intheclinict multiplesclerosis
TRANSCRIPT

In the ClinicT
Multiple SclerosisMany groundbreaking advances have
occurred in the field of multiple sclerosissince this series last reviewed the disorder
in 2014. The U.S. Food and Drug Administrationhas approved 7 new medications for relapsing–remitting multiple sclerosis and approved the firstmedication for primary progressive multiple sclero-sis. The McDonald criteria for diagnosing multiplesclerosis were updated in 2017. New blood testscan now differentiate patients with multiple sclero-sis from those with neuromyelitis optica spectrumdisorder, and 3 new medications have been app-roved specifically for the latter disorder. Also, newmedications for treating the symptoms of multiplesclerosis have been introduced.
CME/MOC activity available at Annals.org.
Physician WriterMichael J. Olek, DOTouro University Nevada,Henderson, Nevada
doi:10.7326/AITC202106150
This article was published at Annals.org on 8 June 2021.
CME Objective: To review current evidence for diagnosis and treatment ofmultiple sclerosis.
Funding Source: American College of Physicians.
Acknowledgment: The author thanks Daniel M. Harrison, MD, author of theprevious version of this In the Clinic.
Disclosures: Dr. Olek, ACP Contributing Author, reports that he is the first authorof the chapter on multiple sclerosis in UpToDate. Disclosures can also be viewedat www.acponline.org/authors/icmje/ConflictOfInterestForms.do?msNum=M21-0830.
With the assistance of additional physician writers, the editors of Annals ofInternal Medicine develop In the Clinic using MKSAP and other resources ofthe American College of Physicians. The patient information page was written byMonica Lizarraga from the Patient and Interprofessional Partnership Initiative atthe American College of Physicians.
In the Clinic does not necessarily represent official ACP clinical policy. For ACPclinical guidelines, please go to https://www.acponline.org/clinical_information/guidelines/.
© 2021 American College of Physicians
Diagnosis
Treatment
COVID-19 andMultiple Sclerosis
Annals of Internal MedicineT

Multiple sclerosis is an autoim-mune condition that results ininflammatory damage to the cen-tral nervous system (CNS). Thepathologic hallmarks are diffuseand focal areas of inflammation,demyelination, gliosis, and neuro-nal injury in the optic nerves,brain, and spinal cord. In additionto affecting white matter tracts,multiple sclerosis results in injuryto the cortical and deep gray mat-ter. The neurologic symptoms anddisability that patients experienceare a direct consequence of thesepathologic processes, resulting inacute and chronic disruption ofwhite matter tracts and gray mat-ter structures.
Multiple sclerosis is the most com-mon nontraumatic cause of neuro-logic disability in persons youngerthan 40 years. In 2010, the esti-mated prevalence in the UnitedStates was 309.2 per 100000 per-sons, or 727433 adults (1). Itoccurs in a female–male ratio of2.8 to 1 (1).
The cause of multiple sclerosis ismultifactorial and is probably thecumulative result of multiplegenetic and environmental riskfactors. Studies have shown
concordance rates between 20%and 30% in monozygotic twinsand between 2% and 3% in dizy-gotic twins (2). Genome-wideassays have identified risk allelesin the genes for major histocom-patibility complex, interleukin-2receptor, and interleukin-7 recep-tor, among others (3,4). Geo-graphic location of residencebefore adolescence also predictsrisk, with increased rates in north-ern and southern latitudes com-pared with equatorial areas. Thismay be related to the observationthat persons with vitamin D defi-ciency seem to have increasedrisk for multiple sclerosis. Becauseultraviolet radiation to the skin isthe major source of vitamin D syn-thesis, vitamin D deficiency ismore common among personsliving in regions with low levels ofseasonal sunlight (5). Risk mayalso be influenced by exposure orlack of exposure to infectiousagents because antibodiesagainst certain viruses, such asEpstein–Barr virus, are more fre-quently seen in patients with mul-tiple sclerosis than in thosewithout it (6).
DiagnosisWhat characteristic symptomsor physical findings shouldalert clinicians to the diagnosisof multiple sclerosis?
Symptoms typically occur as aconsequence of focal inflamma-tory plaques that cause functionalareas of neuronal loss or interrup-tion of critical axonal tracts. Inmost patients, focal lesions occurintermittently and acutely, leadingto a “relapse” or “flare” in whichsymptoms evolve over the courseof days andmay last for weeks ormonths before improving, if theydo improve.
Because multiple sclerosis canaffect nearly any part of the CNS,
clinical presentations vary widely.Themost common initial clinicalmanifestations are the result ofinflammation of the optic nerve(optic neuritis), focal inflammationwithin the spinal cord (myelitis),and brainstem or cerebellarlesions. Each of these is termed aclinically isolated syndrome (CIS).Optic neuritis often presents withsubacute vision changes that varyfrom blindness to a central sco-toma or a horizontal oval scotomaembracing both the fixation pointand the blind spot (centrocecalscotoma)—predominantly in 1 eye(90%) and rarely in both eyes(10%)—along with pain during eye
1. Wallin MT, Culpepper WJ,Campbell JD, et al; USMultiple SclerosisPrevalence Workgroup. Theprevalence of MS in theUnited States: a popula-tion-based estimate usinghealth claims data.Neurology. 2019;92:e1029-e1040. [PMID:30770430]
2. Islam T, Gauderman WJ,Cozen W, et al. Differentialtwin concordance for multi-ple sclerosis by latitude ofbirthplace. Ann Neurol.2006;60:56-64. [PMID:16685699]
3. Patsopoulos NA, BarcellosLF, Hintzen RQ, et al;IMSGC. Fine-mapping thegenetic association of themajor histocompatibilitycomplex in multiple sclero-sis: HLA and non-HLAeffects. PLoS Genet.2013;9:e1003926. [PMID:24278027]
4. Beecham AH, PatsopoulosNA, Xifara DK, et al;International MultipleSclerosis GeneticsConsortium (IMSGC).Analysis of immune-relatedloci identifies 48 new sus-ceptibility variants for mul-tiple sclerosis. Nat Genet.2013;45:1353-60. [PMID:24076602]
5. Sintzel MB, Rametta M,Reder AT. Vitamin D andmultiple sclerosis: a com-prehensive review. NeurolTher. 2018;7:59-85.[PMID: 29243029]
6. Lassmann H, Niedobitek G,Aloisi F, et al;NeuroproMiSe EBVWorking Group. Epstein–Barr virus in the multiplesclerosis brain: a controver-sial issue—report on afocused workshop held inthe Centre for BrainResearch of the MedicalUniversity of Vienna,Austria. Brain.2011;134:2772-86. [PMID:21846731]
7. de la Cruz J, KupersmithMJ.. Clinical profile ofsimultaneous bilateraloptic neuritis in adults. Br JOphthalmol. 2006;90:551-4. [PMID: 16622084]
8. Thompson AJ, Banwell BL,Barkhof F, et al. Diagnosisof multiple sclerosis: 2017revisions of the McDonaldcriteria. Lancet Neurol.2018;17:162-73. [PMID:29275977]
9. O’Riordan JI, Thompson AJ,Kingsley DP, et al. Theprognostic value of brainMRI in clinically isolatedsyndromes of the CNS. A10-year follow-up. Brain.1998;121:495-503. [PMID:9549525]
10. Weinshenker BG, Bass B,Rice GP, et al. The naturalhistory of multiple sclero-sis: a geographicallybased study. I. Clinicalcourse and disability.Brain. 1989;112:133-46.[PMID: 2917275]
© 2021 American College of Physicians ITC2 In the Clinic Annals of Internal Medicine

movement (7). Ocular examina-tion usually reveals a reduction invisual acuity, a visual field deficit,and a decreased ability to differ-entiate colors. Examination of thepupil in patients with unilateraloptic neuritis reveals paradoxicaldilation of the pupil in the affectedeye when light is rapidly andrepeatedly shifted from one eyeto the other (afferent pupillarydefect). If the anterior portion ofthe optic nerve is involved, fundu-scopic examination may alsoreveal inflammatory changes ofthe optic disc (papillitis).
Myelitis usually manifests as sen-sory or motor symptoms belowthe affected spinal level, and ex-amination often reveals focal mus-cle weakness and reducedsensation in the same distribution.Muscles can be flaccid in theacute setting, but spasticity devel-ops over time in patients who donot recover completely from theattack. Unlike other spinal cordprocesses, multiple sclerosistends to cause a partial myelitis,so symptoms similar to a full-cordtransection are exceedingly rare.Some patients may also have atight, band-like sensation aroundthe chest or abdomen during theacute inflammatory process;shock-like sensations radiatingdown the spine or limbs inducedby neck movements (Lhermittesign); and urinary frequency, uri-nary urgency, or urine retention.
Disruption of vestibular or cere-bellar pathways can lead to ataxiaand vertigo. Examination can alsofind impaired ability to performsmoothly coordinated voluntarymovements of the limbs or trunk(appendicular or truncal ataxia),dysmetria on finger-to-nose test-ing, and dysfunction during tan-dem gait. Brainstem involvementcan lead to eye movement abnor-malities that cause symptoms ofdiplopia or a sensation of jerkingof the visual field (oscillopsia).
Oculomotor examination can alsofind disconjugate eyemovements,nystagmus, or an inability toadduct 1 eye with nystagmus inthe abducting eye (internuclearophthalmoplegia).
In addition to the developmentof acute or subacute focal symp-toms, patients with multiple scle-rosis may have chronic symptomsdue to widespread cortical demy-elination and global brain atro-phy. Commonmanifestationsinclude cognitive dysfunction andmental and physical fatigue.
Many patients with multiple scle-rosis also have transient worsen-ing of baseline neurologicsymptoms when body tempera-ture is elevated (Uhthoff phenom-enon) because electricalmessages travel more slowly overareas with demyelination-relatedinjury when temperature isincreased. These events aresometimes termed “pseudo-relapses.” Theymust be differenti-ated from true relapses becausethey do not represent new inflam-matory events; do not requiredirect treatment; and typicallyresolve in cooler temperatures orafter resolution of fever and infec-tion, which usually indicates anasymptomatic urinary tract infec-tion. If the elevated temperature isdue to an infection, it is evenmoreimportant to distinguish a pseudo-relapse from a true relapsebecause antibiotics are indicatedand steroids may make the infec-tion worse.
What are the characteristicsof each subtype of multiplesclerosis?The time course of symptom onsetand the evolution of symptomsdetermine the clinical subtype ofmultiple sclerosis, and this is im-portant for choosing the correctdisease-modifying therapy (DMT).For example, it is important to dif-ferentiate relapsing–remittingmul-tiple sclerosis (RRMS) from primary
11. Kremenchutzky M, RiceGP, Baskerville J, et al.The natural history ofmultiple sclerosis: ageographically basedstudy 9: observations onthe progressive phase ofthe disease. Brain.2006;129:584-94.[PMID: 16401620]
12. Filippi M, Rocca MA,Ciccarelli O, et al;MAGNIMS Study Group.MRI criteria for the diag-nosis of multiple sclero-sis: MAGNIMSconsensus guidelines.Lancet Neurol.2016;15:292-303.[PMID: 26822746]
13. Bakshi R, Thompson AJ,Rocca MA, et al. MRI inmultiple sclerosis: cur-rent status and futureprospects. LancetNeurol. 2008;7:615-25.[PMID: 18565455]
14. Stangel M, Fredrikson S,Meinl E, et al. The utilityof cerebrospinal fluidanalysis in patients withmultiple sclerosis. NatRev Neurol.2013;9:267-76. [PMID:23528543]
15. Gronseth GS, AshmanEJ. Practice parameter:the usefulness of evokedpotentials in identifyingclinically silent lesionsin patients with sus-pected multiple sclerosis(an evidence-basedreview): report of theQuality StandardsSubcommittee of theAmerican Academy ofNeurology. Neurology.2000;54:1720-5.[PMID: 10802774]
16. Costello F, Burton JM.Retinal imaging with op-tical coherence tomogra-phy: a biomarker inmultiple sclerosis. EyeBrain. 2018;10:47-63.[PMID: 30104912]
17. Garcia-Martin E, PabloLE, Herrero R, et al.Diagnostic ability of alinear discriminant func-tion for spectral-domainoptical coherence to-mography in patientswith multiple sclerosis.Ophthalmology.2012;119:1705-11.[PMID: 22480742]
18. Solomon AJ, NaismithRT, Cross AH.Misdiagnosis of multiplesclerosis: impact of the2017 McDonald criteriaon clinical practice.Neurology. 2019;92:26-33. [PMID: 30381369]
19. Jarius S, Wildemann B.The history of neuromye-litis optica. JNeuroinflammation.2013;10:8. [PMID:23320783]
20. Wallach AI, Tremblay M,Kister I. Advances in thetreatment of neuromye-litis optica spectrum dis-order. Neurol Clin.2021;39:35-49. [PMID:33223088]
Annals of Internal Medicine In the Clinic ITC3 © 2021 American College of Physicians

progressive multiple sclerosis(PPMS) and secondary progressivemultiple sclerosis (SPMS).
Approximately 85% of patientswith multiple sclerosis initiallyhave RRMS, in which neurologicsymptoms appear as repeatedepisodes of relapse followed byrecovery. Patients who do notmeet the full criteria for multiplesclerosis when they have their firstevent are said to have had a CIS.Because DMTs can extend thetime from the first clinical event tothe second event, it is importantto correctly identify patients whohave RRMS or have a high likeli-hood of having the diagnosis con-firmed at a later date, which is whyspecific diagnostic criteria are soimportant (8). For example, peo-ple who have an acute demyeli-nating attack, such as opticneuritis or partial myelitis withbrain lesions onmagnetic reso-nance imaging (MRI) scans, have a10-year risk of approximately 90%for eventually meeting criteria formultiple sclerosis. In contrast,those who have a similar eventwithout brain lesions have a risk ofapproximately 10% to 20% (9).
The symptoms of an individualrelapse tend to peak after a fewdays or weeks. A period of recov-ery follows that may last weeks ormonths. During the first few years,many patients experience signifi-cant recovery of previous function-ing. However, as time passes andmore relapses occur, the amountof recovery from each relapsediminishes and permanent disabil-ity can occur. In approximately50% to 60% of patients with RRMS,relapses become infrequent orcease completely after a median of10 to 15 years, but neurologic defi-cits continue to accrue in a slowlyprogressive manner (10). Thisstage of multiple sclerosis istermed secondary progressivemultiple sclerosis.
Approximately 15% of patientswith multiple sclerosis have steadyaccumulation of progressive
disability from the time of diseaseonset, with only a rare relapse. Thissubtype is termed primary pro-gressive multiple sclerosis, and itoften presents later in life, with thefirst symptoms typically occurringin the fifth or sixth decade. Theaccumulation of disability canoccur rapidly. Early studies of thenatural history of this subtype impli-cated sex and age at onset as pre-dictors of rapid progression, butrecent studies support only accrualof early disability as a predictor oflong-term progression rates (11).
What are the McDonaldcriteria, and how can they helpclinicians diagnose multiplesclerosis?Confirming the diagnosis of multi-ple sclerosis requires a full assess-ment of clinical symptoms,physical examination, testing, andconsideration of other conditionsin the differential diagnosisbecause diagnostic biomarkersfor this condition do not exist. The2017McDonald criteria are widelyaccepted as the best way to inte-grate the different types of evi-dence (8). For example, toestablish a diagnosis of multiplesclerosis, the McDonald criteriamay require 2 relapses plus 2objective signs over time or 1relapse (as a CIS) plus 2 clinicalsigns plus specific MRI findings(12). There also must be no betterexplanation for the patient'ssymptoms, clinical findings, andMRI findings. The McDonald crite-ria are readily available online (forexample, at www.aan.com).Although clinical research studiesusually adhere strictly to theMcDonald criteria, manyspecialists use them in individualpatients more as a guideline thanas strict criteria. For example, aclinician may diagnose possiblemultiple sclerosis and start a DMTeven though the patient does notmeet criteria because the tradeoffbetween risk and benefit favorsearly treatment.
21. Goldschmidt C, McGinleyMP. Advances in the treat-ment of multiple sclerosis.Neurol Clin. 2021;39:21-33. [PMID: 33223085]
22. Amato MP, Fonderico M,Portaccio E, et al. Disease-modifying drugs canreduce disability progres-sion in relapsing multiplesclerosis. Brain.2020;143:3013-24.[PMID: 32935843]
23. Buron MD, Chalmer TA,Sellebjerg F, et al. Initialhigh-efficacy disease-mod-ifying therapy in multiplesclerosis: a nationwidecohort study. Neurology.2020;95:e1041-e1051.[PMID: 32636328]
24. Polman CH, O’ConnorPW, Havrdova E, et al;AFFIRM Investigators. Arandomized, placebo-con-trolled trial of natalizumabfor relapsing multiplesclerosis. N Engl J Med.2006;354:899-910.[PMID: 16510744]
25. Bloomgren G, Richman S,Hotermans C, et al. Riskof natalizumab-associatedprogressive multifocal leu-koencephalopathy. N EnglJ Med. 2012;366:1870-80. [PMID: 22591293]
26. Reuwer AQ, Heron M, vander Dussen D, et al. Theclinical utility of JC virusantibody index measure-ments in the context ofprogressive multifocal leu-koencephalopathy. ActaNeurol Scand. 2017;136Suppl 201:37-44. [PMID:29068484]
27. Kolcava J, Hulova M,Benesova Y, et al. Thevalue of anti-JCV antibodyindex assessment in mul-tiple sclerosis patientstreated with natalizumabwith respect to demo-graphic, clinical and radio-logical findings. MultScler Relat Disord.2019;30:187-91. [PMID:30785075]
28. Lee P, Plavina T, Castro A,et al. A second-generationELISA (STRATIFY JCVTM
DxSelectTM) for detectionof JC virus antibodies inhuman serum and plasmato support progressivemultifocal leukoencephal-opathy risk stratification. JClin Virol. 2013;57:141-6. [PMID: 23465394]
29. Gold R, Kappos L, ArnoldDL, et al; DEFINE StudyInvestigators. Placebo-con-trolled phase 3 study oforal BG-12 for relapsingmultiple sclerosis. N EnglJ Med. 2012;367:1098-107. [PMID: 22992073]
30. Freeman L, Kee A, Tian M,et al. Evaluating treatmentpatterns, relapses, health-care resource utilization,and costs associated withdisease-modifying treat-ments for multiple sclero-sis in DMT-naïve patients.Clinicoecon OutcomesRes. 2021;13:65-75.[PMID: 33519217]
© 2021 American College of Physicians ITC4 In the Clinic Annals of Internal Medicine

TheMcDonald criteria can also beused to diagnose PPMS. These cri-teria require at least 1 year of pro-gressive neurologic disability plusat least 2 of the following: dissemi-nation in space on a brain MRIscan, dissemination in space on aspinal cord MRI scan, or cerebro-spinal fluid (CSF) findings consist-ent with multiple sclerosis.
Proper application of theMcDonald criteria can also helpdifferentiate multiple sclerosisfrom other conditions and thusprevent unnecessary neurologictesting and referrals. This is espe-cially true for common conditions,such asmigraine, microvascular is-chemic disease, and head trauma,which can cause white matterlesions onMRI scans but do notcause lesions that meet theMcDonald criteria for location.
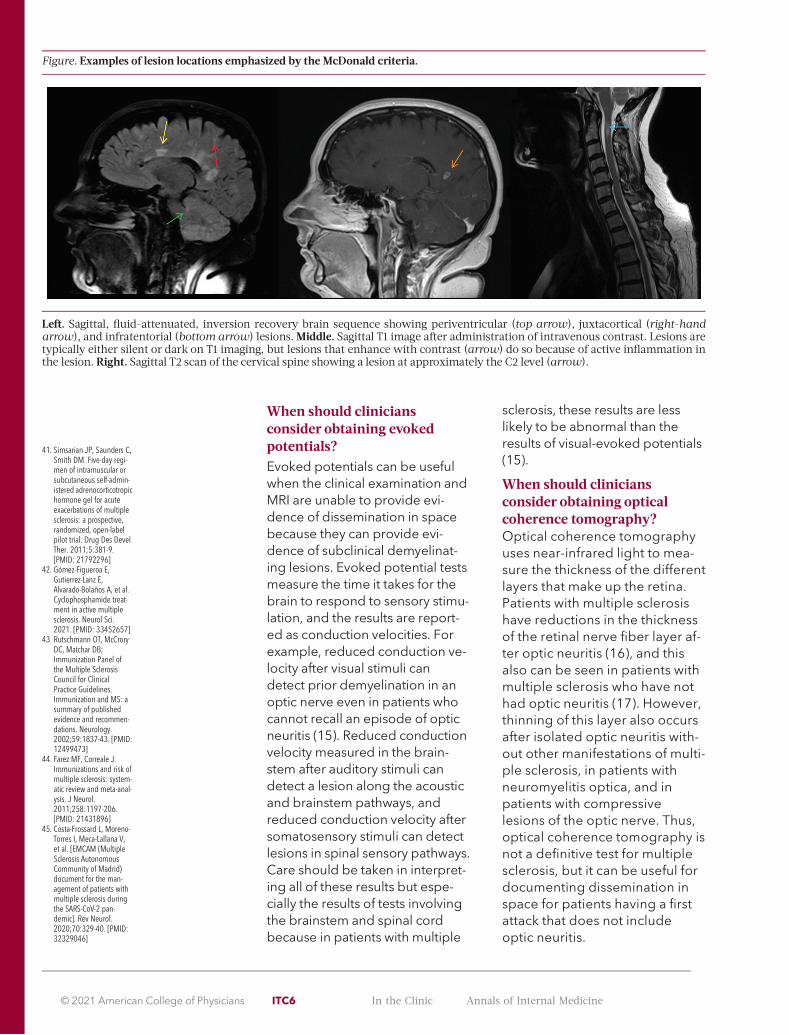
What is the role of MRI indiagnosis?MRI is the primary diagnostic andprognostic tool for the evaluationof patients with multiple sclerosis.For most patients, the McDonaldcriteria require confirmation withMRI findings. Typical MRI findingsare lesions in white matter regionsthat appear hyperintense on T2-weighted and fluid-attenuatedinversion recovery images andhypointense on T1-weightedimages. These lesions are areas ofdemyelination and gliosis. In addi-tion, administration of gadoliniumcontrast will enhance lesions thatare undergoing an active inflam-matory process with breakdownof the blood–brain barrier. TheFigure shows examples of lesionsin each of the 4 locations empha-sized by the McDonald criteria:periventricular, juxtacortical,brainstem and cerebellum (infra-tentorial), and spinal cord.Dissemination in space can bedemonstrated by characteristicT2-hyperintense lesions that arein 2 or more of the 4 locations.Dissemination in time can be
demonstrated by the simultane-ous presence of a gadolinium-enhancing lesion and a nonen-hancing lesion or by a new T2-hyperintense or gadolinium-enhancing lesion not present on abaseline scan, regardless of thetiming of the baseline scan.
Although diagnostic criteria focusspecifically on the presence oflesions in white matter, other MRIchanges can be seen, includingdemyelinating lesions in the cor-tex; atrophy of cortical and deepgray matter; atrophy of white mat-ter structure; and alterations inlesions and normal-appearingwhitematter indicated by magnet-ization transfer, diffusion tensorimaging, and other quantitativeMRI measures (13).
What role does lumbarpuncture play in diagnosis?
TheMcDonald criteria do notrequire testing of CSF to confirmthe diagnosis of RRMS. For the di-agnosis of PPMS, CSF testing isnecessary only if MRI findings donot meet criteria for disseminationin space. However, CSF testingcan be a useful diagnostic tool incases where the diagnosis is notclear. CSF testing with isoelectricfocusing finds unique oligoclonalbands in 90% to 95% of patientswith multiple sclerosis (14). Anelevation of the IgG index is seenin 50% to 75% of patients, andmild pleocytosis is seen in abouthalf of patients. Given the sensitiv-ity and specificity of these tests,negative CSF test results by them-selves cannot rule out the diagno-sis of multiple sclerosis. However,when negative CSF test resultsoccur in patients with a low suspi-cion for multiple sclerosis basedon clinical and radiologic findings,clinicians should consider otherpossible diagnoses and advisepatients that they probably do nothavemultiple sclerosis.
31. Boffa G, Massacesi L,Inglese M, et al; ItalianBMT-MS study group.Long-term clinical out-comes of hematopoieticstem cell transplantationin multiple sclerosis.Neurology. 2021.[PMID: 33472915]
32. Correale J, Ysrraelit MC,Gaitán MI. Gender dif-ferences in 1,25 dihy-droxyvitamin D3immunomodulatoryeffects in multiple scle-rosis patients andhealthy subjects. JImmunol.2010;185:4948-58.[PMID: 20855882]
33. Mowry EM, Waubant E,McCulloch CE, et al.Vitamin D status predictsnew brain magnetic res-onance imaging activityin multiple sclerosis.Ann Neurol.2012;72:234-40.[PMID: 22926855]
34. Simpson S Jr, Taylor B,Blizzard L, et al.. Higher25-hydroxyvitamin D isassociated with lowerrelapse risk in multiplesclerosis. Ann Neurol.2010;68:193-203.[PMID: 20695012]
35. Soilu-Hänninen M, AivoJ, Lindström BM, et al. Arandomised, doubleblind, placebo con-trolled trial with vitaminD3 as an add on treat-ment to interferon b-1bin patients with multiplesclerosis. J NeurolNeurosurg Psychiatry.2012;83:565-71.[PMID: 22362918]
36. Miclea A, Bagnoud M,Chan A, et al. A briefreview of the effects ofvitamin D on multiplesclerosis. FrontImmunol. 2020;11:781.[PMID: 32435244]
37. Runia TF, Hop WC, deRijke YB, et al. Lower se-rum vitamin D levels areassociated with a higherrelapse risk in multiplesclerosis. Neurology.2012;79:261-6. [PMID:22700811]
38. Ramo-Tello C, Grau-López L, Tintor�e M, et al.A randomized clinicaltrial of oral versus intra-venous methylpredniso-lone for relapse of MS.Mult Scler.2014;20:717-25.[PMID: 24144876]
39. Morrow SA, Stoian CA,Dmitrovic J, et al. The bi-oavailability of IV meth-ylprednisolone and oralprednisone in multiplesclerosis. Neurology.2004;63:1079-80.[PMID: 15452302]
40. Trebst C, Reising A,Kielstein JT, et al.Plasma exchange ther-apy in steroid-unrespon-sive relapses in patientswith multiple sclerosis.Blood Purif.2009;28:108-15.[PMID: 19521072]
Annals of Internal Medicine In the Clinic ITC5 © 2021 American College of Physicians
When should cliniciansconsider obtaining evokedpotentials?Evoked potentials can be usefulwhen the clinical examination andMRI are unable to provide evi-dence of dissemination in spacebecause they can provide evi-dence of subclinical demyelinat-ing lesions. Evoked potential testsmeasure the time it takes for thebrain to respond to sensory stimu-lation, and the results are report-ed as conduction velocities. Forexample, reduced conduction ve-locity after visual stimuli candetect prior demyelination in anoptic nerve even in patients whocannot recall an episode of opticneuritis (15). Reduced conductionvelocity measured in the brain-stem after auditory stimuli candetect a lesion along the acousticand brainstem pathways, andreduced conduction velocity aftersomatosensory stimuli can detectlesions in spinal sensory pathways.Care should be taken in interpret-ing all of these results but espe-cially the results of tests involvingthe brainstem and spinal cordbecause in patients with multiple
sclerosis, these results are lesslikely to be abnormal than theresults of visual-evoked potentials(15).
When should cliniciansconsider obtaining opticalcoherence tomography?Optical coherence tomographyuses near-infrared light to mea-sure the thickness of the differentlayers that make up the retina.Patients with multiple sclerosishave reductions in the thicknessof the retinal nerve fiber layer af-ter optic neuritis (16), and thisalso can be seen in patients withmultiple sclerosis who have nothad optic neuritis (17). However,thinning of this layer also occursafter isolated optic neuritis with-out other manifestations of multi-ple sclerosis, in patients withneuromyelitis optica, and inpatients with compressivelesions of the optic nerve. Thus,optical coherence tomography isnot a definitive test for multiplesclerosis, but it can be useful fordocumenting dissemination inspace for patients having a firstattack that does not includeoptic neuritis.
41. Simsarian JP, Saunders C,Smith DM. Five-day regi-men of intramuscular orsubcutaneous self-admin-istered adrenocorticotropichormone gel for acuteexacerbations of multiplesclerosis: a prospective,randomized, open-labelpilot trial. Drug Des DevelTher. 2011;5:381-9.[PMID: 21792296]
42. Gómez-Figueroa E,Gutierrez-Lanz E,Alvarado-Bolaños A, et al.Cyclophosphamide treat-ment in active multiplesclerosis. Neurol Sci.2021. [PMID: 33452657]
43. Rutschmann OT, McCroryDC, Matchar DB;Immunization Panel ofthe Multiple SclerosisCouncil for ClinicalPractice Guidelines.Immunization and MS: asummary of publishedevidence and recommen-dations. Neurology.2002;59:1837-43. [PMID:12499473]
44. Farez MF, Correale J.Immunizations and risk ofmultiple sclerosis: system-atic review and meta-anal-ysis. J Neurol.2011;258:1197-206.[PMID: 21431896]
45. Costa-Frossard L, Moreno-Torres I, Meca-Lallana V,et al. [EMCAM (MultipleSclerosis AutonomousCommunity of Madrid)document for the man-agement of patients withmultiple sclerosis duringthe SARS-CoV-2 pan-demic]. Rev Neurol.2020;70:329-40. [PMID:32329046]
Figure. Examples of lesion locations emphasized by the McDonald criteria.
Left. Sagittal, fluid-attenuated, inversion recovery brain sequence showing periventricular (top arrow), juxtacortical (right-handarrow), and infratentorial (bottom arrow) lesions.Middle. Sagittal T1 image after administration of intravenous contrast. Lesions aretypically either silent or dark on T1 imaging, but lesions that enhance with contrast (arrow) do so because of active inflammation inthe lesion. Right. Sagittal T2 scan of the cervical spine showing a lesion at approximately the C2 level (arrow).
© 2021 American College of Physicians ITC6 In the Clinic Annals of Internal Medicine
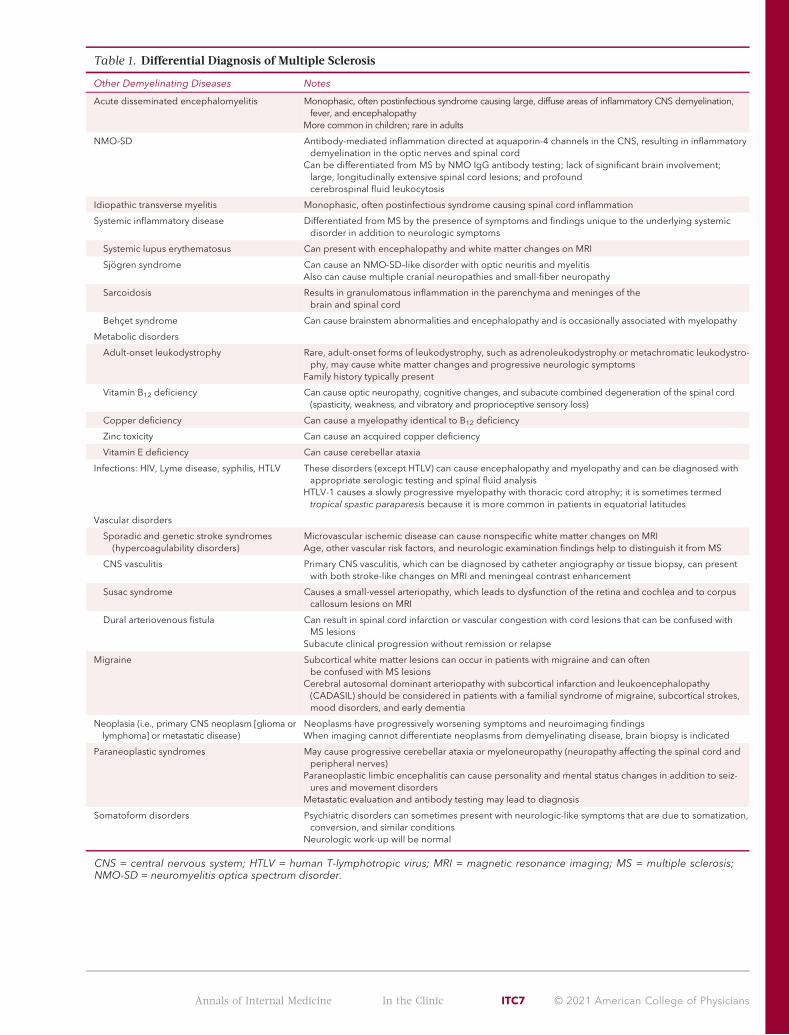
Table 1. Differential Diagnosis of Multiple Sclerosis
Other Demyelinating Diseases Notes
Acute disseminated encephalomyelitis Monophasic, often postinfectious syndrome causing large, diffuse areas of inflammatory CNS demyelination,fever, and encephalopathy
More common in children; rare in adults
NMO-SD Antibody-mediated inflammation directed at aquaporin-4 channels in the CNS, resulting in inflammatorydemyelination in the optic nerves and spinal cord
Can be differentiated from MS by NMO IgG antibody testing; lack of significant brain involvement;large, longitudinally extensive spinal cord lesions; and profoundcerebrospinal fluid leukocytosis
Idiopathic transverse myelitis Monophasic, often postinfectious syndrome causing spinal cord inflammation
Systemic inflammatory disease Differentiated from MS by the presence of symptoms and findings unique to the underlying systemicdisorder in addition to neurologic symptoms
Systemic lupus erythematosus Can present with encephalopathy and white matter changes on MRI
Sjögren syndrome Can cause an NMO-SD–like disorder with optic neuritis and myelitisAlso can cause multiple cranial neuropathies and small-fiber neuropathy
Sarcoidosis Results in granulomatous inflammation in the parenchyma and meninges of thebrain and spinal cord
Behçet syndrome Can cause brainstem abnormalities and encephalopathy and is occasionally associated with myelopathy
Metabolic disorders
Adult-onset leukodystrophy Rare, adult-onset forms of leukodystrophy, such as adrenoleukodystrophy or metachromatic leukodystro-phy, may cause white matter changes and progressive neurologic symptoms
Family history typically present
Vitamin B12 deficiency Can cause optic neuropathy, cognitive changes, and subacute combined degeneration of the spinal cord(spasticity, weakness, and vibratory and proprioceptive sensory loss)
Copper deficiency Can cause a myelopathy identical to B12 deficiency
Zinc toxicity Can cause an acquired copper deficiency
Vitamin E deficiency Can cause cerebellar ataxia
Infections: HIV, Lyme disease, syphilis, HTLV These disorders (except HTLV) can cause encephalopathy and myelopathy and can be diagnosed withappropriate serologic testing and spinal fluid analysis
HTLV-1 causes a slowly progressive myelopathy with thoracic cord atrophy; it is sometimes termedtropical spastic paraparesis because it is more common in patients in equatorial latitudes
Vascular disorders
Sporadic and genetic stroke syndromes(hypercoagulability disorders)
Microvascular ischemic disease can cause nonspecific white matter changes on MRIAge, other vascular risk factors, and neurologic examination findings help to distinguish it from MS
CNS vasculitis Primary CNS vasculitis, which can be diagnosed by catheter angiography or tissue biopsy, can presentwith both stroke-like changes on MRI and meningeal contrast enhancement
Susac syndrome Causes a small-vessel arteriopathy, which leads to dysfunction of the retina and cochlea and to corpuscallosum lesions on MRI
Dural arteriovenous fistula Can result in spinal cord infarction or vascular congestion with cord lesions that can be confused withMS lesions
Subacute clinical progression without remission or relapse
Migraine Subcortical white matter lesions can occur in patients with migraine and can oftenbe confused with MS lesions
Cerebral autosomal dominant arteriopathy with subcortical infarction and leukoencephalopathy(CADASIL) should be considered in patients with a familial syndrome of migraine, subcortical strokes,mood disorders, and early dementia
Neoplasia (i.e., primary CNS neoplasm [glioma orlymphoma] or metastatic disease)
Neoplasms have progressively worsening symptoms and neuroimaging findingsWhen imaging cannot differentiate neoplasms from demyelinating disease, brain biopsy is indicated
Paraneoplastic syndromes May cause progressive cerebellar ataxia or myeloneuropathy (neuropathy affecting the spinal cord andperipheral nerves)
Paraneoplastic limbic encephalitis can cause personality and mental status changes in addition to seiz-ures and movement disorders
Metastatic evaluation and antibody testing may lead to diagnosis
Somatoform disorders Psychiatric disorders can sometimes present with neurologic-like symptoms that are due to somatization,conversion, and similar conditions
Neurologic work-up will be normal
CNS = central nervous system; HTLV = human T-lymphotropic virus; MRI = magnetic resonance imaging; MS = multiple sclerosis;NMO-SD = neuromyelitis optica spectrum disorder.
Annals of Internal Medicine In the Clinic ITC7 © 2021 American College of Physicians

What is thedifferential diagnosis?Whenever the diagnosis of multi-ple sclerosis is being considered,conditions that mimic it (Table 1)should be part of the differential di-agnosis. These include disordersthat can cause neurologic symp-toms and changes inMRI scans thatare sometimes incorrectly diag-nosed asmultiple sclerosis. Forexample, a recent study found thatapproximately 30% of patientsreferred to a tertiarymultiple sclero-sis center had an incorrect diagno-sis (18). The best way to distinguishpatients with multiple sclerosis fromthose with other diagnoses is toconduct a comprehensive review ofthe patient's medical history, review
of systems, and physical examina-tion. Knowledge about otherpotential diagnoses that might beconfusedwithmultiple sclerosis isalso useful.
One condition that may be con-fused with multiple sclerosis isneuromyelitis optica spectrumdisorder (Table 1). Since 2004, ithas been possible to diagnosethis disorder by testing for a novelserum autoantibody termed neu-romyelitis optica IgG or AQP4-Ab(19). An important reason to diag-nose this disorder is that the U.S.Food and Drug Administration(FDA) has approved 3medica-tions to treat it in the past 2 years
(eculizumab, inebilizumab, andsatralizumab-mwge) (20).
When should cliniciansconsider consulting witha neurologist or anotherspecialist for diagnosis?
Given the complexity of the diag-nosis, if initial findings suggestmultiple sclerosis, the clinicianshould refer the patient to a neu-rologist for further evaluation andtesting. For cases in which the di-agnosis is unclear or if initial treat-ment has failed, clinicians shouldconsider obtaining a second opin-ion from 1 or more multiple scle-rosis specialty clinics.
Diagnosis... Patients presenting with symptoms of a demyelinating disorder should have a thorough review oftheir medical history and physical examination, with special attention to the possibility of optic neuritis, myelitis,and brainstem or cerebellar lesions, and they should have anMRI scan of their brain and spinal cord. The diagno-sis of multiple sclerosis is made by applying the revised 2017McDonald criteria, which use a combination of find-ings to show dissemination of disease activity over space and time. Early referral to a neurologist is encouraged.Additional testing, such as lumbar puncture, evoked potentials, optical coherence tomography, and serummarkers for other diseases, is not required but can be helpful in some patients for separating multiple sclerosisfrom other disorders.
CLINICAL BOTTOM LINE
TreatmentWhat is the overall approach totreating patients with multiplesclerosis?The care of patients with multiplesclerosis requires a multidiscipli-nary approach and a comprehen-sive strategy with medication andnonmedical approaches forrelapse management; preventionof relapses and delay of diseaseprogression; andmanagement offatigue, cognitive function, spas-ticity, bladder dysfunction, andother symptoms. An increasingnumber of effective medicationsare available for these purposes.Treatment should also includeassisting patients in maximizingdaily function. Use of all of thesetools has led to significantimprovements in quality of life formany patients with multiple scle-rosis. Although reducing disease
progression currently focuses oncontrolling inflammatory diseaseactivity early in RRMS, ongoingresearch provides hope for allevi-ating tissue injury throughenhanced repair and the preven-tion of neurodegeneration.
What role does clinical subtypeplay in guiding treatmentdecisions?Assigning a clinical subtype is acritical first step before startingany drug therapy. Most of theFDA's approvals for DMTs havebeen for CISs, RRMS, and activeSPMS, but 1 newmedication hasbeen approved for PPMS (21).
Immunotherapy is indicated assoon as the diagnosis is establishedfor most patients with CISs, RRMS,or PPMS. If patients with SPMS arehaving relapses, a DMT should be
considered; if the patient is declin-ing slowly, general immunosup-pressive agentsmay be used.
What medications are typicallyused, and what are theirbenefits, potential harms,and costs?
First-line DMTs include immuno-modulatory and immunosuppres-sive medications that have beenshown onMRI scans to reduce riskfor relapse, disease progression,and new lesion formation (22). Inaddition, recent evidence sup-ports the idea that some DMTsprovide real-world clinicalbenefits.
ADanish registry compared 194patients started on high-efficacyDMTs (natalizumab, fingolimod,
© 2021 American College of Physicians ITC8 In the Clinic Annals of Internal Medicine

alemtuzumab, cladribine, andocrelizumab) with 194 patientsreceiving medium-efficacy DMTs.The high-efficacy patients hadlower rates of clinical worseningand fewer on-treatment relapses.In addition, an Italian registry con-cluded that starting patients within2 years of diagnosis on a high-efficacy DMT (rituximab, ocrelizu-mab, mitoxantrone, alemtuzumab,or natalizumab) was associatedwith less disability 6 to 10 yearsafter disease onset (23).
Before 1993, there were no FDA-approvedmedications for multi-ple sclerosis. Since then, the FDAhas approved 23 DMTs (Table 2)with different routes of administra-tion, mechanisms of action, andpotential adverse effects. A com-prehensive review of all DMTs bynonpartisan groups may be foundat https://ms-coalition.org/wp-content/uploads/2019/06/MSC_DMTPaper_062019.pdf. Thisdocument provides the route ofadministration, mechanism ofaction, adverse effects, warnings,and clinical andMRI data for allDMTs and is updated on a regularbasis. TheAppendix Figure(available at Annals.org) showsthe current understanding of thepathophysiology of multiple scle-rosis as well as the mechanisms ofaction of the major medications.The following sections provideinformation on 2 frequently usedmedications.
NatalizumabNatalizumab is a monoclonal anti-body that is administered bymonthly intravenous infusion. Itreduces entry of activated T cellsthrough the blood–brain barrierinto the CNS by inhibiting thea4-integrin cellular adhesionmol-ecule on these immune cells andthus interfering with binding tothe vascular endothelium.Natalizumab is highly effective;it reduces relapse rates by 68%compared with placebo and slowsdisability progression by
approximately 40% (24). Anotheradvantage is adherence, giventhat the medication is adminis-tered once monthly by infusion ina clinical setting rather than by thepatient as an oral or injectablemedication. Despite its efficacy,natalizumab is limited by its riskfor progressive multifocal leu-koencephalopathy (PML), a poten-tially fatal demyelinating infectioncaused by reactivation of the JohnCunningham (JC) virus in theCNS. This is more likely to occur inpatients with low CD4 T-cellcounts, such as those treated withnatalizumab, those on long-termimmunosuppressive regimens, orthose with AIDS. The estimatedinitial risk for PML in patients be-ginning treatment with natalizu-mab is approximately 1 in 1000but is significantly higher in thosewith previous exposure to immu-nosuppressants or chemotherapyand those with elevated serumtiters of antibodies against the JCvirus (25). The results of tests forantibodies against JC virus maybe reported as direct antibodylevels or as an index (theSTRATIFY or JC antibody index),which is a ratio of direct antibodylevels to levels in a calibrator sam-ple (26). An index value below 0.2is regarded as evidence of sero-negativity, between 0.2 and 0.4 asindeterminate, and above 0.4 asevidence of seropositivity. A se-rum test for JC virus antibodies isan effective risk stratification toolbefore starting use of natalizumaband for monitoring risk duringuse. For example, a positive base-line anti–JC virus antibody indexabove 0.90 predicts stable posi-tive JC virus serostatus (27) and isa reason to use a DMT other thannatalizumab.
An assessment of the sera of morethan 1300 patients with multiplesclerosis receiving natalizumabshowed a seroprevalence of 50%to 60% positivity. In an assessmentof the sera of 63 patients whodeveloped PML while receiving
natalizumab, antibodies to the JCvirus were present before PML di-agnosis in all cases. The risk forPML increased to approximately3 cases per 1000 patients in thosewith a positive antibody result atscreening or during treatment andto 13 cases per 1000 patients ifthere was a history of immunosup-pression (28).
Dimethyl fumarate
Oral dimethyl fumarate exerts itsimmunomodulatory effects bymodulating the nuclear factor–like2 transcriptional pathway.
In the pivotal clinical trial of di-methyl fumarate, the annualizedrelapse rate in patients receiving240mg twice daily was 0.17 com-pared with 0.36 for placebo (P<0.001). The relative risk reductionfor disability progression was 38%compared with placebo (P=0.005), and new lesions onMRIscans were reduced comparedwith placebo.
These data led to FDA approvalfor use of this medication inpatients with RRMS (29). The pack-age insert has been updated toinclude CISs, RRMS, and SPMSwith relapses.
The cost of multiple sclerosistreatment has skyrocketed in thepast decade, and this is beingincreasingly questioned bypatients and analysts. A 2021 arti-cle that examined cost data from5906 patients with multiple sclero-sis reported that the yearly rangefor DMTs was $70000 to $82000(30).
Current treatment varies greatly,with different specialists using dif-ferent medications for differentstages of the disease. Oneapproach is as follows:
� For patients with a newly diag-nosed CIS or RRMS, start intrave-nous natalizumab and performtests for JC virus antibodies andtheir index. If the results are pos-itive, continue natalizumab for1 year and then switch to oraldimethyl fumarate.
Annals of Internal Medicine In the Clinic ITC9 © 2021 American College of Physicians

Table 2. Disease-Modifying Therapies for Multiple Sclerosis
Medication Route ofAdministration
Warnings, Contraindications,and Potential AEs
RecommendedMonitoring
PregnancyCategory*
Interferon-b1a andinterferon-b1b
Intramuscular orsubcutaneous injection
AEs: Flu-like symptoms, fatigue,depression, increased spasticity,transaminitis, injection site reactions,seizures, congestive heart failure,leukopenia, autoimmune disorders
CBC and liver function test-ing every 6 mo
C
Glatiramer acetate Subcutaneous injection AEs: Injection site reactions,lipoatrophy of skin at injection sites,rare systemic panic attack–likesyndrome
None B
Daclizumab Subcutaneous injection Black box warning: Hepatic injury,including autoimmune hepatitis andother immune-mediated disorders
Contraindications: Preexisting hepaticdisease or hepatic impairment,including alanine aminotransferaseor aspartate aminotransferase level≥2 times the upper limit of normaland history of autoimmune hepatitisor other autoimmune conditioninvolving the liver
AEs: Injection site reactions, upper re-spiratory infections, depression,transaminitis
Liver function testing every3–6 mo
No adequate data; see fullprescribing information
Ofatumumab Subcutaneous injection Contraindication: Active HBV infec-tion
AEs: Upper respiratory tract infec-tions, headache, injection-relatedreactions, reduction in immunoglo-bulins, local injection site reactions
Must have HBV screeningand serum immunoglobu-lins before use
No adequate data; see fullprescribing information
Fingolimod Oral Contraindications:� Recent myocardial infarction,unstable angina, stroke, transientischemic attack, decompensatedheart failure with hospitalization,or class III/IV heart failure
� History of Mobitz type II second-or third-degree AV block or sicksinus syndrome, unless patienthas pacemaker
� Baseline QTc interval ≥500 ms� Treatment with class Ia or class IIIantiarrhythmic drugs
AEs: Transaminitis, lymphopenia,increased risk for serious herpesvirusinfection, hypertension, PML, poste-rior reversible encephalopathy syn-drome, cutaneous tumors,bradycardia (usually only with thefirst dose), macular edema
Cardiac monitoring foradministration of firstdose; ophthalmologicscreening; liver functiontesting and CBC; yearlyskin examinations
C
Dimethyl fumarate Oral AEs: Diarrhea, nausea, abdominalcramping, flushing, lymphopenia
Monitor CBC frequently inthe first 6 mo, every 6 mothereafter as well as forinfections
C
Diroximel fumarate Oral Same as dimethyl fumarate, plus PMLand transaminitis
Same as dimethyl fumarateplus liver function testsbefore start
C
Monomethyl fumarate Oral Same as diroximel fumarate Same as diroximel fumarate C
Teriflunomide Oral Black box warnings: Hepatotoxicityand risk for teratogenicity
Contraindications: Severe hepaticimpairment, pregnancy, hypersensi-tivity, current leflunomide treatment
AEs: Alopecia, respiratory infections(including tuberculosis), pancreatitis,transaminitis, lymphopenia, hyper-tension, peripheral neuropathy
Monitor CBC, hepaticpanel, amylase, lipase,and blood pressure fre-quently in the first 6 mo,every 6 mo thereafter
X
Continued on following page
© 2021 American College of Physicians ITC10 In the Clinic Annals of Internal Medicine

Table 2—Continued
Medication Route ofAdministration
Warnings, Contraindications,and Potential AEs
RecommendedMonitoring
PregnancyCategory*
Cladribine Oral Black box warnings: Cancer and riskfor teratogenicity
Contraindications:� Patients with current cancer� Pregnant women and adults ofreproductive potential who do notplan to use effective contraceptionduring cladribine dosing and for 6mo after the last dose in each treat-ment course
� HIV infection� Active chronic infections(e.g., hepatitis or tuberculosis)
� History of hypersensitivity to cladri-bine
� Women intending to breastfeed ona cladribine treatment day and for10 d after the last dose
AEs: Upper respiratory infection, head-ache, lymphopenia, liver injury
CBC every 3–6 mo; screenfor TB, hepatitis, shingles,or other infections asappropriate
D
Siponimod Oral Contraindications:� Patients with a CYP2C9*3/*3genotype
� Patients with myocardial infarc-tion, unstable angina, stroke, TIA,decompensated heart failurerequiring hospitalization, or classIII/IV heart failure in the past 6 mo
� Presence of Mobitz type II second-or third-degree AV block or sicksinus syndrome, unless patient hasfunctioning pacemaker
AEs: Headache, hypertension, transa-minitis, infection
Obtain CBC, liver functiontests, electrocardiogram,and ophthalmologicassessment before initiat-ing treatment
Monitor for infection duringtreatment
Do not start in patients withactive infection
Other warnings include mac-ular edema, bradyarrhyth-mia, respiratory effects,liver injury, increased bloodpressure, and fetal risk
No adequate data; see fullprescribing information
Ozanimod Oral Same as siponimod, plus contraindi-cation for severe untreated sleepapnea
Same as siponimod Same as siponimod
Alemtuzumab Intravenous Black box warnings: Autoimmunity,infusion reactions, tumors
Contraindication: HIV infectionAEs: >90% of patients in clinical trialsexperienced infusion reactions(rash; fever; headache; muscleaches; temporary recurrence of pre-vious neurologic symptoms; and,rarely, anaphylaxis and heartrhythm abnormalities)
Serious AEs: Autoimmunity, infusionreactions, tumors, immune thrombo-cytopenia, glomerular nephropa-thies, thyroid disorder, otherautoimmune cytopenias, infections,pneumonitis, immediate and signifi-cant depletion of lymphocytes; her-pes simplex and zoster infectionsmore common in patients whoreceived alemtuzumab in clinical tri-als, especially soon after infusions;prophylaxis with antiviral agent is rec-ommended for ≥2 mo or until CD4count is >0.200 � 109 cells/L
Available only through re-stricted distribution under aRisk Evaluation MitigationStrategy program
C
Natalizumab Intravenous Black box warning: Increased risk forPML
AEs: headache, chest discomfort(common); hepatotoxicity, infusionreactions, anaphylaxis (rare)
Rigorous, regimented,industry-sponsored moni-toring (TOUCH program)
JC virus antibody and indextesting
C
Continued on following page
Annals of Internal Medicine In the Clinic ITC11 © 2021 American College of Physicians

� For patients with RRMS who al-ready are receiving a DMT andare doing well—meaning thatthey can tolerate themedication,have had no relapses in 1 to 2years, and have had no changeson their MRI scans for 1 year—maintain them on that therapy.For those who are not doingwell, switch to a different DMT.
� For patients with newly diag-nosed PPMS, start ocrelizumab.
� For patients with SPMS who arestable with no medication, maxi-mize physical therapy and symp-tomatic medications. Do notstart a DMT because of the riskfor infection.
� For patients with SPMS who areusing a DMT but continue tohave relapses, add an immuno-suppressant agent or considerswitching to a different DMT.
� For patients with SPMS who con-tinue to have attacks despitehaving usedmultiple differentDMTs, start intravenous cyclo-phosphamide.
Bonemarrow transplant, a moreaggressive approach that is notFDA approved for multiple sclero-sis, has been used as a rescuetherapy for patients who do not
respond to therapy and thosewith SPMS.
In a recent study of autologous he-matopoietic stem cell transplantpatients, 210 with RRMS or SPMSunderwent this procedure. Forpatients with RRMS, 85% had noworsening of disability at 5 yearsand 71.3% had no worsening at10 years. For patients with SPMS,71% showed no worsening of dis-ability at 5 years and 57.2%showed no worsening at 10 years(31).
When should cliniciansconsider immunomodulatorytherapy?Immunomodulatory drugs shouldbe initiated at the time of diagno-sis. In the past, clinicians wereencouraged to wait until a clini-cally definite diagnosis of multiplesclerosis could be established.Guidelines now recommend ini-tiating immunomodulatory treat-ment at the time of first clinicalsymptoms for those with RRMSand for those with a CIS and riskfactors for later conversion to adiagnosis of multiple sclerosis.
What is the role of vitamin D?Researchers have establishedclear links between vitamin D defi-ciency and the pathophysiologyof multiple sclerosis.
Immunoregulatory vitamin Dreceptors are present on T cells,and vitamin D interacts with theimmunomodulatory effects ofestrogen and testosterone (32).Reduced serum vitamin D levelshave been shown to predict accu-mulation of new lesions onMRIscans, and high levels are associ-ated with decreased risk forrelapse (33, 34).
A randomized, double-blind, pla-cebo-controlled trial of the addi-tion of vitamin D supplements(14007 IU/d) to interferon-b treat-ment found that vitamin D supple-mentation reduced lesionaccumulation onMRI scans com-pared with placebo (35). Anothertrial found that the number of newgadolinium-enhancing lesions orT2 lesions that were new or enlarg-ing was reduced by 32% inpatients supplemented with chole-calciferol compared with placebo(36).
Although the ideal serum 25-hydroxyvitamin D levels are stillunknown, most studies haveshown benefit for levels of 50nmol/L or greater (37), so somemultiple sclerosis specialists mea-sure vitamin D levels in all of theirpatients and prescribe supple-ments if the values are less than50 nmol/L.
Table 2—Continued
Medication Route ofAdministration
Warnings, Contraindications,and Potential AEs
RecommendedMonitoring
PregnancyCategory*
Ocrelizumab Intravenous Contraindication: Active HBV infec-tion
AEs: Infusion reactions (possibly life-threatening), infections, possibleincrease in tumors
Prescreen for hepatitis B No adequate data; see fullprescribing information
Mitoxantrone Intravenous Black box warnings: Cardiotoxicityand acute myeloid leukemia
AEs: Infection, nausea, oral sores, alo-pecia, menstrual irregularities, bluediscoloration of urine
Required monitoring of car-diac function by echocar-diography or multigatedradio-nucleotide angiog-raphy before each infusionand regular CBC
D
AE = adverse effect; AV = atrioventricular; CBC = complete blood count; HBV = hepatitis B virus; JC = John Cunningham; PML =progressive multifocal leukoencephalopathy.* B = fetal risk in animal studies but no adequate human studies or fetal risk in animal studies but adequate human studies with norisk; C = fetal risk in animal studies and no adequate human studies, but potential benefit to pregnant women may outweigh risk; D =fetal risk in human studies, but potential benefit to pregnant women may outweigh risk; X = studies in animals or humans have dem-onstrated fetal abnormalities and/or there is positive evidence of human fetal risk based on adverse reaction data from investigationalor marketing experience, and the risks involved in use of the drug in pregnant women clearly outweigh potential benefits.
© 2021 American College of Physicians ITC12 In the Clinic Annals of Internal Medicine

How should clinicians choosetherapy for patients having anacute relapse?Relapses are defined by the de-velopment of new or worseningneurologic symptoms lasting 24hours or more without an increasein body temperature, identifiableinfection, or another trigger for apseudo-relapse. When a relapsehas been confirmed, the standardtreatment is high-dose corticoste-roids, which are typically adminis-tered as an intravenous infusion ofmethylprednisolone, 1 g/d for 3to 5 days, with no oral taper.Recent trials have shown that oralmethylprednisolone, 1 g/d for 5days (38), and oral prednisone,1250 mg/d for 5 days (39), haveequivalent efficacy. For relapsesthat do not respond to steroids,plasma exchange (40), 5 days of
intramuscular or subcutaneousadrenocorticotrophic hormonegel (41), and pulse-dose intrave-nous cyclophosphamide (42) areavailable rescue treatments.
When should a patient withmultiple sclerosis behospitalized?
Most relapses do not require hos-pitalization. Oral steroid treatmentdoes not require observation inthe hospital, andmost insuranceplans cover home nursing servicesfor intravenous infusions of cortico-steroids because this is more cost-effective than hospitalization anddecreases the chance of infection.
Hospitalizationmay be beneficialfor severe relapses causing com-plete loss of mobility or impairedbladder or bowel control, which
can lead to serious infection risks.Patients who havemarked worsen-ing during relapse require nursingand rehabilitation services, whichare often beyond the capacity oftheir family. Hospitalization mayalso be beneficial for patients whorequire special monitoring whilereceiving relapse treatment, suchas blood glucosemonitoring forsteroid administration in a patientwith diabetes. Rescue treatmentfor steroid-refractory relapses withadrenocorticotrophic hormone geldoes not require hospitalization,but plasma exchange or pulse-dose cyclophosphamide therapyshould be done in the hospital.
What treatments are used toalleviate chronic symptoms?To adequately treat a patient withmultiple sclerosis, it is important
Table 3. Symptom Management in Multiple Sclerosis
Symptom Nonpharmacologic Management Pharmacologic Management
Spasticity Physical therapy, stretching, massagetherapy
Baclofen (oral or intrathecal pump), tizani-dine, cyclobenzaprine, dantrolene, gaba-pentin, benzodiazepines, carisoprodol,botulinum toxin
Neuropathic pain Not applicable Gabapentin, pregabalin, duloxetine, tricyclicantidepressants, tramadol, carbamazepine,topiramate, capsaicin patch
Fatigue Proper sleep hygiene, regular exercise Modafinil, armodafinil, amantadine,fluoxetine or amphetamine stimulants
Depression Individual or group counseling Antidepressants (such as SSRIs, SNRIs,tricyclic antidepressants, antipsychotics)
Cognitive dysfunction Cognitive rehabilitation and accommoda-tion strategies
No proven therapy
Mobility Physical and occupational therapy; use of bra-ces, canes, rolling walkers, electrostimulatorywalk-assist devices
Dalfampridine
Urinary urgency/frequency Timed voids, avoidance of caffeine Oxybutynin, tolterodine, desmopressin,darifenacin, tamsulosin, mirabegron,imipramine, solifenacin, botulinum toxin,implantable bladder stimulators
Urine retention Manual pelvic pressure, intermittentcatheterization
Antibiotics for urinary tract infectionConsider BPH, which can be treated witha-blocker and/or 5-a reductase inhibitor
Bowel dysfunction None Metamucil, docusate, bisacodyl, milk ofmagnesia, mineral oil, enemas orsuppositories
Erectile dysfunction Vacuum pump Sildenafil, tadalafil, vardenafil, alprostadil,avanafil
Heat intolerance Avoidance of hot weather and hot tubsCooling equipment (fans, cooling vests)
None
Pseudobulbar affect None Dextromethorphan/quinidineLimb tremor Occupational therapy Isoniazid, clonazepam, botulinum toxin, tha-
lamic stimulation via deep-brain stimulator
BPH = benign prostatic hypertrophy; SNRI = serotonin–norepinephrine reuptake inhibitor; SSRI = selective serotonin reuptakeinhibitor.
Annals of Internal Medicine In the Clinic ITC13 © 2021 American College of Physicians

to use DMTs and to addresssymptoms that remain chronicafter a previous relapse or pro-gression. Table 3 provides a com-prehensive review of symptommanagement. It is important torecognize the usefulness of theseinterventions for increasing qualityof life in patients with multiplesclerosis.
How should clinicians monitorpatients being treated formultiple sclerosis?Monitoring should involve regularassessments of the efficacy andsafety of DMTs. There are no clini-cal guidelines for monitoringtreatment efficacy, but the prac-tices developed for clinical trialscan provide indirect guidance. Inthese trials, DMTs have beenshown to decrease the frequen-
cies of relapse and newMRIlesions and to reduce the accumu-lation of disability. Therefore, clini-cal assessment of efficacy shouldinclude documentation of relap-ses, periodic neurologic examina-tions, and regular MRI scans.Clinicians should consider chang-ing immunomodulatory treatmentfor patients with recurrent relap-ses, new lesion formation onMRI,or progressive accumulation ofdisability. Safety assessments aretargeted toward the knownadverse effects of the immunomo-dulatory treatment being used.Recommendedmonitoring testsare listed in Table 2.
Should patientswithmultiplesclerosis receive immunizations?The American Academy ofNeurology clinical practice
guidelines recommend the sameimmunizations for patients withmultiple sclerosis that are recom-mended for others (43). One rea-son is that the risk for relapsesincreases during the weeks sur-rounding infectious episodes. Inaddition, there is no evidencethat multiple sclerosis worsens asa consequence of immunizationwith any vaccines, including thoseagainst influenza, hepatitis B,varicella, tetanus, and tuberculosis(bacille Calmette–Gu�erin vaccine)(44). However, fingolimoddecreases a patient's ability torecover from viral infections, andthe manufacturer recommendsthat patients avoid live viralvaccines while receiving thedrug.
Treatment... Treatment includes medications to prevent relapses, additional medications during acute relapses,and other medications and nonmedication treatments for symptommanagement. DMTs are approved to preventrelapses in patients with CISs, RRMS, and PPMS and in those with SPMS who have recurrent relapses. Less disabil-ity over time has been associated with high-efficacy DMTs (natalizumab, fingolimod, alemtuzumab, cladribine,ocrelizumab, rituximab, and mitoxantrone). Vitamin D supplementation may also be helpful when serum levels arelow. High-dose corticosteroids are the standard treatment for acute relapses, although plasma exchange, adreno-corticotrophic hormone gel, and cyclophosphamide can be used. Symptoms are managed on an individual basisthrough combined use of pharmacologic and nonpharmacologic means.
CLINICAL BOTTOM LINE
COVID-19 and Multiple SclerosisThe COVID-19 NeurologyResource Center (www.aan.com/tools-and-resources/covid-19-neurology-resource-center)keeps practitioners updated on
the latest developmentsregarding the interactionbetween SARS-CoV-2 and neu-rologic conditions, includingmultiple sclerosis. Current
practice is to continue DMTs inpatients with multiple sclerosisbecause these therapies andCOVID-19 do not seem to affecteach other (45).
© 2021 American College of Physicians ITC14 In the Clinic Annals of Internal Medicine

In the Clinic
Tool KitMultiple Sclerosis
Patient Informationhttps://medlineplus.gov/multiplesclerosis.htmlhttps://medlineplus.gov/spanish/multiplesclerosis.html
Information and handouts in English and Spanish fromthe National Institutes of Health's MedlinePlus.
www.ninds.nih.gov/disorders/all-disorders/multiple-sclerosis-information-pagehttps://espanol.ninds.nih.gov/trastornos/esclerosis_multiple.htm
Information in English and Spanish from the NationalInstitute of Neurological Disorders and Stroke.
www.nationalmssociety.org/What-is-MSwww.nationalmssociety.org/Resources-Support/Library-Education-Programs/Informacion-en-Espanol
Resources in English and Spanish from the NationalMultiple Sclerosis Society.
Information for Health Professionalswww.thelancet.com/journals/laneur/article/PIIS1474-4422(17)30470-2/fulltext
2017 revisions of the McDonald criteria for diagnosis ofmultiple sclerosis.
www.aan.com/Guidelines/home/GuidelineDetail/899
2018 practice guideline systematic review summary ondisease-modifying therapies for adults with multiplesclerosis from the American Academy of Neurology.
www.aan.com/Guidelines/home/GuidelineDetail/974
2019 practice guideline update summary on vaccine-preventable infections and immunization in multiplesclerosis from the American Academy of Neurology.
www.nationalmssociety.org/For-Professionals/Clinical-Care
Resources from the National Multiple Sclerosis Society. IntheClinic
Annals of Internal Medicine In the Clinic ITC15 © 2021 American College of Physicians

WHAT YOU SHOULD KNOWABOUT MULTIPLE SCLEROSIS
In the ClinicAnnals of Internal Medicine
What Is Multiple Sclerosis?Multiple sclerosis is a progressive, chronic diseasethat affects the central nervous system. It causesthe immune system to attack cells in the brain,spinal cord, and optic nerves. It is important todiagnose and treat multiple sclerosis early toprevent relapse, delay disease progression, andmaximize quality of life.
Doctors don't know for sure what causes multiplesclerosis, but it is most likely a combination ofenvironmental and genetic factors. It affectswomen more than men.
What Are the Symptoms?Symptoms differ depending on where the nervecells are damaged. Symptoms may come and go,or they may be permanent. They can include:
• Changes in vision (1 eye more common thanboth eyes)
• Muscle weakness• Fatigue• Loss of balance or trouble with coordination• Tremors, numbness, or slurred speech• Partial or total paralysis• Thinking or memory problems• Frequent urge to urinateMany patients with multiple sclerosis experience“flares” or “relapses” when symptoms suddenlyget worse or new ones appear and last morethan 24 hours.
How Is It Diagnosed?• No single test is available to diagnose multiplesclerosis. Your doctor will ask about your medicalhistory, do a physical examination, and run acombination of other tests.
• Blood tests may show signs of other illnesses thatcause symptoms similar to those of multiplesclerosis.
• Magnetic resonance imaging is essential for diag-nosis. It takes a detailed picture of your brain andspinal cord, where lesions that suggest multiplesclerosis may be present.
• More specialized testing may be needed if the di-agnosis is unclear.
How Is It Treated?• You and your neurologist will come up with atreatment plan that is best for you based on thetype of multiple sclerosis you have.
• Early treatment with immunotherapy is veryimportant and has been shown to lower risk forrelapse, disease progression, and developmentof new lesions in many patients.
• A multidisciplinary approach to care that includesnondrug therapies (physical, occupational, andspeech therapy) and symptom management(pain, muscle stiffness and spasms, fatigue, andbladder problems) may help preserve functionand quality of life.
• Steroids, such as prednisone, can reduce nerveinflammation during a relapse or flare.
• Low levels of vitamin D are common in patientswith multiple sclerosis and are associated withincreased risk for relapse. You may be instructedto take a vitamin D supplement.
• Lifestyle changes, including a healthy diet, beingphysically active, and getting enough sleep, mayalso help symptoms.
Questions for My Doctor• What kind of multiple sclerosis do I have?• What can I do to manage my symptoms?• Will my symptoms get worse over time?• What treatments are available to me?• What are the risks and side effects of thetreatment?
• How often should I have follow-up visits?
For More InformationMedlinePlushttps://medlineplus.gov/multiplesclerosis.html
National Multiple Sclerosis Societywww.nationalmssociety.org/What-is-MS
© 2021 American College of Physicians ITC16 In the Clinic Annals of Internal Medicine
Patie
ntInform
ation

Appendix Figure. Overview of the components of the immune system that are involved in pathogenesis of MS and where variousmedications exert their actions.
Plasmapheresis
K-channelblockers
Ab+C
Foxp3
Th2Th3Trl
Th2Th3Trl
IL-10TGF�
IFN�TNF�
IFN�TNF�
MCP-1MIP-1�IP-10RANTES
Pl
B
B
B
NO
Minocycline
CD8Oligo��T
MemantineRiluzole
Glutamate
Microglia
MinocyclineMMP-2/9VCAM-1
MitoxantroneAlemtuzumabFingolimodLaquininmodTeriflunomideCladribineRapamycinDaclizumab
VLA-4 VLA-4
IL-4 & IL-10
Statins, E2
IL-6/TGF�
IL-12
APC
B7
CD4CD4
ThpThp
APC
VCAM-1
Rituximab
IL-4IL-5IL-6IL-13TGF�
BBB CD40
CD40 CD40L
Sade 27
CD28
CD28
Thl Thl7
ThlThl7
CD40L
B7
Immunopathogenesis of the MS Lesion
GA
IFN-�Antegren
Steroids
5-HT= 5-hydroxytryptamine; Ab+C = antibody plus complement; APC = antigen-presenting cell; APRIL = a proliferation-inducingligand; ATP = adenosine triphosphate; B = B cell; BAFF = B-cell–activating factor; CTL = cytotoxic T lymphocytes; FcR = Fc receptor;GA = glatiramer acetate; ICAM-1 = intercellular adhesionmolecule 1; IFN = interferon; IL = interleukin; IP-10 = interferon c-inducibleprotein-10; LFA-1 = lymphocyte function-associated antigen 1; MCP = monocyte chemotactic protein; MIP = macrophage inflamma-tory protein; MMP = matrix metalloproteinase; MS = multiple sclerosis; NAA =N-acetyl aspartate; NO = nitric oxide; Oi = free oxygenradicals; Pl = plasma cell; RANTES = regulated on activation, normal T cell expressed and secreted; TACI = transmembrane activatorand calcium-modulating cyclophilin ligand; TGFb = transforming growth factor b; Th = T helper; Thp = T-helper precursor; TNFa =tumor necrosis factor a; VCAM-1 = vascular cell adhesion molecule 1; VLA-4 = very late antigen 4. Reprinted from Journal ofNeuroimmunology, vol. 176, Dhib-Jalbut S, Arnold DL, Cleveland DW, et al, “Neurodegeneration and Neuroprotection in MS andOther Neurodegenerative Diseases,” pp. 198-215, copyright 2006, with permission from Elsevier.
Annals of Internal Medicine In the Clinic © 2021 American College of Physicians