impact and cost effectivene of rotavirus vaccine introduction in afghanistan
TRANSCRIPT

Draft for Discussion
IMPACT AND COST-
EFFECTIVENESS
ANALYSIS
O
F ROTAVIRUS VACCINE
INTRODUCTIONAFGHANISTAN, 13th June 2017

Outlin
e Introduction
Study objectives
Introduction to the economic model
Key model parameters and study
inputs
Preliminary results
Sensitivity analysis
Conclusion
2

Introduction to Cost-Effectiveness
Analysis
3

What is “cost-effectiveness”
(CE)?Analysis of the costs and benefits of rotavirus (RV)
vaccination to determine whether investment in rotavirus
vaccine introduction achieves greater or lesser health
outcomes relative to no intervention.
DALY: Disability-adjusted life-year
DALYs measure the total years lost to death and disability,
attributable to a particular disease.
Incremental cost-effectiveness ratio (ICER): The cost to avert one DALY
This ratio is then compared to per capita GDP to determine the country
specific (or WHO) threshold values for cost-effectiveness*
• Compare ICER to threshold to determine if it is a good value from the country’s
perspective
4

Disability-adjusted life-year5

Incremental cost-effectiveness ratio
(ICER)6
Assessing COSTS…Vaccine procurement
Immunization program incremental costTreatment cost (economic burden of disease)
… and BENEFITSBased on vaccine effectiveness and impact:
Reduction in cases, Outpatient and inpatient visits,
Deaths

Important questions which cost-effectiveness can
help to
answer What would be the budget impact of introducing RV
vaccine?
How many lives would be saved by introducing RV
vaccine?
How many hospital admissions? Cases?
What is the cost associated with RV disease and
with a RV vaccine program?
What is the added value in terms of costs and benefits
of RV
vaccine?
7

Study
Objectives
8

Study
objectives1. Evaluate the impact and cost-effectiveness of introducing
RV
vaccine into Afghanistan’s national immunization program
(NIP).
2. Develop and consolidate the evidence base to support a
decision about introducing rotavirus vaccine into the NIP.
3. Provide evidence to enable government’s buy-in,
support, and commitment to the vaccination program.
4. Strengthen Afghanistan’s national capacity to perform
economic
evaluations.
Strengthen evidence-based vaccine decision making.
9

Snapshot:
Illustrative Afghanistan RV
burdenOutcomes related to rotavirus in children
aged 1-59 months during one year (without vaccination)
Annual incidence per 100,000 10,000
Cases 497,999
Outpatient visits 269,898
Hospital admissions 20,069
Deaths 4,880
Total health service costs
government/societyUS$640,836/ US$14,280,283
10

Introduction to the Economic Model:
UNIVAC
11

Economic model:
UNIVAC UNIVAC (version 1.2.09)
A single universal vaccine impact and cost-effectiveness decision support model
Developed by Andrew Clark from the London School of Hygiene andTropical Medicine
Excel-based static cohort model
Evaluates vaccine introduction impact, costs, and cost-effectiveness/cost- utility
Building on prior economic tools developed for PAHO’s ProVac initiative and used widely in the America’s and beyond since 2006
12

Country decisions supported by ProVac
tools13

Model compares
scenarios14

Model
overview15

Key Model Parameters and Study
Inputs
16

Key model parameters and study
inputs Study population: children 1-59 months of age
10 cohorts starting in 2017 through 2027
Demographic data from UN population division,2015revision
Governmental perspective and societal
perspective
Severe rotavirus gastroenteritis (RVGE) and non-severe RVGE cases (with 7 and 3 days duration,respectively)
Disease event age distribution based on
17

Key model parameters and study inputs
(cont.)Rotarix (RV1)
2-dose schedule at 6 and 10 weeks of age
Vaccine efficacy against outcomes53% vaccine efficacy after two doses
28% vaccine efficacy after one dose
77.3% dose 1 coverage (70.5% dose 2) in year of introduction, with assumption to reach 90% coverage by end of 2020
18

Key model parameters and study inputs
(cont.) Vaccine price per dose: US$2.02 vs US$0.2 (co-
financing)
International handling: 5% of vaccine price
International delivery: 7% of vaccine price
Incremental delivery cost: US$1.06 per dose
Vaccine wastage rate: 8%
All monetary units in US$ and adjusted to 2017
3% discount rate
19
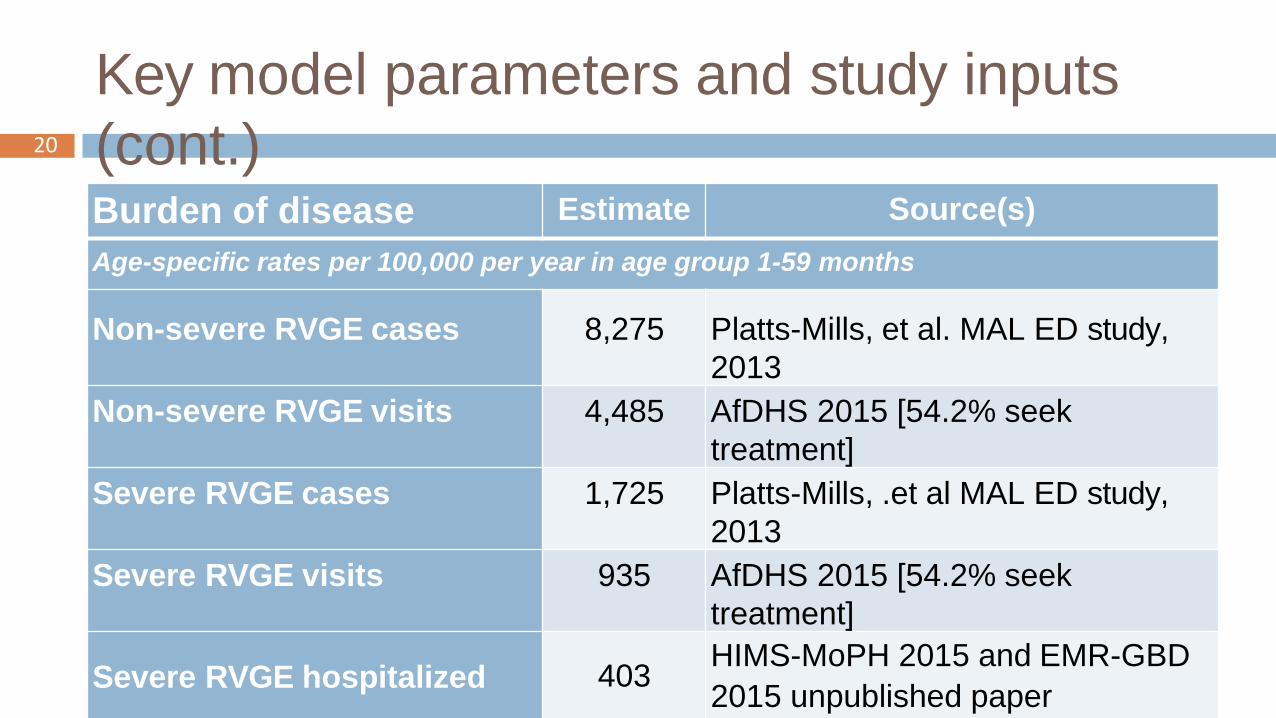
Key model parameters and study inputs
(cont.)Burden of disease Estimate Source(s)
Age-specific rates per 100,000 per year in age group 1-59 months
Non-severe RVGE cases 8,275 Platts-Mills, et al. MAL ED study,
2013
Non-severe RVGE visits 4,485 AfDHS 2015 [54.2% seek
treatment]
Severe RVGE cases 1,725 Platts-Mills, .et al MAL ED study,
2013
Severe RVGE visits 935 AfDHS 2015 [54.2% seek
treatment]
Severe RVGE hospitalized 403HIMS-MoPH 2015 and EMR-GBD
2015 unpublished paper
20

Key model parameters and study inputs
(cont.)
Healthcare costsGovernme
nt cost(estimates in
US$)
Societal
cost (government
and
households
costs,
estimates in
US$)
Sources
Non-severe cases(facility
outpatient)
1.72 3.69BPHS costing –Integrated
child illness (IMCI)
/caseSevere cases (facility
outpatient)1.72 8.80 BPHS costing – IMCI
/caseHouseholds cost from
21

Preliminary
Results
22

Potential changes in outcomes with RV
vaccine
introduction (10 cohorts)23
Benefits among vaccinated infants only, no indirect effect
considered
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
CASES VISITS HOSPITALIZATION DALYS
5,045,332
2,734,395
203,327
3,130,230
3,824,319
2,072,648
154,120
2,373,577
No Vaccine With RV1

50,000
45,000
40,000
35,000
30,000
25,000
20,000
15,000
10,000
5,000
0
49,444
37,478
Deaths
Without vaccine
With RV1
Potential changes in outcomes with RV
vaccine
introduction (10 cohorts)24

Summary of outcomes and cost averted (10
cohorts)
OutcomesOutcom
es
averted
Cost /
outcome averted
from government
perspect.
Cost /
outcome
averted from
societal
perspect.
Cases 1,22 million cases - -
Outpatient visits 661,746 visits US$1,138,204 US$34,228,547
Hospital
admissions
49,207 hospital
admissionsUS$433,020 US$784,357
DALYs 756,653 - -
Deaths 11,966 - -
25
All figures undiscounted

Rotavirus vaccination program
cost Over 10 years, the rotavirus vaccination program is estimated
to cost US$79,789,755or US$7.98 million per year on averageif considering full vaccine price
If accounting for Gavi support Afghanistan can benefit, the cost over 10 years is of US$41,879,563or US$4.2 million per year on average
cMYP total cost projection for 2017 = US$77,723,947
Rotavirus vaccination program would represent 5.4%
Total health expenditures (2014) = US$1,847,853,457
Rotavirus vaccination program would represent 0.2%
26
All figures undiscounted

From the government perspective, ICER = US$103 per DALY
averted
From the societal perspective, ICER = US$59 per DALY
averted
Incremental cost-effectiveness
ratio27
All figures discounted

Interpreting cost-effectiveness of an intervention: use of
thresholds
Former WHO guidance, updated in 2016 highlighting the need to consider
factors other than CE (affordability, feasibility, etc…) as well as developing
country specific thresholds
What economic study threshold should be used for Afghanistan?
28
1 - <3 x GDP per capita
0 - <1 x GDP per capita
>3 x GDP per capita
US$ / DALY avertedis negative
Cost-EffectiveHighly Cost-
EffectiveNot Cost-EffectiveCost Savings
US$0 US$594 US$1,782
US$103

Sensitivity
Analysis
29

Sensitivity
analysis30
We presented the results of a base case scenario calculated
from the
most realistic set of inputs
Each parameter introduces an additional range of uncertainty
in the
analysis
Uncertainty analysis allows us to evaluate different policy
scenarios and/or ranges of parameter estimates by creating
a series of ‘what if’ scenarios

Alternative
scenariosScenarios Description
Scenario 1 Base case -
Scenario 2Base case
accounting for
Gavi subsidy
Vaccine price lowered to US$0.20 per dose to reflect co-financing
amount paid by the country.
Scenario 3Higher burden
of disease
Incidence of rotavirus disease was increased by 15% for all sorts of
cases, visits, hospitalizations, and deaths. Vaccine price per dose
US$0.20.
Scenario 4Lower
coverage
rates
Accounting for lower coverage rates in the first four years of the
vaccination program to reflect 2015 DHS data. Vaccine price per
dose US$0.20.
Scenario 5
Low burden of
disease and
high vaccine
delivery costs
Accounting for a reduced burden of disease (accounting for a reduced
number of severe cases visits and number of deaths based on IHME
GBD data).
Double incremental health system cost per dose (US$2.12 instead of
initial
31

Resul
ts
Threshold used is 1 time Afghanistan GDP per capita
(US$594)
32

Conclusi
on
33

Summary of
results In Afghanistan, the introduction of RV vaccine is highly cost-effective
compared to the current situation, with incremental cost-effectiveness
ratios ranging from US$59 to US$103 per DALY averted depending
on the study perspective
Considering the support the country can receive from Gavi, the Vaccine
Alliance,
ICER ranges from US$53 to US$9
The average yearly cost of a RV vaccination program would represent
5.4% of the total immunization cost expected in 2017 and 0.2% of the
total health expenditures
A RV vaccination program has the potential to avert 1.22M RV cases;
661,746 outpatient visits; 49,207 hospitalizations; and 11,966 deaths
over 10 years
34

Discussi
onEconomic study threshold (GDP vs. country-
specific)
Study limitations mainly linked to local data
availability: vaccine efficacy, cost of illness…
Other alternative scenarios?
What other information would be important for
buy-in
and support to the program from the government?
Other questions?
35

Thank
you36