intrathecal cytotoxic t-cell immunotherapy for metastatic...
TRANSCRIPT

Vol. 7, 917s-924s, March 2001 (Suppl.) Clinical Cancer Research 917s
Intrathecal Cytotoxic T-Cell Immunotherapy for Metastatic Leptomeningeal Melanoma a
A n n e t t e R. C l e m o n s - M i l l e r , G u r k a m a l S. Chat ta ,
L a u r a H u t c h i n s , E d g a r d o J. A n g t u a c o ,
A n t o n e l l a Ravagg i , A l e s s a n d r o D. Sant in , and
M a r t i n J. C a n n o n 2 Departments of Geriatrics [A. R. C-M., G. S. C.], Medicine [G. S. C., L. H.], Radiology [E. J. A.], Obstetrics and Gynecology [A. R., A. D. S.], and Microbiology and Immunology [A. R. C-M., M. J. C.], University of Arkansas for Medical Sciences, Little Rock, Arkansas 72205, and Division of Gynecologic Oncology, University of Brescia Medical School, Brescia, Italy [A. R., A. D. S.]
Abstract A 49-year-old patient with primary, recurrent melanoma
on the lower extremity developed metastatic leptomeningeal melanoma that did not respond to treatment with radiation therapy or intrathecal interleukin 2 (IL-2). Disease was char- acterized by neurological symptoms, including loss of hearing, loss of short-term memory, and gait disturbance. CD8 + CTLs were generated in vitro using autologous dendritic cells pulsed with peptides from the melanoma-associated antigens tyrosin- ase (145-156), Melan-A/MART-1 (26-35), and gpl00/Pmel 17 (209-217). The CTLs exhibited up to 74% specific lysis against peptide-pulsed autologous EBV-transformed B cells, with Melan-A-specific CTLs yielding the greatest lytic activity. CD8 + CTLs possessed a type 1 cytokine profile, expressing tumor necrosis factor oL and IFN~/but not IL-4. Infusions of CTLs were supported with systemic low-dose IL-2 administra- tion. 111In labeling and computerized gamma imaging were used to monitor the distribution of CTLs up to 48 h after infusion. Intra-arterial delivery via the right carotid artery was followed by redistribution of the CTLs to the lungs, liver, and spleen within 16 h. In contrast, delivery via an indwelling Ommaya reservoir resulted in prolonged retention of CTLs within the brain for at least 48 h after infusion. Marked but transient elevations in tumor necrosis factor e~, IFN-% and IL-6 in the cerebrospinal fluid were observed within 4 h of CTL infusion. There was no evidence of tumor progression throughout the treatment period, and clinically the patient showed some resolution of neurological symptoms.
Introduct ion Although the immunogenic potential of melanoma has
been recognized for some time, clinical trials involving the use
of tumor-infiltrating lymphocytes or lymphokine-activated killer cells in the treatment of malignant melanoma have met with only modest success (1-6). The reasons for the limited efficacy may include poor definition of the effector cells, failure of the effector cells to recognize defined antigens, and poor localization of the effector cells to the site of the tumor. The recent identification of defined melanoma-associated tumor an- tigens such as gp 100, Melan-A/MART-1, tyrosinase, MAGE-1, and MAGE-3 (7-12), combined with the ability to induce T-cell responses of defined function and phenotype, has led to a strong resurgence of interest in immunotherapy of melanoma. Most notably, the application of DCs 3 as powerful inducers of mela- noma tumor antigen-specific CD8 + cytotoxic CTL responses has provided investigators with the tools necessary for a targeted approach to the treatment of disease (13-19).
Notwithstanding the major advances in DC-based induc- tion of tumor-antigen-specific T-cell responses in patients with malignant disease, clinical administration of autologous anti- gen-specific CTLs presents some practical challenges. One of the more important issues centers on election of an appropriate route of delivery for optimal localization and retention of CTLs at the tumor site. The use of radioisotopic cell labeling and subsequent imaging of T-cell localization in the patient affords us the opportunity to tailor the route and method of CTL immunotherapy for optimum delivery to the tumor. Isotopes such as ~ I n can be used for short-term visualization and tracking of cellular components in real time using standard scanning techniques (20-23).
In this study, we have used autologous DCs pulsed with defined HLA-restricted peptides from the gpl00, Melan-A/ MART-l, and tyrosinase melanoma antigens to stimulate CD8 + CTLs for immunotherapeutic treatment of a patient with metastatic leptomeningeal melanoma. Antigen-specific CTLs were delivered through catheterization of the internal carotid artery or local deliv- ery through an indwelling intracranial Ommaya reservoir. ~11In labeling and computerized gamma imaging were used to monitor CTL migration and elucidation of the most effective route of delivery. CTL activity in vivo was assessed indirectly through measurement of T-cell and inflammatory cytokine production in the CSF at various time points after treatment.
Materials and Methods Case History. A 49-year-old woman presented with a
melanocytic nevus (Breslow thickness, 0.8 ram), which was re- moved in February 1995. A local recurrence (Breslow thickness,
1 This study was supported by NIH Grants CA 63931 (to M. J. C.) and CA 76033 (G. S. C.) and the Arkansas Cancer Research Center. a To whom requests for reprints should be addressed, at Department of Microbiology and Immunology, Mail Slot 511, University of Arkansas for Medical Sciences, 4301 West Markham, Little Rock, AR 72205. Phone: (501)296-1254; Fax: (501)686-5359; E-mail: cannonmartin@ exchange.uams.edu.
3 The abbreviations used are: DC, dendritic cell; PBMC, peripheral blood mononuclear cell; CSF, cerebrospinal fluid; MRI, magnetic res- onance imaging; GM-CSF, granulocyte/macrophage-colony stimulating factor; TNF, tumor necrosis factor; IL, interleukin; NK, natural killer; PMA, phorbol myristate acetate; CNS, central nervous system.
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

918s CTL Immunotherapy for Leptomeningeal Melanoma
Fig. 1 MRI analysis prior to induction of adoptive T-ceil immunotherapy. MRIs obtained without (A) and with (B) contrast revealed multiple areas of enhancement along the ependymal surfaces of the ventricles and within the brain parenchyma, a small ring enhancing lesion in the left parietal gray/white matter junction measuring <1 cm in size, and bi- lateral enhancing lesions at the internal acoustic canals (not visible in this plane).
3.3 ram) was removed in November 1995. Additional local recur- rences, diagnosed as melanoma, were treated by wide local exci- sion, followed by high-dose IFN therapy. IFN treatment was cur- tailed because of excessive neurological side effects. Further local recurrences were excised in April and August 1997, followed by local radiation therapy. In April 1997, the patient was enrolled on a vaccine t]ial with an anti-idiotype antibody (TriGem), targeting disialoganglioside GD2, After an initial weekly induction phase, the patient remained on s.c. monthly vaccine therapy until March 1999, receiving a total of 2.7 mg (27 doses) of TriGem (TriGem Phar- maceuticals, Inc., South San Francisco, CA) admixed with QS-21 adjuvant (Biopharmaceuticals, Inc., Worcester, MA).
The patient remained disease free and asymptomatic until December 1998, when she presented with symptoms of dizzi- ness and difficulties with balance and hearing. A MRI scan of the brain showed nodular enhancement along the corpus callo- sum in the lateral ventricles, two enhancing left parietal lesions, and involvement of both internal auditory canals. CSF cytology was consistent with melanoma. Whole-body scanning did not reveal disease at any other site, and serum chemistries were normal. In January 1999, she was treated with daily intrathecal IL-2 via an Ommaya reservoir receiving a total of 10 doses (1 • 106 units/me/dose). She failed to respond and suffered acute toxic side effects. In February 1999, she underwent radiation therapy, receiving a total of 3750 cGy in 15 fractions to the whole brain and a total of 1250 cGy in 5 fractions to the ventricles. A repeat MRI in April 1999 indicated disease pro- gression and a new lesion in her left parietal region (Fig. 1). The parietal lesions were treated with gamma knife stereotactic radiosurgery in April 1999, followed by intrathecal GM-CSF in May 1999. Five doses of intrathecal GM-CSF were adminis- tered at 200 Ixg/m2/dose/day. The patient continued to have persistent neurological symptoms, and hence from June to No- vember 1999, she was treated under a Food and Drug Admin- istration-approved, melanoma antigen-specific CTL immuno- therapy protocol (IND #8422), as described in this report.
Media and Reagents. DC and CTL culture medium was AIM-V (Life Technologies, Inc., Grand Island, NY). Recombi- nant human GM-CSF (Leukine; 5.6 • 106 units/mg) was from Immunex Corp. (Seattle, WA), and recombinant human IL-4 (2.9 • 10 4 units/Ixg) and TNF-oL (1.1 • 105 units/Ixg) were from
R&D Systems (Minneapolis, MN). Recombinant human IL-2 for in vitro T-cell culture was provided by the Biological Re- sponse Modifiers Program, National Cancer institute, whereas the IL-2 for patient treatment was from Chiron (Emeryville, CA). Prostaglandin E 2 was from Sigma Chemical Co. (St. Louis, MO). The HLA-Al-restricted tyrosinase peptide 145- 156, and the HLA-A2-restricted Melan-A/MART-1 peptide 26-35 and gpl00 peptide 209-217 (24-27) were synthesized by Genemed Synthesis, Inc. (South San Francisco, CA). PCR primers were synthesized by Life Technologies, Inc.
Reverse Transcr ipt ion-PCR Analysis . RNA from mel- anoma cells isolated from the patient's CSF, and from the MEL-24 cell line (American Type Culture Collection, Rock- ville, MD) was extracted with TRIzol (Life Technologies, Inc.), according to the manufacturer's instructions. RNA was reverse- transcribed into cDNA using the SuperScript One-Step RT-PCR System (Life Technologies, Inc.). The Melan-A/MART-1 exter- nal primer sequences were 5'-ATG CCA AGA GAA GAT GCT CAC-3' and 5'-AGC ATG TCT CAG GTG TCT GC-3', yield- ing a 384-bp product (28), and the internal primer sequences were 5'-CAC GGC CAC TCT TAC ACC AC-3' and 5'-GGA GCA TTG GGA ACC ACA GG-3', yielding a nested product of 252 bp (29). The tyrosinase external primer sequences were 5'-TTG GCA GAT TGT CTG TAG CC-3' and 5'-AGG CAT TGT GCA TGC TGC TT-3', yielding a 284-bp product (30, 31), and the internal primer sequences were 5'-GTC TTT ATG CAA TGG AAC GC-3' and 5'-GCT ATC CCA GTA AGT GGA CT-3', yielding a nested product of 207 bp (31). The gpl00 external primer sequences were 5'-GCT TGG TGT CTC AAG GCA ACT-3' and 5'-CTC CAG GTA AGT ATG AGT GAC-3', yielding a 751-bp product (28), and the internal primer se- quences were 5'-CAG CTG TAT CCA GAG TGG ACA-3' and 5'-TCA GCT TCA GCC AGA TAG CCA-3', yielding a nested product of 626 bp. PCR products were resolved in 2% agarose gels and visualized with the Gelprint 2000i system (Biophoton- ics Corp., Ann Arbor, MI).
DCs. DCs were generated as described previously (32), with minor modifications. Briefly, PBMCs were allowed to adhere to six-well culture dishes (5 • 106 PBMCs/well) at 37~ in AIM-V medium. After 2 h, nonadherent cells were removed, and the adherent cells were cultured in AIM-V (3 ml/well) plus
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 919s
1000 units/ml GM-CSF and 500 units/mt IL-4. An additional 1000 units/ml GM-CSF and 500 units/ml IL-4 were added to the cells every 3 days, and 1000 units/ml TNF-ot and 1 ~M pros- taglandin E 2 were added on day 6 (33). Mature DCs were collected on day 8 and pulsed with 50 Ixg/ml peptide for 1.5 h at 37~ after which the DCs were washed once with AIM-V medium prior to stimulation of T cells.
Generation of Peptide-specific CD8 + CTLs. Peptide- pulsed DCs were cultured with autologous PBMCs at ratios of 20-30:1 PBMCs:DCs, at a final concentration of 106 PBMCs/ml in AIM-V medium supplemented with 10 units/ml IL-2. Cultures were fed every 3 days by half changes of AIM-V medium supple- mented with 10 units/ml IL-2. Responder T cells were restimulated every 7-14 days with peptide-pulsed DCs in AIM-V medium plus 100 units/ml IL-2. After two rounds of stimulation in vitro, CD8 + T cells were positively selected with mlti-CD8 Dynabeads (Dynal, Inc., Lake Success, NY), according to the manufacturer's instruc- tions. Resulting populations were >95% CD8 +, as determined by flow cytometric analysis. To achieve the cell numbers needed for immunotherapy, CD8 + CTL cultures were expanded by stimula- tion with 0.5 Ixg/ml anti-CD3 monoclonal antibody (OKT3) and irradiated (2500 cGy) autologous PBMCs in AIM-V medium plus 100 units/ml IL-2.
Cytotoxicity Assays. Standard 51Cr-release assays were performed essentially as described (34). Briefly, autologous EBV-transformed lymphoblastoid cells (LCL) were pulsed with peptide (50 Ixg/ml, 1 h at 37~ subsequently labeled for 1 h with 50 0oCi Na2[ 5 l Cr]O4 (New England Nuclear, Boston, MA), and washed three times before use. NK-sensitive K562 target cells were similarly 51Cr labeled. Target cells were plated at 1 • 104/well in 96-well round-bottomed plates with CD8 + effector T cells at the ratios indicated. 51Cr released into the supernatant after target cell lysis was measured on a Cobra Auto Gamma counter (Packard, Meriden, CT). Assays were performed in triplicate wells, and the percentage of target cell lysis was calculated as described (34).
Intracellular Cytokine Assays. Flow cytometric analy- sis of intracellular cytokine expression by CD8 + T cells was performed as described (34). CD8 § T cells were treated with or without 50 ng/ml PMA (Sigma) and 500 ng/ml ionomycin (Sigma) in 24-well plates at 37~ After 3 h of incubation, 10 txg/ml Brefeldin A (Sigma) were added to each well. After 6 h of incubation, the cells were collected, washed, and fixed with 2% paraformaldehyde in PBS for 10 min, washed once more with PBS, and permeabilized with 0.5% saponin (Sigma) and 1% BSA (Sigma) in PBS. Nonactivated and activated CD8 + T cells were then stained with FITC-anti-IFN-y and phyco- erythrin-anti-IL-4 (Becton Dickinson, San Jose, CA) for 30 min at room temperature, washed twice with 0.5% saponin and 1% BSA in PBS, and once with 0.5% BSA in PBS, and fixed a second time with 2% paraformaldehyde in PBS. Fluorescence was recorded with a FACScan (Becton Dickinson), and data were analyzed with WinMDI software (kindly provided by Joe Trotter, Scripps Research Institute, La Jolla, CA).
Indium Labeling. CD8 + T cells were labeled with 1111n oxine (Amersham Life Science, Arlington Heights, IL) as de- scribed (20). Briefly, 108 T cells were spun down and resus- pended directly in 1 mCi of ~ 11In oxine (approximate volume, 1 ml) and incubated at room temperature for 20 min. Labeling was
terminated by the addition of 2 ml of autologous serum, fol- lowed by one wash with excess PBS. T cells were then resus- pended in 5-10 ml, injection-grade saline plus 2% autologous serum. Incorporated radiolabel was measured with a nuclear medicine dose calibrator prior to infusion. Incorporated activity averaged 750 IxCi. Digital gamma camera images after T-cell transfer to the patient were recorded with a Siemens Diacam (Siemens, Chicago, IL) at 1, 16, 24, and 48 h after infusion.
Cytokine ELISA. CSF samples collected via the Om- maya reservoir were centrifuged to remove cellular components and then frozen at 20~ ELISAs for TNF-o~, IFN-3,, IL-6, and IL-10 were conducted with ELISA kits (Caltag, Burlingame, CA), according to the manufacturer's instructions.
Safety Tests. In accordance with Food and Drug Admin- istration requirements, lymphocyte cultm'es were tested for bac- terial contamination by Gram's stain and microbiological cul- ture. Mycoplasma tests were performed by PCR assay (Stratagene, La Jolla, CA), and the presence of endotoxins was assessed by the Limulus amebocyte lysate test by an independ- ent laboratory (ViroMed Biosafety, Camden, NJ). All cultures tested negative for bacterial and Mycoplasma contamination, and the levels of endotoxin were less than 0.03125 EU/ml.
Results Antigen Expression by Melanoma Tumor Ceils. Nu-
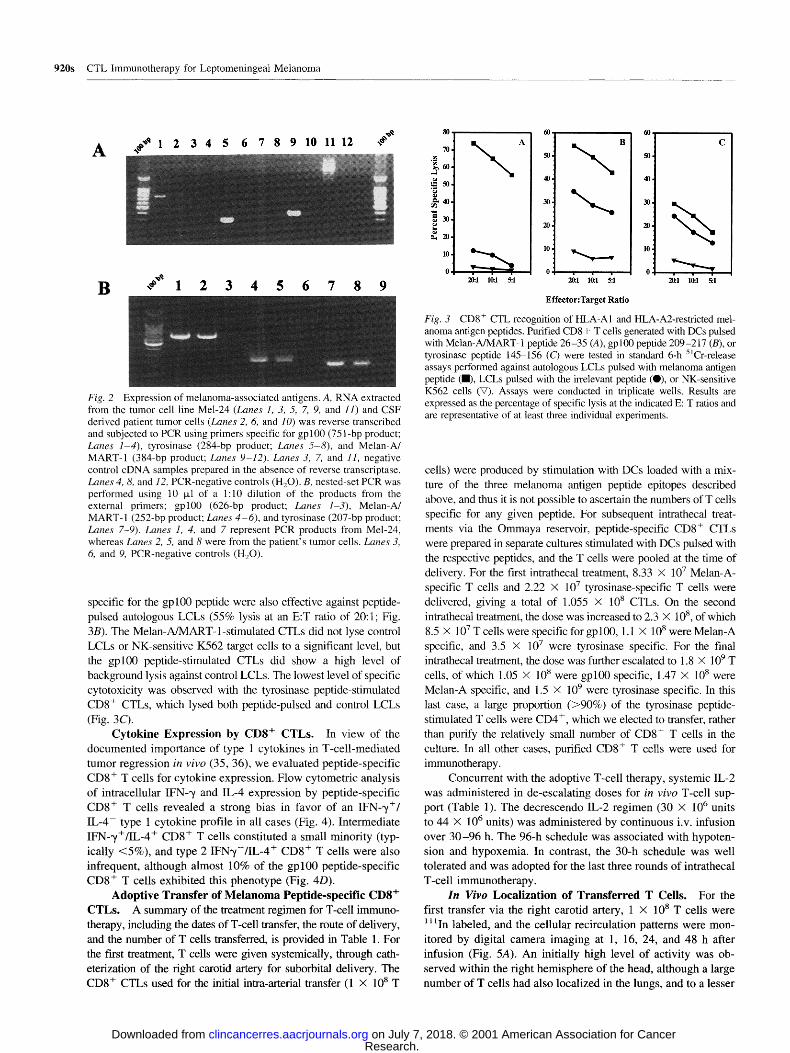
merous studies have shown that the melanoma differentiation antigens tyrosinase, gpl00, and Melan-A/MART-1 are fre- quently expressed in metastatic lesions (8-10). Accordingly, we tested for expression of these antigens in tumor cells recovered from the patient's CSF. Melanoma cells were found in very low numbers (< 100/ml) in CSF drawn via the Ommaya reservoir, and thus the cellular fractions from several CSF samples were pooled, and the RNA was extracted and subject to nested set PCR. The outer primers gave PCR products for gpl00, tyrosin- ase, and Melan-A from RNA extracted from the MEL-24 mel- anoma cell line (Fig. 2A, Lanes 1, 5, and 9). However, an initial round of PCR using the outer primers failed to detect tyrosinase or gpl00 expression and revealed only faint expression of Melan-A (Fig. 2A, Lanes 2, 6, and 10) in the patient-derived RNA. In contrast, a second round of PCR using nested primers resulted in amplification of products for all three antigens from the patient-derived RNA sample (Fig. 2B, Lanes 2, 5, and 8).
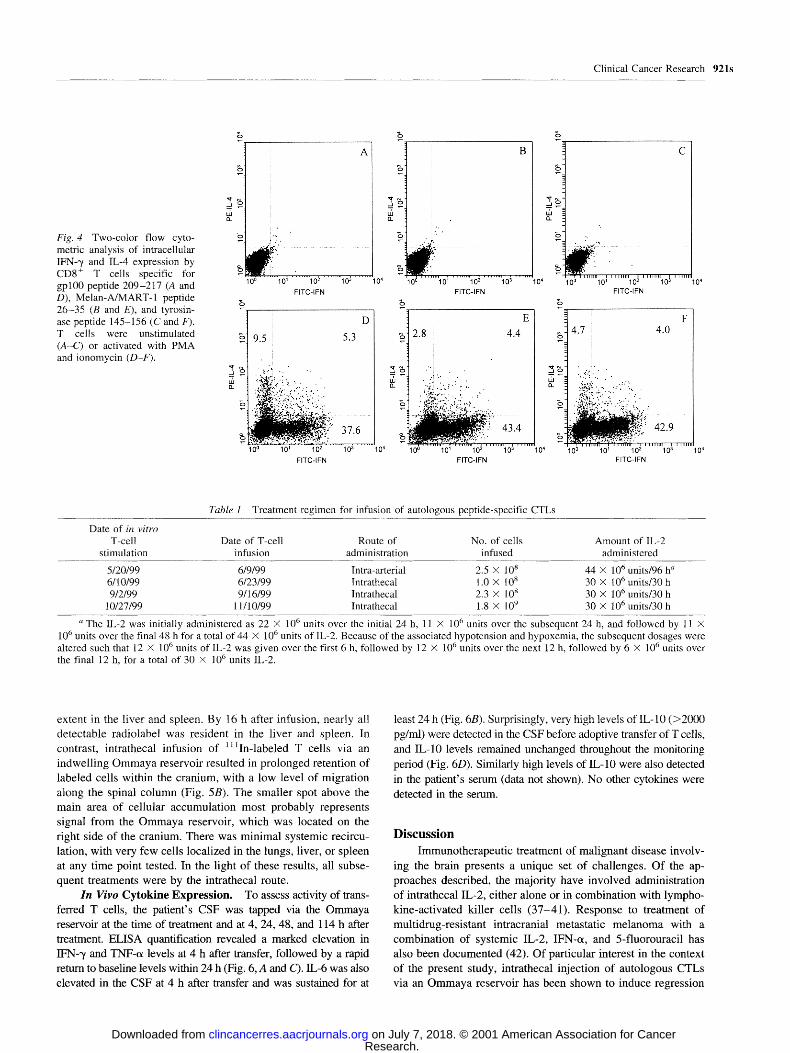
Generation of Melanoma Antigen-specific CD8 + CTLs. The patient's class I HLA type (AI, A2, B7, B62) included both the A1 and A2 alleles, which afforded us a wide choice of potential T-cell epitope targets within the gpl00, tyrosinase, and Melan-A/ MART-I antigens found to be expressed in tumor cells from the CSF. The ttLA Al-binding tyrosinase 145-156 peptide and the HLA A2-binding gpl00 209-217 and Melan-A/MART-1 26-35 peptides were selected for DC-based stimulation of specific CD8 + CTLs. Cytotoxicity was assessed after two rounds of in vitro stimulation, followed by purification of CD8 + T cells. The inac- cessibility of aumlogous tumor cells flom this patient did not permit direct assessment of potential antitumor T-cell cytotoxicity. For this reason, we tested CD8 + CTL function against autologous LCLs pulsed with peptides. Melan-A/MART-1 peptide-specific CTLs showed the highest level of lysis (up to 75% at an E:T ratio of 20:1) against peptide-pulsed autologous LCLs (Fig. 3A). CTLs
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
A , , ~ 1 2 3 4 5 6 7 8 9 10 11 12 ,#'~
920s CTL Immunotherapy for Leptomeningeal Melanoma
B ,~** 1 2 3 4 5 6 7 8 9
Fig. 2 Expression of melanoma-associated antigens. A, RNA extracted from the tumor cell line Mel-24 (Lanes 1, 3, 5, 7, 9, and l l ) and CSF derived patient tumor cells (Lanes 2, 6, and 10) was reverse transcribed and subjected to PCR using primers specific for gpl00 (751-bp product; Lanes 1-4), tyrosinase (284-bp product; Lanes 5-8), and Melan-A/ MART-1 (384-bp product; Lanes 9-12). Lanes 3, 7, and 11, negative control cDNA samples prepared in the absence of reverse transcriptase. Lanes 4, 8, and 12, PCR-negative controls (H20). B, nested-set PCR was performed using 10 ~1 of a 1:10 dilution of the products from the external primers; gpl00 (626-bp product; Lanes 1-3), Melan-A/ MART-1 (252-bp product; Lanes 4-6) , and tyrosinase (207-bp product; Lanes 7-9). Lanes 1, 4, and 7 represent PCR products from Mel-24, whereas Lanes 2, 5, and 8 were from the patient's tumor cells. Lanes 3, 6, and 9, PCR-negative controls (H20).
specific for the gpl00 peptide were also effective against peptide- pulsed autologous LCLs (55% lysis at an E:T ratio of 20:1; Fig. 3B). The Melan-A/MART-l-stimulated CTLs did not lyse control LCLs or NK-sensitive K562 target cells to a significant level, but the gpl00 peptide-stimulated CTLs did show a high level of background lysis against control LCLs. The lowest level of specific cytotoxicity was observed with the tyrosinase peptide-stimulated CD8 + CTLs, which lysed both peptide-pulsed and control LCLs (Fig. 363.
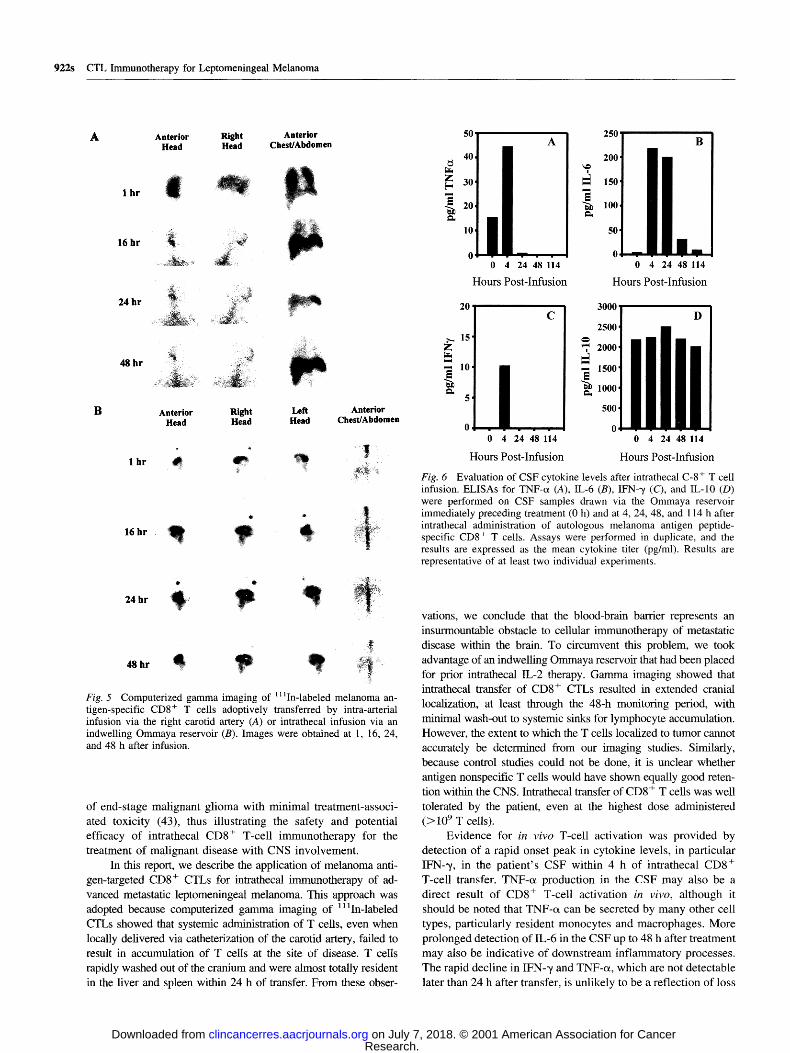
Cytokine Expression by CD8 + CTLs. In view of the documented importance of type 1 cytokines in T-cell-mediated tumor regression in vivo (35, 36), we evaluated peptide-specific CD8 + T cells for cytokine expression. Flow cytometric analysis of intracellular IFN--,/ and IL-4 expression by peptide-specific CD8 + T cells revealed a strong bias in favor of an IFN-'y+/ IL-4 type 1 cytokine profile in all cases (Fig. 4). Intermediate IFN-~/+/IL-4 + CD8 + T cells constituted a small minority (typ- ically <5%), and type 2 IFN'y-/IL-4 + CD8 + T cells were also infrequent, although almost 10% of the gp l00 peptide-specific CD8 + T cells exhibited this phenotype (Fig. 4D).
Adoptive Transfer of Melanoma Peptide-specific CD8 + CTLs. A summary of the treatment regimen for T-cell immuno- therapy, including the dates of T-cell transfer, the route of delivery, and the number of T cells transferred, is provided in Table 1. For the first treatment, T cells were given systemically, through cath- eterization of the right carotid artery for suborbital delivery. The CD8 + CTLs used for the initial intra-arterial transfer (1 x 108 T
80.
70.
~0. 50.
~40. ~,~ ,
~30. g ~,20.
10.
0
~ A
40,
20.
10,
�9 . , 0 , ,,,, ,
E f f e c t o r : T a r g e t R a t i o
60 ,
40,
10.
20:.1 10:1 5:1
Fig. 3 CD8 + CTL recognition of HLA-A1 and HLA-A2-restricted mel- anoma antigen peptides. Purified CD8+ T cells generated with DCs pulsed with Melan-A/MART-1 peptide 26-35 (A), gpl00 peptide 209-217 (B), or tyrosinase peptide 145-156 (C) were tested in standard 6-h SlCr-release assays performed against autologous LCLs pulsed with melanoma antigen peptide (1), LCLs pulsed with the irrelevant peptide (O), or NK-sensitive K562 cells (V). Assays were conducted in triplicate wells. Results are expressed as the percentage of specific lysis at the indicated E: T ratios and are representative of at least three individual experiments.
cells) were produced by stimulation with DCs loaded with a mix- tnre of the three melanoma antigen peptide epitopes described above, and thus it is not possible to ascertain the numbers of T cells specific for any given peptide. For subsequent intrathecal treat- ments via the Ommaya reservoir, peptide-specific CD8 + CTLs were prepared in separate cultures stimulated with DCs pulsed with the respective peptides, and the T cells were pooled at the time of delivery, For the first intrathecal treatment, 8.33 X 10 7 Melan-A- specific T cells and 2.22 X 107 tyrosinase-specific T cells were delivered, giving a total of 1.055 X 108 CTLs. On the second intrathecal treatment, the dose was increased to 2.3 X t08, of which 8.5 X 107 T cells were specific for gpl00, 1.1 X 108 were Melan-A specific, and 3.5 x 10 7 w e r e tyrosinase specific. For the final intrathecal treatment, the dose was further escalated to 1.8 x 10 9 T cells, of which 1.05 x 10 s were gpl00 specific, 1.47 x 108 were Melan-A specific, and 1.5 X 109 were tyrosinase specific. In this last case, a large proportion (>90%) of the tyrosinase peptide- stimulated T cells were CD4 +, which we elected to transfer, rather than purify the relatively small number of CD8 + T cells in the culture. In all other cases, purified CD8 + T cells were used for immunotherapy.
Concurrent with the adoptive T-cell therapy, systemic IL-2 was administered in de-escalating doses for in vivo T-cell sup- port (Table 1). The decrescendo IL-2 regimen (30 X 10 6 units to 44 x 10 6 units) was administered by continuous i.v. infusion over 30-96 h. The 96-h schedule was associated with hypoten- sion and hypoxemia. In contrast, the 30-h schedule was well tolerated and was adopted for the last three rounds of intrathecal T-cell immunotherapy.
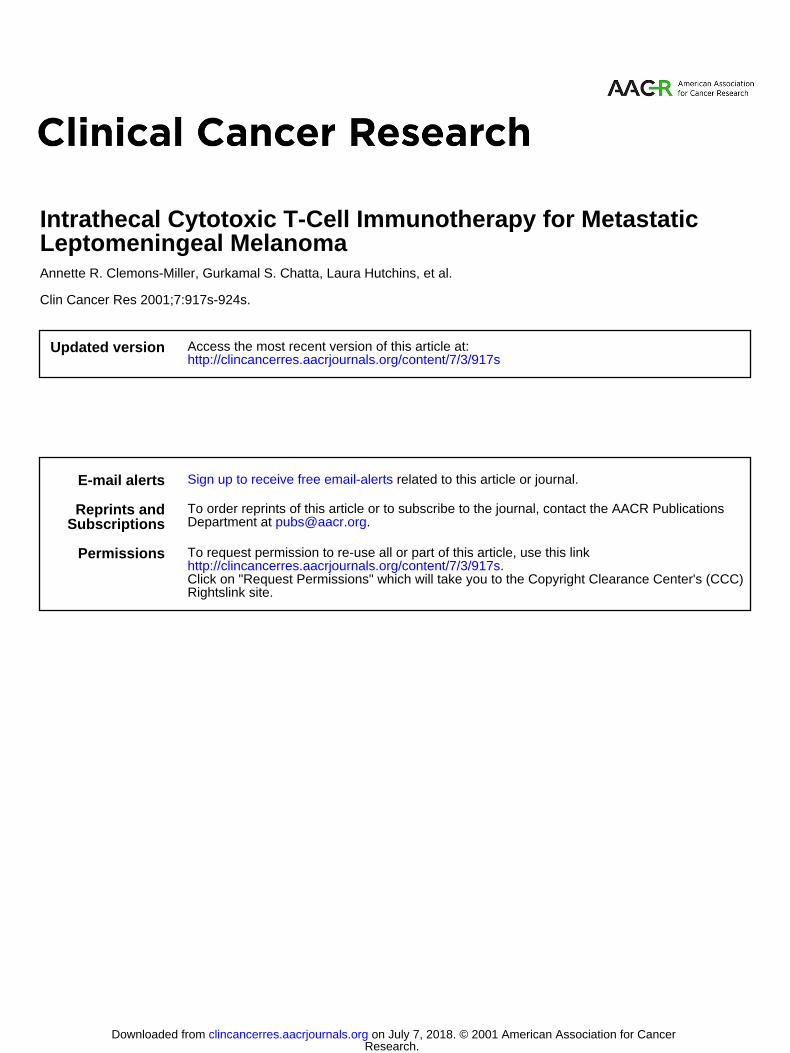
In Vivo Localization of Transferred T Cells. For the first transfer via the right carotid artery, 1 X 108 T cells were 11 ~In labeled, and the cellular recirculation patterns were mon- itored by digital camera imaging at 1, 16, 24, and 48 h after infusion (Fig. 5A). An initially high level of activity was ob- served within the right hemisphere of the head, although a large number of T cells had also localized in the lungs, and to a lesser
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Clinical Cancer Research 9 2 1 s
Fig. 4 Two-color flow cyto- metric analysis of intracellular IFN-'~ and IL-4 expression by CD8 § T cells specific for gpl00 peptide 209-217 (A and D), Melan-A/MART-1 peptide 26-35 (B and E), and tyrosin- ase peptide 145-156 (C and F). T cells were unstimulated (A-C) or activated with PMA and ionomycin (D-F).
'~,E, "7
[ �9 ; "
10 0 10 ~ 10 2 10 3 10 4
F ITC- IFN
E,
1 D ~' 95 5.3
�9 ,:.., .." ..
.j.,~...:,: ...:.........:.. �9
o . ~ , . ,~:...-:..?;:..~:..',.;...
: .,~, ~';" 37.6
10 ~ 10 '~ 10 z 10 3 10 4
F ITC- IFN
t . t -
, ",, ,!,,,, . . . . . . . . , . . . . . . . . . . . . D ~ 101 10 2 10 3
F ITC- IFN
10 4
~,1 2.8 4.4
-t
~1 "" ' "
1 :,;.. '.~,,..,.,......; .
. ,'.4~?;: ....:.',:;,..'.:..
43.4 ~ . ~ , : , : : - : ' i 0 6 . . . . . . . . 10 ~ . . . . . . . i 0 ~ . . . . . . . . 10:; . . . . . . . 10 4
F ITC- IFN
:i ..... i .......... ii 10 0 10"= 10 2 10 '~
F ITC- IFN
E,
10 4
~1 4.7 i 4.0
I
_ ?z " ..,'!'. �9
- 4ii. : : :
42.9
'10; . . . . . . . . 101 . . . . . . . . 10 ~ . . . . . . . '10 ~ . . . . . . . . 10 4
F ITC- IFN
Table 1 Treatment regimen for infusion of autologous peptide-specific CTLs
Date of in vitro T-cell Date of T-cell Route of No. of cells Amount of 1L-2
stimulation infusion administration infused administered
5/20/99 6/9/99 Intra-arterial 2.5 • 108 44 X l06 units/96 h a 6/10/99 6/23/99 Intrathecat 1.0 • 108 30 • 106 units/30 h 9/2/99 9/16/99 lntrathecal 2.3 • 108 30 • 106 units/30 h
10/27/99 11/10/99 lntrathecal 1.8 • 109 30 • 106 units/30 h
a The IL-2 was initially administered as 22 • 106 units over the initial 24 h, 11 • l06 units over the subsequent 24 h, and followed by 11 • 106 units over the final 48 h for a total of 44 • 106 units of IL-2. Because of the associated hypotension and hypoxemia, the subsequent dosages were altered such that 12 • 106 units of IL-2 was given over the first 6 h, followed by 12 • 106 units over the next 12 h, followed by 6 • 106 units over the final 12 h, for a total of 30 • 106 units IL-2.
extent in the liver and spleen. By 16 h after infusion, nearly all detectable radiolabel was resident in the liver and spleen. In contrast, intrathecal infusion of 11tin_labeled T cells via an
indwell ing O m m a y a reservoir resulted in pro longed retention of labeled cells within the cranium, with a low level of migration
along the spinal co lumn (Fig. 5B). The smaller spot above the main area of cellular accumulat ion most probably represents signal f rom the O m m a y a reservoir, which was located on the right side of the cranium. There was minimal systemic recircu-
lation, with very few cells localized in the lungs, liver, or spleen at any t ime point tested. In the light of these results, all subse- quent treatments were by the intrathecal route.
In Vivo C y t o k i n e E x p r e s s i o n . To assess activity of trans- ferred T cells, the patient's CSF was tapped via the Ommaya reservoir at the time of treatment and at 4, 24, 48, and 114 h after
treatment. ELISA quantification revealed a marked elevation in IFN-~/and TNF-o~ levels at 4 h after transfer, followed by a rapid
return to baseline levels within 24 h (Fig. 6, A and C). IL-6 was also
elevated in the CSF at 4 h after transfer and was sustained for at
least 24 h (Fig. 6B). Surprisingly, very high levels of IL-10 (>2000
pg/ml) were detected in the CSF before adoptive transfer of T cells,
and IL-10 levels remained unchanged throughout the monitoring
period (Fig. 6D). Similarly high levels of IL-10 were also detected
in the patient's serum (data not shown). No other cytokines were
detected in the serum.
D i s c u s s i o n
Immunotherapeut ic treatment of mal ignant disease involv-
ing the brain presents a unique set of challenges. Of the ap- proaches described, the majority have involved administration of intrathecal IL-2, either alone or in combinat ion with lympho-
kine-activated killer cells (37-41) . Response to treatment of multidrug-resistant intracranial metastatic me lanoma with a combinat ion of systemic IL-2, IFN-~, and 5-fluorouracil has also been documented (42). Of particular interest in the context
of the present study, intrathecal injection of autologous CTLs via an O m m a y a reservoir has been shown to induce regression
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
922s CTL Immunotherapy for Leptomeningeal Melanoma
A Anterior Right Anterior Head Head Chest/Abdomen
I hr
16 hr
24 hr
48 hr
Anterior Right Left Head Head Head
Anterior Chest/Abdomen
1 hr
16 hr , ~
24 hr i q i : I
Fig. 5 Computerized gamma imaging of i1 ~In-labeled melanoma an- tigen-specific CD8 + T cells adoptively transferred by intra-arterial infusion via the right carotid artery (A) or intrathecal infusion via an indwelling Ommaya reservoir (B). Images were obtained at 1, 16, 24, and 48 h after infusion.
of end-stage malignant glioma with minimal treatment-associ- ated toxicity (43), thus illustrating the safety and potential efficacy of intrathecal CD8 ~ T-cell immunotherapy for the treatment of malignant disease with CNS involvement.
In this report, we describe the application of melanoma anti- gen-targeted CD8 + CTLs for intrathecal immunotherapy of ad- vanced metastatic leptomeningeal melanoma. This approach was adopted because computerized gamma imaging of 111In-labeled CTLs showed that systemic administration of T cells, even when locally delivered via catheterization of the carotid artery, failed to result in accumulation of T cells at the site of disease. T ceils rapidly washed out of the cranium and were almost totally resident in the liver and spleen within 24 h of transfer. From these obser-
0tl A I 40 200
0 0 4 24 48 114 0 4 24 48 114
Hours Post-Infusion Hours Post-Infusion
20 3000
2500 ~. 15
Z~ ~'7' 2000]
- , IO, i ~ 1500 ,ooo 0 4 24 48 114 0 4 24 48 114
Hours Post-Infusion Hours Post-Infusion
Fig. 6 Evaluation of CSF cytokine levels after intrathecal C-8 + T cell infusion. ELISAs for TNF-a (A), IL-6 (B), IFN-',/ (C), and IL-10 (D) were performed on CSF samples drawn via the Ommaya reservoir immediately preceding treatment (0 h) and at 4, 24, 48, and 114 h after intrathecal administration of autologous melanoma antigen peptide- specific CD8 + T cells. Assays were performed in duplicate, and the results are expressed as the mean cytokine titer (pg/ml). Results are representative of at least two individual experiments.
vations, we conclude that the blood-brain barrier represents an insurmountable obstacle to cellular immunotherapy of metastatic disease within the brain. To circumvent this problem, we took advantage of an indwelling Ommaya reservoir that had been placed for prior intrathecal IL-2 therapy. Gamma imaging showed that intrathecal transfer of CD8 + CTLs resulted in extended cranial localization, at least through the 48-h monitoring period, with minimal wash-out to systemic sinks for lymphocyte accumulation. However, the extent to which the T cells localized to tumor cannot accurately he determined from our imaging studies. Similarly, because control studies could not be done, it is unclear whether antigen nonspecific T cells would have shown equally good reten- tion within the CNS. Intrathecal transfer of CD8 + T cells was well tolerated by the patient, even at the highest dose administered (> 109 T cells).
Evidence for in vivo T-cell activation was provided by detection of a rapid onset peak in cytokine levels, in particular IFN-~, in the patient's CSF within 4 h of intrathecal CD8 + T-cell transfer. TNF-o~ production in the CSF may also be a direct result of CD8 + T-cell activation in vivo, although it should be noted that TNF-oL can be secreted by many other cell types, particularly resident monocytes and macrophages. More prolonged detection of IL-6 in the CSF up to 48 h after treatment may also be indicative of downstream inflammatory processes. The rapid decline in IFN-3~ and TNF-oL, which are not detectable later than 24 h after transfer, is unlikely to be a reflection of loss
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

Clinical Cancer Research 923s
of T-cell viability, because the indium scans clearly indicate prolonged residence of viable cells.
One of the more intriguing observations was the detection of very high levels of IL-10, both in the CSF and in the patient's serum, both prior to T-cell immunotherapy and throughout the posttreatment monitoring period (up to 114 h). IL-10 is widely regarded as an immunosuppressive cytokine (44) and can also down-regulate the transporter associated antigen processing (45) and inhibit HLA class I and class II expression (46, 47). IL-10 may thus play a key role in tumor evasion of T-cell immuno- surveillance and may also represent a barrier to T-cell immu- notherapy. In contrast, however, IL-10 has also been reported to increase cytotoxic potential in cervical tumor-specific CD8 + CTLs (48) and may thus enhance cytotoxic effector function in
vivo. In this case, the impact of IL-10 on intrathecal CD8+-T cell immunotherapy is open to conjecture.
For almost 2 years (April 1997 to March 1999), the patient was also treated with the TriGem vaccine, an anti-idiotype anti- body, targeting the disialoganglioside GD2. Preliminary results from the TriGem vaccine trial (n = 47) in advanced melanoma were reported recently (49) and revealed minimal clinical re- sponses. However, it is conceivable that this vaccine influenced the biology of the patient's disease, given that to date (June 2000), she has no evidence of recurrent melanoma outside the CNS.
Clinically, the patient showed a significant improvement in neurological symptoms and general performance status thi'ough the treatment period. Radiological examination has indicated stabiliza- tion of the leptomeningeal lesions, coincident with intrathecal T- cell immunotherapy (June through November, 1999), and up to the present time (June 2000). However, some progression of the lesion in the left parietal region has been observed since the last treatment, suggesting that this site is less amenable to CTL immunotherapy. Collectively, we conclude that intrathecal CD8 + CTL immuno- therapy may be a viable and well-tolerated approach to treatment of metastatic leptomeningeal melanoma but may be less effective against parenchymal CNS disease. Our results provide some evi- dence for in vivo T-cell activation after transfer and further suggest that some therapeutic benefit may accrue from this novel treatment strategy.
A c k n o w l e d g m e n t s We thank Dr. Warren Stringer and Dr. Erik Kilgore, Department of
Radiology, University of Arkansas for Medical Sciences, for helpful interpretation of cranial MRI images. We thank Michelle Welch for assistance in obtaining the numerous CSF samples, and we also thank Cassian Yee, University of Washington, and Mike Lotze, University of Pittsburgh, for numerous insightful discussions.
R e f e r e n c e s
I. Aebersold, P., Hyatt, C., Johnson, S., Hines, K., Korcak, L., Sanders, M., Lotze, M., Topalian, S., Yang, J., and Rosenberg, S. A. Lysis of autologous melanoma cells by tumor-infiltrating lymphocytes: associa- tion with clinical response. J. Natl. Cancer Inst., 83: 932-937, 1991. 2. Pockaj, B. A., Sherry, R. M., Wei, J. P., Yannelli, J. R., Carter, C. S., Leitman, S. F., Carasquillo, J. A., Steinberg, S. M., Rosenberg, S. A., and Yang, J. C. Localization of 111indium-labeled tumor infiltrating lymphocytes to tumor in patients receiving adoptive immunotherapy. Augmentation with cyclophosphamide and correlation with response. Cancer (Phila.), 73: 1731-1737, 1994. 3. Ravaud, A., Legrand, E., Delaunay, M. M., Bussirres, E., Coulon, V., Cany, L., Huet, S., Verdier, D., Kind, M., and Chomy, F. A Phase
I trial of repeated tumour-infiltrating lymphocyte (TIL) infusion in metastatic melanoma. Br. J. Cancer, 71: 331-336, 1995. 4. Keilholz, U., Scheibenbogen, C., Brado, M., Georgi, P., Maclachlan, D., Brado, B., and Hunstein, W. Regional adoptive immunotherapy with interleukin-2 and lymphokine-activated killer (LAK) cells for liver metastases. Eur. J. Cancer, 30A: 103-105, 1994. 5. Dutcher, J. P., Creekmore, S., Weiss, G. R., Margolin, K., Markow- itz, A. B., Roper, M., Parkinson, D., Ciobanu, N., Fisher, R. I., and Boldt, D. H. A Phase II study of interleukin-2 and lymphokine-activated killer cells in patients with metastatic malignant melanoma. J. Clin. Oncol., 7." 477-485, 1989. 6. Kradin, R. L., Kurnick, J. T., Lazarus, D. S., Preffer, F. I., Dubinett, S. M., Pinto, C. E., Gifford, J., Davidson, E., Grove, B., and Callahan, R. J. Tumour-infiltrating lymphocytes and interleukin-2 in treatment of advanced cancer. Lancet, 1: 577-580, 1989. 7. van der Bruggen, P., Traversari, C., Chomez, P., Lurquin, C., De Plaen, E., Van den Eynde, B., Knuth, A., and Boon, T. A gene encoding an antigen recognized by cytolytic T lymphocytes on a human mela- noma. Science (Washington DC), 254: 1643-1647, 1991. 8. Brichard, V., Van Pel, A., W/31fel, T., Wrlfel, C., De Plaen, E., Lethr, B., Coulie, P., and Boon, T. The tyrosinase gene codes for an antigen recognized by autologous cytolytic T lymphocytes on HLA-A2 mela- nomas. J. Exp. Med., 178: 489-495, 1993. 9. Kawakami, Y., Eliyahu, S., Delgado, C. H., Robbins, P. F., Rivoltini, L., Topalian, S. L., Miki, T., and Rosenberg, S. A. Cloning of the gene coding for a shared human melanoma antigen recognized by autologous T cells infiltrating into tumor. Proc. Natl. Acad. Sci. USA, 91: 3515-3519, 1994. 10. Kawakami, Y., Eliyahu, S., Delgado, C. H., Robbins, P. F., Sak- aguchi, K., Appella, E., Yannelli, J. R., Adema, G. J., Miki, T., and Rosenberg, S. A. Identification of a human melanoma antigen recog- nized by tumor-infiltrating lymphocytes associated with in vivo tumor rejection. Proc. Natl. Acad. Sci. USA, 91: 6458-6462, 1994. 1 I. Gaugler, B., Van den Eynde, B., van der Bruggen, P., Romero, P., Gaforio, J. J., De Plaen, E., Lethr, B., Brasseur, F., and Boon, T. Human gene MAGE-3 codes for an antigen recognized on a melanoma by autologous cytolytic T lymphocytes. J. Exp. Med., 179: 921-930, 1994. 12. Kirkin, A. F., Dzhandzhugazyan, K., and Zeuthen, J. The immuno- genic properties of melanoma-associated antigens recognized by cyto- toxic T lymphocytes. Exp. Clin. Immunogenet., 15: 19-32, 1998. 13. Oelke, M., Moehrle, U., Chen, J., Behringer, D., Cerundolo, V., Lindemann, A., and Mackensen, A. Generation and purification of CD8 + Melan-A-specific cytotoxic T lymphocytes for adoptive transfer in tumor immunotherapy. Clin. Cancer Res., 6: 1997-2005, 2000. 14. Abdel-Wahab, Z., DeMatos, P., Hester, D., Dong, X. D., and Seigler, H. F. Human dendritic cells, pulsed with either melanoma tumor cell lysates or the gpl00 peptide(280-288), induce pairs of T-cell cultures with similar phenotype and lytic activity. Cell Immunol., 186: 63-74, 1998. 15. Nestle, F. O., Alijagic, S., Gilliet, M., Sun, Y., Grabbe, S., Dummer, R., Burg, G., and Schadendorf, D. Vaccination of melanoma patients with peptide- or tumor lysate-pulsed dendritic cells. Nat. Med., 4: 328-332, 1998. 16. Rivoltini, L., Squarcina, P., Loftus, D. J., Castelli, C., Tarsini, P., Mazzocchi, A., Rini, F., Viggiano, V., Belli, F., and Pamfiani, G. A superagonist variant of peptide MART1/Melan A27-35 elicits anti-mela- noma CD8+ T cells with enhanced functional characteristics: implication for more effective immunotherapy. Cancer Res., 59: 301-306, 1999. 17. Valmori, D., Pittet, M. J., Rimoldi, D., Lirnard, D., Dunbar, R., Cerundolo, V., Lejeune, F., Cerottini, J. C., and Romero, P. An antigen- targeted approach to adoptive transfer therapy of cancer. Cancer Res., 59: 2167-2173, 1999. 18. Kaplan, J. M., Yu, Q., Piraino, S. T., Pennington, S. E., Shankara, S., Woodworth, L. A., and Roberts, B. L. Induction of antitumor immunity with dendritic cells transduced with adenovirus vector-encoding endoge- nous tumor-associated antigens. J. Immunol., 163: 699-707, 1999. 19. Kirkin, A. F., Thor, S., Hansen, M. R., Barfoed, A., Dzhandzhu- gazyan, K. N., and Zeuthen, J. Establishment of gpl00 and MART-I/ Melan-A-specific cytotoxic T lymphocyte clones using in vitro immu-
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

924s CTL Immunotherapy for Leptomeningeal Melanoma
nization against preselected highly immunogenic melanoma ceil clones. Cancer Immunol. Immunother., 48: 239-246, 1999. 20. Beightol, R. W., and Baker, W. J. Labeling autologous leukocytes with ind ium-I l l oxine. Am. J. Hosp. Pharm., 37: 847-850, 1980. 21. Dutcher, J. P. Labeled cells in patients with malignancy. Semin. Nucl. Med., 14:251-261, 1984. 22. Mtiller, C., Zielinski, C. C., Linkesch, W., Ludwig, H., and Sin- zinger, H. In vivo tracing of indium-111 oxine-labeled human peripheral blood mononuclear cells in patients with lymphatic malignancies. J. Nucl. Med., 30:1005-1011, 1989. 23. Mackensen, A., Krause, T., Blum, U., Uhrmeister, P., Mertelsmann, R., and Lindemann, A. Homing of intravenously and intralymphatically in- jected human dendritic cells generated in vitro from CD34+ hematopoietic progenitor cells. Cancer Immunol. Immunother., 48:118-122, 1999. 24. Kawakami, Y., Robbins, P. F., Wang, X., Tupesis, J. P., Parkhurst, M. R., Kang, X., Sakaguchi, K., Appella, E., and Rosenberg, S. A. Identification of new melanoma epitopes on melanosomal proteins recognized by tumor infiltrating T lymphocytes restricted by HLA-A1, -A2, and -A3 alleles. J. Immunol., 161: 6985-6992, 1998.
25. Romero, P., Gervois, N., Schneider, J., Escobar, P., Valmori, D., Pannetier, C., Steinle, A., Wolfel, T., Lienard, D., Brichard, V., Van Pel, A., Jotereau, F., and Cerottini, J. C. Cytolytic T lymphocyte recognition of the immunodominant HLA-A*0201-restricted Melan-A/MART- t an- tigenic peptide in melanoma. J. Immunol., 159: 2366-2374, 1997. 26. Valmori, D., Fonteneau, J. F., Lizana, C. M., Gervois, N., Lienard, D., Rimoldi, D., Jongeneel, V., Jotereau, F., Cerottini, J. C., and Ro- mero, P. Enhanced generation of specific tumor-reactive CTL in vitro by selected Melan-A/MART-1 immunodominant peptide analogues. J. Im- munol., 160: 1750-1758, 1998. 27. Skipper, J. C., Gulden, P. H., Hendrickson, R. C., Harthun, N., Cald- well, J. A., Shabanowitz, J., Engelhard, V. H., Hunt, D. F., and Slingluff, C. L. J. Mass-spectrometric evaluation of HLA-A*0201-associated pep- tides identifies dominant naturally processed forms of CTL epitopes from MART-1 and gpl00. Int. J. Cancer, 82: 669-677, 1999. 28. de Vries, T. J., Fourkour, A., Wobbes, T., Verkroost, G., Ruiter, D. J., and van Muijen, G. N. Heterogeneous expression of immunother- apy candidate proteins gpl00, MART-l, and tyrosinase in human mel- anoma cell lines and in human melanocytic lesions. Cancer Res., 57: 3223-3229, 1997. 29. Sarantou, T., Chi, D. D., Garrison, D. A., Conrad, A. J., Schmid, P., Morton, D. L., and Hoon, D. S. Melanoma-associated antigens as messenger RNA detection markers for melanoma. Cancer Res., 57: 1371-1376, 1997. 30. Smith, B., Selby, P., Southgate, J., Pittman, K., Bradley, C., and Blair, G. E. Detection of melanoma cells in peripheral blood by means of reverse transcriptase and polymerase chain reaction. Lancet, 338: 1227-1229, 1991. 31. Hoon, D. S., Wang, Y., Dale, P. S., Conrad, A. J., Schmid, P., Garrison, D., Kuo, C., Foshag, L. J., Nizze, A. J., and Morton, D. L. Detection of occult melanoma cells in blood with a multiple-marker polymerase chain reaction assay. J. Clin. Oncol., 13:2109-2116, 1995. 32. Romani, N., Reider, D., Heuer, M., Ebner, S., K~impgen, E., Eibl, B., Niederwieser, D., and Schuler, G. Generation of mature dendritic cells from human blood. An improved method with special regard to clinical applicability. J. Immunol. Methods, 196:137-151, 1996. 33. Rieser, C., B6ck, G., Klocker, H., Bartsch, G., and Thurnher, M. Prostaglandin E2 and tumor necrosis factor c~ cooperate to activate human dendritic cells: synergistic activation of interleukin 12 produc- tion. J. Exp. Med., 186: 1603-1608, 1997. 34. Nazaruk, R. A., Rochford, R., Hobbs, M. V., and Cannon, M. J. Functional diversity of the CD8 + T-cell response to Epstein-Barr virus (EBV): implications for the pathogenesis of EBV-associated lympho- proliferative disorders. Blood, 91: 3875-3883, 1998. 35. Wei, C., Willis, R. A., Tilton, B. R., Looney, R. J., Lord, E. M., Barth, R. K., and Frelinger, J. G. Tissue-specific expression of the
human prostate-specific antigen gene in transgenic mice: implications for tolerance and immunotherapy. Proc. Natl. Acad. Sci. USA, 94: 6369-6374, 1997.
36. Nishimura, T., Iwakabe, K., Sekimoto, M., Ohmi, Y., Yahata, T., Nakui, M., Sato, T., Habu, S., Tashiro, H., Sato, M., and Ohta, A. Distinct role of antigen-specific T helper type 1 (Thl) and Th2 cells in tumor eradication in vivo. J. Exp. Med., 190: 617-627, 1999.
37. Shimizu, K., Okamoto, Y., Miyao, Y., Yamada, M., Ushio, Y., Hayakawa, T., Ikeda, H., and Mogami, H. Adoptive immunotherapy of human meningeal gliomatosis and carcinomatosis with LAK cells and recombinant interleukin-2. J. Neurosurg., 66: 519-521, 1987.
38. Heimans, J. J., Wagstaff, J., Schreuder, W. O., Wolbers, J. G., Baars, J. W., Polman, C. H., Scharenberg, J. G., Scheper, R. J., Palmer, P. A., and Franks, C. R. Treatment of leptomeningeal carcinomatosis with continuous intraventricular infusion of recombinant interleukin-2. Surg. Neurol., 35: 244-247, 1991.
39. List, J., Moser, R. P., Steuer, M., Loudon, W. G., Blacklock, J. B., and Grimm, E. A. Cytokine responses to intraventricular injection of interleukin 2 into patients with leptomeningeal carcinomatosis: rapid induction of tumor necrosis factor e~, interleukin 113, interleukin 6, ",/-interferon, and soluble interleukin 2 receptor (M, 55,000 protein). Cancer Res., 52:1123-1128, 1992.
40. Samlowski, W. E., Park, K. J., Galinsky, R. E., Ward, J. H., and Schumann, G. B. Intrathecal administration of interleukin-2 for menin- geal carcinomatosis due to malignant melanoma: sequential evaluation of intracranial pressure, cerebrospinal fluid cytology, and cytokine in- duction. J. Immunother., 13: 49-54, 1993. 41. Herrlinger, U., Weller, M., and Schabet, M. New aspects of immuno- therapy of leptomeningeal metastasis. J. Neurooncol., 38: 233-239, 1998. 42. Savas, B., Arslan, G., Gelen, T., Karpuzoglu, G., and Ozkaynak, C. Multidrug resistant malignant melanoma with intracranial metastasis responding to immunotherapy. Anticancer Res., 19: 4413-4420, 1999. 43. Tsurushima, H., Liu, S. Q., Tuboi, K., Matsumura, A., Yoshii, Y., Nose, T., Saijo, K., and Ohno, T. Reduction of end-stage malignant glioma by injection with autologous cytotoxic T lymphocytes. Jpn. J. Cancer Res., 90: 536-545, 1999.
44. Moore, K. W., O'Garra, A., de Waal Malefyt, R., Vieira, P., and Mosmann, T. R. Interleukin-10. Annu. Rev. Immunol., I1:165-190, 1993. 45. Salazar-Onfray, F., Charo, J., Petersson, M., Freland, S., Noffz, G., Qin, Z., Blankenstein, T., Ljunggren, H. G., and Kiessling, R. Down- regulation of the expression and function of the transporter associated with antigen processing in murine tumor cell lines expressing IL-10. J. Immunol., 159: 3195-3202, 1997. 46. de Waal Matefyt, R., Haanen, J., Spits, H., Roncarolo, M. G., te Velde, A., Figdor, C., Johnson, K., Kastelein, R., Yssel, H., and de Vries, J. E. Interleukin 10 (IL-10) and viral 1L-10 strongly reduce antigen-specific human T cell proliferation by diminishing the antigen-presenting capacity of monocytes via downregulation of class 1i major histocompatibility com- plex expression. J. Exp. Med., 174: 915-924, 1991.
47. Matsuda, M., Salazar, F., Petersson, M., Masucci, G., Hansson, J., Pisa, P., Zhang, Q. J., Masucci, M. G., and Kiessling, R. Interleukin 10 pretreatment protects target cells from tumor- and allo specific cytotoxic T cells and downregulates HLA class I expression. J. Exp. Med., 180: 2371-2376, 1994. 48. Santin, A. D., Hermonat, P. L., Ravaggi, A., Bellone, S., Pecorelli, S., Roman, J. J., Parham, G. P., and Cannon, M. J. Interleukin-10 increases Thl cytokine production and cytotoxic potential in human papillomavirus-specific CD8 § cytotoxic T lymphocytes. J. Virol., 74: 4729-4737, 2000.
49. Foon, K. A., Lutzky, J., Baral, R. N., Yannelli, J. R., Hutchins, L., Teitelbaum, A., Kashala, O. L., Das, R., Garrison, J., Reisfeld, R. A., and Bhattacharya-Chatterjee, M. Clinical and immune re- sponses in advanced melanoma patients immunized with an anti- idiotype antibody mimicking disialoganglioside GD2. J. Clin. Oncol., 18: 376-384, 2000.
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
2001;7:917s-924s. Clin Cancer Res Annette R. Clemons-Miller, Gurkamal S. Chatta, Laura Hutchins, et al. Leptomeningeal MelanomaIntrathecal Cytotoxic T-Cell Immunotherapy for Metastatic
Updated version
http://clincancerres.aacrjournals.org/content/7/3/917s
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/7/3/917sTo request permission to re-use all or part of this article, use this link
Research. on July 7, 2018. © 2001 American Association for Cancerclincancerres.aacrjournals.org Downloaded from