influence of dorzolamide on corneal thickness, endothelial cell count and corneal sensibility
TRANSCRIPT
A O S 1998
78
Influence of dorzolamide oncorneal thickness, endothelial cellcount and corneal sensibilityStephan Kaminski, Anton Hommer, Didem Koyuncu,Robert Biowski, Talin Barisani and Isabella Baumgartner
University Eye Clinic Vienna, Austria
ABSTRACT.Purpose: Dorzolamide (TrusoptA) is the first topical carbonic anhydrase inhibi-tor (CAI) that is in clinical use in glaucoma therapy. It is known that CAI havea negative effect on corneal endothelial pumpfunction and therefore on thewhole corneal physiology.Methods: 20 patients with open angle glaucoma or ocular hypertension and anelevated intraocular pressure (IOP) over 21 mmHg and without prior oral CAI-treatment were included in this study. Trusopt was administered t.i.d. as mono-therapy and b.i.d. in combination with other topical antiglaucoma drugs. Cor-neal ultrasound pachymetry, corneal endothelial cell count and aesthesiometrywere performed prestudy and on days 1, 8, 15, 30, 60 and 90.Results and Conclusions: Mean corneal thickness was slightly increased on dayone (statistically non-significant) and returned to baseline measurements at thefollowing visits, no changes in endothelial cell count and corneal aesthesia werefound. Topical dorzolamide is not associated with clinically meaningful changesof the cornea.
Key words: dorzolamide – corneal thickness – corneal endothelium – corneal aesthesia.
Acta Ophthalmol. Scand. 1998: 76: 78–79Copyright c Acta Ophthalmol Scand 1998. ISSN 1395-3907
With 2% dorzolamide hydrochloridea newly developed topical car-
bonic anhydrase inhibitor is available forthe treatment of glaucoma (CAI). Dorzo-lamide is a highly water-soluble CAI thathas been formulated as an ophthalmicpreparation and was effective in reducingaqueous production and lowering intrao-cular pressure without showing systemicadverse reactions that can occur with oralCAIs. Multiple studies indicate that 2%dorzolamide shows clinically significantocular hypotensive efficacy and accept-able ocular tolerability (Wilkerson etal.1993; Strahlmann et al. 1995).
Not only is carboanhydrase an import-ant enzyme for aqueous production inthe ciliary epithelium, it is also a majorcatalyst for corneal endothelial pumpingfunction. Evidence that bicarbonate is in-timately involved in the pumping mech-
anism has come from measurements ofcorneal rate of deturgescence in it’s pres-ence and absence (Kuang et al. 1990;Hodson et al. 1974), from the observedinhibition of corneal deturgescence andtransendothelial electrical potential dif-ference by CAI, and from observations ofnet HCO3
ª movement across the the en-dothelium (Hodson et al. 1976; Fishbarg1974).
Therefore, we decided to determine theinfluence of the topical CAI on cornealthickness, endothelial cell count, and cor-neal sensibility.
Patients and Methods25 patients (7 male, 18 female), aged69.5∫12.76 years, with chronic openangle glaucoma or ocular hypertension
and an elevated intraocular pressure(IOP) over 21 mm Hg with a duration of39.73∫53.26 months were enrolled in thisstudy. None of the patients had prior oralCAI-treatment. 12 patients were givendorzolamide monotherapy t.i.d. (group1) and 13 patients had dorzolamide b.i.d.in combination with either Timolol 0.5%b.i.d. or pilocarpine 1% t.i.d. (group 2).Ultrasound pachymetry (Storz, Omega),non-contact endothelial biomicroscopy(Konan) and Cochet-Bonnet aesthesi-ometry were performed on day 0, 1, 7,14and month 1, 2 and 3. IOP measurementswere taken at every visit.
Group comparisons were made via t-tests, after analysis of variance; any p-value less than 0.05 was regarded as stat-istically significant. In more than 90% itwas possible to detect a 10% differencebetween pre- and post-treatment in meanpercent of corneal thickness increase, as-suming an SD of 12%, aΩ0.05, two-tailed.
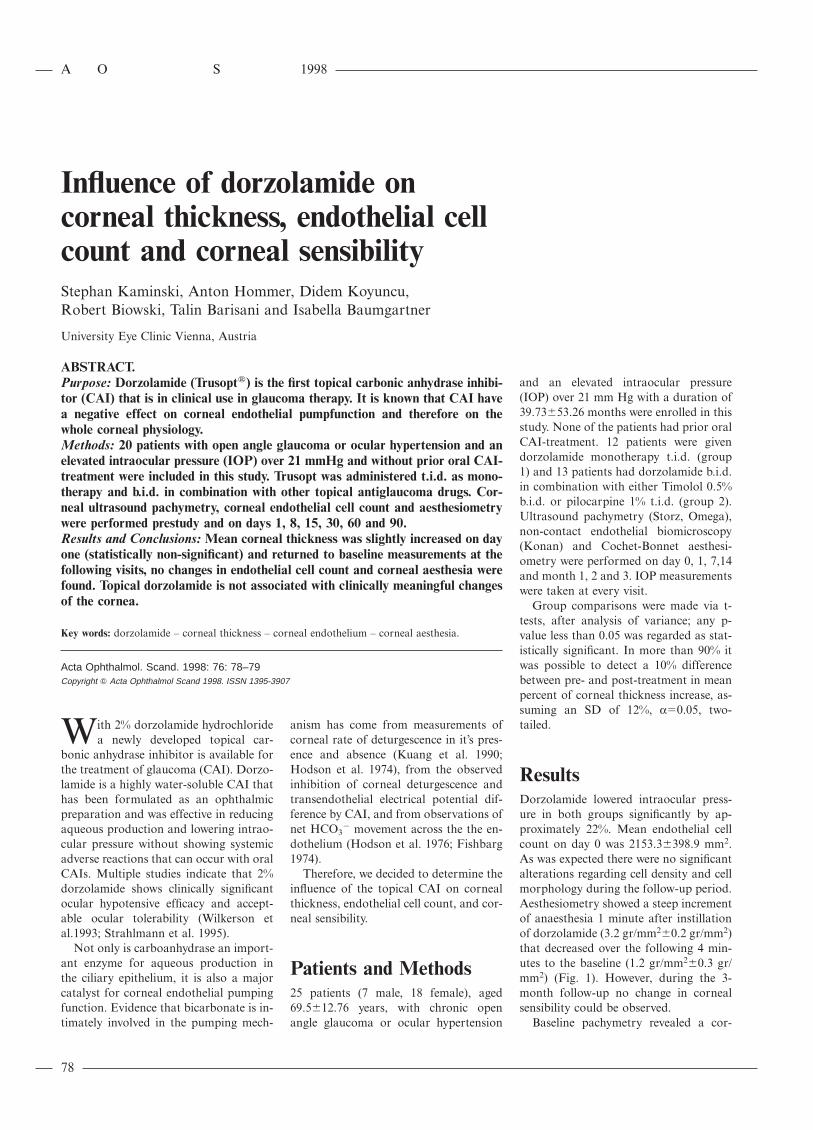
ResultsDorzolamide lowered intraocular press-ure in both groups significantly by ap-proximately 22%. Mean endothelial cellcount on day 0 was 2153.3∫398.9 mm2.As was expected there were no significantalterations regarding cell density and cellmorphology during the follow-up period.Aesthesiometry showed a steep incrementof anaesthesia 1 minute after instillationof dorzolamide (3.2 gr/mm2∫0.2 gr/mm2)that decreased over the following 4 min-utes to the baseline (1.2 gr/mm2∫0.3 gr/mm2) (Fig. 1). However, during the 3-month follow-up no change in cornealsensibility could be observed.
Baseline pachymetry revealed a cor-
A O S 1998
79
Fig. 1. Corneal aesthesia after instillation of one drop of 2% dorzolamide measured with theCochet-Bonnet aesthesiometer.
neal thickness of 559.9∫29.7 mm. On day1 a slight increase of corneal thicknesswas measured (573.2∫19.5 mm) that wasnot statistically significant (pΩ0.39). Thefollowing measurements did not revealthis corneal thickening but correspondedto the baseline values.
No statistically significant differencesbetween group 1 and group 2 were ob-served.
DiscussionCarboanhydrase plays a major role incorneal deturgescence (Hodson et al.1974, 1976; Fishbarg 1974). HCO3
ª isgenerated intracellularly in the cornealendothelium by the action of carbonicanhydrase both from exogenous andendogenous CO2. The apical cell mem-brane bears an electrogenic HCO3
ª
transporter and a Naπ reentry pathway.As a consequence of cellular electrolytetransport intercellular fluid transportfrom corneal stroma to the aqueoushumor is achieved (Kuang et al. 1990).The predominant carbonic anhydrase iso-enzyme in corneal endothelium is CA II(Wistrand et al. 1986). As dorzolamide isa CAI that specifically blocks isoenzymeCA II one would expect a decrease ofHCO3
ª production and therefore adiminished pump activity, leading tostromal swelling and to an overall in-
crease in corneal thickness. This might beconsistent with our measurements on day1. However, corneal thickness decreasedto baseline levels at all other follow-upvisits.
The fluid transport reemerging afterthe first administration of dorzolamidemay be related to generation of HCO3
ª
via an uncatalyzed conversion of CO2.Furthermore, it has been discussed thatPO4
3ª might somehow replace HCO3ª as
a cotransporter substrate (Kuang et al.1990). Also chip28 water related aquapo-rin channels might play a major role influid transport in the absence of HCO3
ª
(Chepelinsky et al. 1995).One study demonstrated corneal de-
compensation in patients treated withtopical dorzolamide (Konowal et al.1996), however, all patients had compro-mised corneal endothelium and onewould expect that the alternative path-ways might not be sufficient to maintainthe fluid transport.
No change in endothelial cell densityoccurred, but follow-up time might betoo short to detect changes related totopical dorzolamide. Also, no change incorneal aesthesia could be measured.
In summary, this study has shown thatdorzolamide given three times a day inmonotherapy or twice daily in combi-nation with timolol or pilocarpine has nomeaningful adverse effects on cornealphysiology.
AcknowledgementsThis paper was presented in part at the 5thCongress of the European Glaucoma Society,June 19–22, 1996, Paris, France.
LiteratureChepelinsky A, Parker-Wilson D, Kuang K &
Fishbarg J (1995): A new water channel ex-pressed in corneal endothelial cells. InvestOphthalmol Vis Sci (Abstract) 36: 31.
Fishbarg J & Lim JJ (1974): Role of cations,anions and carbonic anhydrase in fluidtransport across rabbit endothelium. J Phy-siol (Lond.) 241: 647–675.
Hodson S & Miller F (1976): The bicarbonatepump ion in the endothelium which regu-lates the hydration of rabbit cornea. J Physi-ol (Lond.) 263: 563–577.
Hodson S (1974): Evidence for bicarbonate-de-pendent sodium pump in corneal endo-thelium. Exp Eye Res 11: 20–29.
Konowal A, Epstein R, Dennis R & Brown S(1996): Irreversibel corneal decompensationin patients treated with topical dorzolamide.Invest Ophthalmol Vis Sci (Abstract) 37: 79.
Kuang K, Xu M, Koniarek JP & Fischbarg J(1990): Effects of ambient bicarbonate,phosphate and carbonic anhydrase inhibi-tors on fluid transport across rabbit cornealendothelium. Exp Eye Res 50: 487–493.
Strahlmann E, Tipping R, Vogel R and the In-ternational Dorzolamide Study Group(1995): A double-masked, randomized 1-year study comparing Dorzolamide (Tru-sopt), Timolol, and Betaxolol. ArchOphthalmol 113 (8): 1009–1016.
Wilkerson M, Cyrlin M, Lippa EA, EspositoD, Deasy D, Panebianco D et al. (1993):Four-week safety and efficacy study of dor-zolamide, a novel active topical carbonicanhydrase inhibitors. Arch Ophthalmol111(10): 1343–1350.
Wistrand PJ, Schenholm M & Lonnerholm G(1986): Carbonic anhydrase isoenzymes CAI and CA II in the human eye. InvestOphthalmol Vis Sci 27: 419–428.
Received on November 11th, 1996.Accepted on June 4th, 1997.
Corresponding author:
Dr. Stephan KaminskiUniversity Eye Clinic, ViennaWahringer Gurtel 18–20A-1090 ViennaAustria