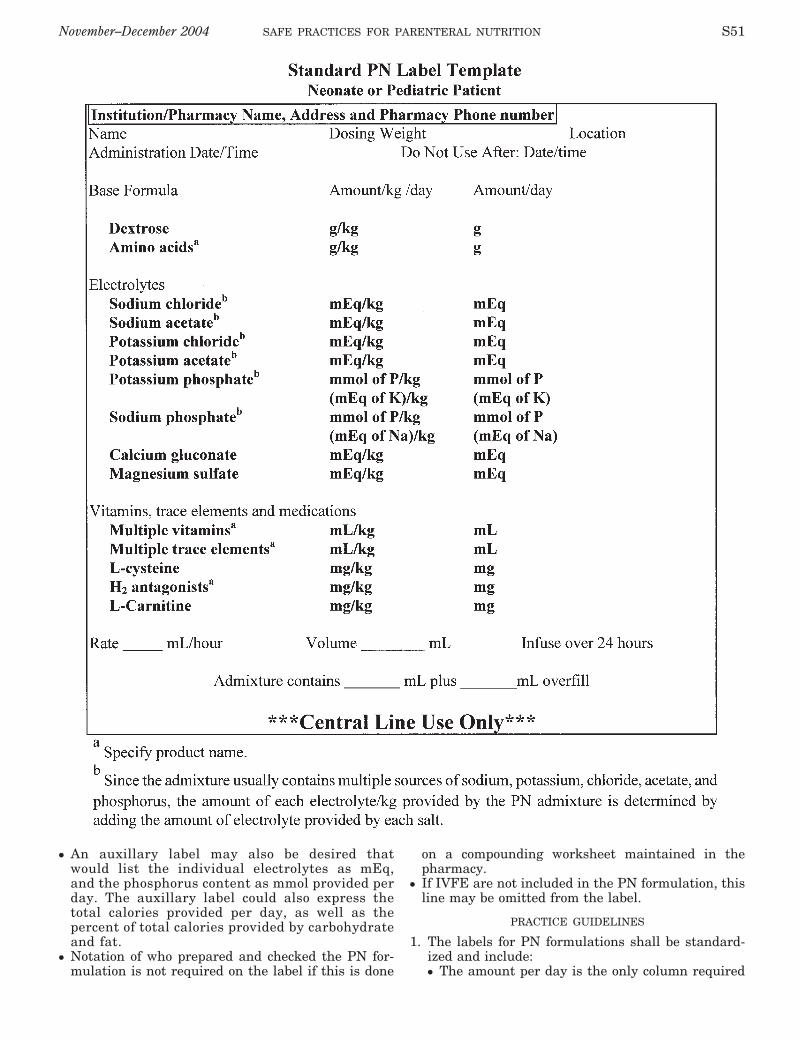
● An auxillary label may also be desired thatwould list the individual electrolytes as mEq,and the phosphorus content as mmol provided perday. The auxillary label could also express thetotal calories provided per day, as well as thepercent of total calories provided by carbohydrateand fat.
● Notation of who prepared and checked the PN for-mulation is not required on the label if this is done
on a compounding worksheet maintained in thepharmacy.
● If IVFE are not included in the PN formulation, thisline may be omitted from the label.
PRACTICE GUIDELINES
1. The labels for PN formulations shall be standard-ized and include:● The amount per day is the only column required
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S51
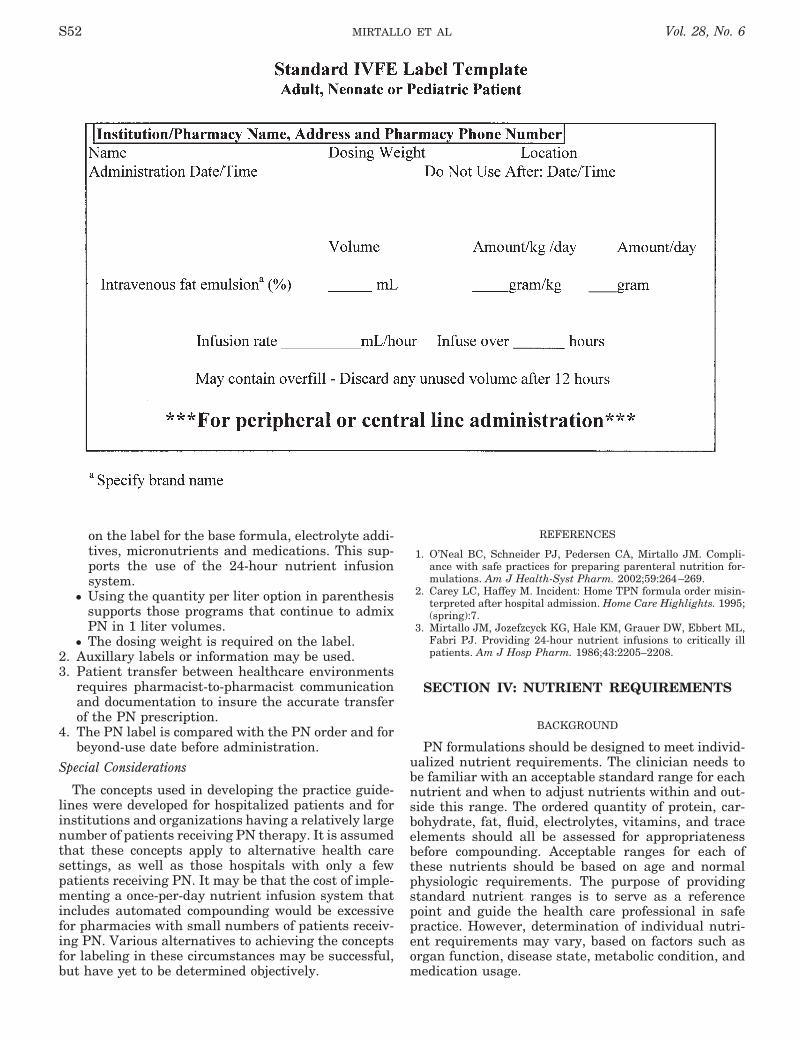
on the label for the base formula, electrolyte addi-tives, micronutrients and medications. This sup-ports the use of the 24-hour nutrient infusionsystem.
● Using the quantity per liter option in parenthesissupports those programs that continue to admixPN in 1 liter volumes.
● The dosing weight is required on the label.2. Auxillary labels or information may be used.3. Patient transfer between healthcare environments
requires pharmacist-to-pharmacist communicationand documentation to insure the accurate transferof the PN prescription.
4. The PN label is compared with the PN order and forbeyond-use date before administration.
Special Considerations
The concepts used in developing the practice guide-lines were developed for hospitalized patients and forinstitutions and organizations having a relatively largenumber of patients receiving PN therapy. It is assumedthat these concepts apply to alternative health caresettings, as well as those hospitals with only a fewpatients receiving PN. It may be that the cost of imple-menting a once-per-day nutrient infusion system thatincludes automated compounding would be excessivefor pharmacies with small numbers of patients receiv-ing PN. Various alternatives to achieving the conceptsfor labeling in these circumstances may be successful,but have yet to be determined objectively.
REFERENCES
1. O’Neal BC, Schneider PJ, Pedersen CA, Mirtallo JM. Compli-ance with safe practices for preparing parenteral nutrition for-mulations. Am J Health-Syst Pharm. 2002;59:264–269.
2. Carey LC, Haffey M. Incident: Home TPN formula order misin-terpreted after hospital admission. Home Care Highlights. 1995;(spring):7.
3. Mirtallo JM, Jozefzcyck KG, Hale KM, Grauer DW, Ebbert ML,Fabri PJ. Providing 24-hour nutrient infusions to critically illpatients. Am J Hosp Pharm. 1986;43:2205–2208.
SECTION IV: NUTRIENT REQUIREMENTS
BACKGROUND
PN formulations should be designed to meet individ-ualized nutrient requirements. The clinician needs tobe familiar with an acceptable standard range for eachnutrient and when to adjust nutrients within and out-side this range. The ordered quantity of protein, car-bohydrate, fat, fluid, electrolytes, vitamins, and traceelements should all be assessed for appropriatenessbefore compounding. Acceptable ranges for each ofthese nutrients should be based on age and normalphysiologic requirements. The purpose of providingstandard nutrient ranges is to serve as a referencepoint and guide the health care professional in safepractice. However, determination of individual nutri-ent requirements may vary, based on factors such asorgan function, disease state, metabolic condition, andmedication usage.
S52 MIRTALLO ET AL Vol. 28, No. 6

NUTRIENT REQUIREMENTS: ADULTS
General guidelines for protein, calorie, and fluidrequirements in adult patients are provided in Table I.A dosing weight shall be determined for each patient.Various methods for adjusting the body weight of obesepatients have been suggested, but none have beenclearly validated.1,2 Assessment of energy expenditurein obese patients can be problematic. Indirect calorim-etry may be required to improve the accuracy of energyrequirement estimations, due to limitations of predic-tive equations in obese patients.3,4
Protein requirements have been estimated based onmetabolic demand. Restriction of protein is seldomrequired in patients with renal or hepatic disease.5 Inpatients receiving renal replacement therapy, proteinmay need to be supplemented. In patients with liverdisease, protein restriction should be implemented forthe acute management of overt hepatic encephalopa-thy only when other treatment modalities have failed.Protein restriction is not indicated in the managementof chronic hepatic disease.
The standard distribution of nonprotein calories is70–85% as carbohydrate and 15–30% as fat. This dis-tribution may be adjusted based on tolerance; however,there is limited clinical benefit when fat contentexceeds 30% of nonprotein calories.6 Further methodsto estimate dosing are based on body weight. In adultpatients, it is recommended that the fat content of thePN formulation not exceed 2.5 g/kg/day and carbohy-drate content not exceed 7 g/kg/day.
Although rare in recent years, essential fatty aciddeficiency (EFAD) may still occur in the contemporaryperiod of specialized nutrition support. Failure to pro-vide at least 2% to 4% of the total caloric intake aslinoleic acid and 0.25% to 0.5% of total caloric intake asalpha linolenic acid may lead to a deficiency of thesetwo essential fatty acids. Manifestations of this syn-drome can include alterations in platelet function, hairloss, poor wound healing, and dry, scaly skin unrespon-sive to water miscible creams. The time in which EFADmay develop during administration of fat-free PN isvariable, based upon the underlying nutritional status,disease state, and age of the patient. In general, themajority of hospitalized adults who receive no dietaryfat, develop biochemical evidence of EFAD after 4weeks of fat-free PN. Hypocaloric feeding may providesome protection against development of EFAD whilereceiving fat-free PN. This is presumed to be secondaryto the liberalization of essential fatty acids (EFAs)from endogenous fat stores into the circulation.Although 2 weeks of a high-protein, hypocaloric fat-
free PN regimen has been shown to maintain plasmalinoleic acid levels in postsurgical patients,7 clinicalsigns of EFAD have been detected in obese patientswho received no exogenous EFAs for 20 days.8 Studiesof patients receiving home PN have shown that bio-chemical evidence of EFAD syndrome may developafter several months of not receiving IVFE.9 Theamount of fat taken by mouth and the efficiency ofabsorption were identified as factors influencing theneed for the continued provision of IVFE. In determin-ing the adequacy of EFA provision, it is important torecognize the varying EFA content of various IVFEsources. For example, commercially available IVFE inthe United States contain approximately 55–60% oftotal calories as linoleic acid and 3–4% of total caloriesas alpha linolenic acid. Structured lipid products avail-able in Europe contain significantly lower proportionsof EFAs, owing to the substitution of long-chain EFAsby medium-chain fatty acids. Topical EFA applicationhas been shown to be effective in preventing EFAD insome patients but it has demonstrated poor efficacywhen used to treat an already existing EFAD.10,11
Standard ranges for parenteral electrolytes assumenormal organ function and normal losses (Table II).Sodium and potassium requirements for a givenpatient are highly variable and generally not limitedby compatibility restraints; however, large quantitiesof these cations may destabilize IVFE. In general,sodium and potassium requirements in the PN formu-lation are 1–2 mEq/kg/day, but should be customized tomeet individual patient needs. Restrictions of potas-sium, phosphate, or magnesium may be required inpatients with renal disease due to impaired excretion.Conversely, requirements of these electrolytes may beincreased due to excessive losses, intracellular shifts,or increased metabolic demands. As discussed in sec-tion VI, the parenteral supplementation of phosphate,magnesium, and calcium in the PN formulation is lim-ited by physical compatibility. Some commerciallyavailable amino acid injection products contain phos-phorus, the content of which shall also be considered indetermining compatibility. Chloride and acetate con-tent should be adjusted to maintain acid-base balance.In general, acid-base balance can be maintained byusing approximately equal amounts of chloride andacetate, but may require adjustment based on the clin-ical situation. Amino acid solutions themselves containvarious amounts of chloride and acetate, depending onthe individual product, for buffering purposes.12 For
TABLE IIDaily electrolyte additions to adult PN formulations*
Electrolyte Standard RequirementCalcium 10–15 mEqMagnesium 8–20 mEqPhosphorus 20–40 mmolSodium 1–2 mEq/kgPotassium 1–2 mEq/kgAcetate As needed to maintain acid-base balanceChloride As needed to maintain acid-base balance
*Standard intake ranges based on generally healthy people withnormal losses.
TABLE IDaily protein & calorie requirements for the adult
ProteinMaintenance 0.8–1 g/kgCatabolic patients 1.2–2 g/kgChronic renal failure
(renal replacement therapy) 1.2–1.5 g/kgAcute renal failure � catabolic 1.5–1.8 g/kg
EnergyTotal calories 20–30 kcal/kg
Fluid 30–40 mL/kg
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S53

this reason, it is necessary to state the specific aminoacid product name used in compounding on the PNlabel in order to account for its electrolyte content.However, it is not recommended that the electrolytecomponents of the amino acid solution be listed on thePN label with the electrolyte additives as this may leadto confusion.
All patients receiving PN should receive a parenteralvitamin preparation daily. Available commercial prod-ucts for adults contain 13 or 12 known vitamins (i.e.with or without vitamin K). In April 2000, the FDAamended requirements for marketing of an “effective”adult parenteral vitamin formulation and recom-mended changes to the 12-vitamin formulation thathas been available for over 20 years.13 The require-ments for increased dosages of vitamins B1, B6, C, andfolic acid as well as addition of vitamin K are basedupon the recommendations from a 1985 workshopsponsored jointly by the American Medical Associa-tion’s (AMA) Division of Personal and Public HealthPolicy and FDA’s Division of Metabolic and EndocrineDrug Products. Specific modifications of the previousformulation include increasing the provision of ascor-bic acid (vitamin C) from 100 mg/day to 200 mg/day,pyridoxine (vitamin B6) from 4 mg/day to 6 mg/day,thiamin (vitamin B1) from 3 mg/day to 6 mg/day, folicacid from 400 mcg/day to 600 mcg/day, and addition ofphylloquinone (vitamin K) 150 mcg/day (Table III).When using the 12-vitamin formulation, vitamin K canbe given individually as a daily dose (0.5–1 mg/d) or aweekly dose (5–10 mg one time per week). Patients whoare to receive the anticoagulant warfarin should bemonitored more closely when receiving vitamin K toassure the appropriate level of anticoagulation is main-tained. It is reasonable to supplement the PN withthiamin (25–50 mg/d) in PN patients who have a his-tory of alcohol abuse, especially when they did notreceive thiamin at hospital admission, or in times ofparenteral vitamin shortages (common in the U.S. inthe 1990s). The United States has been plagued withtwo periods of short supply of parenteral vitamin prod-ucts in the 1990s. This has resulted in vitamin defi-ciencies in patients receiving PN without parenteralvitamins. Several recommendations emanated fromA.S.P.E.N. following the latest parenteral vitamin
shortage: (1) use oral vitamins when possible, espe-cially liquid vitamins of defined content via feedingtubes, (2) restrict the use of vitamin products in PNduring periods of short supply, such as one infusionthree times per week, (3) administer thiamin, ascorbicacid, niacin, pyridoxine, and folic acid daily as individ-ual entities in the PN during periods of short supply,(4) administer vitamin B12 at least once per monthduring periods of short supply.
Guidelines for parenteral trace element require-ments in adults are provided in Table IV.14,15 Theguidelines should be considered approximations, and itshould be recognized that variations among individualpatients may exist. Reductions in manganese and cop-per dosing should be considered in patients with hepa-tobiliary disease due to impaired excretion. In addi-tion, many of the components of the PN formulationhave been shown to be contaminated with trace ele-ments such as zinc, copper, manganese, chromium,selenium, and aluminum.16 Therefore, patients receiv-ing long-term use of PN therapy are at risk of traceelement toxicity and serum monitoring is necessary.
Iron is not routinely recommended in patientsreceiving PN therapy and is not a component of currentinjectable multiple trace element preparations.17 Par-enteral supplementation of iron should be limited toconditions of iron deficiency when the oral route isineffective or not tolerated. In patients with iron defi-ciency anemia, therapeutic (replacement) doses of ironmay be estimated based on weight and hemoglobinconcentration. Provision of maintenance iron therapyis generally not required but has been used in patientsreceiving long-term PN. In the absence of blood loss, aparenteral iron dose of 25 to 50 mg once monthly isestimated to meet maintenance requirements. How-ever, it is important to monitor iron status on a routinebasis (e.g., serum ferritin every 1–3 months) wheneverproviding ongoing doses of iron in order to minimizethe risk of iron overload. Iron dextran has been addedto nonIVFE-containing PN formulations, but requirescaution due to compatibility limitations. It shall not beadded to TNA because it can destabilize the IVFE andresult in the formation of large oil droplets that may beharmful if infused (see compatibility section). Ironsucrose and sodium ferric gluconate provide therapeu-tic options for the parenteral supplementation of iron,but compatibility data with PN formulations is notavailable.
TABLE IIIDaily requirements for adult parenteral vitamins*
Vitamin Requirement
Thiamin (B1) 6 mgRiboflavin (B2) 3.6 mgNiacin (B3) 40 mgFolic acid 600 mcgPantothenic acid 15 mgPyridoxine (B6) 6 mgCyanocobalamin (B12) 5 mcgBiotin 60 mcgAscorbic Acid (C) 200 mgVitamin A 3300 IUVitamin D 200 IUVitamin E 10 IUVitamin K 150 mcg
*FDA requirements for marketing an effective adult parenteral vita-min product.13
TABLE IVDaily trace element supplementation to adult PN formulations*
Trace Element Standard Intake14,15
Chromium 10–15 mcgCopper 0.3–0.5 mgIron Not routinely addedManganese 60–100 mcg†Selenium 20–60 mcgZinc 2.5–5 mg
*Standard intake ranges based on generally healthy people withnormal losses.†The contamination level in various components of the PN formula-tion can significantly contribute to total intake. Serum concentra-tions should be monitored with long-term use.
S54 MIRTALLO ET AL Vol. 28, No. 6

NUTRIENT REQUIREMENTS: PEDIATRICS
Standard nutrient ranges for infants and childrenreceiving PN have been established. Rapidly changingorgan function, metabolic immaturity, and normal butrapid weight gain, particularly in neonates andinfants, result in age-related descriptors of nutrientneed. Therefore, each table characterizes ranges forneonates, infants, children, and adolescents (Tables Vthrough X). As can be readily appreciated, require-ments for fluids,18 protein, and energy are substan-tially higher on a unit-of-weight basis for children thanfor adults. Careful monitoring of growth is necessary,as a component of assessing adequacy of nutrient pro-vision. Above 18 years of age, estimated nutritionalrequirements should be established using nutrientranges suggested for the adult population.
Protein restriction in certain disease states such ashepatic and renal failure should be done with cautionand in consideration of the need for adequate protein tosupport growth in the pediatric population. Addition-ally, protein losses during dialysis need to be consid-ered and appropriately replaced.
Manufacturers of neonatal/infant amino acid for-mulations recommend the addition of L-cysteinehydrochloride to the 2-in-1 PN formulation justprior to administration. A commonly recommendeddose is 40 mg L-cysteine hydrochloride per gram ofamino acids.19 Current practice suggests supple-mentation with L-cysteine hydrochloride for thefirst year of life, although practice varies widely.Addition of L-cysteine hydrochloride to the PN for-mulation reduces the pH, thereby improving cal-cium and phosphorus solubility.20 It has also beenshown to normalize plasma taurine levels.21
The distribution of PN nonprotein calories for pedi-atric patients does not vary significantly from that forthe adult receiving PN; however, it is worth noting thatthe typical enteral diet of the neonate or infant derivesapproximately 50% of nonprotein calories from fat.Therefore, a PN formulation appears less physiologi-cally similar to standard enteral feedings in the neo-nate or infant than in the older child and adult.
There is evidence that the 20% IVFE is preferable tothe 10% product, especially for use in neonates and
infants. In addition to its greater caloric content perunit volume, the lower content of surface active agents(egg phosphatides) per gram of fat results in morenormal concentrations of components of circulatinglipoproteins, especially low density lipoproteins.22 Inthe very low birth weight infant, the use of the 20%IVFE does require accurate and low flow pump deliv-ery systems. In general, 3 g/kg/day is the accepted limitfor IVFE administration in the small for gestationalage neonates and preterm neonates less than 32 weeksgestational age.23,24 Concerns regarding EFAD areaddressed in the adult section of nutrient re-quirements.
A limited endogenous store of fatty acids in neonatesand infants versus adults contribute to the discrepancyin time in which EFAD syndrome may occur. Neonateshave been reported to develop biochemical signs ofEFAD as early as the second day of life and up to 2weeks after fat-free PN.
Standard ranges for electrolytes, vitamins, and traceelements for infants and children with normal organfunction are provided in Tables VIII through X. Cal-cium and phosphorous requirements of the neonateand infant are substantially different from those of theolder child and are dramatically different from theadult requirements (Table VIII). These differences inneeds are reflected in the composition of neonatal andinfant formulas and human milk. When one attemptsto meet these increased requirements in pediatric PNformulations, problems can arise because of incompat-ibility of calcium and phosphate salts. In a child weigh-ing more than 50 kg, adult electrolyte dosage guide-lines should generally be used.
Guidelines for vitamin and trace element additionsto PN solutions for pediatric patients up to age 11 havebeen published (Tables IX and X).25 Adult multivita-mins should be used for a child who weighs more than40 kg or is greater than 11 years of age. Like adults,the guidelines should be considered approximations ofneed, with individual patient variation to be expected.Alteration of trace element dosage may be required incases of hepatic or renal dysfunction. The long-termuse of multiple trace element products at recom-mended doses has been associated with excessiveserum concentrations of chromium.26 The ratio of traceelements in commercially available pediatric multipletrace element products results in excessive intake ofmanganese if recommended doses of zinc are given. Itis clear that micronutrient requirements for childrenreceiving PN is a fertile area for research and an areain which further commercial product development isrequired. In general, the recommendations for the useof iron in pediatric PN are consistent with those pre-
TABLE VDaily fluid requirements for pediatric patients18
Body weight Amount
�1500 g 130–150 mL/kg1500–2000 g 110–130 mL/kg2–10 kg 100 mL/kg�10–20 kg 1000 mL for 10 kg � 50 mL/kg for each kg �10�20 kg 1500 mL for 20 kg � 20 mL/kg for each kg �20
TABLE VIDaily protein requirements (g/kg) for pediatric patients*
Preterm neonates 3–4Infants (1–12 months) 2–3Children (�10 kg or 1–10 yrs) 1–2Adolescents (11–17 yrs) 0.8–1.5
*Assumes normal age-related organ function.
TABLE VIIDaily energy requirements (total kcal/kg) for pediatric patients
Preterm neonate 90–120�6 months 85–1056–12 months 80–1001–7 yr 75–907–12 yr 50–75�12–18 yr 30–50
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S55

sented previously for adults. However, total iron needscan be dramatically lower in the pediatric patient, com-pared to adults. This necessitates vigilance, regardingthe iron dose administered. The concentration of someparenteral iron preparations can result in life-threat-ening doses, even with the use of �1 mL of thesecommercial iron preparations.
Aluminum contamination. Since the late 1970s, evi-dence has been accumulating to show that small vol-ume parenteral products, large volume parenteralproducts and pharmacy bulk packages used in com-pounding PN formulations are largely contaminatedwith aluminum.27 Contamination occurs primarilyfrom the introduction of raw materials during the man-ufacturing process, with the aluminum-contaminatedproduct sources of primary concern being calcium andphosphate salts, heparin, and albumin. Variable levelsof contamination have also been noted with some traceelement and vitamin products. Infants and childrenare extremely vulnerable to aluminum toxicity due toimmature renal function and the likelihood for long-term PN. Alterations in bone formation, mineraliza-tion, parathyroid hormone secretion, and urinary cal-cium excretion have been attributed to aluminumtoxicity in long-term PN patients or patients with renalimpairment.28 Although they may not be receiving PN,thermal injury patients are at an increased risk foraluminum toxicity from the large quantities of humanalbumin and calcium gluconate they receive in thetreatment of their burn injuries.29–31 The FDArecently mandated that manufacturers of productsused in compounding PN shall measure the aluminumcontent of their products and disclose it on the label byJuly 2004.32,33 Large volume parenterals (i.e., aminoacid solutions, concentrated dextrose solutions, IVFEand sterile water for injection) have a maximum limitof 25 mcg/L of aluminum. Small volume parenterals
(i.e., electrolyte salts) and pharmacy bulk packages(i.e., parenteral multivitamins, trace element solu-tions) must be labeled with the maximum level of alu-minum in the product at expiry. The FDA identified 5mcg/kg/day as the maximum amount of aluminum thatcan be safely tolerated and amounts exceeding thislimit may be associated with central nervous system orbone toxicity. The intent of the FDA ruling is to edu-cate health care practitioners about aluminum expo-sure and facilitate the administration of low-aluminumparenteral solutions to patients in high-risk groups.
PRACTICE GUIDELINES
1. Determination of protein, calorie, fluid, electrolyte,vitamin, and trace element components of a PNformulation should be based on standard nutrientrequirements. The dose of each nutrient shouldfall within the accepted age-based standardrange except when warranted by specific clinicalsituations.
2. IVFE in a dose sufficient to prevent EFAD should beprovided to adult and pediatric patients who areNPO. Adults who fail to receive EFAs for 20 daysare at risk for development of EFAD. In the absenceof EFAs, children can develop EFAD over a shorterperiod of time, with neonates at risk of EFAD within2 days of initiating lipid-free PN.
3. All patients receiving PN should receive a paren-teral vitamin preparation on a daily basis.
4. Health care providers should choose PN compo-nents with the lowest aluminum content when pos-sible to minimize parenteral aluminum exposure.
5. When the use of a commercially available multipletrace element combination product results in or
TABLE VIIIDaily electrolyte and mineral requirements for pediatric patients*
Electrolyte Preterm neonates Infants/children Adolescents and children � 50 kg
Sodium 2–5 mEq/kg 2–5 mEq/kg 1–2 mEq/kgPotassium 2–4 mEq/kg 2–4 mEq/kg 1–2 mEq/kgCalcium 2–4 mEq/kg 0.5–4 mEq/kg 10–20 mEqPhosphorus 1–2 mmol/kg 0.5–2 mmol/kg 10–40 mmolMagnesium 0.3–0.5 mEq/kg 0.3–0.5 mEq/kg 10–30 mEqAcetate As needed to maintain acid-base balance As needed to maintain acid-base balance As needed to maintain acid-base balanceChloride As needed to maintain acid-base balance As needed to maintain acid-base balance As needed to maintain acid-base balance
*Assumes normal age-related organ function and normal losses.
TABLE IXDaily dose recommendations for pediatric multiple vitamins*†
Manufacturer AMA-NAG
Weight (kg) Dose (mL) Weight (kg) Dose
�1 1.5 �2.5 2 mL/kg1–3 3.25 �2.5 5 mL�3 5
*Assumes normal age-related organ function.†Pediatric multiple vitamin formulation (5 mL): A 2300 IU, D 400IU, E 7 IU, K 200 mcg, C 80 mg, B11.2 mg, B21.4 mg, B317 mg, B55mg, B6 1 mg, B121 mcg, Biotin 20 mcg, Folic acid 140 mcg.
TABLE XTrace element daily requirements for pediatrics*†
Traceelement
Pretermneonates �3 kg
(mcg/kg/d)
Term neonates3–10 kg
(mcg/kg/d)
Children10–40 kg(mcg/kg/d)
Adolescents�40 kg
(per day)
Zinc 400 50–250 50–125 2–5 mgCopper 20 20 5–20 200–500 mcgManganese 1 1 1 40–100 mcgChromium 0.05–0.2 0.2 0.14–0.2 5–15 mcgSelenium 1.5–2 2 1–2 40–60 mcg
*Assumes normal age-related organ function and normal losses.†Recommended intakes of trace elements cannot be achievedthrough the use of a single pediatric multiple trace element product.Only through the use of individualized trace element products canrecommended intakes of trace elements be achieved.25
S56 MIRTALLO ET AL Vol. 28, No. 6
increases the risk of trace element toxicity or defi-ciency states, the use of individual trace elementproducts is warranted.
6. Parenteral iron shall not be routinely supplementedin patients receiving PN therapy. It should be lim-ited to conditions of iron deficiency when oral ironsupplementation fails and followed closely in anongoing monitoring plan.
Special Considerations
Further work is required to determine optimal par-enteral trace element requirements in adult and pedi-atric patients and develop commercially available mul-tiple trace element solutions that better meet theserequirements. The use of currently available multipletrace element solutions may result in toxicity or defi-ciency of certain trace elements in some disease states.This problem may be compounded by trace elementcontamination, particularly aluminum, found in largevolume parenterals and additives.
REFERENCES
1. Saltzman E, Shah A, Shikora S. Obesity. IN Gottschlich MM, ed.The Science and Practice of Nutrition Support: A Case-BasedCore Curriculum. Silver Spring, MD: A.S.P.E.N.; 2001:677–699.
2. Barak M, Wall-Alonso E, Sitrin MD. Evaluation of stress factorsand body weight adjustments currently used to estimate energyexpenditure in hospitalized patients. JPEN J Parenter EnteralNutr. 2002;26:231–238.
3. Glynn CC, Greene GW, Winkler MF, Albina JE. Predictive ver-sus measured energy expenditure using limits-of-agreementanalysis in hospitalized, obese patients. JPEN J ParenterEnteral Nutr. 1999;23:147–154.
4. Choban PS, Flancbaum L. Nourishing the obese patient. ClinNutr. 2000;19:305–311.
5. A.S.P.E.N. Board of Directors and The Clinical Guidelines TaskForce. Guidelines for the use of parenteral and enteral nutritionin adult and pediatric patients. JPEN J Parenter Enteral Nutr.2002;26(Suppl 1):1SA–138SA. (Errata: 2002;26:144).
6. Delafosse B, Viale JP, Tissot S, et al. Effects of glucose-to-lipidratio and type of lipid on substrate oxidation rate in patients.Am J Physiol. 1994;267(5 Part 1):E775–E780.
7. Stegink LD, Freeman JB, Wisps J, Connor WE. Absence ofbiochemical symptoms of essential fatty acid deficiency in surgi-cal patients undergoing protein sparing therapy. Am J ClinNutr. 1977;30:388–393.
8. Dickerson RN, Rosato EF, Mullen JL. Net protein anabolismwith hypocaloric parenteral nutrition in obese stressed patients.Am J Clin Nutr. 1986;44:747–755.
9. Mascioli EA, Lopes SM, Champagne C, Driscoll DF. Essentialfatty acid deficiency and home total parenteral nutritionpatients. Nutrition. 1996;12:245–249.
10. Press M, Hartop PJ, Prottey C. Correction of essential fatty aciddeficiency in man by cutaneous application of sunflower seed oil.Lancet. 1974;1:597–599.
11. Miller DG, Williams SK, Palombo JD, Griffin RE, Bistrian BR,Blackburn GL. Cutaneous application of safflower oil in prevent-ing essential fatty acid deficiency in patients on home parenteralnutrition. Am J Clin Nutr. 1987;46:419–423.
12. McEvoy, GK (ed). American Hospital Formulary Service (AHFS)Drug Information. Bethesda, MD: American Society of Health-System Pharmacists Inc; 2003.
13. Federal Register. 2000; 65:21200–21201.14. American Medical Association Department of Foods and Nutri-
tion. Guidelines for essential trace element preparations forparenteral use. A statement by an expert panel. JAMA. 1979;241:2051–2054.
15. Fleming CR. Trace element metabolism in adult patients requir-ing total parenteral nutrition. Am J Clin Nutr. 1989;49:573–579.
16. Pluhator-Murton MM, Fedorak RN, Audette RJ, Marriage BJ,Yatscoff RW, Gramlich LM. Trace element contamination of
total parenteral nutrition. 1. Contribution of component solu-tions. JPEN J Parenter Enteral Nutr. 1999;23:222–227.
17. Kumpf VJ. Update on parenteral iron therapy. Nutr Clin Pract.2003;18:318–326.
18. Holliday MA, Seger WE. The maintenance need for water inparenteral fluid therapy. Pediatrics. 1957;19:823–832.
19. Fitzgerald KA, MacKay MW. Calcium and phosphate solubilityin parenteral nutrient solutions containing TrophAmine. Am JHosp Pharm. 1986;43:88–93.
20. Eggert LD, Risho WJ, MacKay MW, Chan GM. Calcium andphosphorus compatibility in parenteral nutrition solutions forneonates. Am J Hosp Pharm. 1982;39:49–53.
21. Helms R, Storm MC, Christensen ML, Hak EB, Chesney RW.Cysteine supplementation results in normalization of plasmaconcentrations in children receiving home parenteral nutrition.J Pediatr. 1999;134:358–361.
22. Haumont D, Deckelbaum RJ, Richelle M, et al. Plasma lipidconcentration in low birth weight infants given parenteral nutri-tion with twenty or ten percent lipid emulsion. J Pediatr. 1989;115:787–793.
23. A.S.P.E.N. Board of Directors. Nutrition support for low-birth-weight infants. JPEN J Parenter Enteral Nutr. 1993;17(Suppl):8SA–33SA.
24. American Academy of Pediatrics Committee on Nutrition. Nutri-tional needs of low-birth-weight infants. Pediatrics. 1985;76:976–986.
25. Green HL, Hambidge KM, Schanler R, Tsang RC. Guidelines forthe use of vitamins, trace elements, calcium, magnesium, andphosphorus in infants and children receiving total parenteralnutrition: Report of the Subcommittee on Pediatric ParenteralNutrient Requirements from the Committee on Clinical PracticeIssues of the American Society for Clinical Nutrition. Am J ClinNutr. 1988;48:1324–1342.
26. Moukarel AA, Song MK, Buchman AL, et al. Excessive chro-mium intake in children receiving total parenteral nutrition.Lancet. 1992;339:385–388.
27. Klein GL. Aluminum contamination of parenteral nutrition solu-tions and its impact on the pediatric patient. Nutr Clin Pract.2003;18:302–307.
28. Klein GL. Aluminum in parenteral solutions revisited—again.Am J Clin Nutr. 1995;61:449–56.
29. Koo WWK, Kaplan LA, Horn J, Tsang RC, Steichen JJ. Alumi-num in parenteral solutions –sources and possible alternatives.JPEN J Parenter Enteral Nutr. 1986;10:591–595.
30. Milliner DS, Shinaberger JH, Shuman P, Coburn JW. Inadver-tent aluminum administration during plasma exchange due toaluminum contamination of albumin-replacement solutions.N Engl J Med. 1985;312:165–167.
31. Fell GS, Shenkin A, Halls D. Aluminum contamination of intra-venous pharmaceuticals, nutrients, and blood products[letter].Lancet. 1986;1:380.
32. Federal Register. 2000; 65:4103–4111.33. Federal Register. 2003;68: 32979–32981.
SECTION V: STERILE COMPOUNDING OFPARENTERAL NUTRITION FORMULATIONS
SCREENING THE PN ORDER
Background
Serious disorders and death have been attributed toPN formulations having inappropriate nutrient compo-sitions. Deficiencies of trace elements and EFAs havebeen reported in both pediatric and adult patient pop-ulations.1,2 The most dramatic, yet insidious, exampleof the dangers associated with the omission of micro-nutrients occurred during the 2 periods when therewas a national parenteral vitamin shortage.3,4 At thattime, omission of parenteral vitamins resulted in threedeaths of patients predisposed to vitamin deficiencies.Specifically, a refractory lactic acidosis led to the deathof three patients associated with thiamin deficiency
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S57

that was accentuated by the administration of dextrosein the PN formulation. Similarly, a death related to theomission of dextrose from a neonatal PN caused irre-versible brain damage. Finally, life-threatening defi-ciencies have resulted when patients received phos-phate-free PN.5 Overdoses of nutrients included in PNmay also be harmful. As explained in Section I, theincorrect admixture of PN resulting in excessive dex-trose infusions led to a patient’s death, and a 50-folderror in an iron dextran solution caused serious liverdamage in a child. In all these cases, there was inad-equate review of the PN prescription for appropriate-ness of dose and adequacy of nutrient composition. It isthe responsibility of the pharmacist-by education,training, and experience to review each prescription forappropriate indication, dose, and route of administra-tion, and the potential for drug-drug, drug-nutrientand drug-laboratory interactions.6 Patient informationsuch as height, dosing weight, serum electrolyte andglucose values, hepatic and renal and gastrointestinalfunction should be available to assess the adequacy ofthe PN prescription.7
For those systems requiring that the PN prescriptionbe rewritten each day, the potential exists for tran-scription errors that omit or significantly increasenutrient doses. In this regard, it is important whenrefilling the day’s order for PN therapy that the phar-macist review the contents of the PN for consistencywith the previous day’s prescription. Major deviationsshould be questioned, to avoid nutrition-related com-plications. For example, the pharmacist should clarifywith the prescribing clinician a prescription for apatient if regular insulin was present in the previousday’s order at a dose of 20 units and the present orderis for 100 units without a change in the quantity ofdextrose received between the two days. In this case, itis both professionally appropriate and clinically rea-sonable to question the order. Other orders that mightbe appropriately questioned are drug and nutrientquantities; other large-scale changes including omis-sions, dramatic increases, or decreases; and othertypes of extreme day-to-day fluctuations.
PRACTICE GUIDELINES
1. The calorie, protein, fluid, electrolyte, vitamin, traceelement and medication content is reviewed for eachand every PN prescription to assure that a completeand balanced nutrient formulation is provided. Bal-anced is defined as the presence of the proper pro-portion of calories, protein, fluid, electrolytes, vita-mins and trace elements, to assure adequate use byand assimilation into the body.
2. Each of the PN components should be assessed forappropriateness of dose and for the potential of acompatibility or stability problem.
3. Any dose of a nutrient outside a normal range, thatis not explained by a specific patient condition orhistory, shall be questioned and clarified before thePN is compounded.
Special Considerations
Traditionally, the pharmacist is assigned the respon-sibility of verifying the indication, dose, and use of adrug or nutrient, as is the case with PN. It is recog-nized that because of the variety in the organization ofnutrition support teams, this responsibility may bereassigned to other team members in addition to thepharmacist. Also, some computer programs for PNadmixture may be programmed to cue the pharmacistthat the PN formulation is inappropriate when nutri-ent doses are outside an acceptable range.
PN COMPOUNDING
Background
The 1994 FDA Safety Alert (referred to in Section I)highlights the serious consequences that are possiblewhen quality-compounding practices are not in place.The responsibility of the dispensing pharmacist is toassure that the PN is prepared, labeled, controlled,stored, dispensed, and distributed properly.7 PN for-mulations are considered medium-risk sterile prepara-tions because of the large number of chemical entitiesfound in the admixture process and the complex natureof PN admixing, whether with gravimetric or auto-mated compounding.8–10 Serious harm may come topatients receiving a PN formulation that has precipi-tates resulting from a chemical interaction betweencomponents that are present in an excessive dose,exposed to extremes of temperature, or admixed in animproper sequence. Automated or manual methods ofPN compounding are available. The compounding ofthe PN formulation can be accomplished manuallythrough the separate addition of nutrients via syringeand needle delivery or with the aid of sterile solutiontransfer sets. The manual method allows the pharma-cist to decide the order of mixing and should be care-fully undertaken to avoid potentially lethal incom-patibilities. Alternatively, automated compoundingdevices are widely available that admix PN under com-puter-assisted commands connected to special hard-ware housed with sterile, disposable compoundingsets. According to The American Society of Health Sys-tem Pharmacists (ASHP) guidelines, the risk level ofthe compounding procedure for automated PN prepa-rations is such that it is recommended that the phar-macist verify data entered into the compounding deviceprior to PN preparation; perform end-product checks toverify compounding accuracy and, periodically observethe operation of the device to assure it is workingproperly.9 Assistance in optimizing the compoundingsequence for automated compounding devices shouldbe obtained through consultation with the manufac-turer of macronutrients currently used at the institu-tion as well as the manufacturer of the compoundingdevice because brand-specific issues might influencecompatibility of the final formulation. PN products pre-mixed by the manufacturer are available in a variety offorms that include, for example, crystalline aminoacids with electrolytes, amino acids/dextrose kits aseither separate entities or in the same container sepa-rated by a divider that can be released or activated to
S58 MIRTALLO ET AL Vol. 28, No. 6

produce the final admixture. However, even these pre-assembled units of use packaging may require somelevel of pharmaceutical compounding in an asepticenvironment prior to use.
Professional organizations have published guide-lines for compounding and dispensing sterile products.ASHP had published guidelines10 in 2000 on qualityassurance for pharmacy-prepared sterile products,while the United States Pharmacopeia (USP) recentlypublished the official compendium The United StatesPharmacopeia and The National Formulary, whichincludes a chapter on pharmaceutical compounding ofsterile preparations in 2003.8 Sterile products aredivided into three levels of risk based upon the proba-bility of exposing multiple patients to microbial con-taminants (microorganisms, spores, endotoxins) andphysical contaminants (foreign chemicals and physicalmatter). ASHP and the USP use slightly different ter-minologies for the risk levels of microbial contamina-tion for sterile products compounded within pharma-cies. The ASHP guidelines utilize the risk-levelclassification to the patient from least (level 1) to great-est (level 3) potential based upon the danger of expos-ing patients to inaccurate ingredients or pathogens. Itis also based upon microbial growth factors influencedby product storage time, temperature and product abil-ity to support microbial growth, surface and time expo-sure of critical sites, and microbial bioload in the envi-ronment. Drawing a sterile product into a sterilesyringe or transferring a sterile product from a vialinto a commercially produced intravenous bag is anexample of an ASHP risk level 1 (or a USP low-riskprocess). Risk level 2 within the ASHP guidelinesapplies to the automated compounding of PN formula-tions due to the complex and numerous manipulationsof sterile ingredients obtained from licensed manufac-turers into a sterile container by using closed-systemaseptic transfer. The newer USP compounded sterilepreparations (CSP) risk levels are designated as low,medium, and high based upon the corresponding prob-ability of contaminating a sterile preparation withmicrobial and chemical/physical contamination. Theserisk levels apply to the quality of CSP immediatelyafter the final aseptic mixing and were adopted asrequired standards for pharmacies/pharmacists in theUnited States. Compounding PN formulations is clas-sified by USP as medium-risk level given the multipleinjections, detachments, and attachments of nutrientsource products to be delivered into a final sterile con-tainer. If a non-sterile ingredient such as glutamine isadded to the PN formulation, the risk level increases tohigh. According to the ASHP guidelines and USP stan-dards, all compounded sterile preparations shall beprepared in a class 100 environment, such as a certifiedhorizontal- or vertical-laminar-airflow workbench. Per-sonnel are required to wear clean gowns or cover-alls,as scrub attire by itself is not acceptable. Gloves,masks, hair covers, shoe covers and removal of hand,finger and wrist jewelry are recommended during thecompounding process. Mishandling of these prepara-tions has resulted in reports of septic morbidity andeven death due to extrinsic contamination.
There are two critical factors in establishing beyond-use dating (currently designated as “do not use after”dating) for a PN formulation, namely microbial steril-ity and chemical stability. Unfortunately, microbialsterility testing of batch-prepared PN formulationsrarely occurs in most pharmacies. If sterility testingwithin the pharmacy is not performed for a PN formu-lation and literature sources are unavailable support-ing beyond-use dating, then the beyond-use dating ofthe preparation cannot exceed the published limits bythe USP (Table 1). Chemical stability is defined as aPN formulation maintaining its labeled strengthwithin 10% until its beyond-use date and is rarelybased on preparation-specific chemical assay results.Exposure temperatures during storage and use, char-acteristics of the sterile container used (e.g., multi-layer bags), and hydrolysis or oxidation of ingredientsare only a few of the time-dependent factors used toestablish chemical stability.
Observing the physical appearance of the final PNformulation is one of the most fundamental qualityassurance measures that pharmacists routinely apply.Although it represents a crude measure of compatibil-ity, it does identify gross particulate matter that likelyrepresents the greatest clinical risk of embolic events ifinfused into the patient. The process generally includesa detailed assessment of the final formulation againsta dark background under high-intensity illumination.For translucent intravenous solutions, the highlytrained eye is searching for the presence of insolubleparticulate matter, such as ‘cores’ from elastomeric vialenclosures, cotton fibers from alcohol wipes, as well ascharacteristic indicators of an incompatible formula-tion such as gas formation, turbidity or haziness, andcrystal formation. It is important to remember that inthe absence of any obvious physical signs of incompat-ibility, visual clarity does not equate with safety. Sub-visible particulate matter may exist and are capable ofinducing an embolic event that originates at the levelof the capillaries. However, visual assessments arevaluable and necessary in the routine quality assur-ance process, but they should be supplemented withother safety-enhancing measures that include suffi-cient documentation of the concentrations of nutrientsprepared, use of filters in the manufacturing process orduring the infusion, and possibly particle-size analysiswhen available. Documentation of the daily compound-ing activities for PN, irrespective of the products orprocedures used, should include batch records for allformulations prepared that are consistent with insti-tutional policies and procedures.
For opaque parenteral dispersions such as TNAs,visual assessments can still be performed. The princi-
TABLE IBeyond-use dating
USP risk level Controlled room temperature 2°–8°C ��20°C
Low �48 hours �14 days �45 daysMedium* �30 hours �7 days �45 daysHigh �24 hours �3 days �45 days
*Level assigned to PN formulation compounding from USP Chapter797.
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S59

pal aim of these assessments is focused on signs ofphase separation, in which the unstable emulsion ismanifested by the presence of free oil either as individ-ually discernible fat droplets or a continuous layer atthe surface of the formulation. In general, light cream-ing is a common occurrence and not a significant deter-minant of infusion safety except in extreme cases.
PRACTICE GUIDELINES
1. The additive sequence in compounding shall be opti-mized and validated as a safe and efficaciousmethod.
2. If the manual method currently in use at an insti-tution has not been recently reviewed, or if thecontract with a particular manufacturer of macro-nutrients is about to change, then a review of thecompounding method is strongly recommended.This review shall include an evaluation of the mostcurrent literature as well as consultation with themanufacturer when necessary.
3. Manufacturers of automated methods of PN com-pounding shall provide an additive sequence thatensures the safety of the compounding device. Thiscompounding sequence should be reviewed with themanufacturer of the parenteral nutrient productsused by the institution. As most institutions in theU.S. are represented by buying groups with manyparticipants, such buying groups should not onlyensure the safety and support of the automatedcompounding device, but should avoid splitting PNcontracts (mixing brands of amino acids, dextroseand IVFE) unless such combinations have adequatephysicochemical data that ensures the stability,compatibility and safety of the final formulationscommensurate with the data for single source PNproducts.
4. Each PN formulation compounded should be visu-ally inspected for signs of gross particulate contam-ination, particulate formation and/or phase separa-tion of TNAs.
QUALITY ASSURANCE OF THE COMPOUNDING PROCESS
Background
Numerous cases have been reported of adverseevents associated with erroneous final concentrationsof dextrose in parenteral fluids. Also, infectious eventshave occurred from microbial contamination of phar-macy-prepared PN formulations.11
In-process or end-product testing of PN should beperformed in accordance with USP standards andASHP guidelines for sterile product admixture.8–10
Because of the complex nature of PN formulations,these processes may be modified to accommodate thespecial physicochemical characteristics of PN with useof the methodologies for gravimetric, chemical, orrefractometric analysis and in-process testing.
Gravimetric Analysis
Weight-based delivery of PN additives is the princi-pal method by which automated compounders preparePN formulations. These devices provide a high degree
of accuracy and accomplish it in a fraction of the timeit takes with use of manual, gravity-fed compoundingtechniques. In general, as a final check, the PN formu-lation is weighed and is expected to be within anacceptable margin of error. However, while some auto-mated compounding devices evaluate only the weightof the total contents, other compounding devices weighthe final admixture as well as individual additives. Toensure that certain additives having a narrow marginof safety are assessed individually, pharmacists canapply gravimetric techniques similar to those used bythe compounding device. This is particularly importantfor additives such as potassium chloride and highlyinteractive salts such as phosphates. In the case ofpotassium chloride, a 2000-mL final PN volume with a5% compounding error acceptance means that a100-mL overfill would be tolerated. If the entire overfillcame from the potassium chloride container(s), it couldbe lethal. Thus individual monitoring of certain PNadditives is recommended, and this monitoring can besimply accomplished within the sterile compoundingfacility each day. The gravimetric method is preferred,with use of the analytical balance associated with theautomated compounder.
Chemical Analysis
A random, but continuously applied assessment ofthe final dextrose concentration is reasonable. Oneapproach is through the use of glucose measuringdevices that allow for direct assessment of the dextroseconcentration. Although these instruments have a lim-ited effective range of detection, appropriate dilutionsmay be made from a PN aliquot to measure the finalconcentrations of dextrose and to assure that they arein accordance with the prescribed quantities intendedfor the patient. When this quality assurance method isdevised, it is important to outline a stepwise procedure,validate the findings against appropriate control dex-trose solutions, and apply the appropriate error anal-ysis that gauges an acceptable margin of error.
Refractometric Analysis
Refractometers have been used in pharmacy practicefor determining dextrose content. However, they mayrequire training and experience in order to obtain con-sistent and reliable results. In addition, because refrac-tometry measures a physical characteristic of dextrose(e.g., refractive index), it is an indirect determinant ofdextrose concentration and is subject to interference byother components, as well as to variation in techniquefrom one operator to another and in subsequent inter-pretation of the final results. As with direct measure-ment techniques of dextrose concentration, the proce-dures should be validated in a similar manner toassure the integrity of the results. Refractometers arerendered inoperable with TNAs, and therefore are ofno use for these formulations.
In-Process Testing
There are three ways to test the integrity of thesterile compounding process of PN formulations, and
S60 MIRTALLO ET AL Vol. 28, No. 6
all three can be accomplished at any time before, dur-ing, or after the hours of operation for PN preparation.For purposes of this summary, ‘in-process’ can includeany one of the aforementioned periods. The amount ofpotassium chloride used after each stock bottleexchange, along with the appropriate density conver-sion for the additive tested, can be determined gravi-metrically at multiple points during the day, withinthe compounding facility. As long as the number ofpatients who received a portion of the stock from acontainer is properly recorded, the pharmacist candetermine whether the delivery is accurate by analyz-ing a subset of the PN formulations and can takeappropriate action for only those formulations affected,thereby reducing the costs associated with waste ifthey need to be remade. Similarly, individual PN con-tainers can be analyzed for dextrose content duringchemical or refractometric analysis, which can beapplied in a cost-effective manner.
In addition to these assessments of hardware func-tion, the software can be similarly challenged to seewhether the response is appropriate to the command.For example, if an extraordinary amount of calciumand phosphorus are entered into the compounding pro-gram, does the software recognize a potential incom-patibility? However, such challenges to the softwareprogram are best performed either before or after PNadmixture, rather than during the time of operation.Such tests run the risk of an inadvertent compoundingcommand that may be overlooked and could result indispensing an incompatible and potentially dangerousformulation.
Process validation of aseptic procedures is recom-mended for PN formulations.8,10 Individuals involvedin PN compounding should successfully complete aprocess validation of aseptic technique prior to beingallowed to admix PN. Process simulation of the PNformulation may also be used but is more difficult sincethe PN formulation itself may limit or inhibit microbialgrowth if inadvertently contaminated during the com-pounding process.
PRACTICE GUIDELINES
1. Gravimetric analyses that indirectly assess theaccuracy of the individual additives delivered or thefinal contents of the PN can be readily applied in thepharmacy practice setting. Particular attentionshould be focused on the most dangerous additivesthat tolerate the least margin of error, such as thepotassium salts.
2. Chemical analyses that directly measure the finalcontent of the individual additives can be incorpo-rated into the PN compounding operations of thepharmacy. The accuracy of the PN dextrose contentis an example of an additive that may be associatedwith significant morbidity and mortality.
3. Refractometric analysis is an alternative, as well asan indirect measure of the final additive concentra-tion. For example, dextrose concentration is fre-quently assessed by this technique. However, thismethod is limited to PN formulations that do notcontain IVFE.
4. In-process or end-product testing of PN formula-tions is recommended daily so as to assure a safe,final formulation is dispensed to the patient.
5. End-product testing of PN formulations preparedwith automated compounding devices is recom-mended to verify compounding accuracy.
6. The aseptic sterile preparation of intravenousadmixtures intended for patient administrationshould adhere to the USP (797) PharmaceuticalCompounding-Sterile Preparations Chapter8 andthe ASHP Guideline on Quality Assurance for Phar-macy-Prepared Sterile Products.10
Special Considerations
Use of dual-chamber bags for PN formulationsresolve the long-term stability issues of TNA especiallyfor home PN patients. However, aseptic techniqueissues related to IVFE transfer from the original con-tainer to the dual chamber compartment may be sim-ilar to those for transfer to syringe as discussed in thePN administration section. This is not known and aprocess should be in place to assure sterile admixture,storage and administration of the IVFE component ofthe dual-chamber bag.
REFERENCES
1. Heller RM, Kirchner SA, O’Neill JA, et al. Skeletal changes ofcopper deficiency in infants receiving prolonged parenteral nutri-tion. J Pediatr. 1978;92:947–949.
2. Riella MC, Broviac JW, Wells M, Scribner BH. Essential fattyacid deficiency in human adults during total parenteral nutri-tion. Ann Intern Med. 1975;83:786–789.
3. Anonymous. Death associated with thiamin deficient total par-enteral nutrition. MMWR. 1987;38:43.
4. Alliou M, Ehrinpreis MN. Shortage of intravenous multivitaminsolution in the United States. [Letter]. N Engl JMed. 1997;337:54–55.
5. Travis SF, Sugarman HJ, Ruberg RL, et al. Alterations of red-cell glycolytic intermediates and oxygen transport as a conse-quence of hypophosphatemia in patients receiving intravenoushyperalimentation. N Engl J Med. 1971;285:763–768.
6. Spotlight on the key elements of the medication system. ISMPMedication Safety Alert. 2003;2: 3–4.
7. A.S.P.E.N. Board of Directors. Standards for nutrition supportpharmacists. Nutr Clin Pract. 1999;14:151–162.
8. (797) Pharmaceutical Compounding—Sterile Preparations.United States Pharmacopeial Convention, PharmacopeialForum 2003;29:940–965.
9. American Society for Health-System Pharmacists, ASHP Guide-lines on Safe Use of Automated Compounding Devices for thePreparation of Parenteral Nutrition Admixtures. Am J Health-Syst Pharm. 2000;57:1343–1348.
10. American Society for Health-System Pharmacists, ASHP.Guidelines on quality assurance for pharmacy-prepared sterileproducts. Am J Health-Syst Pharm. 2000;57:1150–1169.
11. Bozetti F, Bonfanti G, Regalia E, Calligaris L, Cozzaglio L.Catheter sepsis from infusate contamination. Nutr Clin Pract.1990;5:156–159.
SECTION VI. STABILITY ANDCOMPATIBILITY OF PARENTERAL
NUTRITION FORMULATIONS
PN STABILITY
Background
The stability of PN formulations principally focuseson the degradation of nutritional components over
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S61

time. The Maillard reaction (‘the browning reaction’) iswell-known and involves the complexation of carbohy-drates by certain amino acids such as lysine, which isfacilitated by temperatures used for sterilization ofcommercial products. Thus the combination of aminoacids and dextrose is usually prepared in the pharmacywith stability of the final formulation determined by itsstorage conditions prior to administration. It is gener-ally recognized that the sterile compounding of any PNaccelerates the rate of physicochemical destabilization.Presently, certain amino acids, vitamins and IVFE aremost susceptible to instability. Except for an isolatedcase report, the discoloration of commercial amino acidproducts forming a bluish hue is not associated withadverse effects. However, the oxidation reactioninvolving tryptophan that produces the discolorationshould be prevented by storage away from light and,preferably, keeping the manufacturer’s protectivepackaging intact until the time of use.
From a clinical perspective, the physicochemical sta-bility of PN formulations is largely focused on vita-mins, several of which are known to deteriorate sub-stantially over time and in the presence of oxygen. Forthe most part, despite their degradation, very few pro-duce clinically significant disturbances in the acutecare setting. They tend to be more important inpatients with marginal body stores and who are depen-dent on long-term PN support. The clearest example ofthis was demonstrated in a case report of a home PNpatient who received weekly batches of PN prepared bya hospital pharmacy in which the vitamins were addedfor a period of up to 7 days. Within 6 months, thepatient had night blindness, was treated with a largeintramuscular dose of vitamin A, and the symptomsresolved. Six months later, the patient had a relapse insymptoms, prompting an investigation into why theparenteral vitamin supplement was insufficient inmeeting the patient’s needs. Because the vitaminswere added up to a week before the solution wasadministered, substantial amounts of vitamin A werelost to degradation and adsorption into the plasticmatrix of the infusion container. Adding the vitaminsto the PN formulation daily just prior to infusionresolved the problem.1
Similarly, when ascorbic acid was added in a batchfashion, it degraded and resulted in the formation of alarge, discernible precipitate in the PN formulation.Careful analysis revealed that the precipitate was cal-cium oxalate. Oxalic acid is a degradation product ofvitamin C that readily reacts with free calcium. Signif-icant degradation can be avoided by adding vitaminsjust prior to infusion.2
The sterile preparation of L-glutamine for additionto PN poses several concerns. L-glutamine has limitedstability in PN formulations, and it requires special-ized parenteral manufacturing techniques not rou-tinely available in most institutional or home carepharmacies. The formulation needs to be evaluated toassure that its final contents meet the desired concen-tration and that it is sterile and free of pyrogens.Assuming the sterile compounding facility is qualifiedto make such a product, it is the pharmacist’s respon-sibility to quarantine the product and ensure that it
passes the aforementioned tests prior to its infusion. Inmost cases, the quarantine period is at least 7 days inorder to complete the microbiological analyses for theappearance of slow-growing pathogens. For productswith limited stability, however, USP standards doallow for release of the product prior to the end of thequarantine period. Therefore, although less than ideal,quality control issues arising after quarantine can bedealt with retrospectively.
In addition to the above concerns for PN formula-tions, the stability of submicron lipid droplets shallalso be maintained in TNA dispersions during theperiod of infusion. Because an anionic emulsifier sta-bilizes the TNA dispersion and numerous destabilizingcations (e.g., calcium, magnesium, sodium and potas-sium) are routinely included, the risk of infusing anunstable and potentially dangerous formulation ispresent. Generally, when producing a TNA, the man-ufacturer of the IVFE product clearly delineates itsphysicochemical limitations. The pharmacist is urgedto use this brand-specific information and not extrap-olate to other products.
The use of dual-chamber bags, whereby for example,the IVFE is physically separated from the remainingadmixture components, can enhance the shelf life ofTNAs. It’s greatest utility appears to be in the home-care setting where batch preparation of PN formula-tions is most common. Once all the nutrients from bothchambers are combined for infusion, the new beyond-use date for completion of infusion should not exceed24 hours and compatibility should be based on param-eters for TNAs.
Although TNAs have been formulated for use in theneonate/infant, stability of lipid particles within theformulation shall be established for each combinationof additives before use. The higher content of divalentcations (e.g. calcium and magnesium) can reduce par-ticle zeta potential (negative surface charge), resultingin coalescence. Additionally, the higher content of cal-cium and phosphate in neonatal/infant PN formula-tions increases the risk of precipitation, which can goundetected because of TNA opacity.
PN COMPATIBILITY
The complex formulations typical of PN pose severalpossible physicochemical incompatibilities. The mostserious risk of incompatibility in PN formulations andthus the most imminent threat to the patient ariseswhen macroprecipitates exceeding 5 microns developin the formulation and pass into the central circula-tion. Two forms of precipitates (solid and liquid) mayappear in the prepared formulation. Commonly, theexistence of crystalline matter is most frequently citedin PN formulations, yet with the use of TNA, phaseseparation with the liberation of free oil constitutes theliquid precipitate.
Solid precipitates can develop when an incompatiblecombination of various salts is added to a PN formula-tion; this results in the formation of insoluble product.Calcium salts are one of the most reactive compoundsand readily form insoluble products with a number ofadditives. Dibasic calcium phosphate (CaHPO4) is an
S62 MIRTALLO ET AL Vol. 28, No. 6

example of one of the most dangerous incompatiblecombinations and has resulted in embolic deaths wheninfused in the clinical setting. This can be avoidedthrough a variety of measures. First, calcium gluconateis the preferred form of calcium used in multi-compo-nent PN formulations. Calcium chloride is far morereactive than an equivalent amount of calcium glu-conate salt. Therefore, solubility curves for calciumgluconate cannot be applied to calcium chloride. Sec-ond, the order of compounding is extremely importantin order to avoid the formation of an insoluble precip-itate that would otherwise be soluble if added in thecorrect sequence. Generally, phosphate should beadded first, and calcium should be added near the endof the compounding sequence to take advantage of themaximum volume of the PN formulation. Other risks offorming solid precipitates include the use of bicarbon-ate salts when indicated to correct a base deficitthrough the PN. Again, bicarbonate reacts with cal-cium to form the insoluble product calcium carbonate.If an alkalinizing salt is indicated, then sodium orpotassium acetate should be used. The dose of thealkalinizing salt is the same for either bicarbonate oracetate (1 mEq of bicarbonate has the same alkaliniz-ing power as 1 mEq of acetate). Finally, ascorbic acid isa highly unstable vitamin that is sometimes added insupraphysiologic quantities (up to 2000 mg per day) inthe PN for its antioxidant effects. However, because ofits unstable characteristics, it readily degrades in thepresence of oxygen to form oxalic acid, which is alsohighly reactive with calcium, forming the insolubleproduct calcium oxalate. Thus the use of this vitaminin supraphysiologic quantities should be given via sep-arate infusion and not in the PN formulation.
Phase separation and the liberation of free oil fromthe destabilization of TNAs can result over time whenan excess of cations is added to a given formulation.The higher the cation valence, the greater the destabi-lizing power; thus trivalent cations such as Fe�3 (fromiron dextran) are more disruptive than divalent cationssuch as calcium and magnesium. Monovalent cationssuch as sodium and potassium are least disruptive tothe emulsifier, yet when given in sufficiently high con-centrations, they may also produce instability. There isno safe concentration of iron dextran in any TNA.3 Ofthe divalent and monovalent cations, most adultpatients’ clinical needs can be met without significantconcern of producing an unstable and potentially dan-gerous formulation. Even the order of compoundingcan cause instability of TNAs, and the compoundingsequence shall not place destabilizing additives such asthe cations or hypertonic dextrose in close sequencewith a minimally diluted IVFE. In general, the phar-macist should be guided by the instructions of themanufacturer for the macronutrients and the auto-mated compounder in use to assure that all PN formu-lations are compounded optimally, and that they aresafe and compatible.
The presence of enlarged lipid globules can be suc-cessfully identified if the proper techniques are used.There are only two stages of emulsion destabilizationthat are visually detectable by the naked eye, namelycreaming and coalescence. As visual observation is the
most routinely applied quality assurance methodemployed by practicing pharmacists, an appreciation ofthe physical signs of TNA integrity is essential. Theinitial stage in emulsion breakdown is creaming whichoccurs almost immediately upon standing once IVFEhas been mixed with the other chemical constituents.The presence of a cream layer is visible at the surfaceof the emulsion as a translucent band separate fromthe remaining TNA dispersion, although the lipid par-ticles in the cream layer are destabilized; their individ-ual droplet identities are generally preserved. As such,this phase (creaming) of emulsion breakdown is stillsafe for patient administration.
The terminal stage of emulsion destabilization is thecoalescence of small lipid particles forming large drop-lets that may vary in size from 5–50� microns andpose potential clinical danger yet escapes visual detec-tion. The existence of coalesced lipid particles in a TNAformulation is characterized by the variable presenceof yellow-brown oil droplets at or near the TNA surface.In its usual presentation, the free oil may exist asindividual spherical droplets or as segmented (discon-tinuous) oil layers. Careful observation of each TNAformulation is required to detect the subtle appearanceof coalescence. In its most extreme form, the oil pre-sents as a continuous layer of yellow-brown liquid atthe surface of the formulation that is readily discern-ible from the remaining dispersion, and can be accom-panied by marbling or streaking of the oil throughoutthe formulation. In either case, the presence of free oilin any form in a TNA should be considered unsafe forparenteral administration4. The danger associatedwith the infusion of unstable lipid droplets enlargedthrough electromechanical destabilization is unclear.However, the existence of lipid globules 5 microns indiameter comprising 0.4% of the total fat present hasbeen shown to be pharmaceutically unstable, and suchformulations are considered unfit for intravenousadministration.3
Finally, standard PN formulations have been usefulto organizations whereby the physicochemical stabilityand compatibility are assured via adequate documen-tation by the institution or the manufacturer of PNproducts. Such standardization limits the risk of com-pounding and dispensing potentially unstable orincompatible PN formulations. However, any changein the composition of standard formulations needs tobe applied cautiously and with adequate assurancethat the new or revised formulation is stable andcompatible.
Medication Administration with PN
Since PN is infused intravenously, it is often consid-ered as a vehicle for medication administration. Due tothe complex nature of PN and potential for physico-chemical interactions with drug-nutrient combina-tions, admixture of medications with PN is not advised.However, there are occasions when there is no otherreasonable alternative. When this occurs, the predom-inant admixture issues that need to be resolved includethe following5:
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S63

● medication stability and compatibility with the PN orTNA is assured;
● evidence supports the clinical value of the medicationadministered in this manner.Insulin use with PN. Insulin is commonly adminis-
tered with PN. As noted in the Introduction, it is alsoassociated with frequent harmful events. This isrelated to the variable methods used to control bloodglucose levels in patients receiving PN. No one methodof glucose control has been shown to be superior. Insu-lin requirements are generally higher and most vari-able during the first 24 hours of intensive care forcritically ill patients. Strict serum glucose control at avalue less than 110 mg/dL with a separate continuousinsulin infusion has been shown to improve clinicaloutcomes (i.e. shorter ICU stay, ventilator use andmortality) in select surgical critically ill patients.6 Dueto the potential for serious adverse events, insulin usein PN should be done in a consistent manner adheringto a defined protocol, in which healthcare personnelhave adequate knowledge. One such approach can besummarized as follows:
Hyperglycemia and insulin resistance occur fre-quently in patients receiving PN. Diabetic patientsreceiving PN have been shown to have a 5-foldincrease in catheter-related infections compared tonondiabetics.7 Clinical studies suggest that carbohy-drate administration via PN greater than 4–5mg/kg/min or greater than 20–25 kcal/kg/dayexceeds the mean oxidation rate of glucose, givingrise to significant hyperglycemia, lipogenesis, andfatty liver infiltration.8 Although no clear consensusexists for the ideal level of glucose control in thehospitalized patient receiving PN, a reasonable tar-get is a blood glucose level of 100 to 150 mg/dL.
Many approaches can be used to achieve appropriateglucose control in patients with diabetes or stress-induced hyperglycemia receiving PN. Patientsshould not receive more than 150 to 200 grams ofdextrose on day 1 of PN. For patients previouslytreated with insulin, oral hypoglycemic agents, orpatients with a fasting glucose concentration 200mg/dL but in whom hyperglycemia is likely to occur,no more than 100 grams of dextrose per day shouldbe administered. A basal amount of human regularinsulin should also be added to the PN formulation tokeep blood glucose concentrations less than 150mg/dL in patients previously treated with insulin ororal hypoglycemic agents. (NOTE: only regularhuman insulin is compatible with PN formulations;other insulin products such as NPH, ultralente,lente, lispro, aspart, and glargine are NOT compat-ible with PN). A common initial regimen is 0.1 unitsof insulin per gram of dextrose in the PN infusion. Ifthe patient is already hyperglycemic (�150 mg/dL),0.15 units of insulin per gram of dextrose should beused.9 If the blood glucose is 300 mg/dL, PN shouldnot be initiated until glycemic control is improved (�200 mg/dL). Obese patients with type 2 diabetes mayrequire as much as 0.1 units of insulin for every 0.5grams of dextrose whereas thin, type 1 diabetics may
require only 0.1 units of insulin per 2 grams of dex-trose.10 In general, the dextrose content of the PNshould not be increased until glucose concentrationsduring the previous 24-hour period are consistently�200 mg/dL. If glucose is controlled with a specificinsulin dose, the dose of insulin must be reassessedwhenever the dextrose dose is modified.
Capillary glucose levels should be monitored every 6hours and supplemented with an appropriatelydosed sliding-scale insulin coverage given subcuta-neously as needed to maintain glucose in goal range.Once glucose concentrations are stable, the fre-quency of measuring capillary glucose concentra-tions often can be decreased. The insulin dosage inthe PN formulation ratio is modified daily based onthe amount of insulin given with sliding-scale insu-lin coverage over the previous 24 hours. If hypergly-cemia persists when 0.3 units of insulin per gram ofPN dextrose is exceeded, initiation of a separateintravenous insulin infusion should be used toachieve more appropriate glycemic control. In apatient whose insulin needs are dynamic or difficultto predict (e.g. infection, inflammatory response), aseparate intravenous infusion is preferred.
Another method of medication administration withPN is co-infusion through the same intravenous tub-ing. This should be avoided unless physical and chem-ical compatibility of the medication with the PN for-mulation is assured prior to its administration in thismanner. Studies11,12 of medication compatibility withPN found that the compatibility differed for TNA ver-sus 2-in-1 formulations, emphasizing that compatibil-ity in one formulation does not predict compatibility inthe other. As such, compatibility information should bederived for PN that closely match the formulation pre-scribed for the patient in question. If the medication isnot compatible with PN, the PN infusion should not beinterrupted for medication administration. The medi-cation should be administered via another intravenousroute. Finally, the compatibility of some medicationswith a TNA may be dependent on drug concentration.For example, morphine sulfate is compatible with TNAat a concentration of 1 mg/ml but not 15 mg/ml.
PRACTICE GUIDELINES
1. The dose, admixture preparation, packaging, deliv-ery process, and storage and administration methodshould be confirmed to ensure that the PN is stableand all components are compatible.
2. The responsible pharmacist should verify that theadministration of drugs with PN either admixed inthe PN or co-infused through the same intravenoustubing is safe, clinically appropriate, stable, andfree from incompatibilities.
3. If there is no information concerning compatibilityof the medication with PN, it should be adminis-tered separately from the PN.
4. Compatibility information should be evaluatedaccording to concentration of the medication used
S64 MIRTALLO ET AL Vol. 28, No. 6
and whether the base formulation is a 2-in-1 or aTNA.
5. Insulin use in PN should be done in a consistentmanner according to a method that healthcare per-sonnel have adequate knowledge.
6. Decisions related to stability and compatibility aremade according to the most reliable informationavailable from the literature or manufacturer ofintravenous nutrients. If no information exists, sta-bility and compatibility of the PN shall be deter-mined in consultation with the manufacturer beforeit is dispensed to the patient.
7. Given the limited amount of published stabilityinformation available, the use of a 2-in-1 formula-tion with separate administration of IVFE is recom-mended for neonatal/infant patients.
REFERENCES
1. Howard L, Chu R, Feman S, et al. Mintz H, Ovesen L, Wolf B.Vitamin A deficiency from long-term parenteral nutrition. AnnIntern Med. 1980;93:576–577.
2. Gupta VD. Stability of vitamins in total parenteral nutrientsolutions. Am J Hosp Pharm. 1986;43:2132.
3. Driscoll DF, Bhargava HN, Li L, et al. Physicochemical stabilityof total nutrient admixtures. Am J Hosp Pharm. 1995;52:623–634.
4. Driscoll DF. Total nutrient admixtures: Theory and practice.Nutr Clin Pract. 1995;10:114–119.
5. Driscoll DF, Baptista RJ, Mitrano FP, et al. Parenteral nutrientadmixtures as drug vehicles. Theory and practice in the criticalcare setting. Ann Pharmacother. 1991;25:276–283.
6. Van den Berg G, Wouters P, Weekers F, et al. Intensive insulintherapy in critically ill patients. N Engl J Med. 2001;345:1359–1367.
7. McMahon MM, Rizza RA. Nutrition support in hospitalizedpatients with diabetes mellitus. Mayo Clinic Proc. 1996;71:587–594.
8. Rosmarin DK, Wardlaw GM, Mirtallo J. Hyperglycemia associ-ated with high continuous infusion rates of total parenteralnutrition dextrose. Nutr Clin Pract. 1996;11:151–156.
9. McCowen KC, Malhotra A, Bistrian BR. Stress-induced hyper-glycemia. Crit Care Clin. 2001;17:107–124.
10. Boord JB, Graber AL. Christman HW, Powers AC. Practicalmanagement of diabetes in critically ill patients. Am J RespirCrit Care Med. 2001;164:1763–1767.
11. Trissel LA, Gilbert DL, Martinez JF, Baker MB, Walter WV,Mirtallo JM. Compatibility of parenteral nutrient solutions withselected drugs during simulated Y-site administration. Am JHealth-Syst Pharm. 1997;54:1295–1300.
12. Trissel LA, Gilbert DL, Martinez JF, Baker MB, Walter WV,Mirtallo JM. Compatibility of medications with 3-in-1 parenteralnutrition admixtures. JPEN J Parenter Enteral Nutr. 1999;23:67–74.
SECTION VII: PARENTERAL NUTRITIONADMINISTRATION
Optimal, safe PN administration requires an ade-quate understanding of multiple integrated key con-cepts. Comments from respondents to the 2003 Surveyof PN Practices noted several problems with adminis-tration including; incorrect PN rate and volume andPN administered to the wrong patient or via the wrongvenous access site. This section will address the con-cepts pertinent to safe administration of PN including:proper venous access device selection, care and assess-ment; appropriate use of the medical equipmentneeded to deliver the PN solution; the chemical prop-erties of the PN formulation itself and monitoring the
patient’s response to the PN therapy. The institutionaluse of PN from home or another facility is an issueaddressed in this section.
VENOUS ACCESS SELECTION, CARE AND ASSESSMENT
To safely and properly administer PN, the indica-tions for intravascular catheter use, proper proceduresfor the insertion and maintenance of intravascu-lar catheters and appropriate infection control mea-sures to prevent catheter-related infections shall beunderstood.
The proper selection of a venous access site (centralvs peripheral vein) depends on nutrient requirementsand duration of PN.1–6 Due to the hypertonic nature ofmost PN formulations, it is recommended that the PNbe administered through a central venous access cath-eter (CVC) with tip placement in the superior venacava2 adjacent to the right atrium.4,7 Proper cathetertip placement also reduces the risk for cardiac injury7
and decreases the chance for problems infusing orwithdrawing fluids from the catheter.4 Infusion of PNvia a peripheral vein requires careful consideration ofthe formulation’s osmolarity along with judicious mon-itoring of the venous access site for signs of phlebitisand/or infiltration. Since 10% and 20% IVFE productsare isotonic, they may be infused separately via aperipheral vein or as part of a TNA when osmolaritydoes not exceed 900 mOsm/L.8
In general, selection of the most appropriate paren-teral access device is based on the patient’s vascularcondition, vascular anatomy, vascular access history,type and duration of therapy, coagulation status, caresetting (acute care, long-term care, and home care) andunderlying disease. Additional considerations whenselecting a venous access device for PN include thepatient’s physical ability to care for the catheter, cog-nitive function, activity level, body image concerns andcaregiver involvement. Temporary percutaneous non-tunneled CVCs (subclavian, jugular) are most oftenused in the acute care setting for short duration ther-apy. Femoral CVC’s are associated with a higher risk ofvenous thrombosis and catheter related sepsis; theyare not recommended for PN administration unless noother venous access can be attained.9 In circumstanceswhere the tip of the femoral catheter is not located inthe inferior vena cava, adjustment of the PN content toeffectively reduce the osmolarity similar to peripheralPN is recommended. Care and maintenance of the fem-oral catheter should be with the same vigilance as anyother CVC. Tunneled percutaneous catheters (e.g.Hickman®, Groshong®) or implanted subcutaneousinfusion ports are most appropriate for long-term ther-apy outside of the acute care setting. The peripherallyinserted central catheter (PICC) for central venousaccess is used for PN administration in a variety ofhealth care settings. The PICC is a reasonable CVCoption to consider if the anticipated length of PN isweeks and not long-term provided the appropriateplacement of the catheter tip can be achieved and ver-ified. Generally, tunneled catheters or implanted portsshould be considered for longer access durations andmore permanent therapy.
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S65

Guidelines have been developed for the daily careand maintenance of the catheter once the proper CVCis inserted.3,6 Prior to the initial administration of PNthrough a CVC, and any other time there aresigns/symptoms indicative of a compromised catheterposition, the catheter tip location shall be verifiedradiographically. Proper catheter tip placement shallalso be confirmed and or validated in the pediatricpatient as growth and maturity occur. The infectiouscomplications of PN administration are also reducedwhen catheter access devices are dedicated solely toPN usage (or the designation of one port solely for PNadministration if a multi-lumen catheter is used) andcatheter manipulations are minimized.3 Reductions incatheter associated sepsis have been reported whennurses are educated in the proper care of the CVCbased on established standards and guidelines.1,3 Ifcontinued care and monitoring is required beyond theacute care setting, it is the health care provider’sresponsibility to ensure education of the patient and/orcaregiver in proper care techniques.
MEDICAL EQUIPMENT FOR PN ADMINISTRATION
Filters
The use of in-line filters has been recommended dur-ing the administration of intravenous products such asPN formulations.6,10–12 The rationale for this recom-mendation is related to the filter’s ability to eliminateor reduce infusion of particulates, microprecipitates,microorganisms, pyrogens and air. Due to the multipleadditives used to prepare PN formulations, a largenumber of particulates may contaminate the fluidbeing administered. Particles of 5 microns or larger arecapable of obstructing blood flow, which could lead tocomplications such as pulmonary embolism. These for-eign particles may also produce phlebitis at the injec-tion site, a therapy-limiting problem when PN isadministered peripherally. An in-line filter can reducethe incidence of phlebitis.
Microprecipitates form under certain pH and tem-perature conditions such that the rate and extent aredependent on these factors in addition to the concen-tration of PN additives. Microprecipitates of calciumphosphate are known to cause serious problems. Initialvisual inspection of PN is a primary method to avoidproblems with microprecipitates but this cannot berelied upon since it is unlikely the precipitate will forminstantaneously. In most situations, precipitates maytake hours to develop. As such, visual inspection of thePN formulation should be done periodically throughoutthe compounding, dispensing and administration pro-cesses. Visual detection is limited however since parti-cles �50 microns cannot be easily detected with theunaided eye and problems are possible with particles ofthis size. Since particles may clog filters, filters havebeen criticized because they may require frequentnursing interventions. It should be recognized that aclogged filter and associated infusion pump alarm is apotential sign of a precipitate. It is never appropriate toremove a clogged filter and allow the formulation toinfuse without a filter.
Use of a 0.22 micron filter for PN administration canremove microorganisms but this practice is limited touse with 2-in-1 formulations. The integrity of the IVFEis compromised when infused through filters �1.2microns in size. A 1.2 micron filter however does notremove most microorganisms from a contaminated PNformulation even though it is effective in removingparticulates and microprecipitates. PN formulationsare considered high-risk admixtures and can becomecontaminated during compounding or administrationsetup. There have been frequent reports of patientinfections caused by contaminated PN fluids. The useof aseptic technique in preparation and administrationof PN formulations is critical to avoid infections due tocontaminated PN formulations.
Filters have been shown to be effective in removingpyrogens from 2-in-1 formulations and those with airventing can prevent air emboli. The use of filters mayreduce the potential for contaminated PN formulationsto infect a patient but do not eliminate the possibility.As such, the CDC does not recommend in-line filterssolely for infection control purposes.3
Use of in-line filters has limitations. They can causedecreased flow rates, clogs, or air locks. This may leadto increased manipulation of the intravenous adminis-tration set, creating a potential for microbial contami-nation. For PN administration, a 0.22 micron filter isrecommended for a 2-in-1 formulation. A 1.2 micronfilter should be used for TNAs. When considering par-ticulate and microprecipitate contamination only, a 1.2micron filter can be used for all PN formulations.
Infusion Pumps and Administration Sets
Specific recommendations also exist to guide the useof PN administration tubing sets. PN administrationsets shall be changed using aseptic technique and uni-versal precautions.3 Changes of “add on devices” to thePN administration set (e.g., extension tubing, filters orneedle-less devices) should coincide with changing ofthe PN administration set to maintain the entire PNadministration system as a closed system.6 TNAadministration sets are changed every 24 hours andimmediately upon suspected contamination or if theproduct integrity has been compromised.2,3,6 Adminis-tration sets used for separate IVFE infusions (notTNA) are discarded after each unit is infused, unlessadditional units are administered consecutively. Whenseparate IVFE infusions are administered consecu-tively, the administration set shall be replaced every24 hours.3,6 As with TNA, lipid emulsion sets arechanged immediately if contamination is suspected orif the product integrity has been compromised. Admin-istration sets infusing PN formulations containing onlydextrose and amino acids shall be changed every 72hours.3 PN final containers and administration setsfree of the plasticizer; di (2-ethylhexyl) phthalate(DEHP) shall be used to prevent DEHP contaminationof TNAs or separate IVFE infusions.13 Since DEHP ishighly lipophilic, IVFE are capable of extracting DEHPfrom the polyvinylchloride (PVC) final containers andadministration sets. Concern over adverse effects fromDEHP is related to its potential for neurotoxicity, car-
S66 MIRTALLO ET AL Vol. 28, No. 6

cinogenicity, and hepatotoxicity in animals. Use ofDEHP-free bags and tubing is especially important inchronic long-term patients, pregnant patients, andpediatric patients receiving PN.
Intravenous (IV) infusion pumps are an integralcomponent of PN administration.2,5,6 Use of an elec-tronic infusion pump to safely administer PN is recom-mended.2,6 Infusion pumps assure accurate volume(rate) control and contain safety alarms (visual andauditory) for sensing air and pressure changes in theIV tubing; some pumps also have a programmable ratecycling feature to minimize infusion errors. These fea-tures are important to PN because of the hypertonicnature, fluid volume, dextrose and potassium contentof PN formulations. JCAHO National Patient SafetyGoals include recommendations for infusion pumps.14
Free-flow protection is important to the safety of PNadministration to avoid serious harm caused by rapidadministration of potassium and dextrose. Regularpreventative maintenance and testing should assureproper functioning of clinical alarm systems becausehealth care practitioners administering the PN, andindividuals receiving the PN, rely on those alerts tooptimize safe infusion of the PN formulation.
Safe administration guidelines are not only intendedto protect those patients receiving PN, they are alsoimportant to protect the health care provider adminis-tering PN from blood-borne pathogens. Health careproviders face daily exposure to blood when adminis-tering PN via a venous access device. Among the risksare human immunodeficiency virus (HIV), hepatitis Band hepatitis C. Federal government agencies havepublished standards to prevent needle-stick injuries inhealth care settings, as well as, enforcement proce-dures for the occupational exposure to blood-bornepathogens.15,16 In 2000, the Needle-stick Safety andPrevention Act was signed into law and in 2001, incor-porated into the revised OSHA Blood-borne PathogenDirective.17 The Act highlights the importance of usingnew technologies and requires employers who are cur-rently covered by the Blood-borne Pathogen Standardto evaluate and implement medical devices that reducethe risk of needle-stick injuries, as well as, eliminate orreduce exposure to blood-borne pathogens. Health careproviders administering PN should take an active rolein identifying, evaluating and selecting effective med-ical devices to reduce their exposure to blood-bornepathogens. Examples of compliance for PN administra-tion is the use of a commercially available needle-lesssystem to draw blood or applying a needle-free catheterpatency device to a CVC to eliminate the back flow ofblood into the catheter lumen. It is important to notethat the Needle-stick Safety and Prevention Actchanges OSHA’s 1991 Blood-borne Pathogens Stan-dard from an “agency directive” to a law, enforceable inthe same manner as any other OSHA public law.
ADMINISTRATION ISSUES RELATED TO PN ADMIXTUREPROPERTIES
Prior to PN administration, the identity of thepatient is verified using at least two identifiers.14 ThePN label is reviewed for accuracy, expiration date and
patient identity. Also, the PN formulation and con-tainer is visually inspected for leaks, color changes,emulsion cracking, clarity and expiration dates. Do notuse any parenteral fluid that has expired, has visualturbidity, leaks, emulsion cracking or particulate mat-ter.3 The TNA presents a more complex scenario forinspection because of the inability to visualize precip-itate or particulate matter in the opaque admixture.18
It is essential to visually assess the TNA for destabili-zation or separation of the lipid components. Any TNAthat exhibits evidence of destabilization (heavy cream-ing, cracking or discoloration) shall not be adminis-tered or shall be discontinued immediately if the solu-tion is already infusing.19,20 The pharmacist evaluatesthe TNA formulation before dispensing, and the nurse,patient and/or caregiver is responsible for ongoingevaluation of the TNA while it is infusing.
As discussed previously, IV medications are fre-quently prescribed for patients receiving PN. Pub-lished information regarding PN compatibility withparenteral medications is available, but limited.1,20–23
The appropriate administration of parenteral medica-tions to individuals receiving PN is based on stabilityand compatibility data. It is recommended that stabil-ity and compatibility data be validated if the medica-tion is expected to have direct contact with the PN. Ifan incompatibility or unstable condition exists, or ifthere is no information available, the medicationshould be administered separate from the PN.
The characteristics of IVFE favor an environment inwhich pathogenic organisms can thrive. These 10%and 20% preparations are nearly iso-osmotic (250–290mOsm/L), have a near-neutral alkaline pH (pH � 7.5),and contain glycerol, all of which are conducive to thegrowth of microorganisms. However, when IVFE arecombined with crystalline amino acids and hydrateddextrose to form TNA, the pH drops (pH�6.0) and theosmolarity increases to provide a poor growth me-dium.24 Several reports of microbial growth potentialin commercially available IVFE bottles prompted theCenters for Disease Control and Prevention in 1982 tolimit the “hang time” to 12 hours after the manufac-turer’s container is spiked with the appropriate admin-istration set. IVFE have been associated with reportsof fungemia in the neonatal population, including bothCandida species and Malassezia furfur.25–27 It appearsthat IVFE were administered as separate infusions inthese reports. When IVFE is transferred from its orig-inal container to another sterile device (e.g., syringe) orrecipient container for infusion separate from PN, onecould argue that a more conservative 6-hour hang timeshould be followed. This recommendation would beconsistent with the FDA-approved labeling for propofol(Diprivan®) emulsion when manipulated for adminis-tration via a syringe delivery system, even with theexistence of antimicrobial agents not present in IVFEmanufactured for nutritional use. A standard for prod-uct dating of prepared sterile dosage forms when theproduct is altered from its original packaging hasrecently been revised by the United States Pharmaco-peia (USP).28 The USP refers to this newly assigneddate as the “beyond-use date” and it limits the timeperiod in which the product can be used in patients.
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S67

Because of the concern for microbial contamination,the USP recommends that IVFE products be usedwithin 12 hours of opening the original container ifthey are to be infused as a separate infusion. Theinfusion rate should not exceed 0.125 g/kg/hr, thus a200-mL bottle of 20% IVFE should not be infused morerapidly than over 6 hours (0.095 g/kg/hour) in the 70-kgreference man. If a slower infusion is desirable and theselected rate of administration exceeds 12 hours, thenthe lipids shall be given in two separate bottles so asnot to exceed a 12 hour hang time for any single con-tainer. If the IVFE is admixed directly to the PN toform a TNA, the final PN formulation can be infusedover a 24-hour period since it provides a safe vehiclewith respect to infectious risks.
Patient Response to PN Administration
No discussion of safe PN administration would becomplete without briefly mentioning a few key moni-toring concepts unique to the patients receiving PN.Considerable cost and serious complications are oftenassociated with PN administration. Once it is deter-mined that the individual will receive PN, goals fornutrition support should be set with specific markersand outcomes to be measured.1,29 These goals mayinclude improved or replenished protein stores, nor-malization of clinical laboratory values, and reductionin morbidity/mortality and improvement in quality oflife or optimization of clinical outcomes. Monitoringindividuals receiving PN is necessary to determine theefficacy of the specialized nutrition therapy; detect andprevent complications; evaluate changes in clinicalcondition and document clinical outcomes. All patientsreceiving PN should be monitored for fluid and electro-lyte imbalances, proper blood glucose control andsigns/symptoms of CVC infections. Typically, labora-tory monitoring of serum chemistries and visceral pro-teins are more frequent when PN is initiated and thendecrease in frequency as clinically indicated. Thehealth care provider is also alert to potential changesin fluid status and should closely monitor intake andoutput, edema, vital signs and weights with attentionto changes, patterns or trends that could indicate prob-lems or progress toward achieving nutritional goals.Regular assessment and meticulous care of the paren-teral access device assures a reliable delivery systemfor the PN and minimizes the chance for infection. It isimportant that the healthcare provider periodicallycompare the actual PN nutrients delivered to thepatient with the recommended measured or estimatednutrition needs to assure optimal treatment. Patientsmay tolerate the PN infusion better if the refrigeratedPN is removed from the refrigerator 30–60 minutesprior to the scheduled infusion times; PN patients occa-sionally complain of discomfort while the chilled solu-tion is infused into the central circulation.6 Individualsreceiving their first PN formulation should be moni-tored closely for any adverse reactions. Compatibilityand stability of a new parenteral medication shall beassured along with a review of the medication profilefor potential effects on safe administration of othermedications. It is also important to reassess gastroin-
testinal function and readiness for oral/enteral feedingif the patient’s clinical condition should change.
IVFE infusion in hypertriglyceridemic patients. Confu-sion surrounds the safe administration of IVFE inpatients with hypertriglyceridemia. As previouslymentioned, several investigators have determined thatthe rate for infusion of IVFE not exceed 0.125 g/kg/hourin order to avoid serious metabolic effects.30 Thus,IVFE should be infused at rates to avoid serum triglyc-eride levels �400 mg/dL in adults and �200 mg/dL inneonates. The clinical consequences associated withhypertriglyceridemia in both adults and neonatesinclude an increased risk of pancreatitis, immunosup-pression, and altered pulmonary hemodynamics, whilehypertriglyeridemia in the preterm infant with physi-ologic jaundice and hyperbilirubinemia (�18 mg/dL) isassociated with kernicterus. Doses of IVFE should belimited to the provision of EFAs (e.g., 250 mL of 20%IVFE, once or twice weekly) when triglyceride concen-trations rise above 400 mg/dL in adult patients. Tem-porary interruption of IVFE infusions for 12 to 24hours are recommended when serum triglyceride con-centrations exceed 275 mg/dL in neonates and infants;a decrease in infusion rate by 0.02–0.04 g/kg/hour issuggested when IVFE infusions are restarted.31 With-holding IVFE in adults shall be considered whenserum triglyceride concentrations are greater than 500mg/dL. The presence of excess phospholipid content of10% versus 20% IVFE is also associated with greaterplasma lipid alterations. The excess phospholipids pro-duce lipoprotein X-like substances that can competewith chylomicron remnants for hepatocyte bindingsites. This can interfere with lipid clearance by delay-ing peripheral hydrolysis of triglycerides by lipoproteinlipase. Use of 20% IVFE allows for more efficient tri-glyceride clearance and metabolism.
In conclusion, there is extensive attention directedtowards monitoring the patient’s physiologic responseto PN therapy; it is equally important that the individ-ual’s developmental, emotional and psychological re-sponses to the PN also be assessed and monitored.
Use of PN Prepared by Another Facility
Organizations commonly admit patients fromanother facility or home who are receiving PN. Theadmission may or may not be directly related to the PNor underlying disease. These organizations are fre-quently in the position of dealing with PN formulationsbrought in from home or infusing into patients trans-ferred from other inpatient facilities. Due to the com-plex nature of PN formulations from a dosing, compat-ibility, sterility and stability perspective, the use of thePN by the organization is a difficult issue. Evidence tosupport, guide or describe current practices is lackingso the issue was addressed in the 2003 Survey of PNPractices. As discussed in the introduction, there wasno consensus as to whether PN formulations com-pounded elsewhere should be administered in theadmitting organization’s facility. Several points forconsideration (pro or con) were identified in the com-ments to the survey question along with Task Forceinput (Table I).
S68 MIRTALLO ET AL Vol. 28, No. 6
If the PN was infusing at the time of patient admis-sion, responders to the question stated that it wasallowed to finish then the hospital pharmacy preparedall subsequent PN formulations. In another scenario, ifthe PN was compounded by the health care systems’own home infusion pharmacy, the PN was allowed tobe used.
There is no consensus to the problems addressedtherefore; it is difficult to provide specific guidelines.Guidelines for use of oral medications from homereferred to as ‘bring-in’ medications (i.e., patient’s ownsupply) have been developed and may provide someinsight when considering PN formulations brought infrom an outside facility. Principles addressed in theseguidelines32 are outlined as follows:● The use of a patient’s own supply in the hospital
should be avoided unless they are not obtainable bythe pharmacy;
● If used, a physician order shall be written.� The identity of the medication should be verified
▪ If not identifiable, it shall not be used.� It should be dispensed as a part of the pharmacy
distribution system, not separate from it.PN formulations are much more complex than oral
medications. It may also be prudent to consider thefollowing for PN:● A policy and procedure is developed to address the
issue.● When the use of PN is allowed, a physician’s order is
required.� All components of the PN formulation are entered
into the patient’s medical record as an active order.● Issues related to maintaining PN integrity during
storage, delivery and administration are resolved.● If there is any reason that the compounding or stor-
age conditions of the PN formulation have been com-promised, its use shall not be allowed.
● The appropriateness of the PN formulation for thepatient’s current condition is assured prior to itsadministration.
PRACTICE GUIDELINES
1. Central PN is administered via a CVC with thedistal tip placed in the superior vena cava adjacentto the right atrium.
2. The use of femoral catheters for PN administrationshould be avoided.
3. Proper CVC tip placement shall be confirmed priorto initial PN administration and/or any other timesigns/symptoms indicate an improper catheterposition. Proper CVC tip placement shall also be
confirmed/validated in the pediatric patient whenthere has been significant growth.
4. Care and maintain venous catheters used for PNaccording to published standards.
5. Equipment used to administer PN formulationsshall be selected based on the safest mode of deliv-ery for both the patient and the healthcareprovider.
6. A 1.2 micron filter may be used for all PN formu-lations. Alternatively a 0.22 micron filter may beused for 2-in-1 formulations.
7. A filter that clogs during PN infusion may be indic-ative of a problem and may be replaced but shallnever be removed.
8. PN final containers and administration sets shallbe free of the plasticizer, DEHP if IVFE is a com-ponent of the nutrient regimen.
9. Administration sets for IVFE infusions separatefrom PN formulations shall be discarded after useor if the IVFE is infused continuously, at leastevery 24 hours.
10. Administration sets for TNA are changed every 24hours.
11. Administration sets for 2-in-1 formulations arechanged every 72 hours.
12. PN is to be administered via an infusion pumphaving adequate protection from ‘free flow’ andreliable, audible alarms.
13. Medical devices for PN administration should beused that minimize risk of needle-stick injuriesand exposure to blood-borne pathogens.
14. Prior to PN administration, the patient’s identityis verified and the PN label is reviewed for accu-racy and expiration dates.
15. Visually inspect each PN prior to administration,do not infuse the PN formulation if visual changesor precipitates are apparent.
16. The PN infusion shall be completed within 24hours of initiating the infusion.
17. IVFE infused separately from PN formulationsshall be completed within 12 hours of entry intothe original container.
18. The patient receiving PN should be monitoredto determine the efficacy of the PN therapy; de-tect and prevent complications; evaluate changesin clinical conditions; and document clinicaloutcomes.
19. A policy and procedure should be in place to dealwith the use of PN formulations prepared by anoutside facility.
TABLE IPros and cons: use of PN compounded by another facility
Reasons for use Reasons not to use
Prevents wastage of unused home PN Inability to adequately validate PN integrity from a stability andsterility perspective
Provides specific information concerning PN contents and therapy Creates billing and reimbursement issuesPN formula may contain products not available to admitting
organizationMedico-legal responsibility for PN administration problems
unclearAvoids an interruption in therapy Unfamiliar PN tubing set or infusion pump
November–December 2004 SAFE PRACTICES FOR PARENTERAL NUTRITION S69
REFERENCES
1. A.S.P.E.N. Board of Directors and the Clinical Task Force.Guidelines for the use of parenteral and enteral nutrition inadult and pediatric patients. JPEN J Parenter Enteral Nutr.2002;26 (Suppl):1SA–138SA (Errata: 2002;26:114).
2. Ford CD, Vizcarra C. Parenteral nutrition. IN: Terry J, ed.Intravenous Therapy: Clinical Principles and Practice. Philadel-phia, PA: Intravenous Nurses Society, WB Saunders; 1995:219–248.
3. Centers for Disease Control and Prevention. Guidelines for thePrevention of Intravascular Catheter-Related Infections.MMWR. 2002;51:RR-10.
4. Steiger E. Obtaining and Maintaining Vascular Access in theHome Parenteral Nutrition Patient. JPEN J Parenter EnteralNutr. 2002;26(Suppl 5):S17–S20.
5. Krzywda EA, Andris DA, Edmiston CE, Wallace JR. Parenteralaccess devices. IN Gottschlich MM, ed. The Science and Practiceof Nutrition Support: A Case-Based Care Curriculum. Dubuque,IA: American Society for Parenteral and Enteral Nutrition,Kendall/Hunt; 2001:225–250.
6. Intravenous Nurses Society. Infusion Nursing: Standards ofPractice. J Intraven Nurs. 2000;23 (Suppl):S1–S88.
7. Collier PE, Goodman GB. Cardiac tamponade caused by centralvenous catheter perforation of the heart: a preventable compli-cation. J Am Coll Surg. 1995;181:459–463.
8. Isaacs JW, Millikan WJ, Stackhouse J, Hersh T, Rudman D.Parenteral nutrition of adults with 900-milliosmolar solution viaperipheral vein. Am J Clin Nutr. 1977;30:552–559.
9. Harden JL, Kemp C, Mirtallo J. Femoral catheters increase riskof infection in total parenteral nutrition patients. Nutr ClinPract. 1995;10:60–66.
10. Bethune K, Allwood M, Grainger C, Wormleighton C. BritishPharmaceutical Nutrition Group Working Party. Use of filtersduring the preparation and administration of parenteral nutri-tion: position paper and guidelines prepared by a British phar-maceutical nutrition group working party. Nutrition. 2001;17:403–408.
11. National Advisory Group on Standards and Practice Guidelinesfor Parenteral Nutrition: Safe Practices for Parenteral NutritionFormulations. JPEN J Parenter Enteral Nutr. 1998;22:49–66.
12. Food and Drug Administration, Safety Alert: Hazardous of Pre-cipitation Associated with Parenteral Nutrition. Am J Hosp.Pharm. 1994;51:1427–1428.
13. Dickerson RN. Di (2-ethylhexyl) phthalate as a plasticizer forintravenous bags and tubing: a toxicological quandary. Nutri-tion. 1997;13:1010–1012.
14. www.jcaho.org/accredited�organizations/patient�safety/04�npsg/04_npsg.html.
15. U.S. Department of Health and Human Services, Public HealthService Centers for Disease Control and Prevention (CDC),National Institute for Occupational Safety and Health Settings(NIOSH). Preventing Needlestick Injuries in Health Settings.NIOSH Publication No. 2000–108. Cincinnati, OH: NIOSH;November 1999.
16. U.S. Department of Labor, Occupational Safety and HealthAdministration (OSHA). Enforcement Procedures for the Occu-
pational Exposure to Bloodborne Pathogens. Directives No. CPL2–2. 44D. Effective Date: November 5, 1999.
17. U.S. Department of Labor, Occupational Safety and HealthAdministration (OSHA). Occupational Exposure to BloodbornePathogens; Needlesticks and Other Sharp Injuries; Final RuleFederal Legislation, Public Law 106–430. Effective Date: April18, 2001.
18. Barber JR, Miller SJ, Sacks GS. Parenteral feeding formula-tions. IN Gottschlich MM, ed. The Science and Practice of Nutri-tion Support: A Case-Based Care Curriculum. Dubuque, IA:American Society for Parenteral and Enteral Nutrition,Kendall/Hunt; 2001:251–268.
19. Rollins CJ. Total nutrient admixtures: stability issues and theirimpact on nursing practice. J Intraven Nurs. 1997;6:299–304.
20. Strausberg KM. Parenteral nutrition admixture. IN Merritt RJ,ed. A.S.P.E.N. Nutrition Support Manual. Silver Spring, MD:American Society for Parenteral and Enteral Nutrition; 1998:8–1-8–12.
21. Kumpf VJ, Gervasio J. Pharmacotherapeutics. IN GottschlichMM, ed. The Science and Practice of Nutrition Support: A Case-Based Care Curriculum. Dubuque, IA: American Society forParenteral and Enteral Nutrition, Kendall/Hunt; 2001:287–299.
22. Klang MG, Hayes EM, Bloss CS. Drug-nutrient considerations-parenteral nutrition. IN Merritt RJ, ed. A.S.P.E.N. NutritionSupport Practice Manual. Silver Spring, MD: American Societyfor Parenteral and Enteral Nutrition; 1998:10–1-10–11.
23. Trissel LA, Gilbert DL, Martinez JF, Baker MB, Walter WV,Mirtallo JM. Compatibility of medications with 3-in-1 parenteralnutrition admixtures. JPEN J Parenter Enteral Nutr. 1999;23:67–74.
24. Sacks GS, Driscoll DF. Does lipid hang time make a difference?Time is of the essence. Nutr Clin Pract. 2002;17:284–290.
25. Curry CR, Quie PG. Fungal septicemia in patients receivingparenteral hyperalimentation. N Engl J Med. 1971;285:1221–1225.
26. Dankner WM, Spector SA, Fierer J, Davis CE. Malassezia fun-gemia in neonates and adults: complications of hyperalimenta-tion. Rev Infect Dis. 1987;9:743–753.
27. Weiss SJ, Schoch PE, Burke AC. Malassezia furfur fungemiaassociated with central venous catheter lipid emulsion infusion.Heart Lung. 1991;20:87–90.
28. Okeke CC, Bailey L, Medwick T, Grady LT. Revised USP stan-dards for product dating, packaging, and temperature monitor-ing. Am J Health-Syst Pharm. 2000;57:1441–1445.
29. A.S.P.E.N. Board of Directors, Clinical Pathways and Algo-rithms for Delivery of Parenteral and Enteral Nutrition inAdults. Silver Spring, MD: American Society for Parenteral andEnteral Nutrition; 1998.
30. Carpentier YA, Kinney JM, Sidedrova VS, et al. Hypertriglycer-idemic clamp: a new model for studying lipid metabolism. ClinNutr. 1990;9(Suppl 1):1–9.
31. Sacks GS, Mouser JF. Is IV lipid emulsion safe in patients withhypertriglyceridemia? Nutr Clin Pract. 1997;12:120–123.
32. American Society of Hospital Pharmacists. ASHP technicalassistance bulletin on hospital drug distribution and control.Am J Hosp Pharm. 1980;37:1097–1103.
S70 MIRTALLO ET AL Vol. 28, No. 6
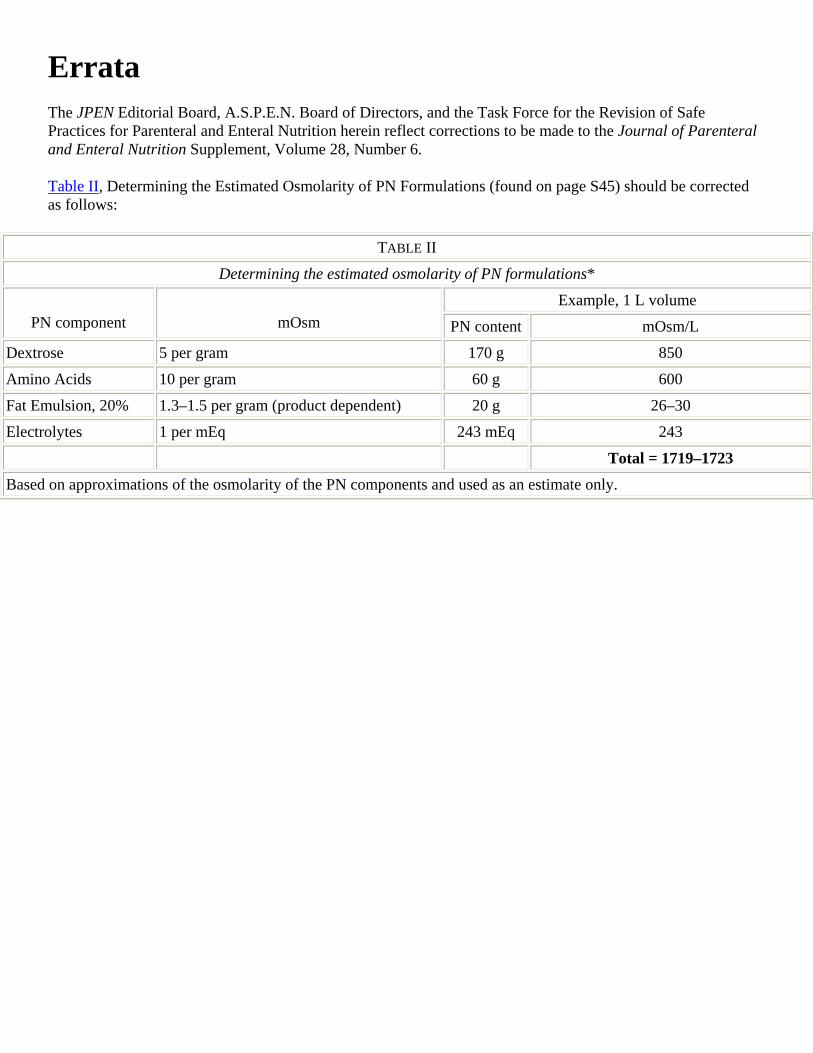
Errata The JPEN Editorial Board, A.S.P.E.N. Board of Directors, and the Task Force for the Revision of Safe Practices for Parenteral and Enteral Nutrition herein reflect corrections to be made to the Journal of Parenteral and Enteral Nutrition Supplement, Volume 28, Number 6.
Table II, Determining the Estimated Osmolarity of PN Formulations (found on page S45) should be corrected as follows:
TABLE II
Determining the estimated osmolarity of PN formulations*
Example, 1 L volume PN component mOsm PN content mOsm/L
Dextrose 5 per gram 170 g 850
Amino Acids 10 per gram 60 g 600
Fat Emulsion, 20% 1.3–1.5 per gram (product dependent) 20 g 26–30
Electrolytes 1 per mEq 243 mEq 243
Total = 1719–1723 Based on approximations of the osmolarity of the PN components and used as an estimate only.