is knowledge power? developing an infrastructure that enhances patient safety pharmacy cqi in...
TRANSCRIPT
Is Knowledge Power?Developing An Infrastructure That
Enhances Patient Safety
Pharmacy CQI In Florida
David B. Brushwood, R.Ph., J.D.
Professor of Pharmacy Health Care Administration
The University of Florida
College of Pharmacy

Who says the system is broken?• The media
– Television programs
– Magazines
– Newspapers
• State regulators
• The courts
• The IOM Report
• But…
– No pharmacist wants to make a mistake
– No pharmacy manager wants pharmacists to make a mistake
• Maybe the system just needs to be organized better.

Harco Drugs v. Holloway669 So.2d 878 (Ala. 1995).
Harco Drugs v. Holloway669 So.2d 878 (Ala. 1995).
“We note that the jury was also informed of 233 incident reports that had been prepared by Harco employees during the three years preceding the incident. This evidence, in addition to evidence of complaints filed with the State Board of Pharmacy and the evidence of lawsuits filed alleging misfilled prescriptions, was relevant to show Harco’s knowledge of problems, and Harco’s having failed to initiate sufficient institutional controls over the manner in which prescriptions were filled.”

Alternative Responses• Do Nothing.
• Punishment.– Advantages
• Practical Appeal.• Political Appeal.• Emotional Appeal.
– Disadvantages• Ineffective
– Too little
– Too much
• Unreliable• Unfair
• Centralized Data Reporting and Feedback
• Centralized QA Program • Error Prevention Clinic• Mandatory or
Recommended CQI• Regulating for Outcomes
(Responsive Regulation) Brennan and Berwick, New Rules (1996).
Ten (Possible) Approaches
• Continuous Quality Improvement Program
• Professional Performance Evaluation
• Consumer Surveys• Criteria and Standards• Localized Minimum
Data Set
• Periodic Self Audit• Centralized
Performance Database• Practice
Accountability Audit• Initial Licensure by
Portfolio• Relicensure by
Portfolio

Continuous Quality Improvement
• Identify and record failures of quality.
• Take a systems view.• Involve all personnel.• Learn from past and
plan for improved future.
• Records available for inspection.

CQI ProgramCQI Program
Not Necessary
6%
Essential12%
Significant42%
Useful40%
Not Necessary
Useful
Significant
Essential

Consumer Surveys
• Conducted at least once per year.
• Pertinent Questions– Is the pharmacist accessible?
– Can you read your prescription label?
– Is your drug therapy helping you get better?
• Evidence of completion available for inspection.

Consumer SurveysConsumer Surveys
Not Necessary
14%
Significant30%
Essential5%
Useful51% Not Necessary
Useful
Significant
Essential
Criteria and Standards
• Criterion: Predetermined elements with which comparison can be made.– Example: No refills more
frequently than day’s supply indicates.
• Standard: Acceptable variation from criterion.– Example: Within 20% (6
days for 30 day period) ok.

Criteria and StandardsCriteria and Standards
Not Necessary
8%
Essential15%
Significant47%
Useful30%
Not Necessary
Useful
Significant
Essential

Periodic Self Audit
• Have criteria and standards been met?– Drug-drug interaction
overrides.
– Duplicative drug therapy.
– Absence of documented patient education.
• Benchmark over time.

Periodic Self AuditPeriodic Self Audit
Not Necessary
12%
Essential10%
Significant38%
Useful40%
Not Necessary
Useful
Significant
Essential
Centralized Performance Database
• Aggregate data from a large number of practice sites.– Uploaded to board.
– Purchased from payer.
• Picture of quality throughout state.
• Compare practice sites.

Centralized Performance DatabaseCentralized Performance Database
Not Necessary
14%
Significant30%
Essential5%
Useful51% Not Necessary
Useful
Significant
Essential

Practice Accountability Audit
• Evaluates Performance Database
• Triggered by violation of criteria/standards
• Request explanation of violation.
• Done by board or by profession.
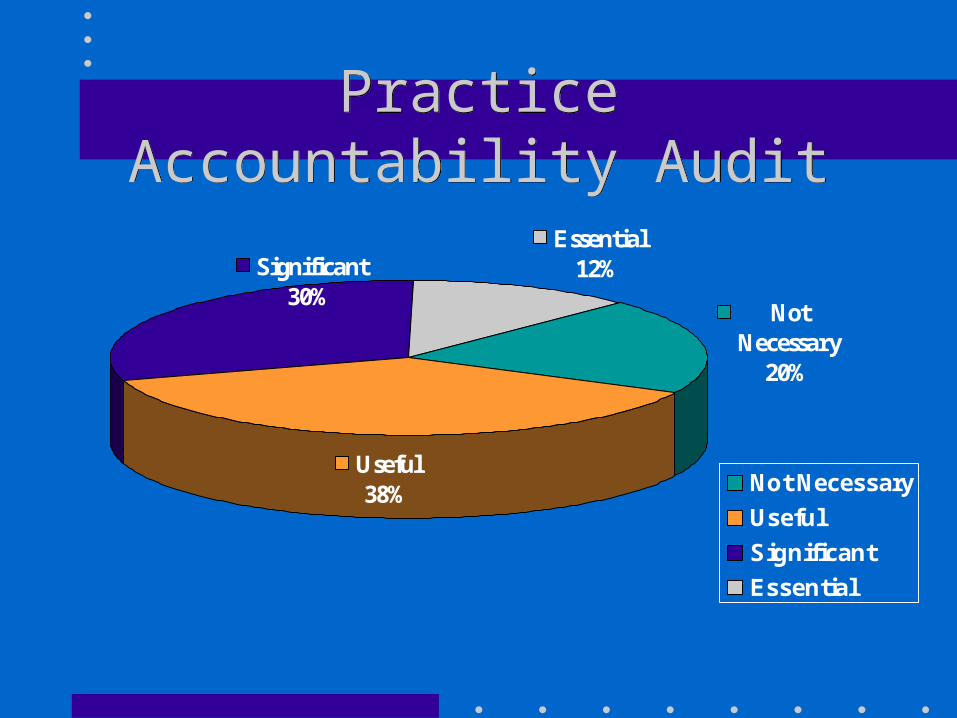
Practice Accountability AuditPractice Accountability Audit
Not Necessary
20%
Essential12%Significant
30%
Useful38% Not Necessary
Useful
Significant
Essential
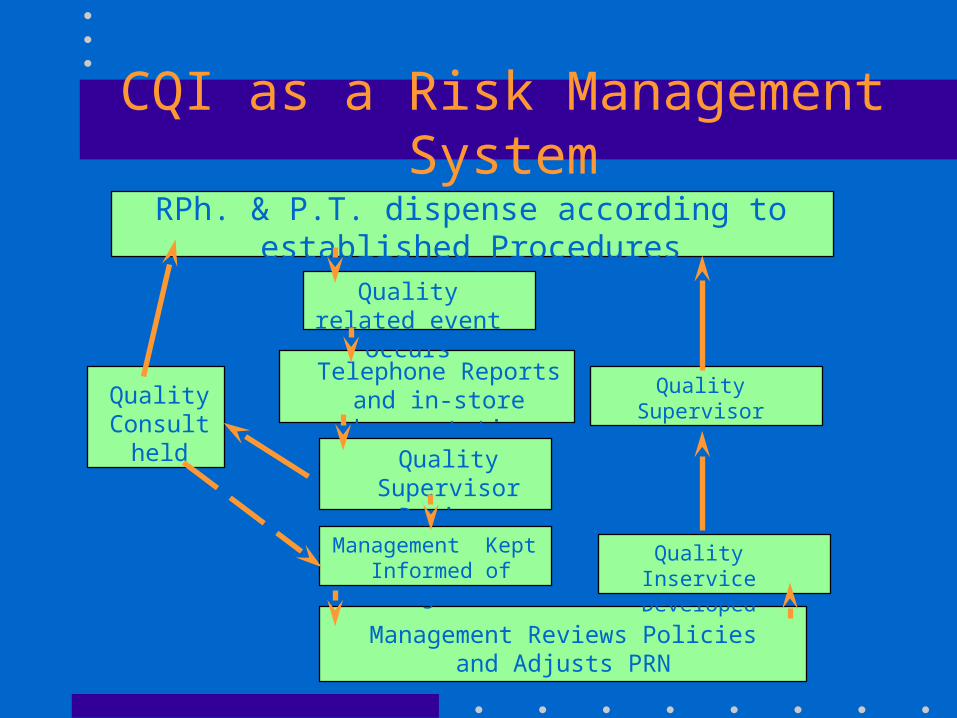
CQI as a Risk Management System
RPh. & P.T. dispense according to established Procedures
Quality related event occurs
Quality Supervisor Reviews
Telephone Reports and in-store documentation
Quality Supervisor Reviews
Quality Inservice Developed
Management Kept Informed of Progress
Management Reviews Policies and Adjusts PRN
Quality Consult
held

CQI and the Florida BOP
– (2) "Quality‑Related Event" means the inappropriate dispensing of a prescribed medication including:
– (a) a variation from the prescriber's prescription order, including, but not limited to:
– 1. dispensing an incorrect drug;– 2. dispensing an incorrect drug strength;– 3. dispensing an incorrect dosage form;– 4. dispensing the drug to the wrong
patient; or– 5. providing inadequate or incorrect
packaging, labeling, or directions.
– (b) a failure to identify and manage:
– 1. over‑utilization or under‑utilization;
– 2. therapeutic duplication;
– 3. drug‑disease contraindications;
– 4. drug‑drug interactions;
– 5. incorrect drug dosage or duration of drug treatment;
– 6. drug‑allergy interactions; or
– 7. clinical abuse/misuse.
64B16‑27.300 Standards of Practice ‑‑ Continuous Quality Improvement Program.(1) "Continuous Quality Improvement Program" means a system of standards and procedures to identify and evaluate quality‑related events and improve patient care.

CQI Components• P&P Manual• CQI Committee• Record QREs• Review Record at least once every 3 months
– staffing levels– workflow– technological support
• Summarization Document (no identifiers)• Protection from Discovery (766.101 FS)

RESULTS
• Inspector looks for evidence of CQI program and compliance.
• Inspector is educator and enabler, to prevent errors not react to them.
• Punishment for failure to conduct CQI, not for failure to be perfect.
• Commercial product available.