inter-agency care planning the eicd / darebin community health perspective carolyn hines manager –...
TRANSCRIPT

Inter-Agency Care Planning
The EICD / Darebin Community Health perspective
Carolyn Hines
Manager – Chronic and Complex Care Program

Today’s presentation
• The Early Intervention in Chronic Disease (EICD) program model (Health Wise)
• Health Wise and inter-agency care planning
• Issues and challenges
• The way forward

Background• Care planning at DCH
- Some discipline-specific care planning for internal use only
- Inter-agency care planning is limited - Specific to certain programs eg HARP
• HARP- Austin Health, St Vincent’s, Northern Health - Inter-agency care planning occurs to varying
degrees• Early Intervention in Chronic Disease (EICD)
- Health Wise- Care planning is in development stage
LEVEL 4
LEVEL 3
LEVEL 2
LEVEL 1
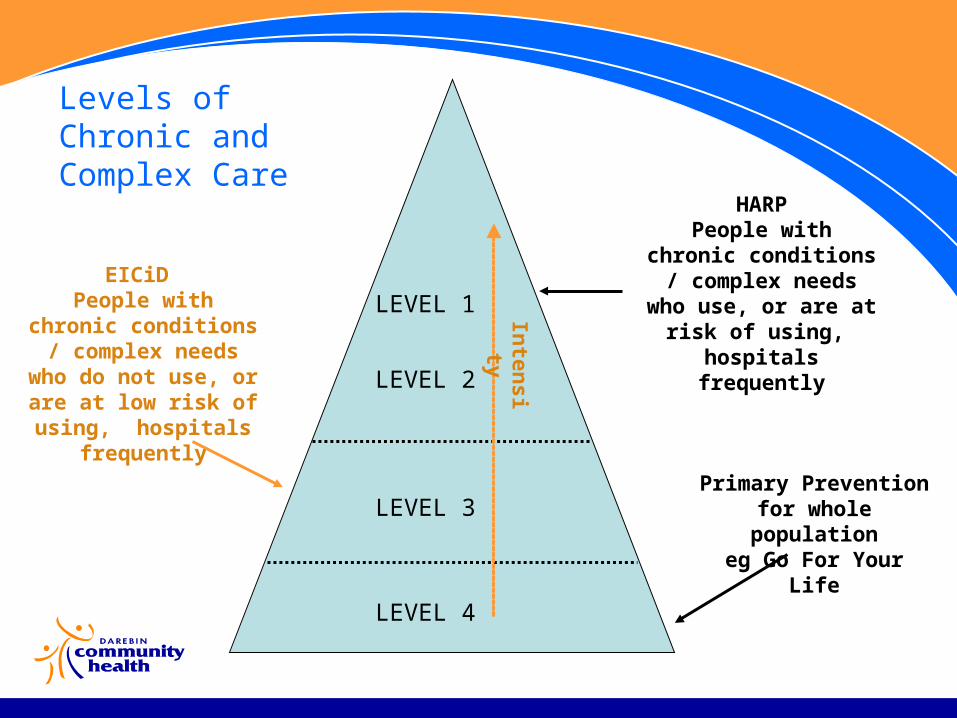
Levels of Chronic and Complex Care
Primary Prevention for whole population
eg Go For Your Life
HARPPeople with chronic conditions / complex
needs who use, or are at risk of using,
hospitals frequently
EICiD People with chronic conditions / complex
needs who do not use, or are at low risk of
using, hospitals frequently
Inten
sity
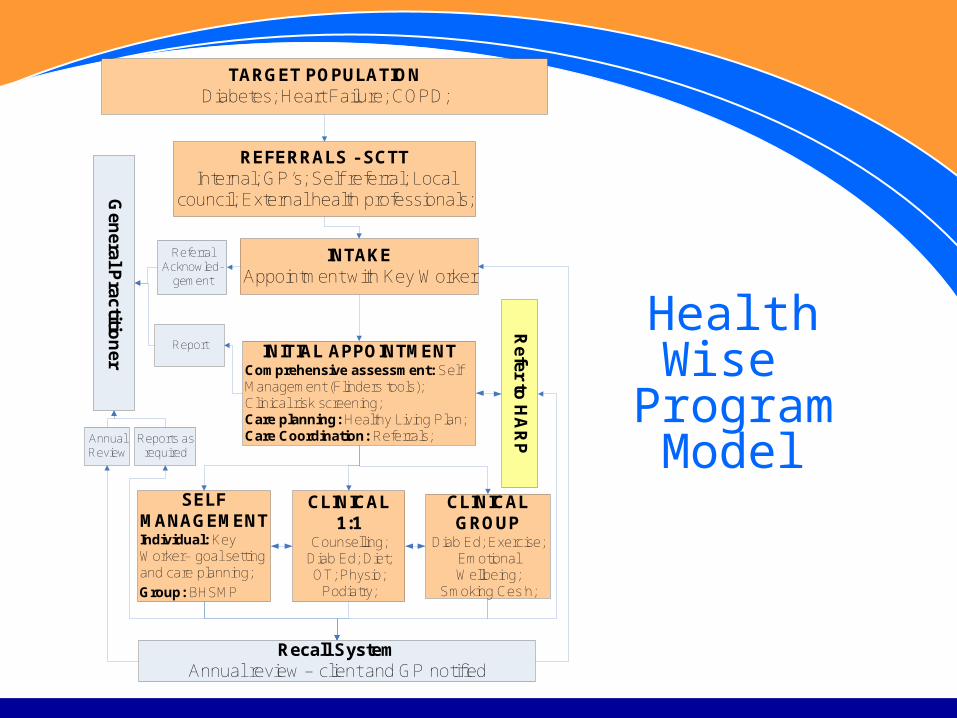
Health Wise Program
Model
INITIAL APPOINTMENTComprehensive assessment: Self Management (Flinders tools); Clinical risk screening;Care planning: Healthy Living Plan; Care Coordination: Referrals;
REFERRALS - SCTT Internal; GP’s; Self referral; Local
council; External health professionals;
INTAKEAppointment with Key Worker
SELF MANAGEMENTIndividual: Key Worker– goal setting and care planning;
Group: BHSMP
Refer to
HA
RP
TARGET POPULATIONDiabetes; Heart Failure; COPD;
CLINICAL 1:1
Counselling; Diab Ed; Diet; OT; Physio;
Podiatry;
CLINICALGROUP
Diab Ed; Exercise; Emotional Wellbeing;
Smoking Ces’n;
Recall SystemAnnual review – client and GP notified
Gen
eral Practitio
ner
Referral Acknowled-
gement
Report
Reports as required
Annual Review

Key Worker role
• Comprehensive assessment - general chronic disease screening, self management assessment (Flinders), Client Survey (DHS)
• Preparation of a Healthy Living Care Plan based on self management needs / goals (Flinders)
• Further appointments with KW for 1:1 self management; referral to other services (internal or external) as required
• The main point of contact for client and GP • Extent of involvement with each client will vary according to
needs

Healthy Living Care PlanFlinders Care Plan V9 April 06
Client Problem Statement: This Problem interferes with my daily activities 0 1 2 3 4 5 6 7 8 does not slightly definitely often severely
Client Goal/s: My progress towards achieving this goal 0 1 2 3 4 5 6 7 8100% 75% 50% 25% no success
IDENTIFIED ISSUES [INCLUDING SELF
MANAGEMENT]
MANAGEMENT AIMS
INTERVENTION WHO IS RESPONSIBLE
DATE REVIEWED
PROGRESS (eg no progress, some
progress, completed)
Sign Off - PatientI ……………………………………(patient name) agree that the information contained within this care plan is true and correct and currently reflects my needs for the forthcoming year. Additionally, I consent to this information relevant to my care will be released to my health providers.
Signature: ………………………………….. Date: ………/………/………Sign Off - DoctorI ……………………………………(GP name) agree that the services prescribed within this care plan are true and correct at the time of development but are subject to review based on the patient's needs and / or my professional opinion as the responsible Medical Practitioner. Provider No:[ ] [ ] [ ] [ ] [ ] [ ] [ ] Date: ………/………/………
Care Plan Review Date: ………/………/……… Signature: ………………………..… MBS ITEM: GP Management Plan - 721
Team Care Arrangements - 723

INITIAL APPOINTMENTComprehensive assessment: Self Management (Flinders tools); Clinical risk screening;Care planning: Healthy Living Plan; Care Coordination: Referrals;
REFERRALS - SCTT Internal; GP’s; Self referral; Local
council; External health professionals;
INTAKEAppointment with Key Worker
SELF MANAGEMENTIndividual: Key Worker– goal setting and care planning;
Group: BHSMP
Refer to
HA
RP
TARGET POPULATIONDiabetes; Heart Failure; COPD;
CLINICAL 1:1
Counselling; Diab Ed; Diet; OT; Physio;
Podiatry;
CLINICALGROUP
Diab Ed; Exercise; Emotional Wellbeing;
Smoking Ces’n;
Recall SystemAnnual review – client and GP notified
Gen
eral Practitio
ner
Referral Acknowled-
gement
Report
Reports as required
Annual Review
The HARP / EICD interface
The GP / EICD Interface
Health Wise and inter-agency care planningFocus will be:• General practitioners• HARP programs and other external organisations /
programs• Internal service providers
- Maintain communication - Streamline client care

Health Wise and inter-agency care planning (cont)Progress to date:• Working group has been established with staff from
EICD project the DCH Medical Practice (GP, Practice Nurse, Chronic Condition Practice Coordinator)
• Started investigating care planning options- Service Coordination Plan - HARP

Community Care Plan
Coordinator: GP: Other care provider:
Phone: 9290 6615 Phone: Phone:
Fax: 9290 6650 Fax: Fax:
Client’s address and phone number (if different to usual):
Participants and Service Provider Details
Name Position Contact Details Date
Helen Glouftsis Cardiac Nurse 9290 6615
Community Care Plan
UR NO:Surname: Given Names: DOB: Sex:
Authority to proceed with care planThe purpose of this care plan has been explained. I/my carer, give permission for its preparation and for the discussion of my medical history and diagnosis, with the providers listed above.All participants are to retain confidentiality.I/my carer have been asked if any medical/personal information should be withheld from other participantsI am aware that my GP will bill me in their usual way for their participation and that a Medicare rebate is available for this service
Signature: Helen Glouftsis Date: Client / Carer / Verbal (please circle)
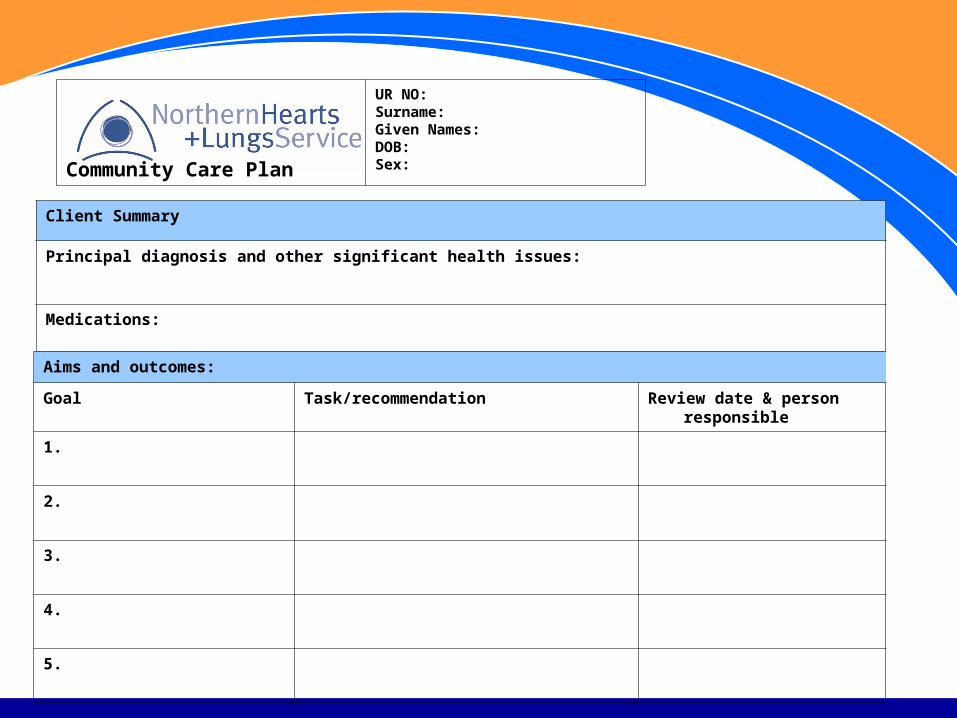
Community Care Plan
UR NO:Surname: Given Names: DOB: Sex:
Client Summary
Principal diagnosis and other significant health issues:
Medications:
Aims and outcomes:
Goal Task/recommendation Review date & person responsible
1.
2.
3.
4.
5.

Issues / challenges• Multiple options available• Multiple views about the ideal care plan• Terminology - medical care plans, service coordination
plans, community care plans…………. • Commitment to self-management - need to incorporate
client-centred goals• Don’t want to reinvent the wheel!

What do we need?• We can’t do it alone!• Small EICD project managers network but cuts across
different regions • Regional approach (state-wide)
- Support and leadership from DHS- Bring service providers / Divisions of General
Practice together to establish definitions, common needs, standard care plan format/s
- Strategy to promote the “why” and “how” to agencies / staff