indications for sublobar resection for localized nsclc
TRANSCRIPT

Indications for sublobar resection for localized NSCLC
David H Harpole Jr, MD Professor of Surgery
Associate Professor in Pathology Vice Chief, Division of Surgical Services
Duke University School of Medicine Durham, North Carolina
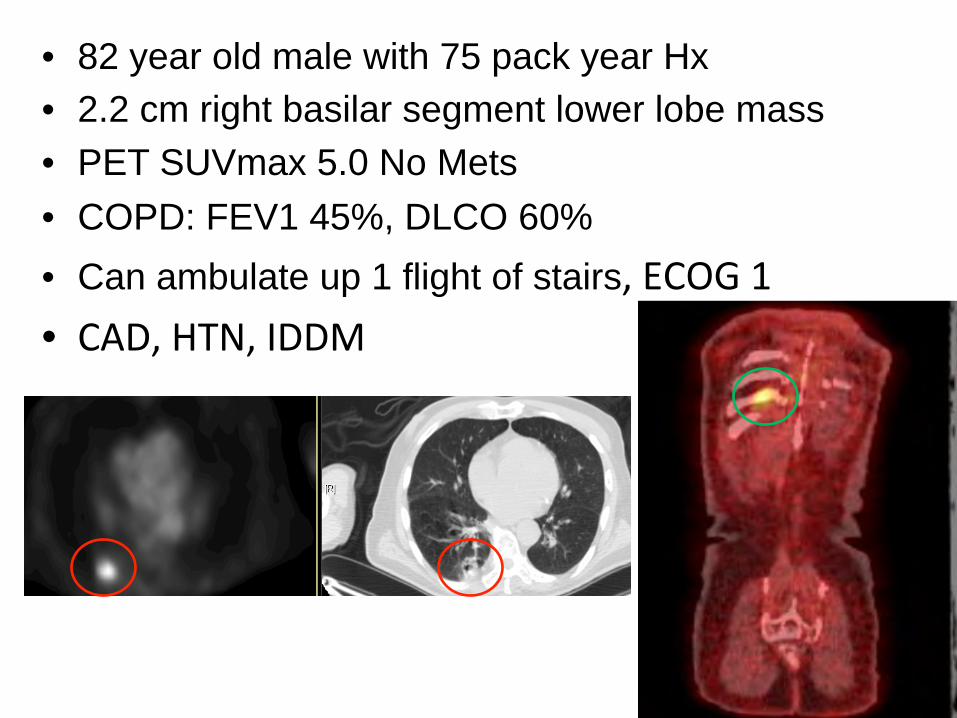
• 82 year old male with 75 pack year Hx • 2.2 cm right basilar segment lower lobe mass • PET SUVmax 5.0 No Mets • COPD: FEV1 45%, DLCO 60% • Can ambulate up 1 flight of stairs•

• • • • • •

Indications for sublobar resection for localized NSCLC
David H Harpole Jr, MD Professor of Surgery
Associate Professor in Pathology Vice Chief, Division of Surgical Services
Duke University School of Medicine Durham, North Carolina
Disclosure
No relevant conflicts of interest to disclose
Who Gets Wedge Resection?
• Not Defined in 2016 • Usually Patients at high-risk for lobectomy
– 15-20% Local recurrence with sub-lobar resection
• ACOSOG trial Z04032: Randomized Phase III – VATS Wedge + / - Intraop Brachytherapy
• Tufts / Pitts data suggest lower recurrence rate – Not a candidate for lobectomy – Two of following: FEV1< 40%, DLCO<40%, Age > 75, CHF, Pulmonary hypertension, Home O2

ACOSOG 4032: High-Risk Wedge
252/250 enrolled, No difference in Outcome, ASCO 2013

Solitary Pulmonary Nodule
Left Upper Lobe Lesion T1N0 NSCLC

Small T1 Lung Cancers (≤ 1cm)
• Mayo clinic retrospective n=100; 1980-1999 – 3-10 mm diameter, majority adenocarcinoma – Lobectomy + MLND (90%) – 93 T1N0, 5 T1N1, 2 T1N2
• Japanese also observed 10% N1 or N2
– 85% 5-year cancer-specific survival – 64% overall survival – Recommend lobectomy as operation
Miller et al., Ann Thorac Surg, 2001

CALGB 140503 Solitary Pulmonary
Nodule <2.0 cm by CT
Randomize; n=900
Verify NSCLC
All N1 + N2 (-)
Lobectomy N=450 Limited Resection
N=450 Accrual 600/900

Anatomic Segmentectomy • Initially described by Churchill and Belsey (1939) • Interest has been increasing as an option for:
– Very small tumors (<2.0cm) – A superior oncologic therapy for those with margin
pulmonary reserve (better than non-anatomic wedge) – Most commonly performed include:
• Superior segment lower lobe • Basilar segments of lower lobe • Lingual-sparing left upper lobe bi-segment • Lingular bi-segment • Others can also be completed.

Segmentectomy for Small Tumors Fukuoko Japan 2001-2004 (n=34) • Phase II protocol for primary therapy for stage 1A (<2.0 cm)
NSCLC • Outcomes simlar to historical lobectomies in same institution
Shiraishi et al., Surg Endosc 2004
Akashi City, Japan 1985-2002 (n=1272) • Long-term outcomes for pulmonary resections
Tumor Size Lobectomy Segmentectomy p-value < 2.0 cm 92% (159) 97% (129) NS 2.0 to 3.0 cm 87% (268) 85% (161) NS 3.0 cm 81% (497) 63% (53) p=0.01
Okada et al. J Thorac Cardiovasc Surg 2004

Wedge Resection vs Segmentectomy for Patients with T1a N0 Non-Small Cell Lung Cancer

To assess outcomes of patients who underwent wedge resection or segmentectomy for stage T1a N0 NSCLC National Cancer Database
Hypothesis: Segmentectomy is associated with improved long-term survival when compared to wedge resection
Objective

Matched Patient Characteristics

Perioperative Outcomes: No Difference

Overall Survival Results: Propensity-score-matched Analysis

Survival of Patients with Tumors ≤ 1 cm: Propensity-score-matched Analysis

Overall Survival Results: Subgroup Analysis
No comorbidities Bronchioloalveolar Carcinoma

In an analysis of a population-based data set, a large proportion of patients was found to have received wedge resection for cT1a N0 NSCLC Segmentectomy for T1a N0 NSCLC had improved long-term survival when compared to wedge resection, even for patients with very small tumors ≤ 1 cm and for patients with no comorbidities No significant differences in 30-day mortality between wedge and segmentectomy
Segmentectomy should be the preferred sublobar resection for cT1a N0 NSCLC
Conclusion
• • • • •

• •