intermediate hepatocellular carcinoma management · intermediate hepatocellular carcinoma...
TRANSCRIPT

esmo.org
INTERMEDIATE HEPATOCELLULAR CARCINOMA MANAGEMENT
GI Preceptorship Nov 2018
Dr Choo Su Pin
Senior Consultant and Deputy Head, Medical Oncology
Co-Chair , Comprehensive Liver Cancer Centre
National Cancer Centre Singapore

2
Disclosures
� Advisory role and honoraria: Bayer, Sirtex, Bristol-Myers Squibb, Shire, Eisai, Ipsen, Norvatis, Celgene
� Speaker fees: Lilly Oncology, Sirtex. BMS
� Research funding: BMS, Sirtex

3
HBV is leading cause of HCC in Asia and China• 594 Mio cases in Asia2
HCV and life style is the leading cause of HCC in western population• 96 Mio cases in Nothern America and Europe
• 6th most common form of cancer worldwide more prominent in male
• Around 50% of HCC are diagnosed at advanced stage globally
Liver cancer is a common and deadly disease
1. Gravitz L, Nature 2014:516(7529):S1. 2. GloboCan 2012 http://globocan.iarc.fr/. 3. US National Cancer Institute Surveillance, Epidemiology, and End Results Program. 4. Ahmed, F. et al. Prev. Chronic Dis. 2008; 5:A74. 5. Scudellari N. Nature 2014; 2014:516(7529):S4; 6.Nature Outlook 12/14.
554000
228000
782,000 global new cases of liver cancer in 2012
Men Women
Very common Exceptionally lethal Heterogeneous Diseas e
• Second only to lung cancer in terms of mortality2,3
• Only 20% of diagnosed UK patients live longer than a year after diagnosis1
• Liver Cancer mortality in the US is growing at a higher rate than other cancers
Before 2017: estimated median survival for advanced HCC <
12 months

4
BCLC staging and treatment outcomes
Median OS 20 m Median OS 6.5 to 10.7m

5
ESMO
guidelines

6
The problem with intermediate HCC
� High heterogeneity� Clinical decisions differ from centre to centre coz of lack of clear
scientific evidence for many therapies� Thus, there are treatment discrepancies between guidelines


LOCOREGIONAL THERAPIES FOR INTERMEDIATE HCC:- NOT AMENABLE TO RESECTION/ TRANSPLANT OR ABLATION
- Transarterial Chemoembolisation ( TACE )
- Selective Internal radiotherapy (SIRT)
- Sorafenib
TACE
• Is there survival benefit
• What are the factors that affect TACE
outcomes?
• What is the best method for TACE
• How often should we TACE / what is
deemed TACE failure ?

TAE/TACE vs Best Supportive Care:
2-year Survival
Random effects model (DerSimonian and Laird)Odds ratio (95% CI)Author, journal year
Overall
Heterogeneity p=0.14 Favours treatment Favours contro l
Patients
503
Lin, Gastroenterology 1998 63
GETCH, NEJM 1995 96
Bruix, Hepatology 1998 80
Pelletier, J Hepatol 1998 73
Lo, Hepatology 2002 79
Llovet, Lancet 2002 112z=–2.3p=0.017
Llovet JM, et al. Lancet. 2003;362:1907–17Der Simonian R, Laird N. Controlled Clin Trials. 1986;7:177–88
0.01 0.1 0.5 1 2 10 100
Meta-analysis of 7 RCTs showed survival
benefit with TACE, OR 0.53, RR35% Llovet et al Hepatology 2003
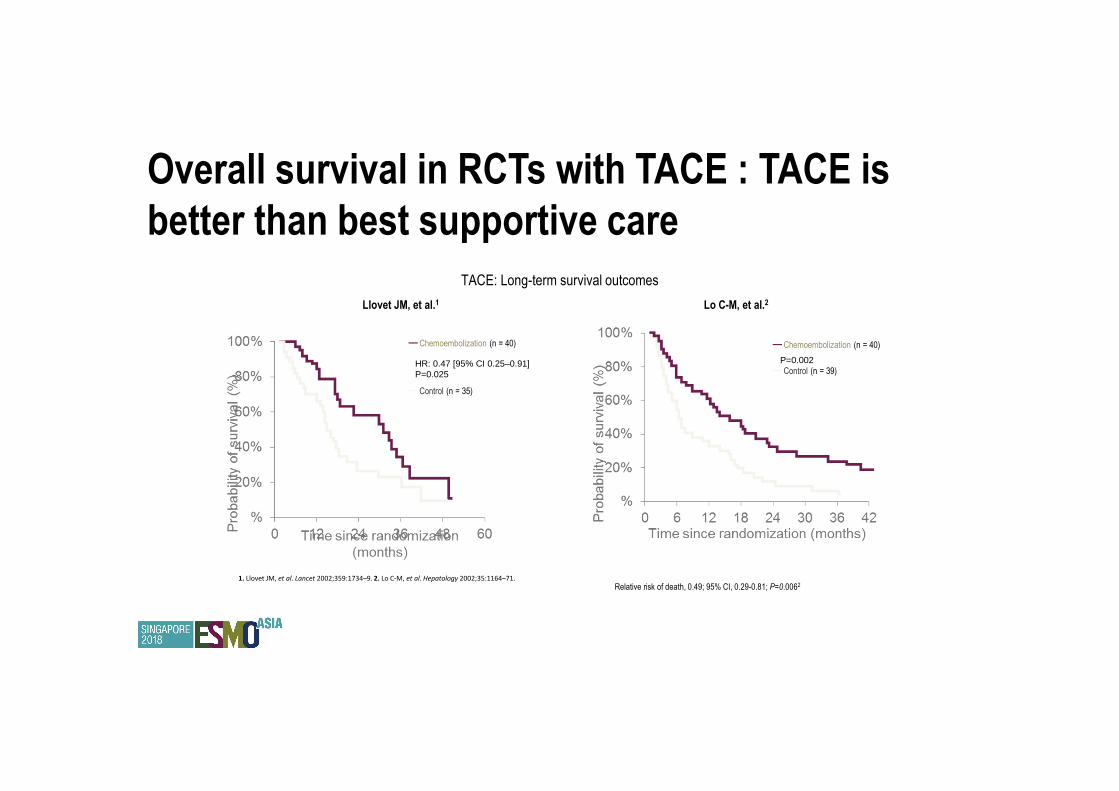
Overall survival in RCTs with TACE : TACE is
better than best supportive care
TACE: Long-term survival outcomes
P=0.002
Llovet JM, et al.1 Lo C-M, et al.2
HR: 0.47 [95% CI 0.25–0.91]P=0.025
Relative risk of death, 0.49; 95% CI, 0.29-0.81; P=0.006253
1. Llovet JM, et al. Lancet 2002;359:1734–9. 2. Lo C-M, et al. Hepatology 2002;35:1164–71.
━Chemoembolization (n = 40)
━Control (n = 35)
━Chemoembolization (n = 40)
━Control (n = 39)

Factors affecting TACE outcomes: Prognostic scores in patients undergoing TACE
HAP score ART Score ABCR score
Child-Pugh score/
Albumin-bilirubin
Albumin <35g/L Child-Pugh increase
following TACE : +1,
+2 points)
Child-Pugh increased
following TACE ( >2
points)
Bilirubin > 17mmol/L
Tumor stage Tumor diameter > 7vm BCLC stage (B,C)
AFP AFP> 400ng/dL AFP> 200ng/ml
AST AST> 25% from
baseline
Radiological response Lack of radiological
response
Presence of
radiological response
Hucke et al 2014; Adhoute
2015; Kadalayi 2013

13
Contraindications to TACE
Absolute contraindications� Thrombus in the main portal vein and portal vein ob struction (high risk liver failure)� Encephalopathy� Biliary obstruction� Child-Pugh C cirrhosis� Renal failure� Extensive tumour burden� TechnicalRelative contraindications include a variety of other factors including, but not limited to:� Bile duct occlusion or incompetent papilla� Reduced PS� Impaired liver function (CP B)� High risk oesophageal varices � Branch portal vein thrombosis
Vogel ESMO guidelines
14
Complications of TACE
� Post-embolization syndrome (60 – 80%)� Ischaemic damage with consequent liver failure � Hepatic abscess, biliary duct injury, cholecystitis (2%)� Gastroduodenal ulceration (3-5%)� Renal dysfunction (2%)� Pulmonary and cerebral lipiodol embolization (rare but can be
fatal)� Mortality approx. 2-3%

15
Conventional TACE vs DCBeads TACE� PRECISION V Trial : Phase 2 randomised , Europe, n=200 � Arm 1: TACE with doxorubicin� Arm 2: DC Beads with doxorubicin (150mg)
� Up to 3 times at 0,2,4mths
� Primary endpoint was = RR at 6 monthsResults:
� Less liver toxicity (p<0.001) and less doxorubicin toxicity (p=0.0001)with DC Beads.
DC Bead cTACE
Response rate 52% 44% p not sig
Disease Control Rate
63% 52% p not sig

16

17
Courtesy
Dr Huang
18
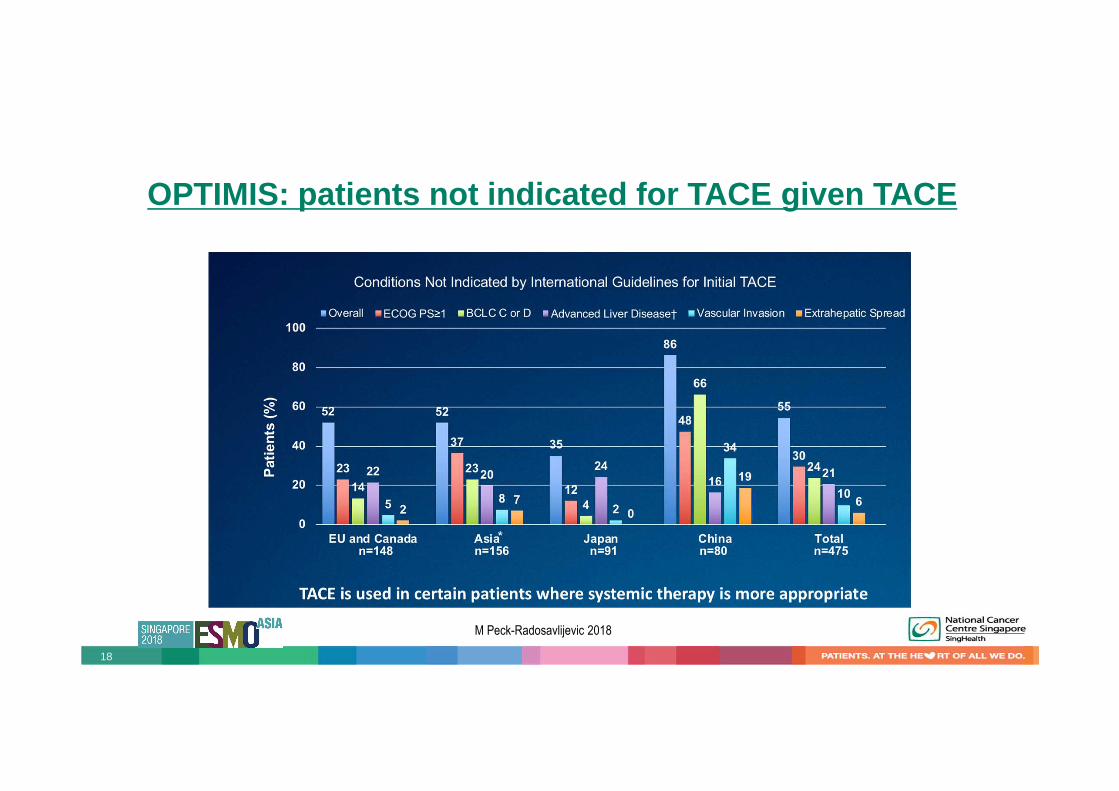
OPTIMIS: patients not indicated for TACE given TACE
M Peck-Radosavlijevic 2018

19
OPTIMIS: Variation in Timing to TACE Unsuitability Across Regions
Median days (SD)
EU & CANADAn=148
ASIA* n=156
JAPANn=91
CHINAn=80
Totaln=475
Median time to TACE unsuitability
79.5 (n=20)
109.5(n=20)
127.0(n=17)
42.0(n=5)
92.0(n=62)
Mean (SD) time between 1st & 2nd TACE
84.7 (70.9)(n=87)
83.5 (61.3)(n=75)
118.2 (101.7)(n=51)
80.8 (61.9)(n=37)
90.6 (75.4)(n=250)
TACE to initiation of other treatment
161.8 (69.0)(n=13)
142.6 (96.6)(n=20)
155.7 (73.3)(n=11)
72.0(66.2)(n=7)
140.4 (82.9)(n=46)
Timing After Initial TACE Treatment
Data on file. Bayer HealthCare. Whippany, New Jersey.*Excludes Japan and China.
There is a need to initiate treatment sooner following TACE unsuitability
M Peck-Radosavlijevic 2018

20
OPTIMIS: Liver Dysfunction Observed After TACE Treatment
Summary Deterioration
EUROPEN=148(100%)
ASIA* N=156 (100%)
CHINAN=80(100%)
JAPANN=91(100%)
TotalN=475(100%)
Any Parameter 38 (25.7%) 66 (42.3%) 28 (35.0%) 38 (41.8 %) 170 (35.8%)
Alanine Aminotransferase 13 (8.8%) 16 (10.3%) 7 (8.8%) 10 (11.0%) 46 (9.7%)
Albumin 20 (13.5%) 25 (16.0%) 16 (20.0%) 24 (26.4%) 85 ( 17.9%)
Aspartate Aminotransferase 17 (11.5%) 35 (22.4%) 14 (17 .5%) 15 (16.5%) 81 (17.1%)
Bilirubin 12 (8.1%) 26 (16.7%) 13 (16.3%) 2 (2.2%) 53 (1 1.2%)
Prothrombin INR 9 (6.1%) 18 (11.5%) 9 (11.3%) 11 (12.1% ) 47 (9.9%)
Worsening of Lab AE Grade Relevant to the Liver
• After TACE, changes in liver laboratory values are documented
• It is essential to preserve liver function in order to maximize the
treatment potential for systemic therapy
M Peck-Radosavlijevic 2018

21
What is TACE failure?Proposed algorithm based on ART score
Raoul 2014

WILL ADDING SYSTEMIC THERAPY TO TACE IMPROVE OUTCOMES?
Median OS with TACE alone about 20
months
---At least 5 negative trials
Rationale for combining TACE with
sorafenib:
• TACE is not curative and
repeated TACE compromises
the liver function
• TACE recurrence is associated
with upregulation of VEGF and
angiogenesis which sorafenib
can inhibit.
BRISK-TA (TACE +/- brivanib)and ORIENTAL (TACE +/- orantinib) trials negative

COMPARISON OF TACE COMBINATION TRIALSPost-TACE
Phase 3 (n=458)
SPACE
Rand ph2 (n=307)
TACE-2
Phase 3 ( n=399)
TACTICS
Rand ph 2 ( n=156)
Sites Japan/Korea Global (excl Japan) UK ( terminated early) Japan only
CP score A A A A to B7
Inclusion criteria <7cm; < 10 tumors
Responded toTACE
Unresectable Not for resection or
transplant
<10cm
< 10 tumors
TACE used cTACE, on demand DEB-TACE, at3,7 and
13m and then 6mthly
DEB-TACE ,on
demand
cTACE, on demand
Primary end point TTP 5.4m vs 3.7m,
HR 0.87, p=0.252
TTP 5.6 vs 5.5m
HR 0.797, p=0.072
PFS 7.8m vs 7.7m
HR 0.99, p=0.94
PFS 25.2m vs 13.5m
HR 0.59, p=0.006
Secondary endpoint OS 29.7 m, HR1.06
p=0.79
OS not reached,
HR 0.898 , p =0.295
OS 21.1m vs 19.7m
HR0.97, p=0.57
Not reached yet
Definition of PD RECICL2014 mRECIST RECIST1.1 unTACE-able
progression
Sorafenib duration 17 weeks 21 weeks 17.1 weeks 38.7 weeks
Adapted from Kudo, Oncology 2017

Slides courtesy of: Masatoshi Kudo, MD, PhD
Study Schema
Inclusion criteria
・Unresectable HCC
・Child-Pugh score;<7
・Prior TACE; 0-2
・Viable tumor
(<10 nodules , <10cm)
・Adequate organ function
Exclusion criteria
・EHS/MVI
TACESorafenib
(400mg od→400㎎ bid)
UnTACEable progression/
Progression to TACE failure
Ran
do
miz
atio
n (
1:1)
Co-Primary Endpoint
PFS/OS (Gatekeeping strategy)
Secondary Endpoint
TTUP, TTP, ORR
Safety
n=156
• Sorafenib 400mg daily was started 2-3 weeks before 1st TACE to check the tolerability and
to block the VEGF receptors after TACE followed by 800mg daily
• Sorafenib was interrupted 2days before and 3 days after each TACE session as long as
organ function is maintained within TACE re-starting criteria
• Repeated TACE is recommended on demand when viable lesion is more than 50%
compared with baseline tumor volume or in the investigator’s discretion
• Radiological assessment was done every 8 weeks by investigators
Sorafenib arm (n=80)
Control arm (n=76)
Stratification: sites, within Milan, No of prior TACE
4. TACTICS trial

Presented by: Masatoshi Kudo, MD, PhD
Definition of Progression Free Survival (PFS)
Time from the randomization day to the following events:
1. Progression:� Untreatable (UnTACEable) progression
(Defined as inability of a patient to further receive or benefit from TACE)
1) Intrahepatic tumor progression (25% growth, RECICL JSH 20091)*
2) Deterioration of liver function to Child-Pugh C
3) Appearance of extrahepatic spread
4) Appearance of major vascular invasion
(*Note: In this trial new lesion is not regarded as “Tumor progression” since it is not the
treatment failure nor suggesting next line of treatment)
� Progression that meets the TACE failure/refractoriness criteria by JSH definition2
2. Any cause of death
1Kudo M, et al, Hepatol Res. 2010;40:686-692. 2Kudo M, et al. Dig Dis 2011;29:339-364RECICL: Response Evaluation Criteria In Cancer of the Liver JSH: Japan Society of Hepatology
Presented by: Masatoshi Kudo, MD, PhD
Definition of TACE failure/refractoriness (JSH Criteria)1
Intrahepatic lesion
i. Two or more consecutive insufficient responses of the treated tumor (viable
lesion >50%) even after changing the chemotherapeutic agents and/or reanalysis
of the feeding artery seen on response evaluation CT/MRI at 1–3 months after
having adequately performed selective TACE
ii. Two or more consecutive progressions in the liver (tumor number increases as
compared to tumor number before the previous TACE procedure) even after having
changed the chemotherapeutic agents and/or reanalysis of the feeding artery seen
on response evaluation CT/MRI at 1–3 months after having adequately performed
selective TACE
1Kudo M, et al. TACE Failure criteria JSH guideline. Dig Dis 2011;29:339-364
Presented by: Masatoshi Kudo, MD, PhD
Main inclusion / exclusion criteria
• Patients aged 20 years or over
• Life expectancy more than 12 weeks
• Typical HCC by histology, cytology, or diagnostic imaging such as dynamic CT (MRI)
• Unresectable HCC: the maximum diameter <10 cm, and the maximum number <10
• No or 1-2 prior history of TACE therapy before enrollment (prior TACE must be >4 M before)
• ECOG Performance Status (PS) score of 0 or 1
• Child-Pugh score of 7 points or less
Main inclusion criteria
Main exclusion criteria
• Macrovascular invasion (MVI)
• Extrahepatic spread (EHS)

Baseline Patient Characteristics
Characteristics Category
TACE with
Sorafenib
(n=80)
TACE
alone
(n=76)
Median Age at enrollment (range) 72.0(36-85) 73.0(53-86)
Male, n (%) Male 63 (78.8) 55 (72.4)
Female 17 (21.2) 21 (27.6)
Performance status, n(%) 0 71 (88.8) 67 (88.2)
1 9 (11.3) 9 (11.8)
Etiology, n(%) Hepatitis B 10 (12.5) 2 (2.6)
Hepatitis C 38 (47.5) 53 (69.7)
Child-Pugh score , n(%) 5 64 (80.0) 54 (71.1)
6 15 (18.8) 17 (22.4)
7 1 (1.3) 5 (6.6)
AFP, n(%) <200 ng/mL 64 (80.0) 60 (78.9)
≥200 ng/mL 16 (20.0) 16 (21.1)
Characteristics Category
TACE with
Sorafenib
(n=80)
TACE
alone
(n=76)
Tumor burden, n(%) Within Milan 26 (32.5) 31 (40.8)
Over Milan 54 (67.5) 45 (59.2)
BCLC stage, n(%) A 25 (31.3) 30 (39.5)
B 46 (57.5) 37 (48.7)
C 9 (11.3) 9 (11.8)
Prior TACE, n(%) 0 45 (56.3) 48 (63.2)
1-2 35 (43.8) 28 (36.8)
Presented by: Masatoshi Kudo, MD, PhD


POSSIBLE REASONS WHY THESE TRIALS FAILED OR SUCCEEDEDPost-TACE SPACE TACE-2 TACTICS
Mean daily dose of
sorafenib was only
386mg/ day ( 73% dose
reductions and 91%
interruptions)
Three were significant
differences in TTP
between Korean and
Japan cohorts
- Korean patents had
longer duration of
treatment
- Japanese patients
had more lesions
and were more
elderly
Scheduled TACE- could this have
resulted in unnecessary
compromise of liver function or
inadequate TACE in some? E.g.
One-third of those in sorafenib arm
received only 1 x TACE
Asians had better HR than non-
Asians and were also on longer
duration of sorafenib (30 weeks vs
17.4 weeks) and more TACE
- More non-Asians had
unTACEable progression due to
liver function deterioration rather
than lack of response
As RECIST 1.1 used for
determining progression,
new intrahepatic lesionsin
non-TACEd areas were
considered PD
- Does this mean
treatment is not
working and do TACE
trials require a
different definition of
PD
- Should time to TACE
progression ( TTTP)
be used instead?
Different definition of PFS
–and what is considered
TTTP
Longer sorafenib
treatment duration (38.7
weeks) may be the key
of success of this trial
as compared with
previous failed trials
(Post TACE; 17.0 wks,
SPACE; 21.0 wks, TACE
2; 17.1 wks).
these trials suggest that the duration of sorafenib ( +/- TACE
duration) results in better outcomes

� What is optimal duration and frequency of TACE
� What is best method and chemotherapy for TACE
� Do the results of TACTICS apply to everyone else?
UNANSWERED QUESTIONS ABOUT TACE

SIRT (SELECTIVE INTERNAL RADIATION THERAPY)
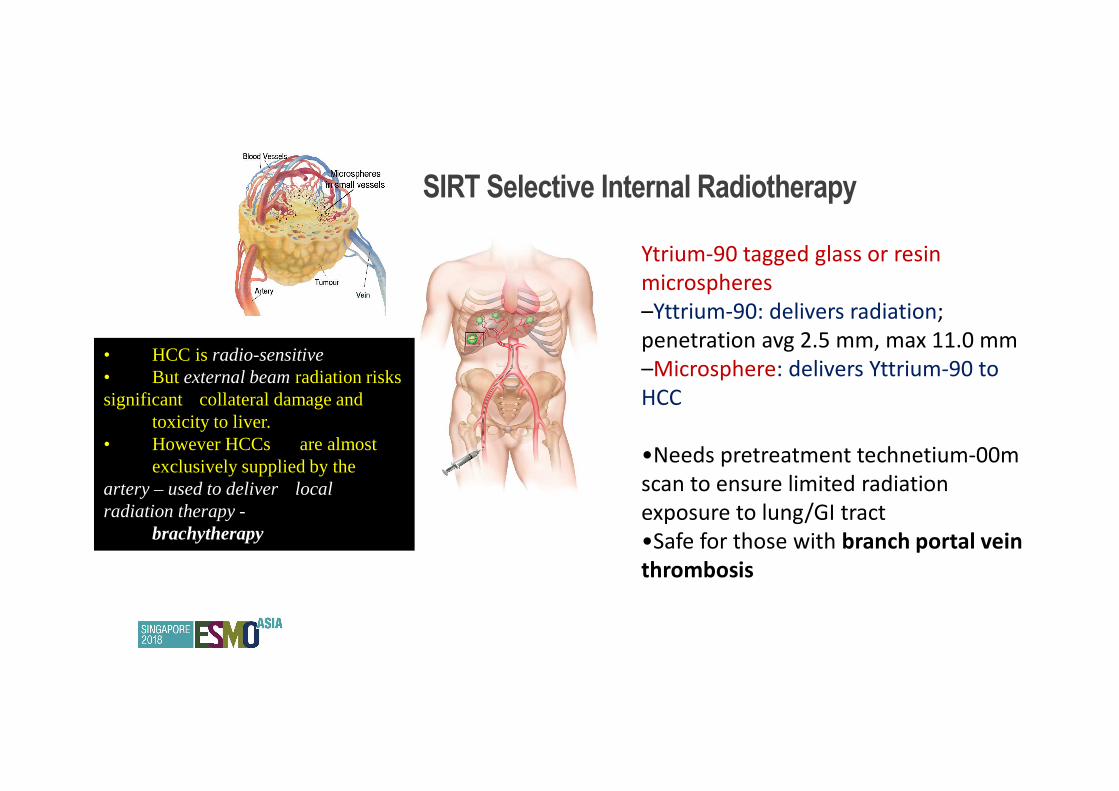
• HCC is radio-sensitive• But external beam radiation risks significant collateral damage and
toxicity to liver.• However HCCs are almost
exclusively supplied by the artery – used to deliver local radiation therapy -
brachytherapy
Ytrium-90 tagged glass or resin
microspheres
–Yttrium-90: delivers radiation;
penetration avg 2.5 mm, max 11.0 mm
–Microsphere: delivers Yttrium-90 to
HCC
•Needs pretreatment technetium-00m
scan to ensure limited radiation
exposure to lung/GI tract
•Safe for those with branch portal vein
thrombosis
SIRT Selective Internal Radiotherapy

�
90Y microspheres in Patients with HCC and PVT

35
SIRT vs TACE
Zhang Y, 2015 Meta-analysis N=8 trials Better OS and TTP
with SIRT vs TACE
Salem R 2016 Randomised phase
2 trial
SIRT vs cTACE in
BCLC A and B HCC
TTP 26m vs 6.8 m
� No randomized phase 3 trials comparing both modalities

36
Slide 14
Presented By Edward Kim at 2018 Gastrointestinal Cancers Symposium
Courtesy
of E Kim

37
Slide 15
Presented By Edward Kim at 2018 Gastrointestinal Cancers Symposium
Courtesy
of E Kim
38
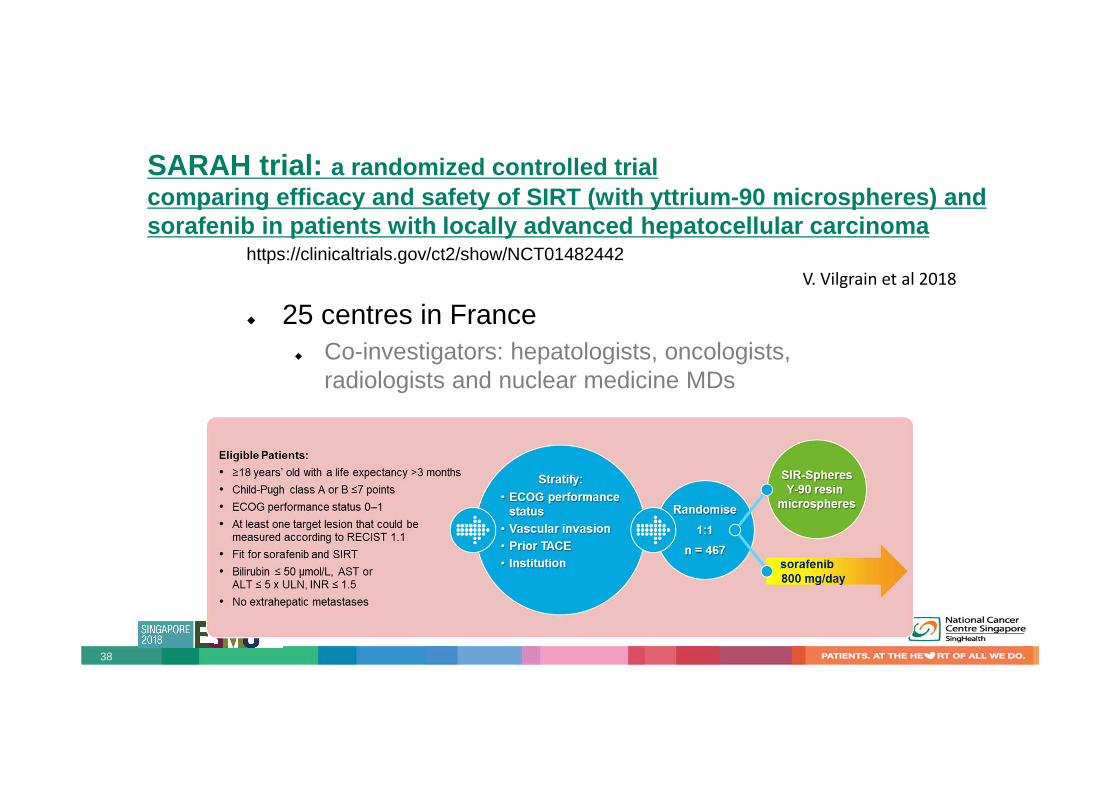
SARAH trial: a randomized controlled trial comparing efficacy and safety of SIRT (with yttrium -90 microspheres) and sorafenib in patients with locally advanced hepatoc ellular carcinoma
https://clinicaltrials.gov/ct2/show/NCT01482442
� 25 centres in France� Co-investigators: hepatologists, oncologists,
radiologists and nuclear medicine MDs
V. Vilgrain et al 2018

39
Study Design and Assessments
Presented By Pierce Chow at 2017 ASCO Annual Meeting
SIRveNIB trial: Phase II multi-centre, open label randomized controlled trial of SIRT versus
sorafenib in locally advanced HCC

40
SARAH vs SIRveNIB : trial endpoints and criteriaSARAH SIRveNIB
Primary Endpoint OS OS
Secondary endpoints Safety and tolerability
QOL
PFS at 6 months
Safety and tolerability
QOL
PFS at 6 months
Inclusion criteria Unresectable HCC
- BCLC C
- BCLC A/B if new lesions or unsuitable for
further radical therapy or no response after
TACEx2
- CP A to B7
- ECOG 0-1
- Fit for sorafenib or SIRT
Unresectable HCC with or without PVT
- BCLC B or C without extrahepatic
metastases
- CP A to B7
- ECOG 0-1
- Fit for sorafenib or SIRT
- Not more than 2 prior hepatic artery
directed therapies
- 26.6% did not get SIRT and 7.2% did not get
sorafenib
- 28.6% did get SIRT and 9% did not get
sorafenib

41
SARAH SIRveNIB
Sample size 467 360
Main PVT 32% 30%
Etiology Alcohol. 68%
HCV. 25%
NASH. 23%
HBV 51%
HCV 14.3%
Both HBV+HCV 2.2%
BCLC stage A/B/C 3.8/ 27.8/ 68.4% 0/ 54.9/ 44.5%
OS SIRT 8m vs sorafenib 9.9m
HR 1.15, p=0.18
SIRT 8.9m vs soraf 10m
HR1.12 , p=0.36
PFS/ TTP PFS 4.3 vs 3.7m
HR0.97, p=0.77
TTP 6.08 vs 5.36m
HR 0.88, p=0.287
ORR ( CR + PR) 19% vs 11.6%, p=0.042 16.5% vs 1.7% , p<0.0001

42
In SARAH: Better QOL with SIRT compared to sorafeni b In SIRveNIB: Better safety profile with SIRT
Intention-To-Treat populationN=459

SCREENING
1⁰ endpointNon-inferiority (1 st step) or superiority (2 nd step) of Primovist-MRI vs. CE-CT
MICRO-Tx SYSTEMIC Tx
Randomise
11:10
n = 375
sorafeni
b
SIR-
Spheres
sorafeni
b
Palliative Group
Local Ablation Group(<4 tumours; <5 cm each)
Randomise
1:1
n = 290
sorafeni
b
placebo
RFA
Contrast-
enhanced CT
Primovist®-
enhanced MRI
Off Study• BCLC 0• BCLC D
Time to Recurrence
Overall Survival
1⁰ endpoint
Assign to
study arm
Imaging Sub-Study
SORAMIC Trial: SchemaEuropean Trial
NEGATIVE trial
SIRT + sorafenib vs sorafenib: OS
12.1m vs 11.5m
44
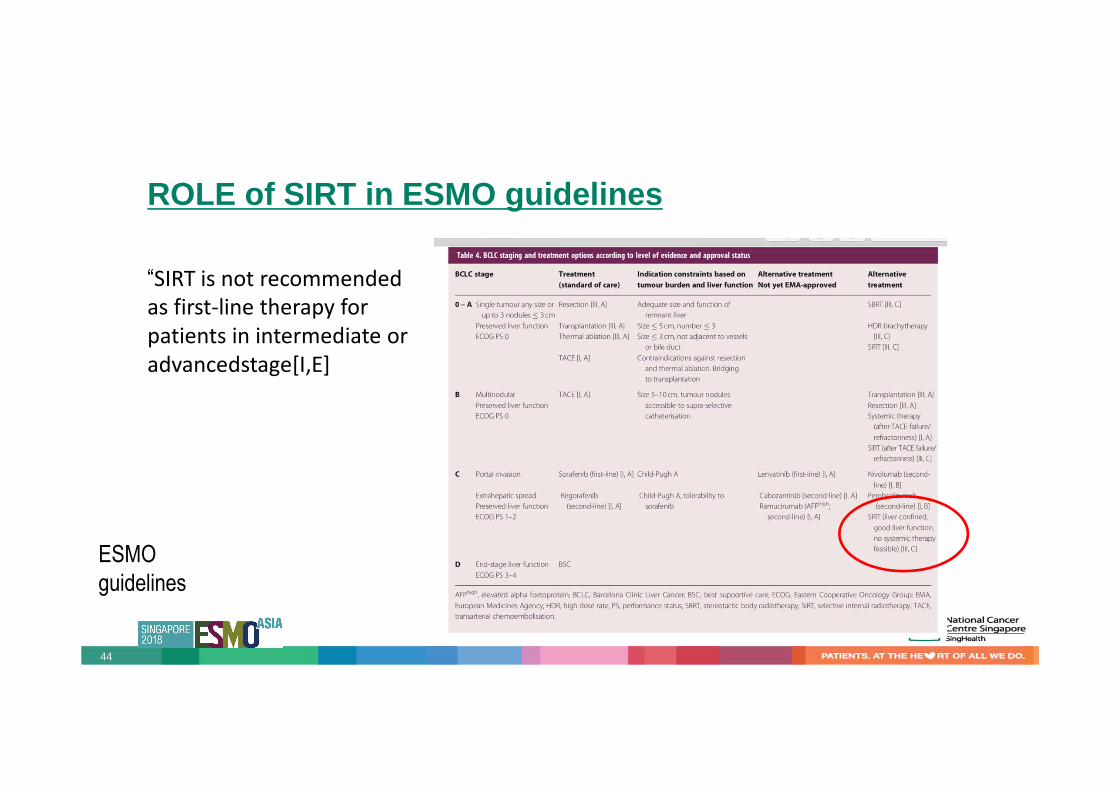
ROLE of SIRT in ESMO guidelines
ESMO
guidelines
“SIRT is not recommended
as first-line therapy for
patients in intermediate or
advancedstage[I,E]
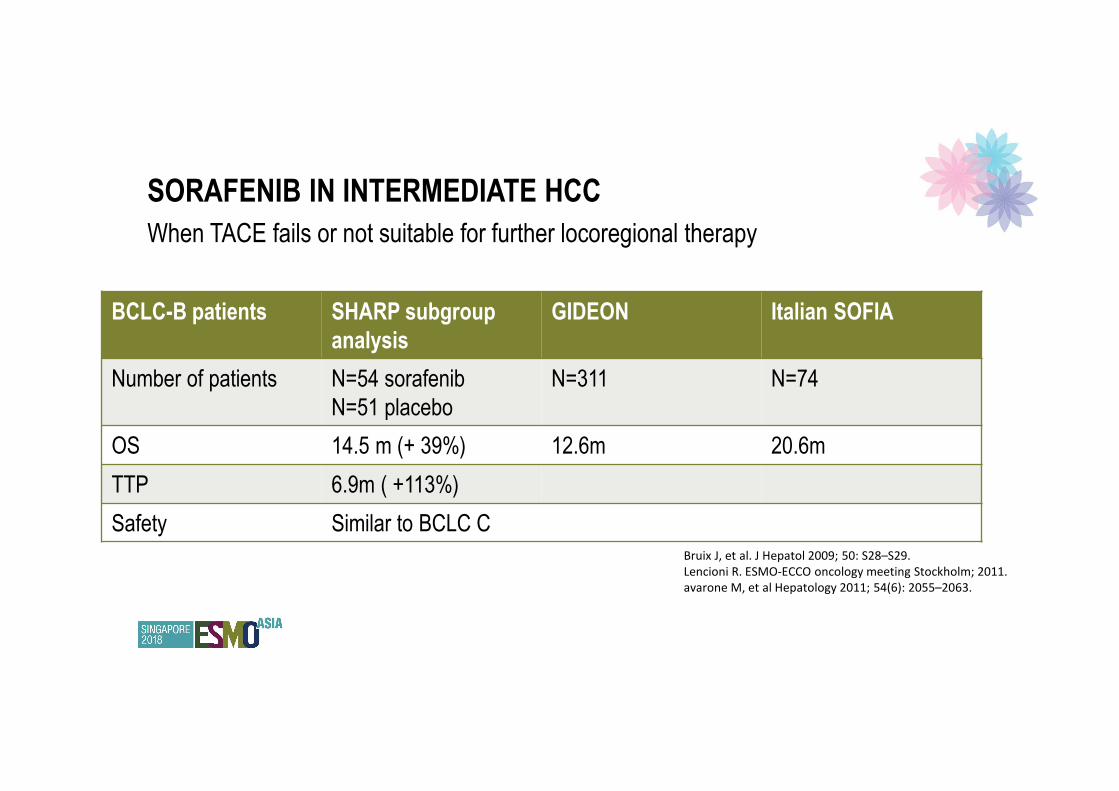
SORAFENIB IN INTERMEDIATE HCC
When TACE fails or not suitable for further locoregional therapy
Bruix J, et al. J Hepatol 2009; 50: S28–S29.
Lencioni R. ESMO-ECCO oncology meeting Stockholm; 2011.
avarone M, et al Hepatology 2011; 54(6): 2055–2063.
BCLC-B patients SHARP subgroup
analysis
GIDEON Italian SOFIA
Number of patients N=54 sorafenib
N=51 placebo
N=311 N=74
OS 14.5 m (+ 39%) 12.6m 20.6m
TTP 6.9m ( +113%)
Safety Similar to BCLC C

ESMO GUIDELINES FOR HCC

FUTURE FOR INTERMEDIATE HCC
- Combining locoregional therapy with newer TKIs or immuno-oncology
agents
- Starting systemic therapy earlier in the treatment algorithm with increasing
evidence of good outcomes with newer systemic therapies and limits of
TACE
NCT03143270 A Multicenter Pilot Study of Nivolumab With Drug
Eluting Bead Transarterial Chemoembolization in
Patients With Advanced Hepatocellular
Carcinoma
Cohort 1:TACE – nivolumab 2 weeks later
Cohort 2: nivolumab 4 weeks before TACE –then nivo
continued x 1 year (No dosing on TACE day)
Cohort 3: nivolumab 4 weeks before TACE –then nivo
continued x 1 year ( Dosing on TACE day)
USA
NCT02837029 Phase I/Ib Study of Nivolumab in Combination With
Therasphere (Yttrium-90) in Patients With
Advanced Hepatocellular Carcinoma
Therasphere – nivolumab 4 weeks later USA
NCT03099564 A Pilot Study of Pembrolizumab in Combination
With Y90 Radioembolization in Subjects With
Poor Prognosis Hepatocellular Carcinoma With
Preserved Liver Function
SIRspheres –pembrolizumab 1 week later USA
NCT03203304 Phase I Study of Stereotactic Body Radiotherapy
(SBRT) Followed by Nivolumab or Ipilimumab
With Nivolumab in Unresectable Hepatocellular
Carcinoma
40Gy – nivolumab or nivolumab + ipilumumab 2 weeks
later
USA
NCT02821754 A Pilot Study of Combined Immune Checkpoint
Inhibition in Combination With Ablative Therapies
in Subjects With Hepatocellular Carcinoma
(HCC) or Biliary Tract Carcinomas (BTC)
Tremelimumab + Durvalumab with RFA or TACe or
cryoablation
USA
NCT03316872 Pembrolizumab and Stereotactic Radiotherapy
Combined in Subjects With Advanced
Hepatocellular Carcinoma - A Phase II Study
Pembrlizumab – SBRT from day 2 Canada
48
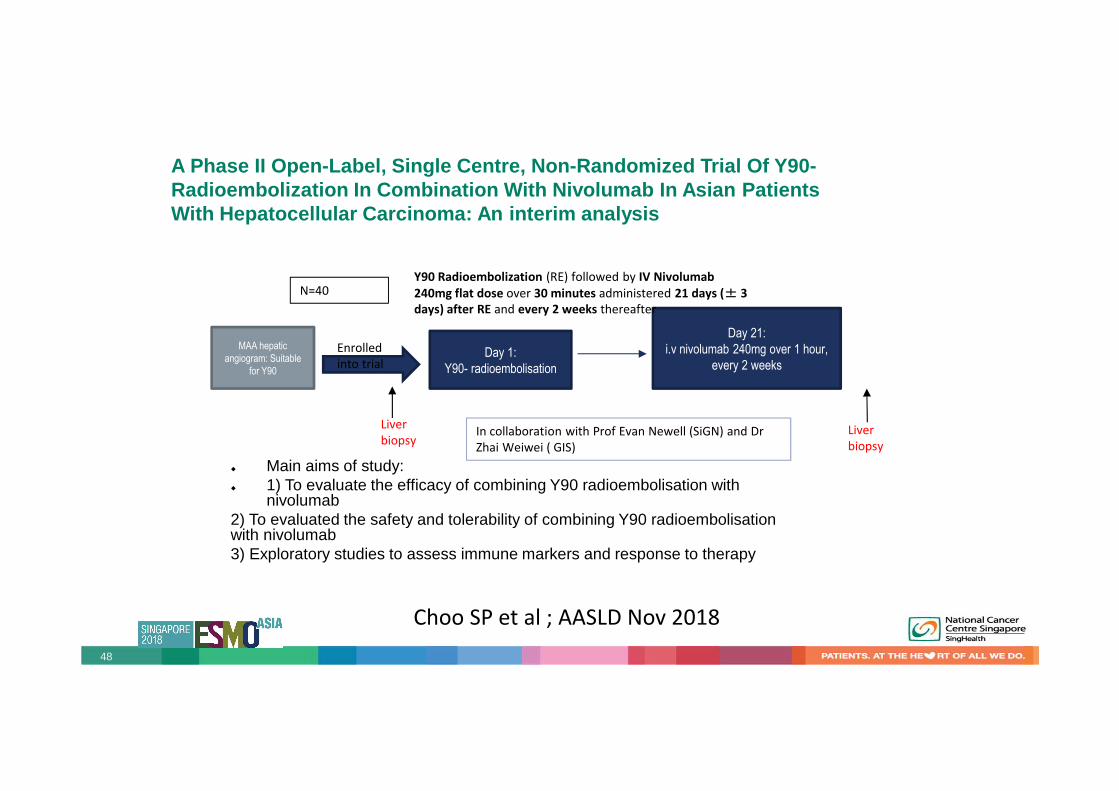
A Phase II Open-Label, Single Centre, Non-Randomize d Trial Of Y90-Radioembolization In Combination With Nivolumab In Asian Patients With Hepatocellular Carcinoma: An interim analysis
� Main aims of study: � 1) To evaluate the efficacy of combining Y90 radioembolisation with
nivolumab2) To evaluated the safety and tolerability of combining Y90 radioembolisationwith nivolumab3) Exploratory studies to assess immune markers and response to therapy
Day 1:
Y90- radioembolisation
Day 21:
i.v nivolumab 240mg over 1 hour,
every 2 weeks
MAA hepatic
angiogram: Suitable
for Y90
Enrolled
into trial
Liver
biopsyLiver
biopsy
Y90 Radioembolization (RE) followed by IV Nivolumab
240mg flat dose over 30 minutes administered 21 days (± 3
days) after RE and every 2 weeks thereafter
N=40
In collaboration with Prof Evan Newell (SiGN) and Dr
Zhai Weiwei ( GIS)
Choo SP et al ; AASLD Nov 2018

SHOULD WE BE STARTING SYSTEMIC THERAPY EARLIER IN
INTERMEDIATE HCC?
Galle 2017
Potentail new
therapeutic options
as other therapies
prove to be more
efficacious

CONCLUSION
• TACE is still the standard of care for intermediate HCC with good liver function
• In patients with TACE failure, PVT or poorer liver function , systemic therapy
should be given
• While SIRT resulted in better ORR, it did not result in better OS compared to
sorafenib. Thus role of SIRT is largely for very selected patients who are not
suitable for TACE or sorafenib ( not everyone agrees with this)
• Treatment of intermediate HCC will evolve as results from combination trials
become available
THANK YOU
For fellows and junior consultants
interested in clinical research:
SSO-ACORD Trial Concept
Development Workshop
4th July 2019
- Look out for submission date for
1-page study proposals
- Check out Singapore Society of
Oncology website and facebook