j am dent assoc 2009 spear 1160 6
TRANSCRIPT

5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 1/8
2009;140;1160-1166 J Am Dent Assoc
Frank SpearAnterior Tooth ReplacementImplants or Pontics: Decision Making for
jada.ada.org ( this information is current as of July 27, 2011):The following resources related to this article are available online at
http://jada.ada.org/content/140/9/1160in the online version of this article at:
including high-resolution figures, can be foundUpdated information and services
http://jada.ada.org/content/140/9/1160/#BIBL, 0 of which can be accessed free:15 articlesThis article cites
http://www.ada.org/990.aspxthis article in whole or in part can be found at:of this article or about permission to reproducereprintsInformation about obtaining
© 2011 American Dental Association. The sponsor and its products are not endorsed by the ADA.

5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 2/8
1160 JADA, Vol. 140 http://jada.ada.org September 2009
PERSPECTIVES CLINICAL DILEMMAS
Science has provided
today’s restorative
dentist with continu-
ally improving tools for
the replacement of
missing teeth, and providing
esthetically pleasing outcomes
for single missing anterior teeth
is a highly predictable procedure
in the hands of most clinicians.
The predictability decreases
substantially when significantbone and soft tissue also have
been lost; however, even in this
scenario, a competent interdisci-
plinary team generally can pro-
duce an acceptable result by
using an implant or a fixed par-
tial denture with an ovate pontic
to replace the missing tooth.
When the loss is not of one tooth
but of numerous teeth, particu-
larly if those teeth are adjacent
to each other, the esthetic chal-
lenge is immensely morecomplex.
As implants have improved
and placement techniques have
evolved to take advantage of
those improvements, the
informed clinician may gravitate
toward use of implants as the
preferred solution for all missing
teeth. As implant science con-
tinues to improve, the use of
fixed partial dentures may
become an anachronism, much
like the specialized preparations
of hemisectioned molars re-
quired in perioprosthodontics.
At one time, the technique for
creating these unusual prepara-tions was taught in every dental
school; today, it is a lost art.
Fortunately, the loss is realized
only in situations in which bone
grafting, implant placement or
both are impossible—an ever-
decreasing occurrence. Although
it may be preferable to have a
“root” wherever a tooth is
missing, the esthetic challenges
presented by multiple missing
anterior teeth often require the
combination of implants andovate pontics to achieve accept-
able esthetic results.
The average papillary height
above bone between natural
teeth is 4.5 millimeters.1,2 When
a single-tooth implant is placed,
papillary levels are determined
by the height of the bone on the
adjacent natural teeth, not by
that of the bone around the
implant.3-5 Therefore, the papil-
lary height between a tooth and
an implant will be similar to
what it was before tooth
removal. The facial gingival
margin around the implant is
related to the bone levels on theimplant, as well as to the thick-
ness and position of the free gin-
gival margin before tooth
removal.6,7
SINGLE MISSING ANTERIORTEETH
The least predictable soft-tissue
outcome with a single anterior
implant is associated with inter-
proximal bone loss in the adja-
cent natural teeth. Because
interproximal bone determinespapillary height, creating
esthetic papillary heights can be
difficult. If the newly edentulous
space is to receive not an
implant but rather a pontic as
part of a fixed partial denture,
the bone level on the teeth adja-
cent to the space still will deter-
mine the papillary heights.
Implants or ponticsDecision making for anterior tooth replacement
Frank Spear, DDS, MSD
Copyright © 2009 American Dental Association. All rights reserved. Reprinted by permission.

5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 3/8
JADA, Vol. 140 http://jada.ada.org September 2009 1161
PERSPECTIVES C L I N I C A L D I L E M M A S
The most significant differ-
ence between a pontic and an
implant is that the clinician can
significantly alter the soft tissue
that will surround a pontic and
create a papilla by means of soft-tissue grafting procedures.
When the clinician places a soft-
tissue graft, the amount of
tissue above the bone between a
pontic and a natural tooth, or
between a pontic and an
implant, averages 6.5 mm—an
increase of 2.0 mm, or 44 per-
cent. In some patients, the
tissue height after grafting can
be as high as 9.0 mm.8
When natural teeth adjacent
to a single edentulous spacehave bone loss, soft-tissue ridge
augmentation followed by place-
ment of a pontic always will
achieve greater coronal papil-
lary height than will a single-
tooth implant placed into the
edentulous space. In a situation
in which the papilla, to be
esthetically acceptable, must be
more than 4.5 mm above the
level of the bone, placement of a
fixed partial denture with anovate pontic is the most appro-
priate treatment decision.
MULTIPLE MISSING ANTERIOR TEETH
When multiple teeth are
missing or require removal, the
soft-tissue ramifications are dif-
ferent because of the biology of
the periodontium and the
responses of the bone and soft
tissues. To understand these
ramifications, it is helpful toconsider the biological response
of the soft tissue after tooth
removal. In a case involving the
removal of two central incisors,
the interproximal bone height
on the lateral incisors will deter-
mine the papillary height be-
tween the lateral incisors and
whatever is placed in the space.
The soft tissue on the mesial
side of the lateral incisor will act
exactly as it would in the case of
a single-tooth replacement. The
facial free gingival margin
height in each central incisorsite also will be similar in
response to a single missing
tooth. The facial bone level and
tissue thickness will determine
the height at which the facial
gingival margin stabilizes. The
difference between the single
edentulous space and the space
created by removal of the two
central incisors is what happens
to the papilla that existed
between them before the
extractions.9,10
If we assume no periodontaldisease existed before tooth
removal, the osseous crest
around both central incisor sites
will follow the scalloped form of
the cementoenamel junction.
The gingiva on the facial bone
will be positioned so that, on
average, the free gingival
margin is 3.0 mm coronal to the
osseous crest. As the cemento-
enamel junction flows from the
facial aspect into the interprox-
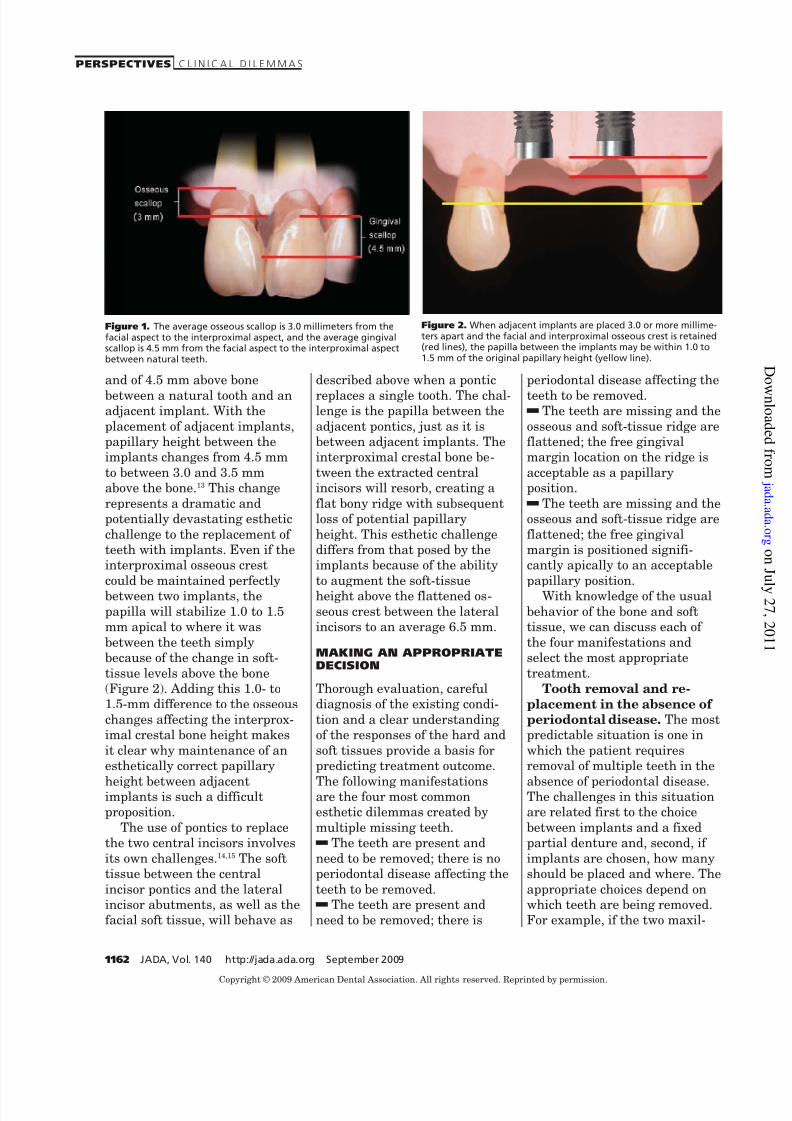
imal aspect, the bone follows,and an average osseous scallop
of 3.0 mm is created. Because
soft tissue follows the scallop of
the bone, the osseous scallop
presumably should result in a
gingival scallop of 3.0 mm. How-
ever, when teeth are present, an
interesting phenomenon occurs:
the papilla is 1.5 mm more
coronal to the osseous crest than
to the facial tissue. This addi-
tional 1.5 mm added to the
3.0-mm average osseous scallop
results in the tip of the papilla’s
matching the 4.5-mm averagenoted previously (Figure 1). The
restorative challenge created by
the loss of both central incisors
relates directly to the osseous
scallop that existed between
those incisors.
Replacement of the central
incisors with two single
implants adjacent to each other
is one of the prosthetic restora-
tive options available. During
placement, the clinician places
the implant apically until theplatform is level with the facial
osseous crest. Most implants in
use today are not scalloped;
because the bone is scalloped,
the interproximal platform of
the implant may be apical to the
interproximal osseous crest by
as much as 3.0 mm. Although
implant placement retains bone
that would be lost if the site
remained edentulous, a certain
amount of bone adjacent to theimplant is expected to resorb
across time, usually to the level
of the first thread of the
implant.11,12 Resorption of the
interproximal osseous crest
results in a flattening of the
osseous crest. Maintaining a
minimum distance of 3.0 mm
between implants seems to
lessen this flattening, but
researchers agree that, regard-
less of the distance between
implants, the crestal boneundergoes some degree of
resorption and flattening.13
The visible and esthetic issue
in these osseous changes is the
corresponding flattening of the
gingival architecture. Tarnow
and colleagues13 identified a
papillary height of 4.5 mm above
bone between two adjacent teeth
The restorative challenge
created by the loss of both
central incisors relatesdirectly to the osseous
scallop that existed
between those incisors.
Copyright © 2009 American Dental Association. All rights reserved. Reprinted by permission.
5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 4/8
1162 JADA, Vol. 140 http://jada.ada.org September 2009
PERSPECTIVES C L I N I C A L D I L E M M A S
and of 4.5 mm above bone
between a natural tooth and anadjacent implant. With the
placement of adjacent implants,
papillary height between the
implants changes from 4.5 mm
to between 3.0 and 3.5 mm
above the bone.13 This change
represents a dramatic and
potentially devastating esthetic
challenge to the replacement of
teeth with implants. Even if the
interproximal osseous crest
could be maintained perfectlybetween two implants, the
papilla will stabilize 1.0 to 1.5
mm apical to where it was
between the teeth simply
because of the change in soft-
tissue levels above the bone
(Figure 2). Adding this 1.0- to
1.5-mm difference to the osseous
changes affecting the interprox-
imal crestal bone height makes
it clear why maintenance of an
esthetically correct papillary
height between adjacentimplants is such a difficult
proposition.
The use of pontics to replace
the two central incisors involves
its own challenges.14,15 The soft
tissue between the central
incisor pontics and the lateral
incisor abutments, as well as the
facial soft tissue, will behave as
described above when a pontic
replaces a single tooth. The chal-lenge is the papilla between the
adjacent pontics, just as it is
between adjacent implants. The
interproximal crestal bone be-
tween the extracted central
incisors will resorb, creating a
flat bony ridge with subsequent
loss of potential papillary
height. This esthetic challenge
differs from that posed by the
implants because of the ability
to augment the soft-tissueheight above the flattened os-
seous crest between the lateral
incisors to an average 6.5 mm.
MAKING AN APPROPRIATEDECISION
Thorough evaluation, careful
diagnosis of the existing condi-
tion and a clear understanding
of the responses of the hard and
soft tissues provide a basis for
predicting treatment outcome.
The following manifestationsare the four most common
esthetic dilemmas created by
multiple missing teeth.
dThe teeth are present and
need to be removed; there is no
periodontal disease affecting the
teeth to be removed.
dThe teeth are present and
need to be removed; there is
periodontal disease affecting the
teeth to be removed.dThe teeth are missing and the
osseous and soft-tissue ridge are
flattened; the free gingival
margin location on the ridge is
acceptable as a papillary
position.
dThe teeth are missing and the
osseous and soft-tissue ridge are
flattened; the free gingival
margin is positioned signifi-
cantly apically to an acceptable
papillary position.With knowledge of the usual
behavior of the bone and soft
tissue, we can discuss each of
the four manifestations and
select the most appropriate
treatment.
Tooth removal and re-
placement in the absence of
periodontal disease. The most
predictable situation is one in
which the patient requires
removal of multiple teeth in the
absence of periodontal disease.The challenges in this situation
are related first to the choice
between implants and a fixed
partial denture and, second, if
implants are chosen, how many
should be placed and where. The
appropriate choices depend on
which teeth are being removed.
For example, if the two maxil-
Figure 1. The average osseous scallop is 3.0 millimeters from thefacial aspect to the interproximal aspect, and the average gingivalscallop is 4.5 mm from the facial aspect to the interproximal aspectbetween natural teeth.
Figure 2. When adjacent implants are placed 3.0 or more millime-ters apart and the facial and interproximal osseous crest is retained(red lines), the papilla between the implants may be within 1.0 to1.5 mm of the original papillary height (yellow line).
Copyright © 2009 American Dental Association. All rights reserved. Reprinted by permission.

5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 5/8
JADA, Vol. 140 http://jada.ada.org September 2009 1163
PERSPECTIVES C L I N I C A L D I L E M M A S
lary central incisors are being
removed and they are supported
by healthy bone, placing adja-
cent implants can result in a
predictable and esthetic final
result. The papilla between thecentral incisor implants and the
adjacent lateral incisors will be
excellent, the facial gingival
margins can be augmented
easily, if required, and the
papilla between the central
incisor implants should remain
within 1.0 to 2.0 mm of the pre-
extraction papillary level if the
clinician places the implants
3.0 mm apart and most of the
interproximal osseous crest is
maintained (Figure 3). The clini-cian could treat this same
patient with a fixed prosthesis
by using the lateral incisors as
abutments. Since the interprox-
imal bone between the extracted
central incisors most likely will
be lost, the risk of soft-tissue
recession in the area in which a
papilla needs to be created
between central incisor pontics
is an esthetic challenge. As
described previously, soft-tissueaugmentation before completing
the restoration creates signifi-
cant tissue height that could be
used to form an excellent papilla
between the pontics.
When the teeth to be removed
involve a central incisor and a
lateral incisor, or a lateral
incisor and a canine, the treat-
ment choices become much less
clear. The difficulty encountered
is twofold. First, placement of
adjacent implants in the centralincisor and lateral incisor sites,
or the lateral incisor and canine
sites, is difficult if the surgeon is
to maintain a minimum of 3.0
mm between the platforms of
the implants. This situation
means there is a high risk that
interproximal osseous crest will
be lost between the implants
across time, with subsequent
loss of papillary height (Figure
4). Second, when papillary
height is lost between the cen-
tral incisor and lateral incisor
on one side while natural teeth
exist on the other side, the dis-
crepancy in papillary height ismuch more noticeable than a
slight loss of papillary height in
the middle of the face between
adjacent central incisor im-
plants. These reasons—combined
with the fact that use of adja-
cent implants to replace a cen-
tral incisor and a lateral incisor,
or a lateral incisor and a canine,
is not required for force manage-
ment in the anterior aspect—
make placement of a single
implant in the site of the centralincisor or the canine, with a can-
tilever replacing the lateral
incisor as an ovate pontic,
esthetically more predictable
and functionally acceptable.
An alternative for prosthetic
replacement of a missing central
incisor and lateral incisor or lat-
eral incisor and canine is sur-
gical soft-tissue augmentation
and placement of a fixed partial
denture. Although this method
can create a pleasing esthetic
result, it is a much more com-
plex restoration structurally and
functionally, particularly when
the lateral incisor and thecanine are being replaced by
pontics.
When removal of three or four
adjacent anterior teeth with
good periodontal support is
required, my preference is place-
ment of implants separated by
one or two pontics. If both cen-
tral incisors and one lateral
incisor need to be removed, I
would choose placement of one
implant in the proximal central
incisor site, placement of a cen-tral incisor ovate pontic and
placement of the second implant
in the lateral incisor site. This
design allows the creation of
excellent papillary heights in all
locations because of the pre-
dictability of the soft-tissue aug-
mentation in the ovate pontic
site (Figure 5).
Figure 3. A. A patient who required the extraction of both central incisors. Note theexcellent bone level and papillary height. B. Because the interproximal osseous crest wasmaintained and the soft tissue supported at the time of tooth removal, an excellent interim-plant papilla exists. C. Final restorations exhibit minimal change in papillary height whencompared with pre-extraction height. Even in this ideal situation, the difference is 1.0 to 1.5millimeters apically. Photographs courtesy of Dr. Greggory Kinzer.
A
B
C
Copyright © 2009 American Dental Association. All rights reserved. Reprinted by permission.

5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 6/8
1164 JADA, Vol. 140 http://jada.ada.org September 2009
PERSPECTIVES C L I N I C A L D I L E M M A S
If removal of all four incisors
is required and good periodontal
support exists, the clinician has
two equally acceptable options
for implant prostheses. One is
placement of implants in both
lateral incisor locations, with
the replacement of both central
incisors as ovate pontics. The
second is placement of the
implants in the central incisor
locations with a mediating space
of at least 3.0 mm; the lateral
incisor ovate pontics then can be
cantilevered from the central
incisors. Both options produce
acceptable esthetic, structural
and functional results.
Tooth removal and re-
placement in the presence of
periodontal disease. Consid-
ering the same manifestationsdiscussed previously, but adding
the presence of pre-existing bone
loss resulting from periodontal
disease, provides new chal-
lenges. Foremost among these is
the loss of predictability of the
papillary height after tooth
removal in the areas of peri-
odontal disease. When peri-
odontal disease is present, the
bone does not always respond as
it would if it were healthy,
which often leads to greaterresorption of bone and a greater
degree of papillary recession.
Therefore, to avoid an open gin-
gival embrasure, the clinician
must position contacts more api-
cally than is esthetically desir-
able. The clinician is left with
the challenge of using implant
restorations that will be accept-
able functionally and struc-
turally but less so esthetically,
or of forgoing the use of implants and using soft-tissue
grafting with fixed partial den-
tures in areas in which grafting
and pontics can produce signifi-
cantly more soft tissue over the
interproximal bone. The differ-
ence between tissue heights of
3.5 and 6.5 mm above bone can
be the difference between an
esthetic success and an esthetic
failure. The final decision about
which modality is best suited for
success will be based on theesthetic requirements created by
the lip line and mobility and the
condition of the remaining teeth.
If the adjacent teeth are unre-
stored, it may be preferable to
conserve tooth structure by
using implants rather than
preparing unrestored teeth.
Some esthetic compromise may
Figure 4. A. Adjacent implants placed in central and lateral positions. Note excellent inter-proximal bone but minimal interimplant distance. B. At insertion, no black triangle waspresent; however, six months after insertion, papilla has receded as bone is lost. C. Twelvemonths after implant placement, soft tissue has migrated apically as bone between theimplants has continued to resorb.
A
B
C
A B
C D
Figure 5. A. A patient with three ankylosed teeth but with excellent bone levels.B. Teeth nos. 8, 9 and 10 were removed and immediate implants placed at no. 8 andno. 10. C. Connective-tissue grafting in pontic area no. 9 and over implant no. 10. D. Finalrestoration after grafting: a three-unit zirconia prosthesis consisting of an implant abutment
at no. 8, a pontic at no. 9 and an abutment at no. 10.
Copyright © 2009 American Dental Association. All rights reserved. Reprinted by permission.

5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 7/8
JADA, Vol. 140 http://jada.ada.org September 2009 1165
PERSPECTIVES C L I N I C A L D I L E M M A S
be in the patient’s best interest
and should not be dismissed
without serious consideration
and discussion.
Slow orthodontic eruption
before extraction is anotheroption to consider when it is
necessary to remove multiple
adjacent teeth with periodontal
disease.15 Although eruption of a
single tooth that is to be ex -
tracted does not alter the final
papillary heights, because those
heights are dictated by the bone
on the adjacent teeth, the erup-
tion of multiple teeth before
extraction may move interprox-
imal bone coronally. This move-
ment of the bone is not highlypredictable, however, so the
clinician must inform the
patient that a perfect esthetic
result is unlikely and that short
papillae, long contacts and more
rectangular final restorations
could be expected (Figure 6).
Tooth replacement in the
presence of a flattened ridge.
The final two manifestations,
both involving a flattened ridge,
are the most difficult to manageesthetically. When multiple
teeth are removed, the bony
ridge tends to flatten rapidly
unless the clinician does some-
thing to alter the process. In
cases in which the teeth have
been missing for a significant
time, the interproximal osseous
crest will be gone completely.
Recreating vertical bone height
in situations in which multiple
teeth have been removed is diffi-
cult and unpredictable. For thisreason, when the teeth are
missing before any treatment,
use of adjacent implants results
in inadequate papillary height.
Using a connective graft and
pontics, however, can create and
maintain significantly more soft
tissue above the interproximal
bone than is possible with adja-
cent implants. Therefore, the
clinician must inform the
patient that the best esthetic
result may involve pontics
rather than implants in some
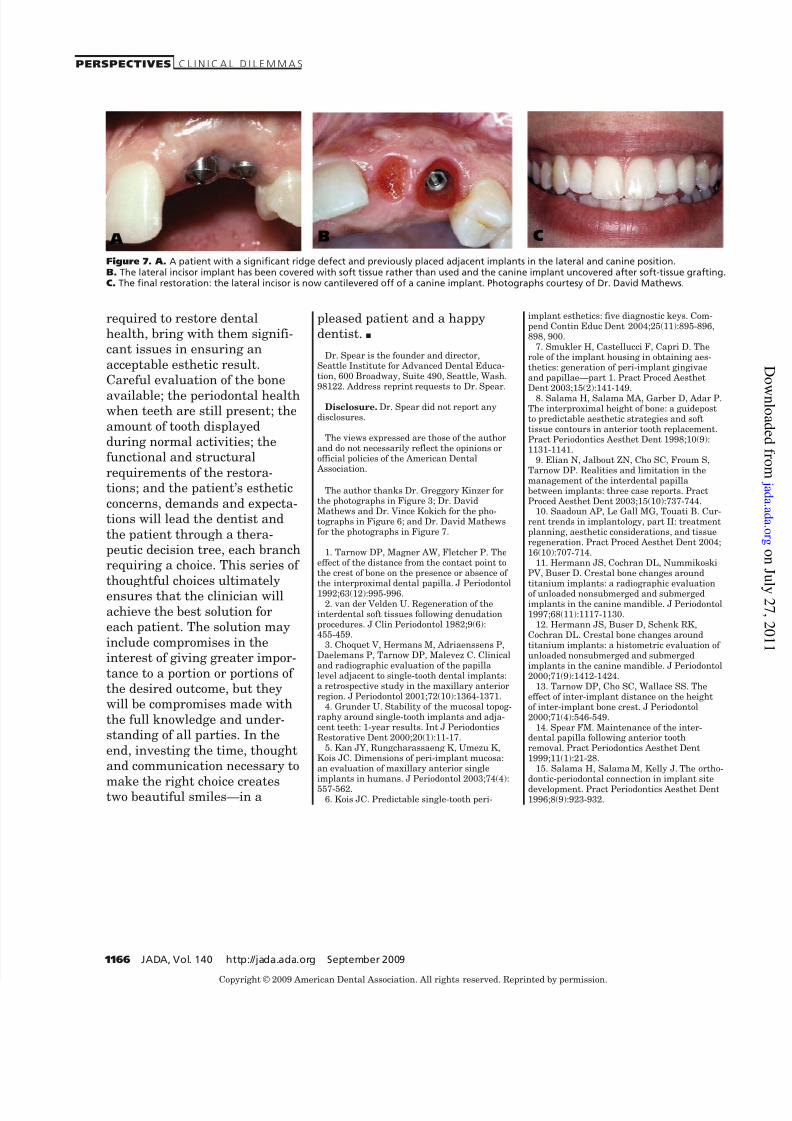
sites. Selection of the most
appropriate sites for using
connective-tissue grafting and a
pontic next to an implant will
minimize esthetic compromises
and can achieve an excellent
esthetic result (Figure 7).
CONCLUSION
Patients who have multiple
missing anterior teeth, or
patients for whom removal of
multiple anterior teeth is
Figure 6. A. A patient requiring extraction of teeth nos. 8 and 9 because of extensivebone loss. Note excellent papillary levels. B. Significant bone loss has occurred, creating anesthetic dilemma regarding soft-tissue position. C. Orthodontic eruption was used toattempt to move the bone coronally. D. After the eruption, there has been minimal if anyimprovement. E. Implant placement. F. Final restorations. Note the minimal gingival scallopcaused by an apically placed papilla and a long contact. This esthetic compromise wasexpected owing to the patient’s significant interproximal bone loss before implant place-ment. Photographs courtesy of Dr. David Mathews and Dr. Vince Kokich.
A
B
C
D
E F
Copyright © 2009 American Dental Association. All rights reserved. Reprinted by permission.
5/8/2018 J Am Dent Assoc 2009 Spear 1160 6 - slidepdf.com
http://slidepdf.com/reader/full/j-am-dent-assoc-2009-spear-1160-6 8/8
1166 JADA, Vol. 140 http://jada.ada.org September 2009
PERSPECTIVES C L I N I C A L D I L E M M A S
required to restore dental
health, bring with them signifi-
cant issues in ensuring an
acceptable esthetic result.
Careful evaluation of the bone
available; the periodontal healthwhen teeth are still present; the
amount of tooth displayed
during normal activities; the
functional and structural
requirements of the restora-
tions; and the patient’s esthetic
concerns, demands and expecta-
tions will lead the dentist and
the patient through a thera-
peutic decision tree, each branch
requiring a choice. This series of
thoughtful choices ultimatelyensures that the clinician will
achieve the best solution for
each patient. The solution may
include compromises in the
interest of giving greater impor-
tance to a portion or portions of
the desired outcome, but they
will be compromises made with
the full knowledge and under-
standing of all parties. In the
end, investing the time, thought
and communication necessary to
make the right choice createstwo beautiful smiles—in a
pleased patient and a happy
dentist. ■
Dr. Spear is the founder and director,Seattle Institute for Advanced Dental Educa-tion, 600 Broadway, Suite 490, Seattle, Wash.98122. Address reprint requests to Dr. Spear.
Disclosure. Dr. Spear did not report anydisclosures.
The views expressed are those of the authorand do not necessarily reflect the opinions orofficial policies of the American Dental Association.
The author thanks Dr. Greggory Kinzer forthe photographs in Figure 3; Dr. DavidMathews and Dr. Vince Kokich for the pho-tographs in Figure 6; and Dr. David Mathewsfor the photographs in Figure 7.
1. Tarnow DP, Magner AW, Fletcher P. Theeffect of the distance from the contact point tothe crest of bone on the presence or absence of
the interproximal dental papilla. J Periodontol1992;63(12):995-996.2. van der Velden U. Regeneration of the
interdental soft tissues following denudationprocedures. J Clin Periodontol 1982;9(6):455-459.
3. Choquet V, Hermans M, Adriaenssens P,Daelemans P, Tarnow DP, Malevez C. Clinicaland radiographic evaluation of the papillalevel adjacent to single-tooth dental implants:a retrospective study in the maxillary anteriorregion. J Periodontol 2001;72(10):1364-1371.
4. Grunder U. Stability of the mucosal topog-raphy around single-tooth implants and adja-cent teeth: 1-year results. Int J PeriodonticsRestorative Dent 2000;20(1):11-17.
5. Kan JY, Rungcharassaeng K, Umezu K,Kois JC. Dimensions of peri-implant mucosa:an evaluation of maxillary anterior single
implants in humans. J Periodontol 2003;74(4):557-562.6. Kois JC. Predictable single-tooth peri-
implant esthetics: five diagnostic keys. Com-pend Contin Educ Dent 2004;25(11):895-896,898, 900.
7. Smukler H, Castellucci F, Capri D. Therole of the implant housing in obtaining aes-thetics: generation of peri-implant gingivaeand papillae—part 1. Pract Proced Aesthet
Dent 2003;15(2):141-149.8. Salama H, Salama MA, Garber D, Adar P.The interproximal height of bone: a guidepostto predictable aesthetic strategies and softtissue contours in anterior tooth replacement.Pract Periodontics Aesthet Dent 1998;10(9):1131-1141.
9. Elian N, Jalbout ZN, Cho SC, Froum S,Tarnow DP. Realities and limitation in themanagement of the interdental papillabetween implants: three case reports. PractProced Aesthet Dent 2003;15(10):737-744.
10. Saadoun AP, Le Gall MG, Touati B. Cur-rent trends in implantology, part II: treatmentplanning, aesthetic considerations, and tissueregeneration. Pract Proced Aesthet Dent 2004;16(10):707-714.
11. Hermann JS, Cochran DL, NummikoskiPV, Buser D. Crestal bone changes around
titanium implants: a radiographic evaluationof unloaded nonsubmerged and submergedimplants in the canine mandible. J Periodontol1997;68(11):1117-1130.
12. Hermann JS, Buser D, Schenk RK,Cochran DL. Crestal bone changes aroundtitanium implants: a histometric evaluation of unloaded nonsubmerged and submergedimplants in the canine mandible. J Periodontol2000;71(9):1412-1424.
13. Tarnow DP, Cho SC, Wallace SS. Theeffect of inter-implant distance on the heightof inter-implant bone crest. J Periodontol2000;71(4):546-549.
14. Spear FM. Maintenance of the inter-dental papilla following anterior toothremoval. Pract Periodontics Aesthet Dent1999;11(1):21-28.
15. Salama H, Salama M, Kelly J. The ortho-
dontic-periodontal connection in implant sitedevelopment. Pract Periodontics Aesthet Dent1996;8(9):923-932.
Figure 7. A. A patient with a significant ridge defect and previously placed adjacent implants in the lateral and canine position.B. The lateral incisor implant has been covered with soft tissue rather than used and the canine implant uncovered after soft-tissue grafting.C. The final restoration: the lateral incisor is now cantilevered off of a canine implant. Photographs courtesy of Dr. David Mathews.
A B C
Copyright © 2009 American Dental Association. All rights reserved. Reprinted by permission.