intelligent prescribing - mm3 admin€¦ · taylor, santosh & swanson (2002) submitted...
TRANSCRIPT

Optimizing Medication Treatments in ADHD
Dr Dave Coghill
Intelligent Prescribing

Source Consultant AdvisoryBoard
Stock Equity
>$10,000
SpeakerResearch
Lilly X X X
Janssen/McNeil
X X X
UCB X X
Shire X X X
Medikinet/ Flynn
X X
NHS: HTAMHRN
XX

• Severe, pervasive, disabling?
• Problems at home?• Problems at school?
• Persistent after treatment?
• Comorbid problems?
Home CBT
Liaison+ self-instruction
Medication
Taylor, Santosh & Swanson (2002) submitted
Treatment Decisions

• Severe, pervasive, disabling?
• Problems at home?• Problems at school?
• Persistent after treatment?
• Comorbid problems?
Home CBT
Liaison+ self-instruction
Medication
Taylor, Santosh & Swanson (2002) submitted
Treatment Decisions

• Severe, pervasive, disabling?
• Problems at home?• Problems at school?
• Persistent after treatment?
• Comorbid problems?
Home CBT
Liaison+ self-instruction
Medication
Taylor, Santosh & Swanson (2002) submitted
Treatment Decisions

• Severe, pervasive, disabling?
• Problems at home?• Problems at school?
• Persistent after treatment?
• Comorbid problems?
Home CBT
Liaison+ self-instruction
Medication
Taylor, Santosh & Swanson (2002) submitted
Treatment Decisions

• Severe, pervasive, disabling?
• Problems at home?• Problems at school?
• Persistent after treatment?
• Comorbid problems?
Home CBT
Liaison+ self-instruction
Medication
Taylor, Santosh & Swanson (2002) submitted
Treatment Decisions

ADHDResponse to Stimulants
0
10
20
30
40
Best Response(Percent)
Dextroamphetamine Methylphenidate Equal response to either stimulant
Meta-analysis of within-subject comparative trials evaluating response to stimulant medications
36%
26%
38%
Greenhill et al. JAACAP 1996;35:1304.
About 70% of patients respond to methylphenidate, 70% respond to amfetamineand overall 95% respond to one or the other

Response Analysis: LYBI (≥40% Reduction in ADHD RS Total Score)
Respondersto ATX
Nonrespondersto ATX Total
Responders to OROS® 76 24 100
Nonrespondersto OROS 29 35 64
Total 105 59 164
p<.001, Fisher’s exact test
Patients with at least one week on ATX
About 40% of patients who do not respond to stimulants, do respond to atomoxetine
NICE 2006
• The decision regarding which drug to use should be based on the following: – the presence of comorbid conditions (for example, tic disorders, Tourette’s syndrome, epilepsy)
– the different adverse effects of the drugs
– specific issues regarding compliance for example problems created by the need to administer a mid‐day treatment dose at school
– the potential for drug diversion and/or misuse
– the preferences of the child/adolescent and/or his or her parent or guardian.

NICE 2008• Methylphenidate should be the first‐line drug used in pharmacological treatment of ADHD as this has the largest evidence base.
• Atomoxetine is useful as a second‐line drug for those who do not respond to, or have problems with, methylphenidate, and as a first‐line agent in some instances.
• Antipsychotics are not recommended in the treatment of ADHD.
Attention deficit hyperactivity disorder: Diagnosis and management of ADHD in children, young people and adults - NICE guideline Draft for consultation, January 2008

NICE 2008
• When prescribing methylphenidate for the treatment of children or young people, modified release (MR) preparations should be considered for; – Convenience
– Improving adherence
– Reducing stigma (because the child does not need to take medication at school)
– Reducing the problems schools have in storing and dispensing a controlled drug
– Because of its smoother pharmacokinetic profile.
Attention deficit hyperactivity disorder: Diagnosis and management of ADHD in children, young people and adults - NICE guideline Draft for consultation, January 2008

NICE 2008
• Atomoxetine is generally used as a second‐line treatment, but may be considered as a first‐line treatment in the following circumstances: – Comorbid tics or Tourette’s disorder
– Comorbid anxiety disorder
– Comorbid stimulant substance misuse.
Attention deficit hyperactivity disorder: Diagnosis and management of ADHD in children, young people and adults - NICE guideline Draft for consultation, January 2008

Initiating Treatment
• Psychoeducation• Focussing on desired outcome and target symptoms
• Importance of using standardised ratings and recording baseline information
• Methylphenidate titration strategies– Forced dose– Single dose trials– Starting with long‐acting preparations
• Atomoxetine titration strategies

Psychoeducation
• About the disorder and treatment options
• About the specific pharmacological interventions and important issues associated with their use
• What is and is not known
• Time to response• “paracetamol” model
• Beliefs about medication
• Fears about addiction

The process of pharmacotherapy
• Assessment, diagnosis, target symptoms
• Choose medication– Algorithm approach– Baseline measurements
• Determine starting dose, initial target dose and how to get there– Look at the literature– Take advice– “Start low go slow” but not to slow
• When reach initial target dose wait expected length of time for therapeutic response to occur– Remember that different effects take different times– Adverse events often arise earlier than therapeutic effects
Target Symptoms and Problems
• Core ADHD symptoms
• Behaviour in the home
• Classroom behaviour
• Academic functioning
• Peer group relationships
• Associated symptoms – rage, oppositionality etc.

Forced Dose Titration ‐ Dundee
• 4 week titration with weekly dose increments• Baseline and weekly monitoring conducted by nurses• Standardised forms and assessments
– 10 item Connors‐P & Connors‐T– ADHD‐RS ‐ clinician scored– CGI‐S & CGI‐I – clinician scored– Side effects – may be better rated as “other symptoms”
• End of titration – Dr and nurse joint visit
Maximum Benefit – Minimum Dose

Other symptomsNot
presentPresent but
not impairing
Present and impairing
Present and severely impairing
Write note↓
Insomnia or trouble sleeping 0 1 2 3Nightmares 0 1 2 3Drowsiness 0 1 2 3Nausea 0 1 2 3Anorexia (Less hungry than other children)
0 1 2 3
Stomach-aches 0 1 2 3Headaches 0 1 2 3Dizziness 0 1 2 3Sad/unhappy 0 1 2 3Prone to crying 0 1 2 3Irritable 0 1 2 3Thoughts of self-harm 0 1 2 3Suicidal ideation 0 1 2 3Euphoric/unusually happy 0 1 2 3Anxious 0 1 2 3Tics or nervous movements 0 1 2 3“Spaced-out” / “Zombie-like” 0 1 2 3Less talkative than other children 0 1 2 3Less sociable than other children 0 1 2 3

Forced Titration
0
2
4
6
8
10
ADHD‐RSHyp/Imp
ADHD‐RSInatt
CTRS CGAS Low Mood Irritability
Baseline
5mg tds
10mg tds
15mg tds
20mg tds

Single dose trials of MPH
• 5mg on weekend/holiday morning. Parents introduce cognitively demanding task 1 hour later, observe general effect
• 10 mg on another weekend/holiday morning• (15mg on another in teenagers)
Parents draw conclusion as to tolerance and likely effect. If favourable can discuss with prescriber, extend to mornings only during school week with e.g. CTRS‐R, comparing a.m. vs p.m.

Two models for introducing atomoxetine
1. Traditional0.5 mg/kg/day for 7 days, then 1.2 mg/kg/day
2. “German”7‐14 days each of 10 mg, 18, mg, 25 mg and so on following capsule size aiming for 1.2 mg/kg/day
In both instances hang on at 1.2 mg/kg/day for at least 8 (preferably 12) weeks before either giving up or
increasing dose


Monitoring ongoing treatment
• Teamwork
• Coherent and consistent protocols
• Routine measurement
• Identification of “other problems”
• Remember the importance of concordance and adherence

Team Treatment
• Multimodal treatments are often the most appropriate, and one person generally can not do it all
• The team must be mutually supportive
• Don’t underestimate the role/task of the pharmacotherapist

Measurement
• Clinical improvement– Diagnostic specific symptoms– Associated symptoms– Global measures
• Combine observer rated and patient rated measures but don’t assume they measure the same things
USE APPROPRIATE VALID INSTRUMENTS AT APPROPRIATE TIMES
Continuing Care – Dundee Protocol
• Regular follow up appointments by doctor and nurse, particularly at the outset of treatment and for those with complex comorbidity
• Main aims are – to monitor medication– Identify “other problems” which require further assessment / treatment
• The continued routine use of standardised– Data capture proforma– Assessment tools
• ADHD‐RS• CGI‐S & CGI‐I• Side effects
• Teacher Conners before each appointment
• Record weight, height and BP at least six monthly

OPTIMISING TREATMENT WITH LONG ACTING STIMULANT PREPARATIONS

If...If ...you are going to start an extended‐
release stimulant preparation how
do you decide which one to use?
ANSWER
The one that best suits that child at that time
This will depend on pharmacodynamic profile This is determined by:• Methylphenidate or Amfetamine• Proportions IR/ER• Duration of action• Delivery mechanism
Methylphenidate – Concerta XL, Equasym XL / Metadate CD, Medikinet Retard
Duration of action • Equasym XL, Medikinet Retard = 8 hours
• Concerta XL = 12 hours
IR / ER proportions• Concerta XL = 22 / 78 %
• Equasym XL = 30 / 70 %
• Medikinet Retard = 50 / 50 %
Banaschewski T et al., Eur Child Adolesc Psychiatry 2006;15(8):476-495
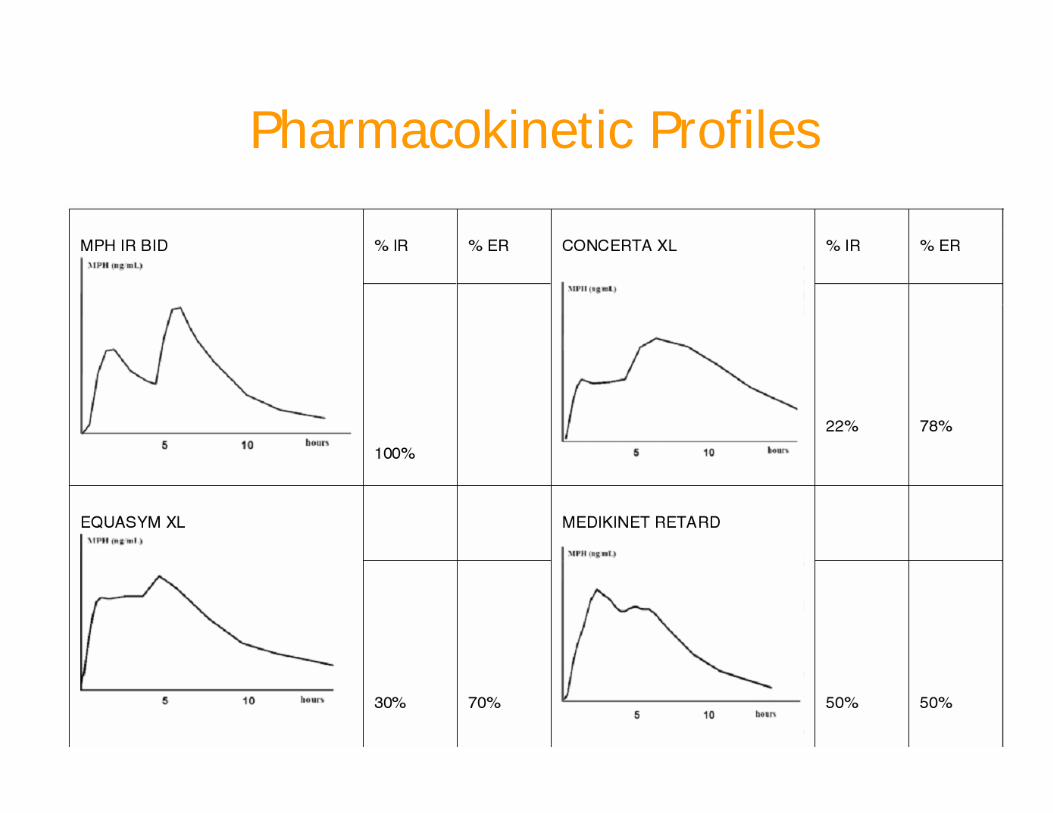
Pharmacokinetic ProfilesBanaschewski T et al. Eur Child Adol Psych 2006
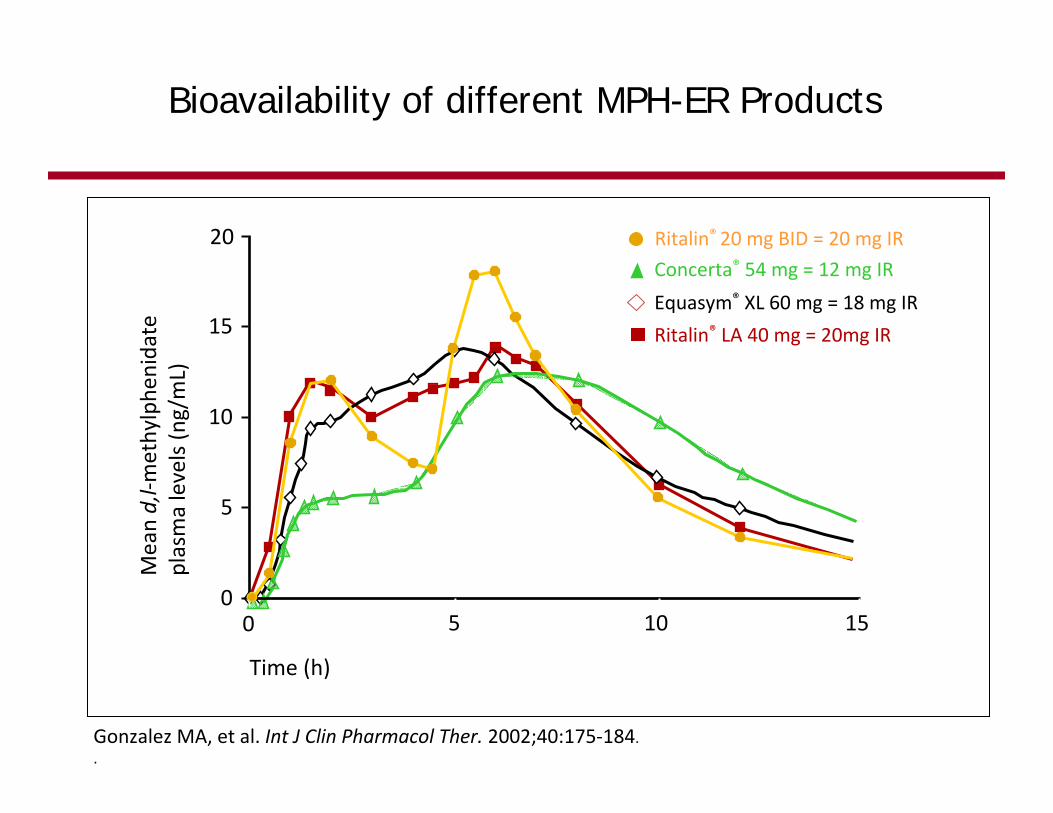
Ritalin® LA 40 mg = 20mg IR
Equasym® XL 60 mg = 18 mg IR
Concerta® 54 mg = 12 mg IR
Time (h)
0 5 10 150
5
10
15
20
Mean d,l‐m
ethylphe
nidate
plasma levels (n
g/mL)
Bioavailability of different MPH-ER Products
Ritalin® 20 mg BID = 20 mg IR
Gonzalez MA, et al. Int J Clin Pharmacol Ther. 2002;40:175‐184..
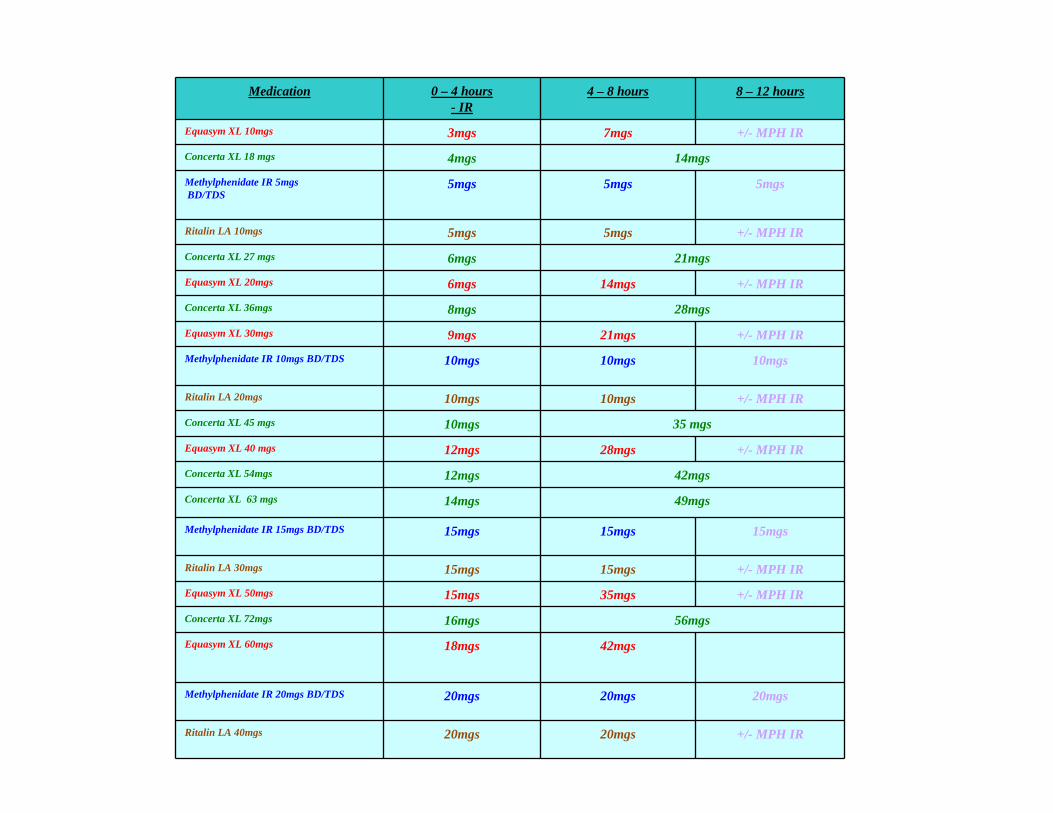
Medication 0 – 4 hours- IR
4 – 8 hours 8 – 12 hours
Equasym XL 10mgs 3mgs 7mgs +/- MPH IR
Concerta XL 18 mgs 4mgs 14mgs
Methylphenidate IR 5mgsBD/TDS
5mgs 5mgs 5mgs
Ritalin LA 10mgs 5mgs 5mgs +/- MPH IR
Concerta XL 27 mgs 6mgs 21mgs
Equasym XL 20mgs 6mgs 14mgs +/- MPH IR
Concerta XL 36mgs 8mgs 28mgs
Equasym XL 30mgs 9mgs 21mgs +/- MPH IR
Methylphenidate IR 10mgs BD/TDS 10mgs 10mgs 10mgs
Ritalin LA 20mgs 10mgs 10mgs +/- MPH IR
Concerta XL 45 mgs 10mgs 35 mgs
Equasym XL 40 mgs 12mgs 28mgs +/- MPH IR
Concerta XL 54mgs 12mgs 42mgs
Concerta XL 63 mgs 14mgs 49mgs
Methylphenidate IR 15mgs BD/TDS 15mgs 15mgs 15mgs
Ritalin LA 30mgs 15mgs 15mgs +/- MPH IR
Equasym XL 50mgs 15mgs 35mgs +/- MPH IR
Concerta XL 72mgs 16mgs 56mgs
Equasym XL 60mgs 18mgs 42mgs
Methylphenidate IR 20mgs BD/TDS 20mgs 20mgs 20mgs
Ritalin LA 40mgs 20mgs 20mgs +/- MPH IR
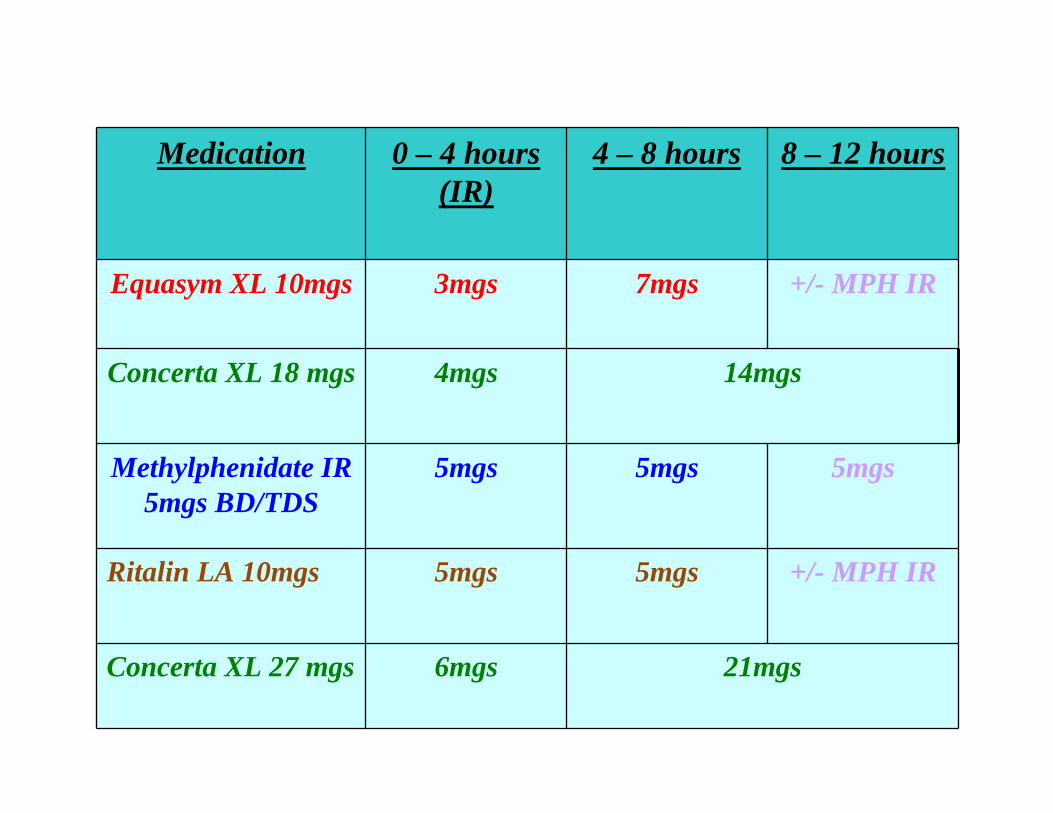
Medication 0 – 4 hours(IR)
4 – 8 hours 8 – 12 hours
Equasym XL 10mgs 3mgs 7mgs +/- MPH IR
Concerta XL 18 mgs 4mgs 14mgs
Methylphenidate IR 5mgs BD/TDS
5mgs 5mgs 5mgs
Ritalin LA 10mgs 5mgs 5mgs +/- MPH IR
Concerta XL 27 mgs 6mgs 21mgs


XX X
X
X
XX X
X X
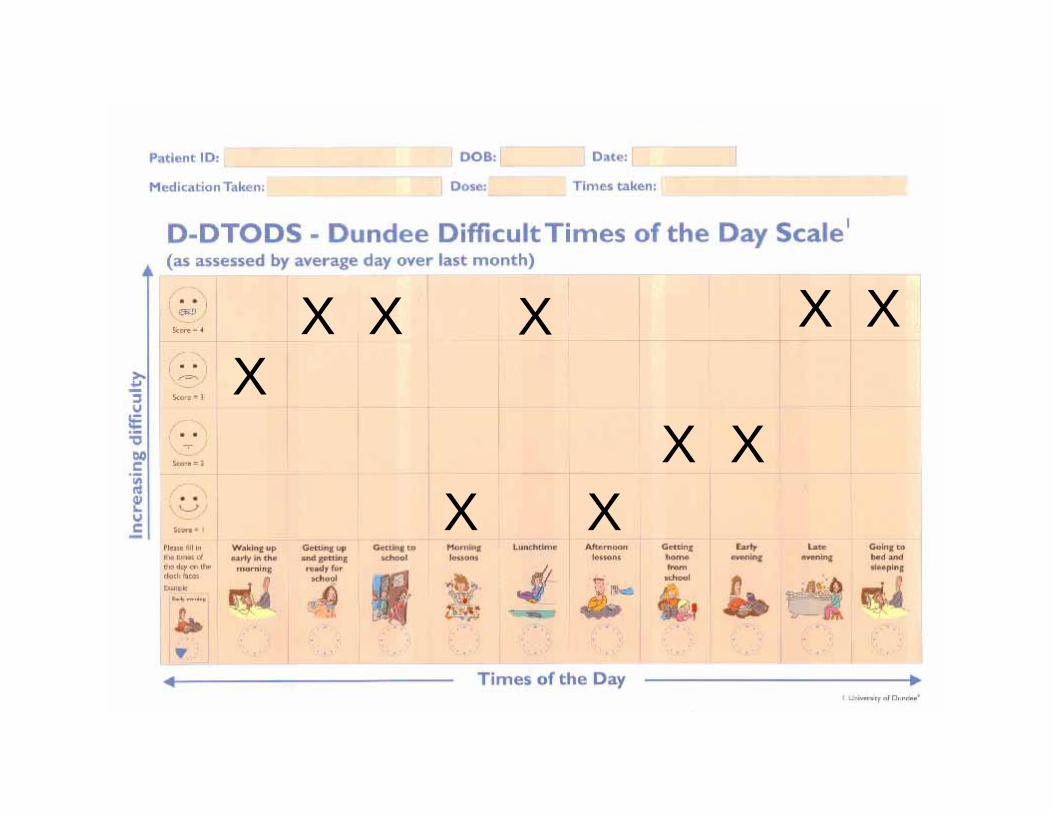
Lunchtime
Even after a settled morning seems to be getting into constant bother in playground and at dinner. School observation suggests this is due to breakthrough symptoms rather than any psychosocial probs.
Peers avoiding contact, often kept in at breaktime
Problems at weekend as haingdifficulties at football
Switch from IR MPH to either Concerta to see if helps to manage breakthrough symptoms

XX
X
X
X
XX X
X X


Changing Treatments
• Ensuring optimization of current treatment
• Switching treatment
• Combining different formulations
• Combining different medications

Questions you could ask before changing to a different drug
• Have I titrated properly?• Is this drug/preparation working well at any times during the
day?• Have I got good enough information from school• Are parents and school in agreement about the effects of the
drug?• Am I targeting the right symptoms?• Is there a behavioural explanation for the drug “wearing off”• What else is going on in patients life / family life?• Is the medication working but effects limited by side effects?• Have I missed any comorbidity?• Is the diagnosis right?

European Guidelines Summary of results
IR stimulants ER stimulants Atomoxetine
Efficacy● Effect sizes● Numbers needed to
treat
++++
++++
+++
Efficacy duration + ++ ++
Compliance + ++ (?) ++ (?)
Dosing flexibility ++ + +
Abuse potential ++D-AMP: +++
+ (?) -
Costs - - - - -

European Guidelines Summary of recommendations
• If a child responded to immediate‐release methylphenidate there could be reasons to move them to extended‐release
• If a child had an adverse event on methylphenidate then next step often to move to atomoxetine
• If a child has failed to respond to methylphenidate, the next option may be dexamfetamine or atomoxetine
• Choice of extended‐release preparation will depend on profile of action over time