immunology lecture 5 · web viewtype i hypersensitivity reactions, is the most common type of...
TRANSCRIPT

Immunology Lecture 5
Allergy and Hypersensitivity Reaction
The same immune reactions that protect us from infection can also inflict a great deal of damage, not simply on a pathogen, but on our own cells and tissues. As it became clear that different immune mechanisms give rise to distinct hypersensitivity reactions, two immunologists, Gell and Coombs, proposed a classification scheme to discriminate among the various types of hypersensitivity (see Figure below). Type I hypersensitivity reactions are mediated by IgE antibodies, and include many of the most common allergies to respiratory allergens, such as pollen and dust mites. Type II hypersensitivity reactions result from the binding of IgG or IgM to the surface of host cells, which are then destroyed by complement- or cell-mediated mechanisms. In type III hypersensitivity reactions, antigen-antibody complexes deposited on host cells induce complement fixation and an ensuing inflammatory response. Type lV hypersensitivity reactions result from inappropriate T-cell activation.
Figure: The four types of hypersensitivity reactions.
1

Immunology Lecture 5
Type I hypersensitivity reactions
Type I hypersensitivity reactions, is the most common type of allergic reactions, including hay fever, asthma, atopic dermatitis, and food allergies.Initiated by interaction between an IgE antibody and a multivalent antigen. Healthy individuals generate IgE antibodies only in response to parasitic infections. However, some people, referred to as atopic, are predisposed to generate IgE antibodies against common environmental antigens, such as those listed in the table below. Chemical analysis revealed that most, if not all, allergens are either protein or glycoprotein in nature, with multiple antigenic sites, or epitopes, per molecule.
Common allergens associated with type I hypersensitivity
IgE antibodies alone are not destructive. Instead, they cause hypersensitivity by binding to Fc receptors specific for their constant regions (FcεRs). These are expressed by a variety of innate immune cells, (including mast cells, basophils, and eosinophils). The binding of IgE antibodies to FcεRs activates these granulocytes, inducing a signaling cascade that causes cells to release the contents of intracellular granules into the blood, a process called degranulation (see Figure below). The contents of granules vary from cell to cell, but typically include histamine, heparin, and proteases. Together with other mediators that are synthesized by activated granulocytes (leukotrienes, prostaglandins, chemokines, and cytokines), these mediators act on surrounding tissues and other immune cells, causing allergy symptoms.
2

Immunology Lecture 5
Figure: General mechanism underlying an immediate type I hypersensitivity reaction.
1-Systemic Anaphylaxis
Systemic anaphylaxis is a shocklike and often fatal state that occurs within minutes of exposure to an allergen. It is usually initiated by an allergen introduced directly into the bloodstream or absorbed from the gut or skin. Symptoms include labored respiration, a precipitous drop in blood pressure leading to anaphylactic shock, followed by contraction of smooth muscles leading to defecation, urination, and bronchiolar constriction. This leads to asphyxiation, which can lead to death within 2 to 4 minutes of exposure to the allergen. These symptoms are all due to rapid antibody-mediated degranulation of mast cells and the systemic effects of their contents. A wide range of antigens has been shown to trigger this reaction in susceptible humans, including the venom from bee, wasp, and ant stings; drugs such as penicillin, and foods such as seafood and nuts. If not treated quickly, these reactions can be fatal. Epinephrine, the drug of choice for treating systemic anaphylactic reactions, counteracts the effects of mediators such as histamine relaxing the smooth muscles of the airways and reducing vascular permeability. Epinephrine also improves cardiac output, which is necessary to prevent vascular collapse during an anaphylactic reaction.
2- Localized Hypersensitivity Reactions
In localized hypersensitivity reactions, the pathology is limited to a specific target tissue or organ, and often occurs at the epithelial surfaces first exposed to allergens. Atopic allergies include a wide range of IgE-mediated disorders,
3

Immunology Lecture 5
such as allergic rhinitis (hay fever), asthma, atopic dermatitis (eczema), and food allergies.Symptoms result from the inhalation of common airborne allergens (pollens, dust, viral antigens), which react with IgE molecules bound to sensitized mast cells in the conjunctivae and nasal mucosa. Cross-linking of IgE receptors induces the release of histamine and heparin from mast cells, which then cause vasodilation, increased capillary permeability, and production of exudates in the eyes and respiratory tract. Tearing, runny nose, sneezing, and coughing are the main symptoms.
Antibody-Mediated (type II) Hypersensitivity Reactions
Type II hypersensitivity reactions involve antibody-mediated destruction of cells by immunoglobulins of heavy chain classes other than IgE. Antibody bound to a cell-surface antigen can induce death of the antibody-bound cell by three distinct mechanisms. First, certain immunoglobulin subclasses can activate the complement system, creating pores in the membrane of a foreign cell. Secondly, antibodies can mediate cell destruction by antibody dependent cell-mediated cytotoxicity (ADCC), in which cytotoxic cells bearing Fc receptors bind to the Fc region of antibodies on target cells and promote killing of the cells. Finally, antibody bound to a foreign cell also can serve as an opsonin, enabling phagocytic cells with Fc or C3b receptors to bind and phagocytose the antibody-coated cell.
1- Transfusion Reactions
Several proteins and glycoproteins on the membrane of red blood cells are encoded by genes with several allelic forms. An individual with a particular allele of a blood-group antigen can recognize other allelic forms in transfused blood as foreign, and mount an antibody response. Blood types are referred to as A, B, or O, and the antigens that are associated with the blood types are identified as A, B, and H, respectively. (Note that the H antigen is present in all blood types).
Figure shows ABO (ABH) blood groups.
4

Immunology Lecture 5
An individual with blood type A recognizes B-like epitopes on microorganisms and produces isohemagglutinins to the B-like epitopes. This same individual does not respond to A-like epitopes on the same microorganisms because they have been tolerized to self-A epitopes. If a type A individual is transfused with blood containing type B cells, a transfusion reaction occurs in which the preexisting anti-B isohemagglutinins bind to the B blood cells and mediate their destruction by means of complement-mediated lysis. Individuals with blood type O express only the H antigen. Although they can donate blood to anyone, they have antibodies that will react to both A-type or B-type blood. Their anti-A- and anti-B-producing B cells were never exposed to A or B antigens and therefore were never deleted.
Typical symptoms include fever, chills, nausea, clotting within blood vessels, pain in the lower back, and hemoglobin in the urine. Treatment involves prompt termination of the transfusion and maintenance of urine flow with a diuretic.
2-Antibodies to other blood-group antigens such as Rh factor
3- Hemolytic Disease of the Newborn
Hemolytic disease of the newborn develops when maternal IgG antibodies specific for fetal blood-group antigens cross the placenta and destroy fetal red blood cells. The consequences of such transfer can be minor, serious, or lethal. Severe hemolytic disease of the newborn, called erythroblastosis fetalis, most commonly develops when the mother and fetus express different alleles of the Rhesus (Rh) antigen. An Rh- mother fertilized by an Rh+ father is in danger of developing a response to the Rh antigen and rejecting an Rh+
fetus.
During pregnancy, fetal red blood cells are separated from the mother’s circulation by a layer of cells in the placenta called the trophoblast. During her first pregnancy with an Rh+ fetus, an Rh- woman is usually not exposed to enough fetal red blood cells to activate her Rh-specific B cells. However, at the time of delivery, separation of the placenta from the uterine wall allows larger amounts of fetal umbilical cord blood to enter the mother’s circulation. These fetal red blood cells stimulate Rh-specific B cells to mount an immune response, resulting in the production of Rh-specific plasma cells and memory B cells in the mother. The secreted IgM antibody clears the Rh+ fetal red cells from the mother’s circulation, but memory cells remain, a threat to any subsequent pregnancy with an Rh+ fetus. Importantly, since IgM antibodies do not pass through the placenta, IgM anti-Rh antigens are no threat to the fetus. Activation of IgG-secreting memory cells in a subsequent pregnancy results
5

Immunology Lecture 5
in the formation of IgG anti-Rh antibodies, which, however, can cross the placenta and damage the fetal red blood cells. Mild to severe anemia can develop in the fetus, sometimes with fatal consequences.
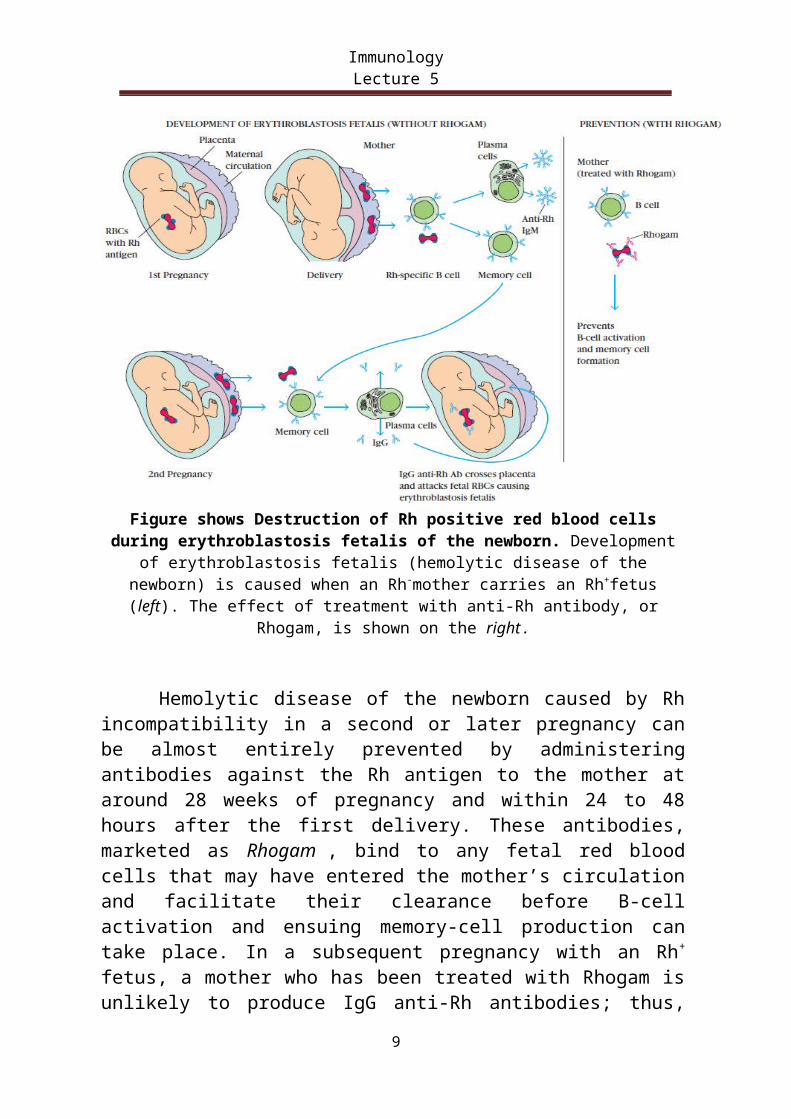
Figure shows Destruction of Rh positive red blood cells during erythroblastosis fetalis of the newborn. Development of erythroblastosis fetalis (hemolytic disease of the
newborn) is caused when an Rh-mother carries an Rh+fetus (left). The effect of treatment with anti-Rh antibody, or Rhogam, is shown on the right.
Hemolytic disease of the newborn caused by Rh incompatibility in a second or later pregnancy can be almost entirely prevented by administering antibodies against the Rh antigen to the mother at around 28 weeks of pregnancy and within 24 to 48 hours after the first delivery. These antibodies, marketed as Rhogam , bind to any fetal red blood cells that may have entered the mother’s circulation and facilitate their clearance before B-cell activation and ensuing memory-cell production can take place. In a subsequent pregnancy with an Rh+ fetus, a mother who has been treated with Rhogam is unlikely to produce IgG anti-Rh antibodies; thus, the fetus is protected from the damage that would occur when these antibodies cross the placenta.
4- Hemolytic anemia can be drug induced
6

Immunology Lecture 5
Certain antibiotics (e.g., penicillin, cephalosporins, and streptomycin), as well as other well-known drugs (including ibuprofen and naproxen), can adsorb nonspecifically to proteins on red blood cell membranes, forming a drug protein complex. In some patients, such drug-protein complexes induce formation of antibodies. These antibodies then bind to the adsorbed drug on red blood cells, inducing complement-mediated lysis and thus progressive anemia. When the drug is withdrawn, the hemolytic anemia disappears. Penicillin is notable in that it can induce all four types of hypersensitivity with various clinical manifestations
Immune Complex-Mediated (type III) Hypersensitivity
The reaction of antibody with antigen generates immune complexes. Generally, these complexes facilitate the clearance of antigen by phagocytic cells and red blood cells. In some cases, however, the presence of large numbers and networks of immune complexes can lead to tissue-damaging type III hypersensitivity reactions. The magnitude of the reaction depends on the number and size of immune complexes, their distribution within the body, and the ability of the phagocyte system to clear the complexes and thus minimize the tissue damage. The deposition of these complexes initiates a reaction that results in the recruitment of complement components and neutrophils to the site, with resultant tissue injury. Immune complexes bind to mast cells, neutrophils, and macrophages via Fc receptors, triggering the release of vasoactive mediators and inflammatory cytokines, which interact with the capillary epithelium and increase the permeability of the blood vessel walls. Immune complexes then move through the capillary walls and into the tissues where they are deposited and set up a localized inflammatory response.
Complex deposition in the tissues can give rise to symptoms such as fever, urticaria (rashes), joint pain, lymph node enlargement, and protein in the urine. The resulting inflammatory lesion is referred to as vasculitis if it occurs in a blood vessel, glomerulonephritis if it occurs in the kidney, or arthritis if it occurs in the joints.
1- Arthus Reactions Are Localized Type III Hypersensitivity Reactions
One example of a localized type III hypersensitivity reaction has been used extensively as an experimental tool. If an animal or human subject is injected intradermally with an antigen to which large amounts of circulating antibodies
7

Immunology Lecture 5
exist (or have been recently introduced by intravenous injections), antigen will diffuse into the walls of local blood vessels and large immune complexes will precipitate close to the injection site. This initiates an inflammatory reaction that peaks approximately 4 to 10 hours post injection and is known as an Arthus reaction.
2- Serum sickness is an example of a systemic form of immune complex disease, which resulted in arthritis, skin rash, and fever.
3- Systemic Lupus Erythematosus (SLE):
The antigen in the immune complex is an autoantigen, persistent antibody responses to autoantigens are an identifying feature of the disease, and complexes are deposited in the joints, kidneys, and skin of patients.Examples of diseases resulting from type III hypersensitivity reactions are found in the table below:
Autoimmune diseases Systemic lupus erythematosusRheumatoid arthritis
Multiple sclerosis
Drug reactions Allergies to penicillin and sulfonamidesInfectious diseases Poststreptococcal glomerulonephritis
MeningitisHepatitis
MononucleosisMalaria
Trypanosomiasis
Delayed-Type (Type IV) Hypersensitivity (DTH)
Type lV hypersensitivity, commonly referred to as Delayed- Type Hypersensitivity (DTH), is the only hypersensitivity category that is purely cell mediated rather than antibody mediated. The hallmarks of a type IV reaction are its initiation by T cells (as distinct from antibodies), the delay required for the reaction to develop, and the recruitment of macrophages (as opposed to neutrophils or eosinophils) as the primary cellular component of the infiltrate that surrounds the site of inflammation. The most common type IV hypersensitivity is the contact dermatitis.
8
Immunology Lecture 5
A DTH response begins with an initial sensitization by antigen, followed by a period of at least 1 to 2 weeks during which antigen-specific T cells are activated and clonally expanded (Figure below). A variety of Antigen- Presenting Cells (APCs) are involved in the induction of a DTH response, including Langerhans cells (dendritic cells found in the epidermis) and macrophages. These cells pick up antigen that enters through the skin and transport it to regional lymph nodes, where T cells are activated. In some species, including humans, the vascular endothelial cells express class II MHC molecules and can also function as APCs in the development of the DTH response. Generally, the T cells activated during the sensitization phase of a traditional DTH response are CD4+, primarily of the TH1 subtypes. However, recent studies indicate that TH2, and CD8+ cells can also play a role. A second exposure to the sensitizing antigen induces the effector phase of the DTH response (see Figure). In the effector phase, T cells are stimulated to secrete a variety of cytokines, including interferon- γ (IFN- γ ), which recruit and activate macrophages and other inflammatory cells.
Figure shows: The DTH response
9

Immunology Lecture 5
1- DTH response to Mycobacterium antigens
Immunity to the intracellular bacterium (Mycobacterium tuberculosis) involves a DTH response in which activated macrophages wall off the organism in the lung and contain it within a granuloma-type lesion called a tubercle (see Figure below). Often, however, the release of concentrated lytic enzymes from the activated macrophages within the tubercles damages the lung tissue that the immune response aims to preserve.
Figure: A prolonged DTH response can lead to formation of a granuloma
2- Contact Dermatitis
Contact dermatitis is one common manifestation of type IV hypersensitivity. The simplest form of contact dermatitis occurs when a reactive chemical compound binds to skin proteins and these modified proteins are presented to T cells in the context of the appropriate MHC antigens. The reactive chemical may be a pharmaceutical, a component of a cosmetic or a hair dye, an industrial chemical such as formaldehyde, metal ion such as nickel.
At present the best way to avoid a DTH response it to avoid the causative antigen. Once hypersensitivity has developed, topical or oral corticosteroids can be used to suppress the destructive immune response.
10