increase opportunities for person-centered care planning
TRANSCRIPT

3/24/2015
1
©Pathway Health 2013
Are We REALLY Offering the Resident Their
Choice? Increase Opportunities for
Person-Centered Care Planning and Decision Making
Susan LaGrange, RN, BSN, NHA Director of Education
Pathway Health
1 ©Pathway Health 2013
Upon completion of the presentation, attendees will be able to:
1. Describe the key strategies in developing a culture that leads to successful outcome of true resident choice
2. Verbalize a system to verify positive
outcomes related to resident choice
3. Identify resources available in the industry to assist facilities for further learning and system implementation
Objectives
2
©Pathway Health 2013
Culture Change!
3
©Pathway Health 2013
• It takes
– planning!
– It takes a bit of time!
– It takes a little digging!
– It takes patience!
– It takes creativity!
Collaboration WITH the Resident
4
©Pathway Health 2013
• Also Takes:
– Planning
– Time
– Digging
– Patience
– Intuition
– Creativity
Collaboration WITH the Family
5 ©Pathway Health 2013
Where does a good amount of our information come from for the initial care
plan?
The Admission Process
Let’s Look at Our Processes
6

3/24/2015
2
©Pathway Health 2013
• What are the nurses doing on that Friday pm when many of the residents are admitted?
– Passing medications – Treatments – Processing orders that came back after
the day shift left
– Calling practitioners for updates – Assessment follow up, documentation,
etc……
Admission Assessment
7 ©Pathway Health 2013
• Preadmission Assessment
– How is the information communicated?
– Are the nurses looking at the information from the hospitals?
• H&P
• IDT Notes
• Medication Review/Reconciliation
• Discharge Summary
From the Beginning…
8
©Pathway Health 2013
• Who completes them?
– Friday pm or weekend admissions
– 24 Hour Care Plan?
• Where is the information derived?
• How is this communicated?
Admission Care Plans
9 ©Pathway Health 2013
Are WE MISSING a Piece of the Puzzle
10
©Pathway Health 2013
Traditional
• Staff directed
• Medical/Diagnosis based
• Staff goals
• Therapy goals
• **Based on assessments when resident’s admitted to the facility
Person-Centered
• Resident directed
• Preferences (choice)
• Habits
• Routines
• History of Medical Management
• The resident’s understanding of medical management of conditions
• Resident’s goals
Traditional vs. Person-Centered
11 ©Pathway Health 2013
RAI PROCESS
12
MDS
CATs
CAAs
CARE PLAN
CAA SUMMARY
CARE ASSESSMENTS RESIDENT INTERVIEWS

3/24/2015
3
©Pathway Health 2013
Preferences for Customary Routine and Activities:
INTENT:
• To obtain resident’s own preferences for both routines and activities
• Should be obtained directly from the resident or family/significant other
• To be used for Care Planning
• Is not all-inclusive
MDS Section F
13 ©Pathway Health 2013
• Clothing choice
• Personal belongings (caring for and securing)
• Bathing/showering
• Snacking
• Staying up at night
• Who should be involved in care discussions
• Privacy with phone calls
• Activity preferences
– Reading materials -Out of facility activities
– Music -Outdoor activities
– Group Activities -Religious activities
MDS Section F
14
©Pathway Health 2013
CAA
15 ©Pathway Health 2013
• Based on the Comprehensive Assessment
• Based on Resident Choice and Preferences
• Individualized
• Goals that are realistic, measureable and make
sense to the resident!
• Approaches: Unique to the resident needs that
assist the resident in achieving the goal!
• Consistently Implemented
• Evaluation Process/Revisions as Necessary
Care Plan Essentials
16
©Pathway Health 2013
• Begin even before admission if possible to set the tone and prepare for a successful transition.
• Upon admission, teach staff to take the time to identify resident choices and preferences for care, document them and communicate this to the care givers
• Take the time to include the resident in the RAI process with choices for care plan goals and intervention
• Educate all departments on resident choices and care planning decisions
Processes Necessary for Collaboration
17 ©Pathway Health 2013
• Where are the preferences/choices/habits of the resident documented:
– Nursing Notes
– Social Service Notes
– Activity/Recreational Therapy Notes
– Dietary Notes
***How do we put it all together??
Putting it all TOGETHER
18

3/24/2015
4
©Pathway Health 2013
• I like to teach staff person centered care in a variety of ways:
– Making a pizza
– Planning a vacation
– Shopping trip
– Decorating a room
Key: We all have different preferences – and when we weave in the resident’s choices – we improve the odds of true person centered care!
Moving Staff Forward
19 ©Pathway Health 2013
• Education
• Shift to Shift
• Department to Department
• Documentation (C.N.A. Care Plans, Care Records, Care Cards, etc.)
• Ongoing rapport with the resident/family
Communication
20
©Pathway Health 2013
• Formal Interviews
• Informal Visits
• Resident Council
• Family Input
• Care Plan Conferences
Resident Interviews
21 ©Pathway Health 2013
• To sort through the information and identify the individualized needs and wishes of each resident
• What is THEIR perception?
• Asking, “What would YOU like to see differently?
Taking the TIME…
22
©Pathway Health 2013
GROUP EXERCISE
23 ©Pathway Health 2013
Resident: Identify 3 Unique things about you that you would want in your care plan Care Giver: Describe how you would Care Plan this and ensure that these 3 areas are incorporated in care
24

3/24/2015
5
©Pathway Health 2013
How Do WE Verify Choice Inclusion?
25
©Pathway Health 2013
1. Audit charts (See Handout)
2. Interview the Resident
3. Interview the Staff
4. Observe
5. Check the 24 hour report
a) Are new problems/concerns added to CP?
b) Are the goals and interventions consistent with resident choice?
c) What does the resident say?
How Do We Verify
26
©Pathway Health 2013
Area for Correction Plan Date Due Responsible Party
Care plan does not contain specific individualized information from the CAA
1. Education will be provided for all IDT members involved in CAA and care planning process.
2. All care plans will be reviewed and updated with individualized goals and interventions with next MDS cycle
3. Audits will be completed weekly to monitor compliance
4. Results of audits will be addressed in the Quarterly QA Committee Meeting
5/15/15 Starting 5/15/15 for 3 months Starting 6/1/15 7/1/15
DON or Designee DON or Designee IDT Team DON or Designee
C.N.A. Care Record not updated with current care plan information
1. Education will be provided for all IDT members involved in care planning to update C.N.A. Care Record
2. All C.N.A. Care Records will be cross-referenced/updated with Care Plans
3. Audits will be completed weekly to monitor compliance
4. Results of audits will be addressed in the Quarterly QA Committee Meeting
5/15/15 Starting 5/15/15 for 3 months Starting 6/1/15 7/1/15
DON or Designee DON or Designee IDT Team DON or Designee
Action Plan
27
©Pathway Health 2013
Examples of Tools
28
©Pathway Health 2013 29
©Pathway Health 2013 30
3/24/2015
6
31
©Pathway Health 2013
Resources
32
©Pathway Health 2013
• https://www.nhqualitycampaign.org/goalDetail.aspx?g=PCC
• https://www.pioneernetwork.net/CultureChange/
• http://thegreenhouseproject.org/
• http://www.edenalt.com/
• http://www.polisherresearchinstitute.org/#!assessment-instruments/c16rg
• http://www.amda.com/consumers/CultureChangeMar10.pdf
• http://www.commonwealthfund.org/publications/in-the-literature/2010/jan/person-centered-care-for-nursing-home-residents
Informational Websites
33 ©Pathway Health 2013
Thank You!!!
34
©Pathway Health 2013
Sue LaGrange, RN, BSN, NHA, CDONA
Director of Education
Pathway Health 35

ACTION PLAN
Area of Action Findings Recommendations Goal Date Responsible Person(s)
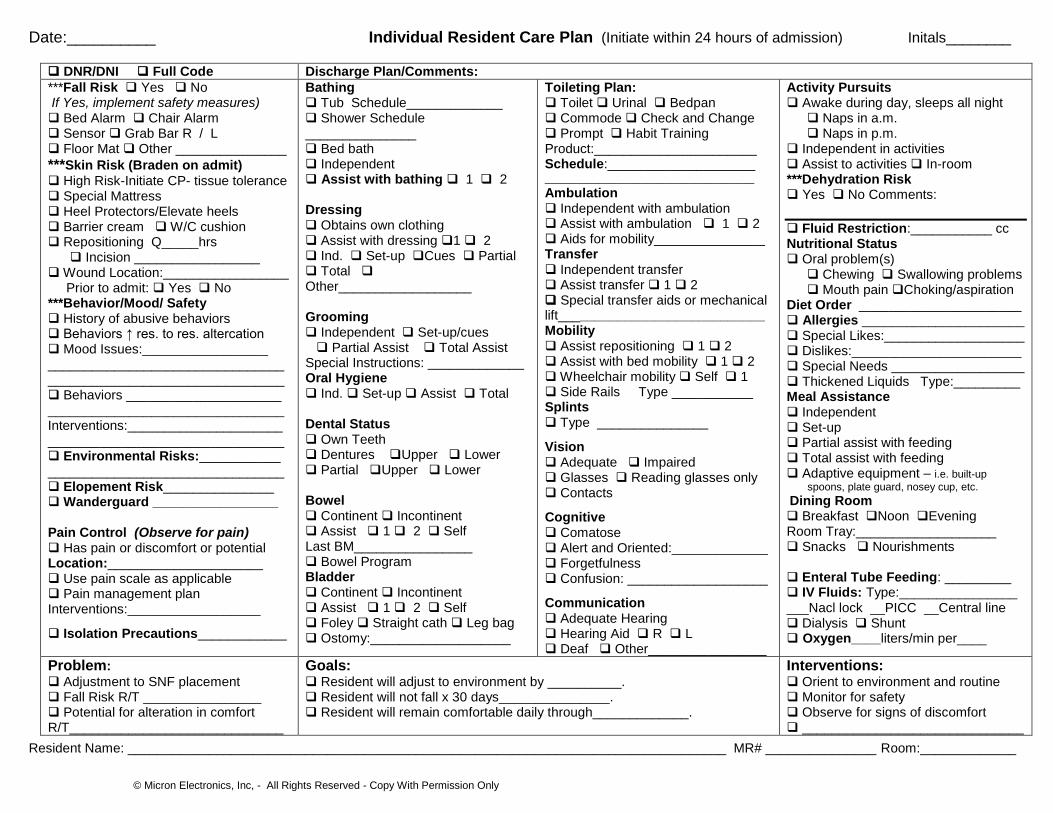
Date:__________ Individual Resident Care Plan (Initiate within 24 hours of admission) Initals________
© Micron Electronics, Inc, - All Rights Reserved - Copy With Permission Only
DNR/DNI Full Code Discharge Plan/Comments:
***Fall Risk Yes No If Yes, implement safety measures) Bed Alarm Chair Alarm Sensor Grab Bar R / L Floor Mat Other _______________
***Skin Risk (Braden on admit) High Risk-Initiate CP- tissue tolerance Special Mattress Heel Protectors/Elevate heels Barrier cream W/C cushion Repositioning Q_____hrs Incision _________________ Wound Location:_________________ Prior to admit: Yes No ***Behavior/Mood/ Safety History of abusive behaviors Behaviors ↑ res. to res. altercation Mood Issues:_________________ ________________________________________________________________ Behaviors _____________________ ________________________________ Interventions:_____________________ ________________________________ Environmental Risks:___________ ________________________________ Elopement Risk_______________ Wanderguard _________________ Pain Control (Observe for pain) Has pain or discomfort or potential Location:_____________________ Use pain scale as applicable Pain management plan Interventions:__________________
Isolation Precautions____________
Bathing Tub Schedule_____________ Shower Schedule _______________ Bed bath Independent Assist with bathing 1 2 Dressing Obtains own clothing Assist with dressing 1 2 Ind. Set-up Cues Partial Total Other__________________ Grooming Independent Set-up/cues Partial Assist Total Assist Special Instructions: _____________ Oral Hygiene Ind. Set-up Assist Total Dental Status Own Teeth Dentures Upper Lower Partial Upper Lower Bowel Continent Incontinent Assist 1 2 Self Last BM________________ Bowel Program Bladder Continent Incontinent Assist 1 2 Self Foley Straight cath Leg bag Ostomy:___________________
Toileting Plan: Toilet Urinal Bedpan Commode Check and Change Prompt Habit Training Product:______________________ Schedule:____________________ ___________________________________
Ambulation Independent with ambulation Assist with ambulation 1 2 Aids for mobility_______________ Transfer Independent transfer Assist transfer 1 2 Special transfer aids or mechanical lift____________________________ Mobility Assist repositioning 1 2 Assist with bed mobility 1 2 Wheelchair mobility Self 1 Side Rails Type ___________ Splints Type _______________
Vision Adequate Impaired Glasses Reading glasses only Contacts
Cognitive Comatose Alert and Oriented:_____________ Forgetfulness Confusion: ___________________
Communication Adequate Hearing Hearing Aid R L Deaf Other________________
Activity Pursuits Awake during day, sleeps all night Naps in a.m. Naps in p.m.
Independent in activities Assist to activities In-room ***Dehydration Risk Yes No Comments:
Fluid Restriction:___________ cc Nutritional Status Oral problem(s) Chewing Swallowing problems Mouth pain Choking/aspiration
Diet Order ______________________ Allergies ______________________ Special Likes:___________________ Dislikes:_______________________ Special Needs __________________ Thickened Liquids Type:_________ Meal Assistance Independent Set-up Partial assist with feeding Total assist with feeding Adaptive equipment – i.e. built-up
spoons, plate guard, nosey cup, etc.
Dining Room Breakfast Noon Evening Room Tray:___________________ Snacks Nourishments Enteral Tube Feeding: _________ IV Fluids: Type:________________ ___Nacl lock __PICC __Central line Dialysis Shunt Oxygen____liters/min per____
Problem: Adjustment to SNF placement Fall Risk R/T ________________ Potential for alteration in comfort R/T_____________________________
Goals: Resident will adjust to environment by __________. Resident will not fall x 30 days_______________. Resident will remain comfortable daily through_____________.
Interventions: Orient to environment and routine Monitor for safety Observe for signs of discomfort ______________________________
Resident Name: _________________________________________________________________________________ MR# _______________ Room:_____________

Date:__________ Individual Resident Care Plan (Initiate within 24 hours of admission) Initals________
© Micron Electronics, Inc, - All Rights Reserved - Copy With Permission Only
Date Problem Related to Goal Goal Date
Intervention Discipline Responsible
Date: Nurse Signature: Resident Name: _________________________________________________________________________________ MR# _______________ Room:_____________

© HP - All Rights Reserved - Copy With Permission Only
PERSON-CENTERED CARE PLAN AUDIT
Care Plan Problem Goal is measureable,
realistic and individualized based on documentation, assessments and CAA’s
Interventions are individualized and meaningful toward goal
New problems identified are added timely to the care plan
Information is located on the C.N.A. care plan or care record
Staff interviewed and aware of goal and interventions
Evidence of review and revisions are noted
Resident #: ________________________________ Date of Audit: _________________
Signature: _________________________________