implementation / quality improvement some practical wisdom
TRANSCRIPT

Implementation / Quality
Improvement Some practical wisdom
Tim Stephens BA (Hons), MSc, RGN QI Specialist & Nurse Researcher
Critical Care and Perioperative Medicine Research Group, Queen Mary, University of London

Learning objectives
1. Understand the development of the sciences of improvement & implementation
2. Learn some key strategies for doing improvement at the frontline
3. Learn some strategies for doing good, robust improvement research

1. Methods for improving quality and safety
Q & S in healthcare
Audit
QI
IS
Legal
Prof
Training

The Audit Cycle
Problem #1 with the audit cycle is that is a before and after study – so you can understand how the system may be at variance to the standards, but not the variation in the system

The Audit Cycle
Problem #2 with the audit cycle is that ‘implement change’ belies the often challenging and complex nature of improvement activities, and the need for specific change methods

Quality Improvement & Implementation Science

The science of QI
• Knowledge from industry • Juran and Deming – Japanese car industry • Promoted by the IHI since late 1990s • Primarily process and system
improvement • More practical than academic • Underpinned by:
– understanding variation – using local expertise – understanding the psychology of change – an ethos of learning by doing

Donabedian's model of quality assessment
1. Access to imaging
2. Emergency theatre capacity
3. On-call rotas
1. Pathways 2. Cons
delivered care
3. Mortality risk scoring
4. Time to theatre
5. Critical care admission
1. LOS 2. Mortality

Quality Improvement
• “Every system is perfectly designed to achieve the results that it gets; if you want to improve results then you have to change the system”
• Paul Batalden, IHI
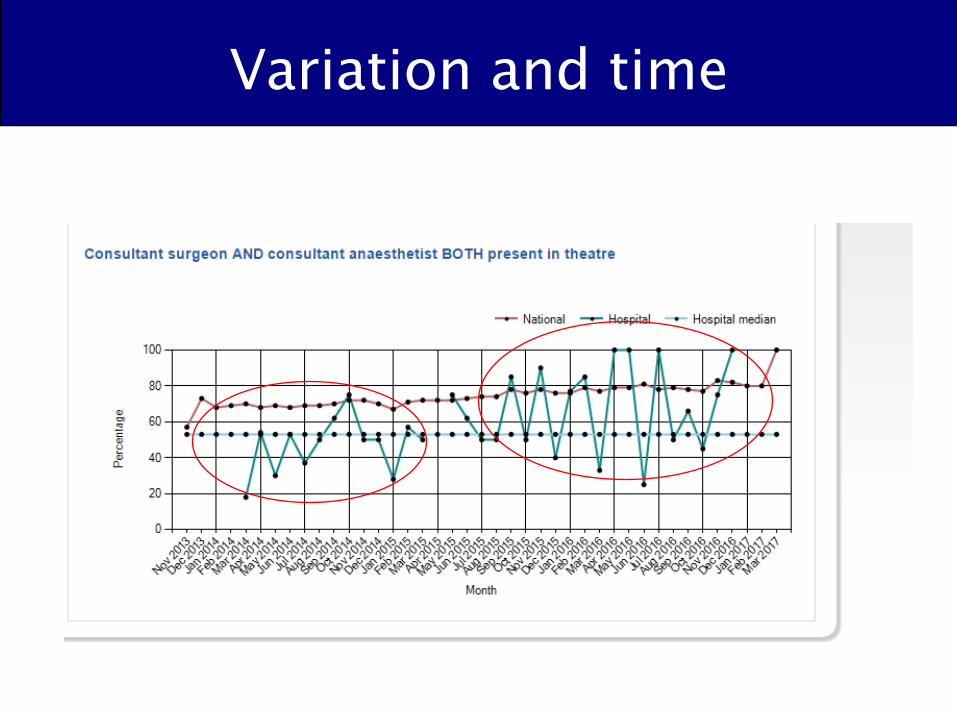
• “If I was to say what was the one most important thing to improve quality, it is understanding and reducing variation…”
• Don Berwick, IHI

Variation and time

Variation and time
Variation and time

Variation and time

Variation and time

Variation and Time
Median
0
5
10
15
20
25
30
Mar-12
Apr-12
May-12
Jun-12
Jul-12
Aug-12
Sep-12
Oct-12
Nov-12
Dec-12
Jan-13
Feb-13
Mar-13
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
% Overall 30 Day Mortality
Pathway Implemented

What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make that will result in
improvement?
The Model for Improvement
Source:
Langley, et al. The Improvement Guide, 1996.
The three questions provide the
strategy
Act Plan
Study Do
Act Plan
Study Do
Act Plan
Study Do
Act Plan
Study Do
Quality Improvement
• Extension and improvement on audit cycle
• Generally (not always) continuous measures
• Explicit change method – usually PDSA


Implementation Science
• Developed from the social and behavioural sciences
• Based upon theoretical frameworks – Diffusion of Innovation theory – Theoretical Domains Framework – Consolidated Framework for Implementation
• More interested in influencing people • Attempts to embrace complexity • Perhaps more academic than practical

Consolidated Framework for Implementation and ResearchDamschroder et al (2009)
Milbank QuarterlyVolume 82, Issue 4, pages 581-629, 9 DEC 2004 DOI: 10.1111/j.0887-378X.2004.00325.x http://onlinelibrary.wiley.com/doi/10.1111/j.0887-378X.2004.00325.x/full#f3

One definition of improvement:
• “The conception of improvement finally reached as a result of the review was to define improvement as better patient experience and outcomes achieved through changing provider behaviour and organisation through using a systematic change method and strategies”
• Øvretveit J. 2009 Does improving quality save money? A review of the evidence of which improvements to quality reduce costs to health service providers. London: Health Foundation,

All improvement has…
A ‘hard core’:
A ‘soft periphery’:
Context:
Langley A, Denis J Beyond evidence: the micropolitics of improvement Quality and Safety in Health Care 2011;20:i43-i46.

All improvement has…
A ‘hard core’: Clinical intervention / process
A ‘soft periphery’: Strategy to get intervention into practice / improve process
Context: Team / organizational culture, pressures, leadership etc

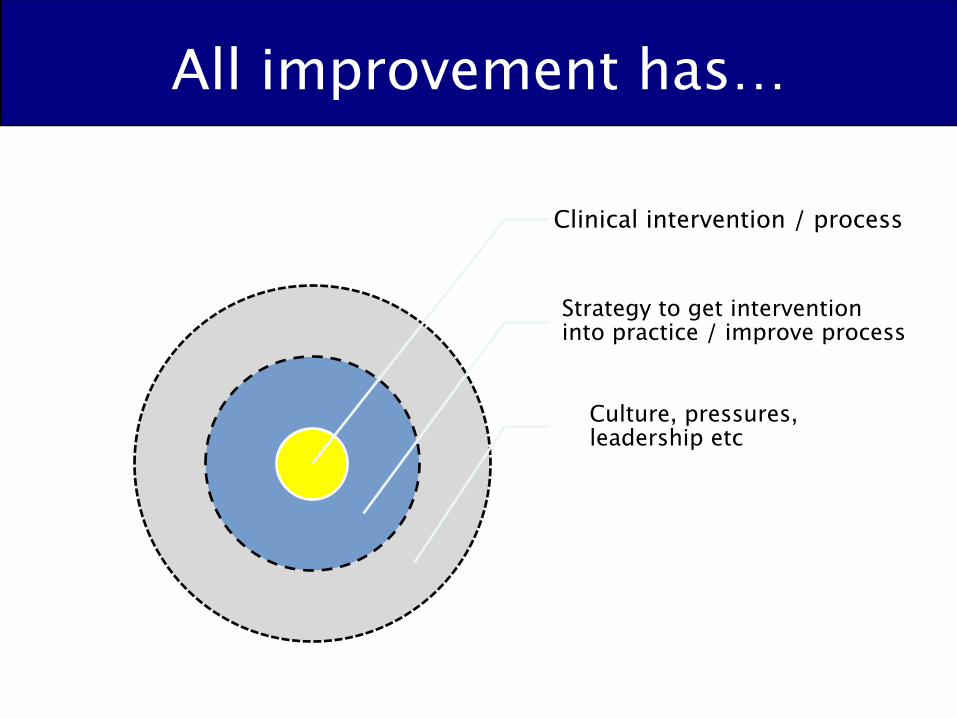
All improvement has…
Clinical intervention / process
Strategy to get intervention into practice / improve process
Culture, pressures, leadership etc

Audit, implementation of research findings and QI

Difference b/t QI and implementation
• QI – problem focussed • Implementation – solution focussed • QI – both the hard core (the ‘what’) and
the soft periphery (‘the how’) are explored
• IS – usually just the soft periphery (the ‘how’, because the ‘what’ is known)

Quality Improvement
• How to get more EmLap patients to theatre in a timely manner? – No one single correct way – Different solutions will work in different contexts – Understanding the local context vital to success
– No evidence based solutions – But...
• can learn from other centres experiences (whose ideas may or may not work for you)
• Generate and test ideas from your team

Implementation
• Evidence based intervention(s) exist
• In an ideal world, the solution would be in reliably delivered in a very similar way everywhere
• Context is key to the implementation, but not to the clinical solution

2. Doing improvement
• ‘Every system is perfectly designed to get the results it gets. The only way to get real change is to change the system. To do this you need ‘will, ideas and execution’.
ü You must have the Will to make the system change ü You must have Ideas about how you could change
things ü You must have skills to make it happen: Execution.
Paul Batalden IHI 1984

1. Convince people that there is a problem 2. Convince people of the proposed solution 3. Establish sound data / measurement systems 4. Avoid over-ambition / ‘projectness’ 5. Consider organisational context and capacity 6. Overcome tribalism - ownership / shared goals 7. Getting leadership right 8. Incentivise participation/use ‘hard-edges’ carefully 9. Sustainment - use team approach / embed practice 10. Be aware of side effects

Clinical vs improvement interventions
• Would you prescribe / give a patient a clinical intervention without a clear rationale for its: – purpose? – mechanism of effect? – predicted result?
• Yet we often ‘treat’ clinical systems with interventions with very little thought for if and how the intervention will work

Rationale: treating new onset hypertention in 60 yr old man
• If: – Amlodipine 5mg is trialled & – BP and side effects monitored & – Lifestyle advice given
• Then: – BP is physiologically lowered (calcium channel blockade) & – Medication can be titrated according to effect & – Lifestyle causes of hypertension may be reduced
• So that: – New onset hypertension can be safely treated
• So that: – Hypertension related organ dysfunction is prevented

Rationale / Theory of change If -‐ Relevant data are reviewed and fed back to teams regularly, &
-‐ Key professionals come together to form an improvement team, &
-‐ QI leads and colleagues learn basic quality improvement approaches, &
-‐ Relevant stakeholders are made aware of the project and improvement goals
Then
-‐ A shared view of performance and improvement gaps can be created , &
-‐ Professionals can work as a team to define and achieve local improvement goals, &
-‐ Basic quality improvement approaches can be employed to achieve the improvement goals, &
-‐ Stakeholders will be more engaged in the need for change and aware of how improvement will occur
So that
-‐ Improvements in care delivery in line with the recommended care pathway can be achieved
So that
-‐ Mortality aGer emergency laparotomy can be reduced.

Collaborative goals and drivers
Goal: Cholecystectomy within 8 days of
presentation (Measure: % eligible admitted patients having surgery ≤8
days)
Primary Driver 1: Reduce time to
diagnosis to within 24hrs from
presentation
2⁰ Driver 1: Timely imaging / diagnosis
2⁰ Driver 2: Timely decision making
Primary Driver 2: Reduce time to surgery To within 2 days from diagnosis (IP); 7 days
(OP)
2⁰ Driver 3: Clear pathway of care
2⁰ Driver 4: Surgical capacity
2⁰ Driver 5: Theatre capacity
2⁰ Driver 6: Support of theatre team &
management

1. Convince people that there is a problem 2. Convince people of the proposed solution 3. Establish sound data / measurement systems 4. Avoid over-ambition / ‘projectness’ 5. Consider organisational context and capacity 6. Overcome tribalism - ownership / shared goals 7. Getting leadership right 8. Incentivise participation/use ‘hard-edges’ carefully 9. Sustainment - use team approach / embed practice 10. Be aware of side effects

The 7 Steps to QI Measurement

1. Convince people that there is a problem 2. Convince people of the proposed solution 3. Establish sound data / measurement systems 4. Avoid over-ambition / ‘projectness’ 5. Consider organisational context and capacity 6. Overcome tribalism - ownership / shared goals 7. Getting leadership right 8. Incentivise participation/use ‘hard-edges’ carefully 9. Sustainment - use team approach / embed practice 10. Be aware of side effects

¢
What are we trying to accomplish?
How will we know that a change is an improvement? What change(s) can we make that will result in
improvement?
The Model for Improvement
Act Plan
Study Do Source: Langley, et al. The Improvement Guide, 1996.
The three questions provide
the strategy
The PDSA cycle provides the
tactical approach to
work

What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make that will result in
improvement?
The Model for Improvement
Source:
Langley, et al. The Improvement Guide, 1996.
The three questions provide the
strategy
Act Plan
Study Do
Act Plan
Study Do
Act Plan
Study Do
Act Plan
Study Do

What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make that will result in
improvement?
The Model for Improvement
Source:
Langley, et al. The Improvement Guide, 1996.
The three questions provide the
strategy

What are we trying to accomplish?
How will we know that a change is an improvement?
What changes can we make that will result in
improvement?
The Model for Improvement
Source:
Langley, et al. The Improvement Guide, 1996.
The three questions provide the
strategy

¢
What are we trying to accomplish?
How will we know that a change is an improvement? What change(s) can we make that will result in
improvement?
The Model for Improvement
Source: Langley, et al. The Improvement Guide, 1996.
The three questions provide
the strategy

Some change methods
The ‘hard core’
The ‘soft periphery’
Your context!

Rationale
• Why do you think that this/these interventions will work to improve care in your context at this time?
All improvement has…
Clinical intervention / process
Strategy to get intervention into practice / improve process
Culture, pressures, leadership etc

¢
What are we trying to accomplish?
How will we know that a change is an improvement? What change(s) can we make that will result in
improvement?
The Model for Improvement
Source: Langley, et al. The Improvement Guide, 1996.
The three questions provide
the strategy
3. Doing improvement research
• Tension between: – doing improvement and – studying improvement
• Sometimes doing is all that is possible but
• Studying & doing develops the science • If planned right, studying can improve
doing



Guidance on QI reporting

RATIONALE / THEORY
• Frameworks, models, concepts, theories used
• Ideas / assumptions that guided intervention development
• “Why do you think this intervention(s) will work in this setting at this point in
time?”

Tips for developing your rationale:
• Make sure all the problem(s) have been identified – ask all stakeholders
• Make sure you keep good records of this process, it will help you with context/methods writing
• Develop explicit diagrams to outline why you are doing what you are doing – your Mum should be able to follow your reasoning


STUDY OF THE INTERVENTION
Assessment of: • Impact of the intervention on the
systems and people • (Did it work?) • Whether or not the observed change was
likely a result of your intervention • (Did it work for the reasons you think it did?)

Tips for ‘studying the intervention’
• Should be built into your work – not easily done afterward
• Check fidelity of your implementation/uptake – Process measures
• Collect data on predicted effect modifiers – e.g. colleague reaction to new practice / process
• Always be a little sceptical of your success: – look for alternative explanations – consider potential confounders
• Check for unintended effects –good and bad
CONTEXT
• The setting in which the problem occurs and the work is done
• Like “setting” in biomedical model - only much more
• Called ‘thick description’ in social sciences • ‘All the things that are not your
intervention’ • Contextual elements that interacted with the
intervention(s) (All the things that made it succeed /
made it fail)
Summary
• Improving quality ≠ Quality Improvement • Many different change methods • RelaLvely limited evidence base currently • Rapidly evolving area of applied health research
• Use the 3 quesLons in the Model for Improvement and be clear why you are doing what you are doing!


References
• Perla, R.J., Provost, L.P. and Murray, S.K., 2011. The run chart: a simple analytical tool for learning from variation in healthcare processes. Quality and Safety in Health Care, 20(1), pp.46-51.
• Dixon-Woods, M., McNicol, S. and Martin, G., 2012. Ten challenges in improving quality in healthcare: lessons from the Health Foundation's programme evaluations and relevant literature. BMJ Qual Saf, pp.bmjqs-2011.
• Goodman, D., Ogrinc, G., Davies, L., Baker, G.R., Barnsteiner, J., Foster, T.C., Gali, K., Hilden, J., Horwitz, L., Kaplan, H.C. and Leis, J., 2016. Explanation and elaboration of the SQUIRE (Standards for Quality Improvement Reporting Excellence) Guidelines, V. 2.0: examples of SQUIRE elements in the healthcare improvement literature. BMJ Qual Saf, 25(12), pp.e7-e7.
• Shouls, G., Jarrar, Z. and Wickenden, J., 2014. Improving phlebotomy handover to doctors: a quality improvement project. BMJ quality improvement reports, 3(1), pp.u204813-w2033.
Examples
• Improving phlebotomy / FY Dr working • ELPQUIC • EPOCH

• “Every system is perfectly designed to achieve the results that it gets; if you want to improve results then you have to change the system”
• Paul Batalden, IHI
• “If I was to say what was the one most important thing to improve quality, it is understanding and reducing variation…”
• Don Berwick, IHI