intestinal ischemia michele young, md chief gi phoenix va hospital banner/va gi fellowship program...
TRANSCRIPT

Intestinal IschemiaMichele Young, MDChief GI Phoenix VA HospitalBanner/VA GI Fellowship Program Director

Outline
•Types•Anatomy•Pathophysiology•Acute Mesenteric Ischemia•Mesenteric Vein Thrombosis•Focal Segmental Ischemia•Colon Ischemia•Chronic Mesenteric Ischemia•Vasculitides

Types
TYPE FREQUENCY (%)
Colon ischemia 75
Acute mesenteric ischemia 25
Focal segmental ischemia <5
Chronic mesenteric ischemia <5

Anatomy – Celiac Axis
•Supplies stomach, duodenum, pancreas, and liver
•Three branches: left gastric, common hepatic, splenic
•Common hepatic: gastroduodenal, right gastroepiploic, anterior superior pancreaticoduodenal
•Splenic: pancreatic and left gastroepiploic

Anatomy – Celiac Axis

Anatomy – Superior Mesenteric Artery (SMA)•Anterior and posterior inferior
pancreaticoduodenal•Middle colic•Right colic•Ileocolic

Anatomy - SMA

Anatomy – Inferior Mesenteric Artery (IMA)•Left colic•Sigmoid branches•Superior rectal•Supply distal transverse to proximal
rectum•Distal rectum: internal iliac

Anatomy - IMA

Pathophysiology
•Bowel can tolerate 75% reduction of blood flow and oxygen consumption for 12 hours
•Collaterals open immediately •After hours, vasoconstriction reduces
collateral flow (NOMI)•Hypoxia, reperfusion injury
▫ROS by xanthine oxidase▫Microvascular injury by PMNs

Acute Mesenteric Ischemia
CAUSE FREQUENCY (%)
SMA embolus 50
Nonocclusive mesenteric ischemia 25
SMA thrombosis 10
Mesenteric venous thrombosis 10
Focal segmental ischemia 5

Clinical Features•Acute abdominal pain in patient with CV risks•Rapid and forceful bowel evacuation (SMAE)•Pain out of proportion to exam•Some more indolent (MVT)•Unexplained abdominal distention (sign of
infarction) or GI bleeding (NOMI)•Physical findings worsen with progressive
loss of bowel viability• Infarction: 70-90% mortality

Diagnosis• Labs
▫ 75% have WBC > 15▫ 50% have metabolic acidosis
• Plain films▫ Poorly sensitive (30%) and nonspecific▫ Formless loops of small intestine▫ Ileus, thumbprinting, pneumatosis▫ Portal or mesenteric vascular gas
• CT▫ Colon dilatation▫ Bowel wall thickening▫ Lack of enhancement of arterial vasculature▫ Ascites
• CT angiography▫ Better evaluation of vessels
• Selective mesenteric angiography▫ Gold standard
• Prompt laparotomy if angiography not available






Portal Gas


Treatment
•General▫Resuscitation, Broad-spectrum antibiotics
•Superior Mesenteric Artery Embolus▫Cardiac origin▫Major: proximal to ileocolic
Intra-arterial papaverine Surgical revascularization
▫Minor and no peritoneal signs Intra-arterial papaverine (or thrombolytics) Anticoagulation

SMA Embolus
Pre and post treatment

Treatment
•Nonocclusive Mesenteric Ischemia▫Vasoconstriction from preceding
cardiovascular event▫Angiography
Narrowing of SMA branch origins Irregularities in intestinal branches Spasm of arcades Impaired filling of intramural vessels
▫SMA infusion of papaverine for 24 hours▫Surgery if peritoneal signs are present

NOMI
Pre and post treatment

Treatment
•Acute Superior Mesenteric Artery Thrombosis▫Severe atherosclerotic narrowing▫Often superimposed on chronic mesenteric
ischemia ▫Demonstrated on aortography▫Management same as SMA embolism

Mesenteric Vein Thrombosis
•Age: mid-60s to 70s•20% mortality•Manifest as colon ischemia, acute
mesenteric ischemia, or focal segmental ischemia
•Causes▫Arterial hypertension▫Neoplasms▫Coagulation disorders▫Estrogen

Mesenteric Vein Thrombosis• Acute
▫ Pain out of proportion to exam, n/v▫ Lower GI bleeding suggests infarction
• Diagnosis▫ CT is study of choice (finds >90%)▫ Mesenteric arteriography
Slow or absent filling of mesenteric veins Failure of arterial arcades to empty Prolonged blush in involved segment
• Treatment▫ Incidental: up to six months of anticoagulation (AC)▫ Peritonitis: surgery, papaverine, post-op heparin▫ No peritoneal signs: heparin followed by 3-6 mos AC

Mesenteric Vein Thrombosis
•Subacute▫Abdominal pain for weeks to months but no
infarction•Chronic
▫Asymptomatic▫May develop GI bleeding from varices▫Treatment: control bleeding

Focal Segmental Ischemia• Involves small bowel• Causes
▫Atheromatous emboli▫Strangulated hernias▫ Immune complex disorders ▫Trauma▫Segmental venous thrombosis▫Radiation therapy▫Oral contraceptives
• Usually adequate collaterals to prevent infarction• Presentation: enteritis, stricture, acute abdomen
▫Chronic can resemble Crohn's

Focal Segmental Ischemia
•Radiologic studies▫Smooth tapered stricture▫Abrupt change to normal distally▫Dilated proximally
•Treatment: resection

Colon Ischemia
TYPE FREQUENCY (%)*
Reversible colopathy and transient colitis >50
Transient colitis 10
Chronic ulcerating colitis 20
Stricture 10
Gangrene 15
Fulminant universal colitis <5

Colon Ischemia
•Most common form of intestinal ischemia▫7.2 cases per 100,000 person-years
•Female predilection•Most > 60 years old•Young pt: vasculitis, coagulation
disorders, cocaine, medications•Right colon ischemia
▫May have small intestinal ischemia

Medications• Penicillins• Alkaloid and taxanes• Constipation-Inducing Agents • Pseudoephedrine • Diuretics • Oral contraceptive pills • Amphetamines (R sided)• Cocaine (L sided)• Kayexelate• Magnesium citrate• Sodium phosphate • Bisacodyl• Glycerin enemas• NSAIDs• Sumatriptan• Alosetron

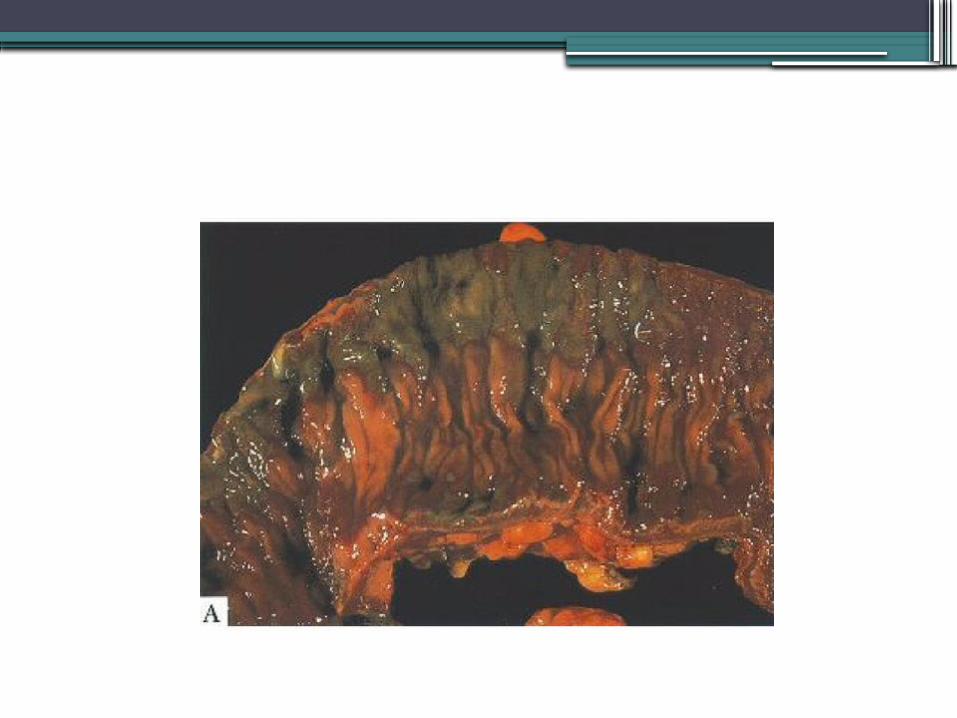
Pathology
•Mild: mucosal and submucosal hemorrhage and edema
•More severe: ulcerations, crypt abscesses, pseudopolyps, pseudomembranes, iron-laden macrophages, submucosal fibrosis (stricture)
•Most severe: transmural infarction

Clinical Features•Sudden cramping•Mild left lower quadrant pain•Urgent desire to defecate•Hematochezia within 24 hours•Location:
▫Sigmoid 23%▫Descending-to-sigmoid 11%▫Cecum-to-hepatic flexure 8% (worse prognosis)▫Descending 8%▫Pancolonic 7%

Diagnosis
•CT scan•If nonspecific, colonoscopy within 48
hours▫Unprepped, low air
•Colon single-stripe sign▫Line of erythema with erosion or ulceration
along the longitudinal axis of the colon▫Milder course

Colonoscopy




Treatment• NPO, IVF, antibiotics• EKG, Holter, echo• Colonic infarction
▫Laparotomy and resection▫Serosa can be misleading
• Segmental Ulcerating Colitis▫Recurrent fevers and sepsis▫Continuing or recurrent bloody diarrhea▫Persistent or chronic diarrhea with protein-
losing colopathy▫Treat by resection

Treatment• Ischemic Stricture
▫ Dilation or resection • Universal Fulminant Colitis
▫ Colectomy with ileostomy• Isolated Ischemia of the Right Colon
▫ Check CTA for concurrent AMI• Carcinoma/Obstructive Lesions (<5%)
▫ Lesion distal, increased intracolonic pressure proximal• Irritable Bowel Syndrome
▫ Colon ischemia 3.4 to 3.9x more common▫ ?Hypersensitivity of the colonic vasculature
• Complicating Aortic Surgery▫ Up to 7% of surgeries (60% for ruptured aneurysm)▫ Colonoscopy within 2-3 days if high risk
Ex: ruptured aneurysm, prolonged cross-clamping time, post-op diarrhea

Chronic Mesenteric Ischemia
•“Intestinal angina”•Mesenteric atherosclerosis•Pain from small bowel ischemia
▫Blood stolen to meet increased gastric demand from food

Clinical Features
•Gradual cramping discomfort within 30 minutes of eating, resolves over hours
•Fear of eating, weight loss•Nonhealing antral ulcers without H. pylori•1/3 to ½: cardiac, cerebral, peripheral
vascular disease•Exam
▫Abdomen soft and nontender▫Bruit common but nonspecific

Diagnosis• Gastric tonometry exercise testing (GET)
▫NG tube and arterial line▫Patient on PPI▫Obtain gastric juice and arterial blood fasting,
during, after exercise▫Measure gastric-arterial PCO2 gradients▫ Increase after exercise indicates ischemia
• Combine with duplex U/S• Angiography
▫Should show occlusion of ≥2 splanchnic arteries▫Does not make diagnosis in itself

Treatment
•Revascularization▫Need occlusive involvement of ≥2 major
arteries▫Surgical if healthy▫Otherwise percutaneous +/- stent