imaging of blunt abdominal trauma, part i - scbtmr.org ruedi theoni md... · blunt abdominal trauma...
TRANSCRIPT
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
IMAGING OF BLUNTABDOMINAL TRAUMA, PART I
Ruedi F. Thoeni, M. D.University of California, San Francisco
IMAGING OF BLUNTIMAGING OF BLUNTABDOMINAL TRAUMA, PART IABDOMINAL TRAUMA, PART I
Ruedi F. Thoeni, M. DRuedi F. Thoeni, M. D..University of California, San FranciscoUniversity of California, San Francisco
SCBT-MR Summer Practicum, Williamsburg, 2009SCBTSCBT--MRMR Summer Practicum, Williamsburg, 2009Summer Practicum, Williamsburg, 2009
Learning Objectives for blunt Learning Objectives for blunt abdabd. Trauma. Trauma
• General imaging considerations in abd. trauma
• Features and grading of trauma to liver
• Findings often associated with liver trauma
• Features and grading of trauma to spleen
• Features and grading of trauma to pancreas
•• General imaging considerationsGeneral imaging considerations in in abdabd. trauma. trauma
•• Features and grading ofFeatures and grading of trauma to livertrauma to liver
•• Findings often associated with liver traumaFindings often associated with liver trauma
•• Features and grading ofFeatures and grading of trauma to spleentrauma to spleen
•• Features and grading ofFeatures and grading of trauma to pancreastrauma to pancreas

ROLE OF CT IN TRAUMAROLE OF CT IN TRAUMA
• To guide management of patients
• To identify patients with internal injury
• To triage patients for emergent intervention:
• Surgery
• Interventional management (endovascular)
•• To guide management of patientsTo guide management of patients
•• To identify patients with internal injuryTo identify patients with internal injury
•• To triage patients forTo triage patients for emergent intervention:emergent intervention:
•• SurgerySurgery
•• Interventional management (endovascular)Interventional management (endovascular)
DEDICATED ABD. TRAUMA MDCTDEDICATED ABD. TRAUMA MDCT
• Contrast Materials:– Oral contrast (if possible): 3 cups of 450 ml of
2.2% Gastrografin (10 mL/450 of water)– IV contrast: 3 cc/sec for 150 ml– Rectal contrast (for penetrating trauma:
40 cc of Conray 60% in 1000 mL normal saline: use 500-1000 mL as tolerated
• Important:– Clamp bladder catheter to achieve full
distention of bladder
•• Contrast Materials:Contrast Materials:–– Oral contrast (if possible):Oral contrast (if possible): 3 cups of 450 ml of3 cups of 450 ml of
2.2% Gastrografin (10 mL/450 of water)2.2% Gastrografin (10 mL/450 of water)–– IV contrast:IV contrast: 3 cc/sec for 150 ml3 cc/sec for 150 ml–– Rectal contrastRectal contrast (for penetrating trauma:(for penetrating trauma:
40 cc of Conray 60% in 1000 mL normal saline: 40 cc of Conray 60% in 1000 mL normal saline: use 500use 500--1000 mL as tolerated1000 mL as tolerated
•• Important:Important:–– Clamp bladder catheter to achieve full Clamp bladder catheter to achieve full
distention of bladderdistention of bladder
DEDICATED ABD. TRAUMA MDCTDEDICATED ABD. TRAUMA MDCT
• 16 (64) - slice MDCT:Detector configuration: 16 (64) x 0.625 mm, reconstruction thickness and interval: 5 mm
• Scan delay:80 sec or smart prep, diaphragm to ischial tuberosity
• Important:• Single acquisition: “total body” trauma CT scan:
head, cervical spine, chest, abdomen & pelvis• Delayed scans (5 min) optional: parenchymal organs,
excretory system incl. bladder, vasc. extravasation• CT cystogram for bladder injury: 300-400 cc of
20 cc of 60% contrast/500 cc of sterile saline
•• 16 (64) 16 (64) -- slice MDCT:slice MDCT:Detector configuration: 16 (64) x 0.625 mm, Detector configuration: 16 (64) x 0.625 mm, reconstruction thickness and interval: 5 mmreconstruction thickness and interval: 5 mm
•• Scan delay:Scan delay:80 sec or smart prep80 sec or smart prep, diaphragm to ischial tuberosity, diaphragm to ischial tuberosity
•• Important:Important:•• Single acquisitionSingle acquisition: : ““total bodytotal body”” trauma CT scan: trauma CT scan:
head, cervical spine, chest, abdomen & pelvishead, cervical spine, chest, abdomen & pelvis•• Delayed scans (5 min) optionalDelayed scans (5 min) optional: parenchymal organs, : parenchymal organs,
excretory system incl. bladder, vasc. extravasationexcretory system incl. bladder, vasc. extravasation•• CT cystogram for bladder injuryCT cystogram for bladder injury: 300: 300--400 cc of 400 cc of
20 cc of 60% contrast/500 cc of sterile saline20 cc of 60% contrast/500 cc of sterile saline
IDENTIFY/CHARACTERIZE INTRAIDENTIFY/CHARACTERIZE INTRA--PERITONEAL FLUID COLLECTIONSPERITONEAL FLUID COLLECTIONS
• Water density (1-10 HU)
• Mixed density (10-20 HU): urinary bladder, bowel, gallbladder rupture
• Hemoperitoneum: CT attenuation > 30 HU
• Sentinel clot (45-70 HU): densest close to injury
• Active arterial extravasation: > 100 HU
•• Water density (1Water density (1--10 HU)10 HU)
•• Mixed density (10Mixed density (10--20 HU): urinary bladder, bowel, 20 HU): urinary bladder, bowel, gallbladder rupturegallbladder rupture
•• Hemoperitoneum: Hemoperitoneum: CT attenuation CT attenuation > 30 HU> 30 HU
•• Sentinel clot (45Sentinel clot (45--70 HU): densest close to injury70 HU): densest close to injury
•• Active arterial extravasation: > 100 HUActive arterial extravasation: > 100 HU
Always use ROI for fluid in trauma!Always use ROI for fluid in trauma!Always use ROI for fluid in trauma!

HEMOPERITONEUM VS. WATERHEMOPERITONEUM VS. WATER--DENSEDENSETRAUMATIC INTRAPERITONEAL FLUIDTRAUMATIC INTRAPERITONEAL FLUID
BB
10 HU10 HU
45 HU45 HU
85 HU85 HU
15 HU15 HU

IDENTIFY LIFEIDENTIFY LIFE--THREATENING INJURIESTHREATENING INJURIES
• Active extravasation
• Massive hemorrhage
• Major vascular injuries
• Signs of shock
• Bowel perforation
•• Active Active extravasationextravasation
•• Massive hemorrhageMassive hemorrhage
•• Major vascular injuriesMajor vascular injuries
•• Signs of shockSigns of shock
•• Bowel perforationBowel perforation
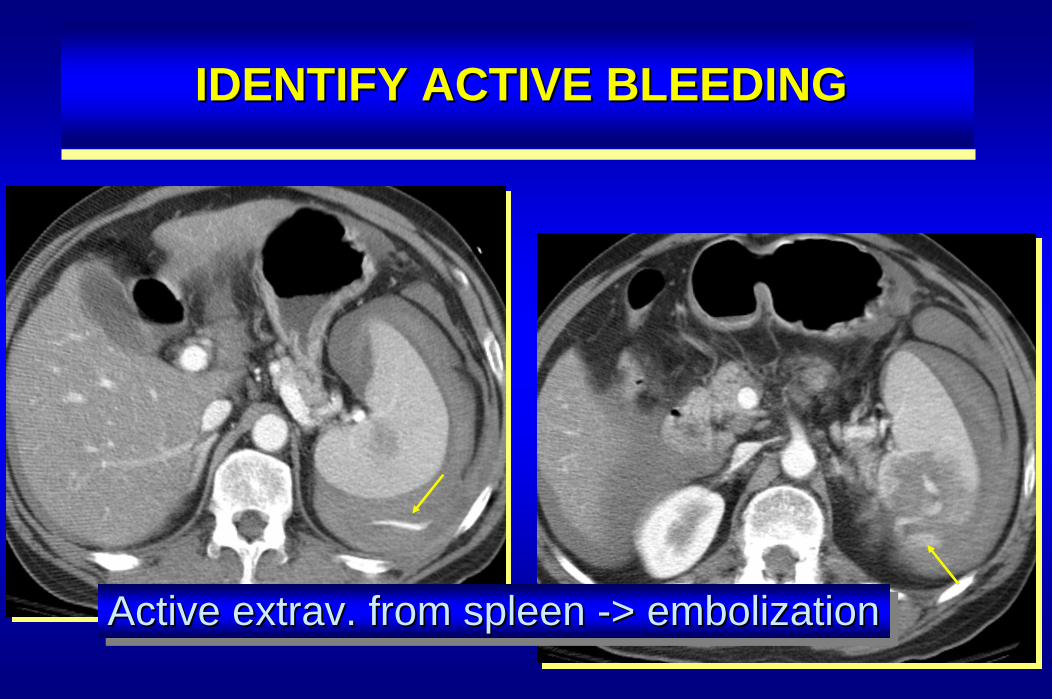
IDENTIFY ACTIVE BLEEDINGIDENTIFY ACTIVE BLEEDING
Active extrav. from spleen -> embolizationActive extrav. from spleen Active extrav. from spleen --> embolization> embolization
LIVER INJURIESLIVER INJURIES
• Prevalence:– occurs in up to 25% of patients with
blunt abdominal trauma undergoing CT
• Mortality– ~ 4 - 12% overall– 50-80% with juxtahepatic venous injury
•• Prevalence:Prevalence:–– occurs in up to 25% of patients with occurs in up to 25% of patients with
blunt abdominal trauma undergoing CTblunt abdominal trauma undergoing CT
•• MortalityMortality–– ~ 4 ~ 4 -- 12% overall12% overall–– 5050--80% with juxtahepatic venous injury80% with juxtahepatic venous injury
Matthes G, Stengel D, Seifert J, et al. Blunt liver injuries in polytrauma: results from a cohort studywith regular use of whole body helical computed tomography.World J Surg 2003; 27: 1124-1130.
LIVER TRAUMA: IDENTIFYLIVER TRAUMA: IDENTIFY
• Liver laceration• Hematoma (54 HU, 28-82)• Active hemorrhage (155 HU, 91-274)• Juxtahepatic venous injury• (Periportal low attenuation)• (Flat IVC)
•• Liver lacerationLiver laceration•• Hematoma (54 HU, 28Hematoma (54 HU, 28--82)82)•• Active hemorrhage (155 HU, 91Active hemorrhage (155 HU, 91--274)274)•• Juxtahepatic venous injuryJuxtahepatic venous injury•• (Periportal low attenuation)(Periportal low attenuation)•• (Flat IVC)(Flat IVC)
Willmann JK, Roos JE, Platz A, et al. Multidetector CT: detection of active hemorrhagein patients with blunt abdominal trauma. AJR 2002; 179: 437-444.
PARENCHYMAL INJURY TO LIVERPARENCHYMAL INJURY TO LIVER
• BLUNT TRAUMA: • Hematoma
subcapsular or intraparenchymal hematoma • Laceration
linear, stellate, “bear claw” lacerations• Bleeding
recognize arterial or venous injury with extrav.(overall art. extrav. = 18.4%; spleen = 17.7%)
• PENETRATING TRAUMA:• subcapsular hematoma & linear laceration, extrav.
•• BLUNT TRAUMA:BLUNT TRAUMA: • • HematomaHematoma
subcapsular or intraparenchymal hematoma subcapsular or intraparenchymal hematoma • • LacerationLaceration
linear, stellate, linear, stellate, ““bear clawbear claw”” lacerationslacerations
•• BleedingBleedingrecognize arterial or venous injury with recognize arterial or venous injury with extravextrav..(overall art. extrav. = 18.4%; spleen = 17.7%)(overall art. extrav. = 18.4%; spleen = 17.7%)
• • PENETRATING TRAUMA:PENETRATING TRAUMA:•• subcapsular hematoma & linear laceration, subcapsular hematoma & linear laceration, extravextrav..
GRADING HEPATIC INJURYGRADING HEPATIC INJURY
• Hematoma (subcapsular or parenchymal)– I < 1cm diameter– II 1 - 3 cm– III > 3 cm
• Laceration– I < 1 cm deep– II 1 - 3 cm– III > 3 cm
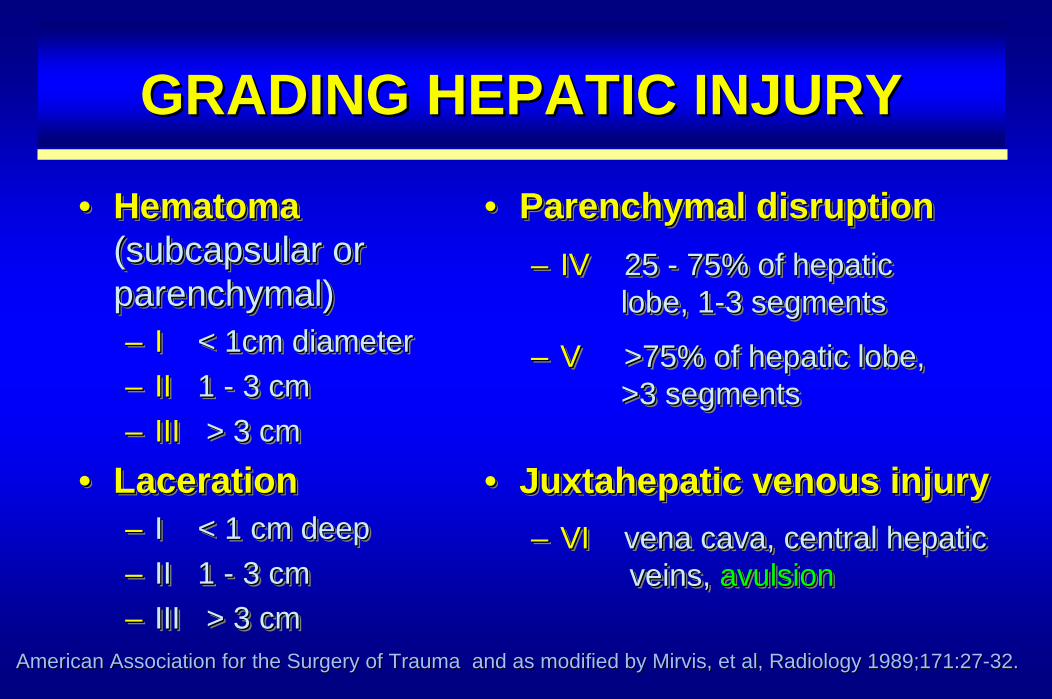
•• Hematoma Hematoma (subcapsular or (subcapsular or parenchymal)parenchymal)–– II < 1cm diameter< 1cm diameter–– IIII 1 1 -- 3 cm3 cm–– IIIIII > 3 cm> 3 cm
•• LacerationLaceration–– I < 1 cm deepI < 1 cm deep–– II 1 II 1 -- 3 cm3 cm–– III > 3 cmIII > 3 cm
American Association for the Surgery of Trauma and as modified American Association for the Surgery of Trauma and as modified by Mirvis, et al, Radiology 1989;171:27by Mirvis, et al, Radiology 1989;171:27--32.32.
• Parenchymal disruption– IV 25 - 75% of hepatic
lobe, 1-3 segments
– V >75% of hepatic lobe, >3 segments
• Juxtahepatic venous injury– VI vena cava, central hepatic
veins, avulsion
•• Parenchymal disruptionParenchymal disruption–– IV IV 25 25 -- 75% of hepatic 75% of hepatic
lobe, 1lobe, 1--3 segments3 segments
–– V V >75% of hepatic lobe, >75% of hepatic lobe, >3 segments>3 segments
•• Juxtahepatic venous injuryJuxtahepatic venous injury–– VI VI vena cava, central hepatic vena cava, central hepatic
veins, veins, avulsionavulsion
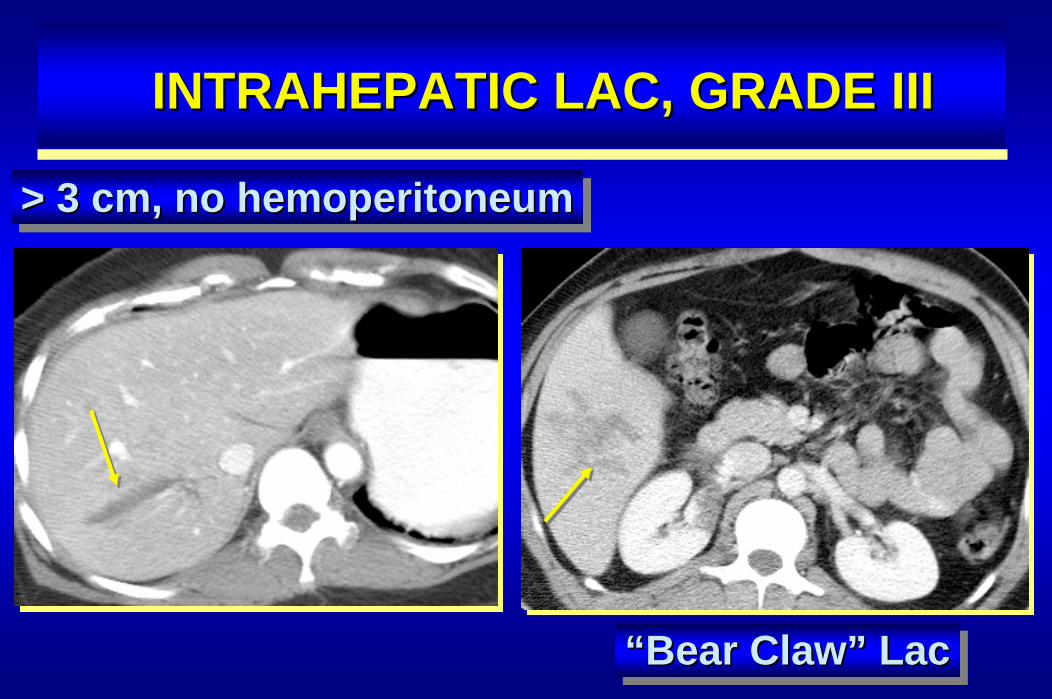
“Bear Claw” Lac““Bear ClawBear Claw”” LacLac
INTRAHEPATIC LAC, GRADE IIIINTRAHEPATIC LAC, GRADE III
> 3 cm, no hemoperitoneum> 3 cm, no hemoperitoneum> 3 cm, no hemoperitoneum
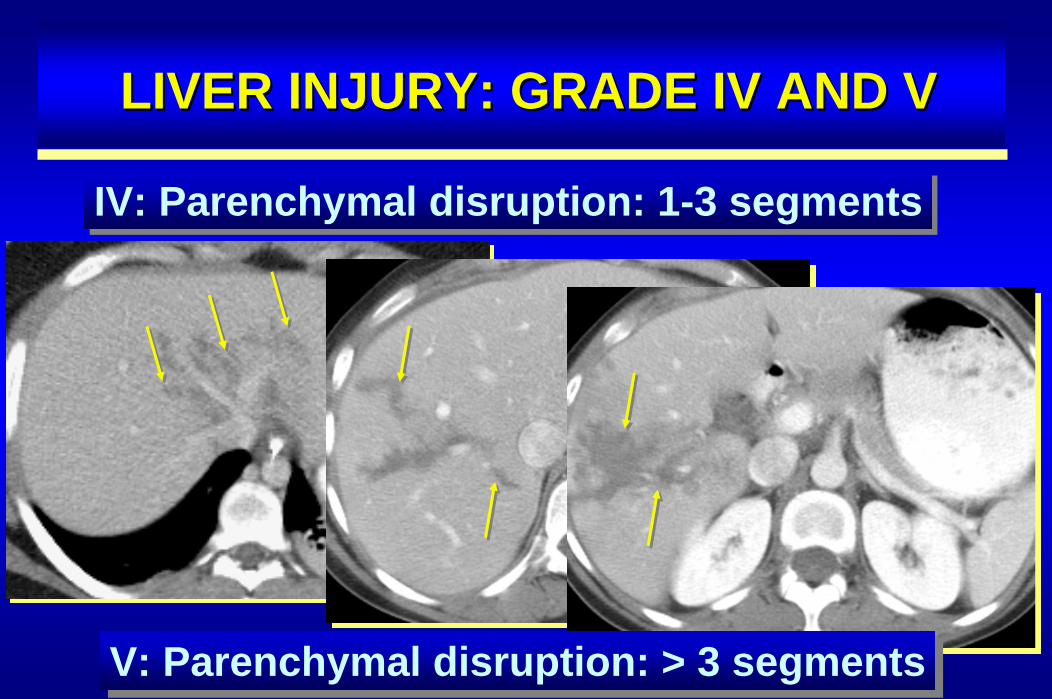
LIVER INJURY: GRADE IVLIVER INJURY: GRADE IV AND VAND V
IV: Parenchymal disruption: 1-3 segmentsIV: Parenchymal disruption: 1-3 segments
V: Parenchymal disruption: > 3 segmentsV: Parenchymal disruption: > 3 segments
BARE AREA OF THE LIVERBARE AREA OF THE LIVER
• Injury to the bare area:– right lobe injury more frequent than left– about 25% of liver injuries limited to
bare area
• Liver lacerations into the bare area: – usually results in retroperitoneal bleed:– bleeding into right anterior pararenal
space or perirenal space
•• Injury to the bare area:Injury to the bare area:–– right lobe injury more frequent than leftright lobe injury more frequent than left–– about 25% of liver injuries limited to about 25% of liver injuries limited to
bare areabare area
•• Liver lacerations into the bare area: Liver lacerations into the bare area: –– usually results in retroperitoneal bleed:usually results in retroperitoneal bleed:–– bleeding into right anterior pararenal bleeding into right anterior pararenal
space or perirenal spacespace or perirenal space
CT PREDICTOR OF FAILURE FOR NONCT PREDICTOR OF FAILURE FOR NON--OPERATIVE OPERATIVE MANAGEMENTMANAGEMENT
Pachter HL, Knudson MM, Esrig B, Ross S, Hoyt D, Cogbill T, et al. Status of nonoperative managementof blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996; 40: 31-38.
• Active bleeding on CT• Injury grade above III
– injury of main trunks of hepatic veins twice as likely to fail
– hepatic veins injured in 13% of patients with liver injury
– IVC injured (retrohepatic IVC: 50% mortality)• Overall nonoperative success rate:
– 80% in adults, 97% in children
•• Active bleeding on CTActive bleeding on CT•• Injury grade above IIIInjury grade above III
–– injury of main trunks of hepatic veins twice as injury of main trunks of hepatic veins twice as likely to faillikely to fail
–– hepatic veins injured in 13% of patients with hepatic veins injured in 13% of patients with liver injuryliver injury
–– IVC injured (retrohepatic IVC: 50% mortality)IVC injured (retrohepatic IVC: 50% mortality)•• Overall nonoperative success rate: Overall nonoperative success rate:
–– 80% in adults, 97% in children80% in adults, 97% in children
FOLLOWFOLLOW--UP CT IN BLUNTUP CT IN BLUNTLIVER TRAUMALIVER TRAUMA
* Pachter HL, Knudson MM, Esrig B, Ross S, Hoyt D, Cogbill T, et al. Status of nonoperative managementof blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996; 40: 31-38.
• Indications for CT in low grades:– abdominal pain in RUQ, jaundice, fever,
anemia or melena• Indications for CT in grades IV to VI:
– identify complications (7 to 10 days post injury*):– bile leakage (biloma, bile peritonitis; 2.8 to 7.4%)– delayed hemorrhage (1.7% to 5.9%)– abscess (0.6% to 4%)– pseudoaneurysm of hepatic artery & hemobilia (1%)
•• Indications for CT in low grades:Indications for CT in low grades:–– abdominal pain in RUQ, jaundice, fever, abdominal pain in RUQ, jaundice, fever,
anemia or melenaanemia or melena
•• Indications for CT in grades IV to VI:Indications for CT in grades IV to VI:–– identify complications (7 to 10 days post injury*):identify complications (7 to 10 days post injury*):–– bile leakagebile leakage (biloma, bile peritonitis; 2.8 to 7.4%)(biloma, bile peritonitis; 2.8 to 7.4%)–– delayed hemorrhagedelayed hemorrhage (1.7% to 5.9%)(1.7% to 5.9%)–– abscess (0.6% to 4%)abscess (0.6% to 4%)–– pseudoaneurysm of hepatic artery & hemobilia (1%)pseudoaneurysm of hepatic artery & hemobilia (1%)

BILE LEAKSBILE LEAKS
• AAST guidelines for grading liver injury does nottake into account bile leaks
• Difficult to predict who will develop a bile leak
• Bile leak asymptomatic in up to 50%
• Symptoms develop if bile infected or biloma large
• Gallbladder injury uncommon: 2-3% with blunttrauma (distended gallbladder!)
•• AAST guidelines for grading liver injury does notAAST guidelines for grading liver injury does nottake into account bile leakstake into account bile leaks
•• Difficult to predictDifficult to predict who will develop a bile leakwho will develop a bile leak
•• Bile leak asymptomatic in up to 50%Bile leak asymptomatic in up to 50%
•• Symptoms develop if bile infected or biloma largeSymptoms develop if bile infected or biloma large
•• Gallbladder injury uncommon: 2Gallbladder injury uncommon: 2--3% with blunt3% with blunttrauma (distended gallbladder!) trauma (distended gallbladder!)
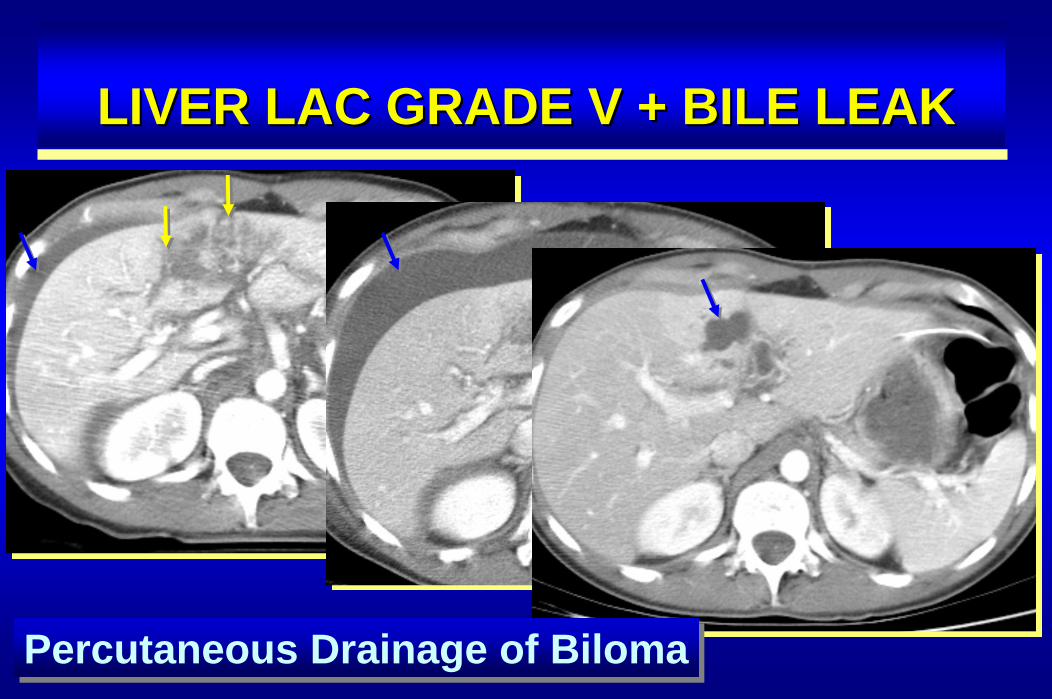
LIVER LAC GRADE V + BILE LEAKLIVER LAC GRADE V + BILE LEAK
Percutaneous Drainage of BilomaPercutaneous Drainage of Biloma

Hepatic repair progresses predictably: Resolution
– Hemoperitoneum 1 week– Laceration 3 weeks– Subcapsular hematoma 6-8 weeks– Parenchymal homogeneity 4-8 weeks– Hematoma, biloma years
Hepatic repair progresses predictably: ResolutionHepatic repair progresses predictably: Resolution
–– HemoperitoneumHemoperitoneum 1 week1 week–– LacerationLaceration 3 weeks3 weeks–– Subcapsular hematomaSubcapsular hematoma 66--8 weeks8 weeks–– Parenchymal homogeneityParenchymal homogeneity 44--8 weeks8 weeks–– Hematoma, bilomaHematoma, biloma yearsyears
FOLLOWFOLLOW--UP CT FINDINGS IN BLUNTUP CT FINDINGS IN BLUNTLIVER TRAUMALIVER TRAUMA
Karp MP, Cooney DR, Pros GA, et al. The nonoperative managementof pediatric hepatic trauma. J Pediatr Surg 1983; 18: 512- 518.
SPLENIC INJURIESSPLENIC INJURIES
• Splenic injury– most commonly injured organ
following blunt abdominal trauma
• Incidence of splenic injury– splenic injury accounts for 40-50% of
patients with abdominal organ injury
•• Splenic injurySplenic injury–– most commonly injured organmost commonly injured organ
following blunt abdominal traumafollowing blunt abdominal trauma
•• Incidence of splenic injuryIncidence of splenic injury–– splenic injury accounts for 40splenic injury accounts for 40--50% of50% of
patients with abdominal organ injurypatients with abdominal organ injury
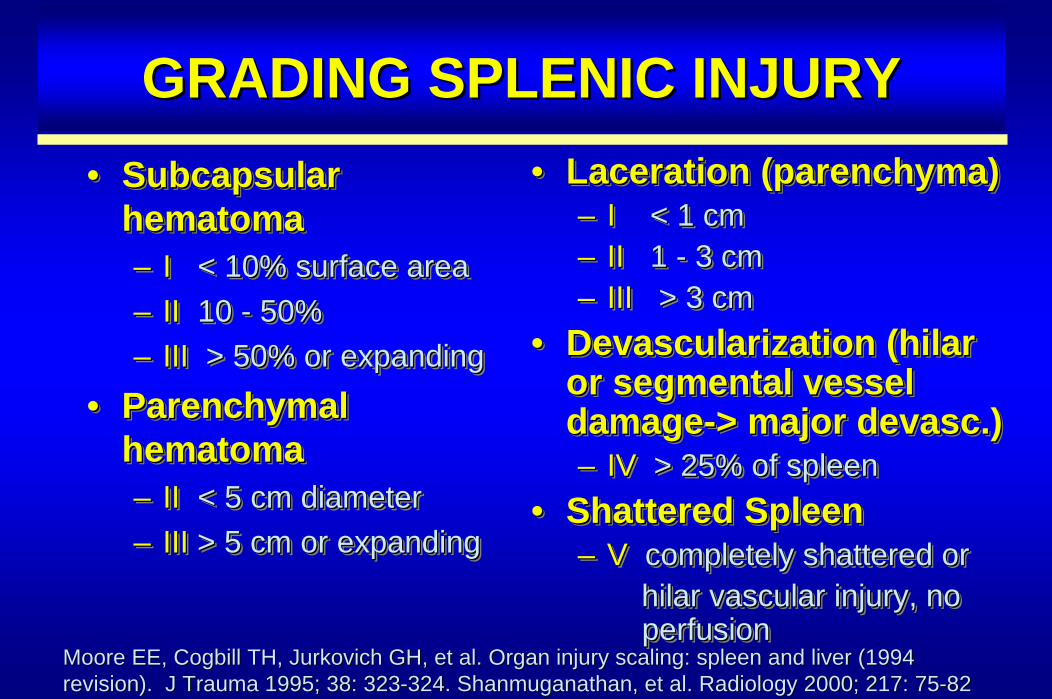
GRADING SPLENIC INJURYGRADING SPLENIC INJURY
Moore EE, Cogbill TH, Jurkovich GH, et al. Organ injury scaling:Moore EE, Cogbill TH, Jurkovich GH, et al. Organ injury scaling: spleen and liver (1994 spleen and liver (1994 revision). J Trauma 1995; 38: 323revision). J Trauma 1995; 38: 323--324. 324. ShanmuganathanShanmuganathan, et al. Radiology 2000; 217: 75, et al. Radiology 2000; 217: 75--8282
• Subcapsular hematoma– I < 10% surface area– II 10 - 50%– III > 50% or expanding
• Parenchymal hematoma– II < 5 cm diameter– III > 5 cm or expanding
•• Subcapsular Subcapsular hematomahematoma–– II < 10% surface area< 10% surface area–– IIII 10 10 -- 50%50%–– III III > 50% or expanding> 50% or expanding
•• Parenchymal Parenchymal hematomahematoma–– IIII < 5 cm diameter< 5 cm diameter–– III III > 5 cm or expanding> 5 cm or expanding
• Laceration (parenchyma)– I < 1 cm– II 1 - 3 cm– III > 3 cm
• Devascularization (hilar or segmental vessel damage-> major devasc.)– IV > 25% of spleen
• Shattered Spleen– V completely shattered or
hilar vascular injury, noperfusion
•• Laceration (parenchyma)Laceration (parenchyma)–– I I < 1 cm< 1 cm–– II II 1 1 -- 3 cm3 cm–– III III > 3 cm> 3 cm
•• Devascularization (Devascularization (hilar hilar or segmental vessel or segmental vessel damagedamage--> major > major devascdevasc.).)–– IV IV > 25%> 25% of spleenof spleen
•• Shattered SpleenShattered Spleen–– V V completely shattered orcompletely shattered or
hilar hilar vascular injury, novascular injury, noperfusionperfusion
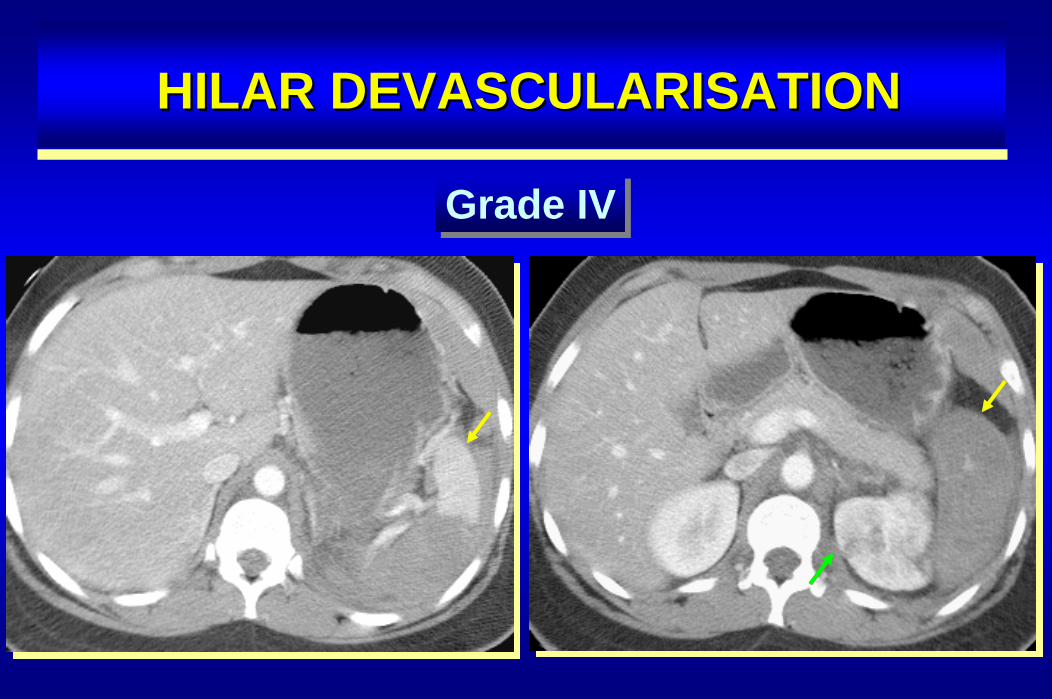
HILAR DEVASCULARISATIONHILAR DEVASCULARISATION
Grade IVGrade IV
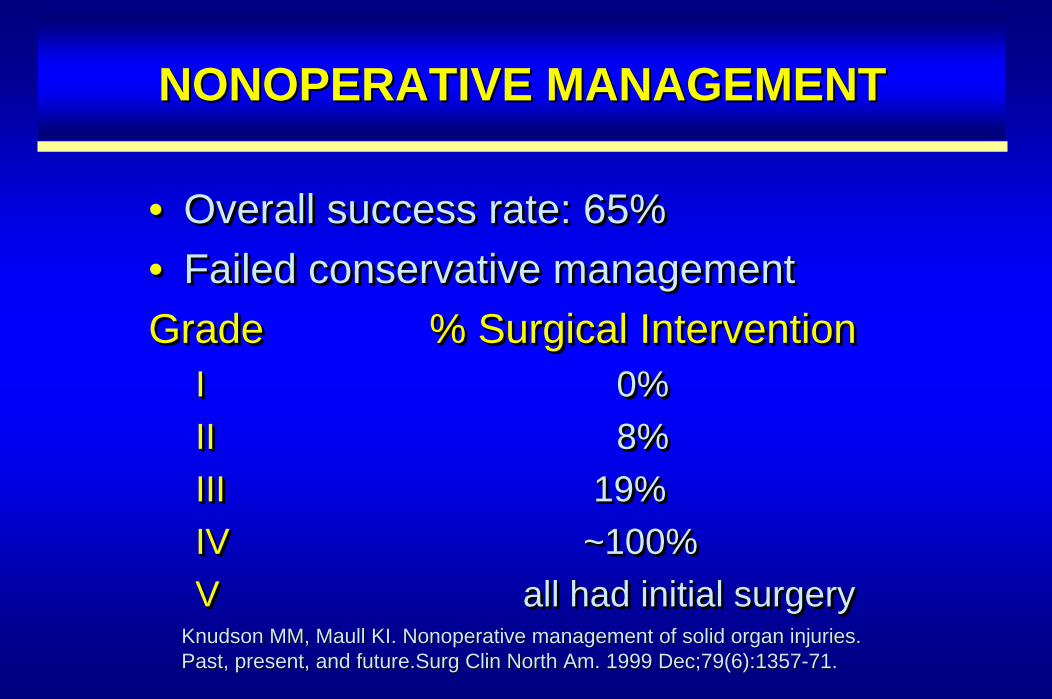
NONOPERATIVE MANAGEMENTNONOPERATIVE MANAGEMENT
Knudson MM, Maull KI. Nonoperative management of solid organ injKnudson MM, Maull KI. Nonoperative management of solid organ injuries.uries.Past, present, and future.Past, present, and future.Surg Clin North Am. 1999 Dec;79(6):1357Surg Clin North Am. 1999 Dec;79(6):1357--71.71.
• Overall success rate: 65%• Failed conservative managementGrade % Surgical Intervention
I 0%II 8%III 19%IV ~100%V all had initial surgery
•• Overall success rate: 65%Overall success rate: 65%•• Failed conservative managementFailed conservative managementGradeGrade % Surgical Intervention% Surgical Intervention
II 0%0%IIII 8%8%IIIIII 19%19%IV IV ~~100%100%VV all had initial surgeryall had initial surgery
SPLENIC INJURIES: COMPLICATIONSPLENIC INJURIES: COMPLICATION
• Active hemorrhage– hyperattenuating area on portal venous
phase with persistent hyperattenuation or increase in size on 5 minute delay
• Pseudoaneurysm– hyperattenuating area on portal venous
phase with wash-out on 5 minute delay (acts like other vessels)
•• Active hemorrhageActive hemorrhage–– hyperattenuating area on portal venoushyperattenuating area on portal venous
phase with persistent hyperattenuation phase with persistent hyperattenuation or increase in size on 5 minute delayor increase in size on 5 minute delay
•• PseudoaneurysmPseudoaneurysm–– hyperattenuating area on portal venoushyperattenuating area on portal venous
phase with washphase with wash--out on 5 minute delay out on 5 minute delay (acts like other vessels)(acts like other vessels)
Anderson SW, Varghese JC, Lucey BC, et al. Blunt Splenic Trauma:Anderson SW, Varghese JC, Lucey BC, et al. Blunt Splenic Trauma: DelayedDelayed--Phase CT for DifferentiationPhase CT for Differentiationof Active Hemorrhage from Contained Vascular Injury in Patients.of Active Hemorrhage from Contained Vascular Injury in Patients. Radiology. 2007; 243:88Radiology. 2007; 243:88--95.95.
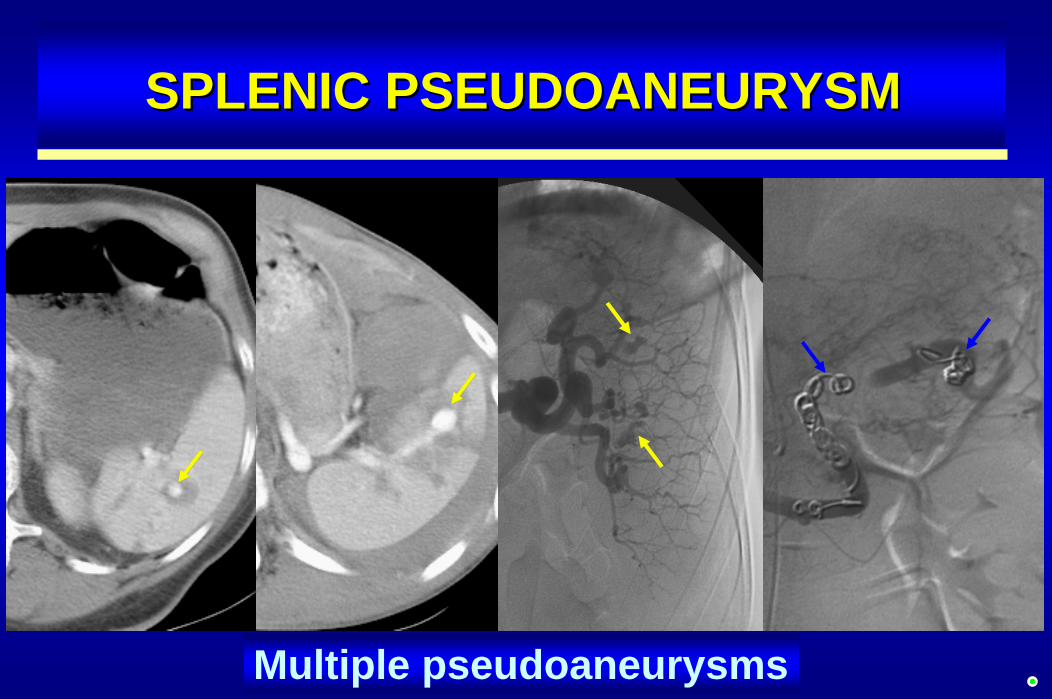
Multiple pseudoaneurysms
SPLENIC PSEUDOANEURYSMSPLENIC PSEUDOANEURYSM
PANCREATIC INJURIESPANCREATIC INJURIES
• Incidence: in 1% - 3% of blunt abd. trauma• Greatest mortality when delay in Dx• 70% of adults (15-30% children) have
associated injuries• Amylase
– initially is neither sensitive nor specific– 1-2 days later will be elevated in 80-90%
• Initial CT sensitivity 68-80%
•• Incidence: in 1% Incidence: in 1% -- 3% of blunt abd. trauma3% of blunt abd. trauma•• Greatest mortality when delay in DxGreatest mortality when delay in Dx•• 70% of adults (1570% of adults (15--30% children) have 30% children) have
associated injuriesassociated injuries•• AmylaseAmylase
–– initially is neither sensitive nor specificinitially is neither sensitive nor specific–– 11--2 days later will be elevated in 802 days later will be elevated in 80--90%90%
•• Initial CT sensitivityInitial CT sensitivity 6868--80%80%
PANCREATIC INJURIESPANCREATIC INJURIES
• More common under 40 years of age• Mechanism: compression against spine• Association with liver and duodenal injuries• CT findings: initially may be normal• Early recognition of duct disruption important
because of possible delayed complications:– Fistula, pseudocyst, abscess
•• More common under 40 years of ageMore common under 40 years of age•• Mechanism: compression against spineMechanism: compression against spine•• Association with liver and duodenal injuriesAssociation with liver and duodenal injuries•• CT findings: CT findings: initially may be normalinitially may be normal•• Early recognition of duct disruption Early recognition of duct disruption important important
because of possible delayed complications:because of possible delayed complications:–– Fistula, pseudocyst, abscessFistula, pseudocyst, abscess
PANCREATIC ORGAN INJURY AAST PANCREATIC ORGAN INJURY AAST SCALESCALE
• Grade I (A*)– minor contusion,
superficial lac, duct intact
• Grade II (A)– major contusion,
major lac, duct intact
•• Grade I Grade I (A*)(A*)–– minor contusion, minor contusion,
superficial lac, duct superficial lac, duct intactintact
•• Grade II Grade II (A)(A)–– major contusion, major contusion,
major lac, duct major lac, duct intactintact
• Grade III (B)– duct injury, distal
transsection• Grade IV (C)
– proximal transsection, ampulla injury
• Grade V (C)– massive disruption of
pancreatic head
•• Grade III Grade III (B)(B)–– duct injury, distal duct injury, distal
transsectiontranssection•• Grade IV Grade IV (C)(C)
–– proximal transsection, proximal transsection, ampulla injuryampulla injury
•• Grade V Grade V (C)(C)–– massive disruption of massive disruption of
pancreatic headpancreatic head* Moore classification: Wong YC, Wang LJ, Lin BC, et al. CT grad* Moore classification: Wong YC, Wang LJ, Lin BC, et al. CT grading of blunt ing of blunt pancreatic injuries:pancreatic injuries:prediction of ductal disruption and surgical correlation. J Compprediction of ductal disruption and surgical correlation. J Comput Assist Tomogr 1997; 21: 246ut Assist Tomogr 1997; 21: 246--250.250.

PANCREATIC INJURIESPANCREATIC INJURIES
Patel et al, Br J Radiol 1998;71:985Patel et al, Br J Radiol 1998;71:985--990990
Grade I & II: minor/major contusion or laceration Grade I & II: minor/major contusion or laceration
Grade III: distal ductdisruptionGrade III: distal ductdisruption
Grade IV: Proximal trans-section, ampullary injuryGrade IV: Proximal trans-section, ampullary injury
Grade V: Pancreas head,duodenal crush injuryGrade V: Pancreas head,duodenal crush injury
CT FINDINGS OF PANCREATIC INJURYCT FINDINGS OF PANCREATIC INJURY
• Focal or diffuse enlargement/edema– focal area of low attenuation = contusion– look for asymmetry of the pancreatic septations– heterogeneous enhancement
• Hemorrhage/fluid in anterior pararenal space– between pancreas and splenic vein– around SMA
• Duct injury (occurs in about 15% of patients)– CT sensitivity low: ERCP or MRCP better; MDCT?– implied disruption if laceration is > 50% pancreas thickness
•• Focal or diffuse enlargement/edemaFocal or diffuse enlargement/edema–– focal area of low attenuation = contusionfocal area of low attenuation = contusion–– look for asymmetry of the pancreatic septationslook for asymmetry of the pancreatic septations–– heterogeneous enhancementheterogeneous enhancement
•• Hemorrhage/fluid in anterior pararenal spaceHemorrhage/fluid in anterior pararenal space–– between pancreas and splenic veinbetween pancreas and splenic vein–– around SMAaround SMA
•• Duct injuryDuct injury (occurs in about 15% of patients)(occurs in about 15% of patients)–– CT sensitivity low: ERCP or MRCP better; MDCT?CT sensitivity low: ERCP or MRCP better; MDCT?–– implied disruption if laceration is > 50% pancreas thicknessimplied disruption if laceration is > 50% pancreas thickness
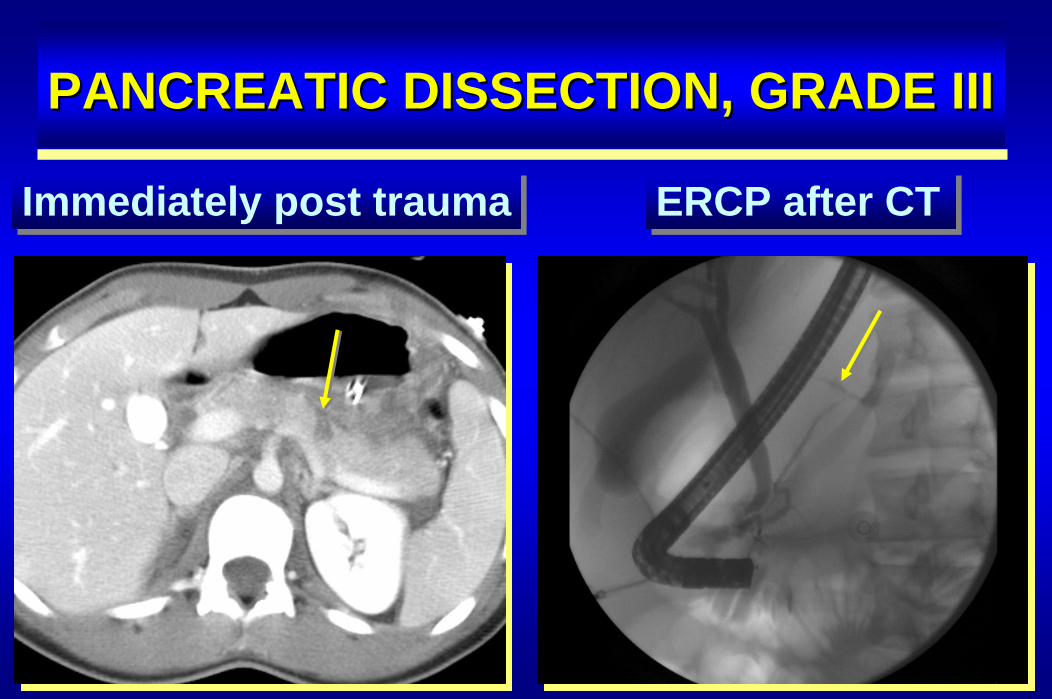
PANCREATIC DISSECTION, GRADE IIIPANCREATIC DISSECTION, GRADE III
Immediately post traumaImmediately post trauma ERCP after CTERCP after CT
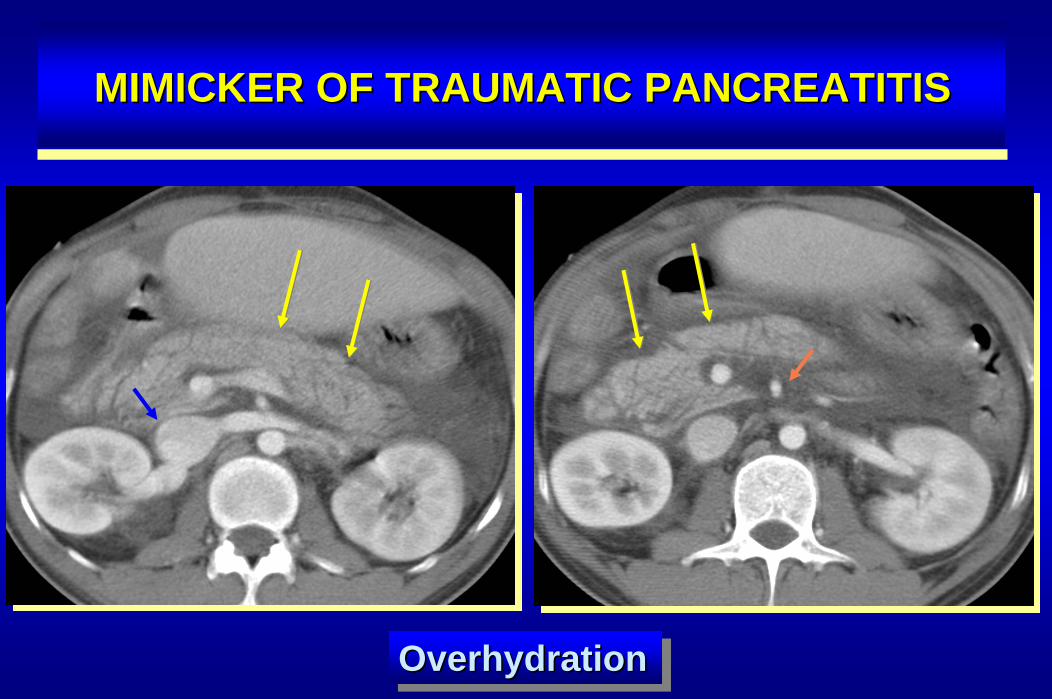
MIMICKER OF TRAUMATIC PANCREATITISMIMICKER OF TRAUMATIC PANCREATITIS
OverhydrationOverhydrationOverhydration
MDCT OF PANCREATIC INJURYMDCT OF PANCREATIC INJURY
• 9/95 (9.5%) patients with blunt abdominal trauma
• Six with MP duct injury, 3 without• Detection of duct injury was
– 97.7% in pancreatic phase– 100% in portal venous phase– 96.8% in equilibrium phase
• High interobserver agreement
•• 9/95 (9.5%) patients with blunt abdominal 9/95 (9.5%) patients with blunt abdominal traumatrauma
•• Six with MP duct injury, 3 withoutSix with MP duct injury, 3 without•• Detection of duct injuryDetection of duct injury waswas
–– 97.7% in pancreatic phase97.7% in pancreatic phase–– 100% in 100% in portal venous phaseportal venous phase–– 96.8% in equilibrium phase96.8% in equilibrium phase
•• High interobserver agreementHigh interobserver agreementWong YC, Wang LJ, Fang JF, et al. MDCT of blunt pancreatic injurWong YC, Wang LJ, Fang JF, et al. MDCT of blunt pancreatic injuries: can contrasties: can contrast--enhanced enhanced multiphasic multiphasic CT detect pancreatic duct injuries? J Trauma 2008; 64: 666CT detect pancreatic duct injuries? J Trauma 2008; 64: 666--672.672.
TAKE HOME MESSAGE FOR INTRATAKE HOME MESSAGE FOR INTRA--AND RETROPERITONEAL INJURYAND RETROPERITONEAL INJURY
• Dedicated trauma protocol
• Timing of iv contrast material critical (smart prep)
• Identify/characterize intraperitoneal fluid collections
• Identify active bleeding
• Identify abdominal parenchymal injuries
• Grade parenchymal injuries for management
• Obtain delayed scans in selected instances
•• Dedicated trauma protocolDedicated trauma protocol
•• Timing of iv contrast material critical (smart prep)Timing of iv contrast material critical (smart prep)
•• Identify/characterize intraperitoneal fluid collectionsIdentify/characterize intraperitoneal fluid collections
•• Identify active bleedingIdentify active bleeding
•• Identify abdominal parenchymal injuriesIdentify abdominal parenchymal injuries
•• Grade parenchymal injuries for managementGrade parenchymal injuries for management
•• Obtain delayed scans in selected instances Obtain delayed scans in selected instances