intramyofiber metastasis in skeletal muscle
TRANSCRIPT
Journal of Surgical Oncology 30:103-105 (1985)
lntramyofiber Metastasis in Skeletal Muscle
DEBA P. SARMA, MD, THOMAS C. WEILBAECHER, MD, AND CORDON L. LOVE, MD
From the Department of Pathology, Veterans Administration Medical Center and Louisiana State University Medical School, New Orleans
Malignant epithelial cells were noted within the sarcolemmal sheath of skeletal muscle fibers in a case of recurrent laryngeal carcinoma. Litera- ture is reviewed to evaluate the diagnostic and prognostic significance of this rare intramyofiber skeletal metastasis by cancer cells.
KEY WORDS: skeletal muscle metastasis, intramyofiber skeletal muscle metastasis, sarcolemmal invasion by tumor cells, metastatic skeletal muscle tumor
INTRODUCTION the invaded muscle. The interstitium in this area was free Skeletal muscle may be invaded by malignant tumors Of tumor Or inflammatory
usually by direct extension. Rarely does a patient clini- tally present with a metastatic tumor in the skeletal mus- Of various Organs and bone did not Yield
A work-up chest roentgenograms and evidence Of
cle [Sarma et al, 19811. Tumor cells usually invade the metastatic disease* interstitial tissues and the lymphatics between the muscle The patient underwent a hyPOpharyngectomy and fibers. A very rare form of invasion of the skeletal proximal muscle is a direct invasion of the individual muscle fibers
esophagectomy with placement Of
feeding jejunostomy tube and gastrostomy. The PoStoP- erative course was uneventful. Two months later, the patient remained free of recurrent or metastatic tumor.
DISCUSSION showing
intramyofiber metastasis. Carcinomas have shown this peculiar form of muscle invasion more commonly than the sarcomas, lymphomas, and leukemias. The breast
to show intramyofiber invasion. Intramyofiber
laryngectomy, right radical neck dissection, and irradia- lymphatic spread. The exact mechanism through which
elucidated from the human cases. However, Carr and strictures that were treated by dilatation.
and extension within the sarcolemmal sheaths. where we
noted an intramyofiber skeletal muscle metastasis and to review the literature to clarify the mechanism and signif- icance of this type of muscle metastasis.
The purpose of this paper is to report a
Table I lists the reports of various
CASE REPORT
complaint of pain in the mid-neck and difficulty in swab A 60-year-old man was admitted to the hospital with a carcinomas appear to be the most commonly
lowing. The Patient had had squamous the larynx l2 Years PreviouslY, which was treated
carcinoma Of invasion by malignant cells appears to be part of a local invasion, rather than part of a distant hematogenous or
There were Occurrences Of the malignant cells enter the myofibers has not been
a fungating lesion in the hY- associates [ 19661, in an elaborate experimental study a recurrent poorly using electron microscopy, have shown that Rd/3 tumor
EsoPhagoscoPY popharynx7 a biopsy Of which
cells in rats directly invade the muscle syncytia, often differentiated squamous cell carcinoma. The malignant epithelial cells had invaded the skeletal accompanied by macrophages and polymorphs.
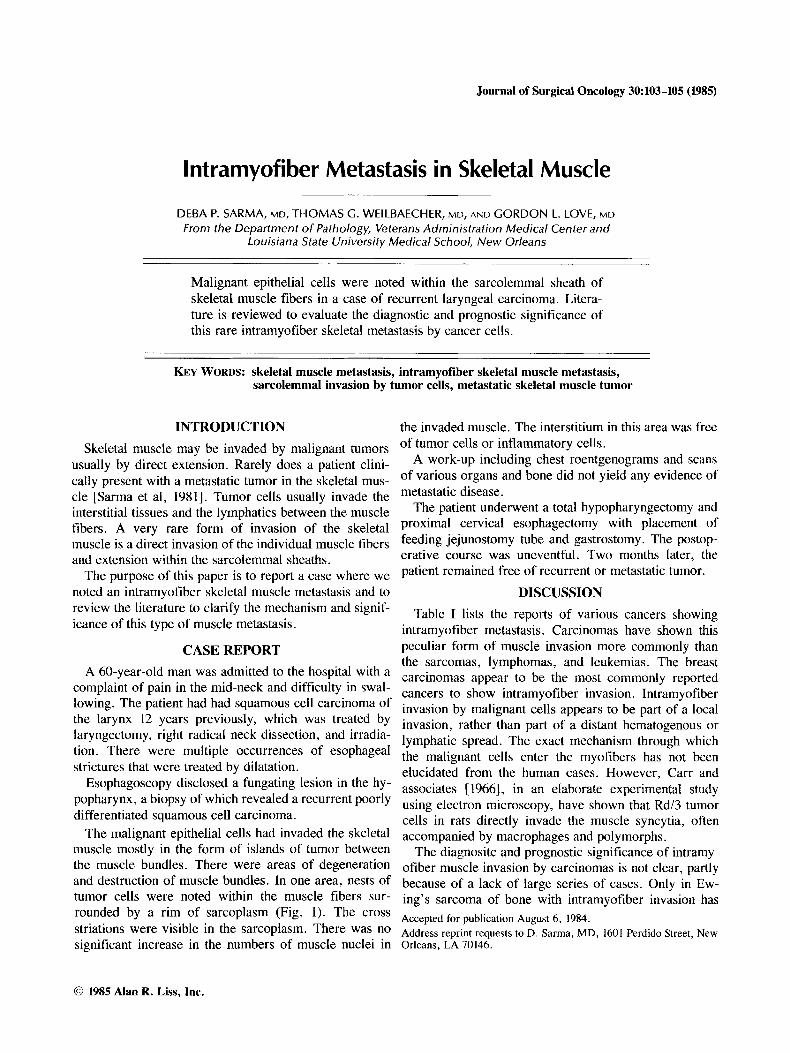
muscle mostly in the form Of islands Of tumor between The diagnositc and prognostic significance of intramy- the bundles. There were areas of degeneration ofiber muscle invasion by carcinomas is not clear, partly and destruction of muscle bundles. In one area, nests of because of a lack of large series of cases. Only in E ~ - tumor cells were noted within the muscle fibers sur- ing's Sarcoma of bone with intramyofiber invasion has
striations were in the sarcoplasm- There was no Address reprint requests to D. Sarma, MD, 1601 Perdido Street, New significant increase in the numbers of muscle nuclei in Orleans, LA 70146.
rounded by a rim Of sarcoplasm (Fig' '1' The cross Accepted for publication August 6, 1984,
0 1985 Alan R. Liss, Inc.
104 Sarma, Weilbaecher, and Love
Fig. 1. Intramyofiber skeletal muscle metastasis by poorly differentiated squamous cell carcinoma of the larynx (H & E, X 280).
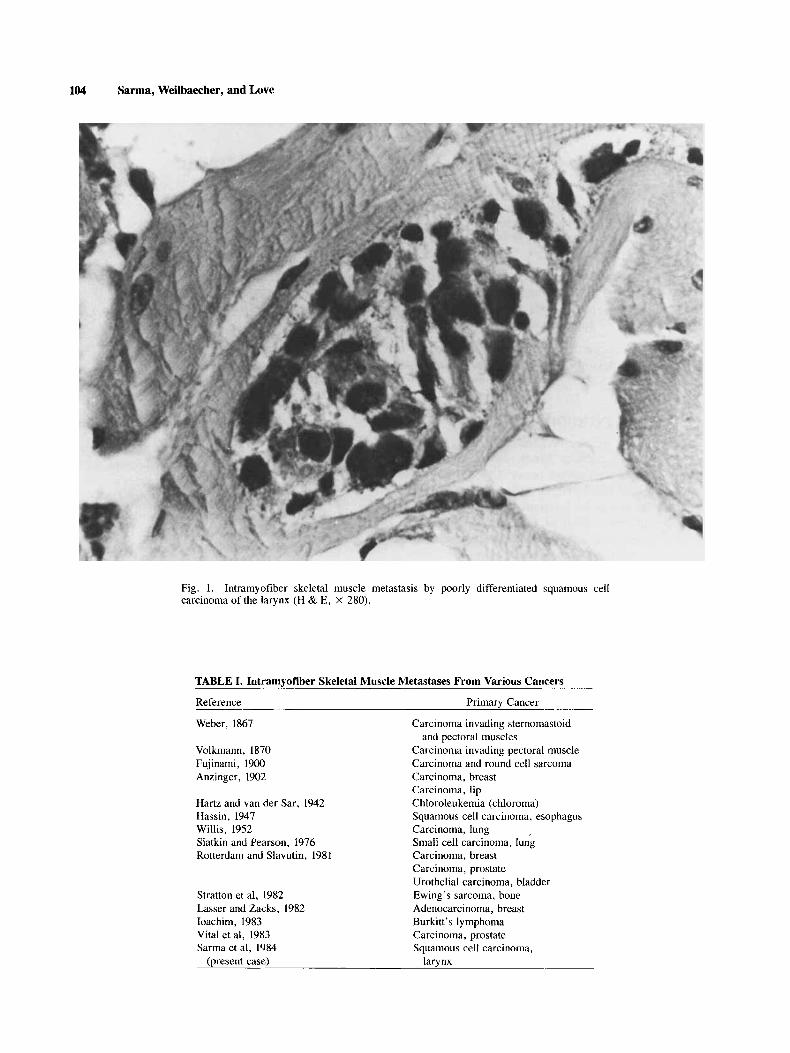
TABLE I. Intramyofiber Skeletal Muscle Metastases From Various Cancers
Reference Primary Cancer
Weber. 1867
Volkmann, 1870 Fujinami, 1900 Anzinger, 1902
Hartz and van der Sar, 1942
Carcinoma invading sternomastoid
Carcinoma invading pectoral muscle Carcinoma and round cell sarcoma Carcinoma, breast Carcinoma, lip Chloroleukemia (chloroma)
and pectoral muscles
Hassin, 1947 Willis, 1952 Carcinoma, lung Slatkin and Pearson, I976 Rotterdam and Slavutin, 1981
Squamous cell carcinoma, esophagus
Small cell carcinoma, lung Carcinoma, breast Carcinoma, prostate Urothelial carcinoma, bladder
Stratton et al, 1982 Ewing’s sarcoma, bone Lasser and Zacks, 1982 Adenocarcinoma, breast Ioachim, 1983 Burkitt’s lymphoma Vital et al, 1983 Carcinoma, prostate Sarma et al, 1984 Squamous cell carcinoma,
(present case) larynx
Intramyofiber Muscle Metastasis 105
an increased development of metastasis and decreased survival been noted [Stratton et al, 19821. It has been recommended that intramyofiber skeletal muscle inva- sion should be looked for and reported while examining the cases of Ewing’s sarcoma with extension into soft tissue [Siegal, 19841.
ACKNOWLEDGMENTS We thank Ms. Laura White for excellent secretarial
assistance.
REFERENCES Anzinger FP: The changes occurring in striped muscle in the neigh-
bourhood of malignant tumors. Am J Med Sci 123:268-284, 1902. Carr I, McGinty F, Norris P: The fine structure of neoplastic inva-
sion: Invasion of liver, skeletal muscle and lymphatic vessels by the Rd/3 tumour. J Pathol 118:91-99, 1966.
Fujinami A: Ueber das histologische Verhalten des quergestreiften Muskels an der Grenze bosartiger Geschwulste. Arch Path Anat
Hartz PH, van der Sar A: Chloroleukemia. Report of a case with special reference to its neoplastic nature. Am J Pathol 18:715-727, 1942.
Hassin GB: Carcinoma of muscle tissue as a cause of laryngeal paralysis. J Neuropathol Exp Neurol6:358-368, 1947.
16: 115-158, 1900.
Ioachim HL: Tumor cells within skeletal muscle cells (letter). Hum Pathol 14:923-924, 1983.
Lasser A, Zacks SI: Intraskeletal myofiber metastasis of breast carci- noma. Hum Pathol 13:104-1046, 1982.
Rotterdam H, Slavutin L: Secondary tumors of soft tissues: An au- topsy study. In Fenoglio CM, Wolff M (eds): “Progress in Sur- gical Pathology,” Vol 111. New York: Masson Publishing, 1981,
Sarma DP, Kovac A, Socorro N: Metastatic carcinoma of the skeletal muscle. South Med J 74:484-485, 1981.
Siegal GP: Intramyofiber skeletal muscle invasion in Ewing’s sar- coma of bone: Clinicopathologic observations from the intergroup Ewing’s sarcoma study (editorial comment). In Brinkhous KM (ed): “The Yearbook of Pathology and Clinical Pathology.” Chi- cago: Yearbook Medical Publishers, 1984, pp 200-201.
Slatkin DN, Pearson J: Intramyofiber metastases in skeletal muscle. Hum Pathol 7:347-349, 1976.
Stratton B, Askin FB, Kissane J M: Intramyofiber skeletal muscle invasion in Ewing’s sarcoma of bone: Clinicopathologic observa- tions from the intergroup Ewing’s sarcoma study. Am J Pediatr Hematol Oncol4:231-235, 1982.
Vital C, Rive1 J, Fournier M: Intramyofiber metastases in skeletal muscle (letter). Hum Pathol 14: 1012, 1983.
Volkmann R: Zur histologic des muskelkrebses. Arch Path Anat 50543, 1870 (cited by Anzinger, 1902).
Weber 0: Arch Path Anat 39: 1867 (cited by Anzinger, 1902). Willis RA: “The Spread of Tumors in the Human Body.” London:
147- 169.
Butterworth and Co., 1952, pp 284-285.