in service 2
TRANSCRIPT

“Managing Hypertension in Physically Active Patients”
Summary By: Jonathan Noury

Risk Factors for HTN in Athletes
• African American
• Elderly
• People who are obese
• Diabetes
• Renal disease
• FHx of HTN
Prevalence:20-30 yrs: 5-10%30-60 yrs: 20-25%
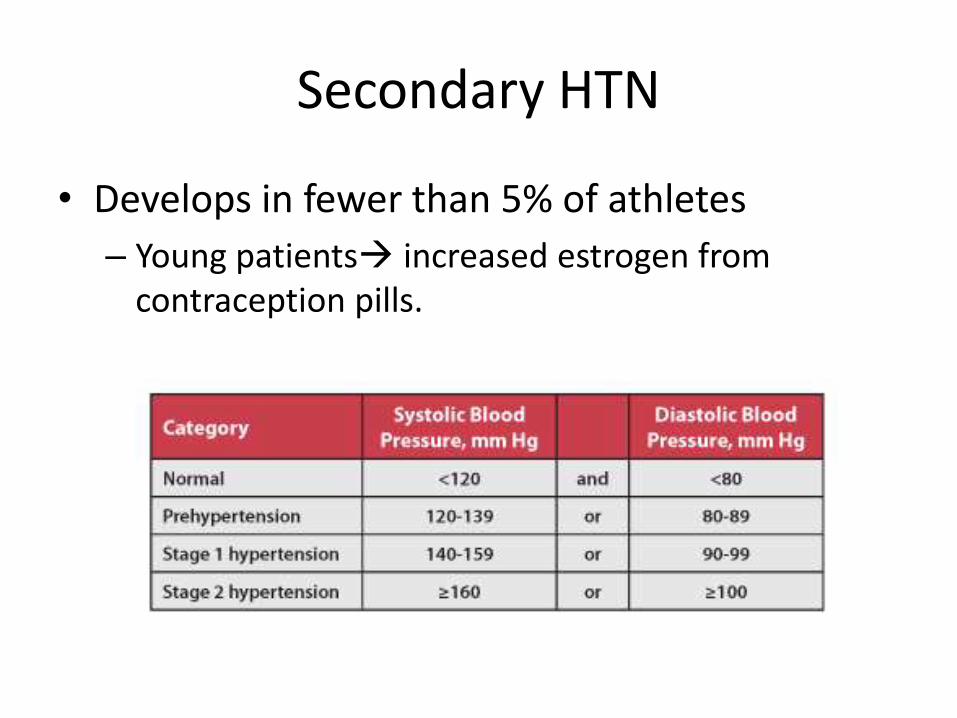
Secondary HTN
• Develops in fewer than 5% of athletes
– Young patients increased estrogen from contraception pills.
Clinical Evaluation
• Hx of behaviors
– High intake of sodium and saturated fats
– Use of alcohol/drugs
– NSAIDS
– Dietary supplements for “energy” or “weight control”
• BP measurement
– Referral for blood work

Treatment
• Compliance with lifestyle modification
– Reduction in sodium, processed food
– Increase intake of potassium
• Weight loss
– Loss of 10 lbs. can lead to significant reduction in BP for overweight patients.
– High fiber foods
• Stress management
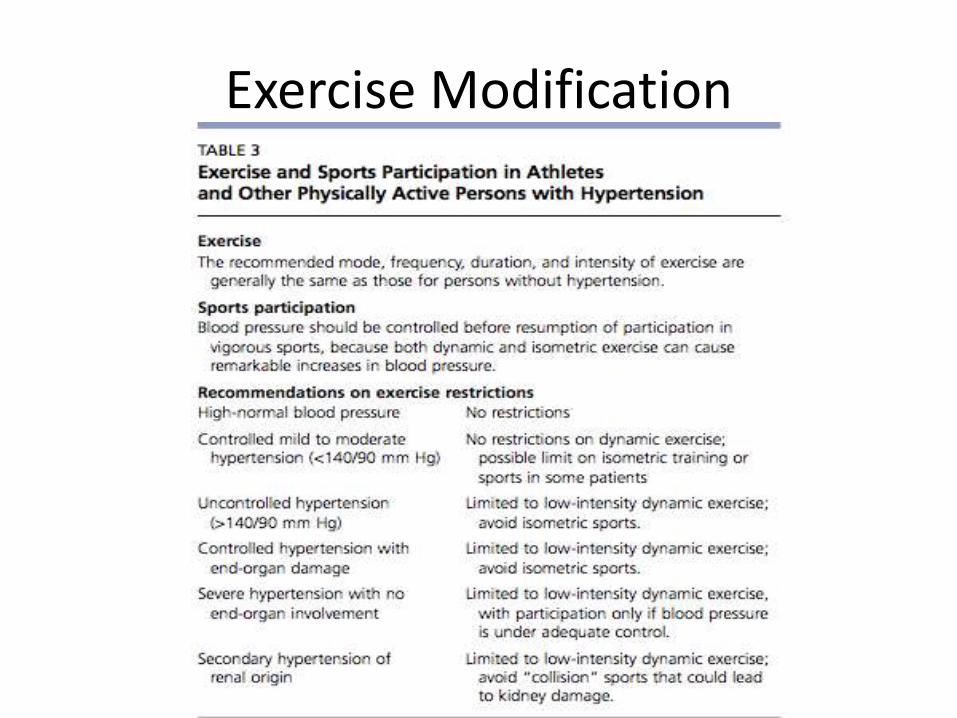
Exercise Modification
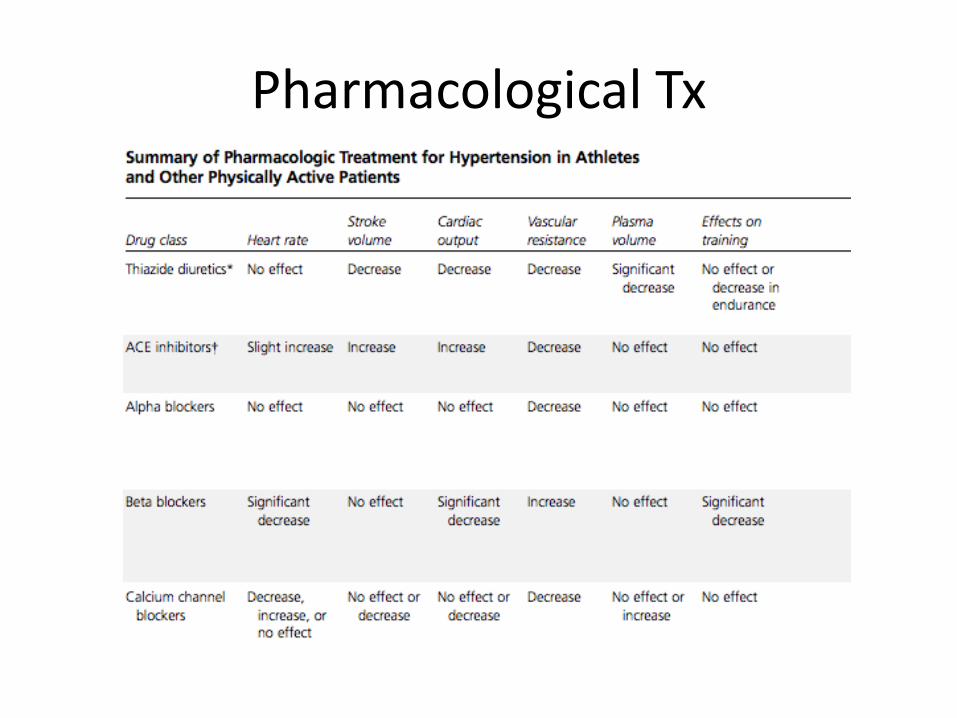
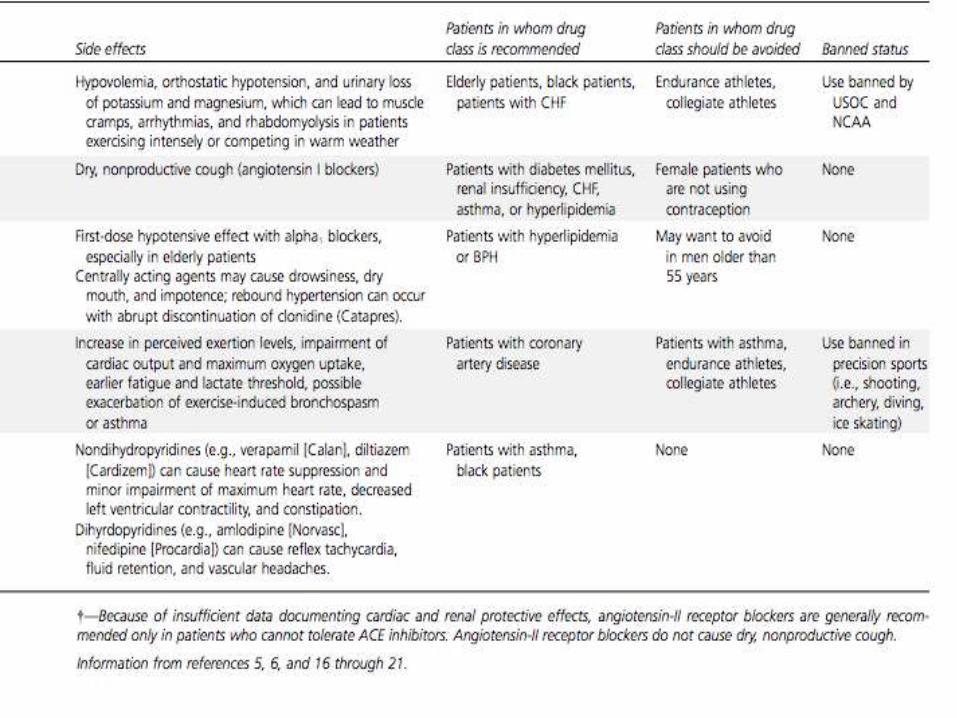
Pharmacological Tx

Calcium Channel Blocker
• Bind to calcium channels located on the vascular smooth muscle, cardiac myocytes, and cardiac nodal tissue
• Responsible for regulating the influx of calcium into muscle cellsstimulates smooth muscle contraction and cardiac myocytecontraction
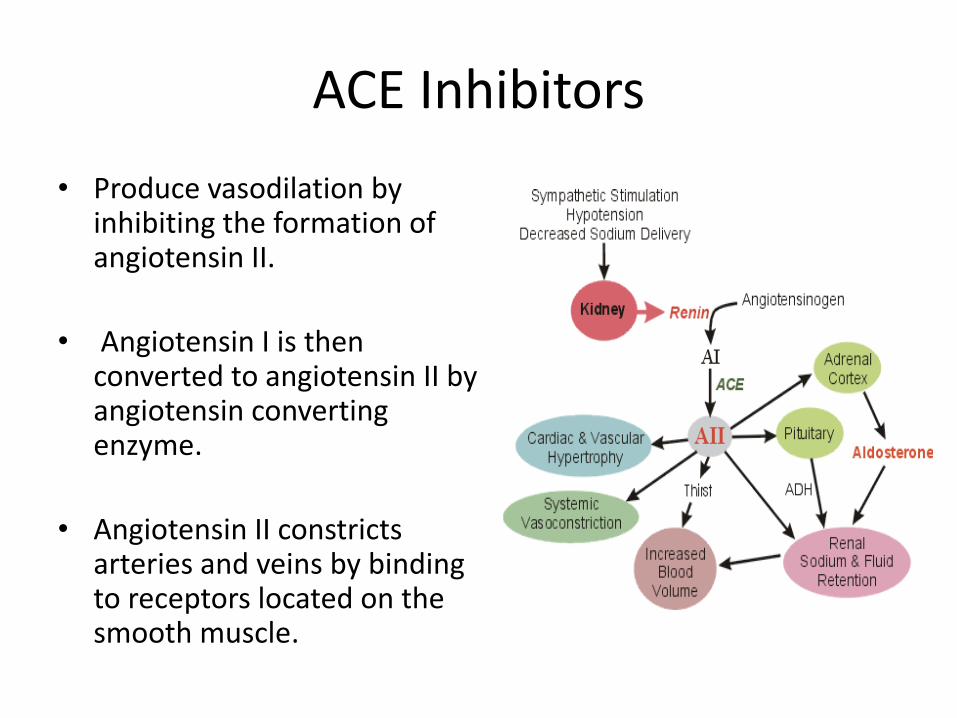
ACE Inhibitors
• Produce vasodilation by inhibiting the formation of angiotensin II.
• Angiotensin I is then converted to angiotensin II by angiotensin converting enzyme.
• Angiotensin II constricts arteries and veins by binding to receptors located on the smooth muscle.

Beta Blockers
• Bind to beta-adrenoceptors and thereby block the binding of norepinephrine and epinephrine
• Inhibits normal sympathetic effects that act through these receptors.
“Sudden Cardiac Death in Competitive Athletes”
“Hypertrophic Cardiomyopathy: A Systems Review”
A Summary By: Jonathan Noury

Sudden Cardiac Death
• “Unexpected sudden cardiac death that occurs within 6 hours of a previously normal state”
Pete Maravich (39)Congenital Missing Left Coronary Artery
Len Bias (23)Cocaine use Cardiac
arrhythmia
Epidemiology
• 1983-1993 (<35 y/o)– Incidence in males:
7.47:1,000,000
– Incidence in females: 1.33:1,000,000
• Older athletes (>35)- Estimated incidence:
1:15,000-1:50,000
Majority of deaths occur in basketball and football players
Even if there was a tool to screen for SCD with 99% sensitivity the PPV would be 0.05% 1 correct positive out of 2000 (1999 FP)
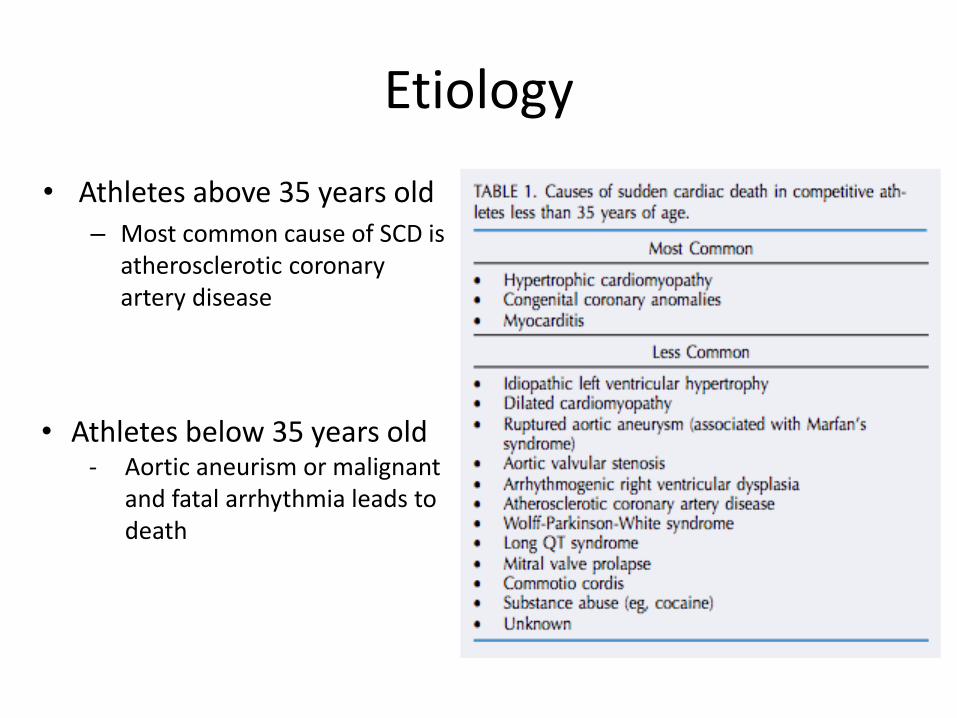
Etiology
• Athletes above 35 years old– Most common cause of SCD is
atherosclerotic coronary artery disease
• Athletes below 35 years old- Aortic aneurism or malignant
and fatal arrhythmia leads to death
Some Causes
• Hypertrophic cardiomyopathy– Autosomal-dominant congenital disorder
• Congenital coronary anomalies– Abnormal anatomical variations of coronaries
– Hypoplastic vessels
• Substance abuse– Leads to arrhythmia
• Wolff-Parkinson-White syndrome– Congenital extra electrical connection inside heart that acts as a
short circuit resulting in tachycardia

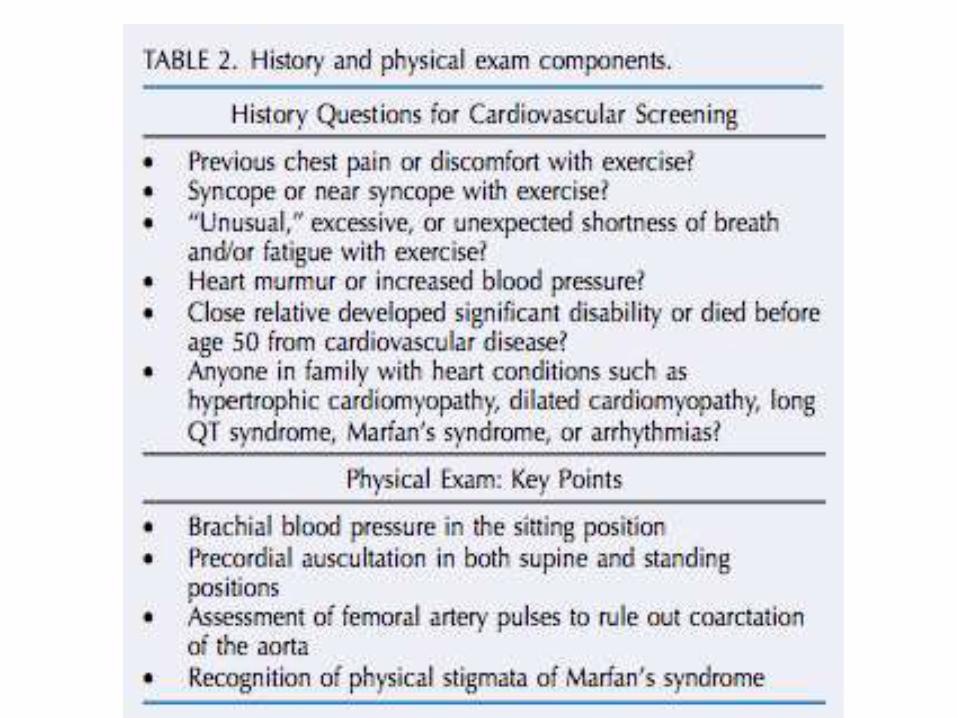
What To Look For
• Auscultation- Arrhythmias, heart sounds-
normal if they disappear with exercise
• History of:• Cardiac arrest • Ventricular Tachycardia• syncope or near syncope
with exercise• Chest pain • Unexpected or
unexplained SOB or fatigue with exercise
•Past detection of heart murmur•Low BP in response to exercise•FHx of SCD or relative who has suffered cardiovascular disease age< 50•FHX of hypertrophic cardiomyopathy, dilated cardiomyopathy, Marfan’ssyndrome
Detailed cardiovascular history

Marfan’s Syndrome
• Skeletal:– Arm span greater than height– Chest wall deformities– Kyphoscoliosis– High arched palate– Hyperextensible joints
• Cardiovascular:– Aortic or mitral regurgitation (murmur)
• Ocular:– Myopia (near-sightedness)– Ectopia lentis (dislocated lens)
Isaiah Austin
Non-Invasive Techniques
• If there is no significant history there is no reason to refer for:
– Stress Test
– Echocardiography
– Genetic Testing- Hypertrophic Cardiomyopathy

No Guarantee
• After examining an athlete for cardiovascular abnormalities the athlete should be advised that he/she is not guaranteed to be free potential sudden death.
• Study:– 134 athletes who had suffered SCD
– 115 undergone standard pre-participation screening
– 15 underwent individualized medical evaluation for heart disease
– Only 8 were accurately diagnosed prior to death
Interventions
• There are no published evidence based studies that show that a prescreen can reduce the risks of SCD.
• HOWEVER:
– In almost all cases of SCD, the final premorbid event was Ventricular fibrillation
• Decreases chance of survival by 10% every minute AED is delayed.
• In cases of V-fib , patient will have no pulse
Hypertrophic Cardiomyopathy
• Incidence: 1:500
– Most common genetic cardiovascular disease
• Typically Non-obstructive disease
– Autosomal dominant
• Mutation in 1/10 genes coding for cardiac sarcomeres
– Diagnosis:
• 2-dimensional Echocardiography/ECG
• Heart murmur
• Family history
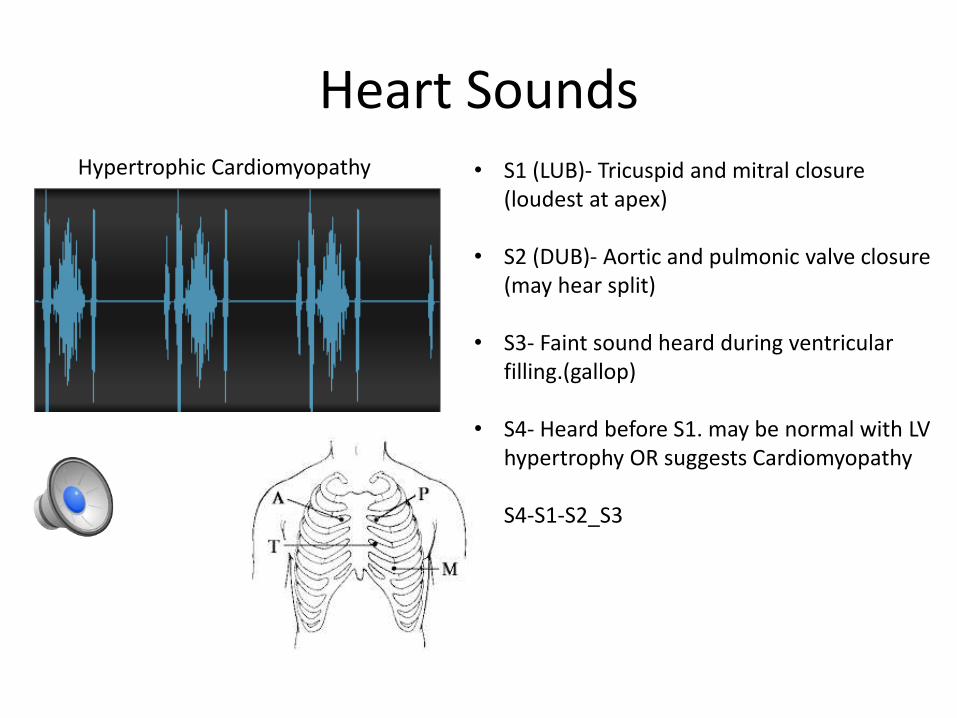
Heart SoundsHypertrophic Cardiomyopathy • S1 (LUB)- Tricuspid and mitral closure
(loudest at apex)
• S2 (DUB)- Aortic and pulmonic valve closure (may hear split)
• S3- Faint sound heard during ventricular filling.(gallop)
• S4- Heard before S1. may be normal with LV hypertrophy OR suggests Cardiomyopathy
• S4-S1-S2_S3
Diagnosis and Screening
• LV wall thickness as seen on echocardiography
– Normal: <13mm
– Mild: 13-15mm (also in trained athletes)
– Massive: >29mm
– 55% of HCM patients will not demonstrate any risk factors and it is uncommon for them to die suddenly

Prognosis
• Genetic testing provides most information regarding favorable or adverse prognosis.– B-myosin heavy chain and Troponin T mutations
may be associated with higher frequency of sudden death.
– If adult has gene but no LVH then their condition is usually benign.
– The less congestive symptoms present the better the prognosis. (unless you have the other risk factors)

What To Look For
• Auscultation- Arrhythmias, heart sounds-
normal if they disappear with exercise
• History of:• Cardiac arrest • Ventricular Tachycardia• syncope or near syncope
with exercise• Chest pain • Unexpected or
unexplained SOB or fatigue with exercise
•Past detection of heart murmur•Low BP in response to exercise•FHx of SCD or relative who has suffered cardiovascular disease age< 50•FHX of hypertrophic cardiomyopathy, dilated cardiomyopathy, Marfan’ssyndrome
Detailed cardiovascular history

Prevention
• Anti-arrhythmia medication, Beta Blockers
• Best not to start meds until symptomatic especially in children due to toxicity risk
• Implantable cardio-verter-defibrillator
– Placed inside chest to prevent arrhythmias
– Based on individual clinical judgment
• Lifestyle modifications
Gold Standard
• Ventricular septal myotomy-myectomy for children and adults with obstructive HCM.
– surgeon removes a small amount of the thickened septalwall to widen the outflow tract from the left ventricle to the aorta. This eliminates the obstruction and the mitral valve regurgitation that occurs with this condition. Patients often experience rapid relief of symptoms after the procedure

Alternate Tx
• Pacemaker- dual chamber pacing
– More accurately replicates ventricular and atrial contraction
• Alcohol septal ablation
– Introduce 1-4 mL of 100% concentrated alcohol (absolute) into coronary artery to infarct that tissue area to reduce the thickness
• Heart Transplant