implementing an early childhood developmental screening and surveillance program in primary care...
TRANSCRIPT

Implementing an Early Childhood Developmental Screening and Surveillance
Program in Primary Care Settings in the State of Illinois: Lessons Learned
Anita Berry MSN, CNP, APN, PMHS
Director, Healthy Steps Program, Advocate Children’s Hospital
Patty Mack MA, RN, LMFT, LPHA
Healthy Steps Specialist, Consultant, Advocate Children’s Hospital
2
Enhancing Developmentally Oriented Primary Care (EDOPC)Who - Advocate Children’s Hospital, the Illinois Chapter American Academy of Pediatrics, the Illinois Academy of Family Practice, the Ounce of Prevention Fund, and the Illinois Department of Health Care and Family Services
Goal – improve the financing, and delivery of preventive health and developmental services for children birth to age 3 years in the state of Illinois.

3
Methods Professional education Ongoing technical assistance for practices Emphasis on referral and connection with community
resources Collection of policy-relevant information on barriers to
care Opportunity for collaboration with stakeholders Access to resources via EDOPC website

4
Presentation Topics• Global development screening• Maternal depression screening• Social/emotional screening• Early autism detection and screening • Coordinating care between early intervention and the primary health care
home• Domestic violence screening*• Effects of domestic violence on children*• Early childhood obesity prevention*• Early childhood behavioral modification and limit setting*• Psychosocial issues for children ages 5 to 8 years*• Effects of trauma and violence on young children*• Bright Futures Guidelines for Health Supervision and Bright Futures Tool and
Resource Kit birth to 10 years • American Academy of Pediatrics Mental Health Tool Kit for Primary Care*
* Designates topics focused on Mental Health
5
Why Screen and Refer• 12% to 16% of American children meet
diagnostic criteria for developmental or behavioral disorder
• Best long-term outcomes when they receive early intervention (EI) services designed
• Research confirms effectiveness of EI • Cost savings
6
Surveillance, Screening, Checklists• What is happening in your practice now?
Define
– Surveillance
– Screening
– Checklist

7
Screening Tools for Primary Care• Ages and Stages Questionnaire third edition (ASQ-3)• Ages and Stages Questionnaire: Social Emotional (ASQ:SE)• Infant Development Inventory (IDI)• Child Development Inventory• Parents’ Evaluation of Developmental Status (PEDS)• Edinburgh Postnatal Depression Scale (EPDS)• Patient Health Questionnaire -9 (PHQ-9)• Modified Checklist for Autism in Toddlers Revised/Follow UP
(M-CHAT R/F)• Hurts, Insults, Threatens, Screams at (HITS)*• Pediatric Symptom Checklist (PSC)
* Not currently billable in Illinois
8
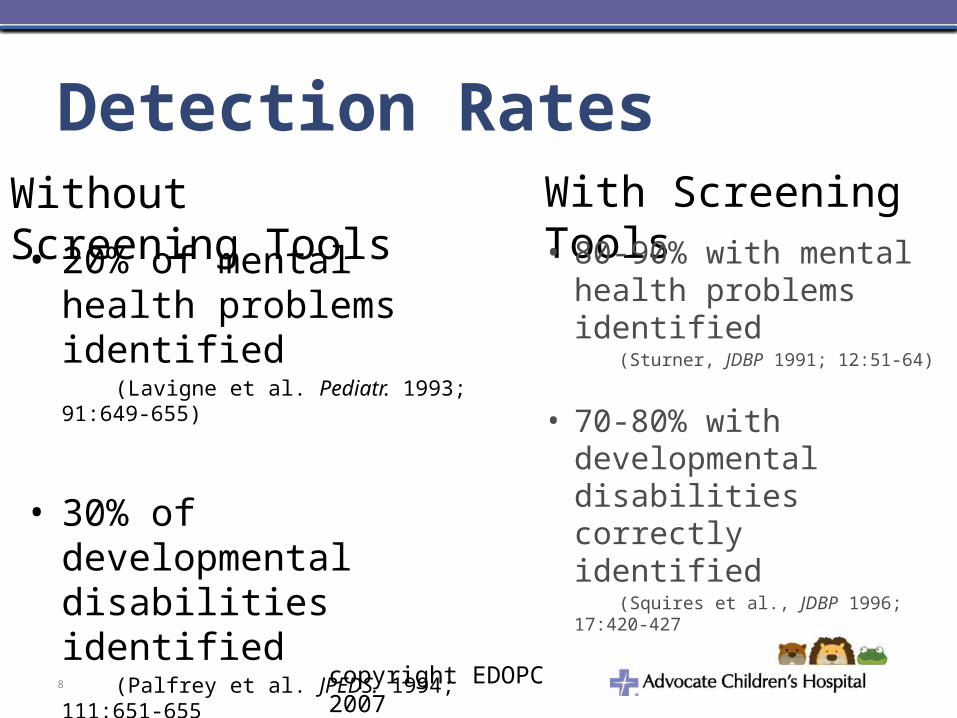
Detection Rates
• 20% of mental health problems identified
(Lavigne et al. Pediatr. 1993; 91:649-655)
• 30% of developmental disabilities identified
(Palfrey et al. JPEDS. 1994; 111:651-655
Without Screening Tools With Screening Tools• 80-90% with mental
health problems identified
(Sturner, JDBP 1991; 12:51-64)
• 70-80% with developmental disabilities correctly identified
(Squires et al., JDBP 1996; 17:420-427
copyright EDOPC 2007

What to Expect When Screening All Children in A Practice
11%: high risk of disabilities & need referrals for further evaluations
20%: low risk of disabilities & need behavioral guidance
26%: moderate risk of disabilities & need developmental promotion/vigilance
43%: low risk of disabilities & need routine monitoring
9
10
Getting a Project Started• Need the “Perfect Storm”
– Interest from key groups– Key partners– Funders

11
Data Regarding Developmental Screening • 90% of providers reported an increase in
skills and confidence after EDOPC intervention
• Prior to project 10% of children screened• Sites reported before intervention 33%
screened by one year visit; one year after intervention approximately 69%

Screening in Illinois Before and After EDOPC Training Intervention
% of site
s perfo
rmed sc
reening
% of patients
screened by t
hose si
tes
% of site
s perfo
rmed sc
reening
% of patients
screened by t
hose si
tes 0
20
40
60
80
1 year
after
perc
enta
ge
0
10
20
30
40
50
60
70
80
90
18 months
afterpe
rcen
tage
beforebefore

% of site
s perfo
rmed sc
reening
% of patients
screened by t
hose si
tes
% of site
s perfo
rmed sc
reening
% of patients
screened by t
hose si
tes 0
20
40
60
80
2 year
after
perc
enta
ge
before
Screening in Illinois Before and After EDOPC Training Intervention

14
CHIPRA Child Core Set Data Book: ODS Performance

15
State’s Steps to Improve Reporting of Developmental Screening
• Prioritize reporting of the Developmental Screening measure within the Medicaid agency.
• Reimburse providers for the 96110 code. • “Unbundle” the 96110 code, for example from EPSDT payments. • Partner across payers, providers, and other systems to collaborate
on performance improvement. • Reinforce the importance of developmental screening • Engage with providers and office staff on the benefits of
developmental screening, the importance of recording the 96110 CPT code.
• Prioritize the Developmental Screening measure in the state’s Medicaid Performance Improvement Projects (PIP) and in any provider pay-for-performance (P4P) programs.
16
Barrier and Solutionsto Screening
Barriers - Provider Expectations• perform physical examination,• administer appropriate
medical screenings• provide vaccinations and
laboratory testing• elicit parental concerns• educate caregivers • provide anticipatory guidance• conduct developmental and mental health
surveillance and/or screening• identify family risk factors and determine the need for referral(s) • lack of sufficient resources solutions• team approach

Communicating Results• Use language that encourages
follow-up• Be sensitive to cultural
meaning of words• Focus on positives first• Practice your language
– “Excellent gross motor skills”
– “He has a wonderful temperament, so adaptable”
– “Would like to help him learn and grow to his full potential”
– “Needs some extra attention and support”
17

Incorporating a Change in Practice:Using Plan Do Study Act Model (PDSA Cycles)
• PLAN: Plan a change or test how something works
• DO: Carry out the plan• STUDY: Look at the
results. What did you find out?
• ACT: Decide what actions should be taken to improve
18
Repeat as needed Until desired goal is achieved
Questions – Technical AssistanceAnita Berry
630-929-6663
Website: http://www.advocatechildrenshospital.com/ach/care-treatment/healthy-steps/
19

20