in the name of god evaluation of patient with chest pain presenting in primary care setting dr....
TRANSCRIPT

IN THE NAME OF GOD
Evaluation of patientEvaluation of patientwith chest pain with chest pain presenting in presenting in primary care settingprimary care setting
Dr. Mohammad Garak Yaraghi,MD
Associate Professor of Cardiology
Isfahan University of Medical sciences

Chest PainChest Pain
Common presentation.Trivial to life-threatening causes.Key to diagnosis is history NOT
INVESTIGATIONS.Negative baseline investigations DO NOT
ruleout serious conditions
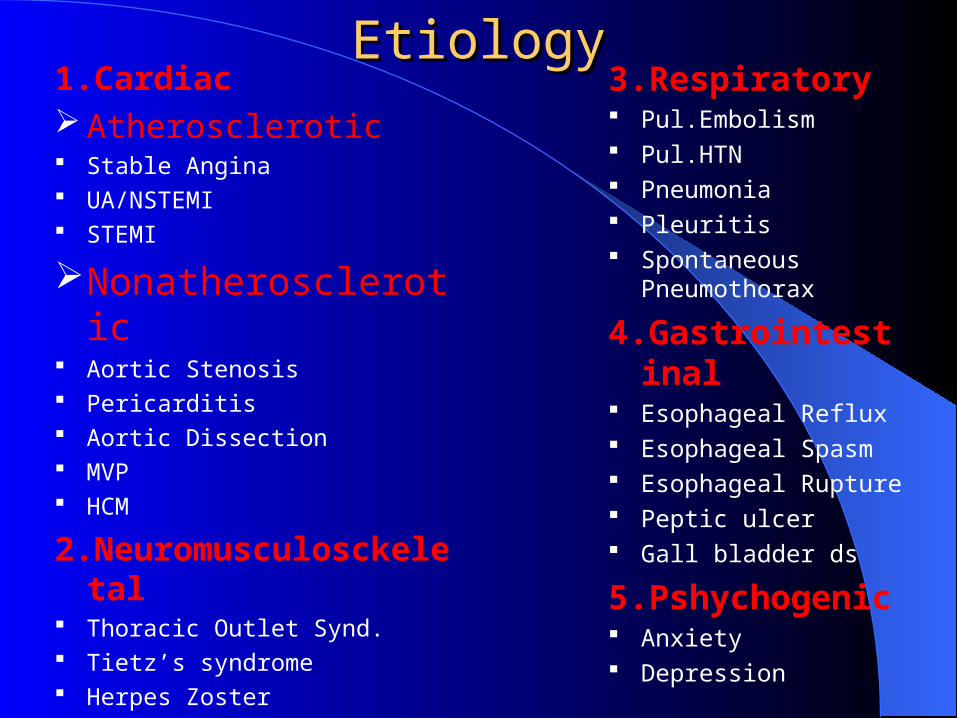
EtiologyEtiology1.Cardiac Atherosclerotic Stable Angina UA/NSTEMI STEMI
Nonatherosclerotic Aortic Stenosis Pericarditis Aortic Dissection MVP HCM
2.Neuromusculosckeletal Thoracic Outlet Synd. Tietz’s syndrome Herpes Zoster
3.Respiratory Pul.Embolism Pul.HTN Pneumonia Pleuritis Spontaneous
Pneumothorax
4.Gastrointestinal Esophageal Reflux Esophageal Spasm Esophageal Rupture Peptic ulcer Gall bladder ds
5.Pshychogenic Anxiety Depression

From Hurst
Differential diagnosis:Differential diagnosis:

Life-threateningLife-threatening Causes ofCauses ofChest PainChest Pain
Myocardial infarction(ACS).Thoracic aortic dissection.Pulmonary embolus.Tension pneumothorax.Oesophageal rupture.
Investigations
ECG most important but history is more important.
20% of patients having an MI will have a normal ECG initally.
Negative cardiac enzymes in A&E are not helpful.
CXR useful to rule out other causes like pneumonia.
Acute Chest PainAcute Chest Pain
Assess pt’s respiratory & hemodynamic statusIf either is compromised -
initially focus on stabilizing pt before diagnostic evaluation.
If pt does not require emergent intervention -focussed history , physical examination, lab investigations.


HistoryHistory Quality of painQuality of pain
Chest discomfort / heaviness/pressure/burning sensation – Stable Angina , UA/NSTEMI, STEMI Lancinating / sharp / knife like / stabbing – Herpes Zoster , Pleuritis , Pneumonia , Pericarditis , Pulmonary embolismTearing / ripping – Aortic DissectionBurning – GERD, Peptic ulcer, Gall bladder ds. ,Herpes
zoster Variable - Psychogenic

History History Location & RadiationLocation & Radiation
Retrosternal , often radiating to left shoulder, neck , jaw- Stable Angina , UA/NSTEMI, STEMI , Aortic Stenosis
Localised to small, specific area pointed with finger – Unlikely to be true angina
Dermatomal – Herpes Zoster, Cervical disc dsRadiating to back – Aortic dissection , Expanding
thoracic aortic aneurysm, Ruptured peptic ulcer, Pancreatitis

History History Location & Radiation Location & Radiation
Retrosternal / towards cardiac apex- PericarditisLateral – Pul.embolismSubsternal – Pul.HTN, Esophageal refluxU/L , localised – PneumoniaEpigastric – Peptic ulcerEpigastric&Rt upper quadrant – Gall bladder ds.
disease.Anterior chest musculoskeletal – Tietz’s syndrome

History History Duration , Frequency , Duration , Frequency ,
RecurrenceRecurrence>2 & <10 min , on exertion , exposure to
cold, heavy meals – Angina 10 – 20 min , unpredictable , on exertion or
at rest – Unstable AnginaVariable > 30 min , not relieved by nitrates
– Acute MI Recurrent episodes as of angina – ASAbrupt unrelenting pain – Aortic dissection Hours – days , episodic - Pericarditis

History History Duration , Frequency , Duration , Frequency ,
RecurrenceRecurrenceAbrupt , several min – few hrs –
Pul.embolismVariable –, Pul.HTN, Herpes zoster ,
Musculoskeltal pain , Emotional , Psychiatric
Periodic – Peptic ulcer10 – 60 min - GERD
History History Modifying FactorsModifying Factors
ppt by exertion , relieved by rest and nitrates – Anginal pain
Emotional upset , anxiety , exposure to cold – Anginal pain
Pain changes in intensity with change in body position – Musculoskeletal pain , Pericarditis ( abates after leaning forward )
History History Associated SymptomsAssociated Symptoms
Dyspnea, nausea, vomiting, diaphoresis, palpitations – Chest pain d/t ischemia
Late peaking systolic murmur radiating to carotids – AS
Pericardial friction rub – PericarditisLoss of peripheral pulse , EDM , pericardial
rub , tamponade – Aortic dissection

History History Associated SymptomsAssociated Symptoms
Dyspnea – Pleuritis , pneumonia , pul.embolism
( tachypnea, tachycardia, hypotension )Relieved by antacids – GERD, peptic ulcerWorsened by postprandial recumbency – GERDAggravated by movement – Musculoskeletal ,
PleuritisCardiac risk factors : smoking , hyperlipidemia ,
HTN , DM , F/H of CAD, Obesity, Postmenopausal
Physical Examination Physical Examination Vital signs – BP – Hyper/hypotensive ? equal / unequal in limbs RR – Tachypneic ? HR – Tachycardia ? pulsus paradoxusGeneral appearance , head & neckLungsCVSAbdomenExtremities – edema – u/l or b/lSkin – vesicles – herpes zoster ?Neurological – mood ?

Lab InvestigationsLab Investigations
Routine – CBC, LFT, S.Electrolytes , S.amylase & lipase
Cardiac enzymes – CK –MB , Trop T & I ECGCXR PA ViewTMT V/Q Scan Chest CT , TEE , MRI – Aortic dissection Spiral CT – Pul.embolism


Stable Angina Stable Angina Classification of Chest PainClassification of Chest Pain
Typical angina1. Steady retrosternal component2. Provoked by exertion or stress 3. Relieved by rest or NTG
Atypical angina– 2 of 3 criteria
Non-anginal chest pain– 1 of 3 criteria

Prevalence of CAD (%) in SymptomaticPrevalence of CAD (%) in Symptomatic Patients According to Age and Sex Patients According to Age and SexTypical angina
3 of 3 criteria
Atypical angina
2 of 3 criteria
Nonang. chest pain
1 of 3 criteriaAGE Men Women Men Women Men Women
30-39 69.7 25.8 21.8 4.2 5.2 0.8
40-49 87.3 55.2 46.1 13.3 14.1 2.8
50-59 92.0 79.4 58.9 32.4 21.5 8.4
60-69 94.3 90.6 90.6 54.6 28.1 18.6
1) Retrosternal discomfort. 2) Provoked by exercise or stress. 3) Relieved by rest or NTG
Stable Angina

Stable AnginaStable Anginaطرف 35خانمی سينه جلوی درد شکايت با ساله
مراجعه شما به ندارد ارتباط فعاليت با که چپ . . به معاينه در ندارد خطر عوامل است نموده
نکته قلب نوک در سيستولی کليک سمع جز . . است طبيعی الکتروکارديوگرام ندارد ديگری
چيست؟ شما اقدامورزش. 1 تستکرونری. 2 آنژيوگرافیسينه. 3 درد علل ساير نظر از بررسیسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaطرف 35خانمی سينه جلوی درد شکايت با ساله
مراجعه شما به ندارد ارتباط فعاليت با که چپ . . به معاينه در ندارد خطر عوامل است نموده
نکته قلب نوک در سيستولی کليک سمع جز . . است طبيعی الکتروکارديوگرام ندارد ديگری
چيست؟ شما اقدامورزش. 1 تستکرونری. 2 آنژيوگرافیسينه. 3 درد علل ساير نظر از بررسیسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaچپ 40آقائی طرف سينه جلوی درد شکايت با ساله
نموده مراجعه شما به ندارد ارتباط فعاليت با کهکنترل. خون پرفشاری فقط خطر ازعوامل است . در چهارم صدای سمع جز به معاينه در دارد شده
. الکتروکارديوگرام ندارد ديگری نکته قلب نوک . چيست؟ شما اقدام است طبيعی
ورزش. 1 تستکرونری. 2 آنژيوگرافیسينه. 3 درد علل ساير نظر از بررسیسينه. 4 عکساکوکارديوگرافی. 5
Stable AnginaStable Anginaچپ 40آقائی طرف سينه جلوی درد شکايت با ساله
نموده مراجعه شما به ندارد ارتباط فعاليت با کهکنترل. خون پرفشاری فقط خطر ازعوامل است . در چهارم صدای سمع جز به معاينه در دارد شده
. الکتروکارديوگرام ندارد ديگری نکته قلب نوک . چيست؟ شما اقدام است طبيعی
ورزش . 1 تست
کرونری. 2 آنژيوگرافیسينه. 3 درد علل ساير نظر از بررسیسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaسينه 52آقائی جناغ زير درد شکايت با ساله
. عوامل است نموده مراجعه فعاليت درموقع . چهارم صدای سمع جز به معاينه در ندارد خطر
. ندارد ديگری نکته قلب نوک در . شما اقدام است طبيعی الکتروکارديوگرام
چيست؟ورزش. 1 تستکرونری. 2 آنژيوگرافیسينه. 3 درد علل ساير نظر از بررسیسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaسينه 52آقائی جناغ زير درد شکايت با ساله
. عوامل است نموده مراجعه فعاليت درموقع . چهارم صدای سمع جز به معاينه در ندارد خطر
. ندارد ديگری نکته قلب نوک در . شما اقدام است طبيعی الکتروکارديوگرام
چيست؟ورزش . 1 تست
کرونری. 2 آنژيوگرافیسينه. 3 درد علل ساير نظر از بررسیسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaفعاليت 65خانمی درموقع سينه جناغ زير درد شکايت با ساله
. ويا استراحت با است نموده درد NTGمراجعه زبانی زير . وديابت خون فشاری پر خطر ازعوامل يابد می بهبود
. در“ چهارم صدای سمع معاينه در دارد شده کنترل نسبتاسيستوليک وسوفل قلب شنيده II/IVنوک آئورت کانون در
. طرح درالکتروکارديوگرام شود می LV Strainمی ديدهشود.
چيست؟ شما اقدامورزش. 1 تستکرونری. 2 آنژيوگرافیميوکارد. 3 پرفيوژن اسکنسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaدرموقع 65خانمی سينه جناغ زير درد شکايت با ساله
. ويا استراحت با است نموده مراجعه زير NTGفعاليت . خون فشاری پر خطر ازعوامل يابد می بهبود درد زبانی
. “ صدای سمع معاينه در دارد شده کنترل نسبتا وديابتسيستوليک وسوفل قلب نوک در کانون II/IVچهارم در
. طرح درالکتروکارديوگرام شود می شنيده LVآئورتStrain . شود می ديده
چيست؟ شما اقدامورزش. 1 تستکرونری. 2 آنژيوگرافیميوکارد. 3 پرفيوژن اسکنسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaفعاليت 63آقائی درموقع سينه جناغ زير درد شکايت با ساله
. ويا استراحت با است نموده درد NTGمراجعه زبانی زير . وديابت خون فشاری پر خطر ازعوامل يابد می بهبود
ومدت“ دارد شده کنترل روزی 30نسبتا است 10سال . قلب نوک در چهارم صدای معاينه در کشد می سيگار
. درالکتروکارديوگرام شود می Poor R progressionشنيدهV1 to V4 . شود می ديدهچيست؟ شما اقدام
ورزش. 1 تستکرونری. 2 آنژيوگرافیميوکارد. 3 پرفيوژن اسکنسينه. 4 عکساکوکارديوگرافی. 5

Stable AnginaStable Anginaفعاليت 63آقائی درموقع سينه جناغ زير درد شکايت با ساله
. ويا استراحت با است نموده درد NTGمراجعه زبانی زير . وديابت خون فشاری پر خطر ازعوامل يابد می بهبود
ومدت“ دارد شده کنترل روزی 30نسبتا است 10سال . قلب نوک در چهارم صدای معاينه در کشد می سيگار
. درالکتروکارديوگرام شود می Poor R progressionشنيدهV1 to V4 . شود می ديدهچيست؟ شما اقدام
ورزش. 1 تستکرونری. 2 آنژيوگرافیميوکارد. 3 پرفيوژن اسکنسينه. 4 عکساکوکارديوگرافی. 5

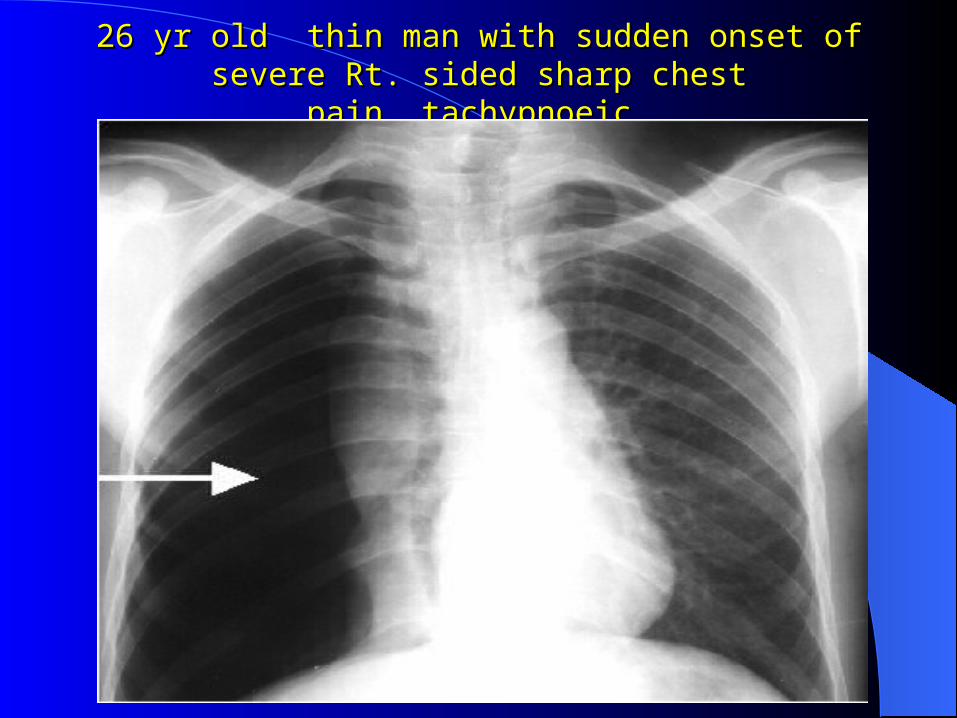
26 yr old thin man with sudden onset of severe Rt. 26 yr old thin man with sudden onset of severe Rt. sided sharp chest pain ,tachypnoeic.sided sharp chest pain ,tachypnoeic.
Right Pneumothorax


65 year old man(H/O DM,HTN) presented with a 1 hour history of 65 year old man(H/O DM,HTN) presented with a 1 hour history of severe central crushing chest pain. He is sweaty, clammy and has severe central crushing chest pain. He is sweaty, clammy and has
vomited twice .vomited twice .
65 year old man(H/O DM,HTN) presented with a 1 hour history of 65 year old man(H/O DM,HTN) presented with a 1 hour history of severe central crushing chest pain. He is sweaty, clammy and has severe central crushing chest pain. He is sweaty, clammy and has
vomited twice .vomited twice .
Anterior (extensive) Myocardial infarction.
Why ?
Male
65 years.
H/O DM+HTN( remember INTERHEART study)
Central Crushing chest pain.
Associated sweaty,clammy,vomiting.

70 years old male with long history of untreated HTN,nonsmoker came complaining of chest pain migrated to interscapular region & became severe(tearing),SBP 200,ECG mild inferior changes

Most likely diagnosis is:Most likely diagnosis is:
? AMI?PE?Esophagear Rupture Aortic Dissection

Aortic dissection: Aortic dissection: ClassificationClassification

Aortic DissectionAortic Dissection•Severe, sharp, “tearing” posterior chest pain or Severe, sharp, “tearing” posterior chest pain or back pain (occurs in 74-90% of pts)back pain (occurs in 74-90% of pts)
•Pain may be associated with syncope, CVA, MI, or CHFPain may be associated with syncope, CVA, MI, or CHF
–Painless dissection relatively uncommon 15%Painless dissection relatively uncommon 15%
•Chest pain is more common with Type A dissectionsChest pain is more common with Type A dissections
•Back or abdominal pain is more common with Type Back or abdominal pain is more common with Type B dissectionsB dissections

Physical ExaminationPhysical Examination
•Pulse deficitPulse deficit
–Weak or absent carotid, brachial, or Weak or absent carotid, brachial, or femoral pulses femoral pulses
–these patients have a higher rate of these patients have a higher rate of mortalitymortality
•Acute Aortic InsufficiencyAcute Aortic Insufficiency
–Diastolic decrescendo murmurDiastolic decrescendo murmur
–Best heard along the right sternal Best heard along the right sternal borderborder

TEE of Aortic Dissection & CT aortaTEE of Aortic Dissection & CT aorta


40 years old male finished 40 years old male finished cardiac evaluation last week cardiac evaluation last week for insurance (every thing is for insurance (every thing is normal) .normal) .Ate a heavy meal with friends Ate a heavy meal with friends (celebrating),followed by (celebrating),followed by severe vomiting then chest severe vomiting then chest pain,vomitus contains streaks pain,vomitus contains streaks of fresh blood.of fresh blood.
40 years old male finished cardiac evaluation last week40 years old male finished cardiac evaluation last week for insurance (every thing is for insurance (every thing is
normal) .ate a heavy meal with friends (celebrating).followed by severe vomiting then chest normal) .ate a heavy meal with friends (celebrating).followed by severe vomiting then chest pain.vomitus contains streaks of fresh blood.pain.vomitus contains streaks of fresh blood.
Likely diagnosis?ACS?PE?Aortic DissectionEsophageal submucosal tear(mallory weiss
syndrome).


A 26 year old woman presented 1 week post A 26 year old woman presented 1 week post delivery of her first baby. She has sharp L sided delivery of her first baby. She has sharp L sided
chest pain and she is short of breath.chest pain and she is short of breath.
Pulmonary EmbolismWhy ?Young femalePegnancy hypercoagulable stateOccurrence one week post partum


26 Old army officer had flu last week,felt chest pain while driving his 26 Old army officer had flu last week,felt chest pain while driving his car,pain increased by deep breath,he has no history of DM or car,pain increased by deep breath,he has no history of DM or
HTN,nonsmoker,lipid profile LDL 2.0 MMMOL/HTN,nonsmoker,lipid profile LDL 2.0 MMMOL/LL

Acute Pericarditis


26 Old army officer had flu last week,felt chest pain 26 Old army officer had flu last week,felt chest pain while driving his car,pain increased by deep breath,ECG while driving his car,pain increased by deep breath,ECG
after 5 daysafter 5 days..
Resolved Pericarditis.

Thank You for Your Attention