it - cardiac arrythmia (bag 1) - alg.pptx
TRANSCRIPT

CARDIAC ARRYTHMIA
Ali Ghanie
Divisi Kardiologi Bagian Penyakit Dalam FK Unsri
DEFINISI
• Aritmia merupakan gangguan irama jantung, akibat gangguan sekuen dari aktifitas listrik.
• Bukan sinonim dari aktifitas jantung yang tidak teratur, karena bisa sinus, ectopic, irama bisa reguler atau ireguler, dengan denyut jantung normal, lambat atau cepat

Mekanisme
• Gangguan pembentukan impul (automatisasi abnormal)
• Gangguan konduksi impul• Kombinasi keduanya
Klasifikasi aritmia
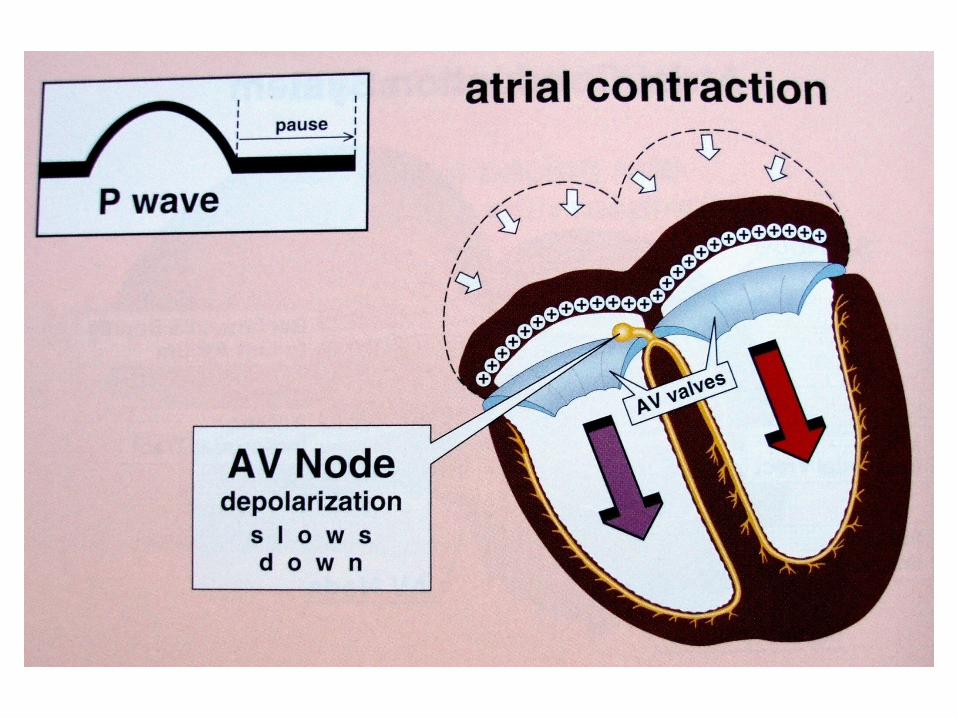
• Supraventrikuler, terjadi pada bagian atas jantung yaitu atrium, sinus, AV-node
• Ventrikuler, terjadi pada bagian bawah jantung yaitu ventrikel
• Kedua aritmia tersebut selanjutnya dibedakan lagi menurut frekwensi denyut jantung, yaitu pelan, cepat sekali, & cepat sekali tak terkoordinasi.
• Bradikadia bila denyut jantung < 60 x/m

Klasifikasi ….sambungan
• Bradikardi bila denyut jantung < 60 x/m• Takikardia bila denyut jantung > 100 x/m• Flutter, denyut cepat sekali, regular• Fibrilasi, denyut jantung cepat sekali dan
aktifitas kontraksi tidak terkoordinasi

Aritmia Supraventrikuler
• Impuls pada bagian atas cabang bundel his, atria atau AV-node
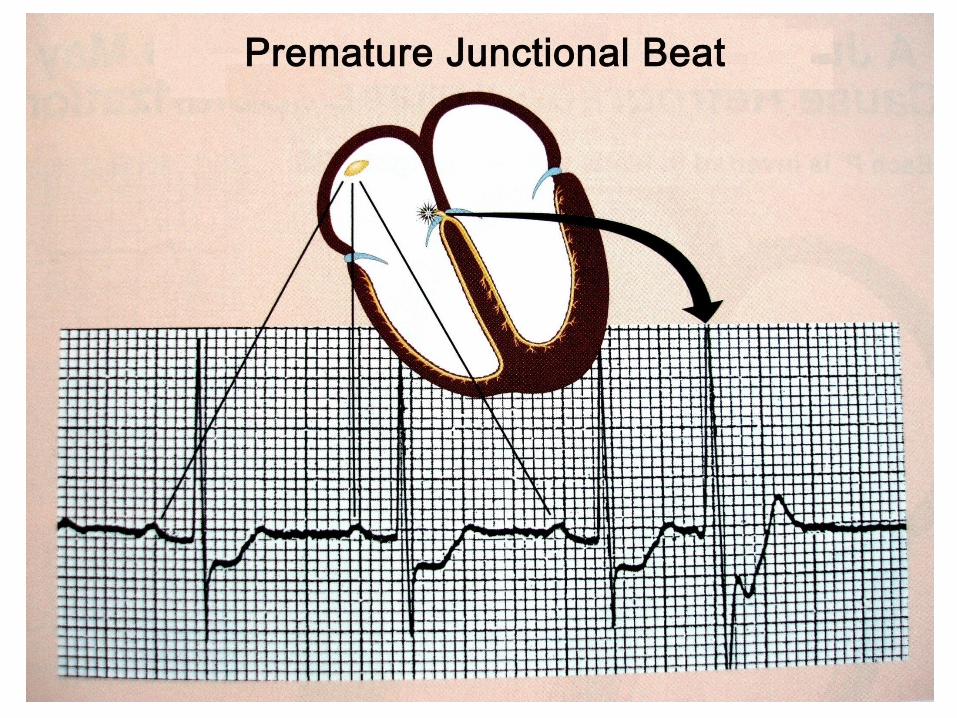
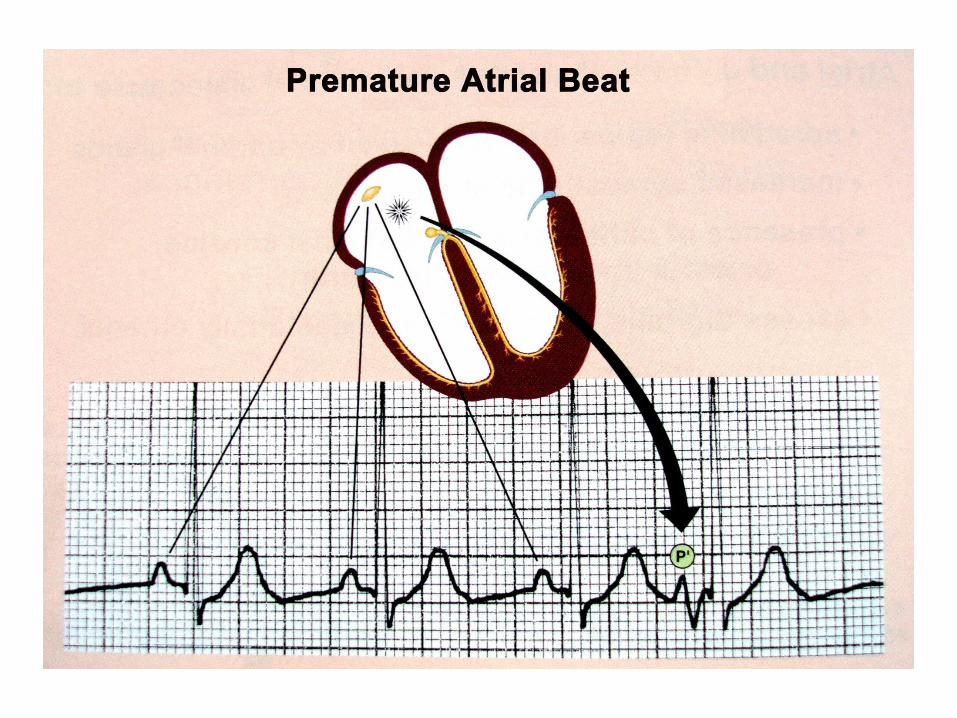
• Sinus bradikardia• Extrasistole, komplek prematur• Takikardia, 3 atau lebih impul dari pace maker
yg sama • Fluter, cepat dan reguler (200-400x/m)• Fibrilasi, cepat ireguler (300-600x/m)

sambungan
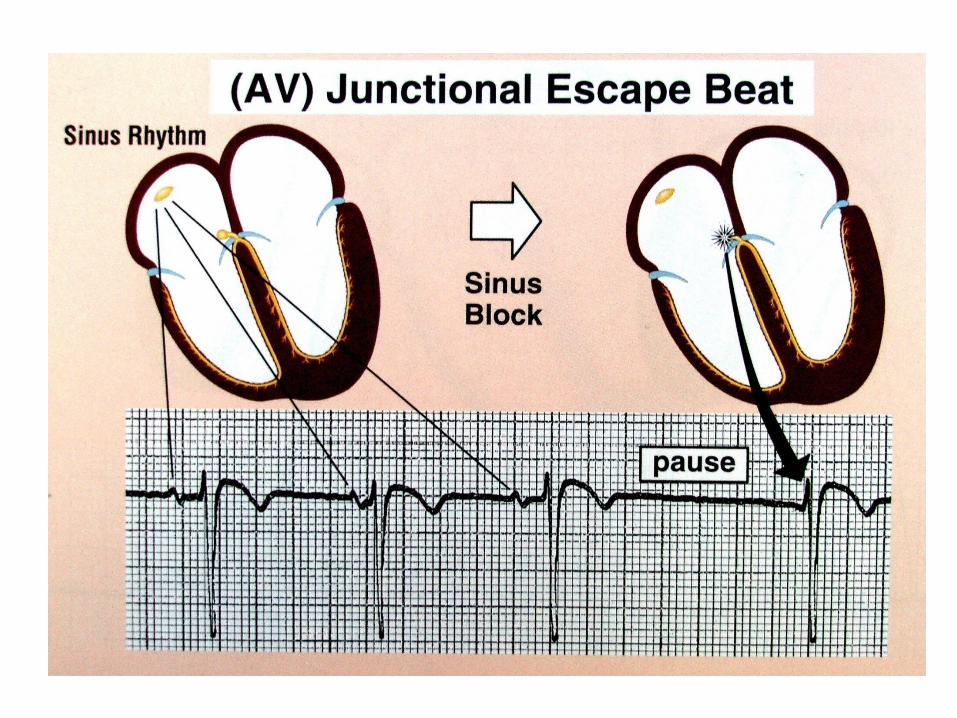
• Escape, 1 atau 2 impul berturut2, dari pace maker atau berbagai pace maker, karena keterlambatan impul dasar.
• Irama escape, bila escape 3 atau lebih berturut2.
Aritmia Ventrikuler
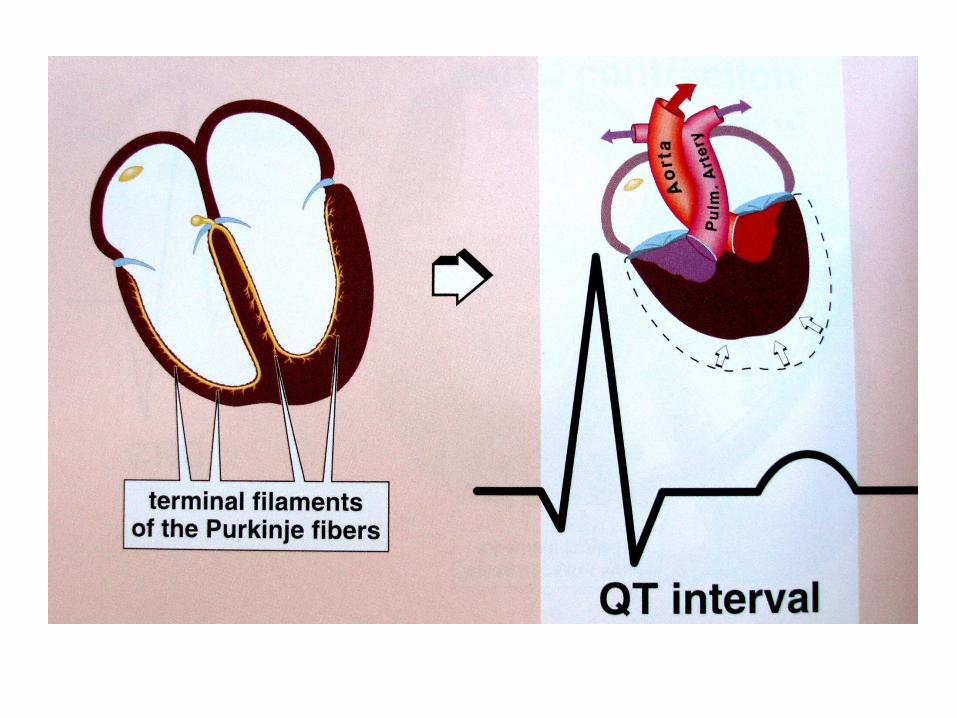
• Impul berasal dari distal bundel his, cabang bundel, atau serabut Purkinye atau miokardium
• Jenis sama dengan aritmia supra ventrikuler, tergantung kecepatan dan irama.


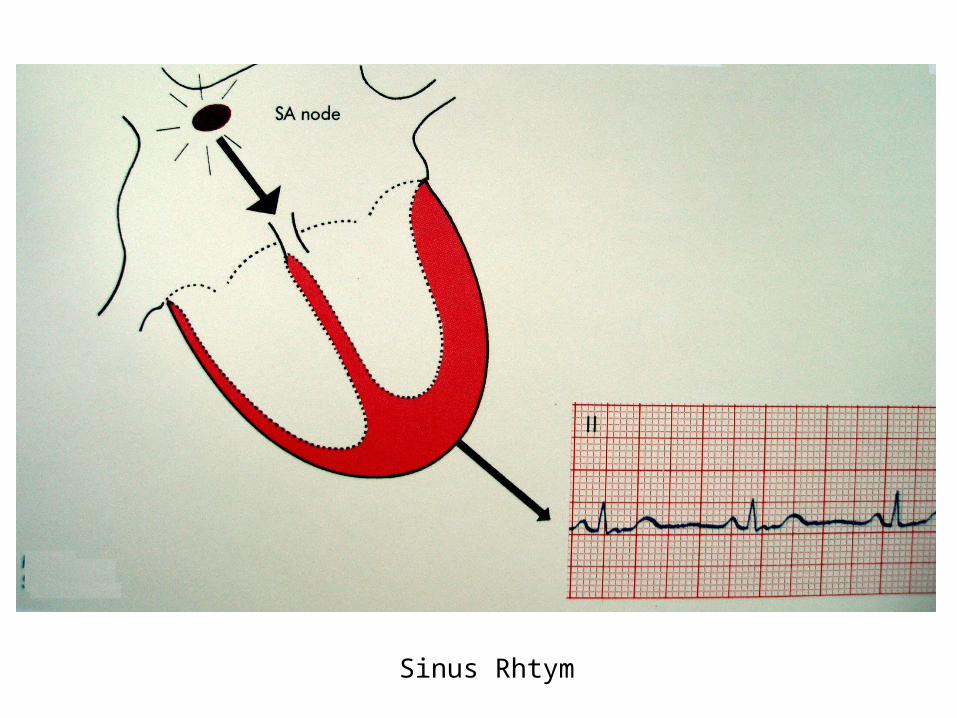
Sinus Rhtym





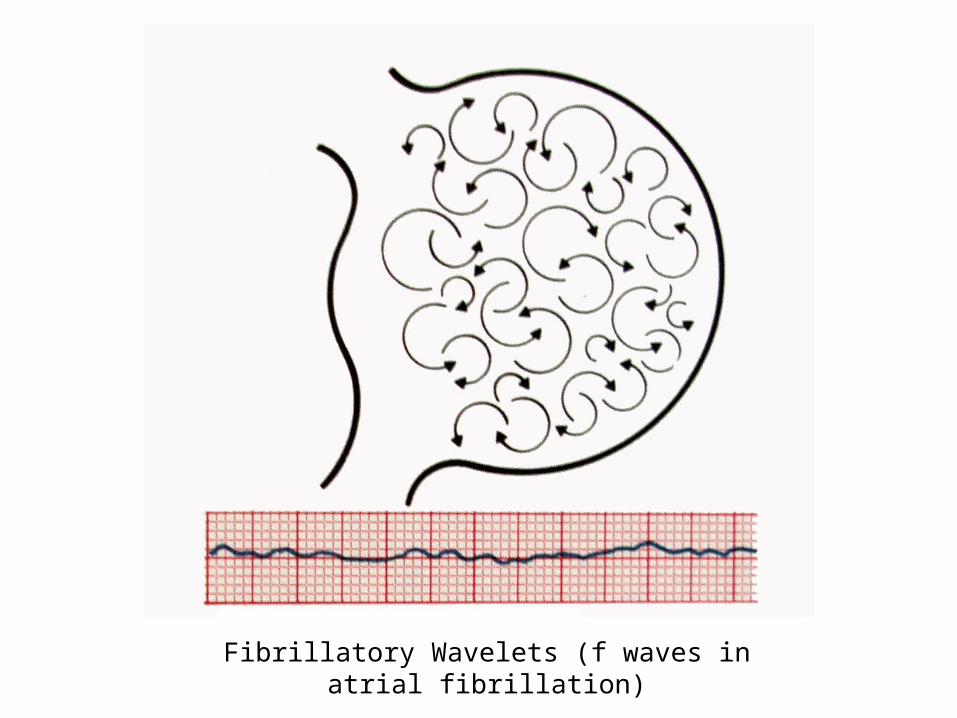
Fibrillatory Wavelets (f waves in atrial fibrillation)

Ventricular tachycardia with AV dissociation. The ventricular origin of the tachycardia is suggested by the wide, monophasic QRS complexes and confirmed by the presence of AV the presence of AV dissociation.
A. Sinus P waves at an unchanged rate are visible just before some of the QRS complexes as a deflection in the ST segment of just after the T wave.
B. The P waves are not clearly visible in the surface lead (V1) but distinctly recorded in the oesophageal lead (E10).

Ventricular tachycardia with AV dissociated and ventricular capture. (Fig.6.28)

A. WPW-syndrome B. Concealed WPW-syndrome C. Short PR syndrome
Anterograde unidirectional block
Pre-exacitation syndrome. AV conduction in sinus rhytm (above) and in re-entry tachycardia (below)
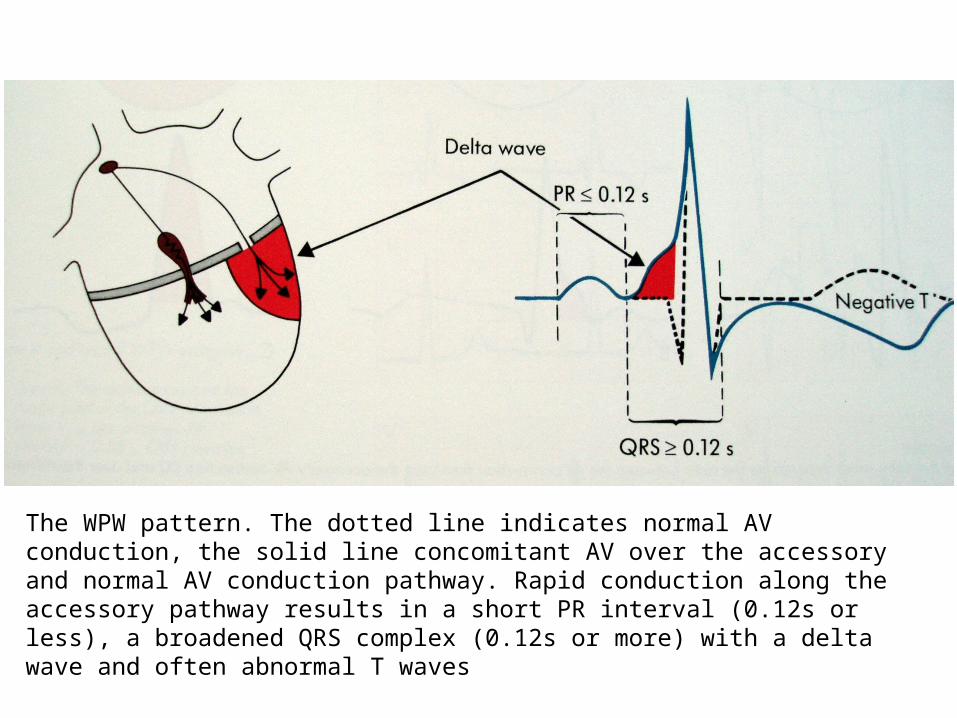
The WPW pattern. The dotted line indicates normal AV conduction, the solid line concomitant AV over the accessory and normal AV conduction pathway. Rapid conduction along the accessory pathway results in a short PR interval (0.12s or less), a broadened QRS complex (0.12s or more) with a delta wave and often abnormal T waves

The WPW pattern. Te widht of the delta wave deponds on the ratio between the AV conduction time over the accessory AV connection (X) and over the AV node and bundle of His (Y)
A. Small delta wave as X is

The WPW syndrome
A. In tachycardia narrow QRS complexs B. On return of sinus rhythm reappearance of the delta wave and a corresponding widening of the QRS complex
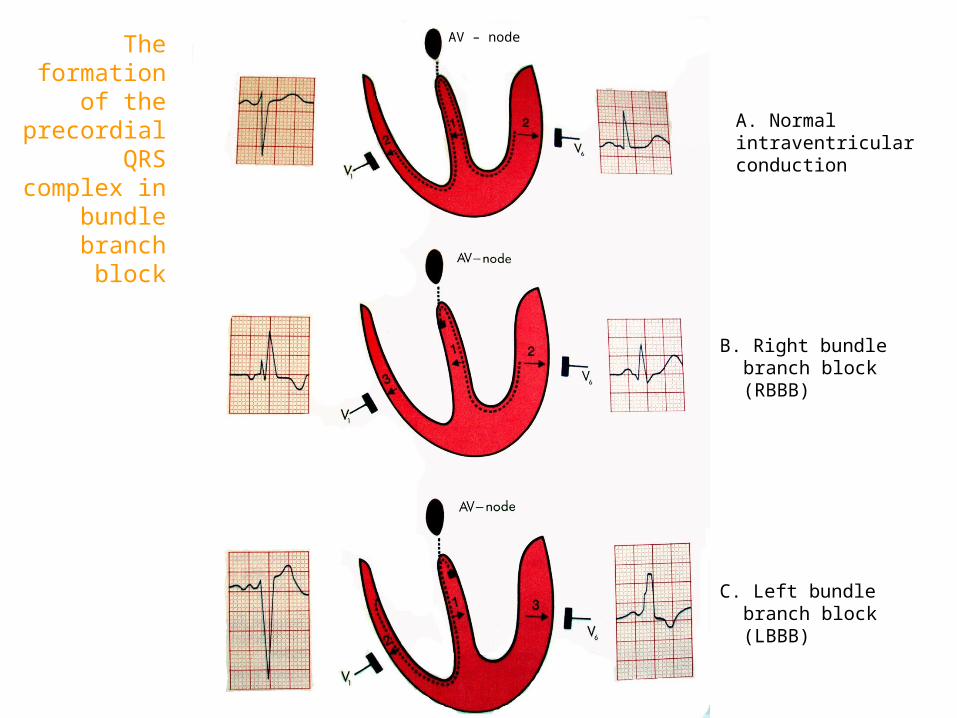
AV – node
C. Left bundle branch block (LBBB)
B. Right bundle branch block (RBBB)
A. Normal intraventricular conduction
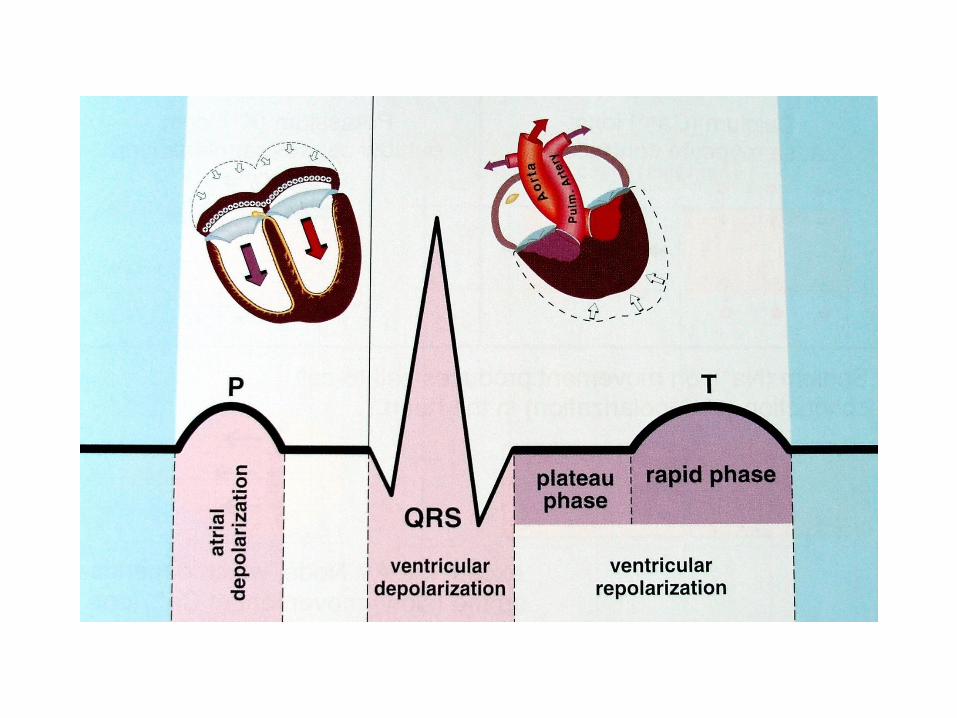
The formation of the
precordial QRS complex
in bundle branch block