imaging indexes of activity and severity for crohn’s disease: current status and future trends
TRANSCRIPT

Imaging indexes of activity and severityfor Crohn’s disease: current status and futuretrends
Jordi Rimola,1 Ingrid Ordas,2 Sonia Rodrıguez,1 Elena Ricart,2 Julian Panes2
1Department of Radiology, Centro de Investigaciones Biomedicas en Red, enfermedades hepaticas y digestivas (CIBER-ehd),
IDIBAPS, Hospital Clınic of Barcelona, Villarroel 170, 08036 Barcelona, Spain2Department of Gastroenterology, Centro de Investigaciones Biomedicas en Red, enfermedades hepaticas y digestivas
(CIBER-ehd), IDIBAPS, Hospital Clınic of Barcelona, Barcelona, Spain
Abstract
Background: Cross-sectional imaging techniques, includ-ing ultrasonography (US), computed tomography (CT),and magnetic resonance imaging (MRI) are increasinglyused for evaluation of Crohn’s disease (CD).Aim: To review the accuracy of cross-sectional imagingindexes for measurement of disease activity and severityin patients with CD, and to evaluate its applicability ondaily clinical practice and research.Methods: Relevant publications were identified by liter-ature search, and selected based on predefined qualityparameters, including a sample size and reference stan-dard. Nineteen publications were chosen.Results: The US-based indexes of activity showed highcorrelation with reference standard indexes. There is agood or very good agreement between the MR-basedindexes and the reference standard when the comparisonis limited to small segments of intestine. Significantdiscrepancies have been found between indexes thatevaluate the colon. Only one CT-based index wasincluded. The main strengths and weaknesses of theindexes, according to its design, are discussed.Conclusion: Standardization of image acquisition proto-cols and patient preparation should be procured,especially for MRI. In daily practice, a simple, semi-quantitative index providing relevant information ondisease activity and severity is preferable. For researchpurposes, a precise and reproducible index should bemandatory.
Key words: Crohn’s disease—Disease activity—Diseaseseverity—Magnetic resonance—Ultrasonography—Computed tomography
Control of symptoms has for many years been the maindriver for clinical decisions and drug development inCrohn’s disease (CD). Treatment intensification by doseincrements or introduction of a different drug class hasbeen based on the presence of symptoms, such as diar-rhea, abdominal pain, impairment of general well-being,or presence of extraintestinal manifestations associ-ated with inflammatory activity. Furthermore, healthauthorities established the Crohn’s Disease Activity In-dex (CDAI) as the gold standard for the evaluation ofdrug efficacy, which is based on the assessment of signsand symptoms together with the measurement ofhematocrit [1].
A growing body of evidence indicates that this hasprobably been an imperfect approach both for clinicaldecision-making and for drug development programs. Ithas become apparent that clinical symptoms, even ifmoderate to severe (CDAI > 220) are not specific forthe presence of inflammatory lesions. In two trials, 18%
of patients with moderate-to-severe clinical symptomsdid not have significant lesions at the endoscopicassessment [2, 3], this fact having important implicationsfor the evaluation of drug efficacy. On the other hand, ithas been shown that patients with CD under sustainedclinical remission may still suffer from ulcerative lesions[4], which have been linked to increased surgicalrequirements [5, 6].
Overall, these observations led us to recommend toclinicians that treatment adjustments (both intensifica-tion and de-intensification) should be based also on
Correspondence to: Jordi Rimola; email: [email protected]
ª Springer Science+Business Media, LLC 2011
Published online: 10 November 2011AbdominalImaging
Abdom Imaging (2012) 37:958–966
DOI: 10.1007/s00261-011-9820-z

objective measures of disease activity, and not only onsymptoms. In the research arena, a number of recenttrials have set the primary endpoint to mucosal healinginstead of symptom control.
Endoscopy continues to be the gold standard for le-sion assessment in CD, but has inherent limitations.Patients with CD and symptoms of active disease maynot accept to undergo the examination. Bowel cleansingneeds to be intense and is cumbersome, and importantly,intubation of the distal ileum can only be completed in80% of the patients for reasons related to disease activityand/or technical aspects [7]. Recent evidence indicatesthat cross-sectional imaging techniques have a highaccuracy for the assessment of mucosal lesions and arereliable alternatives to ileocolonoscopy, offering evensome advantages, including the assessment of extramuralcomplications, such as the presence of fistulas and ab-scesses, or determining the functional repercussion of astenotic lesion [8].
We undertook this systematic review to inform on theavailability, construction, and performance of cross-sec-tional imaging-based indexes to determine the presenceof disease activity and severity in CD, and to providepractical recommendations on the best use of these in-dexes in clinical practice and research.
Search strategy and study selection
A comprehensive literature search was undertaken toidentify all relevant citations. The electronic searchstrategy involved keyword searches of MEDLINE andEMBASE. The electronic search was supplemented bymanually reviewing the reference lists of the includedstudies as well as relevant review articles. Literaturesearch comprised the period of the preceding 15 yearsand the following search criteria were used (all fields):(‘‘Crohn Disease’’ OR ‘‘Crohn’s’’ OR ‘‘inflammatorybowel disease’’) AND (‘‘ultrasound’’ OR ‘‘ultrasonog-raphy’’ OR ‘‘sonography’’ OR ‘‘computed tomography’’OR ‘‘CT scan’’, OR ‘‘Helical CT’’, OR ‘‘CT enterogra-phy’’ OR ‘‘magnetic resonance’’ OR ‘‘magnetic reso-nance imaging’’ OR ‘‘MRI’’ OR ‘‘MR’’). Referencesfrom the articles selected were also examined in search ofadditional studies meeting the inclusion criteria.
The final selection of the articles was performedaccording to the following criteria: (1) 10 or more pa-tients were included; (2) ultrasonography (US) and/orcomputed tomography (CT) and/or magnetic resonanceimaging (MRI) were used for assessment of diseaseactivity; (3) Adequate reference standard, includingileocolonoscopy, capsule endoscopy, enteroscopy, orsurgical or pathological findings for evaluation of smalland large bowel; (4) Data reported to allow calculationof correlation values; (5) The indexes should combine atleast two radiological parameters to be included in thisrevision. Following those criteria, 19 indexes fulfilling all
inclusion criteria were finally included in the analysis: 14MRI-based activity indexes [9–22], four US-basedactivity indexes [14, 23–25], and only one CT-basedactivity index [26]. A summary of selected indexes of CDactivity is provided in Table 1.
Assessment of small bowel and colon
Nine out of the 19 identified indexes evaluated the ter-minal ileum and the colon taking as reference standardileocolonoscopy [9, 10, 13–17, 20, 25]. Four scores wereonly focused on activity of the terminal ileum, threeusing ileoscopy as reference standard [12, 21, 23], andone correlating an MRI index with histology [11]. Twoindexes were constructed to evaluate the entire smallbowel distal to the duodenum, one of them using smallbowel capsule endoscopy (SBCE) as reference standard[19], and another using double balloon enteroscopy asreference standard [18]. Three indexes of activity evalu-ated small and large bowel segments, an US index ofactivity was compared with the combined findings ofileocolonoscopy and barium studies [24], a CT indexof activity was correlated with a pathological index ofactivity [26], and another CT index of activity was cor-related with findings at ileocolonoscopy and doubleballoon enteroscopy [22]. Finally, an MRI-based activityindex focused on ileocolonic anastomosis using ileocol-onoscopy as reference standard [15].
Imaging findings related to activityand severity
The imaging parameters that were selected in each MRI-based index, and the number of studies including eachparticular parameter is summarized in Table 2 andFig. 1, respectively. All the MRI-based indexes ofactivity and severity included wall thickness (in mm) andthe degree of wall enhancement after intravenous con-trast injection. The latter parameter was evaluatedqualitatively by the radiologist in the majority of thestudies, and only a minority determined relative contrastenhancement quantitatively based on measures of basaland post-contrast wall intensity [9, 11, 27]. The cutoffpoint for considering the wall thickness pathologicalranges between 3 and 4 mm depending on the studies. Inanalogy with endoscopic or histological indexes ofactivity where superficial and deep ulcerations are mea-sured as a criterion of severity, nine MRI-based indexes[9–11, 13, 15, 18–20, 22] also included mucosal lesionsranging from subtle mucosal irregularities to deepulcerations as a parameter of severity. The presence ofluminal stenosis was also selected as a criterion foractivity in 9 out of 14 MRI-based indexes [10, 11, 15, 16,18–22], and in most cases, its identification was a crite-rion for severe activity. Other MRI parameters that arecommonly included as part of an index for severity havebeen the target sign which is related to the presence of
J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease 959

Table
1.Accuracy
ofMRI,CT,andUSin
theassessm
entofdisease
severityin
CD
Author
Technique
Patients
(segments)
included
Locationevaluated
Reference
standard
Per
patient
based
Per
segment
based
Results
Chioreanet
al.[26]
MDCT
44(47)
Smallbowel
colon
Pathologicalfindings
No
Yes
Activityr=
0.7
Fibrostenosisr=
0.6
Drewset
al.[23]
US
32(32)
Terminalileum
Ileo-colonoscopy
Yes
Yes
Concordance
k=
0.66
Florieet
al.[10]
MRI
31(142)
Terminalileum
colon
Ileo-colonoscopy
No
Yes
CorrelationbetweenMRIandendoscopic
severity:
0.59(observer
1)–0.53(observer
2)(P
<0.001)
Futagamiet
al.[24]
US
55
Smallbowel
colon
Barium
Endoscopy
Yes
No
Correlationbetweenultrasonographic
activityindex
andendoscopic
orbarium
contrast
studiesr=
0.62
Giromettiet
al.[11]
MRI
52(52)
Terminalileum
Histology
Yes
Yes
S93%;E=
87.55detectionactivity
Horsthuiset
al.[21]
MRI
15
Terminalileum
colon
Ileo-colonoscopy
Yes
No
Sensitivity60.9–91.3
%;Specificity60–90%CD
activity
wasunderstaged
in33%
(obs1),76
%(obs2),80%
(obs3)
Hyunet
al.[22]
MRI
30
Smallbowel
andcolon
Ileocolonoscopy,
double
balloon
enteroscopy
No
Yes
CorrelationbetweenMRIindex
andendoscopicseverity
index
r=
0.85(P
<0.001)
Laghiet
al.[12]
MRI
26(26)
TerminalIleum
Ileo-colonoscopy
Histology
Yes
No
MRIcorrelatedmarkedly
withendoscopy(r
=0.94)
andhistology(r
=0.95)
Neyeet
al.[25]
US
22(126)
Terminalileum
colon
Ileo-colonoscopy
No
Yes
Concordance
K=
0.75–0.91
Oussalahet
al.[13]
MRI
61(211)
Terminalileum
colon
Ileo-colonoscopy
No
Yes
CorrelationbetweenMRIindex
andendoscopicseverity
index
r=
0.659(P
<0.001)
Pascuet
al.[14]
MRI
37
Terminalileum
colon
Ileo-colonoscopy
No
Yes
CorrelationsbetweenMRIandendoscopic
activity
index
r=
0.34
Pascuet
al.[14]
US
37
Terminalileum
colon
Ileo-colonoscopy
No
Yes
CorrelationsbetweenUSandendoscopic
activityindex
r=
0.83
Rim
ola
etal.[9]
MRI
50(213)
Terminalileum
colon
Ileo-colonoscopy
No
Yes
Distinctionbetweenmild-m
oderate
andseveresensitiv-
ity91%,specificity95
%Rim
ola
etal.[27]
MRI
48(258)
Terminalileum
colon
Ileo-colonoscopy
No
Yes
CorrelationbetweenMRIindex
andendoscopicseverity
index
r=
0.84(P
<0.001)
Sailer
etal.[15]
MRI
30(30)
Ileo-colonic
anastomosis
Ileo-colonoscopy
Yes
Yes
Correlationwithendoscopic
severityr=
0.67
(P<
0.01)
Schreyer
etal.[17]
MRI
12(84)
Terminalileum
colon
Ileo-colonoscopy
No
Yes
Severityagreem
entbetweentechniques
in55/84
segments
Schreyer
etal.[16]
MRI
30
Terminalileum
colon
Ileo-colonoscopy
No
Yes
Distinctionbetweenmild-m
oderate
andsevere
S=
69%,E=
99%
Seiderer
etal.[18]
MRI
10(28)
Smallbowel
Double-balloon
enteroscopy
No
Yes
Severityagreem
entbetweentechniques
in21/28
segments
Tillack
etal.[19]
MRI
19(52)
Smallbowel
Capsule
endoscopy
No
Yes
Distinctionbetweenmildmoderate
andsevere:
sensitivity58
%,specificity77%
VanGem
ert-Horsthuis
etal.[20]
MRI
20
Terminalileum
colon
Ileo-colonoscopy
No
Yes
Lack
ofcorrelationbetweenMRIseverityand
endoscopic
severity:r=
0.4
(P=
0.09)
960 J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease

edema, the comb sign which corresponds to the presenceof perienteric hypervascularization, or the presence ofenlarged regional lymph nodes. Each of these threeparameters has been evaluated in 8 of the 13 selectedstudies. Other pathological changes such as a hypersignalon diffusion sequence imaging, a subjective evaluation ofreduction in bowel motility, the presence of penetratinglesions or the presence of fibroffaty proliferation wereevaluated in a minority of studies.
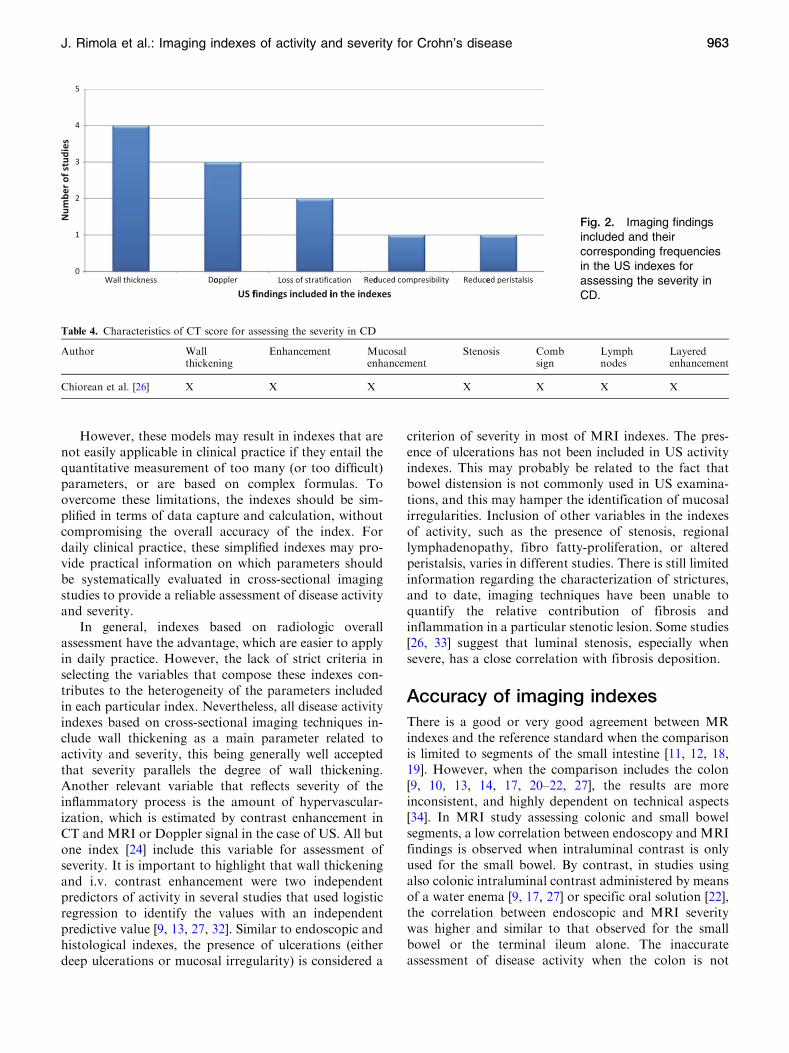
Four studies derived an US-based index of severity[14, 23–25] (Table 3). All the US-based indexes includedwall thickening as a parameter of activity and severity,with a cutoff point ranging from 3 to 4 mm. A semi-quantitative assessment of Doppler signal, previouslydescribed by Limberg [28], is included in the assessmentof severity in three out of the four described indexes [14,23, 25]. Finally, loss of stratification of the bowel wall isincluded in two US indexes [14, 24], and reduced peri-stalsis and compressibility, in one [24] (Fig. 2).
Only one study reporting a CT-scan based index ofinflammatory severity for CD was found. This index isbased on the presence of wall thickening, mucosal ormural enhancement, mural stratification, comb sign, andregional lymph nodes (Table 4) [26]. The same studyproposed an index for assessment of stenotic lesionsbased on the identification of a thickened non-enhancingwall, luminal narrowing, and the presence of pre-stenoticdilation.
Classification of indexes on CDseverity based on the derivationmodel
According to the methodology used for the constructionof the index, cross-sectional activity indexes can be di-vided into two broad groups: (1) indexes using theoverall assessment of the radiologist as the referencestandard, which comprise the majority of the indexespublished so far; and (2) indexes based on an externalreference standard of severity, namely endoscopy and/orhistology [9].
Indexes based on overall radiologist assessment
The majority of the indexes in this category are con-structed by selection of parameters that are associatedwith the presence of disease activity and/or are indicatorsof the presence of severe disease. The number ofparameters present defines the existence of active diseaseand level of severity, usually on a limited 3-point or4-point global scale (i.e., inactive, mild, moderate, orsevere). Alternatively, in other studies, a score of severityis assigned to each of the parameters evaluated, and thefinal value of the index is the sum of the scores of eachindividual parameter [11]. None of the indexes in thiscategory has been constructed using regression modelingT
able
2.Characteristics
ofMRIscoresforassessingtheseverityin
CD
Author
Wall
thickening
Enhancement
Stenosis
Mucosal
irregularity/
ulcers/
cobblestone
Edem
a/
target
sign
Perienteric
vascularization/
combsign
Lymph
nodes
Abscess
or
fistulas
Fibrofat
proliferation
Layered
enhancement
DWI
Peristalsis
Hyunet
al.[22]
XX
XX
XX
XFlorieet
al.[10]
XX
XX
XGiromettiet
al.[11]
XX
XX
XX
XX
XX
Horsthuiset
al.[21]
XX
XLaghiet
al.[12]
XX
Oussalahet
al.[13]
XX
XX
XX
Pascuet
al.[14]
XX
XRim
ola
etal.[9,27]
XX
XX
Sailer
etal.[15]
XX
XX
XSchreyer
etal.[16]
XX
XX
XSchreyer
etal.[17]
XX
XX
Seiderer
etal.[18]
XX
XX
XX
XTillack
etal.[19]
XX
XX
XX
X
J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease 961

to show an independent predictive value of each of theparameters included in the index for the presence ofdisease activity or severity.
Indexes based on external reference standard
Included in this group are the indexes in which the per-formance is compared with an external reference stan-dard, including ileocolonoscopy [9, 13, 27]. In somestudies, the variables composing each index have beenpre-defined [13], whereas, in others, the variables com-posing the index have been selected based on theirindependent predicting value for the presence of diseaseactivity and severity [9, 27].
Although the latter method is a priori more appro-priate, it should be taken into account that the perfor-mance of regression models used in diagnostic andprognostic prediction is generally better on the dataseton which the model has been constructed (derivation set)compared to the performance of the same model on newdata (validation set), especially in small data sets [29].Bootstrapping, cross-validation, and split-samplingtechniques are internal validation techniques, because theperformance is estimated using patients from the model’sderivation set only. However, only pure sampling vari-ability is considered with these techniques, and potential
changes in the patient population are not. By contrast,external validation addresses the accuracy of a model inpatients from a different but plausibly related popula-tion, which may be defined as a selected study populationrepresenting the underlying disease domain [30]. Mostreports evaluating imaging scores focused on the issue ofinternal validity, leaving the important issue of externalvalidity behind, which may compromise the generaliz-ability of a prediction model. The Crohn’s DiseaseEndoscopic Index of Severity (CDEIS) has been sub-mitted to external validation [7, 31], but among the cross-sectional imaging indexes only the Magnetic ResonanceIndex of Activity (MaRIA) has been externally validated,with nearly the same performance in the derivation andvalidation sets [9, 27].
Strengths and weaknesses of each model
In principle, the indexes based on regression models thatpredict activity assessed by an accepted external refer-ence standard are more stringent, since only the variableswith independent predictor value for activity and severityare selected, whereas those without a proven independentpredictor value are excluded from the scoring system,optimizing the evaluation of the imaging technique.
Fig. 1. Imaging findings included and their corresponding frequencies in the MRI indexes for assessing the severity in CD.
Table 3. Characteristics of ultrasonographic scores for assessing the severity in CD
Author Wallthickening
Doppler Loss ofstratification
Reducedperistalsis
Reducedcompressibility
Drews et al. [23] X XFutagami et al. [24] X X X XNeye et al. [25] X XPascu et al. [14] X X X
962 J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease
However, these models may result in indexes that arenot easily applicable in clinical practice if they entail thequantitative measurement of too many (or too difficult)parameters, or are based on complex formulas. Toovercome these limitations, the indexes should be sim-plified in terms of data capture and calculation, withoutcompromising the overall accuracy of the index. Fordaily clinical practice, these simplified indexes may pro-vide practical information on which parameters shouldbe systematically evaluated in cross-sectional imagingstudies to provide a reliable assessment of disease activityand severity.
In general, indexes based on radiologic overallassessment have the advantage, which are easier to applyin daily practice. However, the lack of strict criteria inselecting the variables that compose these indexes con-tributes to the heterogeneity of the parameters includedin each particular index. Nevertheless, all disease activityindexes based on cross-sectional imaging techniques in-clude wall thickening as a main parameter related toactivity and severity, this being generally well acceptedthat severity parallels the degree of wall thickening.Another relevant variable that reflects severity of theinflammatory process is the amount of hypervascular-ization, which is estimated by contrast enhancement inCT and MRI or Doppler signal in the case of US. All butone index [24] include this variable for assessment ofseverity. It is important to highlight that wall thickeningand i.v. contrast enhancement were two independentpredictors of activity in several studies that used logisticregression to identify the values with an independentpredictive value [9, 13, 27, 32]. Similar to endoscopic andhistological indexes, the presence of ulcerations (eitherdeep ulcerations or mucosal irregularity) is considered a
criterion of severity in most of MRI indexes. The pres-ence of ulcerations has not been included in US activityindexes. This may probably be related to the fact thatbowel distension is not commonly used in US examina-tions, and this may hamper the identification of mucosalirregularities. Inclusion of other variables in the indexesof activity, such as the presence of stenosis, regionallymphadenopathy, fibro fatty-proliferation, or alteredperistalsis, varies in different studies. There is still limitedinformation regarding the characterization of strictures,and to date, imaging techniques have been unable toquantify the relative contribution of fibrosis andinflammation in a particular stenotic lesion. Some studies[26, 33] suggest that luminal stenosis, especially whensevere, has a close correlation with fibrosis deposition.
Accuracy of imaging indexes
There is a good or very good agreement between MRindexes and the reference standard when the comparisonis limited to segments of the small intestine [11, 12, 18,19]. However, when the comparison includes the colon[9, 10, 13, 14, 17, 20–22, 27], the results are moreinconsistent, and highly dependent on technical aspects[34]. In MRI study assessing colonic and small bowelsegments, a low correlation between endoscopy and MRIfindings is observed when intraluminal contrast is onlyused for the small bowel. By contrast, in studies usingalso colonic intraluminal contrast administered by meansof a water enema [9, 17, 27] or specific oral solution [22],the correlation between endoscopic and MRI severitywas higher and similar to that observed for the smallbowel or the terminal ileum alone. The inaccurateassessment of disease activity when the colon is not
Fig. 2. Imaging findingsincluded and theircorresponding frequenciesin the US indexes forassessing the severity inCD.
Table 4. Characteristics of CT score for assessing the severity in CD
Author Wallthickening
Enhancement Mucosalenhancement
Stenosis Combsign
Lymphnodes
Layeredenhancement
Chiorean et al. [26] X X X X X X X
J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease 963

distended may be caused by imprecision in the mea-surement of wall thickness, contrast enhancement, or thepresence of ulcerations.
There is scarce information on the performance ofcross-sectional imaging techniques for evaluation ofdisease activity and severity in small bowel segmentsproximal to the terminal ileum. Only one study evaluatedthe diagnostic accuracy of MRI for assessing the severityof small bowel in CD using SBCE as the referencestandard [19]; agreement with regard to disease severitybetween the two techniques was found in the 75.5% ofsegments. Also, two studies compared the diagnosticaccuracy of MRI using double balloon enteroscopy asthe reference standard. In one study [18], agreement wasfound in 21 out of 28 segments of the small bowel. Theother study found a strong and significant correlationbetween MRI and endoscopical indexes (r = 0.88) [22].Finally, a high agreement (k coefficient > 0.8) has beenshown between MRI and endoscopy findings (Rutgeerts’score) in the evaluation of post-operative CD recurrencein ileocolonic anastomosies [15].
The four US-based indexes of activity showed highcorrelation with reference standard indexes [14, 23–25].In three of the studies, small bowel and colonic segmentswere assessed [14, 24, 25], and, in another study, only theterminal ileum was evaluated [23]. Unlike MRI studies,none of the US studies used the small or large bowelintraluminal contrast; therefore, the demonstrated USaccuracy is not dependent on this technical aspect.
Finally, the only one CT-based index of activityfound high correlation with pathological index ofinflammatory activity, and moderate correlation withpathological index of fibroestenosis [26].
A relevant point is that the accuracy of the cross-sectional indexes is not related to their complexity. In-dexes containing four or less variables have similaraccuracy as those that contain more variables. The sim-plicity to calculate scores with a lower number ofparameters facilitates its acceptance and implementationin daily practice and research, and may reduce interob-server variability.
The majority of indexes of activity of either MRI- orUS-based had found no or weak correlation betweenradiological indexes and clinical indexes or biomarkers.These data support the fact that clinical symptoms aloneare neither sensitive nor specific for assessment of lesionseverity, and more objective tests, such as imaging tech-niques, are required for an optimal clinical managementof patients with CD [2].
Comparison of different imaging techniquesfor assessment of severity in CD
One single study compared the accuracy of MRI and USindexes in the evaluation of disease severity in the colonand terminal ileum using ileocolonoscopy as reference
standard [14]. The endoscopic activity index had a highercorrelation with the US-based activity index (r = 0.83)than the MRI-based activity index (r = 0.12). However,this study did not use colonic intraluminal contrastwhich likely reduced the accuracy of MRI evaluation.
Use of cross-sectional imagingscores in clinical and researchsettings
In clinical practice, cross-sectional imaging techniquesprovide an objective measure of the presence of diseaseactivity and severity, which is needed to treatment opti-mization on an individualized basis. In the symptomaticpatient, objective demonstration of the presence of dis-ease activity may guide the indication for treatmentintensification by means of dose increments or intro-duction of a new drug class, but establishing a person-alized treatment plan commonly will also entail theassessment of lesion severity by means of an index. In-dexes to be used in clinical practice should be composedof variables that are easy to measure, with low interob-server variability, providing relevant prognostic impli-cations, and contributing to choose therapeuticstrategies. Only scores fulfilling these characteristics havegained wide acceptance, for example, the Balthazar scorefor the assessment of severity in acute pancreatitis [35].
Numerous studies have demonstrated that achievingmucosal healing is associated with a more benign courseof the disease [36, 37]. The degree of mucosal healing thatis associated with better outcomes is not necessarilycomplete disappearance of all inflammatory lesions, buthealing of severe lesions, corresponding to ulcers atendoscopy [37]. In this regard, MRI can provide anassessment of the presence of ulcerative lesions by directvisualization of the mucosal defects, but the sensitivity ofthis assessment is around 70% [27]. By contrast, assess-ment by means of a quantitative score that includes alsoa measurement of wall thickness, hyperenhancement,and the presence of edema has a sensitivity and speci-ficity higher than 90% for the detection of the presence ofulcerative lesions [9].
In clinical practice, imaging scoresmay also provide anobjective measure of a therapeutic response in the shortand long term. In ulcerative colitis, US scores have beenshown to have a high concordance with endoscopic scoresin the assessment of a short-term therapeutic response,and also to predict long-term (15-month) disease outcome[38]. Preliminary data on CD also confirm high correla-tion between short-term changes in endoscopic (CDEIS)and MRI scores (MaRIA) in response to induction ther-apy with steroids or anti-TNF antibodies [39].
In the research setting, the use of objective scores todetermine disease activity and severity, therapeutic re-sponses, and long-term outcomes is mandatory. In trialsassessing therapeutic benefits for treatment of active
964 J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease

disease, the scores should assure the inclusion of patientswith active inflammation of a certain severity, andexclusion of patients with symptoms not correspondingto presence of inflammation. This will result in theselection of homogeneous populations, and reduce pla-cebo response rates. For research purposes, assessmentof disease activity by means of cross-sectional imagingmay bring additional relevant information as comparedto endoscopy, in particular, the detection of unsuspectedstricturing or penetrating lesions, that may affect 5–16%
of the population with symptoms [2, 40], and mightconfound the evaluation of treatment efficacy.
Cross-sectional imaging assessment may provideadditional advantages for the evaluation of responses byallowing central reading, thus homogenizing the evalu-ation of the response across the population of patients inmulticenter studies. Clearly, central reading can beimplemented for CT and MRI, but would be morecomplex for US. Implementation of central reading im-poses certain requirements to participating centers, suchas availability of equipment providing certain levels ofresolution, and homogeneous protocols in terms of pa-tient preparation and image acquisition. The latter maybe challenging if centers use equipment from differentproviders.
Future perspectives
Currently available indexes developed for measuringdisease activity and severity in CD, including clinical,endoscopic, and imaging indexes, measure inflammatoryactivity at a certain time point [8]. However, CD is achronic and destructive disease that causes a progressiveloss of gastrointestinal function due to bowel damage.An international cooperative initiative is under way todevelop an instrument that can measure cumulative bo-wel damage, which takes into account damage location,severity, extent, progression, and reversibility, as mea-sured by diagnostic-imaging modalities and the historyof surgical resection [41]. This index (the Lemann’s score)is expected to be able to measure disease progression as afunction of time. This type of measurement is arequirement for the development of long-term trialsassessing the ability of a certain therapeutic strategy toalter disease course, separating these effects from theshort-term beneficial effects on symptoms that a partic-ular treatment may provide [42].
For clinical practice, a simple, semi-quantitative indexof activity is preferred, with a proper validation in anindependent cohort of patients (external validation),optimally developed in the context of a multicenterinternational initiative, all these contributing to thegeneralizability of the index. The index should providerelevant information on disease activity, severity, andprognosis, thus facilitating personalization of treatmentdecisions. Also the index should be responsive to the
healing effects of medical treatment to determine thera-peutic responses.
For research purposes, a precise quantitative measureof disease activity and severity is key to select homoge-neous populations, and to reduce the placebo effect.Standardization of image acquisition protocols and pa-tient preparation should be procured. In this regard,manufacturers should provide compatibility of protocolsbetween different equipments. Whether the quantitative-validated MaRIA index or a simplified index is prefera-ble requires further research. Furthermore, the index ofbowel damage currently under development is requiredto determine the ability of therapeutic strategies tomodify disease course in the long term.
References
1. Best WR, Becktel JM, Singleton JW, Kern F Jr (1976) Develop-ment of a Crohn’s disease activity index: national cooperativeCrohn’s disease study. Gastroenterology 70:439–444
2. Colombel JF, Sandborn WJ, Reinisch W, et al. (2010) Infliximab,azathioprine, or combination therapy for Crohn’s disease. N Engl JMed 362(15):1383–1395. doi:10.1056/NEJMoa0904492
3. Hanauer SB, Feagan BG, Lichtenstein GR, et al. (2002) Mainte-nance infliximab for Crohn’s disease: the ACCENT I randomisedtrial. Lancet 359:1541–1549
4. Lemann M, Mary JY, Colombel JF, et al. (2005) A randomized,double-blind, controlled withdrawal trial in Crohn’s disease pa-tients in long-term remission on azathioprine. Gastroenterology128(7):1812–1818
5. Allez M, Lemann M, Bonnet J, et al. (2002) Long term outcome ofpatients with active Crohn’s disease exhibiting extensive and deepulcerations at colonoscopy. Am J Gastroenterol 97(4):947–953
6. Solberg IC, Vatn MH, Hoie O, et al. (2007) Clinical course inCrohn’s disease: results of a Norwegian population-based ten-yearfollow-up study. Clin Gastroenterol Hepatol 5(12):1430–1438
7. Landi B, Anh TN, Cortot A, et al. (1992) Endoscopic monitoringof Crohn’s disease treatment: a prospective, randomized clinicaltrial. The Groupe d’Etudes Therapeutiques des Affections Inflam-matoires Digestives. Gastroenterology 102(5):1647–1653
8. Panes J, Bouzas R, Chaparro M, et al. (2011) Systematic review:the use of ultrasonography, computed tomography and magneticresonance imaging for the diagnosis, assessment of activity andabdominal complications of Crohn’s disease. Aliment PharmacolTher 34(2):125–145. doi:10.1111/j.1365-2036.2011.04710.x
9. Rimola J, Rodriguez S, Garcia BO, et al. (2009) Magnetic reso-nance for assessment of disease activity and severity in Crohndisease. Gut 58(8):1113–1120. doi:10.1136/gut.2008.167957
10. Florie J, Horsthuis K, Hommes DW, et al. (2005) Magnetic reso-nance imaging compared with ileocolonoscopy in evaluating dis-ease severity in Crohn’s disease. Clin Gastroenterol Hepatol3(12):1221–1228
11. Girometti R, Zuiani C, Toso F, et al. (2008) MRI scoring systemincluding dynamic motility evaluation in assessing the activity ofCrohn’s disease of the terminal ileum. Acad Radiol 15(2):153–164
12. Laghi A, Borrelli O, Paolantonio P, et al. (2003) Contrast enhancedmagnetic resonance imaging of the terminal ileum in children withCrohn’s disease. Gut 52(3):393–397
13. Oussalah A, Laurent V, Bruot O, et al. (2010) Diffusion-weightedmagnetic resonance without bowel preparation for detecting co-lonic inflammation in inflammatory bowel disease. Gut 59(8):1056–1065. doi:10.1136/gut.2009.197665
14. Pascu M, Roznowski AB, Muller HP, et al. (2004) Clinical rele-vance of transabdominal ultrasonography and magnetic resonanceimaging in patients with inflammatory bowel disease of the termi-nal ileum and large bowel. Inflamm Bowel Dis 10(4):373–382
15. Sailer J, Peloschek P, Reinisch W, et al. (2008) Anastomoticrecurrence of Crohn’s disease after ileocolic resection: comparisonof MR enteroclysis with endoscopy. Eur Radiol 18(11):2512–2521
J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease 965

16. Schreyer AG, Golder S, Scheibl K, et al. (2005) Dark lumenmagnetic resonance enteroclysis in combination with MRI colo-nography for whole bowel assessment in patients with Crohn’sdisease: first clinical experience. Inflamm Bowel Dis 11(4):388–394
17. Schreyer AG, Rath HC, Kikinis R, et al. (2005) Comparison ofmagnetic resonance imaging colonography with conventionalcolonoscopy for the assessment of intestinal inflammation in pa-tients with inflammatory bowel disease: a feasibility study. Gut54(2):250–256
18. Seiderer J, Herrmann K, Diepolder H, et al. (2007) Double-balloonenteroscopy versus magnetic resonance enteroclysis in diagnosingsuspected small-bowel Crohn’s disease: results of a pilot study.Scand J Gastroenterol 42(11):1376–1385
19. Tillack C, Seiderer J, Brand S, et al. (2008) Correlation of magneticresonance enteroclysis (MRE) and wireless capsule endoscopy (CE)in the diagnosis of small bowel lesions in Crohn’s disease. InflammBowel Dis 14(9):1219–1228
20. van Gemert-Horsthuis K, Florie J, Hommes DW, et al. (2006)Feasibility of evaluating Crohn’s disease activity at 3.0 Tesla. JMagn Reson Imaging 24(2):340–348
21. Horsthuis K, de Ridder L, Smets AM, et al. (2010) Magnetic res-onance enterography for suspected inflammatory bowel disease in apediatric population. J Pediatr Gastroenterol Nutr 51(5):603–609.doi:10.1097/MPG.0b013e3181dee5bd
22. Hyun SB, Kitazume Y, Nagahori M, et al. (2011) Magnetic reso-nance enterocolonography is useful for simultaneous evaluation ofsmall and large intestinal lesions in Crohn’s disease. Inflamm BowelDis 17(5):1063–1072. doi:10.1002/ibd.21510
23. Drews BH, Barth TF, Hanle MM, et al. (2009) Comparison ofsonographically measured bowel wall vascularity, histology, anddisease activity in Crohn’s disease. Eur Radiol 19(6):1379–1386
24. Futagami Y, Haruma K, Hata J, et al. (1999) Development andvalidation of an ultrasonographic activity index of Crohn’s disease.Eur J Gastroenterol Hepatol 11(9):1007–1012
25. Neye H, Voderholzer W, Rickes S, et al. (2004) Evaluation of cri-teria for the activity of Crohn’s disease by power Doppler sonog-raphy. Dig Dis 22(1):67–72
26. Chiorean MV, Sandrasegaran K, Saxena R, et al. (2007) Correla-tion of CT enteroclysis with surgical pathology in Crohn’s disease.Am J Gastroenterol 102(11):2541–2550
27. Rimola J, Ordas I, Rodriguez S, et al. (2011) Magnetic resonanceimaging for evaluation of Crohn’s disease: validation of parametersof severity and quantitative index of activity. Inflamm Bowel Dis17(8):1759–1768. doi:10.1002/ibd.21551
28. Limberg B (1999) Diagnosis of chronic inflammatory bowel diseaseby ultrasonography. Z Gastroenterol 37(6):495–508
29. Steyerberg EW, Eijkemans MJ, Harrell FE Jr, Habbema JD (2000)Prognostic modelling with logistic regression analysis: a compari-son of selection and estimation methods in small data sets. StatMed 19(8):1059–1079
30. Justice AC, Covinsky KE, Berlin JA (1999) Assessing the general-izability of prognostic information. Ann Intern Med 130(6):515–524
31. Modigliani R, Mary JY, Simon JF, et al. (1990) Clinical, biological,and endoscopic picture of attacks of Crohn’s disease. Evolution onprednisolone. Groupe d’Etude Therapeutique des Affections In-flammatoires Digestives. Gastroenterology 98(4):811–818
32. Punwani S, Rodriguez-Justo M, Bainbridge A, et al. (2009) Muralinflammation in Crohn disease: location-matched histologic vali-dation of MR imaging features. Radiology 252(3):712–720. doi:10.1148/radiol.2523082167
33. Soyer P, Boudiaf M, Sirol M, et al. (2010) Suspected anastomoticrecurrence of Crohn disease after ileocolic resection: evaluationwith CT enteroclysis. Radiology 254(3):755–764. doi:10.1148/radiol.09091165
34. Rimola J, Ordas I, Rodriguez S, Panes J (2010) Colonic Crohn’sdisease: value of magnetic resonance colonography for detectionand quantification of disease activity. Abdom Imaging 35(4):422–427. doi:10.1007/s00261-009-9545-4
35. Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH (1990)Acute pancreatitis: value of CT in establishing prognosis. Radiol-ogy 174(2):331–336
36. Froslie KF, Jahnsen J, Moum BA, Vatn MH (2007) Mucosalhealing in inflammatory bowel disease: results from a Norwegianpopulation-based cohort. Gastroenterology 133(2):412–422. doi:10.1053/j.gastro.2007.05.051
37. Schnitzler F, Fidder H, Ferrante M, et al. (2009) Mucosal healingpredicts long-term outcome of maintenance therapy with infliximabin Crohn’s disease. Inflamm Bowel Dis 15(9):1295–1301. doi:10.1002/ibd.20927
38. Parente F, Molteni M, Marino B (2010) Are colonoscopy andbowel ultrasound useful for assessing response to short-term ther-apy and predicting disease outcome of moderate-to-severe forms ofulcerative colitis?: a prospective study. Am J Gastroenterol105(5):1150–1157. doi:10.1038/ajg.2009.672
39. Ordas I, Rimola J, Ripolles T, et al. (2011) Accuracy of MRI toassess therapeutic responses and mucosal healing in Crohn’s dis-ease. Gastroenterology 140:S-73
40. Higgins PD, Caoili E, Zimmermann M (2007) Computed tomo-graphic enterography adds information to clinical management insmall bowel Crohn’s disease. Inflamm Bowel Dis 13(3):262–268.doi:10.1002/ibd.20013
41. Pariente B, Cosnes J, Danese S, et al. (2011) Development of theCrohn’s disease digestive damage score, the Lemann score. In-flamm Bowel Dis 17(6):1415–1422. doi:10.1002/ibd.21506
42. D’Agostino RB Sr (2009) The delayed-start study design. N Engl JMed 361(13):1304–1306. doi:10.1056/NEJMsm0904209
966 J. Rimola et al.: Imaging indexes of activity and severity for Crohn’s disease