arrythmia . anu k george
TRANSCRIPT

welcome

Case
• 85 y.o. F complaining of feeling “off” and
being “just so tired”
• SOB
• Vaguely recalls feeling a bit “unsteady” on a
couple of occasions
• Hx: osteoporosis, hypothyroidism and
depression
• Meds: Calcium, Vit D, Celexa, Synthroid

Case cont’d
• Vitals:
– HR 45, irregular
– RR 16
– BP 108/75
– Afebrile

:

Arrythmias
heart block
Presented by
Anu k george
Msc (N) II Year

TERMINOLOGIES
Common terms

REVIEW OF CONDUCTION SYSTEM OF HEART

ELECTROCARDIOGRAM
• The electrocardiogram (ECG) is a
representation of the electrical events of the
cardiac cycle.
• Each event has a distinctive waveform, the
study of which can lead to greater insight into
a patient’s cardiac pathophysiology

(300 / 6) = 50 bpm
What is the heart rate?

4 Mechanisms of Arrhythmia
• reentry (most common)
• automaticity
• parasystole
• triggered activity

Fast Conduction Path
Slow Recovery
Slow Conduction Path
Fast Recovery
Premature Beat Impulse
Cardiac
Conduction
Tissue
1. An arrhythmia is triggered by a premature beat
2. The fast conducting pathway is blocked because of its
long refractory period so the beat can only go down the
slow conducting pathway
Repolarizing Tissue
(long refractory period)
Reentry Mechanism
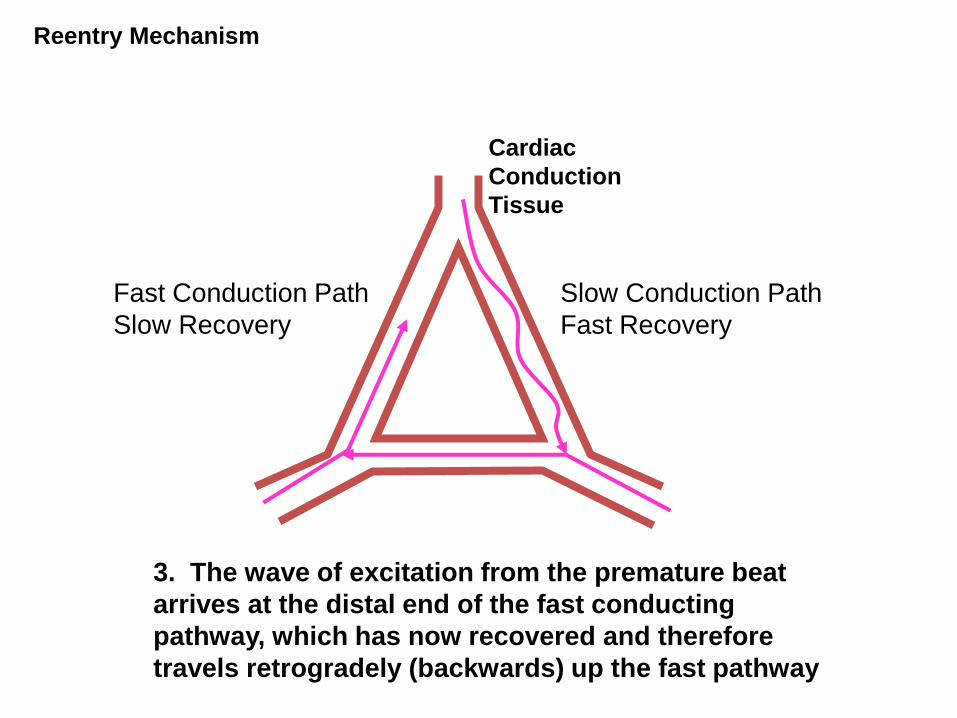
3. The wave of excitation from the premature beat
arrives at the distal end of the fast conducting
pathway, which has now recovered and therefore
travels retrogradely (backwards) up the fast pathway
Fast Conduction Path
Slow Recovery
Slow Conduction Path
Fast Recovery
Cardiac
Conduction
Tissue
Reentry Mechanism

4. On arriving at the top of the fast pathway it finds the
slow pathway has recovered and therefore the wave of
excitation ‘re-enters’ the pathway and continues in a
‘circular’ movement. This creates the re-entry circuit
Fast Conduction Path
Slow Recovery
Slow Conduction Path
Fast Recovery
Cardiac
Conduction
Tissue
Reentry Mechanism

Atrial Reentry
• atrial tachycardia
• atrial fibrillation
• atrial flutter
Atrio-Ventricular
Reentry
• WPW
• SVT
Ventricular Re-entry
• ventricular tachycardia
AV Nodal Reentry
•SVT
Reentry Circuits
SA Node

Automaticity
• Heart cells other than those of the SA node depolarize faster than SA node cells, and take control as the cardiac pacemaker.
• Factors that enhance automaticity include:
SANS, PANS, CO2, O2, H+, stretch, hypokalemia and hypocalcaemia.
Examples: Ectopic atrial tachycardia or multifocal tachycardia in patients with chronic lung disease OR ventricular ectopy after MI

Parasystole…
• is a benign type of automaticity problem that affects only a small region of atrial or ventricular cells.
• 3% of PVCs

Triggered activity…
• is like a domino effect where the arrhythmia is due to the preceding beat.
• Delayed after-depolarizations arise during the resting phase of the last beat and may be the cause of digitalis-induced arrhythmias.
• Early after-depolarizations arise during the plateau phase or the repolarization phase of the last beat and may be the cause of torsades de pointes (ex. Quinidine induced)
Definition
• The term "arrhythmia" refers to any change from the
normal sequence of electrical impulses. The electrical
impulses may happen too fast, too slowly, or erratically –
causing the heart to beat too fast, too slowly, or erratically.
When the heart doesn't beat properly, it can't pump blood
effectively
-American Heart Association

ETIOLOGY
• Dysrhythmias occur as the result of various
abnormalities and disease rate.

Cardiac conditions
• Cardiomyopathy
• Conduction defects
• Heart failure
• Myocardial cell degeneration & MI
• Valve disease

Non cardiac condition
• Acid base imbalance
• Alcohol ,Caffeine & tobacco
• Connective tissue disorder
• Drugs & Toxicity
• Electric shock, hypoxia & shock
• Emotional crisis
• Herbal supplements
• Near drowning and poisoning
• Metabolic condition

TYPES OF DYSRHYTHMIAS

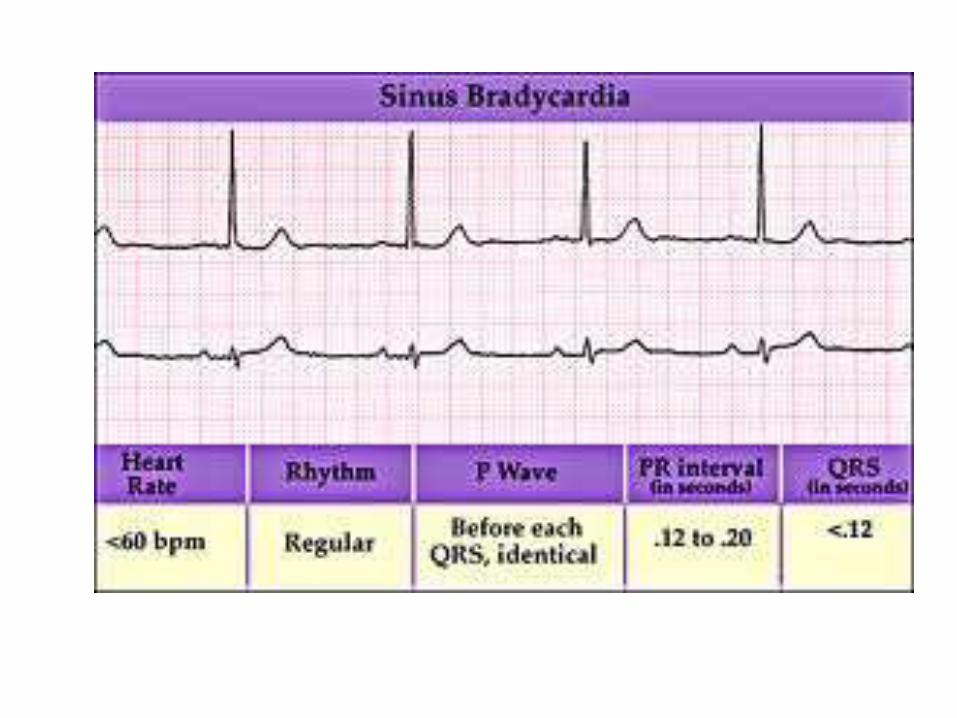
SINUS BRADYCARDIA
• The conduction pathway is the same as that in sinus rhythm but the SA node fires at a rate less than 60beats/min
Absolute bradycardia
Relative bradycardia

Cont…Etiology:
Increased vagal tone
Hypothermia
Increased intraocular pressure
Administration of parasympathomimetic drugs
& adverse drug effects
Acute MI
Disease condition – hypothyroidism, increased
ICP & obstructive jaundice

Cont..Clinical manifestation:
At rest, asymptomatic
Pale, cool skin, hypotension, weakness and angina.
Dizziness or syncope
Confusion and disorientation
Shortness of breath

Cont…
Clinical association- for aerobically trained athletes.
ECG characteristics:
Regular P waves by regular QRS complex

Cont..
Therapy:
Atropine IV o.5mg to I mg
Transcutaneous pacing
Dopamine- 5 to 20µg/kg/min
Epinephrine – 2 to 10µg/min
Isoproterenol- 2 to 10µg/min

SICK SINUS SYNDROME
• SSS also called sinus node dysfunction is a group of
abnormal heart rhythms causes by malfunction of
sinus node.
• Bradycardia-tachycardia syndrome

Cont…
Etiology:
Medication: digitalis, sympatholytic drugs
Sarcoidosis, amyloidosis
Cardiomyopathies
CAD

Cont…
Symptoms:
Dizziness
Palpitation
Chest pain
Angina
Shortness of breath
Fatigue & headache
Nausea and fainting

Cont…
ECG Characteristics:
Combination of sinoatrial and atrioventricular conduction disturbances.


Cont…
• Treatment- artificial pacemaker

SINUS TACHYCARDIA
• Sinus rate more than 100beats/min and is
normally due to increase in sympathetic
activity.
• Conduction pathway is same. Discharge rate
from the sinus node is increased.

Cont…Etiology:
Physical and psychological stressors: exercise,
fever,pain, hypotension, hpovolemia, anemia,
hypoglycemia, MI, HF, anxiety
Adrenergic stimulation
Drugs
Pheochromocytoma
Caffeine
Cont…Clinical manifestation:
Patients intolerance to increased heart rate
Dizziness
Dyspnea
Hypotension
Increased myocardial oxygen consumption

Cont…ECG characteristics:
Treatment: no specific treatment
Never counter shock
Rate: morethan 100 b/min
Rhythm : sinus PR interval:</= 0.20sec
QRS complex-normal

PREMATURE ATRIAL CONTRACTION
PAC is a contraction originating from an ectopic focus in
the atrium in a location other than the sinus node

Cont…
Etiology:
☺Hypoxia
☺Electrolyte imbalance
☺Hyperthyroidism
☺COPD
☺Heart disease- CAD
☺Valvular disorder

Cont…
PATHOPHYSIOLOGY:
• The ectopic signal originates in the LA or RA and
travels across the atria by an abnormal pathway
creating a distorted P wave.
• At the AV node it may stopped (non conducted PAC),
delayed (lengthened PR interval) or conducted
normally.

Cont…
ECG characteristic:

Cont…
Treatment:
Beta blockers

Guess!!!!!!

ATRIAL FLUTTER• It is characterized by large re-entry circuit within the
right atrium, usually encircling the tricuapid annulus
• “Impulses take a circular course around the atria,setting up the flutter waves”
Cont…
Etiology:
♥ Acute coronary syndrome
♥ Mitral and tricuspid valve disorders
♥ Hypoxia, HT, chromic lung disease
♥ Cardiomyopathy
♥ Pulmonary embolus & cor pulmonale
♥ Hyperthyroidism
♥ Drug induced

Cont…Clinical manifestation:
Can be asymptomatic
Palpitation
High ventricular rate- flutter can cause decrease cardiac output--- HF
ECG characteristics:
Classic- saw tooth pattern & no true P wave
Ventricular response- a function of AV node block or conduction of atrial impulses.


Cont…
Treatment:
Calcium channel blocker
Beta adrenergic
blockers
To control ventricular
rate

Cont…
• Electrical cardio version
• Radio frequency catheter ablation
• High risk of stroke-
– Anticoagulate for 3 weeks if more than 48 hours
occurrence – 4 weeks
– IV heparin
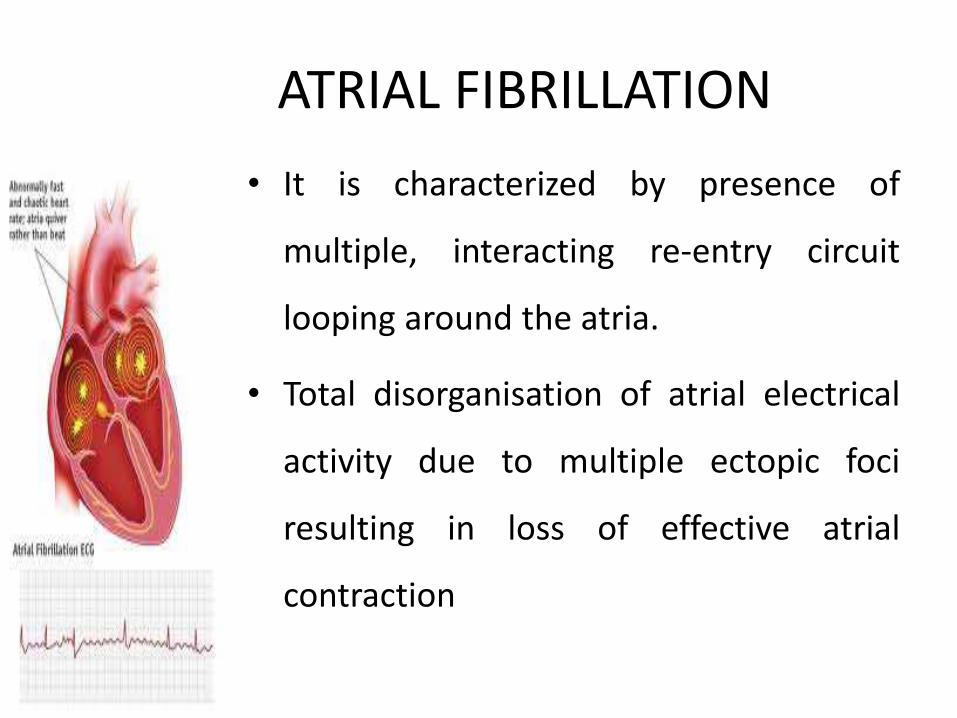
ATRIAL FIBRILLATION
• It is characterized by presence of
multiple, interacting re-entry circuit
looping around the atria.
• Total disorganisation of atrial electrical
activity due to multiple ectopic foci
resulting in loss of effective atrial
contraction

Cont…
Etiology:
Thyrotoxicosis, alcohol intoxication, caffeine use, electrolyte disturbance, stress and cardiac surgery
Atrial impulse faster than the SA node impulses, impulses take multiple , choatic, random pathways
through the atria

Cont…Clinical manifestation:
Atrial fibrillatory waves- AF with rapid ventricular
response
Thrombi form- 5 fold increase risk to get stroke
Decreased cardiac output.

Cont…ECG Characteristics:
“irregularly irregular rhythm- with variation in both interval & amplitude from R wave to R wave”
Rate- wide ranging ventricular response to atrial rate of 300-400 beats/min


Cont…Treatment:
♫ Calcium channel blockers
♫ Beta adrenergic blockers
♫ Antiarrythmic drugs
♫ Anti coagulation therapy
♫ Maze procedure:
• Cryoablation (use of cold)
• Heat (high intensity ultrasound)
Cont…
Rhythm control
• Immediate cardio version after administration of IV
heparin
• To restore sinus rhythm flecainide= 2mg/kg over
30min max dose 150mg
• INR to be maintained 2.0 to 3.0 for a minimum of 3
weeks

Cont…Rate control:
o Digoxin
o Beta blokers
o Rate limiting calcium antagonist
– Verapamil
– diltiazem
o Combination therapy:
• Digoxin + atenolol

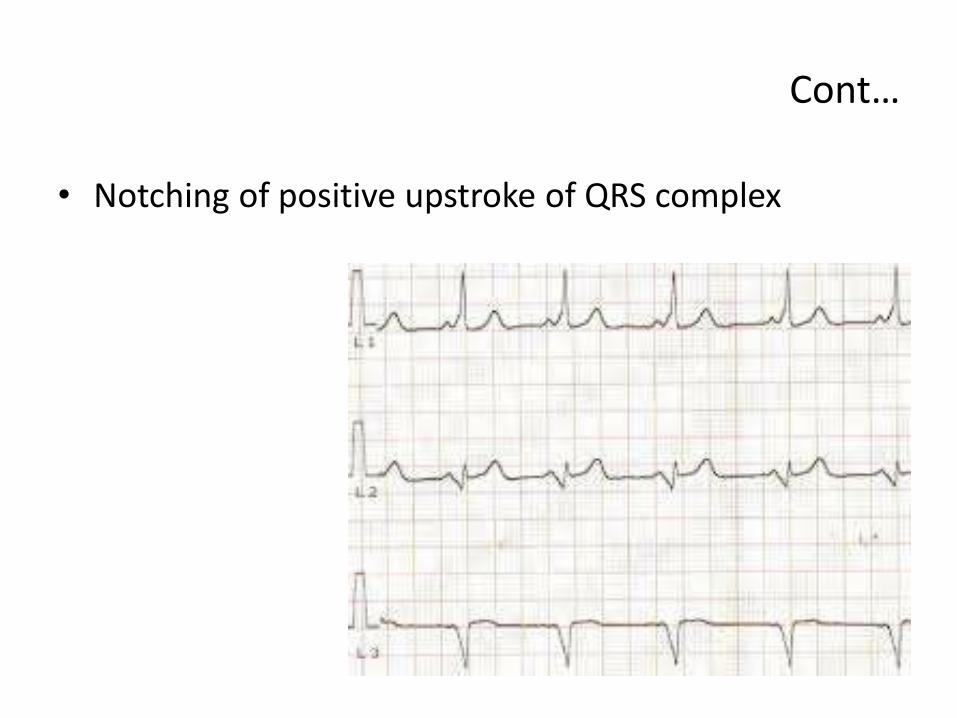
WOLFF PARKINSON WHITE SYNDROME
WPW is one of the severe disorder of the conduction
system. WPW is caused by the presence of an
abnormal electrical conduction pathway between
atria and ventricle
0.1% to 0.3%
PRKAG-2 gene/ congenital

Cont…
• Notching of positive upstroke of QRS complex

Rate: 60-100b/minRhythm: normal sinus except pre-excitation tachycardiaPR interval: shorter

Cont…
Clinical manifestation:
Asymptomatic
Sometimes signs of tachycardia
Treatment:
• Cardio verison
• Anti arrythmic drugs
• Digoxin
• Ca channel blockers and beta blockers

JUNCTIONAL TACHYCARDIA
• It originates in the area of the AV node, primarily
because the SA node has failed to fire or the signal
has been blocked.

Cont…
• Impulse from the AV node usually moves in a
retrograde (backward fashion) that produce an
abnormal P wave just occuring before or after QRS
complex

MULTIFOCAL ATRIAL TACHYCARDIA
• Area of automaticity (impulse formation)
originate irregularly and rapidly at different
points in the atria

Cont…
ECG Characteristic:
“wandering atrial pacemaker”
P waves- 3 or more P wave that differ in polarity(up/down) shape and size since the atrial impulse isgenerated from multiple foci


Cont…
Clinical manifestation:
Signs of less ejection fraction and tachycardia.
Treatment:
Beta blocker
Calcium channel blockers
Amiodarone
No cardio version

PAROXYSMAL SUPRAVENTRICULAR TACHYCARDIA
Ectopic focus anywhere above the bifuraction of
the bundle of his.
Etiology:
Over exersion
Emotional stress
Deep inspiration
RHD, CAD, COPD & CHF

Cont…• PATHOPHYSIOLOGY:
Impulse arise and recycle repeatedly in the AV nodebecause of areas of unidirectional block in thepurkinjie fibers
Reexcitation of the atria when there is a one wayblock
PSVT occurs because of a reentrant phenomenon

Cont…Clinical manifestation:
Prolonged episode and HR greater than 180beats/min
Decreased CO- Hypotension, dyspnea & angina
Anxious and uncomfortable
ECG Feature:

Cont…
Treatment:
Vagal stimulation
IV adenosine
IV Verapamil- 5-10mg
Beta blockers
Cardio version

PREMATURE VENTRICULAR CONTRACTION
Originating ectopic focus in the ventricles.
Premature occurrence of a QRS complex which is wide and distorted in shape.
Multifocal PVC
UnifocalPVC


VENTRICULAR FIBRILLATION
• Ventricle consist of areas of normal myocardium
alternating with areas of ischemic, injured or
infracted myocardium, leading to chaotic pattern of
ventricular depolarization

Cont…
Etiology:
♯ Acute coronary syndrome
♯ Stable to unstable VT
♯ PVC’S with R on T phenomenon
♯ Multiple drug
♯ Electrolyte disturbance
♯ Hypoxia, metabolic acidosis

Cont…
• Quickering ventricle no effective contraction

Cont…
Clinical manifestation:
Pulse disappears with onset of VF
Collapse, unconsiousness
Agonal breath
Onset of reversible death

Cont…
TREATMENT:
• Defibrillation
• Oxygen, CPR, INTUBATION
• Epinephrine
• Vasopressin
• Antiarrythmic

VENTRICULAR TACHYCARDIA
VT Monomorphic
VT polymorphic
Torsades de pointes

MONOMORPHIC VT
• Impulse conduction is slowed around area ofventricular injury, infarct or ischemia
• Ectopic impulses (irritable foci)
• Area of injury can cause the impulse to take acircular course, leading to the re-entryphenomenon and rapid repetitivedepolarization

Cont…
Clinical manifestation:
Asymptomatic
Symptoms of decreased cardiac output
ECG CRITERIA:
Φ 3 or more consecutive PVCs: VT
Φ < 30 sec- non sustained VT
Φ > 30 sec- sustained VT

Wide QRS complex

POLYMORPHIC VT
• Impulse conduction is slowed around multiple areas
of ventricular injury, infarcts or ischemia
• Irritable foci occur in multiple area of the ventricles
• Asymptomatic

TORSADES DE POINTES
• Twisting of the points
• QT interval is abnormally long
• Lead to increase in the relative refractory period
• Increase probability that an irritable focus (PVC) will occur on the T-wave

PULSELESS ELECTRICAL ACTIVITY
• PEA a situation in which electrical activity can be
observed on the ECG, but there is no mechanical
activity of the ventricles and the patient has no
pulse.
• Causes: 5H & 5T

Cont…
• Cardiac conduction impulses occur in organized
pattern , but this fails to produce myocardial
contraction (electromechanical dissociation) or
insufficient filling during diastole or ineffective
contractions

Cont…
Clinical manifestation:
Collapse, unconscious
Agonal respiration or apnea
No pulse

ASYSTOLE
• Total absence of ventricular electrical activity,
• Occasional P wave can be seen

DEFINITION :
This is the inhibition or failure of the
electrical impulses generated in the SA node to
be conducted through the conduction system
to the ventricles . This can occur because of an
abnormality of conduction velocity or complete
refractoriness in the conduction system .
HEART BLOCK

TYPES

AV NODAL BLOCKS (HEART BLOCKS)
Disturbances of the conduction through the heart, occurring at the AV Node
AV Node – damaged/diseased – delay or total block of impulses at the AV Node
This conduction defect can be seen on the ECG

AV Node• AV nodal conduction time is represented on
the ECG as the PR segment.
• But - we always measure the PR interval.

FIRST DEGREE HEART BLOCK (1º)
DEFINITION
It is a type of heart block in which every impulse is
conducted to the ventricles but the duration of AV
conduction is prolonged. After the impulse moves
through the AV node, it is usually conducted normally
through the ventricles.

CAUSES
Myocardial infarction
Chronic ischemic heart disease
Rheumatic fever
Hyperthyroidism
Vagal stimulation
Drugs as digitalis, - adrenergic blockers, verapamil

AV nodal dysfunction accounts for the
majority of cases. First-degree AV block
caused by conduction delay in the His-Purkinje
system often is associated with bundle-branch
block.
PATHOPHYSIOLOGY
ECG CHARACTERISTICS
• SA Node – normal
• Normal P wave
• AV Node conducts more slowly than normal
• Prolonged PR Interval
• Rest of conduction is normal
• Normal QRS

Cont...
Type
of
block
Rate
and
Rhyth
m
P wave PR
Interv
al
QRS
complex
P:QRS
Ratio
First
Degree
Heart
Block
Normal
and
regular
Normal >0.20
sec
Normal 1:1

FIRST DEGREE HEART BLOCK (1º)
PR Interval > 0.2 seconds (5 small sq)
• Note – the PR Interval is constant


CLINICAL SIGNIFICANCE
• Precursor of higher AV block
TREATMENT
• None, monitoring of the rhythm if changes
• Note – this can progress to 2º or 3º heart block

There is no treatment for first degree heart block .
Temporary pacing .
MANAGEMENT

SECOND DEGREE HEART BLOCK (2º)
DEFINITION
It occurs when one atrial impulse at a time
fails to be conducted to the ventricles.
TYPES
• Mobitz Type I (Wenkebach)
• Mobitz Type II
• 2 : 1
SECOND DEGREE HEART BLOCK (2º) MOBITZ TYPE I (WENKEBACH)
DEFINITION
It is a progressive increase in conduction times
of consecutive atrial impulses into the
ventricles until one impulse fails to conduct or
is dropped

CAUSES
Chronic ischemic heart disease
Drugs as digoxin, - adrenergic blockers

ECG CHARACTERISTICS
PR Interval prolongs with each beat until a
dropped beat is seen
The PR Interval is NOT constant
After each dropped beat, the PR interval is
normal and the cycle starts again
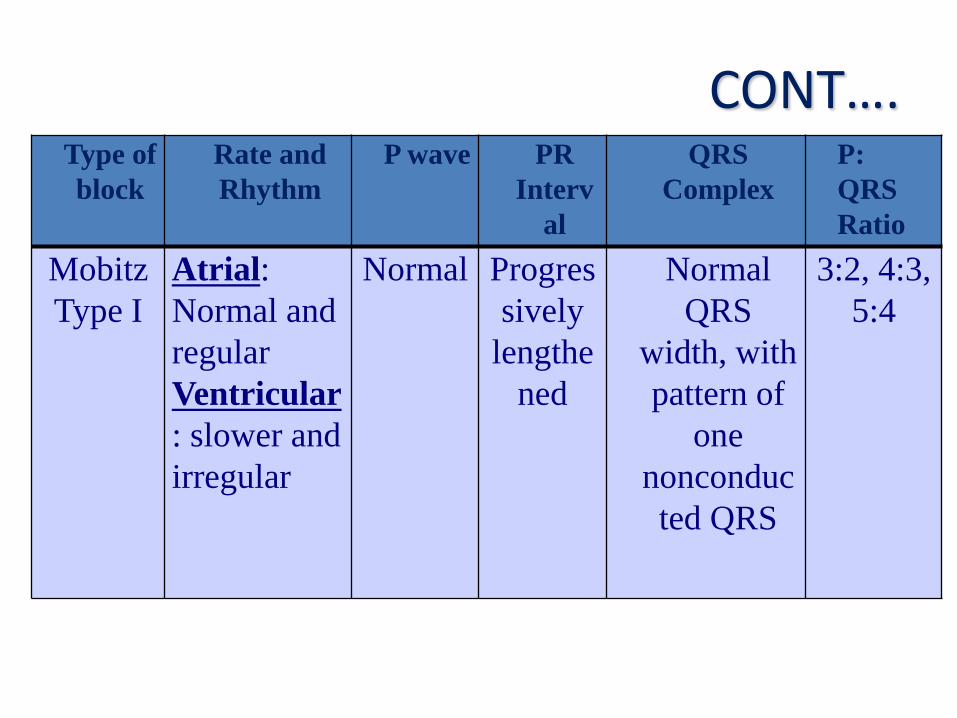
CONT….Type of
block
Rate and
Rhythm
P wave PR
Interv
al
QRS
Complex
P:
QRS
Ratio
Mobitz
Type I
Atrial:
Normal and
regular
Ventricular
: slower and
irregular
Normal Progres
sively
lengthe
ned
Normal
QRS
width, with
pattern of
one
nonconduc
ted QRS
3:2, 4:3,
5:4

SECOND DEGREE HEART BLOCK (2º) MOBITZ TYPE I (WENKEBACH)
PR PR
PR DROPPED BEAT

TREATMENT
Symptomatic = atropine or temporary pacemaker
Asymptomatic = the rhythm should be observed
with a transcutaneous pacemaker on standby.

SECOND DEGREE HEART BLOCK (2º)MOBITZ TYPE II
DEFINITION
It is sudden failure of conduction of an atrial
impulse to the ventricles without progressive increases in
conduction time of consecutive P waves. It occurs below the
AV node and is usually associated with bundle- branch
block; therefore, the dropped beats are usually a
manifestation of bilateral bundle- branch block.

CAUSES
Anterior myocardial infarction
Coronary heart disease
Rheumatic heart disease
Digitalis toxicity

ECG CHARACTERISTICS
PR Interval normal & constant
Occasionally a dropped beat is seen

CONT….Type
of
block
Rate and
Rhythm
P wave PR
Interv
al
QRS
Complex
P:QR
S
Ratio
Mobitz
Type II
Atrial :
Usually
normal and
regular or
irregular
Ventricular:
slower and
regular or
irregular
P wave
occurs in
multiples
Normal
or
prolong
ed
Widened
QRS, no
connectio
n with P
waves
2:1,
3:1,
4:1,
5:1

Second Degree Heart Block (2º)Mobitz Type II
PR PR DROPPED BEAT PR

CLINICAL SIGNIFICANCE
• significant disease.
• This can progress to third degree heart blockand is associated with a poor prognosis.
TREATMENT
• pacemaker
• Drugs as atropine, epinephrine, isoproterenolor dopamine can be used to increase heartrate.

SECOND DEGREE HEART BLOCK (2º)2 : 1
DEFINITION
It is failure of conduction of every otheratrial impulse. The ratio will be as 2 P waves :1 QRS.
• Unable to strictly classify as Mobitz Type I or II
• Particular type of second degree Heart Block
• Ratio 2 P waves : 1 QRS

ECG CHARACTERISTICS
PR interval
• Type I- Longer than normal (more than 0.20
second)
• Type II- Normal
QRS complex
• Type I- Narrow
• Type II- Wide

Second Degree Heart Block (2º)2 : 1

Cont...
CLINICAL SIGNIFICANCE
• Unable to classify as Mobitz type I or II
• Will be associated with symptoms, dizziness, lethargy etc.
• This can deteriorate to 3º Heart Block
TREATMENT
• Pacemaker

THIRD DEGREE HEART BLOCK (3º)(COMPLETE)
DEFINITION
It constitutes one form of AVdissociation in which no impulses from the atriaare conducted to the ventricles. The atria arestimulated and contract independently of theventricles. The ventricular rhythm is an escaperhythm and the ectopic pacemaker may beabove or below the bifurcation of the Hisbundle.

CAUSES
Fibrosis or calcification of cardiac conduction
system
Coronary artery disease
Cardiomyopathy
Myocarditis
Myocardial infarction
• Surgery

ECG CHARACTERISTICS
Complete failure of the AV Node
No impulses from Sinus Node will pass through to the ventricles
Some part if the conducting system will take over as pacemaker of the heart (even a myocardial cell 10-15 bpm)

CONT…
• P wave rate – normal
• Ventricular rate – slow
• Ventricular complex may be broad
• Complete dissociation between P waves & QRS

CONT…
Type
of
block
Rate
and
Rhythm
P wave PR
Interv
al
QRS
Complex
P:QRS
Ratio
Third
degree
heart
block
Ventricula
r rate 20-
40
beats/min
and
regular
Normal
but no
connectio
n with
QRS
complex
Variable Normal
or
widened
QRS, no
connectio
n with P
waves
More P
waves
than
QRS
complex

Third Degree Heart Block (3º)(Complete)
P P P P P
QRS QRS

Cont....CLINICAL SIGNIFICANCE
• Symptoms LOC, Confusion, Dizziness, Low
BP
• Can lead to standstill, VT or VF (stokes
Adams)
TREATMENT - pacemaker

Types of infra-hisan block
Left bundle branch block
Left anterior fascicular block
Left posterior fascicular block
Right bundle branch block

CLINICAL MANIFESTATIONS
Slow heart rate
Irregular heart rate
Arrhythmias
In case of severe block ;
Breathlessness
Breathlessness with exertion
Dizziness

Fainting
Fatigue
Heart block
Chest pain
Shortness of breath
Seizures
Light headedness


MANAGEMENT

Cont…
ANTI ARRYTHMIC DRUGS
DEFIBRILLATION
SYNCHRONIZED DEFIBRILLATOR
IMPLANTABLE CARDIOVERTER DEFIBRILLATOR
RADIOFREQUENCY ABLATION CATHETER

Anti-arrhythmic drugs
• Class I membrane stabilizing agents
• Class II β-adrenoceptor antagonist β blockers
• Class III Amiodarone drugs – prolong action potential
• Class IV Slow calcium channel blockers

Cont…Atropine Sulphate
0.6 mg IV
Maximum 3mg
Adenosine
3 mg IV over 2sec followed by 6mg( if needed)
12 mg 1-2 min interval

Cont…
DIGOXIN
0.2-0.5 mg oral / IV
Digoxin toxity
Extracardiac manifestations – Anorexia, Nausea, Vomiting, Diarrhea, Altered colour vision.
Cardiac manifestations
• Bradycardia, ventricular ectopics
• Atrial & ventricular tachycardia
• Ventricular fibrillation & bigeminy


Radio frequency catheter ablation
It is a procedure that can cure many
types of fast heart beats. Using a special wires
or catheters threaded into the heart. Here
they are using radiofrequency energy.
