improving health outcomes by linking the clinic to the community thomas sequist, md mph
TRANSCRIPT

Improving Health Outcomes by Linking the Clinic to the
Community
Thomas Sequist, MD MPH

What you have heard about US health care
• Poor quality
• Costly

Improving Chronic Care Outcomes
AHRQ National Quality Report 2012

Atrius Health
• Non-profit alliance of six leading independent medical groups▫ Granite Medical▫ Dedham Medical Associates▫ Harvard Vanguard Medical
Associates▫ Reliant Medical Group▫ Southboro Medical Group▫ South Shore Medical Center
• Providing care for ~ 1,000,000 adult and pediatric patients with 1000 physicians, 1450 other healthcare professionals across 35 specialties
.
Atrius Health
• 100% on an electronic medical record combined with corporate data warehouse, used for managing quality and cost.
• Long history with global payments: close to 50% of patients under global risk across Commercial, Medicare and Medicaid
• Widespread use of rosters in population management
• Track record of quality measurement and reporting
• All adult primary care sites accredited as NCQA Level 3 Patient Centered Medical Homes

Harvard Vanguard Medical Associates
• Multi-specialty group practice
• 17 ambulatory health centers
• 400,000 adult patients
• 175 primary care physicians

HVMA Diabetes Care Model
Population Management• Centralized patient mailings
Clinical Information Systems• Electronic medical record
• Computerized alerts
Patient Engagement• Primary care teams
• Diabetes dashboards
• Chronic disease visits
Improved Diabetes Care

Baseline Racial Disparities
White(n=4,858)
Black(n=2,699)
p value
Process measures, % Annual HbA1c test Annual LDL test
Outcomes measures, % HbA1c < 7% LDL < 100 mg/dL BP < 130/80 mmHg
8783
465532
8983
404324
0.140.99
<0.001<0.001<0.001

-15
-10
-5
0
5
0 20 40 60 80 100 120 140
Number of black patients
Bla
ck
-Wh
ite
Dif
fere
nc
e (
%)
Median = - 8.0%IQR = -6.9% to -9.4%p = 0.84
Panel Diversity and Disparities in LDL Control
Sequist; Arch Intern Med 2008

The “Not Me” Phenomenon
010
2030
4050
6070
8090
100
US Health System HVMA Your health center Your patients
% V
ery
or S
omew
hat
Oft
en
Do racial disparities in diabetes care exist in….
Sequist; JGIM 2008

Intervention Components
•Cultural competency training▫ 1 to 2 day course (89% team attendance)▫ Monthly educational materials
•Clinical performance feedback▫ Monthly distribution▫ Race-stratified (HbA1c<7%, LDL < 100, BP <
130/80)▫ Provider level (benchmarked to practice)

Sample Performance Report

Patient Survey Feedback

Impact on Clinician Awareness
8270
635951
43
0
20
40
60
80
100
All health centers Your healthcenter
Your patients% V
ery
or S
omew
hat
Oft
en
Intervention Control
Do racial disparities in diabetes care exist in….
P=0.003 P=0.02 P=0.04
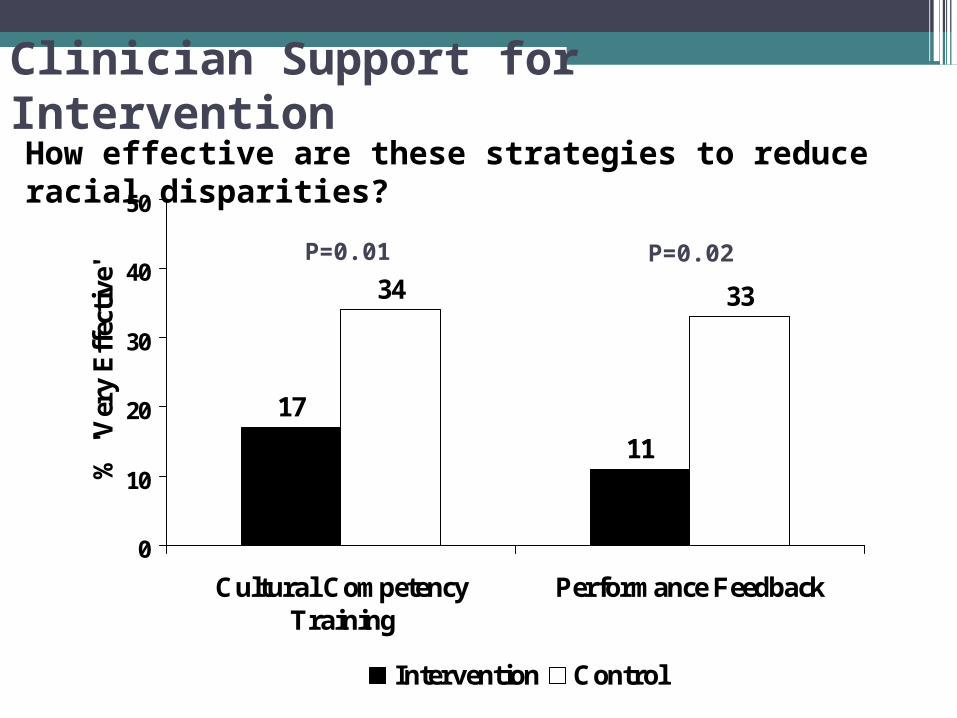
Clinician Support for Intervention
17
11
34 33
0
10
20
30
40
50
Cultural CompetencyTraining
Performance Feedback
% '
Ver
y E
ffec
tive
'
Intervention Control
How effective are these strategies to reduce racial disparities?
P=0.01 P=0.02

Clinician Views on Disparities
“Even though their diabetes might be under horrendous control, it wasn’t the top thing on life’s list. You know they might have a kid in jail, or they might have been in the midst of an eviction proceeding or others are at risk of losing their jobs. There were a lot of other topics that were higher on their list than their HbA1c of 13”
I think that I feel very overwhelmed by this whole kind of concept because in many respects I think that a lot of this is very, very difficult to change because of what happens outside of these four walls.

Clinician Views on Reports
Well it was an initial kind of negative feeling, you know, like I’m failing in these particular situations. But then there was a feeling of, well these are the things that we’ve really got to focus on so we’re just going to have to pull this apart and try and focus on these things.
It’s just not useful information. I see very little that I have accessible at my disposal to make any impact on it, and telling me that it's there, it changes or doesn't change, seems to be random and have absolutely nothing to do with what I personally do or can do.
Views on Cultural Competency Training
• Feeling that training educated on history of racism, trust, and bias
• Helped them to explore these concepts in clinical setting
“You know I never knew there wasn’t a grocery store [there], I felt so stupid, but now I understand…”

Where Does this Leave Us?
•Address social determinants
•Address built environment
•Systematic approach?
The 15 minute office visit will not be enough

Qu
ali
ty o
f P
rim
ary
Care
–
Com
mu
nit
y In
terf
ace
Current State
Ideal State
Integration of care plans
Payment models
Identifying community resources and partners
Primary care resources
Recognition/ ownership of issues
Toward A Rational Process

Different Viewpoints
Medical Clinic
Advantages:Access to health indicatorsDirect management of services
Disadvantages:Piecemeal interactionsLack of broader contextFocus on medical management
Public Health
Advantages:Focus on communitiesContextual approach
Disadvantages:Lack clinical contextNo integration into care plansMultiple constituents

Our Roadmap
• Change measurement paradigm▫ Allow clinicians to view communities
• Target communities for action▫ High disease prevalence▫ Poor quality▫ High penetration
• Identify successful strategies▫ Positive outliers and trajectories▫ Resource catalogue
• Clinical integration▫ Clinician liaison▫ EHR tools
Our Barriers
•Traditional performance focus on clinicians
•Clinician sphere of responsibility
•Systematic approach to community partnership
•Health center resources

Community Base Performance Measurement