implementation research in conceptual and … · implementation research in tdr: conceptual and...
TRANSCRIPT
IMPLEMENTATION RESEARCH IN TDR:CONCEPTUAL AND OPERATIONAL FRAMEWORK
U N D P / W o r l d B a n k / W H O
Special Programme for Research andTraining in Tropical Diseases (TDR)

TDR/IDE/SP/03.1
Copyright © World Health Organization on behalf of the Special Programme for Researchand Training in Tropical Diseases 2003.All rights reserved.
The use of content from this health information product for all non-commercial educa-tion, training and information purposes is encouraged, including translation, quotation andreproduction, in any medium, but the content must not be changed and full acknowl-edgement of the source must be clearly stated. A copy of any resulting product with suchcontent should be sent to TDR,World Health Organization, Avenue Appia, 1211 Geneva27, Switzerland. TDR is a World Health Organization (WHO) executed UNDP/WorldBank/World Health Organization Special Programme for Research and Training in TropicalDiseases.This information product is not for sale.The use of any information or content whatsoev-er from it for publicity or advertising, or for any commercial or income-generating pur-pose, is strictly prohibited. No elements of this information product, in part or in whole,may be used to promote any specific individual, entity or product, in any manner whatso-ever.The designations employed and the presentation of material in this health informationproduct, including maps and other illustrative materials, do not imply the expression of anyopinion whatsoever on the part of WHO, including TDR, the authors or any parties coop-erating in the production, concerning the legal status of any country, territory, city or area,or of its authorities, or concerning the delineation of frontiers and borders.Mention or depiction of any specific product or commercial enterprise does not implyendorsement or recommendation by WHO, including TDR, the authors or any partiescooperating in the production, in preference to others of a similar nature not mentionedor depicted.WHO, including TDR, and the authors of this health information product make no war-ranties or representations regarding the content, presentation, appearance, completenessor accuracy in any medium and shall not be held liable for any damages whatsoever as aresult of its use or application. WHO, including TDR, reserves the right to make updatesand changes without notice and accepts no liability for any errors or omissions in thisregard. Any alteration to the original content brought about by display or access throughdifferent media is not the responsibility of WHO, including TDR, or the authors.WHO, including TDR, and the authors accept no responsibility whatsoever for any inac-curate advice or information that is provided by sources reached via linkages or referencesto this health information product.
Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1 1
CONTENTS
2 . . . . . . . . Rationale
3 . . . . . . . . Objective
4 . . . . . . . . Criteria
5 . . . . . . . . General operating principles
7 . . . . . . . . Challenges
8 . . . . . . . . Product portfolio for Implementation Research
IMPLEMENTATION RESEARCH IN TDR:CONCEPTUAL AND OPERATIONAL FRAMEWORK

2 Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1
There are many examples of potential-ly effective disease control productsthat have had only limited impact onthe burden of disease because of inad-equate implementation resulting inpoor access. Insecticide-impregnatednets (ITNs) have been shown toreduce overall child mortality by15-60% in field trials. But implementingITNs on a large scale has proven diffi-cult and only a fraction of African chil-dren at risk have access to the protec-tion of an ITN. Available antimalarialscould greatly reduce child mortality inAfrica if given promptly when needed,but recent situation analyses in severalAfrican countries showed that lessthan 10% of children with symptoms ofmalaria had access to appropriatetreatment within 24 hours after theonset of fever. TDR studies suggestmeasures that can improve promptdelivery of antimalarial drugs at thehousehold and community levels – e.g.training of shopkeepers and innovativepackaging of antimalarial drugs – andhome management of febrile illnesscan improve child survival. But theseinterventions have not yet been imple-mented on a large scale.
Praziquantel was a breakthrough forschistosomiasis control. Though initiallytoo expensive, the price has now comedown but treatment coverage remainspoor in Africa, the continent with thelargest schistosomiasis burden. Single-dose diethyl carbamazine (DEC) andivermectin were shown to be effectivefor large-scale treatment of lymphaticfilariasis and they are now the recom-mended drug regimen, in combinationwith albendazole, for the global elimi-nation programme. But it is proving difficult to achieve a sufficiently hightreatment coverage to ensure elimina-tion of transmission. Simple interven-tions based on regular washing ofaffected limbs with soap and water cangreatly reduce the suffering of patientswith elephantiasis, but it is not evidenthow to ensure effective implementa-tion of this intervention on a large scale.
All the above products have success-fully completed the classical R&Dprocess, and have been put on theshelf of proven disease control prod-ucts. But they failed to have their fullpotential impact because of majorimplementation problems that imped-
ed access. Research on these productsceased too early. It is now agreed thatresearch should not stop after provid-ing the proof of principle for a prod-uct, or after demonstrating its effec-tiveness in selected situations, but thatit has an additional critical role to playin helping solve major implementationproblems. Experience has shown thatimplementation research can make amajor difference and help ensure thatproven control products have theintended health impact. Examples arethe development of community-directed treatment (ComDT) foronchocerciasis, and development ofhome-management for uncomplicat-ed malaria. These examples used tobe exceptions but under its 2000-2005strategy, TDR is addressing implemen-tation research as an integral part ofthe research process. TDR supportsimplementation research for provenand currently available control prod-ucts, and is preparing for implementa-tion research on new products thatwould have a significant impact on dis-ease burden if access can be assured,such as rectal artesunate for malaria ormiltefosine for leishmaniasis. ■
RATIONALE FOR IMPLEMENTATION RESEARCH
Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1 3
Implementation research will focus ondiseases for which a disease controltool (or package of tools) is availableand proven to be efficacious, and thathas the potential to greatly reduce theburden of disease if the major imple-mentation problems could be resolvedand access be improved. Access isdefined as the facility with which dis-ease-affected populations can obtainrelevant components of specific publichealth interventions. Access reflectsboth the supply of and the demand forthe intervention. ■
OBJECTIVE OF IMPLEMENTATION RESEARCH
In order to achieve this objective, Implementation Research will:
1. Identify common implementation problems, and their main determinants,
which prevent effective access to interventions, and determine which of
these problems are susceptible to research;
2. develop practical solutions to these problems and test whether new imple-
mentation strategies based on these solutions, can significantly improve
access under conditions of routine disease control;
3. determine in collaboration with partners the best way to introduce these
new implementation strategies into the health system and facilitate their
full-scale implementation, evaluation and modification as required.
The overall objective ofimplementation research
is to significantly improveaccess to efficacious interventions against tropical diseases by developing practical
solutions to common, critical problems in theimplementation of these
interventions.

4 Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1
Implementation Research covers abroad research area. TDR will need toset clear priorities for implementationresearch and develop very focusedresearch activities. To help guide theprioritization process, TDR’s Scientificand Technical Advisory Committee(STAC) has defined the following crite-ria for implementation research to beundertaken by TDR:
• Research need for disease control
Implementation research should addresspriority problems for disease controlthat are amenable to research. Theneed for research on these problemsshould have been clearly expressed bydisease control programmes.
• Researchable questions
TDR’s mandate is research and thereneeds to be a clear distinction betweenimplementation research and routineactivities of disease control and pro-gramme implementation, such as moni-toring and evaluation. Implementationresearch will require clearly definedresearchable questions that can beaddressed by scientific methods, it
being understood that the exact defini-tion of research questions may requireexploratory research. The proposedresearch should also offer a goodprospect for innovative solutions todisease control problems.
• Expected health gain
Implementation research aims atimproving access in order to maximizethe impact of interventions on poorand marginalized populations. A majorcriterion for prioritizing implementa-tion research products should there-fore be the expected ultimate healthgain for the poor. This emphasis onhealth gain also implies focusing on alimited number of priority areas toensure the timely development of asolid evidence base for more effectiveimplementation strategies and thusbuild momentum for their application,rather than focusing on a large numberof small isolated issues that are unlikelyto have significant health impact.
• Possibility to extrapolate toother settings and diseases
Priority will be given to research for
which the results will be relevant for
other settings and health systems, and
for other diseases and control strate-
gies. Location-specific problems would
not be covered by implementation
research and would require the devel-
opment of local solutions through
operational research undertaken within
the context of a national control pro-
gramme. However, if similar problems
would occur in several different loca-
tions or settings, there may be an
underlying generic researchable prob-
lem that would justify implementation
research efforts. Most implementation
research may initially be disease specif-
ic, but a research proposal will receive
higher priority if it is likely that the
research findings can be extrapolated
to other diseases.
• Focus on process and outcomeindicators
The aim of implementation research isto improve access, and the evaluationof new and improved implementationstrategies will therefore focus onprocess and outcome indicators ofaccess, such as the percentage of chil-dren with fever receiving appropriatetreatment within 24 hours. STAC
CRITERIA FOR IMPLEMENTATION RESEARCH

Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1 5
deemed the specific focus on processand outcome indicators a necessaryand appropriate step which wouldfacilitate up-scaling of interventions. Itrecommended that the question ofaccess be de-coupled from the ques-tion of health impact: both may beimportant but they will generallyrequire a different study design.
Implementation research is a conceptthat is still evolving in TDR. Furtherexperience is needed to better definethe optimal boundaries, the most effec-tive division of labour with local opera-tional research, and how researchcapacity building can be undertakenmost effectively to optimize the impactof research on disease control. ■
GENERAL OPERATING PRINCIPLES
Implementation research requires adifferent mode of operation than inother research areas in TDR. The fol-lowing are general operating principlesthat are characteristic for implementa-tion research:
• Active link to disease control
Implementation research will needactive links to disease control in orderto properly understand implementa-tion problems, to ensure that pro-posed solutions are appropriate, andto accelerate uptake of these solutionsin disease control. This requires linkswith health services and disease con-trol programmes in endemic coun-tries, as well as active interaction withregional and global disease control ini-tiatives where such exist, e.g. Roll BackMalaria, Stop TB, Global Programmefor Elimination of Lymphatic Filariasis,African Programme for Onchocercia-sis Control, etc.
• Rapid response to needs ofdisease control
Implementation problems require
urgent solutions and implementation
research needs to respond rapidly to
the priority needs of disease control. If
the development of new solutions
takes too long, sub-optimal solutions
may get implemented that would be
diff icult to change at a later stage.
Hence, implementation research must
be rapid and responsive, as well as
flexible and proactive.
• Partnership
Successful implementation of inter-
ventions requires the involvement of
many partners, and special efforts
must be undertaken to ensure that
implementation research becomes an
effective and respected member of
such partnerships. Partnerships are
important to implementation research
as a source of information on devel-
opments in disease control implemen-
tation, and as a major target audi-
ence for reporting the findings and
recommendations of implementation
research, and for implementing the
solutions.
• Involvement of diseaseendemic country scientists
Implementation research requires
active involvement of researchers >

6 Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1
from endemic countries. It provides
them with an important opportuni-
ty to broaden their experiences and
skills in implementation research.
Implementation research will provide
additional support as required (e.g.
through skills training or protocol
development workshops, etc.) to
strengthen the research capacity
of national scientists and disease con-
trol staff. The main focus will be on
"learning by doing".
• Involvement of endemic country health professionals
Equally important is involvement of
health professionals in the area of health
systems development, programme
implementation and disease control
who can help ensure that the research
focuses on the major implementation
bottlenecks and who will be essential
in translating research findings into
improved implementation in real life.
• Smooth and flexible interaction with otherresearch areas of TDR
This is of particular importance forinteraction with the Steering Committee
on Proof-of-Principle research, whichfunds research into the effectiveness ofnew and improved intervention meth-ods, and for interaction with ResearchCapacity Strengthening.
• Collaboration with TDR co-sponsors
Implementation research will activelycollaborate with TDR's co-sponsors,especially at the implementation levelwhere there are important opportuni-ties for synergy between TDR'sresearch and the co-sponsors' supportto large-scale implementation initia-tives. Implementation research willalso work closely with related WHOprogrammes and with all concernedWHO offices at country and regionallevels.
• Active marketing of results
The available disease control tools andthe results of implementation researchmust be actively marketed at all levels:international, national, provincial, dis-trict and community. This will requirespecial implementation research activi-ties to develop cost-effective ways tomarket research findings. ■

Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1 7
Implementation research will bringmany new challenges. Developing agood understanding and building col-laboration with endemic communities,national health systems, Ministries ofHealth, and WHO regional offices,while at the same time remaining wellconnected with research and academ-ic institutions, will require buildingbridges between experts that do nottraditionally work well together. Thestaff profile of TDR may need to bemodified to include more experts inpublic health, health systems and dis-ease control programme manage-ment.
Implementation research could be-come expensive and labour intensive
particularly since real life challengesoccur during large-scale implementa-tion of control strategies. The balancebetween what resources are directlyattributable to control and which onesto research, and how control pro-grammes will contribute, will needcareful consideration.
New ways of fundraising may need to be developed, especially for dis-eases for which TDR does not have atradition of implementation research.Start-up funds may need to be identi-fied to enable TDR to demonstrate itscapability for implementation researchfor those diseases, and establish itscomparative advantage, before signifi-cant additional funding can be secured.
CHALLENGES

8 Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1
The Scientific and Technical AdvisoryCommittee endorsed the above frame-work for implementation research dur-ing its meeting of February 2003 andrequested TDR to clearly show howthe planned implementation researchactivities f it in the overall researcheffort of the Programme.
TDR's overall research priority settingprocess is based on a comprehensiveconsultative analysis of research needsand research opportunities. The resultingpriorities are summarized in the StrategicEmphasis Matrix which includes thestrategic emphases for implementationresearch. A portfolio of research prod-ucts defines the specific research activi-ties that TDR plans to undertake toaddress the strategic emphases. TheStrategic Emphasis Matrix and the prod-uct portfolio are regularly reviewed andupdated according to new researchneeds and opportunities. In January2003, the product portfolio for imple-mentation research was updated toreflect the refocusing on issues of access.The implementation research portfoliofor the 2004/2005 biennium is describedbelow.
In discussing the product portfolio, it is useful to differentiate between twotypes of implementation research:
1. Implementation research that is thenext logical step for products in theTDR research pipeline that are orwill soon be ready for implementa-tion and for which there are impor-tant research questions on howthey should be implemented and
brought up to scale in order toensure effective access.
2. Implementation research on TDRtools that have been developed inthe past and that are now the cor-nerstone of tropical disease controlbut for which there are major obsta-cles to large-scale and sustainedaccess.
PRODUCT PORTFOLIO FOR IMPLEMENTATION RESEARCH
Figure 1. IR as the next and final phase for products in the TDR pipeline
2002 2003 2004 2005 2006
SUp-scaling Home management
SScale up - Immunization plus
Cost-effective delivery strategies
impact of integrated fever mgmt on mortality
impact of rectal art. strategy on mortality
= Implementation research product = Implementation Strategy developed and testedS
Phase IV: safety
IPTI: morbidity impact
Miltefosine registration
SIntegrated fever mgmt
SDelivery of rectal artesunateRectal artesunate registration
Home management methods

Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1 9
The current products in the Implemen-tation Research portfolio are listed inTable 1 (see pages 12-13), which showsfor each product the main researchquestions, current or potential partnersand the resources required. Figure 1shows the timelines for the type 1products and indicates to which otherproducts in the TDR research pipelinethey correspond. Implementation research is the nextstep in the research pipeline for fourmajor TDR products: two drugs thatwere recently or will soon be regis-tered (rectal artesunate and milte-fosine), one intervention methodIntermittent Preventive Treatment ininfants (IPTi) for which the proof ofprinciple is being demonstrated interms of morbidity impact, and oneimplementation method (home man-agement of malaria) that has beenshown effective in improving access toappropriate antimalarial treatment atthe community level and in reducingmalaria mortality.
The home management approach hasbeen adopted by Roll Back Malaria, butas the previous studies were done at
small scale, there remain importantquestions about it's effective up-scalingthrough the public health system.Hence, one implementation researchproduct will focus on this issue in thecontext of up-scaling in RBM leadcountries in Africa. The studies onhome management have also led tothe concept of community-based inte-grated fever management, combiningtreatment against malaria and pneu-monia. There remain many questionsto be resolved about how this can be implemented effectively without jeopardising access to malaria homemanagement while ensuring properuse of antibiotics. This is the subjectof another implementation researchproduct. Similar questions on how todeliver the drug at the communitylevel are the subject of the implemen-tation research on rectal artesunate.
All products shown in Figure 1 areexpected to produce tested implemen-tation strategies within 2-3 years andthese will then be made available toMinistries of Health and control pro-grammes. The tools on which theseinterventions are based have all been
shown to be efficacious in reducingmorbidity. However, this informationmay not be considered sufficient to jus-tify large-scale implementation of rectalartesunate and integrated fever man-agement and it is planned to undertaketrials of their effectiveness in reducingchild mortality, once the implementa-tion strategy has been worked out.
The implementation research productsin Figure 1 cover all major products thatare approaching the end of the devel-opment phase in the TDR researchpipeline, with the exception of Lapdap,where the main questions relate to its effectiveness and safety, and which is therefore covered by anotherresearch activity outside implementa-tion research. Access to artesunatecombination treatment will be coveredby implementation research on homemanagement.
Figure 2 (see page 10) shows thetimelines for the type 2 products, andthe major implementation problemsthey respond to. Three of the diseasesare in TDR's disease category III forwhich the "control strategy is proven >

10 Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1
effective, disease burden falling andelimination is planned". For these dis-eases, TDR's overall strategic emphasisis on improved implementation strate-gies, and hence they feature prominent-ly in the implementation research port-folio.
The tools used in the interventions inFigure 2 have all been developed previously by TDR, i.e. single-doseDEC or ivermectin +/- albendazole forlymphatic filariasis, ivermectin foronchocerciasis, praziquantel for schis-tosomiasis and MDT for leprosy.Significant progress is being made withcontrol of the diseases concerned, butthere remain major implementationchallenges for which research input is urgently required. The need forresearch has been clearly expressed bythose responsible for implementationand this strong demand for researchgreatly facilitates the necessary collabo-ration between research and control. The implementation research productsfor lymphatic filariasis and onchocer-ciasis have already been startedalthough some, e.g. on community levelmanagement of lymphoedema/ADL,
on a very limited scale due to lack offunds. The research on multi-diseaseComDT is a response to both a chal-lenge (sustained annual ivermectintreatment over a period of decades)and an opportunity (the success withcommunity-directed treatment foronchocerciasis providing a possiblemodel for integrated delivery of com-munity-based interventions). This is an example where implementation
research for one disease may con-tribute to health sector development ingeneral and to improved implementa-tion for other diseases. The implemen-tation research products for schistoso-miasis and leprosy have not yet starteddue to lack of funds.
The research questions that all theseproducts address are summarized inTable 1. There are two types: questions
Figure 2. IR in response to priority implementation problems in the field
2002 2003 2004 2005 2006
SDrug delivery in urban areas
SMulti-disease ComDT
SDrug delivery strategies, Africa
Scale-up schisto mapping
SStrategies for integration of residual control
SHome management of Lymphoedema/ADL
= Implementation research product = Implementation Strategy developed and testedS
implementation problems in LF elimination
Community effectiveness
of ComDT
Stagnation of schistosomiasis control in Africa
SWG Leprosy: problems withintegration of leprosy control

Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1 11
Op
en
he
re t
o s
ee
Tab
le 1
on how to implement and ensureeffective access by those in need, andquestions on how to bring the inter-ventions to scale within the context ofthe health system constraints inendemic countries. Both are criticaland both need to be addressed ifTDR's research is to have the intendedimpact.
Table 1 also shows that there areestablished or anticipated links with therelevant international disease con-trol/elimination initiatives and selectedMinistries of Health. Furthermore, theconcerned WHO programmes areinvolved and contribute to the planningand implementation of the researchactivities.
The main problem for ImplementationResearch is that of funding. Funds arecurrently only available for 5 of the 11implementation research products, andfor none of those do the availablefunds meet the requirement. The bestfunded product is that on up-scaling ofmalaria home management, for which70% of the required funds have beensecured from TDR's undesignated
funds. But only 30% of the requiredfunds are available for the product on sustainable management of lym-phoedema/ADL, a level at which theproduct cannot be properly imple-mented. For 6 of the 11 products, nofunds have yet been identified.
TDR has been successful in devel-
oping efficacious interventions
for targetted tropical diseases.
The remaining challenge is to
ensure access to these interven-
tions by those who need them.
Implementation Research will be
critical to make this happen.
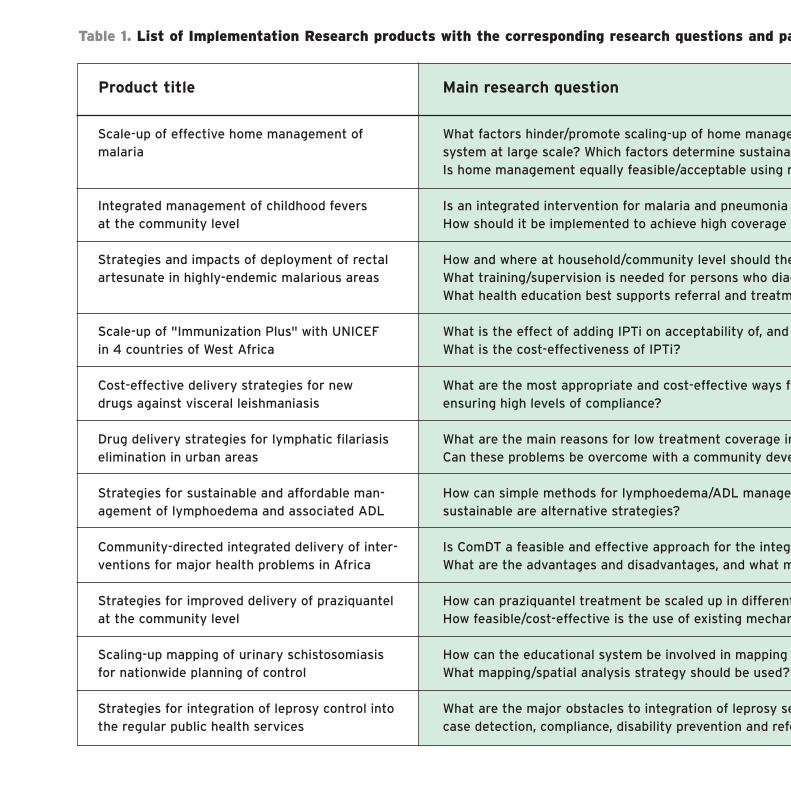
Table 1. List of Implementation Research products with the corresponding research questions and pa
Product title Main research question
Scale-up of effective home management ofmalaria
Integrated management of childhood fevers at the community level
Strategies and impacts of deployment of rectalartesunate in highly-endemic malarious areas
Scale-up of "Immunization Plus" with UNICEF in 4 countries of West Africa
Cost-effective delivery strategies for new drugs against visceral leishmaniasis
Drug delivery strategies for lymphatic filariasiselimination in urban areas
Strategies for sustainable and affordable man-agement of lymphoedema and associated ADL
Community-directed integrated delivery of inter-ventions for major health problems in Africa
Strategies for improved delivery of praziquantelat the community level
Scaling-up mapping of urinary schistosomiasisfor nationwide planning of control
Strategies for integration of leprosy control intothe regular public health services
What factors hinder/promote scaling-up of home managesystem at large scale? Which factors determine sustainaIs home management equally feasible/acceptable using m
Is an integrated intervention for malaria and pneumonia How should it be implemented to achieve high coverage a
How and where at household/community level should theWhat training/supervision is needed for persons who diagWhat health education best supports referral and treatm
What is the effect of adding IPTi on acceptability of, and What is the cost-effectiveness of IPTi?
What are the most appropriate and cost-effective ways foensuring high levels of compliance?
What are the main reasons for low treatment coverage inCan these problems be overcome with a community deve
How can simple methods for lymphoedema/ADL managesustainable are alternative strategies?
Is ComDT a feasible and effective approach for the integrWhat are the advantages and disadvantages, and what m
How can praziquantel treatment be scaled up in differentHow feasible/cost-effective is the use of existing mechan
How can the educational system be involved in mapping What mapping/spatial analysis strategy should be used?
What are the major obstacles to integration of leprosy secase detection, compliance, disability prevention and refe

artners (October 2003)
Current/potential partners
ement of malaria. What is the most cost-effective and sustainable distribution bility? What adaptations are needed for IEC and in urban settings? more effective/expensive drugs?
in children feasible and acceptable to communities? and adherence by caregivers? How to make the intervention sustainable?
e drug be made available for optimal access?gnose, treat, provide referral advice, monitor treatment?
ment advice?
compliance with EPI (including EPI coverage) and how can it be optimized?
or detecting patients, delivering miltefosine to the most affected groups and
n urban areas? elopment and partnership strategy?
ment be brought to scale? How feasible, cost-effective and
rated delivery of community-based interventions? modifications are needed?
t endemic regions in Africa?nisms for other diseases?
schistosomiasis using the red urine questionnaire?
ervices and what are possible solutions that can sustain adequate levels of access,erral?
RBM, MoH, AFRO,WHO/MAL
UNICEF, MAL, CAH
RBM, MAL, EDM
UNICEF
MoH India, CPE
ICMR, NICD, CPE
CPE
APOC, RBM
SCI, CPE
SCI, CPE
International NGOs,CPE
Conceptual and Operational Framework for Implementation Research in TDR • TDR/IDE/SP/03.1 12-13
Design and layout: Lisa SchwarbAll pictures: WHO/TDR/Crump (www.who.int/tdr/media/image.html)
Mailing address:TDRWorld Health Organization20, Avenue Appia1211 Geneva 27Switzerland
Street address:TDRCentre Casai53, Avenue Louis-Casai1216 Geneva Switzerland
Tel: (+41) 22-791-3725Fax: (+41) 22-791-4854E-mail: [email protected]: www.who.int/tdr