jcs january february 2014 volume 6 issue 1
DESCRIPTION
Journal for Clinical Studies - Peer Reviewed Journal, looking into the entire spectrum of the Clinical Research Industry. With particular emphasis on emerging markets.TRANSCRIPT

www.jforcs.com
PEER REVIEWED
Volume 6 - Issue 1
Alzheimer’s Disease without Dementia A New Journey of Care
Logistics in Emerging Markets A New Watch Series
The Role of Regulatory Agencies in New Drug DevelopmentA Global Perspective
Using Questionnaires in Clinical ResearchA Guide through the Data Jungle
JOURNAL FOR
Your Resource for Multisite Studies & Emerging MarketsCLINICAL STUDIESU

We help companies like TauRx® Therapeutics and clinical research sites like Re:Cognition Health soar beyond their aspirations; efficiently enrolling
patients for their clinical trials, to bring medicines to market sooner.
Welcome to MediciGlobal™
We’re one of the world’s leading patient recruitment-retention companies, and we’re at the forefront of successfully engaging patients and their
caregivers for clinical trials.
US Office Philadelphia, TEL: +1 484 674 6800 | UK Office London, TEL: +44(0)20 8834 1447
WE HAVE THE BEST JOB IN THE INDUSTRY
www.PatientRecruitment.com
Accelerating Enrolment Digital Marketing Locating Lost Patients
JCS_Ad_Jan2014_revised.indd 1 1/28/14 12:35 PM

Contents
Journal for Clinical Studies 1www.jforcs.com
06 FOREWORD
WATCH PAGES
08 Specifying Therapeutic Area Standards for Clinical Research
In its efforts to facilitate clinical research and regulatory review of drugs and biologics, the US Food and Drug Administration (FDA) has launched a multi-year initiative to standardise key study data to therapeutic areas (TAs). Guiding the project is the Therapeutic Area Standards Initiative Project Plan, to provide the overall management framework for addressing and accomplishing the objectives of the fifth authorisation of the Prescription Drug User Fee Act (PDUFA V). Deborah A. Komlos of Thomson Reuters explains the new standards.
10 Cardiovascular Therapeutics Watch PageTo help family doctors and general practitioners treat their patients most effectively, hypertension specialists who belong to related professional societies co-author guidance documents published by the societies in the medical literature. Examples include guidelines for the management of arterial hypertension prepared by a task force of experts from the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC), and the recent ESH position paper on the use of ambulatory blood pressure monitoring (ABPM) in both clinical research and clinical practice. J. Rick Turner and Philip Galtry of Quintiles review guidance documentation on hypertension.
12 Logistics in Emerging Markets Column Clinical research was traditionally carried out in the well-funded locations of North America, Western Europe and Australasia, but due to saturation and a lack of naive patients available and willing to take part in trials, companies are seeking new trial sites in emerging markets. Each of these countries represent challenges in logistics, ensuring temperature control, arranging customs clearance and regulatory release. Sue Lee of World Courier examines the many hazards of conducting clinical trials in emerging regions, including arranging shipping, gaining knowledge of local requirements, addressing packages, and airport storage.
REGULATORY
14 Regulation for Paediatric Drug Development in India: Need of the Hour
India is a popular location for clinical research due to the multitude of benefits it offers, including a large patient pool, low costs and ethical flexibility. However, this ethical flexibility has been abused. Per se, there are no specific requirements for the conduct of clinical trials on the paediatric population, resulting in the irrational use of drugs and untoward drug reactions.
MANAGING DIRECTOR Martin Wright
PUBLISHERMark A. Barker
EDITOR Cecilia Stroe
EDITORIAL MANAGERHolly Barnes
DESIGNER Fiona Cleland
RESEARCH & CIRCULATION MANAGEROrsolya Balogh
BUSINESS DEVELOPMENT Reya Kochanova
ADMINISTRATOR Barbara Lasco
FRONT COVER © istockphoto
PUBLISHED BY Pharma PublicationsUnit J413, The Biscuit Factory Tower Bridge Business Complex 100 Clements Road, London SE16 4DGTel: +44 0207 237 2036Fax: +0014802475316Email: [email protected]
Journal for Clinical Studies – ISSN 1758-5678 is published bi-monthly by PHARMAPUBS.
The opinions and views expressed by the authors in this magazine are not necessarily those of the Editor or the Publisher. Please note that although care is taken in preparation of this publication, the Editor and the Publisher are not responsible for opinions, views and inaccuracies in the articles. Great care is taken with regards to artwork supplied, the Publisher cannot be held responsible for any loss or damage incurred. This publication is protected by copyright.
Volume 6 Issue 1 January 2014 PHARMA PUBLICATIONS
JOURNAL FOR
Your Resource for Multisite Studies & Emerging Markets CLINICAL STUDIES U

With the proposed revamping of drug development guidelines in India, Dr M. V. P. Venkatesh of JSS College of Pharmacy and his associates discuss the need to introduce specific guidelines to regulate and protect the paediatric population.
18 Risk-based Monitoring: Moving ForwardAfter issuance of the final guidance document by FDA on Oversight of Clinical Investigations - A Risk-based Approach to Monitoring, the clinical trials industry is embarking on a paradigm shift to reap the benefits of Risk-based Monitoring (RBM). Considering the importance and current interest related to RBM, Cecilia Stroe, Editor of Journal of Clinical Studies talks with Ashok Ghone of MakroCare, USA.
20 The Role of Regulatory Agencies in New Drug Development: A Global Perspective
Regulatory agencies worldwide play a critical role in healthcare as independent reviewers and approvers of applications made by sponsors to conduct clinical trials, and ultimately to market a drug for a particular indication. J. Rick Turner, Theo J. Hoofwijk, and Robin Huff of Quintiles present an overview of the regulatory landscapes for new drug development in the United States (US), Japan, and the European Union (EU); the three geographic regions that came together to form the International Conference on Harmonisation of the Technical Requirements for Registration of Pharmaceuticals for Human Use.
MARKET REPORT
24 Iran InterestNumerous pharmaceutical companies are considering Iran as a strong site for clinical research. With a huge untapped population, the opportunity to conduct all clinical phases from I-IV, a clear process of regulatory application, and the potential to run genetic and observational studies, it is fast becoming a popular location for trials. Adhiti Sharad Kumar of ACRP explicates the registration process, regulatory and ethical stipulations, procedures, and timelines for conducting clinical research in this emerging region.
26 Clinical Trials in Russia - Report on Q3 of 2013The Ministry of Health of the Russian Federation approved 200 new clinical trials of all types during the third quarter of 2013. The main contribution to the total number of studies was made by multinational multi-centre clinical trials (MMCT). The number of bioequivalence studies decreased from 64 studies in Q3 2012 to 51 in Q3, while the number of local clinical trials decreased from 53 to 4. Igor Stevanov of Synergy Research Group summarises developments in the Russian clinical trials market in 2013.
30 Developing a New Branch of Medicine: Cell Therapy in Estonia
A recent announcement from Estonia discussed the
launching of the first human stem cell production laboratory in the Baltic States. Behind the lab is a wider initiative, the Estonian Cell Therapy Cluster, with the objective of developing the field of cell therapy. Andrus Loog of the Estonian Cell Therapy Cluster writes on how the converging of the cluster’s activities is creating treatment opportunities, a research-intensive export possibility for the Estonian medical services, as well as high-added-value jobs.
THERAPEUTICS
34 Alzheimer’s Disease Without Dementia: A New Journey of Care
Much of the debate surrounding Alzheimer’s distracts from the fact that we are on the cusp of a revolution in the diagnosis, treatment and long-term management of the disease. The next five to seven years purports a transformation; from short-term treatment of symptoms to a long-term ‘stable state’, resulting in living with Alzheimer’s without dementia. Importantly, sustaining this state for a significant period of time enables patients to prolong their maintenance of daily function, which in turn extends quality of life for patients as well as their families. Dr J. Emer MacSweeney of Re:Cognition, in conjunction with Liz Moench and Elizabeth Puller of MediciGlobal Ltd, discuss the path towards a significant change in the course of Alzheimer’s disease.
38 Arterial Stiffness and Rheumatoid ArthritisRheumatoid arthritis (RA) is associated with increased cardiovascular morbidity and mortality, while over the past few years, arterial stiffness has emerged as a new marker of cardiovascular disease, independent of traditional risk factors. Dr Winter of AtCor Medical, Inc. discusses why combining arterial stiffness measurements with traditional risk factors significantly improves the prediction of morbidity and mortality.
40 Increasing Therapeutic Complexity in CNS Clinical Tri Trials: The Need for Therapeutically Aligned Staff
The recent rise in protocol complexity has been particularly evident in trials targeting CNS diseases, where, in the wake of some notable late-stage study failures in recent years, sponsors are increasingly emphasising the scientific integrity of experimental drug programmes in this space. To that end, when conducting CNS trials today, it is critical that sponsors and contract research organisations (CROs) implement better and more thorough processes and tools in areas such as patient eligibility screening and confirmation and the review of outcome data assessments, which, for many CNS indications, often contain subjective information. Andrew Silverman of INC Research discusses how, to meet these demands, CNS study teams are increasingly in need of clinical research associates (CRAs) that possess both therapeutic and technical expertise.
Contents
Volume 6 Issue 12 Journal for Clinical Studies

ARIANNE is dedicated to excellence and serving the needs of the biopharmaceutical and medical device industry to develop and deliver healthcare solutions to mankind.
With our expertise and teamwork, we are committed to being your strategic partner and provide flexible all-inclusive, cost-effective approaches to advance product development worldwide.
9444 Waples Street, Suite 160San Diego, CA 92121 – USA
http://www.ariannecorp.com
Clinical Services
Data Management
Clinical Trial Management
Drug Safety
Biostatistics
Quality Assurance
Consulting Services
Product Development
Regulatory Affairs
QA Services
Education
ARIANNE has a global
reach on 5 continents in over 25 countries,
including:
USA, Canada, MexicoSouth Africa, North Africa, Middle East
Asia, East and Central Europe
C
M
Y
CM
MY
CY
CMY
K
Arianne_ad_print.pdf 1 30/01/2014 11:09:36

Volume 6 Issue 14 Journal for Clinical Studies
Contents
44 Collaborative Drug Development for Rare DiseasesPatient groups are essential partners for clinical research as they are usually the most invested, and can therefore drive drug development. Often, patient groups focus on a single disease, and so are prepared to focus all of their time on understanding that disease and seeking solutions for its treatment. However, patient groups cannot work alone; they require the expertise of other partners. Oliver Timmis of the AKU Society and Anthony Hall of Findacure believe that a collaborative approach to drug development for rare diseases is the best way forward, and explore the ten steps leading to clinical research in this article.
IT & LOGISTICS
48 Building the Right Strategic Plan to Manage Clinical Supplies for Your Clinical Trial
In recent years, biomedical research has increased, and as a result, its portion of the clinical trials market / trials market continues to grow. Therefore the need for generating temperature-sensitive biomaterials that biotech companies can implement to ensure the accurate transportation and compliant storage of temperature-sensitive clinical trial drugs and supplies, is mounting. Sule Mene and her associates at MENE Research discuss the logistical procedures of conducting clinical trials in Turkey.
52 Using Questionnaires in Clinical ResearchPatient and physician questionnaires, visual analogue scales, rating scales for the assessment of efficacy, effectiveness, safety, quality of life (QoL), resource use, and treatment costs are becoming more and more important in clinical research. In particular, the increasing emphasis on QoL, treatment costs, real-life effectiveness of drugs, and the need for patient-focused outcomes to achieve market access, leads to a rise in the development and use of scales. Selection, use, analysis, and reporting of questionnaires are tasks that need to be integrated throughout the whole clinical development process, and Thomas Wagner of Trilogy Writing explains the most important steps necessary for an optimal leverage of questionnaire data.
56 Before and After: A Clinical Project Manager’s StoryAccording to research performed with a range of pharmaceutical companies, skills of the operational players in a business relationship and the degree to which the players on both sides operate as one team are critical factors that are instrumental in whether a business partnership delivers against its objectives. In this article, John Faulkes of Agio Interactive explores these factors through the role of the Clinical Project Manager.

myoderm.com
For us, they’re not hard to find.Myoderm knows what’s at stake for our clients, so we scour the world for the comparators they need for clinical trials. Our ability to locate restricted and hard-to-find drugs is unmatched. And we can handle both one-time shipments or the ongoing management and delivery of drugs and supplies to local trial sites. That’s why eight of the world’s top ten pharma companies place their trust in us. You will, too.
© 2014 Myoderm. All rights reserved.
MYO-140_Corp_WordSearch_JCS_210x297.indd 1 1/10/14 3:17 PM

It’s a new year and JCS connects you with the latest regulatory developments, industry trends and challenges. The world of clinical research is changing. New EU rules on clinical trials are being set up and it’s all about a closer collaboration between regulators and ethics committees, meant to encourage research whilst protecting patients’ rights.
In this issue, JCS brings you exclusive insight into the current state of Alzheimer’s disease detection and diagnosis. In their report, Dr J Emer MacSweeney, Medical Director and Principal Investigator at Re:Cognition Health, London UK, Liz Moench, President and CEO, MediciGroup® Inc., and Elizabeth Puller, Senior Account Manager, MediciGlobal Ltd argue that as the burden of Alzheimer’s disease escalates worldwide, efforts to develop effective treatments are failing to keep pace because of the high costs and risks associated with developing Alzheimer’s drugs. Find out how reforming Alzheimer’s drug development
would cut cost and speed progress towards the approval of drugs that slow or stop the disease.
In the R&D landscape, new models of collaboration are emerging to enable drug development in rare diseases. Oliver Timmis, Head of Projects for the AKU Society, and Anthony Hall, co-founder of PSR orphan experts and Findacure, explain how patient groups can become essential partners for clinical research.
Cecilia StroeEditor
Foreword
Editorial Advisory Board
Art Gertel, VP, Clinical Services, Regulatory & Medical writing, Beardsworth Consulting Group Inc.
Ashok K. Ghone, PhD, VP, Global Services MakroCare, USA
Bakhyt Sarymsakova - Head of Department of International Cooperation, National Research Center of MCH, Astana, Kazakhstan
Caroline Brooks - Associate Director, Logistics, ICON Central Laboratories
Catherine Lund, Vice Chairman, OnQ Consulting
Cellia K. Habita, President & CEO, Arianne Corporation
Chris Tierney, Business Development Manager, EMEA Business Development, DHL Exel Supply Chain, DHL Global
Chris Tait, Life Science Account Manager, CHUBB Insurance Company of Europe
Deborah A. Komlos, Senior Medical & Regulatory Writer, Thomson Reuters
Elizabeth Moench, President and CEO of MediciGlobal
Eileen Harvey, Senior VP/General Partner, PRA International
Franz Buchholzer, Director Regulatory Operations worldwide, PharmaNet Development Group
Francis Crawley. Executive Director of the Good Clinical Practice Alliance – Europe (GCPA) and a World Health Organization (WHO) Expert in ethics
Georg Mathis, Founder and Managing Director, Appletree AG
Heinrich Klech, Professor of Medicine, CEO and Executive Vice President, Vienna School of Clinical Research
Hermann Schulz, MD, CEO, INTERLAB central lab services – worldwide GmbH
Janet Jones, Senior Director, ICON Clinical Research
Jerry Boxall, Managing Director, ACM Global Central Laboratory
Jeffrey Litwin, MD, F.A.C.C. Executive Vice President and Chief Medical Officer of ERT
Jeffrey W. Sherman, Chief Medical Officer and Senior Vice President, IDM Pharma.
Jim James DeSantihas, Chief Executive Officer, PharmaVigilant
Mark Goldberg, Chief Operating Officer, PAREXEL International Corporation
Maha Al-Farhan, Vice President, ClinArt International, Chair of the GCC Chapter of the ACRP
Nermeen Varawala, President & CEO, ECCRO – The Pan Emerging Country Contract Research Organisation
Patrice Hugo, Chief Scientific Officer,
Clearstone Central Laboratories
Rabinder Buttar – President & Chief Executive Officer of ClinTec International
Rick Turner, Senior Scientific Director, Quintiles Cardiac Safety Services & Affiliate Clinical Associate Professor, University of Florida College of Pharmacy
Robert Reekie, Snr. Executive Vice President Operations, Europe, Asia-Pacific at PharmaNet Development Group
Sanjiv Kanwar, Managing Director, Polaris BioPharma Consulting
Stanley Tam, General Manager, Eurofins MEDINET (Singapore, Shanghai)
Stefan Astrom, Founder and CEO of Astrom Research International HB
Steve Heath, Head of EMEA - Medidata Solutions, Inc
T S Jaishankar, Managing Director, QUEST Life Sciences
Volume 6 Issue 1 6 Journal for Clinical Studies
Editorial Advisor Keynote on our Five Year Anniversary
Congratulations on your loyalty to our Journal for Clinical StudiesYes, on behalf of the editorial board, I am happy to see that we have been able to meet our promise made five years ago in the foreword of the first issue of the Journal for Clinical Studies, published in September 2008. Since then, Our readers have had plenty of opportunities to enjoy reading our quarterly issues. It was a great pleasure at that time to be invited to write the first “Foreword”, and it is an even greater honour to recapitulate the last five-year period.
The last 20 issues did, of course, deliver input on regulations and implementation guidelines to comply with GCP standards. We wish to cordially thank all authors who shared their knowledge and expertise with our readers by providing practical information on areas ranging from risk evaluation to paediatric trials, outsourcing strategies and central laboratory services and logistics. They have written scientific articles describing innovative research approaches involving biomarkers, human cancer cell lines and stems, to name just a few.
Globalisation of clinical research is impacting our daily life. It is therefore not a surprise to assert that all geographic areas were covered, from Western, Central and Eastern Europe to North Africa, the Near and Middle East, India and China, Southeast Asia and Australia, Japan and, of course, The Americas.In addition to reading the printed issues, our readers may also enjoy the interactive use of our comprehensive website, www.jforcs.com, which extends the Journal’s content to provide information on industry events and gives access to videos and webinars.
The Managing Director and the Publisher, the Editor and her team, all of our creative staff and our Advisory Board - we all want to thank our readers for your loyalty. We also look forward to continuing delivering our promise to create enjoyable, interesting and high-quality articles in each and every future issue.
Dr Hermann Schulz, MD, Chief Executive Officer, INTERLAB central lab services worldwide GmbHEditorial Advisory Board Member

DORA WIRTH (LANGUAGES) LTDNo. 2 • 32 CAXTON ROADLONDON W12 8AJ • UK
TEL No. +44 (0)20 - 7229 4552FAX No. +44 (0)20 - 7727 0744E-mail: [email protected]: www.dwlanguages.com
Over 50 years of excellence in translation
solutions for...
Deliverin
gth
etr
ansl
ated
wor
dto
phar
mac
euti
cal c
ompa
nies
worldwide
n Regulatory Affairs
n Clinical Research
n Medical Research
n Manufacturing
n Medical Publishing
...in languages for
traditional and
emerging markets
DWL Ad Doc_DWL Ad Doc 20/12/2012 10:52 Page 1

Volume 6 Issue 18 Journal for Clinical Studies
Watch Pages
Specifying Therapeutic Area Standards for Clinical Research
In its efforts to facilitate clinical research and regulatory review of drugs and biologics, the US Food and Drug Administration (FDA) has launched a multi-year initiative to standardise key study data to therapeutic areas (TAs). Guiding the project is the Therapeutic Area Standards Initiative Project Plan, to provide the overall management framework for addressing and accomplishing the objectives of the fifth authorisation of the Prescription Drug User Fee Act (PDUFA V). Availability of the plan was announced in October 2013.1
Under the performance goals in PDUFA V, authorised in July 2012 as part of the Food and Drug Administration Safety and Innovation Act (FDASIA), the FDA agreed to prepare a project plan for developing distinct TA terminology standards using a public process that permits stakeholder input through open standards development organisations. The FDA invited this input at a November 2012 public meeting on the advantages and disadvantages of current and emerging alternatives for
the exchange of regulated study data.2,3 The TA project plan was developed based on the input received at that meeting and public comments submitted in response to a Federal Register notice on the prioritisation of TAs.4
The FDA anticipates that the TA standards should enable and enhance the ability to integrate, analyse, report, and share study data. For instance, standardised data elements and terminologies permit data from multiple trials to be grouped for analysis, and for the conduct of meta-analyses within and across drug classes. The agency’s Center for Drug Evaluation and Research (CDER) and Center for Biologics Evaluation and Research (CBER) first identified a set of TAs that could benefit from further standardisation in 2011, and organised them into three tiers of priority. Factors that were considered at the time included number and type of active investigational new drug applications (INDs), existing data standardisation projects underway, and industry input on drug development pipeline activity.
In March 2012, the FDA released an initial roadmap to display the TAs in priority groupings. Revised several

times since that release, the roadmap suggests a series of standardisation projects over time to achieve significant results by December 2017. The roadmap will be updated periodically with progress, opportunity, and additional information becoming available.
One of the FDA’s assumptions for the TA roadmap is that projects are scoped narrowly enough to be achievable within a 12-month period, and that subsequent projects would build on the results. The agency notes that there are many factors affecting the FDA and its external stakeholders that could impact the order in which projects are started. These factors include funds availability, subject matter expertise availability, and priority changes.
The FDA points out that the term “therapeutic area” also includes diagnostic and preventive areas. Some of the areas may represent a disease/domain area. As per an October 2013 update to the roadmap5,6, work has commenced on the following TAs and several are earmarked as “next priority” projects:
Among its other goals for the TA standards initiative, the FDA plans to implement binding guidance — “Providing Regulatory Submissions in Electronic Format–Standardized Study Data” (eStudy data guidance) — with a consistent and predictable approach. The final guidance (after public comment) will require that study data contained in new drug applications (NDAs), abbreviated new drug applications (ANDAs), biologics license applications (BLAs), and INDs be submitted electronically in a standardised format that the FDA can process, review, and archive. Furthermore, the guidance will provide the FDA’s current recommendations on the best means for implementing standardised study data.
Collaborators with the FDA on efforts to support development of the TA standards are the Clinical Data Interchange Standards Consortium (CDISC) and the Critical Path Institute. The FDA is also collaborating with the Clinical Interoperability Council of Health Level Seven (HL7) International and other consortia to define related clinical concepts.
Currently, the Coalition for Accelerating Standards and Therapies (CFAST) — an initiative sponsored by CDISC and the Critical Path Institute, with collaborators including the FDA, TransCelerate BioPharma Inc, and the National Cancer Institute Enterprise Vocabulary Services — is underway to coordinate TA development work streams leading to the delivery of standard data elements, concepts, and terminologies for each TA. Public comments on the TA project plan were accepted by the FDA until December 23, 2013 (Docket No. FDA-2013-N-1277).
References1. Federal Register: October 24, 2013 (Volume 78, Number
206/Pages 63481-63482) 2. Federal Register: August 14, 2012 (Volume 77, Number
157/Pages 48491-48492)3. Federal Register: September 17, 2012 (Volume 77,
Number 180/Page 57055)4. Federal Register: November 20, 2012 (Volume 77,
Number 224/Pages 69637-69638)5. Therapeutic Area Data Standards Roadmap (version 6,
10-29-2013)6. Table of Therapeutic Area (Disease/Domain) Data
Standards Prioritization (version 4, 10-29-2013)
Journal for Clinical Studies 9www.jforcs.com
Watch Pages
Deborah A. Komlos, MS, is the Senior Medical & Regulatory Writer for the Cortellis Regulatory Intelligence US Module at Thomson Reuters. Her previous roles have included writing and editing for magazines, newspapers, online venues, and scientific journals, as well as publication layout and graphic design work. Email: [email protected]

10 Journal for Clinical Studies Volume 6 Issue 1
Watch Pages
Cardiovascular Therapeutics Watch Page
Developing new single-drug and multi-drug therapeutic regimens for cardiovascular diseases (CVD) and obtaining marketing approval for them from regulatory authorities is clearly one central component of treating CVD. However, once these regimens are available to prescribing physicians and hence to their patients, their appropriate use becomes another central component of integrated pharmaceutical medicine1 (viable commercial-scale manufacturing can be regarded as a third component).
In the case of hypertension, appropriate prescription of therapeutic regimens that may include three, four, or more drugs can be challenging. The importance of successfully treating hypertension at the public health level is emphasised by articles published last year in the Lancet that addressed the designation of high blood pressure (BP) as the greatest threat to the global burden of disease.2-4 When discussing these papers, Dolan and O’Brien5 observed that “Ischaemic heart disease, ischaemic, non-ischaemic and haemorrhagic stroke, hypertensive heart disease, atrial fibrillation and flutter, peripheral vascular disease, aortic aneurysm, and chronic renal disease (to which we must now add cognitive impairment and dementia) are all attributed to hypertension.” They also noted the paradox of rampant hypertension in the presence of many pharmacological agents that, if used appropriately, provide therapeutic benefit. While additional drugs and particularly single-pill combinations with enhanced benefit-safety-value profiles are always welcomed,6 Nieuwlaat similarly commented that “Learning how to better implement effective therapies (for CVD) will have a larger effect on patient outcomes than most single new drugs and is a priority for tackling the global burden of CVD.”7
To help family doctors and general practitioners treat their patients most effectively, hypertension specialists who belong to related professional societies co-author guidance documents published by the societies in the medical literature. Examples include guidelines for the management of arterial hypertension prepared by a task force of experts from the European Society of Hypertension (ESH) and the European Society of Cardiology (ECS),8 and the recent ESH position paper on the use of ambulatory blood pressure monitoring
(ABPM) in both clinical research and clinical practice.9 A very recently published paper by Weber and colleagues10 is entitled “Clinical Practice Guidelines for the management of Hypertension in the Community: A Statement by the American Society of Hypertension and the International Society of Hypertension.” In addition, the Asia Pacific Society of Hypertension has endorsed the guidelines.
As noted in the paper’s statement of purpose, “These guidelines have been written to provide a straightforward approach to managing hypertension in the community. We have intended that this brief curriculum and set of recommendations be useful not only for primary care physicians and medical students, but for all professionals who work as hands-on practitioners.”10 These guidelines are therefore noteworthy for their pragmatic approach and their clear descriptions of challenges and potential solutions. The authors also recognise that there are major differences in resources among points of care in communities worldwide, making it inappropriate to attempt to dictate an inflexible single set of guidelines. They therefore acknowledge that “We expect experts who are familiar with local circumstances will feel free to help guide front-line practitioners in providing the best care possible.”10
The paper is divided into 15 sections that cover topics including the following: epidemiology of hypertension; definition, causes, classification, and diagnosis of hypertension; evaluating the patient, including physical examinations; treatment goals for patients with hypertension; non-pharmacologic and pharmacologic treatments; and treatment-resistant hypertension. As noted in the introductory section, approximately one-third of adults in most communities in the developed and developing world have hypertension, and hypertension is the most common chronic condition addressed by primary care physicians, general practitioners, and other health practitioners. The risk of adverse cardiovascular events, strokes, and kidney disease is lowest at a BP of around 115/75 mmHg, and for each increase above this value of 20 mmHg in systolic BP or 10 mmHg in diastolic BP the risk of major cardiovascular and cerebrovascular events doubles. With regard to both non-pharmacologic and pharmacologic treatments in patients diagnosed with hypertension, the figure in the paper summarises the main recommendations presented.
This paper is recommended reading for everyone interested in hypertension.
References1. Turner JR. Drug safety, medication safety, patient safety: An
overview of recent FDA guidances and initiatives. Regulatory Rapporteur. 2009;April issue:4-8.
2. Horton R. GBD 2010: understanding disease, injury, and risk. Lancet. 2013;380:2053-2054.

3. Das P, Samarasekera U. The story of GBD 2010: a “super-human” effort. Lancet. 2013;380:2067-2070.
4. Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013;380:2224-2260.
5. Dolan E, O’Brien E. Hypertension – the major cause of death and morbidity worldwide; where are our policy makers? Irish Medical Times. January 25th, 2013, page 33.
6. Turner JR. Patient and physician adherence in hypertension management. J Clin Hypertens (Greenwich). 2013;15:447-452.
7. Nieuwlaat R, Schwalm JD, Khatib R, Yusuf S. Why are we failing to implement effective therapies in cardiovascular disease? Eur Heart J. 2013;34:1262-1269.
8. Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25:1105-1187.
9. O’Brien E, Parati G, Stergiou, et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31(9):1731-68.
10. Weber MA, Schiffrin EL, White WB, et al. Clinical practice guidelines for the management of hypertension in the
community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich). 2014;16:14-26. Available at: http://onlinelibrary.wiley.com/doi/10.1111/jch.12237/full (Accessed 14th January 2014).
Watch Pages
J. Rick Turner, PhD, is Senior Scientific Director, Clinical Communications, Quintiles. He is an author/co-author of 130 papers, author/co-author of seven textbooks, and an editor/co-editor of five professional volumes. He is also a Senior Fellow at the Center for Medicine in the Public Interest, and a Fellow of the Society of Behavioral Medicine. Email: [email protected]
Philip Galtry is Vice President and Cardiovascular Therapeutic Strategy Head, Cardiovascular and Metabolic Therapeutic Delivery Unit, Quintiles. Philip holds an Honours degree in Biochemistry from the University of Bristol, UK, and has worked in the management of cardiovascular studies for almost 25 years.
www.paediatric-trials.co.uk BOOK BY 20TH DECEMBER AND SAVE £300 / BOOK BY 31ST JANUARY AND SAVE £100
Register online or fax your registration to +44 (0) 870 9090 712 or call +44 (0) 870 9090 711
REGISTER BY 20th DECEMBER 2013 AND RECEIVE A £300 DISCOUNTREGISTER BY 31ST JANUARY 2014 AND RECEIVE A £100 DISCOUNT
SMi present their 8th annual conference on… 31ST MARCH- 1ST APRIL
2014Paediatric Clinical Trials
PLUS AN INTERACTIVE HALF-DAYPOST-CONFERENCE WORKSHOPS
Wednesday 2nd April 2014,The Kensington Close Hotel, London, UK
Paediatric Drug Development & the PaediatricInvestigation Plan (PIP): Background,
Operational Challenges, Negotiation StrategyHosted by Klaus Rose, CEO, Klausrose Consulting
8.30am - 1.00pm
WHY ATTEND THIS EVENT:• Discuss the global paediatric legislations and an impact
assessment of the EU legislation• Learn about PIP submissions• Discover how the FDA changes the regulatory landscape for
paediatric drug development in the US• Explore how clinical trials are organised in Hungary• Analyse vaccines trials vs. antibiotic trials• Evaluate the experience of a paediatrics ethics committee• Examine extrapolation in paediatric drug development• Consider formulation development and paediatric
psychopharmacology
Sponsored by
The Kensington Close Hotel, London, UK
P-099_HPAd_IPIJournal 27/11/2013 18:10 Page 1

Watch Pages
12 Journal for Clinical Studies Volume 6 Issue 1
Clinical research used to be always carried out in the well-funded locations of North America and Western Europe, with a smaller number in Australasia. This is no longer the case because of several factors. Saturation is approaching in available sites in the West, which has led to a lack of naive patients available and willing to take part in trials. This has led companies to seek new locations to run trials, which is much easier than it used to be because of the huge improvements being made in emerging markets in investigator and patient identification and regulatory initiatives.
Countries like India and Brazil have invested in significant infrastructure programmes to improve the way that they handle clinical trials applications, including trial review, and the granting of import licences and permits. IMP supplies can be imported relatively quickly to allow trials to take place at the same time as those in Western Europe and North America. It is possible to make huge cost reductions by performing trials in Eastern Europe, Latin American and Asia. In Russia, China and other countries, it is possible to reduce operational costs and have trials conducted in large hospitals which have patient catchment areas numbering millions to speed patient recruitment.
Additionally, more countries have a requirement that clinical trials must be conducted in that country prior to marketing new drugs. Only once local testing has been done can an application for inclusion in the market be considered. China, for example, spent approximately 66.8 billion US Dollars in 20111 and that level of spend cannot be ignored by any company in the global marketplace.
There are a lot of new countries where trials are taking place; for example, in South America there are a total of 5432 trials, and in South East Asia there are 32502. The really interesting element is how many countries have started running trials. Brunei Darussalam, for example, has one carcinoma study running at the moment, and there are many other countries with small numbers of trials, which can only increase over time. The Middle East and Africa are showing significant growth in clinical trials numbers as the market looks for even more new destinations. Each of these countries represents challenges in logistics, ensuring temperature control, arranging customs clearance and regulatory release. There are many hazards in arranging shipping, requiring knowledge of local requirements, from how to address the package to what storage is available in individual airports.
If sending to Vietnam (and several other countries), you cannot address the package to an individual as it would be considered a personal package, even if a pallet
load, and the recipient is likely to become personally liable for any duty or taxes applied to the shipment. This can lead to problems making deliveries into a big hospital, particularly for time-/temperature-sensitive items, and clinical trial supplies being received into a pharmacy department being stored incorrectly, because personnel with knowledge about the specific storage requirements may not have been advised.
Clearance can take many days, depending on the infrastructure, number of clinical trial shipments arriving at any one time, type of supply and individual country regulations. During this time it may be possible to access the consignment to refresh refrigerant, but a lot of the time reliance is on the warehouse storage facility at the airport. In Cambodia, at Phnom Penh International Airport, there is no freezer, one refrigerator set at +2 to +8C: (4 x 3 x 2m, door size 1.8 x 1m) which is not qualified or controlled, and a ‘controlled ambient’ area set at +20 to +25C, which is also not qualified or controlled. Knowing this kind of information makes it possible to plan, choose the airport of entry, the packaging, and even the time of year to ship. Laos has three seasons in the year: hot, cold, and rainy (although the temperature is rarely below 15°C even in the cooler months). August and September see a significant rise in rainfall with frequent tropical downpours. Given the limited airport facilities and time that shipments can be left on the runway, it is probably prudent to send a couple of weeks early or later, if this can be factored into your plans.
The secret to successful shipping into emerging markets is forward planning and research, local contacts and knowledge, and a degree of flexibility and pragmatism.
References1. International Federation of Pharmaceutical
Manufacturers & Associations. The Pharmaceutical Industry and Global Health Report – Facts and Figures 2012
2. www.clinicaltrials.gov
Logistics in Emerging Markets Column
Sue Lee, Technical Portfolio Manager, World Courier Management, has worked for World Courier for 25 years. During this time she has experienced a variety of customer service and operational functions, including the setting up of numerous, multi national, clinical sites for the transportation of biological samples. She has orchestrated the shipping thousands of shipments with very specific temperature requirements to a host of challenging locations,
and each presenting their own obstacles and dilemmas. Email: [email protected]

INTERLABcentral lab services – worldwide
· 11 labs on all continents
· dedicated project management
· reliable shipping logistics
· broad analytical portfolio
CENTRAL LAB SERVICES FOR CLINICAL TRIALS
www.interlab.deEUROPE · THE AMERICAS · ASIA/INDIA/CHINA · AUSTRALIA · SOUTH AFRICA · NEAR/MIDDLE EAST
ILA-13-011_ANZ_JforCS_210x297+3.indd 1 22.07.13 12:54

Volume 6 Issue 114 Journal for Clinical Studies
Regulatory
India, with 1.21 billion people is the second most populous country in the world, representing almost 17% of the world’s population. Every year, an estimated 26 million children are born in India. With the increase in population, the demand for vaccines and medicines for paediatric care has also seen a significant rise.
India has been a favourite spot for the conduct of clinical trials due to the multitude of benefits it offers, like a large patient pool, low costs, and ethical flexibility. Advantages of ethical flexibility have been used and abused by many, desirous of conducting clinical trials and subsequently launching their drugs. There are no specific requirements, per se, for the conduct of clinical trials on the paediatric population. Even in routine practice there are no specific guidelines for prescribing the dosage regimen for paediatrics. The lack of child-specific guidelines has resulted in irrational use of drugs, leading to untoward drug reactions.
In contrast, in the United States, the Food and Drug Administration has a well-established department for regulation of drug development for paediatrics. In Europe, the European Medicines Agency (EMA) has various directives and paediatric investigation plans (PIPs). In Malaysia, the National Pharmaceutical Control Bureau (NPCB) has
issued paediatric protocols including drug development regulations. Likewise in India, the Central Drugs Standard Control Organization (CDSCO) can implement some regulations specifically for paediatric drug development.
With the proposed revamping of drug development guidelines in India, there is an acute need to address the situation and bring specific drug development guidelines to regulate and protect the interests of the paediatric population.
Keywords: paediatric, clinical trials, drug development guidelines.
Introduction:India, with 1.21 billion people, is the second most populous country in the world. The figures show that India represents almost 17% of the world’s population, which means one out of six people on this planet live in India1. Every year, an estimated 26 million children
are born in India, which is nearly 4 million more than the population of Australia. Every year, many children under five years of age die from pneumonia, diarrhoea, and neonatal causes. Many of these conditions could be treated with safe, effective medicines. Consequently, demand for various vaccines and child-specific medicines has increased exponentially.
However, these essential medicines are often not suitable for use in children. On the other hand, irrational use of the available drugs, and unavailability of paediatric-specific guidelines for drug development in India, have led to adverse drug reactions and drug resistance to the usual pathogens and infections by unusual organisms. Promotion of appropriate and safe drugs in children is the need of the hour in India.
Current Scenario in India:In India, paediatric drugs are developed based on
clinical trials and protocols for a healthy adult human. There are no specific drug development regulations for paediatrics. Indian clinical practice relies heavily upon safety and efficacy data published in other developed countries, or inference from adult dosing. Lack of paediatric-specific guidelines has led healthcare providers and caregivers to estimate the dose (either for therapeutic use or for carrying out clinical trials) by breaking tablets into quarters and halves, crushing tablets, or opening capsules, or if it is liquid, by proportionally reducing volume. Administering medicines in this way is difficult and can cause inaccurate dosing, which may result in reduced efficacy (due to under-dosing) and/or compromise safety (due to over-dosing).
Children are not small adults. They have different pharmacokinetic and pharmacodynamic responses as compared to adults. These differences are mainly due to differences in body water and serum protein composition in the paediatric population. In addition, children, particularly newborns, may suffer from illness specific to their age group that requires medicines not available for adults.
While the present regulatory guidelines for introduction of a new drug in India mandate exposure of the drug to the Indian adult population as part of a stand-alone trial or as part of a global clinical trial, but there is no mention of exposure to the paediatric population. Unfortunately, most of the drugs used in children have never been actually studied in this population. Clinical studies for establishing safety and efficacy of the drugs are generally carried out in adult subjects, and their safety and tolerability data are extrapolated for paediatric population. Even for some drugs for which clinical trials were conducted in paediatric populations, the trial protocols were based
Regulation for Paediatric Drug Development
in India: Need of the Hour

Journal for Clinical Studies 15www.jforcs.com
Regulatory
on general clinical trial guidelines. There are no specific regulations to conduct trials in the paediatric population, except for a clause in the informed consent form (ICF) that if paediatric patients are used then the ICF should be signed by parents or a legal guardian2. There is no specific regulation of dosing or sample collection from the population under consideration. The lack of such regulations may result in the Indian paediatric population ending up as guinea pigs in the hands of drug giants.
ADRs Related to Irrational Use of Drugs in ChildrenThere are many unpleasant yet avoidable adverse effects cases. Such incidents occurred mainly due to irrational use of drugs in children. These ADRs typically occur at lower doses than in adults, and symptoms may be atypical, with these ADRs possibly affecting normal growth and development.
Some severe ADRs related with commonly used drugs in paediatrics are:
1. Hepatotoxicity associated with the use of sodium valproate3.
2. Increased risk of Reye’s syndrome with the use of salicylates in children with viral infection4.
3. ‘Grey baby’ syndrome with chloramphenicol in neonates5.
4. Growth suppression/effects on adrenal function with long-term corticosteroids6.
5. Gastrointestinal bleeds with NSAIDs7.6. Risk of arthropathy due to use of ciprofloxacin in
children8.
Not only active ingredients but also excipients used to make formulations can lead to unpleasant experiences. Some commonly used excipients along with their ADRs are:
1. Benzalkonium chloride-induced bronchospasm from antiasthmatic drugs9,
2. Aspartame induced headache and seizures10, 3. Saccharin-induced cross-sensitivity reactions in
children with sulphonamide allergy9,4. Benzyl alcohol toxicity in neonates receiving
high-dose continuous infusion with preserved medications11,
5. Propylene glycol-induced hyperosmolality and lactic acidosis12.
Global ScenarioIn 1985, the World Health Organization (WHO) defined the rational use of medicines as “patients receiving medications appropriate to their needs, in doses that meet their own individual requirements, for an adequate period of time, and at the lowest cost to them and their community”13. Hence paediatric patients should have medicines according to their body requirements.
In many regulated and emerging countries, the Ministries of Health are taking appropriate steps for
safety of paediatric population and have framed essential paediatric specific guidelines.
The US Food and Drug Administration (USFDA) has come up with a separate department for paediatric drug development, namely the Office of Paediatric Therapeutics14. The FDA has proactively introduced the paediatric exclusivity (PE) clause within the Modernization Act (FDAMA)15. PE provides exclusive rights to the company to market a drug for an extended period of six months if the company undertook paediatric clinical trials. The paediatric rule (PR) introduced by the
FDA in 1999 mandated manufacturers to submit safety and effectiveness data on relevant paediatric age groups before approval. The Best Pharmaceuticals for Children Act (BPCA) was enacted on 4 January 2002 in the USA, shortly after the PE provision of the FDAMA expired16. The USFDA also published the final rule on 21 CFR 50 subpart D on February 29, 2013, describing Additional Safeguards for Children in Clinical Investigations of Food and Drug Administration-Regulated Products17.
The European Medicines Agency (EMA) has issued many directives for paediatric regulations. Directive 2001/20/EC18 Regulation lays down rules concerning the development of medicinal products for human use in order to meet the specific therapeutic needs of the paediatric population, without subjecting the paediatric population to unnecessary clinical or other trials; Regulation (EC) No 1901/200619 aims to facilitate the development and accessibility of medicinal products for use in the paediatric population, to ensure that medicinal products used to treat the paediatric population are subject to ethical research of high quality and are appropriately authorised, and to improve the information available on the use of medicinal products in paediatric populations. Directive EMEA/CHMP/PEG/194810/200520,

Regulatory
Volume 6 Issue 116 Journal for Clinical Studies
“Reflection Paper: Formulations of Choice for the Paediatric Population” assists in the development of paediatric formulations which enable neonates, infants and children of all ages, and their caregivers, to have access to safe and effective medication. The Guideline on the Investigation of Medicinal Products in the Term and Preterm Neonate21, which has Document Reference number EMEA/536810/2008, aims to provide guidance for the development of medicinal products for use in the neonatal period, defined as birth to 27 days post-natal age in term neonates, and birth to a post-menstrual age of 40 weeks and 27 days in preterm neonates. Guidelines EMEA/CHMP/PEG/194810/2005 and EMEA/536810/2008 have also been adopted22 by the Therapeutic Goods Administration (TGA), Australia, for welfare of their paediatric population.
In Malaysia, the government, along with the National Pharmaceutical Control Bureau (NPCB) and Malaysian Paediatric Association (MPA) has issued a paediatric protocol23 which includes drug development and daily therapeutic use regulations. The MPA has also issued many guidelines and articles such as Guidelines for the Management of Cow’s Milk Protein Allergy in Children24, Nutrition in the First 1,000 Days25, and Children in an Urban World: State of the World’s Children26 related to growth, development and nutrition needs of the paediatric population.
Some Recommendations to Address the Issues The paediatric population is a vulnerable group with significant differences in their developmental, physiological and psychological profiles as compared to adults. There is a need to address and consider these developmental differences during the drug research and development process.
As part of the ongoing organisation and revamp of regulatory guidelines to harmonise with global compliances by the Central Drugs Standard Control Organization (CDSCO), there is a strong need to include a paediatric drug development regulation, which in turn will yield more effective results without compromising the safety of the population under discussion.
The suggested paediatric drug development regulations should address:
1.Ethical issues and clinical trial design: a. There is a need to have a list of formulations only for
paediatric use which should be made available to all.b. There should be a paediatric-specific clinical trial
protocol which will prevent the use of children as guinea pigs in clinics.
2. Efficacy and safety compliance: a. Registration of drugs for paediatric use in the Indian
market should ensure safety and efficacy by various studies performed and reports collected from clinical trials.
b. Regulatory authority should be advised by a paediatric subcommittee on efficacy and safety of medicinal products (both new and old) in children.
c. Pharmacovigilance in paediatrics needs to be strengthened by creating awareness among healthcare professionals.
3. Marketing and prescribing of drugs:a. There is a need to establish a dedicated working group
that develops, reviews and consolidates guidelines for regulators and manufacturers on appropriate formulations for children (including consideration of cost-effective formulations, dosing device, pack size and volumes appropriate for children).
b. There is also a need for a working group to create awareness among physicians to prescribe suitable drugs only to the population under concern.
c. There is a need for a surveillance team to look for proper availability of drugs for paediatric use in the market with proper labelling.
Conclusion The paediatric population requires special considerations for prescription of medicines due to their underdeveloped physiologic systems. Any negligence of this very aspect can lead to often deleterious side-effects. For these very reasons there is a need to develop guidelines and regulations in India, similar to other regulated and emerging markets, for the welfare of the paediatric population.
References1. Government of India; Children in India 2012 - A
Statistical Appraisal; Ministry of Statistics and Programme Implementation, p.24
2. Government of India; Drugs and Cosmetics Rules, 1945, Ministry of Health and Family Welfare (Department of Health), 2005 (amended); p.510
3. Hepatotoxicity to sodium valproate: a review; Gut, 1984, 25, 673-681; available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1432377/pdf/gut00391-0101.pdf
4. Risk of Reye’s syndrome in children with viral infections; pharmacological weekly; available at www.pharmacologyweekly.com/custom/archived-content/pharmacotherapy/194
5. Mulhall A, De Louvois J, Hurley R; Chloramphenicol toxicity in neonates: its incidence and prevention; British Medical Journal; November 1983; 287; 1424-1427; available at http://europepmc.org/articles/PMC1549666/pdf/bmjcred00580-0030.pdf
6. Systemic side effects of inhaled corticosteroids in patients with asthma; Ronald Dahl; Respiratory Medicine (2006) 100, 1307–1317; available at http://www.cof.org.cn/pdf/2006/7/Systemic%20side%20effects%20of%20inhaled.pdf
7. Anyanwu LC, Mohammad AM; Gastrointestinal bleeding following NSAID ingestion in children; Annals of Paediatric Surgery: April 2013; 9(2);87–89; available at http://journals.lww.com/aps/Abstract/2013/04000/Gastrointestinal_bleeding_following_NSAID.11.aspx
8. Adefurin A et al; Ciprofloxacin safety in paediatrics: a

www.jforcs.com Journal for Clinical Studies 17
Regulatory
systematic review; Arch Dis Child (2011) ;96; 874–880; available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3155117/pdf/adc-96-9-874.pdf
9. ‘’Inactive’’ Ingredients in Pharmaceutical Products: Update (Subject Review) Committee on Drugs Pediatrics 1997;99;268; available at http://pediatrics.aappublications.org/content/99/2/268.full.html
10. Lipton RB, Newman LC, Cohen JS, Soloman S. Aspartame as a dietary trigger of headache. Headache. 1989 feb;29(2):90–92; available at http://www.ncbi.nlm.nih.gov/pubmed/2708042
11. Benda GI, Hiller JL, Reynolds JW. Benzyl alcohol toxicity: impact on neurologic handicaps among surviving very low birth weight infants. Pediatrics. 1986 Apr;77(4):507–512; available at http://www.ncbi.nlm.nih.gov/pubmed/2421231
12. Huggon I, James I, Macrae D. Hyperosmolality related to propylene glycol in an infant treated with enoximone infusion. BMJ. 1990;301: 19–20; available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1663354/pdf/bmj00187-0023.pdf
13. World Health Organization. The rational use of drugs. Report of the Conference of Experts. Geneva: WHO; 1985; available at http://apps.who.int/medicinedocs/documents/s17054e/s17054e.pdf
14. Office of Pediatric Therapeutics; USFDA; available at h t t p : / / w w w . fd a . g o v / A b o u t F DA / C e n t e r s O f f i c e s /O f f i c e o f M e d i c a l P r o d u c t s a n d T o b a c c o /OfficeofScienceandHealthCoordination/ucm2018186.htm
15. USFDA; Guidance for Industry, Qualifying for Pediatric Exclusivity, Under Section 505A of the Federal Food, Drug, and Cosmetic Act; available at http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/DevelopmentResources/UCM049924.pdf
16. Background of the Best Pharmaceuticals for Children Act; available at http://bpca.nichd.nih.gov/about/index.cfm
17. USFDA; Additional Safeguards for Children in Clinical Investigations; available at http://www.gpo.gov/fdsys/pkg/FR-2013-02-26/pdf/2013-04387.pdf
18. Directive 2001/20/EC of the European Parliament and of the Council; Official Journal of the European Communities; 1.5.2001; available at http://www.eortc.be/services/doc/clinical-eu-directive-04-april-01.pdf
19. Regulation (EC) No 1901/2006 of the European Parliament and of The Council; Official Journal of the European Union; 27.12.2006; available at http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2006:378:0001:0019:en:PDF
20. EMA, Reflection paper: formulations of choice for the paediatric population; CHMP; available at http://www.ema.europa.eu/docs/en_GB/document_l ibrary/Scientific_guideline/2009/09/WC500003782.pdf
21. EMA, Guideline on the investigation of medicinal products in the term and preterm neonate; CHMP; available at http://www.ema.europa.eu/docs/en_GB/d o c u m e n t _ l i b ra r y / S c i e n t i f i c _ g u i d e l i n e / 2 0 0 9 / 0 9 /WC500003750.pdf
22. Australian government therapeutic goods administration;
Clinical guidelines; European Union guidelines adopted in Australia; Paediatric guidelines; available at http://www.tga.gov.au/industry/pm-euguidel ines-adopted-clinical.htm#clinicalpaediatric
23. Paediatric Protocols for Malaysian Hospitals, Kementerian Kesihatan Malaysia, 3rd edition, 2012
24. Malaysian Paediatric Association (MPA); Guidelines for the management of cow’s milk protein allergy in children 2012; available athttp://www.mpaweb.org.my/file_dir/75773798250498e90c5be2.pdf
25. Malaysian Paediatric Association (MPA); Nutrition in the First 1,000 Days; Save the Children; available at http://www.mpaweb.org.my/file_dir/4070132745236bb80c9874.pdf
26. Malaysian Paediatric Association (MPA); Children in an Urban world : State of the World’s Children 2012; UNICEF; available at http://www.mpaweb.org.my/file_dir/1799433358513dde0b7d689.pdf
Achin Jain is currently a Post Graduate student at JSS College of Pharmacy, Mysore. He is graduated (B. Pharma) from JSS University, Mysore. He has published an article titled Formulation and Evaluation of Spray-Dried Esomeprazole Magnesium Microspheres in a reputed journal. email: [email protected]
M.P. Venkatesh is an Assistant Professor in Department of Pharmaceutics in JSS College of Pharmacy, Mysore. He has teaching experience of seven years. He has guided 12 M.Pharm candidates and authored 16 International and National publications in reputed journals. He has attended various national and international conferences and currently he is working on drug regulations in regulated countries. email: [email protected]
T. M. Pramod Kumar is Professor and Head in the Department of Pharmaceutics in JSS College of Pharmacy, Mysore. He has teaching experience of 20 years. He has guided 5 Ph. D candidates. He has authored 70 International and 50 National publications and has chaired scientific sessions nationally & internationally.email: [email protected]
S. Naveen Kumar works as Manager Regulatory Affairs at PharmaLeaf India Pvt. Ltd, Bangalore and has over fve years of experience in the field of regulatory affairs filing dossiers in regulated and emerging markets. He specializes in CMC, documentation of dossiers and is responsible for devising regulatory strategies for dossier filing and product launch.email: [email protected]

Volume 6 Issue 118 Journal for Clinical Studies
Regulatory
Risk-based Monitoring: Moving Forward
After issuance of the final guidance document by FDA on Oversight Of Clinical Investigations - A Risk-based Approach to Monitoring, biopharmaceuticals, medical device companies and CROs are actively embarking on this paradigm shift in clinical research to reap the benefits of risk-based monitoring (RBM). The correct identification of study-specific risks, their sources, categorisation and implementation of risk-based study-specific monitoring strategies, plans are the critical components in implementation of the RBM approach to ensuring high quality, integrity of data, and enhanced human subject protection. With the introduction of centralised monitoring along with on-site monitoring, it is imperative to ponder restructuring of processes, people alignment, and the necessary technology requirements to maximise effectiveness of risk-based monitoring.
Considering the importance and current interest related to RBM in the clinical research industry, Cecilia Stroe, Editor of Journal of Clinical Studies, talks with Ashok Ghone, Ph.D, VP-Global Services, MakroCare, USA on the subject of RBM.
Cecilia: What is risk-based monitoring? Ashok: Risk-based monitoring is all about taking a holistic approach to assess all possible risks related to your study/program planning, conduct, reporting, and then having a proper plan for risk management, which includes systematic monitoring and controlling risks throughout the study or programme. The risk-based monitoring focuses on preventing and mitigating risks to data, processes which are important to achieve study or programme objectives. It is more of a dynamic approach using other monitoring methodologies like centralised monitoring, which facilitates timely, continuous improvement in trial conduct and overall management to enhance data quality and patient safety.
C: How is the clinical research industry looking into RBM?Ashok: The industry is certainly looking into RBM as a good opportunity to improve the overall quality of study conduct, management, reporting, patient safety, and reduce operational cost. As we all know, a typical efficacy clinical trial involves monitoring visits to investigational sites every four to eight weeks for source data verification (SDV). However, the studies/surveys have shown that 100% SDV does not necessarily result in higher data quality. Therefore there is a need for a smart way of monitoring study data by adopting alternative methods and using advanced technology like electronic data capture (EDC), modern data analytics and electronic source documents to ensure improved data quality and patient safety. Moreover, an EMA reflection paper, MHRA Risk-adapted Approaches, and the recent final guidance document from the FDA, encourage and provide further thrust to the industry to adopt an RBM approach to achieve these benefits. The key here is to understand the RBM perspective correctly and implement the best practices of RBM as it involves some of the challenges related to change management like restructuring of operational processes, role
changes, people training, and alignment and use of right technology. Improved data quality, integrity and patient safety are important outcomes of the RBM approach, but it will also help in reducing cost and creating operational efficiencies which have been the ongoing endeavours of clinical R & D for the last few years.
C: What are the key aspects involved in RBM implementation?Ashok: Risk assessment and risk management are the two important aspects of risk-based monitoring. It is necessary to identify root causes and sources of all potential risks, and then look into the impacts or consequences of these risks to categorise them as high (critical), medium or low risks. Once you identify, assess and categorise the risks in terms of consequence and probability of occurrence, or assign them some risk scores, the next step is management of risks. It means to have a robust plan for tracking and controlling risks throughout the study, i.e., what can be done to lessen the impact or probability of occurrence; whether all planned actions are being implemented and effective. The risk assessment and management are dynamic, continuous processes. One needs to monitor and keep asking questions, such as – is the original risk under control? have any changes occurred? are there any new risks? to ensure effective implementation of a risk-based approach. Developing an effective, comprehensive monitoring plan with a balance of on-site and centralised monitoring is vital in successful implementation of RBM. The other important steps of RBM implementation are re-organising operational processes due to introduction of centralised monitoring, managing changes in roles, responsibilities and communication models, people’s training, and selecting the right technology for centralised monitoring.
C: Which are the high-risk data or procedures that one needs to focus on more during risk-based monitoring?Ashok: It is important to identify high (critical) risks up front and then efficiently monitor those risks throughout the study to ensure high quality and integrity of data. The examples of some of the high-risk data like subject eligibility, data related to primary and secondary endpoints, adjudications, randomisation, patient discontinuation and SAE/AE data etc. Similarly, some of the examples of study-related critical procedures are like the ICF procedure, study-related key intervention procedures; e.g., for a CNS study, if MRI needs to be taken exactly one hour after a study drug intake then it becomes critical procedure for efficacy evaluation of the study drug; or examples of other procedures like withdrawal of blood samples at exact point intervals for PK analysis or safety investigations. Similarly, timely reporting of SAE or drug intake as per protocol requirement are the other examples of critical procedures for the study. The criticality of clinical trial data varies study to study, e.g. patient weight can be low or medium risk data for some studies, but it will be high risk data for a clinical trial where the study drug has significant

effect on patient weight. One has to have a systematic and complete study-specific monitoring approach through the combination of centralised and on-site monitoring to monitor these critical data and procedures throughout the study. On-site monitoring time should be used effectively and efficiently to carry out SDV of these critical risk data and procedures to build data quality and ensure patient safety.
C: Could you please comment on requirements of a monitoring plan while implementing an RBM approach? Ashok: The development of a detailed monitoring plan is a crucial part of implementation of RBM. The monitoring plan should provide the clear direction on how you would monitor and control high, medium and low risks related to clinical investigations once you identify and assess risks for your study/programme. With the inclusion of centralised monitoring in the RBM approach, the monitoring plan needs to define clearly the timing, frequency, extent and types of monitoring approaches i.e. on-site and centralised monitoring, that should be used for a given study. It should clearly state what should be achieved through centralised monitoring and what should be monitored on-site, so that one would not only reduce the number of on-site visits but also build higher data quality. It should explain what would be the criteria of findings of centralised monitoring that would trigger change in planned monitoring visits to sites, e.g. some of the findings may just require telephonic discussion with sites as a part of corrective action, whereas some of the events/findings may require changes in monitoring visit schedules or immediate visits to a site to avoid major quality issues and protect the wellbeing and safety of subjects. As we have a routine monitoring visit report template, the monitoring plan should also provide a template to report the findings of centralised monitoring. It also outlines the process of communication with different stakeholders, i.e. what should be the communication plan between the centralised monitoring team and on-site monitors to convey the findings of centralised monitoring to take necessary actions with investigational sites, especially when you are working on large multi-country, regional/global studies. It should list the team members involved in centralised monitoring. It should also delineate their exact roles and responsibilities, and the specific training requirements for a centralised monitoring team. The monitoring plan should also have provision to make amendments based on the new risks identified related to data, procedures, sites or overall operations. Of course, like a traditional monitoring plan, an RBM plan should also describe audit and co-monitoring plans, and processes for addressing significant issues with root cause analysis to build the overall quality in monitoring activities.
C: What is the significance of centralised monitoring in RBM implementation? Ashok: Centralised monitoring should be used effectively to achieve most monitoring aspects remotely. Most of the monitoring activities can be accomplished easily and in a better way by centralised monitoring, such as standard data checks, consistency, completeness of data, and monitoring site performance metrics such as screening failure rate, recruitment, drop-out rate, protocol deviations/violations,
and thereby identifying higher risk sites. Another effective use of centralised monitoring is to identify data trending, e.g. efficacy, safety data trending, AE/SAE trending, distribution, outliers etc. In fact, certain data anamolies like fabrication of data and non-random distribution data can be more easily detected efficiently by centralised monitoring than by on-site monitoring. The ultimate objectives of centralised monitoring should be early detection of risks, issues related to safety, quality, and overall operations, and also increasing the effectiveness of on-site monitoring.The availability of a proper collaborative and analytical e-tool is essential for effective centralised monitoring here, which can collaborate and integrate different e-clinical systems like EDC, CTMS and ePRO, where appropriate study data can be pooled in to provide the required analytical reports to monitor and control various risks. The collaborative and analytical tool should be able to generate various site performance metrics and data trending to generate early signals about quality, safety and operational issues.
C: What metrics should the industry observe while implementing an RBM approach?Ashok: Appropriate implementation of an RBM approach results in high quality and integrity of study data, better human subject protection, and reduced number of on-site visits, and creates cost-efficiencies in overall clinical trial operations. The points listed below are some of the metrics helpful to assess the effectiveness of the RBM approach. The metrics should be compared with a sponsor’s earlier similar studies with a traditional monitoring approach.
Quality metrics like • Reduction in number of protocol deviations/violations • Reduction in number of DCFs
Safety metrics like• Reduction in safety reporting deviation • Reduction in number of patients discontinuing/dropping
out due to AEs/SAEs
Timelines metrics like • Reduction in number of days in database lock from LPLV • Reduction in timelines from DCFs generation to resolution
Budgetary metrics like• Reduction in number of total monitoring visits • Reduction in number of on-site monitoring FTEs • Reduction in overall clinical trial management cost
Journal for Clinical Studies 19www.jforcs.com
Regulatory
Ashok Ghone, Ph.D. is Vice-President, Global Services at MakroCare USA. He has around 20 years of experience in pharmaceutical and clinical research industry. He carries good knowledge & understanding of global clinical research with hands-on experience in clinical operations, project management, process development, site management and patient recruitment activities. He has led various cross-functional teams successfully by providing strategic direction, guidance for accomplishment of local, regional and global projects involving early & late phase clinical studies
in various therapeutic areas. Email: [email protected]

Regulatory
Volume 6 Issue 120 Journal for Clinical Studies
Regulatory agencies worldwide play a critical role in healthcare as independent reviewers and approvers of applications made by sponsors to conduct clinical trials and ultimately to market a drug for a particular indication. In this context, the term sponsor generally refers to a biopharmaceutical company that is developing a new molecular entity (NME), but it can also refer to a group of clinical investigators who wish to conduct clinical trials of a drug that is already marketed, in order to investigate its potential benefits for a different indication.
Before a sponsor submits a request to a regulatory agency for a new drug to be registered for human use in the agency’s jurisdiction, a tremendous amount of highly specified in vitro and non-human animal testing (which together comprise a drug’s non-clinical development programme) and clinical research needs to be performed. The later aspects of non-clinical development and all aspects of clinical research fall under regulatory governance, as does the manufacturing process. We cannot over¬emphasise the importance of ensuring that development programmes meet regulatory expectations. In all cases, procedures and results must be documented appropriately; from a regulatory perspective, if research is not well documented, for all intents and purposes it has not been done. In many cases, regulatory agencies encourage sponsors to seek their input prior to embarking upon large components of a development programme, so that the sponsor and agency can develop a mutual understanding of the programme’s goals.
This commentary presents an overview of the regulatory landscapes for new drug development in the United States (US), Japan, and the European Union (EU), the three geographic regions that came together to form the International Conference on Harmonisation of the Technical Requirements for Registration of Pharmaceuticals for Human Use, a title abbreviated simply as ICH.1 Increasingly, the active participation of non-ICH regions in the development of new guidelines (and revisions of existing ones) is being sought. Initiated in 1990, ICH has various goals, key among which is encouraging the implementation and integration of common standards. Since sponsors frequently wish to market a new drug in multiple countries, a harmonised development programme is of considerable benefit in facilitating a more timely introduction of new therapies, and hence their availability to patients. To this end, ICH Tripartite Harmonised Guidelines were developed to describe requirements for various aspects of drug development programmes: non-clinical; chemistry, manufacturing, and controls (CMC); and clinical. In addition to the Safety, Quality, and Efficacy guideline categories, which cover non-clinical, CMC, and clinical topics, respectively, there are also Multi-disciplinary guidelines such as those describing the timing for non-clinical studies relative to clinical trials and the Common Technical Document submission structure. These guidelines have been adopted by individual regulatory agencies, who may also issue regional guidances on specific topics, both of which guide
biopharmaceutical research and development activities in their respective jurisdictions. In addition, sponsors ‘translate’ the guidelines into standard operating procedures (SOPs) tailored to their individual organisation; SOPs provide a greater level of operational detail, and multiple SOPs may be necessary to support an overarching ICH guideline.
Bringing new drugs to global markets increasingly requires collaboration between multiple stakeholders that includes regulatory agencies. As Grignolo2 observed, “The future of the medicines landscape must evolve toward a more collaborative framework, where regulatory agencies will pursue a greater degree of convergence and where sponsors, regulatory agencies, and payers, as essential stakeholders, will undertake drug development with reimbursement in mind to achieve the common global goal of bringing safe, effective, and affordable medicines to the world’s people.” It is our experience that collaboration between regulatory agencies and sponsors is already occurring, utilising mechanisms such as pre-investigational new drug and end of Phase 2 meetings and special protocol assessment in the US, consultations on clinical trials in Japan, and requests for scientific advice and protocol assistance in the EU. Recent communications from regulatory agencies demonstrate continued support for cooperative and innovative approaches.3 Despite these valuable collaborations, however, differences between regional regulatory authorities still exist, as evidenced by the following overview of the US, Japanese, and European regulatory landscapes. The US Food and Drug AdministrationThe US Food and Drug Administration (FDA), housed within the Department of Health and Human Services, is one of several agencies in the executive branch of the US government charged with implementing statutory laws created by the legislative branch, which it does by creating regulations or administrative law. The FDA is responsible for ensuring that regulated medical products comply with public health laws and regulations, and it is therefore a law enforcement agency with both administrative and judicial means at its disposal. It typically attempts to achieve compliance with its statutes using administrative means, e.g., inspections of products and manufacturing facilities, notices of violation of regulations, and recalls of marketed regulated products. However, if deemed necessary, it can utilise the US court system and the Department of Justice’s assistance to invoke its judicial tools, including seizure, injunction, and prosecution.4
Results from a drug’s CMC and non-clinical development programme are reported to the FDA in an investigational new drug application (IND). This document is reviewed to see if clinical trials should be allowed to start. FDA reviewers have 30 days to respond to the sponsor following submission of the IND. If a sponsor has not been contacted in that timeframe they have implied permission to commence their clinical development programme as described in the IND. Prior to submitting an IND,
The Role of Regulatory Agencies in New Drug Development: A Global Perspective

Journal for Clinical Studies 21www.jforcs.com
Regulatory
a sponsor may request a pre-IND meeting with FDA to obtain answers to specific questions they have regarding their CMC, non-clinical and clinical development plans.
The purpose of an IND is to provide detailed documentation in four broad areas:
• Manufacturing information. These data address the composition and stability of the drug, as well as the process and controls used for its manufacture.
• Animal pharmacology and toxicology studies that have been completed. These non-clinical data permit an assessment of whether the product is considered to be reasonably safe for initial testing in humans.
• Clinical study protocol(s). Protocols include precise accounts of the design, methodology, and analysis considerations necessary to conduct the proposed clinical trials and analyse their results.
• Investigator information. Information on the qualifications of clinical investigators is provided to allow assessment of whether they are qualified to fulfill their duties at the investigational sites used during the clinical trials.
The clinical protocol included in an initial IND is usually for a Phase 1 study designed primarily to collect safety data on the drug, and oftentimes it will be the first time the drug will be administered to humans. Later, when the sponsor is ready to progress to Phase 2 and ultimately pivotal Phase 3 studies, the protocols for these trials are submitted to the same IND, along with any additional supporting CMC and non-clinical data that have been generated. Unlike with the original submission of the IND, the sponsor may commence these subsequent studies upon receipt of the protocol by FDA, rather than waiting for a 30-day review period; however, FDA retains the ability to halt the trial or request a protocol amendment upon their review. In reality, there is generally some lag time between the submission and dosing of patients due to the logistics of initiating clinical sites and the desire of some sponsors to allow for a preliminary FDA review of the protocol.
After completion of the clinical trials conducted under an IND (and completion of all non-clinical studies being conducted contemporaneously: some of the more lengthy and costly animal studies are performed in parallel with clinical trials), a new drug application (NDA) is filed for small-molecule drugs and a biologics license application (BLA) for a biologic. FDA recently published a guidance that summarises four programmes available to expedite development of drugs to treat serious conditions.3 In addition to having these programmes, it is a common practice for sponsors to have an End of Phase 2 meeting with FDA to discuss how best to design and conduct the pivotal Phase 3 trials. Sponsors will then typically meet again with the FDA after the completion of all clinical trials to discuss the content and format of an NDA/BLA prior to its preparation. These meetings can be crucial for the sponsor to understand how to best facilitate the review process for a given submission. The FDA’s review of the NDA/BLA determines whether it finds the evidence concerning safety, efficacy, and manufacturing ability to be compelling, and if it is therefore
prepared to approve the drug for marketing. After approval of a drug, FDA reviews post-marketing safety surveillance data that it receives in the form of individual adverse events reports submitted by patients, healthcare providers, and the sponsor, as well as periodic safety update reports from sponsors.
The Japanese Pharmaceuticals and Medical Devices AgencyLike the FDA, the Japanese Pharmaceuticals and Medical Devices Agency (PMDA) regulates medical products in a single country or jurisdiction. As noted by the PMDA’s Chief Executive, Dr Tatsuya Kondo, the agency takes a drug lifecycle approach and focuses on three key areas: “relief services for adverse health effects, product reviews, and post-marketing safety measures.”5 Because the agency is responsible for providing relief compensation for sufferers from adverse drug reactions and infections caused by biopharmaceutical products, this “safety triangle” is unique to Japan.5
A second notable aspect of the PMDA’s operations was detailed recently by Asahina et al.6 While all concerned would agree with the authors’ assertion that “Drug monitoring after regulatory approval, mainly in terms of safety under conditions of actual use, is as essential as evaluating data before marketing [approval],” the PMDA has formalised re-examination and re-evaluation systems that “play important roles in continuously ensuring the positive benefit-risk balance of drugs in Japan.” At a specified timepoint following marketing approval (which is eight years for an NME) a sponsor must submit all available information that has been accumulated since approval, and the PMDA determines whether or not unacceptable risks associated with the product have occurred in clinical practice.6
In addition to the emphasis placed on safety, PMDA offers consultations regarding clinical trials, advising sponsors how to improve the trial. In 2009, PMDA also began to offer consultations on clinical trial data prior to submission for marketing approval. The European Medicines AgencyUnlike the FDA and PMDA, the European Medicines Agency (EMA) brings together the scientific resources of multiple nations, namely the member states of the EU, of which there are 28 as of the writing this commentary in January 2014.7 Sponsors submit a clinical trial application (CTA) to the individual member states in which they intend to conduct the clinical trial. In March 2014, Parliament will vote on revisions to the EU clinical trial regulations that would enable a single application to be filed through a central portal, and would designate one country to lead the review process and coordinate the input from the other countries. In contrast to an IND, a CTA is protocol-specific; therefore, one must be filed for each study a sponsor wishes to conduct, and hence a collection of CTAs accumulates during a clinical development programme. A separate document, called an investigational medicinal product dossier (IMPD), is submitted with the CTA and contains summaries of CMC, non-clinical, and any previously generated clinical data, as well as an assessment of overall risks and benefits. This document is updated as the development programme progresses, but unlike a US IND, full non-clinical study reports are not included.

Regulatory
Volume 6 Issue 122 Journal for Clinical Studies
Scientific advice on the acceptability of any particular clinical trial can be sought from the regulatory agencies of the individual member states in which the trial is to be conducted, but because of the potential for the drug to be approved for marketing throughout the EU via the centralised procedure (described in due course), sponsors often seek scientific advice/protocol assistance for development programmes from the EMA. Having the prospective input of the EMA on a clinical programme is valuable, because the EMA is the agency that will review the centralised application and recommend to the European Commission whether or not the drug should be approved. When a clinical development programme is completed for a new drug or biologic, a marketing authorisation application (MAA) is submitted.
There are multiple submission routes for MAAs: the centralised authorisation procedure, the decentralised authorisation procedure, the mutual recognition procedure, and the national authorisation procedure. The centralised procedure, initiated in 1995, leads to a single marketing authorisation that is valid in all EU countries. The centralised procedure is compulsory for various drug classes, including, for example, those for HIV/AIDS, cancer, diabetes, neurodegenerative diseases, auto-immune and other immune dysfunctions, viral diseases, and rare diseases (‘orphan diseases’). The centralised procedure, in which the European Commission grants marketing authorisations for all countries in the EU, is intended to allow a sponsor to begin making the drug available to patients and healthcare professionals in all EU member states, but it carries with it the risk that if some countries raise objections during the procedure that impact the vote, then approval is not possible in individual countries. For drugs not falling within the specified classes for which the centralised procedure is mandatory, sponsors can choose which route to follow: national, centralised, decentralised, or mutual recognition. The latter two are closely related in that the sponsor selects the member states from which it seeks approval for the drug, and a single country, the reference member state (RMS), leads the assessment process and coordinates input received from the other countries, the concerned member states (CMSs). The decentralised procedure, which has been available since 2006, is distinguished from the older (1995) mutual recognition procedure, in that it is for products that do not yet have any national approvals, whereas the mutual recognition procedure can be used to expand approval to other EU countries after attaining approval in a single EU country (national approvals can no longer be sought after approval in the first EU country; the mutual recognition procedure must
be used). When a choice between the centralised and the decentralised or mutual recognition routes is possible, a sponsor will weigh various strategic factors, including medical practice in the different countries, manufacturing plans, market forces, and its size, resources, and strengths in the EU.
After approval of a drug, the national regulatory agencies review post-marketing safety surveillance data including individual adverse events reports as well as periodic safety update reports (PSURs) submitted by sponsors (for centrally approved drugs, PSURs are reviewed by EMA).
References 1. ICH home page. Available at: www.ich.org (Accessed 2nd
January 2014).2. Grignolo A. Collaboration and convergence: Bringing new
medicines to global markets in the 21st century. Therapeutic Innovation & Regulatory Science. 2013;47:8-15.
3. FDA. Guidance for Industry. Expedited Programs for Serious Conditions -- Drugs and Biologics. Draft, June 2013. Available at: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM358301.pdf (Accessed 2nd January 2014).
4. Turner JR. New drug development: An introduction to clinical trials, 2nd Edition. New York: Springer, 2010.
5. Message from the Chief Executive, PMDA. Available at: http://www.pmda.go.jp/english/about/message.html (Accessed 2nd January 2014).
6. Asahina Y, Tanaka A, Uyama Y, Kuramochi K, Maruyama, H. The roles of regulatory science research in drug development at the Pharmaceuticals and Medical Devices Agency of Japan. Therapeutic Innovation & Regulatory Science. 2013;47:19-22.
7. European Union web page. Member countries of the European Union. Available at: http://europa.eu/about-eu/countries/member-countries/ (2nd January 2014).
TABLE 1: Documents and Websites for the Regulatory Agencies Discussed
J. Rick Turner, PhD, is Senior Scientific Director, Clinical Communications, Quintiles. He is an author/co-author of 130 papers, author/co-author of seven textbooks, and an editor/co-editor of five professional volumes. He is also a Senior Fellow at the Center for Medicine in the Public Interest, and a Fellow of the Society of Behavioral Medicine. Email: [email protected]
Theo J. Hoofwijk, M.D. is Executive Director, Therapeutic Strategy Development, Quintiles. He has over 20 years of pharmaceutical industry and CRO experience, encompassing virtually all areas of Phase I to Phase 4 clinical research. He has supported the development of numerous new drugs, designing and writing study protocols, Investigator Brochures, Master Development Programs, final Clinical Study Reports, and Safety Update Reports. He also serves as Regional Chief Medical Officer, upholding the ethical
stewardship of studies, protecting subjects, and ensuring appropriate medical governance of Quintiles in Europe, Africa, and the Middle East.Email: [email protected]
Robin Huff, Ph.D. Global Regulatory Strategy Lead Robin provides strategic drug development advice, shaping clinical development programs with global regulatory strategies that consider commercial implications and minimize timelines, while maintaining a high likelihood of regulatory acceptance. In her ten years in the biopharma industry, she developed strategies for a wide variety of clinical programs, and negotiated their acceptance by US FDA, EMA and national regulatory authorities.
Robin began her career as a reviewer and then supervisor at the US FDA.Email: [email protected]
Robin Huff, Ph.D. Global Regulatory Strategy Lead Robin provides strategic drug development advice, shaping clinical development programs with global regulatory strategies that consider commercial implications and minimize timelines, while maintaining a high likelihood of regulatory acceptance. In her ten years in the biopharma industry, she developed strategies for a wide variety of clinical programs, and negotiated their acceptance by US FDA, EMA and national regulatory authorities. Robin began her career as a reviewer and then supervisor at the US FDA.

2013 022 VC adv A4.indd 1 20-06-2013 12:56:33

Volume 6 Issue 124 Journal for Clinical Studies
Market Report
Iran Interest
Why Conduct Clinical Research in Iran• Huge untapped population• All clinical phases from Phase I-IV, genetic, and
observational studies can be conducted in Iran • Clear process of regulatory application for clinical studiesQuick Facts about Iran • Known as Persia until 1935, Iran became an Islamic republic
in 1979• Population: 79,853,900 (July 2013 est.) 1
• Capital: Tehran
IntroductionThe process of application for a clinical study in Iran is quite clear, however the final approval to start a study can vary from 6-8 months, depending on the final approvals from each committee.
Iran Registry of Clinical Trials (IRCT)Any clinical trial that will be conducted in Iran has to be uploaded to the IRCT website.
The process of registering a trial is as follows: 2
1. Register with IRCT website and set up an account.2. IRCT staff will get back to you when the information you
have provided has been verified and accepted.3. You can proceed if you are eligible to do so. The chief
investigator or representatives of the sponsor are among those who can register a trial.
4. You then need to enter all the required information.5. The information will be verified by IRCT staff. When all
information is complete, you will be given your registration ID with IRCT.
6. You then need to keep your trial record up to date by updating your trials when any of the characteristics of your trial, such as design or timings, have changed.
The main objectives of this are:-• Informing public of ongoing trials.• Increasing public awareness of their importance. • Implementing the International Committee of Medical
Journal Editors’ initiative for mandatory registration of trials before the enrolment of the first patient.
Regulatory and Ethics Committees in Iran Food and drug organisation is the regulatory authority for the approval of the clinical study after the approvals of the local ethics committee and the national ethics committee. There are a few research institutions or treatment centres, either governmental or private, that have their own research ethics committee or a review board with ethics review capabilities.
However, the institutions are within the territory of a medical university and, with their vice-chancellery of research, are authorised to assess/approve research projects, and they are the primary references for research proposals.
Each medical university is responsible for a defined geographical area, and covers all private and governmental health/treatment centres in that area. For international or multicentre studies, a further approval from the national ethics committee (NEC) should support the primary approval of the institution or local university’s vice-chancellery. Hence, the local ethics committee communicates its decision to the national ethics committee, along with the supporting documents of the submission package.
Procedure1. The principal investigator submits the documents which,
will include the standard protocol, case report form, investigator brochure etc. to the local ethics committee. Usually the meetings of the local ethics committee are every month.
2. After approval from the LEC, the PI submits all the documents to the national ethics committee (NEC) - this committee meets once every three months.
3. After the NEC approval, all the study materials should be uploaded on the Iranian Clinical Trial Registry (IRCT) website.
4. Submit all the documents along with the NEC approval for the final approval from the Food and Drug Organization.
5. After the final approval from the Food and Drug Organization, the study can be initiated at the site.
Approximate TimelinesConclusion
A lot of pharmaceutical companies are considering Iran as a good and strong site for clinical research.
References1. Cnn.com2. http://www.irct.ir/
Authority TimelineLocal Ethics Committee 1-1.5 monthsNational Ethics Committee 2-2.5 monthsFood and Drug 2-4 months
Adhiti Sharad Kumar, has been working for a clinical research organization, and has been involved in the regulatory, training and marketing activities. Currently, she is also the Coordinator for the Gulf Chapter of the Association of Clinical Research Professionals – ACRP. This group is focused on promoting clinical research around the Gulf, and involves training sessions, networking events, etc. Email: [email protected]

M EENClinical
OrganizationRESEARCH
Site Selection & Feasibility
Monitoring
Site Management
Regulatory Management
Project & Quality Management
Warehouse Consultancy & Training
Pharmacovigilance
Data Management, EDC & Statistics
h DTurkis rug and
c
Medical Devi es Agency
A P OVP R ED
Phase I-V
Medical Devices
PMS
Exportation& Destruction
Delivery
Collection
Reconcilliation
COMPARATORSOURCING
STORAGE FACILITIES DISTRIBUTION
Controlled Substances(2-8 C and 15-25 C)oo
15-25 CAmbient Room
0
2-8 CCold Room
0
2-8 C BiologicalMaterial Cold Room
0
IMPORT & EXPORT
CUSTOMS CLEARENCE
IMPORT
LICENCE
APPLICATION
LABELLING
ACCOUNTABILITY
depot meridian
Clinical Trial Supplies Management Solutions
depot meridian
since 2002
HQ Office:
GOSB Technopark
Gebze-Kocaeli
TURKEY
UK Office:
Leatherhead
Surrey
UNITED KINGDOM
USA Office:
UMBC Baltimore
MD, 21228
USA
www.meneresearch.com
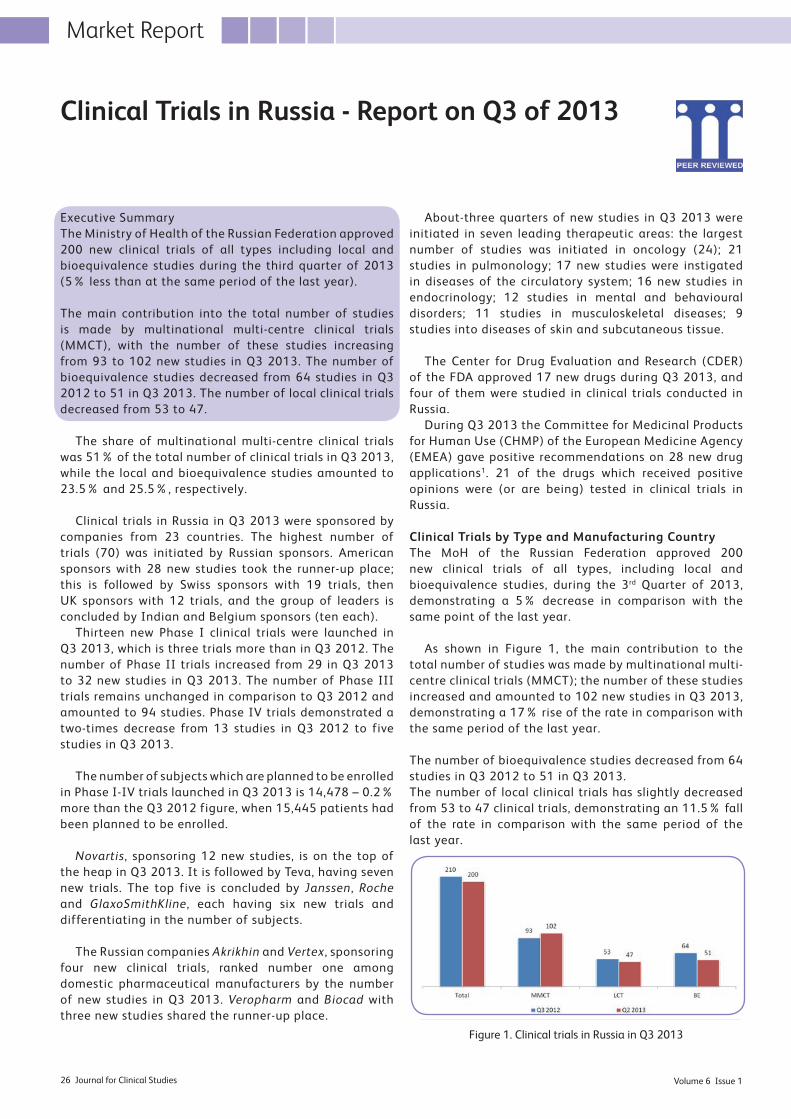
Volume 6 Issue 126 Journal for Clinical Studies
Market Report
Executive SummaryThe Ministry of Health of the Russian Federation approved 200 new clinical trials of all types including local and bioequivalence studies during the third quarter of 2013 (5% less than at the same period of the last year).
The main contribution into the total number of studies is made by multinational multi-centre clinical trials (MMCT), with the number of these studies increasing from 93 to 102 new studies in Q3 2013. The number of bioequivalence studies decreased from 64 studies in Q3 2012 to 51 in Q3 2013. The number of local clinical trials decreased from 53 to 47.
The share of multinational multi-centre clinical trials was 51% of the total number of clinical trials in Q3 2013, while the local and bioequivalence studies amounted to 23.5% and 25.5%, respectively.
Clinical trials in Russia in Q3 2013 were sponsored by companies from 23 countries. The highest number of trials (70) was initiated by Russian sponsors. American sponsors with 28 new studies took the runner-up place; this is followed by Swiss sponsors with 19 trials, then UK sponsors with 12 trials, and the group of leaders is concluded by Indian and Belgium sponsors (ten each).
Thirteen new Phase I clinical trials were launched in Q3 2013, which is three trials more than in Q3 2012. The number of Phase II trials increased from 29 in Q3 2013 to 32 new studies in Q3 2013. The number of Phase III trials remains unchanged in comparison to Q3 2012 and amounted to 94 studies. Phase IV trials demonstrated a two-times decrease from 13 studies in Q3 2012 to five studies in Q3 2013.
The number of subjects which are planned to be enrolled in Phase I-IV trials launched in Q3 2013 is 14,478 – 0.2% more than the Q3 2012 figure, when 15,445 patients had been planned to be enrolled.
Novartis, sponsoring 12 new studies, is on the top of the heap in Q3 2013. It is followed by Teva, having seven new trials. The top five is concluded by Janssen, Roche and GlaxoSmithKline, each having six new trials and differentiating in the number of subjects.
The Russian companies Akrikhin and Vertex, sponsoring four new clinical trials, ranked number one among domestic pharmaceutical manufacturers by the number of new studies in Q3 2013. Veropharm and Biocad with three new studies shared the runner-up place.
About-three quarters of new studies in Q3 2013 were initiated in seven leading therapeutic areas: the largest number of studies was initiated in oncology (24); 21 studies in pulmonology; 17 new studies were instigated in diseases of the circulatory system; 16 new studies in endocrinology; 12 studies in mental and behavioural disorders; 11 studies in musculoskeletal diseases; 9 studies into diseases of skin and subcutaneous tissue.
The Center for Drug Evaluation and Research (CDER) of the FDA approved 17 new drugs during Q3 2013, and four of them were studied in clinical trials conducted in Russia.
During Q3 2013 the Committee for Medicinal Products for Human Use (CHMP) of the European Medicine Agency (EMEA) gave positive recommendations on 28 new drug applications1. 21 of the drugs which received positive opinions were (or are being) tested in clinical trials in Russia. Clinical Trials by Type and Manufacturing CountryThe MoH of the Russian Federation approved 200 new clinical trials of all types, including local and bioequivalence studies, during the 3rd Quarter of 2013, demonstrating a 5% decrease in comparison with the same point of the last year.
As shown in Figure 1, the main contribution to the total number of studies was made by multinational multi-centre clinical trials (MMCT); the number of these studies increased and amounted to 102 new studies in Q3 2013, demonstrating a 17% rise of the rate in comparison with the same period of the last year.
The number of bioequivalence studies decreased from 64 studies in Q3 2012 to 51 in Q3 2013. The number of local clinical trials has slightly decreased from 53 to 47 clinical trials, demonstrating an 11.5% fall of the rate in comparison with the same period of the last year.
Clinical Trials in Russia - Report on Q3 of 2013
Figure 1. Clinical trials in Russia in Q3 2013

The proportions between different study types (multinational multi-centre clinical trials, local studies and bioequivalence trials) slightly changed since last year (see Figure 2).
The share of multinational multi-centre clinical trials studies stayed almost at the same rate: 51% of the total number of clinical trials approved in Q3 2013. The share of the local trials increased at 23.5%, and the share of bioequivalence studies decreased from 30% to 25.5% of the total number of trials approved during Q3 2013.
The proportions between sponsors did not significantly change in comparison with the same period last year. 65% of the total number of new studies in Q3 2013 is sponsored by foreign companies, which is 130 study approvals. The share of studies of local manufacturers insignificantly decreased and amounted to 70 studies (Figure 3).
Clinical trials in Russia in Q3 2013 were sponsored by companies from 23 countries. Figure 4 demonstrates the input of the leading countries of sponsors’ origin into the total number of clinical trials. The highest number of trials (70) was initiated by Russian sponsors. American sponsors with 28 new studies took the runner-up place; they are followed by Swiss sponsors with 19 trials, then by UK sponsors with 12 trials, and the group of leaders is concluded by Indian and Belgian sponsors (ten trials each).
Among others are: France (eight), Germany and Israel (seven trials each), Denmark (six), Austria and Ukraine (three studies each), Belarus, Hungary, Slovenia, Czech
Republic, Japan and Croatia (two trials each), Poland, Italy, Romania, Bulgaria and Sweden each started one new study in Q3 2013.
Clinical Trials by PhaseThe number of Phase I clinical trials changed insignificantly and stood at 13 new studies in Q3 2013. The number of Phase II trials increased from 29 in Q3 2012 to 32 new studies in Q3 2013 (Figure 5).
The number of Phase III trials remains unchanged in comparison to Q3 2012, and amounted to 94 studies. Phase IV trials demonstrated a more than two-times decrease from 13 studies in Q3 2012 to 5 studies in Q3 2013.
1Studies indicated by sponsors as Phase I-II in the applications
submitted to MoH are shown in Phase II studies group; Phase II-III
in Phase III group; Phase III-IV in Phase IV group. BE studies were
not included in any phase group, even in case a specific phase was
indicated in the application.
As shown in Figure 6, the share of Phase III trials in Q3 2013 is 66% of the total number of studies; the share of Phase II trials accounts for 22%, Phase I trials is 9%, and the share of Phase IV studies amounts to 3%.
Figure 2. Clinical trials by type in Q3 2013
Figure 3. Russian and international sponsors in Q3 2013
Figure 4. Countries presented on the Russian clinical trials market in Q3 2013
Figure 5. Clinical trials in Russia in Q3 2013 by phase11
Figure 6. The proportions between study phases in Russia in Q3 2013
Journal for Clinical Studies 27www.jforcs.com
Market Report

Volume 6 Issue 128 Journal for Clinical Studies
Market Report
The number of subjects which are planned to be enrolled in Phase I-IV and BE trials launched in Q3 2013 is 15,478, 0.2% more than in Q2 2012, when 15,445 patients were planned to be enrolled.
312 subjects will be recruited in Phase I trials; 2074 patients in Phase II trials; 10,692 subjects in Phase III studies and 631 patients will be enrolled in Phase IV studies. Other subjects (1769) are healthy volunteers and patients who will enter bioequivalence studies.The minimal number of subjects in a single study is one; the maximum number is 1200.The proportion of the number of patients between different phases is shown in Figure 7. Only studies in which phase is specified were included.
Rating of International SponsorsNovartis, sponsoring 12 new studies is on the top of the heap in Q3 2013. It is followed by Teva having seven new trials. The top five is concluded by Janssen, Roche and GlaxoSmithKline, each having six new trials and differentiating in the number of subjects.
The top five international sponsors by the number of new studies in Q3 2013 are presented in Table 1.
Rating of Russian Sponsors
The Russian companies Akrikhin and Vertex, sponsoring four new clinical trials, ranked number one among domestic pharmaceutical manufacturers by the number of new studies in Q3 2013. Veropharm and Biocad, with three new studies, took the third and fourth places. Seven companies (Mir Pharm, Pharma Bio, Atoll, Nativa, F-Syntez, Pranapharm, Pharmsyntez) with 2 new studies each share the fifth place.
Therapeutic Areas of Clinical Trials in Russia in Q3 2013About three-quarters of new studies in Q3 2013 were initiated in seven leading therapeutic areas: the largest number of studies was initiated in oncology (24); 21 studies in pulmonology; 17 new studies were instigated in diseases of the circulatory system; 16 new studies in endocrinology; 12 studies in mental and behavioural disorders; 11 studies in musculoskeletal diseases; 9 studies in diseases of the skin and subcutaneous tissue.The proportions between different therapeutic areas are shown in Figure 8.
Clinical Trials Results
The Center for Drug Evaluation and Research (CDER) of the FDA approved 17 new drugs during Q3 2013; four of them are new molecular entities (NME); others are new dosages, manufacturers or indications of the already marketed drugs. FOUR drugs were studied in clinical trials involving Russian sites.
The Table 3 shows the drugs which were approved by FDA in Q3 2013 that were being tested in clinical trials in Russia.
During the third quarter of 2013 the Committee for Medicinal Products for Human Use (CHMP) of the
Figure 7. The number of patients in Q3 2013 by study phase
Table 1. Top 5 international study sponsors in Q3 2013
Table 2. Top 5 Russian study sponsors in Q3 2013
Table 3. New drugs approved by FDA in Q3 2013 and tested in Russian sites
Figure 8. Clinical trials in Russia in Q3 2013 by therapeutic area

Market Report
Journal for Clinical Studies 29www.jforcs.com
European Medicine Agency (EMEA) gave positive recommendations on 28 new drug applications1 . 21 of the drugs which received positive opinions were (or are being) tested in clinical trials in Russia (see Table 4).
Igor Stefanov, MBA. CEO graduated from the Moscow Aviation Institute in 1989. After the collapse of the Soviet Union he received an MBA degree in Economics at the Moscow International University in 1993 and went into the business consulting area developing and implementing localization strategies for the Fortune 500 companies in Russia comprising Big Pharma representatives including Pfizer, J&J, GlaxoSmithKline, Roche and others. Prior to joining SynRG in January 2007,
Igor served as General Manager for SmartLock, the Russian hi-tech biometric company and was recognized as an entrepreneur of the month by the Russian edition of Forbes magazine in 2005.Email: [email protected]
Table 4. New Drugs approved by EMEA in Q3 2013 and tested in Russian sites

Market Report
Volume 6 Issue 130 Journal for Clinical Studies
A recent announcement from Estonia discussed the launching of the first human stem cell production laboratory in the Baltic Statesi. A closer look reveals that the number of GMP laboratories for human stem cell production in Europe is quite limited. An event of this type indicates, or leads one to believe, that there should be more going on in the background. This overview introduces the cell therapy situation in Estonia.
Estonian Cell Therapy ClusterBehind the launching of a GMP lab for human stem cell production is a wider initiative. In 2011, the Estonian Cell Therapy Cluster i i was established with the support of Enterprise Estonia. Represented among its members are both public and private institutions, with the University of Tartu and Tallinn University of Technology on the standards, research, and academic side. Tartu University is not only Estonia’s leading centre for research and training, but also logically important to the Cluster because the university’s Faculty of Medicine is the only source of medical doctors in Estonia. The second group includes private and non-profit research institutions: Protobios LLC, Cellin Technologies LLC, Labas Ltd, Kevelt Ltd, EGeen Ltd and the Competence Center for Cancer Research. They each contribute according to their competence: immunoprofiling, cancer research, stem cell separation, growing techniques, cryopreparations, CRO skills, and so on. The third group involves the hospitals that combine medical research with daily medical care. These partners are: Tartu University Hospital; the Hospital for Reconstructive Surgery; The Hospital of Orthopaedics; and The Hospital Vitaclinika. Any kind of stem cell treatment starts and ends in hospital. And, last but not least, the Cluster also includes Biolaborid LLC, which runs the GMP lab for human stem cell production that was mentioned earlier. Funding from the European Regional Development Fund, via Enterprise Estonia (EAS), was used to build up the GMP lab. The Fund also supports the entire Cluster project through EAS.
The Estonian Cell Therapy Cluster’s main objective is the development of the field of cell therapy. The measures supporting this main objective have been grouped into three main aims, namely:
• Internationalisation of the cell therapy field in Estonia, which consists of increasing the volume of both output and export, the creation of additional jobs, and the creation of increased added value;
• improving the quality of human resources; • supplementing regulations and legislation in the fields of
cell therapy and regenerative medicine.
The point of bringing all of the Cluster’s activities together is the creation of treatment opportunities, and consequently the starting up of a research-intensive export possibility for the Estonian medical services, as well as the creation of high-added-value jobs. One of the driving forces here is notifying the public – including the public sector, doctors and patients – about new treatment methods, and ensuring that they have access to cell therapy products and services.
First Estonian Stem Cell TransplantationThe first transplantation in Estonia of a patient’s own stem cells to diseased areas of the body to heal damaged tissues and organs was presented as a medical case at the symposium entitled Stem Cells: A Breakthrough in Regenerative Medicine in 2013.
In stem cell treatment, human fat tissue is used in an entirely new way by using the fat itself, which is a valuable substance. Hospitals apply the technology and devices developed by Cytori Therapeutics to extract from the fat those cells that have a regenerative ability, or, put it simply, stem cells. The patient’s own stem cells are concentrated and then transplanted to diseased parts of the body to cure them.
The first surgery in Estonia with the use of autologous, i.e. the patient’s own, cells which have this regenerative ability was performed at the Hospital of Reconstructive Surgery on 16 April 2013. The patient was an 18-year-old girl with burn injuries. Before the surgery she could not straighten her fingers, her wrist had limited mobility, and the epidermis previously transplanted to her forearm to cure serious burn wounds limited mobility as well. She found it painful to move her hand.
The patient has now undergone four surgeries at the Hospital of Reconstructive Surgery. The first was to straighten the patient’s fingers that were badly clenched and to give her the ability to straighten them more easily. The second, most important surgery involved transplanting stem cells to the patient’s fingers to prevent a new cicatrisation process and to restore the natural elasticity of the skin and subcutaneous tissue. The patient’s hand has been returned to full functionality. In June and August, an additional amount of autologous fat tissue was transplanted to the forearm, which further reduced cicatrisation and improved blood flow in the tissues of the forearm.
The left-handed patient is now able to fully straighten the fingers of her left hand, her wrist has regained normal mobility, the dense and rigid scar on her forearm has softened, and the girl, engaged in the art of dancing, is now free from pain and able to perform a bridge stand.
I hope that this example will encourage you to believe in the future of stem cell treatment.
What Should be Done in order to Develop Something New in the Field of Cell Therapy?Stem cell therapy holds the promise of treating degenerative diseases and cancer, and repairing damaged tissues, for which there are currently no or limited therapeutic options available. Despite the clinical potential of stem cell-based medicinal products, there are also potential and unanticipated risks. These risks deserve a thorough discussion within the purview of current scientific knowledge and experience. An evaluation of the potential risks should be a prerequisite before any clinical use of stem cell-based medicinal products.
The risk profile of stem cell-based medicinal products
Developing a New Branch of Medicine: Cell Therapy in Estonia

Market Report
Journal for Clinical Studies 31www.jforcs.com
depends on many risk factors, which include the type of stem cells, their differentiation status and proliferation capacity, the route of administration, the intended location, in vitro culture and/or other manipulation steps, irreversibility of treatment, the need or possibility for concurrent tissue regeneration in the case of irreversible tissue loss, and the long-term survival of engrafted cells. Together, these factors determine the risk profile associated with a stem cell-based medicinal product. The identified risks (i.e. risks identified in clinical experience) or potential/theoretical risks (i.e. risks observed in animal studies) include tumour formation, unwanted immune responses, and the transmission of adventitious agents.
The vast majority of small-scale clinical trials conducted with mesenchymal stem/stromal cells (MSC) in regenerative medicine applications have not reported major health concerns, suggesting that MSC therapies are relatively safe. However, in some clinical trials, serious adverse events have been reported, which emphasises the need for additional knowledge, particularly with regard to biological mechanisms and long-term safetyi i i. The previously mentioned aspects, together with the traditionally highly-regulated environment of medicine, describe quite well the complexity of the cell therapy world. In order to develop a new and very promising branch of medicine, very close cooperation between all responsible disciplines is required.
Here, a group of Estonian scientists and doctors noticed the potential of Estonia. Its medical and scientific community is relatively small and located in close proximity to one another, which should increase the number of opportunities for co-operation.
Since being established in 2011, much has been done. Thanks to the Cell Therapy Cluster initiative, a solid foundation has been laid for cooperation between surgeons from leading hospitals and cell biologists, geneticists, lawyers, educational authorities, and many others. In cooperation with the relevant health authorities, the group has prepared a broader input for Parliament for the appropriate legislative format, among other concerns. Several research projects have been launched in order to assess the properties of adipose tissue mesenchymal stem cells and culture conditions for developing further practical applications. One of these, submitted by the Hospital of Reconstructive Surgery, would identify molecular and cellular mechanisms that control survival, homing, and differentiation of adipose tissue mesenchymal stem cells (AdMSCs). Results of the current project will serve as the foundation for the development of clinical technology and protocols for the effective isolation of therapeutic AdMSCs, the conditioning of isolated cells in differentiating into specific cell types – for instance, growing blood vessels for patients suffering from diabetes or ischemia. The same GMP laboratory will play an important role in every such project, in order to ensure that every new promising solution may be used in humans. It can also be reported that successful transplantation operations, helping patients with large-scale burns and also in treatment of further scar formation, have taken place using the patients’ own stem cells taken from adipose tissue.
Bearing in mind that cell therapy, with its capabilities, presents new and unknown territory for the general public and also for the majority of healthcare workers, the Cluster has organised a series of conferences targeted at both researchers and doctors, in which the developments and views of cell therapy from all over the world have been introduced, and activities in this area in Estonia have also been presented. Simultaneously, all the information has been shared via the media with the public to
create awareness of cell therapy among the Estonian public. It is necessary to introduce recent and future developments in this field on how patients might be treated with cells found in their own bodies to the public.
Educational View and Recent PublicationsCell therapy, as a field located on the boundary between medicine and science, has set high requirements for specialists. In addition to a professional background and a degree in biology, medicine, or a related field, they need to possess further knowledge about the legislative framework and problems that need to be overcome before a scientific solution can be implemented in practice. Similar concerns are also shared about officials from state agencies, who need to be educated in the basic aspects of biology and the main processes in stem cell production. This field is completely new globally. To this end, the Cluster partners, led by Tallinn University of Technology, have created the necessary input to open a Master’s programme at the universities, as well as to launch training courses for the public. This is expected to happen within the next two years.
Some might believe that Estonia is incapable of contributing to standard research, but this is certainly not the case. Within the last three years, six solid papers have been publishedivin the field of cell therapy. A recently defended PhD thesisv opens the topic of self-renewal and the differentiation of stem and progenitor cells. This particular paper also determines the role played by these cells in the maintenance and regeneration of adult tissues. Taking into account the potential practical value of that paper, it is certainly worth its own separate paragraph.
It is known that mesenchymal stem cells (MSCs) are cells residing in adult tissues, which can proliferate and differentiate into a minimum of three specialised mesodermal cell types, namely adipocytes, osteoblasts and chondrocytes. These qualities cause MSCs to be regarded as potential candidates for cell therapy applications in regenerative medicine. Numerous tissues in the adult body have been found to contain MSC-like cells, including subcutaneous adipose tissue, which holds great promise for therapeutic applications as an easily accessible source of MSCs. However, the molecular characteristics of these cells have been poorly understood. In vitro cultures of adult stem cells exhibit a high degree of heterogeneity in the gene expression of individual cells, as well as in proliferation and differentiation dynamics. However, via manipulation of different cellular signalling systems, cell populations with specific characteristics can be developed for cell therapy applications.
Using various research techniques, including analysis of gene expression in individual cells, and multiplex RNA-seq analysis of whole transcriptomes, followed by a large-scale data analysis, some key aspects of the principles of molecular control in the cell fate decisions of human MSCs have been identified. The most important finding is that, in addition to the expected gene expression heterogeneity between cell populations of distinct tissue origin (adipose-derived MSCs, AdMSCs; and dermal fibroblasts, FBs), and between cells of different donors, dynamic transitions between different cell states of individual stromal cells generate temporal heterogeneity within single cells and spatial heterogeneity between cells of the same population. The results demonstrate that cellular plasticity is a common and inherent property of stromal cells, including AdMSCs and FBs, which can develop into diverse cell types upon stimulation from appropriate extrinsic stimuli.

Market Report
Volume 6 Issue 132 Journal for Clinical Studies
What to Expect in the Near FutureThe vision of the Estonian Cell Therapy Cluster foresees that the fields of regenerative medicine and cell therapy will become the cornerstones of Estonian biotechnology exports in the near future. Cluster members will be the developers of innovative therapies and technologies, as well as the implementers and users of the latter solutions and service offers.
The Cluster has a cleanroom laboratory meeting all GMP standards, which is required for the production of stem cells for use in clinical applications. The human cell therapy laboratory has the latest equipment for R&D activities, in order to prepare for (pre)clinical research as well as to train laboratory specialists according to GMP rules. It offers GMP cleanroom services at grade A level, with a grade B background, accordingly. Taking into account that this type of laboratory still belongs to the “lacking resources” category, they may expect to find another reason for interest in cooperative activities from abroad.
Specific master’s programmes in universities, as well as training courses for the public, will help to further develop the field. Within the next two months, another 5000 square metres of new modern laboratory space will be given for the use of the translational medicine field, which means better conditions for standard research in Estonia.
In addition, this will help interactions with the public in creating awareness and building the necessary relationships between the public and future treatments. The latter is obligatory for the time when new therapies start becoming available.
E-country and E-medicine“e-Estonia” is a term commonly used to describe Estonia’s emergence as one of the most advanced e-societies in the world – an incredible success story that grew out of the partnership between a forward-thinking government, a pro-active ICT sector, and a switched-on, tech-savvy population. Thanks to this success, Estonians and the Estonian state enjoy a wide range of e-solutions that those living elsewhere can only dream aboutvi. For the citizens of Estonia, e-services have become routine: e-voting, e-taxes, e-police, e-healthcare, e-banking, and e-school. The “e” prefix for services has almost become trite in the sense that it has become the norm. Most Estonians would not even consider doing things the old-fashioned way, such as physically visiting an office when the process could easily be completed onlinevi.
The Estonian EHR (Estonian Health Record) is a globally unique enterprise. It encompasses the whole country, registers virtually all residents’ medical history from birth to death, and is based on the comprehensive state-developed basic IT infrastructurevii.
Estonia has an “X-road” – a platform-independent standard interface for secure data processing, connecting all Estonian public-sector databases and information exchanges. In addition, there is the Estonian ID card, which, combined with a smart card reader, acts as a secure electronic identification method – something which needs to be in place in order to guarantee security at the receiver’s end. Estonia also uses a digital prescription system, eliminating the need for paper prescriptions, and thereby decreasing the level of bureaucracy in doctors’ and pharmacists’ work processesvii.
Effective use of resources thanks to e-solutions should accelerate research efforts. Estonian Cell Therapy Cluster would like to use historically strong medical community from one hand and the strenght of small community and its recently invented e-tools from another, in order to develop a new branch of medicine.
References i. http://news.err.ee/v/economy/ef1834e8-831f-4068-a400-
0b68bef13db7ii. http://www.celltherapycluster.eu/en/about-us.html. Visited
23.01.2014iii. Herberts, C.A. et al. Risk factors in the development of stem cell
therapy. J. of Translational Medicine 2011, 9:29 doi:10.1186/1479-5876-9-29.
iv. 1. Protein kinase inhibitor SU6668 attenuates positive regulation
of Gli proteins in cancer and multipotent progenitor cells. Piirsoo A, Kasak L, Kauts ML, Loog M, Tints K, Uusen P, Neuman T, Piirsoo M. Biochim Biophys Acta. 2014 Jan 10
2. Variable expression of lineage regulators in differentiated stromal cells indicates distinct mechanisms of differentiation towards common cell fate. Jääger K, Fatkina A, Velts A, Orav E, Neuman T. Gene. 2014 Jan 1;533(1):173-9.
3. Alternative splicing targeting the hTAF4-TAFH domain of TAF4 represses proliferation and accelerates chondrogenic differentiation of human mesenchymal stem cells. Kazantseva J, Kivil A, Tints K, Kazantseva A, Neuman T, Palm K. PLoS One. 2013 Oct 2;8(10):e74799.
4. CCL5/CCR1 axis regulates multipotency of human adipose tissue derived stromal cells. Kauts ML, Pihelgas S, Orro K, Neuman T, Piirsoo A. Stem Cell Res. 2013 Mar;10(2):166-78.
5. RNA-seq analysis reveals different dynamics of differentiation of human dermis- and adipose-derived stromal stem cells. Jääger K, Islam S, Zajac P, Linnarsson S, Neuman T. PLoS One. 2012;7(6):e38833.
6. Human dermal fibroblasts exhibit delayed adipogenic differentiation compared with mesenchymal stem cells. Jääger K, Neuman T. Stem Cells Dev. 2011 Aug;20(8):1327-36.
v. Jääger, K. Differentiation and Heterogeneity of Mesenchymal Stem Cells. http://digi.lib.ttu.ee/i/?929. Visited 23.01.2014
vi. http://estonia.eu/about-estonia/economy-a-it/e-estonia.html. Visited 23.01.2014
vii. http://e-estonia.com/news/12-03-15/future-medicine-ehealth-and-mhealth visited 23.01.2014
Andrus Loog, MD, Cardiovascular surgeon, member of the board of Estonian Cell Therapy Cluster, founder and member of the board of the Hospital of Reconstructive Surgery since 1993. The Hospital of Reconstructive Surgery is the leading clinic in Estonia in the fields of cardiovascular surgery and plastic reconstructive surgery.
He graduated from the Faculty of Medicine at the University of Tartu in 1987. Between 1991 and 1992, he continued his
studies at the University of Texas in the USA, and worked as a visiting surgeon at the Texas Heart Institute. Dr. Loog is the chairman of the board of the Estonian Society of Vascular Surgeons, and a member of the Estonian Society of Plastic and Reconstructive Surgery and the European Society for Vascular Surgery.

More information:www.worldcourier.com
When everything stopsWorld Courier keeps you on schedule.
About GxP
“GxP” is a collective term for the Good Practice quality guidelines and regulations used in many fi elds, encompassing such internationally recognized standards as GMP (Good Manufacturing Practice), GCP (Good Clinical Practice), GSP (Good Storage Practice) and GDP (Good Distribution Practice). These guidelines are designed to ensure that products are safe, meet their intended use and, in regulated industries such as drugs, food, medical devices and cosmetics, adhere to quality processes during manufacturing, control, storage and distribution.
World Courier – logical risk reduction globally
GxP_Ad_Flight_Board.indd 1 04.07.13 11:13IPI December 2013.indd 69 23/12/2013 14:13:17

Therapeutics
Volume 6 Issue 134 Journal for Clinical Studies
Alzheimer’s Disease Without Dementia:
A New Journey of CareAlzheimer’s has been described as a medical gremlim, feared by many and never far from the headlines. When the general public (in the UK and USA) were surveyed about their future health worries, Alzheimer’s ranked as the leading concern for the over 50s, surpassing both cancer and heart disease, and despite the fear over Alzheimer’s, social stigma and misunderstanding about this and other neuro-degenerative conditions persists, resulting in delayed diagnosis or — equally problematic — a diagnosis where the full extent of Alzheimer’s is not revealed to the patient or family.
Social stigmas are all too familiar in healthcare; one only needs to look at cancer and heart disease, where in the 1980s attitudes parallel to Alzheimer’s today can be seen. It is ironic that while Alzheimer’s is the most written-about disease in the mainstream press, the focus of most journalistic reporting is centred on the failings in dementia care, the miracle benefits of certain exotic foods, and new research discoveries that are years away from even Phase I clinical trials. Conversely, in the trade press, the focus centres on the debate about diagnosis rate (which is variable and frequently reported as lower in the UK than Continental Europe and the USA), the benefits/penalties of screening for dementia, and the accuracy and validity of epidemiological statistics and resulting implications for health policy.
A plurality of clinical views, research agendas, and competing pathways of care is (in our view) a healthy state of affairs. It provides opportunities to compare and contrast different approaches to care and management of Alzheimer’s patients. But this can be confusing to the general public, and this confusion is further compounded by the pace of evolution in understanding the biology of Alzheimer’s and other neuro-degenerative conditions. Furthermore, today’s advances in diagnostic tools and new therapies are in turn resulting in the emergence of new evidence.
Unfortunately, much of this debate, varied opinion and new diagnostic tools distracts from the fact that we are on the cusp of a revolution in the diagnosis, treatment and long-term management of Alzheimer’s disease. The next five to seven years purports a transformation; from short-term treatment of symptoms to a long-term ‘stable state’ resulting in living with Alzheimer’s without dementia. Importantly, sustaining this state for a significant period of time enables patients to prolong their maintenance of daily function, which in turn extends quality of life for patients as well as their families.
Chronic medical conditions are some of the biggest healthcare challenges facing society, and the management of Alzheimer’s can and should evolve to a position of proactive management similar to the evolution of diabetes care. There are major challenges to overcome in achieving this, especially in the UK, but healthcare delivery models for managing Alzheimer’s without dementia are emerging.
Consider the following example: A 53-year-old woman visited her family doctor complaining of anxiety and difficulty coping at work, especially with issues related to financial planning. An MRI brain scan reported normal findings, and while not obviously depressed, the woman was treated with different psychological therapies and subsequently antidepressant drugs, over the following five years, without success. Gradually progressive memory loss and other cognitive problems ensued such that, three years after initial presentation, the woman was unable to work in finance. Within five years she had significant difficulty managing daily tasks. A second MRI scan was performed and again reported as normal. Without a diagnosis, the patient was referred to a London-based medical centre in central London called Re:Cognition Health, specialising in neuro-degenerative disorders.
Current diagnosis of Alzheimer’s relies largely on documenting mental decline. While there are currently no validated biomarkers for Alzheimer’s disease, several promising approaches can be conducted by specialists. Research suggests that Alzheimer’s disease in its earliest stages may cause changes in CSF levels of tau and beta-amyloid, two proteins that form abnormal brain deposits which are very strongly sensitive and specific for Alzheimer’s disease.
Clinical assessment confirmed a significant decline in cognitive function. Diagnostic tests including a mini mental state examination (MMSE) indicated moderate impairment with a score of 22/30. The MRI scan was repeated to specifically include a volumetric analysis of the hippocampi. This additional brain scan was aimed at examining whether atrophy was present. If so, this would be indicative of Alzheimer’s disease (Figure 1). The results of this scan (demonstrated in Figure 2), revealed that the hippocampal volume was below the 5th centile on the age-matched normative graph, a finding consistent with a diagnosis of Alzheimer’s.
Further analysis using CSF confirmed the presence of an abnormal abeta: tau protein ratio. Following an in-depth clinical examination and exclusion of other causes of cognitive impairment, a diagnosis of Alzheimer’s disease was made, in this otherwise fit and healthy individual.
The resulting diagnosis had a significant impact on the family. The patient’s spouse was not prepared to discuss the diagnosis or contemplate sharing the diagnosis with his wife.
His own work required frequent business travel, thus starting therapy without appropriate support and explanation would be
Figure 1. MRI of brain
demonstrating atrophy
of the hippocampi

a challenge. Confounding the situation was the fact that the patient’s three children, all of whom were in full-time education, were dependent on their mother. For the children the impact was also profound; they had difficulty understanding the changes their mother exhibited, including decline in concentration, attention and short-term memory.
Fear is an undercurrent in all of the family dynamics, and this was apparent in this circumstance. These fears come from the images of Alzheimer’s in popular culture, which are almost exclusively of advanced disease: The patient has bursts of anger and paranoia; wanders aimlessly; suffers from inability to recognise family members; lies mute and helpless in a nursing home bed. Such fears also come from observations of severely demented people with blank stares, supported by stories of exhausted carers, traumatised by the emotional and physical toll of caring for increasingly helpless individuals, as well as the gradual loss of companionship and affection. It is rare for medical practitioners to ask a patient what it’s like to be in his/her mind. And, due to the fear, embarrassment and shame that surround the disease, it is unlikely that a person with Alzheimer’s
is going to volunteer their stories. As a result, less is known about the patient’s experience of living with the disease. At the multi-speciality medical centre in London, understanding the patient perspective and overcoming the fear of Alzheimer’s is part of its ‘living with Alzheimer’s without dementia‘ initiative.
At the London centre, a specialist nurse, a counsellor and a neurologist formed a treatment team that worked collaboratively with the patient’s GPs. The holistic approach was more than drug therapy; it considered the needs of the family, provided the necessary steps to guide them in coming to terms with the diagnosis, and gave them a strategy for treatment and support incorporating Re:Cognition Health’s Active Minds Programme™. Importantly, the centre housed all aspects of support including imaging tests in one location; a major departure from the UK’s fractioned care system.
Within months of diagnosis, the patient’s symptomatic medication was stabilised by the neurologist, and a live-in carer was brought into the family as steps to further enable independent living and maintenance of lifestyle. The model of care aimed at ‘living with Alzheimer’s without dementia’,
including multi-speciality medical care, stable dose, diagnostic tests, a live-in carer for ongoing cognitive assessments and well-informed family, provided ideal circumstances for considering the patient for Alzheimer’s-related clinical trials.
In October 2013, the patient was successfully randomised into a global Phase III clinical trial for a tau aggregation inhibitor. At the conclusion of this 18-month trial, the patient will be eligible to receive the study drug during the open-label extension study.
After many years of gradual cognitive decline, worry and anxiety about the cause of her symptoms, this otherwise healthy and previously high-functioning woman is now appropriately supported. She and her family have understanding and knowledge about her condition and she is optimistic that she may be one of the few fortunate individuals whose trajectory of cognitive decline may be significantly altered by early access to a disease-modifying therapy. Without an accurate diagnosis, albeit late, and appropriate post-diagnostic care management, this would not have been possible.
Changing the Trajectory of Alzheimer’s Disease: A Healthcare Priority
So What Needs to Change?1. Reform Alzheimer’s Drug DevelopmentAlzheimer’s is the only leading cause of death still on the rise. As the burden of Alzheimer’s disease escalates worldwide, efforts to develop effective treatments are failing to keep pace because of the high costs and risks associated with developing Alzheimer’s drugs. Reforming Alzheimer’s drug development, so it is more streamlined and efficient, would bring down costs and speed progress toward approval of drugs that slow or stop the disease.
It is projected that a treatment breakthrough by 2015 that delays age of onset of Alzheimer’s disease by just five years would result in a reduction in the number of individuals over age 65 years suffering with severe Alzheimer’s disease by 54% by 2020 and 82% by 2050, and billions in healthcare expenditure would be averted. In Western Europe alone, the number of people with dementia is projected to increase by 48% to around 10 million by 2030, equivalent to 2.4% of the population. A disease-modifying Alzheimer’s drug will benefit more than 5 million people. The increasing clinical burden of Alzheimer’s care will have a direct impact on the costs of meeting the demand for care. These costs not only include direct medical costs, but other related healthcare services and capital investments.
2. More Efficient Pathway for Diagnosis: This needs to be faster, less costly, and more efficient. The onset of this pathway begins in an outpatient setting, ideally in the community or at a primary care facility. Use of expensive diagnostics, such as PET scanning, should be within clearly-defined clinical guidelines.
Alzheimer’s is a clinical diagnosis that relies on a range of diagnostic tools. An initial assessment typically involves a wide range of “bedside” memory tests. These tests result in varying accuracy and specificity. Today the use of technology
Therapeutics
Journal for Clinical Studies 35www.jforcs.com
Figure 2. NeuroQuant analysis of the brain showing hippocampal volume below 5th Centile on age matched reference charts
Figure 2. Volumetric analysis of the brain showing hippocampal volume below 5th centile on age-matched reference charts. Diagram via NeuroQuant®, a product of CorTech Labs Inc.

Therapeutics
Volume 6 Issue 136 Journal for Clinical Studies
for automated memory testing and other aspects of cognitive function is streamlining the initial pathway to diagnosis, recognising that such testing must always be part of a pathway, not stand-alone or opportunistic.
3. Online Self-administered Tests Regulations:Such tests freely available on the internet have typically been unreliable. A recent study which examined 14 of these tests concluded that none had any basis for accuracy or validity, resulting in either undue anxiety, confusion, or potentially a false sense of reassurance. Without controlled tests resulting in marketing clearance or approval, these tests are in violation of the Federal Food, Drug and Cosmetic Act (the FD&C Act). Regulatory agencies should establish clear guidelines for approval of these tests.
4. Promote Clinical Research Collaborations between GPs and Alzheimer’s Speciality CentresWhile the UK’s NHS reports a major increase in the number of patients taking part in research in primary care settings, this increase has not occurred within the speciality care setting, where proactive patient recruitment and in-field educational seminars are at the core of increasing knowledge, understanding and participation in Alzheimer’s research. These collaborations can be further cultivated if barriers within the existing healthcare system are removed.
5. Remove the Historical Boundaries that Impede Alzheimer’s CareExisting care pathways are weighted with neurologists, psychiatrists, GPs and specialist nurses that currently work in silos rather than integrated clinical care teams. This segregation predominantly occurs in community and primary care settings.
Re:Cognition Health provides expert diagnosis and management of all conditions resulting in cognitive impairment at all ages; with respect to those with Alzheimer’s disease Re:Cognition Health is the first specifically designed inter-disciplinary medical centre for Alzheimer’s in the UK that works end-end; from initial diagnostic pathway to post-diagnosis interventions, long term management and support. This model results in earlier diagnosis and access to advanced interventions through clinical research. This is in contrast to the historical situation where diagnosis is late, cognitive impairment is more severe and the focus is on managing significant cognitive-healthcare decline.
6. Standards for the Use of Advanced Diagnostics New PET ligands are being introduced (Amyvid, from Avid Radiopharmaceuticals), with further potential ligands in the pipeline (T807 for tau, also from Avid). While these diagnostics show great promise, they require specific clinical guidelines for use. In the UK, the specialist test centre is engaging with the Administration of Radioactive Substances Advisory Committee (ARSAC) and the Royal College of Radiologists (RCR) to develop
Fig 3: Alzheimer’s Association, 2011 Alzheimer’s Disease Facts and Figures, Alzheimer’s & Dementia, Volume 7, Issue 2 (issued March 2011)

Therapeutics
Journal for Clinical Studies 37www.jforcs.com
guidance around indications and quality assurance. Laboratory testing is also developing fast. A CSF assay for abeta:tau protein ratio and various blood markers are being studied. If progress is shown on the use of genetic markers, genetic counselling services will be required.
7. Equal Access to Clinical Trials for All Patients Based on clinical eligibility, equal access to clinical trials for all patients is crucial. In Alzheimer’s within a multi-speciality centre, almost without exception, patients with educated and motivated relatives are most able to navigate their way to clinical trials. They effectively utilise the internet to access information about Alzheimer’s and Phase III clinical trials. Industry-funded clinical trials for Alzheimer’s are highly competitive on a global basis, and are specialist-dominated. This poses a challenge for other stakeholders, including primary care, charities, social care services, community memory services, and residential living organisations. Whilst all benefit from having patients involved in clinical trials and under the speciality care of integrated medical centres, few are aware of clinical research opportunities and/or steps to take to guide their constituents through the process of screening to enrolment.
While the American Alzheimer’s Association has a ‘Trial Match™’ programme, the Alzheimer’s Society in the UK are seeking to create a national register of patients interested in participating in dementia-related research and trials. But such a venture is costly, and may still be years away from launch.
Achieving Alzheimer’s without DementiaAlzheimer’s without dementia may sound like a stretch but it is a goal within reach. With the emergence of disease-modifying drugs, a future of Alzheimer’s disease without dementia is clearly on the horizon and within our grasp in the next few years. Alzheimer’s is a journey for the patient, the carer and the family. The goal of an integrated healthcare team is to optimise the availability of healthcare resources, including clinical trials, so that those affected directly and indirectly are able to maintain independence, cognitive function and quality of life for as long as possible; adding life to years, not just years to life.
For those who are diagnosed early, when symptoms of cognitive impairment are mild, enrolment in MCI and Alzheimer’s trials with the new emerging agents will offer a future very different from those who fail to participate.
Is dementia screening part of the answer? Probably not, but there is certainly room for improvement in surveillance of cognitive function with age and innovation in initial testing and triage so that patients can be streamed into different pathways ranging from “watchful waiting” to full assessment by a neurologist for complex presentations.
How will we know if we are on track? Neuro-psychometry is important, but arguably patient-reported outcomes measures are equally so, especially from the patient and the carer/family perspective. Improvements in quality of life as disease-modifying drugs slow cognitive decline will be the functional and clinical measures that drive change, and ultimately shift media focus to advances in Alzheimer’s care.
Clinical Research and Innovation Historically, innovation has been difficult for the UK’s National Health Service (NHS), in part due to a fractioned network of clinical resources with separate organisations and separate funding sources, and the national tariff payment system which sets a national tariff (prices and rules) intended to help local clinical commissioning groups work with providers like NHS trusts and foundation trusts, to identify which healthcare services provide best value to their patients. Currently, the national tariff payment system, which sets the prices for services in our public health system, does not extend to Alzheimer’s – Dementia which, in the UK is classified within ‘mental health’ rather than neurology.
However, from a global standpoint, as a result of innovation in healthcare and medical technologies, modern medicine can now tackle disease in a way that was unthinkable only a few years ago. Death rates from diseases the public once feared - such as coronary heart disease, one of the world’s biggest killers - have dropped, and cancer survival rates have been transformed. Through R&D investment and ongoing research in tau aggregation inhibition, we are on the path for significant change in the course of Alzheimer’s.
Dr J Emer MacSweeney is a Medical Director and Principal Investigator at Re:Cognition Health. Dr MacSweeney is a Consultant Neuroradiologist, and previously Director of Neuroradiology at Atkinson Morley’s Hospital, St George’s Healthcare Trust. Dr MacSweeney has extensive experience in both the NHS and independent sector, and currently undertakes clinical sessions as consultant neuroradiologist at St George’s Hospital and holds an honorary neuroradiology appointment at The Royal Brompton and Harefield NHS Trust. Dr MacSweeney trained in
neuroradiology at the National Hospital for Neurology and Neurosurgery, Queen Square; she previously specialised in interventional vascular neuroradiology, and has developed a special interest in neuroradiology of cognitive impairment disorders, with considerable experience in imaging of neurovascular diseases and traumatic brain injury.
Liz Moench, President and CEO of MediciGroup® Inc, has implemented innovative programmes that have changed the pharmaceutical industry twice in her 30-year career. Her achievements include launching industry’s first direct-to-consumer advertising campaign [1983] for Boots-ibuprofen, and pioneering the first direct-to-patient recruitment for clinical trials for Taxotere (Rhone Pulenc Rorer now sanofi Aventis) in 1991. Today her pioneering initiatives include optimising digital strategies and social media for patient recruitment and engagement, including
developing and managing some of the largest online patient communities globally (Team Epilepsy, Gout Study and Lupus Team) to promote clinical research. Email: [email protected]
Elizabeth Puller is a Senior Account Director - Europe at MediciGlobal Ltd, currently based in the U.K., where she is involved in a range of medical communications activities in support of clinical trials. She has a B.S. degree in Scientific and Technical Communication from the University of Washington and an M.S. in Journalism from Columbia University.Email: [email protected]

Therapeutics
Volume 6 Issue 138 Journal for Clinical Studies
Rheumatoid arthritis (RA) is associated with increased cardiovascular morbidity and mortality. When compared to the general population, patients with RA were found to have a 50% increased risk of cardiovascular mortality, a 59% increased risk for fatal ischemic heart disease, and a 52% increased risk for cerebrovascular accidents1. This increased risk, however, is not explained by traditional cardiovascular risk factors such as smoking, hypertension, or diabetes2.
Over the past few years, arterial stiffness has emerged as a new marker of cardiovascular disease, independent of these traditional risk factors. Studies on arterial stiffness and cardiovascular disease recently culminated in a meta-analysis of over 17,000 subjects. This meta-analysis consolidated the evidence that arterial stiffness, as measured by aortic pulse wave velocity (aPWV), was
an independent predictor of cardiovascular risk. However, it also showed that when aPWV was added to traditional
CV risk factors, there was a significant improvement in risk classification. This was especially true in people under 60 years old, among whom 24% of people were correctly reclassified according to their risk of cardiovascular death3.
The aortic pulse wave velocity is typically measured by recording the pressure waveform non-invasively at the carotid and femoral arteries, either simultaneously or with a reference time marker such as an EKG. From the two waveforms, the time interval between the arrival of the waveforms at each site (Δt) is determined, and the distance between the sites (Δx) is used to compute the aPWV.
The morphology of the blood pressure waveform is determined by both cardiac and vascular function, and so is also affected by changes in arterial stiffness. Figure 1 illustrates the two primary components of the central pressure waveform: 1) an incident pressure wave, generated by left ventricular contraction, and 2) a reflected wave returning back from the peripheral vasculature. The influence of the reflected wave on the composite waveform is determined largely by the stiffness of the central arteries and the strength of the reflected wave. New measurement techniques allow the non-invasive measurement of the central pressure waveform and its characterisation. The augmentation index (AIx), as defined in Figure 1, is indicative of changes in arterial stiffness and wave reflection. AIx has also been shown to be independently predictive of CV morbidity and mortality in select populations4. Recent research has shown an approximately 32% increased risk
Arterial Stiffness and Rheumatoid Arthritis

of a cardiovascular event with an absolute 10% increase in the central augmentation index5.
Because rheumatoid arthritis is an inflammatory disease, it is not surprising that vascular changes accompany the disease. Several studies have shown that aPWV is elevated in patients with RA compared to healthy controls (e.g. the studies by Mäki-Petäjä et al.6 and Klocke et al.7). Changes in the central aortic blood pressure waveform have also been reported in RA patients (Cypiene et al.8, Avalos et al.9). Pieringer et al. found that the augmentation index is increased in patients with RA, regardless of the coexistence of traditional CV risk factors, and that the impact of RA on the vascular system was comparable to that of smoking10.
Knowing that RA is associated with increased levels of arterial stiffness and that increased stiffness is a proven cardiovascular risk factor has led to investigations on how current pharmacotherapies aimed at treating RA also affect arterial stiffness. In a study by Galarraga et al., 47 subjects were treated with either etanercept (ETAN) or methotrexate (MTX). Their AIx was measured prior to treatment as well as at four months. The investigators showed that treatment with ETAN, but not with MTX, resulted in a significant reduction in augmentation index11. In another treatment study, Mäki-Petäjä et al. showed not only that baseline values of aPWV are elevated in RA patients, but also that treatment with an anti-inflammatory resulted in a reduction in aPWV to control levels 6 (see Figure 2).
In summary, the increased morbidity and mortality rate associated with RA cannot be fully explained by traditional risk factors. However, combining arterial stiffness measurements with these traditional risk factors significantly improves the prediction of morbidity and mortality. Numerous studies have demonstrated a role
for arterial stiffness in RA, and that measurements of arterial stiffness can be valuable in evaluating CV risk and therapy efficacy in rheumatoid arthritis.
References1. Avina-Zubieta JA et al. (2008). Risk of Cardiovascular
Mortality in Patients with Rheumatoid Arthritis: A Meta-Analysis of Observational Studies. Arthritis Rheum , 59 (12), 1690-1697.
2. del Rincon ID et al. (2001). High incidence of cardiovascular events in a rheumatoid arthritis cohort not explained by traditional cardiac risk factors. Arthritis Rheum , 44 (12), 2737-45.
3. Ben-Shlomo Y et al. (2013, Nov 4). Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J Am Coll Cardiol , in press.
4. London GM et al. (2001, Sep). Arterial wave reflections and survival in end-stage renal failure. Hypertension, 38(3), 434-8
5. Vlachopoulos C et al. (2010, Aug). Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis. Eur Heart J, 31(15), 1865-71.
6. Mäki-Petäjä KM et al. (2006). Rheumatoid Arthritis is Associated With Increased Aortic Pulse Wave Velocity, Which is Reduced by Anti-Tumor Necrosis Factor-alpha Therapy. Circulation , 114 (11), 1185-92.
7. Klocke R et al. (2003). Arterial stiffness and central blood pressure, as determined by pulse wave analysis, in rheumatoid athritis. Ahh Rheum Dis, 62, 414-418.
8. Cypiene et al. (2007). Non-invasive assessment of arterial stiffness indices by applanation tonometry and pulse wave analysis in patients with rheumatoid arthritis treated with TNF-α blocker remicade (infliximab). Proc West Pharmacol Soc, 50, 119-122.
9. Avalos et al. (2007, Nov 15). Increased augmentation index in rheumatoid arthritis and its relationship to coronary artery atherosclerosis. J Rheumatol, 34(12), 2388-94.
10. Pieringer H et al. (2012). Rheumatoid arthritis is an independent risk factor for an increased augmentation index regardless of the coexistence of traditional cardiovascular risk factors. Semin Arthritis Rheum , 42 (1), 17-22.
11. Galarraga B et al. (2009). Etanercept improves inflammation-associated arterial stiffness in rheumatoid arthritis. Rheumatology (Oxford) , 48 (11), 1418-23.
Figure 2: The effect of entanercept on aortic PWV in patients with RA
Dr. Winter is currently Vice-President of Scientific and Clinical Affairs for AtCor Medical, Inc. Prior to joining AtCor, he was Director of Bioengineering at Southwest Research Institute, where he developed the first commercial blood pressure monitor based on arterial tonometry. He is an internationally recognized expert in physiological fluid mechanics, biomechanics and medical device development. Email: [email protected]
Journal for Clinical Studies 39www.jforcs.com
Therapeutics

40 Journal for Clinical Studies Volume 6 Issue 1
Therapeutics
Increasing Therapeutic Complexity in CNS Clinical Trials: The Need for Therapeutically Aligned Staff
The expectations for clinical research staff have reached unprecedented levels amid a perfect storm of several confluent factors, none more significant than the marked rise in clinical trial complexity. According to a report by the Tufts Center for the Study of Drug Development (Tufts CSDD), the average study protocol now includes 13 endpoints, 167 procedures, 35 inclusion and exclusion criteria, and requirements for 11 site visits per patient over a 175-day period.1 The rise in protocol complexity has been particularly evident in trials targeting CNS diseases, where, in the wake of some notable late-stage study failures in recent years, sponsors are increasingly emphasising the scientific integrity of experimental drug programmes in this space. To that end, when conducting CNS trials today, it is critical that sponsors and contract research organisations (CROs) implement better and more thorough processes and tools in areas such as patient eligibility screening and confirmation and the review of outcome data assessments, which, for many CNS indications, often contain subjective information. To meet these demands, CNS study teams are increasingly in need of clinical research associates (CRAs) that possess both therapeutic and technical expertise.
As industry analyses continue to point out, clinical trials have been steadily growing in complexity over the past decade.2
This has led to dramatic increases in study costs. In CNS, specifically, expenses for Phase III trials are the second highest on a per-patient basis, trailing only oncology.3 Further, a recent examination found that Phase I trials in CNS have the widest range of costs per patient per month, at $20,606.4 Spurring the increased complexity in CNS studies has been a greater understanding of the unique intricacies associated with CNS indications; past trial failures can often be attributed to the inability to adequately control extraneous factors (e.g., enrolling the right patients, properly measuring drug effectiveness, tracking and reporting data).
Sponsors, mindful of the financial risks in conducting CNS trials, are increasingly introducing more complex study designs. For example, trials evaluating cognition in schizophrenia are now routinely being planned with anywhere from 8-12 endpoints. These additional endpoints introduce new measurements that require therapeutic training at the site and CRO levels. Further, many involve complex assessments that sponsors now prefer to be carried with more sensitive instruments. For instance, in stroke, tools such as the Fugl-Meyer assessment are being incorporated into trials to improve the chances of separating motor-recovery measurements from placebo. These novel instruments can be difficult to administer without proper training. Complex study designs are also being implemented in depression trials, where multiple baselines are used to address concerns involving placebo response. Other evolving design strategies in CNS include the use of clinical surveillance systems to improve patient and data quality and help prevent adverse events.5
Additional complexities in CNS trials have resulted from new enhancements in drug supply. For example, in stem cell research, neurological regeneration studies (e.g., spinal cord injury) often have extensive article handling requirements and necessitate
transport and storage in extreme temperatures. Similarly, targeted drug delivery methods in CNS, such as those involving ultrasonography, require adherence to a comprehensive set of procedures. For instance, when administering microbubble cavitation to stroke patients, clinical teams, operating in a limited time window, must inject the compound and then properly calibrate the ultrasound projector to focus on the part of the brain where the clot is believed to reside. These technical complexities in CNS trials have grown hand-in-hand with the level of technology required. Studies are increasingly incorporating advanced testing tools to assess treatment fidelity. In Duchenne muscular dystrophy, for example, a whole body scan, known as dual energy X-ray absorptiometry (DEXA), is being used to measure muscle composition. There is also more reliance on technology integral to capturing CNS assessments. For instance, stuttering and dystonia trials use video recording to measure certain endpoints.
With the emergence of new technological approaches in CNS, site and CRO staffs must be able to clearly understand the administrative and protocol requirements governing these

Thanks to our innovative Phase I to II trial delivery…
…we’re helping our clients win the fi ght on cancer
RIGHT DATA • RIGHT TIME • RIGHT DECISION
www.cmedresearch.com
Cmed CS 2012 Ads AW.indd 2 12/1/12 11:45:54

Volume 6 Issue 142 Journal for Clinical Studies
Therapeutics
tools, and the importance of conducting these assessments in a standardised fashion. Coupled with the overall rise in clinical trial complexity, it is clear that the details required to conduct CNS studies effectively have expanded greatly at the site level. To better manage the new complexities, sites themselves should improve both new staff recruitment and experienced staff retention.6 In turn, for CROs providing site training and monitoring for CNS studies, the need to deploy therapeutically aligned staffs – those that combine strong conceptual clinical and technical knowledge with practical experience in a regulated environment – has become essential. To help achieve this dynamic, there needs to be a greater emphasis on evolving traditional training approaches for CRAs. Clinical trial workforces should no longer have to rely strictly on one-off training sessions, but rather be afforded prospective, ongoing training and education.7 In CNS drug development, with its many inherent challenges, the ability to foster flexible thinking and apply key learnings from one study to the next is critical to advancing new medicines in the field.
References1. Getz, K. Clinical Trial Complexity. Tufts Center for the Study
of Drug Development presentation. 2012, http://www.iom.edu/~/media/Files/Activity%20Files/Quality/VSRT LST%20Workshop/Presentations/Getz.pdf.
2. What Do More Complex eCRFs Mean for Clinical Research? Medidata Solutions Inc. Published online Aug. 7, 2012, http://blog.mdsol.com/2012/08/07/what-do-more-complex-ecrfs-mean-for-clinical-research/#.UrHTKxYSPGI.
3. Clinical Trial Costs are Rising Rapidly. Pharmalot. Published online July 26, 2011,http://www.pharmalive.com/clinical-trial-costs-are-rising-rapidly.
4. Average Phase I Trial Costs Approach $9,000 Per Patient
Per Month. Reuters. Published online Sept. 27, 2013, http://www.reuters.com/article/2013/09/27/nc-cutting-edge-idUSnBw275004a+100+BSW20130927.
5. Nations, K. Our Love/Hate Relationship with Clinical Surveillance, and Why Both are Valid. Journal for Clinical Studies. 2013, 5(6): 10-12, http://jforcs.com/jcs/j610-our-lovehate-relationship-with-clinical-surveillance-and-why-both-are-valid/.
6. Clinical Research Sites Struggle With Increasing Trial Complexity. Business Wire. Published online March 10, 2011.
7. h t t p : / / w w w . b u s i n e s s w i r e . c o m / n e w s /home/20110310006139/en/Clinical-Research-Sites-Struggle-Increasing-Trial-Complexity Bonham, A., Califf, R., Gallin, E. and Lauer, M. Appendix E Discussion Paper: Developing a Robust Clinical Trials Workforce. National Academy of Sciences. 2012, http://www.ncbi.nlm.nih.gov/books/NBK114665/.
Andrew Silverman, PhD., Sr. Vice President of CNS Clinical Development at INC Research, has worked in the clinical research industry for nearly 20 years. During this time he has worked broadly in the CRO industry, including in the areas of study development, project management, clinical monitoring, and data management. Currently, Dr Silverman heads the staffing
and administration functions of the CNS Business Unit at INC Research.
Email: [email protected]. Website: www.incresearch.com.

© Copyright 2013 Packaging Coordinators, Inc. All Rights Reserved.
Global Reach with 14 packaging facilities in North America and Europe
Clinical Trial Services
Global Storage & Distribution
Life Cycle Support
www.pciservices.com
AndersonBrecon (UK) Limited trading as Packaging Coordinators, Inc. is a company registered inEngland and Wales with company number 02543975 and VAT registration number GB 549 7026 19whose registered office is at The Broadgate Tower, Third Floor, 20 Primrose Street, London, EC2A 2RS
Our CommitmentTo Deliver an Exceptional Customer Experience.
Successful Clinical Trials Start Here.We believe our customers deserve nothing less than exceptional service,at every stage of their product’s development, from each phase ofclinical development to successful commercialization. Our experienced team offers expertise in all aspects of clinical packaging, storage, anddistribution services. We are with our clients every step of the way,providing scalable solutions to support the earliest Phase I studies tothe largest global Phase III/IV studies.
The ultimate measure of success is commercialization of your product, and PCI helps navigate the clinical phases in launching over 50 newproducts a year. Our expertise helps clients bring products to marketefficiently and effectively, with keen insights to enable launch andcommercial success. With an expert team focused on your investigational product, PCI is uniquely positioned to support your product throughoutits life cycle.
Exceptional customer support for the success of your clinical trial.
PCI - One Partner for all your development needs.
PCI_CommitWKG_UK.indd 1 1/19/14 2:32 PM

Therapeutics
Volume 6 Issue 144 Journal for Clinical Studies
Collaborative Drug Development for
Rare Diseases
Drug development can be driven by patient groups. This is a tenet of two groups we work with, the AKU Society, an entrepreneurial patient group that has kick-started European clinical trials for a rare disease called alkaptonuria (AKU), and Findacure, the fundamental diseases partnership. Findacure supports patient groups and gives them the tools and knowledge to initiate clinical research for their individual diseases. We believe that a collaborative approach to drug development for rare diseases is the best way forward, and in this article we will explore the top 10 steps leading ultimately to clinical research.
1. Find the Right Partners and Unite Them Into a ConsortiumPatient groups are essential partners for clinical research, as they are usually the most invested. Often, patient groups focus on a single disease, and so are prepared to focus all their time on understanding the disease and looking for solutions for its treatment. However, patient groups cannot work alone; they also need the expertise of other partners: the researchers who will unravel the mechanisms of the disease, the clinical researchers who will follow the progression of the disease, the contract research organisations (CROs) that will plan and orchestrate the programmes for clinical trials, the independent labs that will perform unique measurements on the disease outcome parameters and so on. In order to gain the expertise needed for successful research, it is vital to recruit partners from varied backgrounds and then unite them into a project consortium.
A consortium is a formal way of uniting these partners, making all understand the importance of the overall aim: to lead a treatment for the disease into clinical research and make it available for patients. Usually, this will require a consortium agreement, a contract outlining the aims and objectives of the group, and a clear breakdown of the duties and roles of each partner. If industry or commercial partners are included, the agreement may also include consideration of the likely intellectual property (IP) to be generated and a plan for its dissemination.
To engage with academia, the patient groups need to study the literature and identify the leaders in the field of research. These may often be dispersed across several countries, which can represent quite a challenge. Patient groups need guidance on how to get involved with research and how to judge credible work. In one extreme example that we know of, a patient group found an Italian scientist online who claimed to be working on a mouse model of their disease, but who disappeared after the group gave him €20,000.
Engaging with industry may also be difficult initially for patient groups. It might be hard to identify the appropriate company or the right person within it. In addition, industry traditionally tends to keep patient groups at arm’s length, in order to avoid conflicts of interests, so this may be a new experience for both parties
2. Promote Basic ResearchThe first step of any search for a new therapy is to fully understand the disease. This means the development of basic research programmes with teams focusing on the aetiology of the disease, the underlying biochemical and molecular mechanisms and its phenotypic manifestations. For many common diseases, much may already be known about the pathogenesis of the disease, but for rarer diseases, this work may be totally absent. Often interest for basic research into rare diseases does exist at some level: some diseases have interesting connections to other diseases, some researchers want to help patients who have little hope of understanding their disease, and others are keen to work in an area that hasn’t been extensively studied, in order to make their mark.
With an aim for eventual clinical development, basic research is usually most successful through establishing long-term relationships with research teams. This is not a quick process, but the clinical development will benefit from a strong foundation in research.
3. Drug DiscoveryWith collaborative drug development, the discovery process is likely to be taking place in the universities rather than in the research departments of pharmaceutical companies. This research may be funded by patient groups already and this then leads to a natural partnership later in the development process. There are a few examples of biotech companies being funded for several years by a patient group before going on to raise money from investors or partner with a larger company to fund the clinical development. Even if not so funded, the identification of leading experts at the stage of discovery is important for later collaboration.
4. Identify Clinical Outcomes and AssessmentsMany rare diseases have not been well studied and there may be little known of the natural history of the disease. This can make it difficult to decide on the most appropriate measures of efficacy, and often one is learning about the clinical outcomes only during the course of the study. The research interests of the academic experts may already have led them to run natural history studies, identify suitable surrogate markers, and develop novel clinical methodology for assessing disease progression and the effect of treatments.
It is also very valuable to consider trying to set up a recognised national centre at the site of the key clinical expert. This is a large undertaking, but the rewards are the creation of a single centre in the country which can see and treat many of the patients, and it provides a superb base for learning more about the natural history of the disease and a potential pool of patients for subsequent clinical trials.

Therapeutics
Journal for Clinical Studies 45www.jforcs.com
5. Find Funding OpportunitiesOnce a consortium is in place, with good plans for clinical development, it will need to look for larger funding opportunities. Some partners may be in a position to fund themselves, but this will probably be unlikely for all, and especially for smaller partners, such as the patient groups and any small-medium enterprises (SMEs). Funding grants are available, but can be very competitive and there are typically fewer grants available for rare diseases than for more common diseases.
The main difficulty with funding clinical trials is that they are expensive. Our experience in the UK was that there are few funders able to grant a large enough amount to cover even a fairly simple clinical trial. One possibility is to look at the larger funders, such as the European Commission (EC), which offer grants typically at a greater scale than in individual countries.
As may be expected, EC grants are highly competitive and usually have long lead-times. However the time can be well spent, as it will often allow consortia to dedicate more time to planning and evaluation, and the opportunities for peer-review with experts from across the EC can bring in useful suggestions for modifications, both of which can result in a better overall trial. Another alternative would be to look at funding from a pharmaceutical company. However, this would depend on the IP rights connected to the drug in question and the commercial incentive. A company is only likely to get involved with such a consortium if a sound business case can be made.
If funding is to come from grants, it can be worthwhile to involve someone who can advise on how to complete the grant application process (which can be onerous for the larger grants) and maximise the chances of success.
An additional source of funding is crowd-funding. Although this is unlikely to generate sufficient money to run a clinical trial,
it is possible to raise several tens of thousands of dollars from a well-run campaign.
6. Motivate and Manage the ConsortiumPlanning and running clinical trials is a long-term project, which provides plenty of time for consortium partners to question their involvement. Often the most difficult time for consortia is during the previous step, the time spent applying for funding. During this time, the partners are essentially working for free, with no guarantee of eventual funding. Therefore, maintaining the motivation among the consortium is essential. An effective way of keeping momentum is through smaller projects. Gaining funding for a small, distinct project that will generate results useful for a larger application is an effective way to both improve the final application and to keep partners keen. It is the same reason why mobile games become addictive: small and frequent rewards ensures that a consortium’s interest remains focused on the ultimate goal.
Once a consortium is established and funding is in place to allow it to work towards its goal of clinical development, the next issue is to ensure that the consortium can handle the project. Typically, the most invested partner is the patient organisation, and so it may make sense to involve them as a management lead.
In the AKU consortium, we are obliged to follow EC guidelines, and so have regular 18-month reporting periods. However, we decided to build on that, and agreed on six-monthly face-to-face meetings, with smaller reports that build to form the 18-month reports. To ensure that our partners in the consortium felt like part of a wider team, we also started weekly teleconferences. With a set time, they neatly fall into people’s routines, and so are not forgotten; and having them so regularly means all partners understand the pressures and successes of each member. Regular news generated by the patient group

Therapeutics
Volume 6 Issue 146 Journal for Clinical Studies
(e.g. through its website or a newsletter) helps to keep everyone informed.
A typical consortium containing all the partners required for a development programme may have many members. Most (or all) of these partners are unlikely to have any drug development experience and may find it difficult to focus on the key issues for achieving the ultimate objective. This focus often means sidelining interesting ideas which do not directly contribute to the objective. This can be difficult to manage in the matrix-type setting of a consortium, where all parties have an equal say.
7. Regulatory IssuesThere is likely to be a steep learning curve for many partners who may not understand the complexities of drug development and the regulatory environment that will determine the success of the project. The regulatory considerations for drug development are already complicated, but for rare diseases they are more so. In particular, a developer can take advantage of a range of benefits that are offered under the regulations for orphan drugs, but it is important to know how to navigate this path in order to be successful.
For these reasons, it is crucial to involve at least one party with significant drug development experience to advise on these issues and keep the consortium on track. The importance of this aspect can be misjudged even by pharmaceutical companies, so in a consortium where none of the parties has experience, it can easily get missed.
8. Clinical IssuesDesigning a good drug development programme and a good clinical trial is difficult at the best of times, but is even more difficult for rare diseases with small patient populations and uncertain outcome measures. Unless an experienced company is part of the consortium, there is unlikely to be any expertise within the group to do this and so, as for the regulatory issues, it is crucial to involve a party with significant drug development experience to advise on this. It is not possible to explore this in detail here, but the issues to consider in the clinical development plans are discussed in detail in a recent article 1.
9. Engage with PatientsIn clinical research, patients should always be the first priority. Consortia should engage with patients from the start and ensure that their views and concerns are listened to. The best method to achieve this is to involve patient groups, who should have a pre-existing good relationship with a large number of patients. Often they will survey patients and organise workshops, giving an opportunity to consult patients from the outset. Including patients in the planning stages of a clinical trial will mean they have the chance to discuss options for the assessments and share their concerns. The benefit will be a well-designed trial, with outcomes relevant for patients. With early involvement, patients are less afraid of the research and better understand the study design. This can be especially important if there are placebo or no-treatment arms in the study and if the study is of long duration.
The patient organisation can also be a key factor in ensuring recruitment targets are met. For rare diseases, recruitment is likely to be a big challenge and, if the project is funded with a grant, budgets will be tight and it will not be possible to solve recruitment issues by simply opening more sites in more countries.
10. It’s a Marathon!The final message isn’t a tip, but one of encouragement. For a patient group to push forward a promising drug into the clinic is a challenging task, and one that shouldn’t be undertaken lightly. The AKU Society was set up more than ten years ago, in 2003, and its primary aims have always been to see a possible treatment enter clinical research and eventually to become available to patients as a safe and effective treatment. It’s been a long and difficult process to reach this point, but we hope that other patient groups, academia, hospitals and pharmaceutical companies will see the benefit of a collaborative approach to drug development and learn from our experience. For further reading on the subject of challenges and opportunities in drug development for rare diseases led by patient groups, the reader may wish to refer to a recent book on the subject2.
References1. Hall AK, Ludington E. Considerations for successful clinical
development for orphan indications. Expert Opinion on Orphan Drugs. (2013) 1(11): 847-850.
2. Rare Diseases: Challenges and Opportunities for Social Entrepreneurs. Edited by Nicolas Sireau. Greenleaf Publishing. 2013.
Oliver Timmis is the Head of Projects for the AKU Society, a patient organisation supporting those diagnosed with a rare disease, alkaptonuria (AKU). Oliver leads on funding applications for new projects. He graduated with a BA(hons) in Natural Science from Cambridge University in 2010. Oliver volunteers at Eurordis, the RD Connect registries project and is a member of the Patient-centered Special Interest Group at ISPOR. He also volunteers for a new charity, Findacure.Email: [email protected]
Dr Anthony Hall graduated from King’s College London with first class honours in physiology and pharmacology before going on to study medicine at the Royal Free Hospital. He joined the pharmaceutical industry in 1994 and is a co-founder of PSR orphan experts, an orphan drug CRO. Since 2010, Tony has focused exclusively on the rare diseases sector. Tony is Co-Founder of Findacure, to which he devotes part of his time. The rest of his time he works as a consultant, providing advice and guidance on the development of orphan drugs to the
biopharmaceutical industry. Email: [email protected]


IT & Logistics
Volume 6 Issue 148 Journal for Clinical Studies
Building the Right Strategic Plan to Manage the Clinical Supplies for your Clinical Trial
In recent years biomedical research has been increasing, and it’s proportion of clinical trials are getting bigger. This means generating a growing amount of temperature-sensitive biomaterials that biotech companies can implement to ensure the accurate transportation and compliant storage facilities of temperature-sensitive clinical trial drugs and supplies.
If you are planning a new trial nowadays, you need to plan and budget the steps and the time from manufacturing until delivery to the sites of the trial drug much better than in the past. In today’s world, logistics operations have quite exceeded the target of merely transporting the drug from one point to another, and the understanding of high quality as well as management skills – such as correct coordination between processes – are among the important factors.
Today, clinical trials are becoming more and more complex
and expensive, and we see that with the increase in biomedical research, the trial medicals are more sensitive to temperature and storage conditions. Now, trial planners have to plan ahead not just manufacturing, delivery to the sites or randomization, but also the use of appropriate data loggers to ensure that the study drugs remain within the temperature ranges in the main depot, depot and centre line, until they reach their first destination following the manufacturing; and even the qualities of the boxes to be used, depending on the distance and the geographical characteristics of the trial sites.
In case of sensitive study drugs, trial planners should first define the country that they will work in, then they should observe the temperature trend of that country throughout the year, as well as the distances to the point of destination and the duration of shipping. The customs regulations of those countries should be reviewed, and special depot requirements for clinical trials should be known beforehand.
Study supplies will be exposed to various conditions and
temperature changes, or perhaps will change hands many times during the shipping process.
Careful selection of the materials (validated boxes, thermometers, etc.) and of vendors to collaborate with, as well as paying attention to working with well-trained and experienced teams, shall ensure patient safety, the reliability of the trial results, compliance with the country-specific regulations, traceability of the process, predictability, and optimisation of costs.
The Process in Turkey Although Turkey is a member of the European Customs Union, it is not a member of the EU and therefore procedures required for the entry of the clinical trial supplies to the country must be met. Storage conditions and the speed of customs procedures are critical, particularly to temperature-sensitive drug.
Drug exports license are available and valid for one year following the ethics approval of the trial by the Ministry of Health. For import licence applications, it is necessary to pay an application fee as defined by the Ministry of Health, and the application is first made electronically with the application form and its annexes. After receiving an electronic application number, the application file is delivered to the Ministry of Health as hardcopy. Once the hardcopy application procedure is completed, the import licence is issued within five to seven working days. After the import licence is obtained, there is nothing further to hinder the imports of the drugs. After the customs procedures, the drugs are forwarded to the site directly or to the clinical trial specific approved depot, depending upon the wish of the sponsor – as is usually the case today. Shipping the drugs in smaller portions based on the patient recruitment throughout the trial facilitates the monitoring and storage of the drugs under suitable conditions, and also prevents the wasting of the drugs, as the drugs are sent to the sites in line with the patient recruitment pace, which provides great advantages in terms of budget.
It is mandatory to ensure that the drugs are collected, counted and disposed of at the end of the trial, and that the relevant documents are submitted to the Ministry of Health.
Turkey experiences all four seasons in terms of geographical and climate conditions. Temperature differences and the times to deliver the drugs between the east and the west of the country vary accordingly.
For Turkey, drugs are delivered to the trial site within 24 hours on average. The delivery time to the furthest trial site is 48 hours maximum.
Although temperature excursions are rare thanks to technologically advanced validated boxes used in recent years, the experience of the depot team will prevent a potential temperature deviation in deliveries to cities where sudden climate changes, seasonal transitions and extremely high or low temperatures are experienced.
Management and inventory keeping process for all these trial drugs and supplies are rather complicated. SOPs that are well-defined by correctly structured software and processes will ensure that the process is appropriately managed, monitored, audited and reported. Clinical trial planners should be seeking these requirements and features concerning the drug management, and by collaborating with appropriate partners, they should prevent potential undesired surprises.

Clinical documents arethe visible part of
your clinical programme
Successful documents don’thappen by chance
Strategic approach to clinical documents
Tel: +49 69 138 2528-0
Fax: +49 69 138 2528-55
email: [email protected]
www.trilogywriting.com
Trilogy makes surethey do.
Are the regulatorsseeing what yourdocuments have
to say?
TRI020 advert amend 12/9/12 11:58 Page 1

Volume 6 Issue 150 Journal for Clinical Studies
IT & Logistics
In summary, every step should be carefully calculated and detailed in advance, as planning is crucial to successfully manage the obstacles such as study delays, unnecessary overages and unexpected costs.
Sule Mene, MD CEO, Depot Meridian- Mene Research. Sule graduated from Medical Faculty and Business Administration program at Harvard Business School. Certified in Clinical Research in a tradition of scientific excellence at Merck Frost Centre in Canada. Sule held several research core positions in different pharmaceutical companies .Sule is founder partner of Mene Research which was established in 2002. She gave several speeches and presentations in national and international congresses.
Tolga Mene MD, MBA, CFO, at Depot Meridian – Mene Research Tolga graduated from Medical Faculty and got his MBA at Boston University. He held several research core positions in different pharmaceutical companies. He is the partner of Mene Research and in charge of Finance Department.
Burcu Cehreli, MBA, MSc. Mene Research - Depot Meridian OperationsBurcu have a Chemical Engineering BSc degree from Istanbul University and additionally completed MBA program in Galatasaray University and Medical Systems and Information Technologies MSc program in Bogazici University. She is in charge of Clinical Operations /Business Development activities.
Asli Kaya, MSc. Head of Regulatory Affairs at Depot Meridian, Mene ResearchAsli graduated from Fatih University with a degree in Biology. She had her Masters Degree at Temple University in Biology. She joined Mene Research in 2011 and is in charge of Regulatory Affairs Department in the company.
Sehnaz Ozgun Assistant Logistics & Depot Manager - Depot MeridianSehnaz studied Life Sciences at Strasbourg Louis Pasteur University in France. Started her career in a Biotechnology Genetic and Stem cell laboratory, she continued in logistics and operational department in a Pharmaceutical warehouse and was in charge of the national operations to the University and Public Hospitals throughout Turkey. She joined Mene Research in 2013.


IT & Logistics
Volume 6 Issue 152 Journal for Clinical Studies
Using Questionnaires in Clinical Research
Patient and physician questionnaires, visual analogue scales, rating scales for the assessment of efficacy, effectiveness, safety, quality of life (QoL), resource use, and treatment costs are getting more and more important in clinical research. In particular, the recently increasing emphasis on QoL, treatment costs, real-life effectiveness of drugs, and the need for patient-focused outcomes to achieve market access leads to an increase in the development and use of scales. Selection, use, analysis, and reporting of questionnaires are tasks that need to be integrated throughout the whole clinical development process and this article explains the most important steps necessary for optimal leverage of questionnaire data.
Questionnaires to evaluate efficacy and QoL have been used for decades in clinical research in those areas where no objective measurement of efficacy is possible, such as psychiatry, and where QoL has been found to be of major importance for acceptance of a treatment, such as oncology. People who have been working in these areas of clinical research are probably well aware of the caveats and potential pitfalls that go together with analyses of questionnaire results. However, recently, several developments in clinical research have led to an even more widespread use of questionnaires, and most probably this development will continue in the near future. The reasons for this are the increasing importance of data that are closer to clinical practice and which are needed to achieve market access. As an example, the FDA and EMA may require comparative effectiveness data from post-marketing settings in the context of a risk management plan1.
Quality of life, patient wellbeing, and patient-centred outcomes are requested by reimbursement agencies such as NICE in the UK and IQWIG in Germany. In this area, new concepts such as quality-adjusted life years (QUALY) or the standard gamble (or time trade-off) have emerged to measure economical effectiveness, important for reimbursement decisions, and new concepts are still being developed2,3. Most of this information will need to be gathered in a non-interventional setting or in clinical studies that need to be as simple as possible, again excluding the use of laboratory or other “hard” data.
The implementation, analysis, and interpretation of scales in general is not as straightforward as, e.g., measuring blood pressure, and this is even more true if scales are to be introduced into fields where this hasn’t been standard previously and no generally accepted gold standards for questionnaire use are available. With complex questionnaires - often comprising dozens of questions - a huge amount of data is usually generated, from which the important information first needs to be extracted. Errors in the application of questionnaires can lead to the generation of data where only towards the end of the process it is realised that these data cannot be interpreted in a way that is required to provide convincing evidence. This will lead to time-consuming and costly re-analyses or, in the worst case, to data graveyards that are unusable. It is therefore important to plan the appropriate selection, use, and analysis of questionnaires early during a clinical trial or even better, when planning a whole clinical programme.

Journal for Clinical Studies 53
IT & Logistics
www.jforcs.com
The first step is to identify the need for certain types of questionnaires and the selection of the best-suited ones. There are several ways in which questionnaires can be classified (see Figure 1). Usually therapeutic questionnaires, i.e. those that are sensitive to change over time, are used in clinical research, where changes from baseline to endpoint are of interest. Sometimes however, at least at baseline, diagnostic questionnaires may be needed to confirm a certain disease as inclusion criterion or to assess the disease stage (e.g. tumour staging in oncology). Furthermore the subject filling in the questionnaire is important, and different aspects of achieving registration and market access for a drug patient, physician, parent, and caregiver perspective might be of importance. Also, the type of the questionnaire regarding data collection is important as it will impact the data that will need to be processed by data management, statistics and scientific communications. Visual analogue scales (VAS) give one single number anywhere between 0 and 100, whereas Likert (ordinal) scales have pre-defined values that are usually coded as digits (e.g. 1, 2, 3, 4, 5). Full questionnaires consist of an array of questions and the answers are coded in various ways into total scores or subscores (or domains), or may be analysed as single items.
Other criteria for the suitability of a questionnaire are generic (i.e. you can compare results between diseases) vs. specific (i.e. you can address your indication more specifically), short (easy) vs. comprehensive (difficult), suitability for the target population (e.g. children, elderly), possibilities for data entry (e.g. paper, computer, smartphone, datapen). This diversity of available questionnaires can lead to the desire to use a large number of questionnaires to encompass all possible aspects in a product development or even in the pivotal study. However, the time and effort needed by patients and physicians to complete the questionnaires need to be taken into account, as the time needed to complete all questionnaires of a single study visit then quickly reaches a timeframe of several hours. This will compromise the quality and completeness of answers and will even make recruitment of centres and patients more difficult. Thus it should always be challenged if an additional questionnaire is needed in a clinical programme or a specific clinical study.
A comprehensive overview of the concept of rating scales and questionnaires is given by the book “Measuring Health” by Ian McDowell4. In addition, it provides an overview of standard questionnaires available and their advantages and disadvantages in a number of areas such as social health, psychological wellbeing, anxiety, depression, mental status testing (e.g. dementia), pain measurement, general health status and QoL.
At the beginning of a clinical development programme involving questionnaires, it is crucial to define which questionnaires should be used throughout the programme. This decision should be made at an early stage (at the latest before the first Phase II is initiated) and decisions should already be made on the use of questionnaires needed for later stages of development, as earlier studies could already be suitable for gathering these data, saving time and effort later on. Consistency of questionnaire use throughout a development programme is an absolute requirement to maintain comparability between studies. Furthermore, consistency between different development programmes in the same indication (e.g. depression) or drug class is also very
desirable, and should be included in the decision-making process. Sometimes it is better to include an established questionnaire that has already been used and is accepted, instead of using a new one that claims to be better but is not comparable to data already published. Furthermore, in some indications the regulators mandate the use of specific questionnaires for granting approval (e.g. HAM-D or MADRS as primary objectives in depression studies). Therefore a close communication with, e.g., FDA and EMA is often helpful in identifying the relevant questionnaires.
If, in addition to established questionnaires, newer or less frequently used questionnaires should be employed, it is important to check their quality/credibility. In particular, the questionnaire should be validated, and validated translations for all languages used should be available5. A newly-devised “tailor-made” questionnaire should never be used for studies relevant for registration or reimbursement decisions, unless the necessity for devising a new questionnaire was discussed and agreed upon with the respective agencies.
At the end of this initial decision-making, there should be an overall plan available which defines mandatory questionnaires that should be used in every clinical trial of the programme, and optional questionnaires associated to a list of topics (e.g. non-interventional, quality of life, treatment cost, parent perspective) that can be used if the respective topics are to be evaluated in a certain part of the clinical programme or a specific clinical study.
Another important pitfall during the execution of a clinical programme is inconsistency in the analysis approach to a questionnaire. For a number of questionnaires, specific approaches to analysis exist and are presented in scientific manuscripts, instructional books, or websites (e.g. www.euroqol.org for the EQ-5D). These documents define the way scales are to be analysed, how total and subscores are calculated, and how missing data is to be handled during the analysis. Also in a number of cases different approaches for the analysis are possible, but it needs to be assured if the approach selected is suited for the required outcome.
This is often further complicated by the fact that there is more than one version of a questionnaire (e.g. the HAM-D 17, 19, and 24), and it has to be specified from the beginning which version of the questionnaire will be used and which analysis method is to be applied. This decision needs to be communicated to all functions that are involved in performing the clinical trials. This includes data management for the setup of the CRF, clinical research associates for training the investigators and monitoring, statisticians who must state the standard analysis method to be used, physicians who need to make sure that the analyses are interpreted correctly, and medical writers who are informed about the meaning of the specific analyses. During the course of a clinical programme, usually spanning several years, this has to be refreshed and communicated to new team members to avoid unnecessary work and wrong analysis or interpretation of results.
In addition, most analyses of questionnaires require some extensive data handling after extracting the raw data from the CRF, as missing data need to be addressed, factor analyses and statistical models are often performed (e.g. regression analyses

IT & Logistics
Volume 6 Issue 154 Journal for Clinical Studies
or ANCOVA), to be able to interpret the data in a meaningful way6. This means that, ideally, project statisticians and statistical programmers, as well as team members from other functions, should have experience in analysing, selecting and interpreting complex questionnaire data.
Even after a correct and focused analysis of questionnaires, usually a large amount of data is generated, presenting results for, e.g., a total score, subscores, and down to the level of single questions by subgroup and sometimes different methodologies. Maybe the most important step in the communication of results of questionnaires is to be able to select the important parts of the data. This includes, of course, a first step focusing on those analyses that were pre-specified as part of the primary and secondary objectives of a study. However, in a second step it is also important to focus on the target audience for a specific delivery. Whereas for a CSR or a CTD document to be sent to a regulatory agency, the standard primary objective analysis is usually the most important one, a reimbursement dossier or a clinical or health outcomes-related manuscript might require additional analyses from the questionnaires that answer the specific questions of the respective audience.
The crucial step in the successful communication of questionnaire results is, therefore, a detailed publication plan that integrates the results of all questionnaires gathered in the clinical programme with the requirements of the diverse audiences. This plan should contain a grid, linking the questions to be answered with the studies providing the respective questionnaire results, and should allow the communication of these results in a coordinated manner in time from initial communications with FDA or EMA,
over publications of the pivotal results, up to targeted publications dealing with specific topics including targeting locally specific issues. In addition, the target audiences and stakeholders should be identified along with a time schedule that is in accordance with the overall clinical development plan, striving to provide information when it is needed most. A consistent approach in developing all documents related to questionnaires – from initial planning documents and protocol development, up to final publications in congresses, scientific journals, and also including marketing material that can be used to disseminate the findings of questionnaires to daily clinical practice – is mandatory for optimised drug development.
In summary, the use of questionnaires requires a coordinated approach between many functions of clinical research that needs to be maintained across the whole timeframe of a clinical programme, from late Phase I to post-marketing activities. Questionnaires should always be selected, used and communicated, with communication to the target audience in mind – and this includes the use of team members with experience in the field and a dedication to the final goals of the development programmes.
References1. Committee on Comparative Effectiveness Research
Prioritization, Institute of Medicine. Initial national priorities for comparative effectiveness research. The National Academies Press, 2009.
2. Robinson R. Cost-utility analysis. Br Med J. 1993;307:859-862.3. Torrance GW, Feeny D. Utilities and quality adjusted life years.
Int J Technol Assess Health Care. 1989;5:559-575. 4. McDowell I. Measuring health: A guide to rating scales and
questionnaires. Oxford University Press. 2006(3rd ed.).5. DeVellis RF. Scale development. Theory and applications.
Applied Social Research Methods Series 26 (Eds: Bickman L, Rog DJ), Sage Publications, 2012 (3rd ed.).
6. Svensson E. Guidelines to statistical evaluation of data from rating scales and questionnaires. J Rehab Med. 2001; 33:47-48.
Thomas Wagner, after receiving his PhD in Neurobiology and working several years in an academic environment as an Assistant Professor, started his career as a medical writer in 1999. Most of his medical writer career he has spent with Lilly Deutschland before joining Trilogy Writing & Consulting in 2009, a company specialised in providing medical writing services and consulting, and taking the position of Medical Writing Manager. The focus of his work has been writing and coordinating study protocols, study
reports and manuscripts, including health outcome projects. He has more than 10 years experience in Post-marketing Research (PMR) and regularly runs workshops on effective science communication for PMR for the European Medical Writers Association (EMWA) and pharmaceutical companies.E-mail: [email protected]

26th Annual I Vienna 2014
Di� erent Perspectives - One Vision:Better Healthcare for Patients.
EUROMEETING
ACV, Vienna, Austria I 25-27 March 2014
An unbiasedand neutralsetting. .
“
“• Participation of global regulatory agencies• The Role of Social Media in Healthcare• Patient perspective throughout the programme• Interoperability for Healthcare Providers Across the EU• Hot Topic Sessions• European Commission’s eHealth Action Plan 2012-2020• 110+ sessions in 16 parallel themes, 300+ expert speakers• 13 pre-conference tutorials• 170+ Exhibiting companies
For all detailsand to register:diahome.org/EM2014

IT & Logistics
Volume 6 Issue 156 Journal for Clinical Studies
Before and After: A Clinical Project Manager’s Story
According to some research performed with a range of pharmaceutical companies and organisations from other sectors, there are four critical factors that are instrumental to whether a business partnership delivers against its objectives. Firstly, Cultural Differences between the players. This I addressed in an article in the previous edition of JCS. Secondly, Strategic Alignment, which hopefully will be dealt with in the near future. This article deals with three and four - The Skills of the operational players in a business relationship, and the degree to which the players on both sides operate as One Team.
Why Does This Happen?Poor DeliveryThere are many reasons why some partners don’t deliver some of what they promise. But as long as they don’t, there will always be a lack of trust and a resulting relationship that is difficult to manage. No amount of skill on behalf of the people involved can really make a difference if there are fundamental problems – the initial contract is flawed; the CRO sales people over-promised. But in reality, a situation like the one Petra finds herself in is probably a mix of things she can’t change, and things she might be able to.
Team Members Lose HeartThe shortcomings of the company’s senior management are frequently a source of endless conversation and grumbling at the coffee point. If a CRO relationship is not going well, there may be all sorts of difficulties at senior level and a quick resolution is not possible. Unfortunately this is not always obvious to team members. Some may take the view that if there are fundamental reasons for a problem which are not being addressed at top management level, then ‘why bother?’
Some Team Members Can’t Read the People IssuesIn Petra’s situation, although she at first felt powerless to rescue it, it was obvious to her that there were tensions, not only between the two relationship parties, but also within the internal team. Simple observation of body language, of things unsaid – easy signs for many to read. But not for everyone. We are coming to recognise that our companies may well be peppered with ‘STEM’ individuals. These are not always, but frequently Scientific, Technical, Engineering or Mathematical experts, who may display very mild traits of autism, particularly when it comes to social skills. Most of our organisations are science-dominated. Hence, we’re likely to have more of a problem!
Project Managers are Not Fully Trained to Do ThisIn their past career, many project managers such as Petra have been through some leadership and management skills training and to some extent this prepares them to deal with issues such as motivation, teamwork and conflict. However, much of this training is rooted in ‘line management’ skills. The cross-functional project team, with the lack of direct authority over the members, presents some special challenges. The partnership situation, where project leaders essentially have to pull together a group straddling two very different organisations, is even more difficult to handle.
Clinical project managers, although perhaps not classed as ‘STEM’, nevertheless come from a background of science and data. They may readily latch on to the systems and processes of project management, with the focus on project scope, planning, risk assessment, and clear assignment of roles and responsibilities. This is fine as long as, by and large, people do what is expected of them. Trouble is, people don’t always do this.
Before and After – A Clinical Project Manager’s Story
Petra is a CPM within a major European pharma company. They signed a deal with an international CRO about one year ago and have been working fairly intensely ever since. Petra and her internal team (not to say the company’s senior management) have not been completely happy with the CRO’s performance to date. Amongst a list of grumbles, they seem less than enthusiastic to get on with agreed actions to improve recruitment rates and push through various countries’ procedures.
This is addressed at every face-to-face review meeting. The last but one, two months ago, followed a regular pattern and did not go to plan. After sitting down, without any introduction the joint team launched straight into a view of site-by-site recruitment issues. There were arguments about each site. Various outspoken members of the internal team weighed in with criticisms. It was obvious to Petra that the CRO members were stressed and uncomfortable. She had hoped to address this with an agenda item about ‘team review’ later on, but they didn’t have time for it. There were some useful actions taken away by the CRO team, but Petra and her colleagues felt less than confident that they would change things.

IT & Logistics
Journal for Clinical Studies 57www.jforcs.com
How Can We Improve on This?There are several ways that a situation like the one Petra finds herself in could be improved.
The Right Leadership MindsetParticularly at times when the project manager has time to think, they need to weigh up the approaches they will take when it comes to key points of potential conflict in the project, such as meetings.One of the best models to help this thinking is known as ‘Action Centred Leadership’. This is an approach developed by an academic called John Adair in the 1970s. It’s old but perfectly applicable today.Adair said that the leader needed to keep three things in mind at all times: what can I do to help get the Task achieved? What can I do to maintain and develop the Team? What can I do to help and develop Individual team members?
He plotted these three actions as overlapping circles, emphasising their interdependence. For example, the model predicts that even if a set of clear plans is in place to deliver task elements to a deadline, if there is dysfunction in the team, then that will compromise the task delivery.
The leader’s thinking is never too long in one of the circles. Rather it is to ‘hover’ – the ‘helicopter view’ – over all three, as much of the time as possible. Most leaders in our culture will find themselves focusing on ‘Task’ by default. This is what they are measured and monitored on. Certainly in the project environment, good team spirit and alignment, and satisfied individuals, are not readily visible. But they are still essential ‘enablers’ of good task performance and must be attended to.
The ACL model essentially tells the leader what they should focus on, but not obviously how.
Being Nice and Being ToughThe project manager, not uniquely but more than in other management roles, needs to tread a difficult balance between being strong and uncompromising in some situations, inclusive and receptive in others.
Hopefully this becomes obvious to a sufficiently perceptive individual and they will take a balanced approach that will win people over. But what will often not be obvious is the genuine authority that exists in the leader’s role, despite none of it really being formal. A thinking leader will be listened to and where reasonable, followed and obeyed.
There are two actions that will make a difference to the unsatisfactory team situations that we’ve described. Neither of them is intuitive for the typical scientific leader. They are risky, but less than you would think.
The first exemplifies the ‘being nice’ side of things and that is to make time to listen, to hear what people think and feel. One way to make this work is to reserve time at a meeting and ask an open question – such as ‘What is going well in your view, and what is not going so well?’ Then allow everyone present to speak their mind, in turn. A different question might be: ‘What is your view of the situation we are in at the moment’? Again, the leader should enforce a fair level of air-time for each person. You know you are starting to get somewhere when, for example, an internal team member and a CRO member describe the same occurrence very differently. Rather than continuing to fuel a to-and-fro argument, teasing out how such a dichotomy happened will really produce some insight on how you should be doing things differently.
This sort of thing might seem time-consuming and slow to some people, but at the right time it can uncover some causes of conflict that were not obvious.
The second action is on the ‘tough’ side of things, and it is to establish productive behaviours across the teams. One technique is called ‘Non-negotiables and Negotiables’. Again it requires the leader to take some time out with the team. Of course it’s better if this can be done at the ‘kick-off’ of the relationship, but that’s not always possible The real skill of the partnership project manager is to think through their own situation and use various approaches at need. An experienced coach / facilitator can really help to guide the
leader through the process until she becomes used to it. But little by little, leadership behaviour will rub off onto other team members, and aiming to get the bottom of relationship problems will become more common.
Can We Work as ‘One Team’?Organisations are full of ‘subcultures’, by which we mostly mean people having similar professions. It is natural for people to associate with like-minded colleagues, who often work together in departments on a day-to-day basis. This will be seen in what many call ‘silo management’, the classic hierarchical structures of divisions, departments and so on. For many years people have
Figure 1: The Action Centred Leadership Model

Volume 6 Issue 158 Journal for Clinical Studies
IT & Logistics
58 Journal for Clinical Studies
been complaining about how these structures work bureaucratically, slowing decisions and stifling creativity. For these reasons, and in an attempt to bring in a customer focus to the business, we usually work in project teams – a ‘cross-functional’ system where the various disciplines – clinical, preclinical, regulatory and so on – work together.
In a pharma-CRO partnership, there will usually be members of the same subculture on both sides. So for example, there will be a data management person in the internal team, and another in the CRO team.
An untrained ‘fly on the wall’ at a typical partnership review meeting might not pick up any major dysfunctions. Indeed, to follow our earlier example, we would find the data management people chatting in a friendly way about their detailed work, during coffee and lunch breaks. However, although this is a subtle thing to tease out, we often find that what the subculture members have in common is not quite as strong as their default loyalty to their own company, i.e. the partnership will split along company lines fairly easily.
For some, this will be an obvious thing to happen, and rather than a problem, will be something to celebrate. The CRO members are contractors, paid to deliver a service. The fact that all of the pharma sponsor team members align themselves with the business needs of
the company might be seen as a good thing. Ultimately, however, continuing to operate in this way might be risky, however difficult that is to accept. There are two reasons why a partnership should aim to build a form of ‘One Team’ spirit across the two sides.
Firstly, almost every business partnership will not have quite enough resource to deliver what it needs to. There is always a ‘stretch’ required in any project these days. People in companies are very used to this and phrases like ‘going the extra mile’ and ‘stretch targets’ are common. Of course a degree of trust is required in the organisation for people to continue to give extra efforts; building team spirit is one way of making this happen.
Secondly, the only certainty in drug development is that some things will not go as you expect. Changes in plans always happens,
and we need people to absorb and run with these changes. A contract cannot include every minor change that may happen sometime in the future. Building a ‘One Team’ atmosphere will pay dividends and is not that difficult. Set up a simple structure for some conversations and some social time, and natural human behaviour will do the rest.
Trust is built between business people by asking questions such as:• Who are we? What can we share about our backgrounds to get
to know each other more?• How do we work? What are the differences between our
companies in how the management levels work, how we make decisions, the role-names we have and what these mean?
• What exactly does this team need to achieve?• What do we need to clarify about expectations from each of us?
Which decisions can we make? Which can’t we make?• How will we communicate? What is the ideal meeting schedule?
What will we do if certain things go wrong? Who will get involved?
• Anything else we don’t understand?• What shall we do to socialise, if we can?
There may be some more questions, maybe less. But this could take a day. Or at minimum, a short day. You should hire a facilitator. The whole thing could cost you, say £10,000. Scary? Well, the trial is going to cost your company how much? Ten million? You could potentially stop escalation of that budget, or save months of overruns.
Before the most recent face-to-face meeting, Petra had the opportunity to prepare, talking through the options with a leadership coach that the company provided.On the day, following the coffee and usual preliminaries, as they all sat down she resisted the teams’ pressure to work through the latest spreadsheets. They had even been loaded ready, and were projecting on screen!
She turned off the projector and stated that she wasn’t happy with the way things were going, and that some fundamental issues needed to be addressed. Rather than the dissent she feared, there were a range of agreeing nods around the table.She took a deep breath and asked the team members to say how they each felt about things, and gave each person the opportunity to express their view. This took an hour, but it was really worthwhile. There certainly were some resource issues identified about which nobody present could do anything. But plenty of others that hadn’t really been aired before. Several CRO members voiced their stress about the ‘interrogation’ style of the internal members; others said that the meetings’ timing arrangements were very awkward, but hadn’t wanted to complain before. Internal members said that they frequently received very short notice communications about problems. One of the most far-reaching decisions made at the end was to take the detail of the recruitment progress reviews offline to a smaller and more relevant group. This would save huge amounts of time in future! And of course, at the end of this Petra learned a powerful lesson in project team leadership.
John Faulkes began his career as a scientist in the pharma industry, then in HR as an L&D Business Partner, before founding a training /consulting business, and a learning-related IT firm. John has helped Pharmaceutical cross-functional teams and Pharma-CRO partnerships to understand what is preventing them from working efficiently, and helping them to build effective teamwork. John runs training programs, consults with managers and provides coaching to
leaders, particularly those with complex assignments. Email: [email protected]

Tim DavisGlen de Vries
Speakers include
Exco InTouchMedidata Solutions Quintiles Transnational Corp.
Omniscience Mobile mHealth Regulatory Coalition
Pfizer
Tom Ruane
Jeff Lee Bethany J Hills Craig Lipset
A brand new event, exploring the opportunities and barriers to adopting mobile technology in clinical trials.
In association with
CLINICAL TRIALS ARE GOING MOBILE!
+44(0)1306 500 124 [email protected]
Book Your Place Online: www.mct-congress.co.uk
twitter: @mctcongress
or contact Veronique Madsen

Volume 6 Issue 160 Journal for Clinical Studies
IT & Logistics
Going Mobile with Clinical Trials
The use of mobile technology to enhance healthcare services and improve health outcomes is familiar practice across healthcare systems worldwide, but what impact are these kinds of technologies having on the clinical research process? The use of mHealth solutions presents a much-needed opportunity for sponsors to innovate studies, offering the potential to reduce overall development costs, while improving subject recruitment and increasing patient and investigator satisfaction. With billions of people around the world having access to mobile devices, deciding to go mobile with clinical trials is no longer a simple choice, but a strategic necessity for successful patient engagement, effective decision-making and accurate data collection.
Although mHealth has the potential to make a great impact on clinical research, many organisations are still uncertain on how to capitalise on new advances in the field. Here, Journal for Clinical Studies puts some of the industry’s most frequently asked questions to mHealth’s leading influencers to find out their experiences and predictions for what’s in store in 2014 and beyond.
Tim Davis - CEO, Exco InTouch
How will mobile technology shape healthcare in the next five years?The rise in access to mobile communication globally is staggering, and healthcare won’t be alone in seeing enormous changes as a result. Mobile technology and smart devices will become commonplace to help patients and
caregivers better manage conditions. The ability to self-monitor, and receive personalised information and advice as a result, will see us all having greater involvement in our own healthcare. For payers and providers, this provides a wealth of opportunities - I expect to see mobile driving increased access to healthcare as well as payment reforms and changes in hospitalisation patterns in the next few years. Perhaps the question should be ‘how won’t mobile technology shape healthcare.
Jeff Lee - Founder of Omniscience Mobile
What role does mobile technology play in clinical research?The ubiquitous presence of wireless devices stands to fundamentally transform research. Making it easier for data to be collected from patients, and reported by them, increases the accuracy of study findings, while making the research endeavour significantly more efficient. But
that’s not what gets me really excited about this technology. I’m most driven by the opportunity for mobile technology to make research more patient-centric. Mobile phones are intensely
personal devices and they can help a study patient feel more empowered and connected to the research initiative. Mobile technology will increasingly be an essential part of the successful research patient experience.
Bethany J. Hills - Member of the Firm at Epstein Becker Green
In your opinion, what needs to be done from a policy perspective to improve the impact of mHealth in everyday healthcare?Government and private policy should focus on the obstacle faced in providing or obtaining appropriate reimbursement for

Journal for Clinical Studies 61www.jforcs.com
IT & Logistics
the fundamentally different clinical model that can result with the use of mobile medical apps (MMAs). The current reimbursement methodologies do not contemplate regular engagement with patients from remote locations. With the development of clinical evidence of the benefit of MMAs still in the early stages, government and private payers have yet to be convinced of the clinical benefit and the true value proposition with enough confidence to provide direct coverage or to structure value-based incentives that maximise the opportunity that mobile medical applications present.
David Quarm - Solutions Architect at Medidata Solutions Worldwide
How has the mHealth landscape changed over the past five years?The biggest development in the mHealth landscape, and consequently, on patient engagement, is the near ubiquity of the smartphone, and the emergence of mHealth apps that rely on key smartphone capabilities, such as location services,
gyroscopes, accelerometers, and integrated calendaring and alerts. This confluence of personal devices and health apps has also given rise to an explosion of innovation, with such developments as integrated ECG cases, USB glucometers, bluetooth-connected thermometers, and other devices, apps and accessories that surpass previous tools in terms of usability, engagement and the depth and breadth of data being measured.
Matt Kibby - Global Operations Leader at BBK Worldwide
What are the benefits of mHealth in supporting patient engagement?By making an investment in mHealth, your patient recruitment campaign will undoubtedly reap the benefits. With 100 million Americans and more than a billion people globally using mobile devices,
deciding to go mobile is no longer a choice. BBK Worldwide research shows that providing patients with helpful resources upfront can directly support a sponsor’s patient recruitment efforts elsewhere. Moreover, from a patient perspective, a clinical trial sponsor demonstrates their commitment to educating patients about their options and meeting them where they are - online. Simply put, if clinical trial sponsors and study sites do not engage patients online and during the decision-making process, they put their study at risk because patients may go elsewhere.
Dr Steve Hutson - Founding Director of Virtual PV Limited
What do you think the greatest barrier to mHealth innovation is within the industry?Maintaining the confidentiality and integrity of company and patient data are major concerns for pharmaceutical professionals and for regulators. Those
considering novel mHealth technologies want to be confident they can continue to comply with required good pharmaceutical practices (GxPs) and can validate these systems. Unfortunately, many mHealth suppliers don’t fully appreciate the importance of validation to the pharmaceutical industry, or how to develop their software to the required standard. This makes it difficult for adopters to achieve a validated state, and increases the risk of latent faults and vulnerabilities coming to light (with associated costs). Several published papers have raised concerns on this subject. Until more mHealth suppliers address validation, it will remain a significant barrier to the adoption of innovative mHealth solutions within the pharmaceutical industry.
Sheila Rocchio - VP Marketing and Product Management at PHT Corporation
Do you think mHealth has the power to improve the provider-patient experience?Yes, absolutely. During the last 20 years, numerous industries have been transformed by the use of technology and the direct connection of people and products. Amazon, LinkedIn, Facebook,
and NetFlix are just a few examples of technology removing barriers and creating new opportunities to increase customer satisfaction and convenience. Clinical trials have been using the same models for 50+ years with technology systems focused on sponsors and sites but not patients. Mobile phones, physiological measurement devices, video chat and real-time access to data and “blue button” capabilities make research more accessible, convenient and beneficial to patients, and easier for providers. The above contributors will be part of the MCT-Congress, a new mHealth event taking place in Edinburgh, March 20-21, 2014. For further information please visit www.mct-congress.co.uk

Volume 6 Issue 162 Journal for Clinical Studies
Sigma-1 receptor Implicated in Cell Survival of Rare Neurodegenerative Diseases Anavex Life Sciences Corp. announced that a publication in the current issue of scientific journal Neuropathology potentially extends the opportunity for ANAVEX PLUS to additional neurodegenerative diseases beyond Alzheimer’s. The report demonstrates for the first time, evidenced by human brain autopsies, that the sigma-1 receptor (Sig-1R) is also involved in a family of neurodegenerative genetic disorders including Huntington’s disease (HD), dentatorubral-pallidoluysian atrophy (DRPLA), and spinocerebellar ataxia types 1, 2 and 3 (SCA1, SCA2, SCA3). They are caused by abnormal expansion of a polyglutamine stretch in each of the unrelated causative proteins. Sig-1R was consistently expressed and co-localized with neuronal nuclear inclusions in these polyglutamine diseases, confirming the implication of Sig-1R in cell survival in these neurodegenerative diseases.
The report, entitled “Accumulation of the sigma-1 receptor is common to neuronal nuclear inclusions in various neurodegenerative diseases,” was authored by Dr. Yasuo Miki, Department of Neuropathology, Institute of Brain Science, Hirosaki, Japan, and industry colleagues.Source: Anavex Life Sciences Corp.
Researchers identify variation in gene PLD3 can increase risk of late-onset Alzheimer’s diseaseA new study, part-funded by the Medical Research Council (MRC), the Wellcome Trust and Alzheimer’s Research UK, has shown that a fault in a gene called phospholipase D3 (PLD3) can contribute to the overproduction of amyloid-beta in the brain. Increased levels of this chemical are associated with an increased chance of developing Alzheimer’s disease and the results show that, in certain cases, this can double an individual’s risk.
Professor John Hardy who led the UK work at University College London (UCL) and was funded by the Medical Research Council and the Wellcome Trust said: “The use of the new technologies of whole genome and whole-exome sequencing in Alzheimer’s disease is now yielding a rich harvest of genetic variants which influence our risks of developing disease. These re-enforce the critical role of amyloid deposition and breakdown in the brain as one of the ‘main events’ that can cause Alzheimer’s disease.”
Rebecca Wood, Chief Executive of Alzheimer’s Research UK, the UK’s leading dementia research charity, said: “This announcement, made just off the back of the G8 dementia research summit, is a timely reminder of the progress that can be made by worldwide collaboration. Alzheimer’s Research UK is proud to have contributed to this discovery, both by funding researchers and through the establishment of a DNA collection that has been used in many of the recent genetic discoveries in Alzheimer’s.”Source: MRC
Ground-Breaking First-In-Man, First-In-Class Clinical Trial in Oncology with Genetically Modified Mesenchymal Stromal Cells Is Now EnrollingAs a world first, apceth announced that the TREAT ME Phase I/II clinical trial for patients suffering from advanced adenocarcinoma of the gastro-intestinal tract has commenced. This is the first clinical trial world-wide with genetically-modified mesenchymal stromal cells (MSCs).
This innovative next-generation MSC therapy is based on cells harvested from the patient’s own (autologous) bone marrow, which are processed, genetically modified and re-infused into the patient. The cells specifically target the tumor, or its metastases, where the cytotoxic gene product is selectively activated, increasing local efficacy with reduced systemic toxicity, one of the main problems of systemic chemotherapy. This unique principle is also applicable to other cancer types. apceth intends to advance this treatment to an off-the-shelf product where cells obtained for healthy donors will be used to treat multiple patients.“We are the first to use next-generation MSC-based therapies in the clinic. This is a platform technology that carries significant potential and represents the future of cell therapies”, said apceth’s CEO, Dr Christine Guenther.Source: B3C newswire
Nuevolution Enter Drug Discovery Collaboration with The Institute of Cancer Research (ICR) and Cancer Research Technology (CRT)The Institute of Cancer Research (ICR), London, Cancer Research Technology (CRT), London and Nuevolution A/S, Copenhagen have entered into a drug discovery collaboration to identify novel lead candidates for cancer treatment.
Researchers will use Nuevolution’s screening technology, Chemetics®, to screen libraries each of millions of DNA-tagged compounds to identify those that act on a key protein in the stress response pathway, which has an important role in cancer cell survival and resistance to cancer treatments. This state-of the-art screening technology allows potent drug leads to be identified quickly, accurately and from very large and complex compound mixtures.
The three-way deal between the ICR, Nuevolution and CRT, the commercial arm of Cancer Research UK, builds on an existing collaboration between CRT and Nuevolution, which aims to identify drug leads that block the activity of several challenging cancer targets of therapeutic interest. Under the new deal, the Cancer Research UK Cancer Therapeutics Unit at the ICR and Nuevolution will collaborate to screen a key target within the stress response pathway. Researchers from the Cancer Research UK Cancer Therapeutics Unit at the ICR will provide detailed insights and scientific expertise on the specific stress pathway target as well as their extensive experience in cancer drug discovery and development. Nuevolution will provide its proprietary Chemetics®

JCS News
Journal for Clinical Studies 63www.jforcs.com
technology, screening expertise and medicinal chemistry expertise to optimise drug candidates.Source: B3C newswire
Sanofi to expand access to clinical trial dataSanofi will expand access to information and data from clinical trials, sponsored by companies of the Sanofi group, in support of industry-wide efforts to promote a set of Principles for Responsible Sharing of Clinical Trial Data that the Pharmaceutical Research and Manufacturers of America (PhRMA) and the European Federation of Pharmaceutical Industries and Associations (EFPIA) jointly released in July 2013.
Sanofi will provide access to clinical trial data and related documents, including Clinical Study Reports (CSR), for studies sponsored by Sanofi companies that conduct clinical studies in humans. These studies must have been submitted to U.S. and E.U. regulatory agencies and the product must have been approved by both agencies on or after January 1, 2014. For Sanofi Pasteur, requested studies must have been submitted either to the U.S. or E.U. regulatory agencies and the product must have been approved by either agency on or after January 1, 2014.
Sanofi will continue to submit for publication the results from all company-sponsored clinical studies, regardless of the study outcome. In addition, the industry, including Sanofi, is working with regulators to adopt mechanisms so that clinical study sponsors will be able to provide lay language summary results directly to the individuals who participate. To enable the process for requesting and gaining access to clinical trial data, Sanofi is participating in a multi-company portal for clinical trial data sharing (https://clinicalstudydatarequest.com).Source: MedicalNewsToday.com
A new drug for the treatment of type 2 diabetes approved by FDAThe US Food and Drug and Administration has announced the approval of a drug called Farxiga (dapaglifozin) to help treat adults with type 2 diabetes. The tablets, in combination with diet and exercise, are said to improve control of blood sugar levels.
Farxiga, a sodium-glucose co-transporter 2 inhibitor (SGLT2), works by preventing the kidney from reabsorbing glucose. This increases the excretion of glucose and reduces blood sugar levels. According to the US Food and Drug Administration (FDA), 16 clinical trials involving more than 9,400 patients with type 2 diabetes assessed the safety and effectiveness of the drug. These trials demonstrated that Farxiga was able to improve HbA1c (hemoglobin A1c or glycosylated hemoglobin) levels - a measure of blood glucose control - in type 2 diabetic patients.
Dr. Curtis Rosebraugh, director of the Office of Drug Evaluation II at the FDA’s Center for Drug Evaluation and Research, said: “Controlling blood sugar levels is very important in the overall
treatment and care of diabetes, and Farxiga provides an additional treatment option for millions of Americans with type 2 diabetes.”According to FDA, as well as being assessed as a stand-alone therapy, the drug has also been tested in combination with other treatments for type 2 diabetes, including insulin, pioglitazone, metformin, glimepiride, and sitagliptin.Source: MedicalNewsToday.com
Positive top-line data from the pivotal Phase 3 programme of ST10 for the treatment of iron deficiency anaemia (IDA) in inflammatory bowel disease (IBD)Shield Therapeutics (Shield), an independent specialty pharmaceutical company focused on the development of mineral-derived hospital pharmaceuticals, has announced strongly positive top-line data from the pivotal Phase 3 programme of ST10 for the treatment of iron deficiency anaemia (IDA) in inflammatory bowel disease (IBD).
ST10, a novel orally-dosed form of ferric iron, delivered a mean improvement in haemoglobin levels of 2.3g/dL (p <0.0001), clearly meeting the primary endpoint of haemoglobin change after 12 weeks’ treatment compared to placebo. The two AEGIS protocols recruited 128 patients with anaemia secondary to either Crohn’s disease or ulcerative colitis who had previously failed therapy with oral ferrous products due to intolerance and/or inadequate therapeutic benefit.
These results provide confirmatory pivotal clinical data which will form the basis of a Marketing Authorisation Application submission to the European regulatory authorities during 2014. In conjunction with data that will be generated from the study of ST10 in the treatment of IDA in pre-dialysis chronic kidney disease patients that is currently progressing, these results will also form part of a subsequent New Drug Application submission to the FDA in the USA.Source: MedicalNewsToday.com

Volume 6 Issue 164 Journal for Clinical Studies
Advertisers Index
I hope this journal guides you progressively, through the maze of activities and changes taking place in these Emerging Countries.
JCS has also launched a Weekly Newsetter. Please visit www.jforcs.com and sign up to receive the very informative weekly news letter.
Page 11 8th Annual Conference on Paediatric Clinical Trials (SMi Group)
Page 55 26th Annual EuroMeeting (Drug Information Association)
Page 3 ARIANNE Corp
Page 43 Packaging Coordinators, Inc
Page 41 Cmed Group Ltd
Page 7 Dora Wirth Languages
Page 13 INTERLAB GmbH
Page 59 MCT – Congress
IFC MediciGlobal
Page 23 MediLingua Medical Translations B.V.
Page 25 MENE CLINICAL RESEARCH
Page 5 Myoderm
Page 51 Synevo Central Lab
Page 47 Synergy Research Group
Page 49 Trilogy Writing & Consulting GmbH
IBC Woodley Equipment Company Ltd
OBC Turkish Cargo – A Brand of Turkish Airlines
Page 33 World Courier – An AmerisourceBergen Company
www.jforcs.com
PEER REVIEWED
Volume 6 - Issue 1
Alzheimer’s Disease without Dementia A New Journey of Care
Logistics in Emerging Markets A New Watch Series
The Role of Regulatory Agencies in New Drug DevelopmentA Global Perspective
Using Questionnaires in Clinical ResearchA Guide through the Data Jungle
JOURNAL FOR
Your Resource for Multisite Studies & Emerging MarketsCLINICAL STUDIESU
Subscribe today at www.jforcs.com or email at [email protected]
JOURNAL FOR
Your Resource for Multisite Studies & Emerging MarketsCLINICAL STUDIESU

WE KEEP YOUR
CLINICALTRIALSON SPECIFICATION
Blood Pressure Monitoring
Capnography
Centrifuges
ECG Monitoring
Infusion Systems
Laboratory Equipment
Medical Freezersinc. Ultra Low Temperature
Medical Refrigerators
Patient Thermometers
Point of Care
Pulse Oximeter
Spirometer
Temperature Monitoring
Vital Signs Monitoring
Weighing, Measuring & Examination
...we won’t let you down
• Equipment rental/purchase
• Complete worldwide logistics
• Calibration, servicing and technical support available
• Breakdown equipment replaced free of charge
• Global equipment solutions/ outsourced procurement
• Turnkey solutions
Ensuring the simplicity and continuity ofyour study, we are your one centralisedsupplier; delivering the correct, protocol-specified equipment for your clinicaltrials.
As a leading medical and laboratoryequipment supplier, sourcing from allestablished manufacturers, we supportthe largest and smallest clients acrossthe world.
UK Office: T: +44(0)8456 777001 F: +44(0)8456 777002
USA Office: T: 1-800-471-9200 F: 1-508-625-1721
www.woodleyequipment.comFor protocol-specified products visit
Journal for Clinical Studies - full page 22/1/14 07:31 Page 1

C
M
Y
CM
MY
CY
CMY
K
THY CARGO ILAC ING Clinic Journal 210X297.pdf 1 25.12.2013 15:02