imaging in the evaluation of suspected pulmonary...
TRANSCRIPT
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
Imaging in the Evaluation of Imaging in the Evaluation of Suspected Pulmonary EmbolismSuspected Pulmonary Embolism
Elizabeth Elizabeth PinskyPinsky, HMS III, HMS IIIGillian Lieberman, MDGillian Lieberman, MD
November 2003
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
2
Mrs. BWMrs. BW
Mrs. BW is a 74Mrs. BW is a 74--yearyear--old woman with a old woman with a history of HTN, DM, obesity and COPD who history of HTN, DM, obesity and COPD who presents to the EW with acute worsening of presents to the EW with acute worsening of her baseline her baseline dyspneadyspnea..On exam she is On exam she is dyspneicdyspneic and and tachycardictachycardic, , with oxygen saturation of 85% on room air. with oxygen saturation of 85% on room air. She has an elevated JVP, an RV heave, and an She has an elevated JVP, an RV heave, and an audible S4.audible S4.Clinical suspicion for PE is high. What now?Clinical suspicion for PE is high. What now?

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
3
AgendaAgenda
Briefly discuss pulmonary embolism and the Briefly discuss pulmonary embolism and the controversy surrounding its diagnosis.controversy surrounding its diagnosis.Examine the menu of imaging options, and Examine the menu of imaging options, and discuss their advantages, disadvantages, and discuss their advantages, disadvantages, and appropriate use.appropriate use.Review current recommendations for the Review current recommendations for the workwork--up of suspected pulmonary embolism.up of suspected pulmonary embolism.
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
4
Pulmonary Pulmonary ThromboembolismThromboembolismHypercoaguabiltyHypercoaguabilty leads to thrombus formation in deep veins of leads to thrombus formation in deep veins of extremities. Thrombi extremities. Thrombi propogatepropogate proximally, and may dislodge proximally, and may dislodge and and embolizeembolize to pulmonary vasculature .to pulmonary vasculature .Outcomes range from incidental Outcomes range from incidental thromboembolismthromboembolism to severe to severe hypoxemia and acute right sided heart failure.hypoxemia and acute right sided heart failure.Incidence in US exceeds 600,000 per year; PE results in at leastIncidence in US exceeds 600,000 per year; PE results in at least250,000 hospitalizations annually250,000 hospitalizations annually(4)(4). . Risk factors include Risk factors include (2)(2) ::
––
Age >40Age >40––
History of venous History of venous thromboembolismthromboembolism––
Recent surgery, prolonged immobilityRecent surgery, prolonged immobility––
CVA or CHFCVA or CHF––
MalignancyMalignancy––
Pelvis, hip, or tibia fracturePelvis, hip, or tibia fracture––
ObesityObesity––
Pregnancy or recent deliveryPregnancy or recent delivery––
IBDIBD––
Inherited or Inherited or accquiredaccquired
thrombophiliathrombophilia
(Factor V Leiden, lupus anticoagulant, (Factor V Leiden, lupus anticoagulant, etc.)etc.)

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
5
Presentation and Differential Presentation and Differential Diagnosis of Acute PEDiagnosis of Acute PE
PE can present with PE can present with dyspneadyspnea, tachycardia, , tachycardia, hemoptysishemoptysis, chest , chest pain, cough, and even syncope. pain, cough, and even syncope. The differential diagnosis is very broad and includesThe differential diagnosis is very broad and includes(4)(4)::––
Pneumonia or bronchitisPneumonia or bronchitis––
Asthma or COPD exacerbationAsthma or COPD exacerbation––
Myocardial infarctionMyocardial infarction––
Pulmonary edemaPulmonary edema––
AnxietyAnxiety––
Aortic dissectionAortic dissection––
Pericardial Pericardial tamponadetamponade––
Lung cancerLung cancer––
Primary pulmonary hypertensionPrimary pulmonary hypertension––
Rib fractureRib fracture––
PneumothoraxPneumothorax––
CostochondritisCostochondritis––
Musculoskeletal pain Musculoskeletal pain
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
6
The Importance of Accurate The Importance of Accurate DiagnosisDiagnosis
Mortality rate with therapy falls from 30% to 5%, and Mortality rate with therapy falls from 30% to 5%, and 94% of annual deaths from PE are in patients who 94% of annual deaths from PE are in patients who never received treatment never received treatment (1)(1). Sensitivity in diagnosis . Sensitivity in diagnosis is essential to institute therapy in all appropriate is essential to institute therapy in all appropriate cases.cases.Anticoagulation therapy for PE is associated with Anticoagulation therapy for PE is associated with mortality and morbidity; specificity in diagnosis is mortality and morbidity; specificity in diagnosis is essential to avoid unnecessary treatment.essential to avoid unnecessary treatment.Bedside tests, including ABG, and ECG are Bedside tests, including ABG, and ECG are unreliable. Dunreliable. D--DimerDimer has been shown to be close to has been shown to be close to 100% sensitive, but is non100% sensitive, but is non--specific specific (2)(2) ..

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
7
ImagingImagingPulmonary Angiography remains the goldPulmonary Angiography remains the gold--standard standard for diagnosis, and has the potential for therapeutic for diagnosis, and has the potential for therapeutic intervention (through intervention (through percutaneouspercutaneous thrombectomythrombectomy).).It is associated with a 0.5% mortality risk, and a 0.8% It is associated with a 0.5% mortality risk, and a 0.8% risk of major complications risk of major complications (2)(2)..NonNon--Invasive ImagingInvasive Imaging––
CXRCXR––
V/Q V/Q ––
CTACTA––
MRI/MRAMRI/MRA––
USUSV/Q scanning was standard for decades; CTA is V/Q scanning was standard for decades; CTA is gaining wide acceptance as speed, availability, and gaining wide acceptance as speed, availability, and sensitivity improve.sensitivity improve.

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
8
CXR FindingsCXR FindingsCXR is an essential first step in the workCXR is an essential first step in the work--up of PE up of PE to rule out to rule out other other diagnoses, but it is not diagnoses, but it is not sufficiently sensitive or specific for PE diagnosis.sufficiently sensitive or specific for PE diagnosis.Common findings in PE include Common findings in PE include cardiomegalycardiomegaly, , atelectasisatelectasis, pleural effusion, elevation of , pleural effusion, elevation of hemidiaphragmhemidiaphragm, pulmonary edema and , pulmonary edema and prominent pulmonary arteries.prominent pulmonary arteries.Two signs are thought to be more suggestive of Two signs are thought to be more suggestive of PEPE––
Westermark’sWestermark’s
sign sign ––
regional pulmonary regional pulmonary oligemiaoligemia
(decreased (decreased vascularityvascularity).).––
Hampton’s hump Hampton’s hump ––
wedgewedge--shaped, pleuralshaped, pleural--based based
opacity in region of infarction.opacity in region of infarction.
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
9
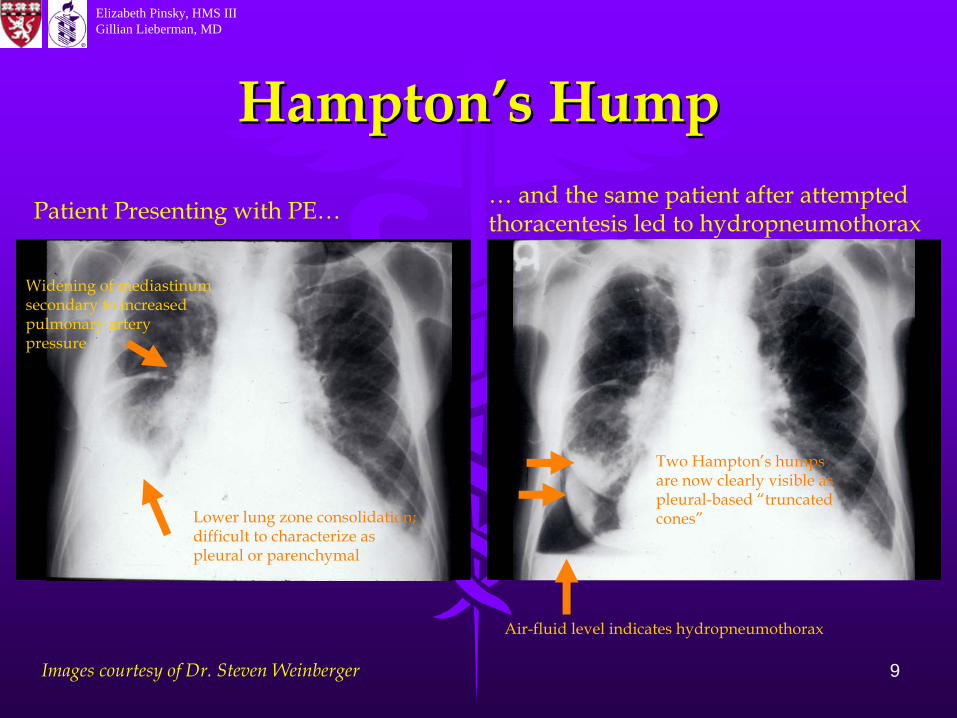
Hampton’s HumpHampton’s Hump
Images courtesy of Dr. Steven Weinberger
Patient Presenting with PE… … and the same patient after attempted thoracentesis
led to hydropneumothorax
Widening of mediastinum
secondary to increased pulmonary artery pressure
Lower lung zone consolidation; difficult to characterize as pleural or parenchymal
Two Hampton’s humps are now clearly visible as pleural-based “truncated cones”
Air-fluid level indicates hydropneumothorax

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
10
VentilationVentilation--Perfusion ScanningPerfusion ScanningV/Q scan is a nuclear study using V/Q scan is a nuclear study using radiolabeledradiolabeled aerosol to trace ventilation and aerosol to trace ventilation and radiolabeledradiolabeled albumin aggregates to trace albumin aggregates to trace perfusion.perfusion.Perfusion defects are interpreted in the Perfusion defects are interpreted in the setting of ventilation defects (if any).setting of ventilation defects (if any).Scans are normal or abnormal; abnormal Scans are normal or abnormal; abnormal scans are further stratified as low, scans are further stratified as low, intermediate, and high probability for PE.intermediate, and high probability for PE.Advantages of VQ scan over CTA include Advantages of VQ scan over CTA include lowlow--dose radiation and accurate dose radiation and accurate representation of physiology.representation of physiology.

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
11
PIOPEDPIOPED (Prospective Investigation Of Pulmonary Embolism Diagnosis(Prospective Investigation Of Pulmonary Embolism Diagnosis
PIOPED study prospectively compared VQ to PIOPED study prospectively compared VQ to pulmonary angiography, and showed high pulmonary angiography, and showed high sensitivity of abnormal scan (98%) and high sensitivity of abnormal scan (98%) and high specificity (97%) of high probability abnormal scanspecificity (97%) of high probability abnormal scan(7)(7)..Problematically, few patients with PE had high Problematically, few patients with PE had high probability scans (sensitivity 42%) and most patients probability scans (sensitivity 42%) and most patients without PE had abnormal scans (specificity 10%) without PE had abnormal scans (specificity 10%) (7)(7) ..PIOPED concluded that V/Q scanning ruled out PE PIOPED concluded that V/Q scanning ruled out PE or was diagnostic only in a minority of patients who or was diagnostic only in a minority of patients who had unequivocal scan findings and concordant had unequivocal scan findings and concordant clinical findings clinical findings (7)(7)..
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
12
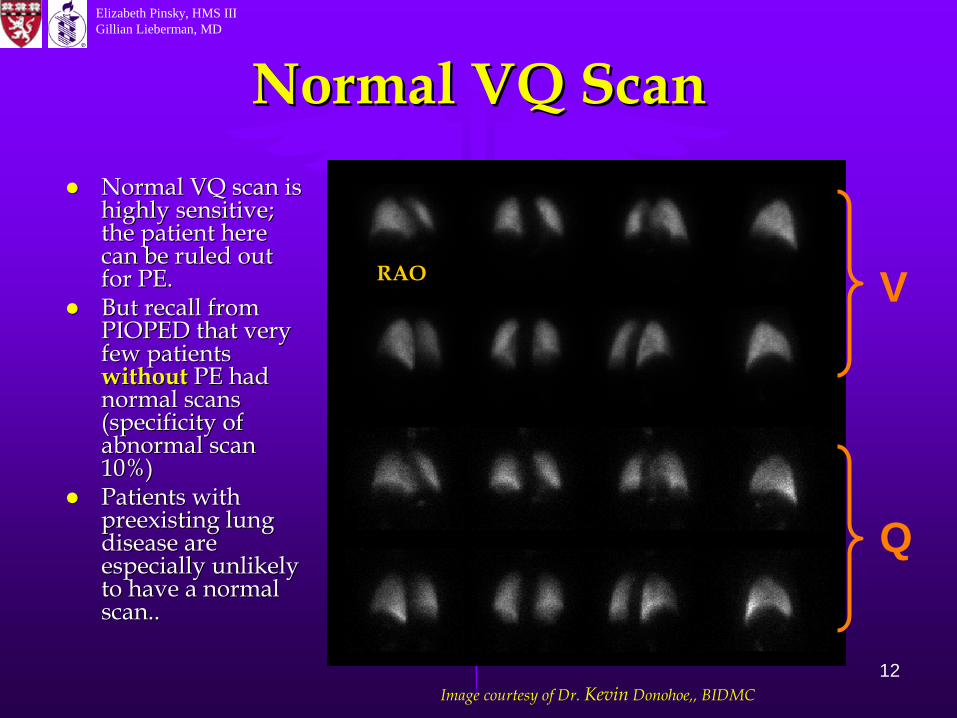
Normal VQ ScanNormal VQ ScanNormal VQ scan is Normal VQ scan is highly sensitive; highly sensitive; the patient here the patient here can be ruled out can be ruled out for PE.for PE.But recall from But recall from PIOPED that very PIOPED that very few patients few patients withoutwithout PE had PE had normal scans normal scans (specificity of (specificity of abnormal scan abnormal scan 10%)10%)Patients with Patients with preexisting lung preexisting lung disease are disease are especially unlikely especially unlikely to have a normal to have a normal scan..scan..
Image courtesy of Dr. Kevin
Donohoe,, BIDMC
V
Q
RAO
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
13
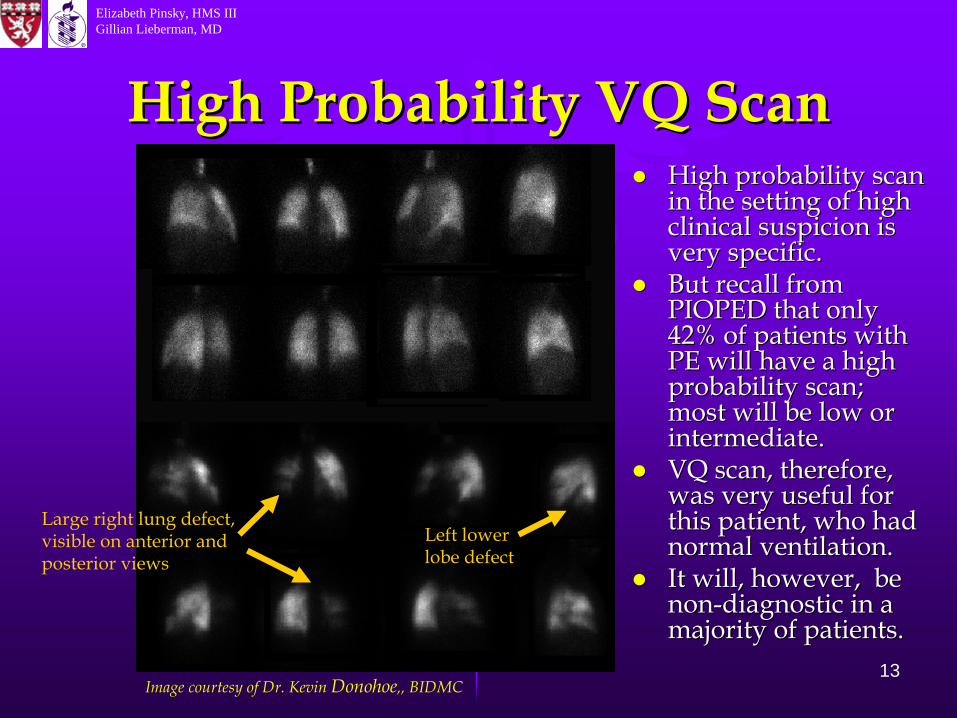
High Probability VQ ScanHigh Probability VQ ScanHigh probability scan High probability scan in the setting of high in the setting of high clinical suspicion is clinical suspicion is very specific.very specific.But recall from But recall from PIOPED that only PIOPED that only 42% of patients with 42% of patients with PE will have a high PE will have a high probability scan; probability scan; most will be low or most will be low or intermediate.intermediate.VQ scan, therefore, VQ scan, therefore, was very useful for was very useful for this patient, who had this patient, who had normal ventilation. normal ventilation. It will, however, be It will, however, be nonnon--diagnostic in a diagnostic in a majority of patients.majority of patients.
Image courtesy of Dr. Kevin Donohoe,, BIDMC
Left lower lobe defect
Large right lung defect, visible on anterior and posterior views
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
14
CTACTAAdvantages include speed, availability, and Advantages include speed, availability, and convenience.convenience.Patients with renal insufficiency or other Patients with renal insufficiency or other contraindications to contrast are not good contraindications to contrast are not good candidates.candidates.CTA is specific, ranging from 78CTA is specific, ranging from 78--100% 100% (2)(2) ..Sensitivity varies widely between studies, Sensitivity varies widely between studies, from 57from 57--100% 100% (2)(2). Variation can be attributed . Variation can be attributed to:to:––
Differing technology; as scanners improve Differing technology; as scanners improve resolution and minimize motion artifact, resolution and minimize motion artifact, sensitivity increases.sensitivity increases.
––
Location of embolus; sensitivity improves with Location of embolus; sensitivity improves with size of vessel.size of vessel.
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
15
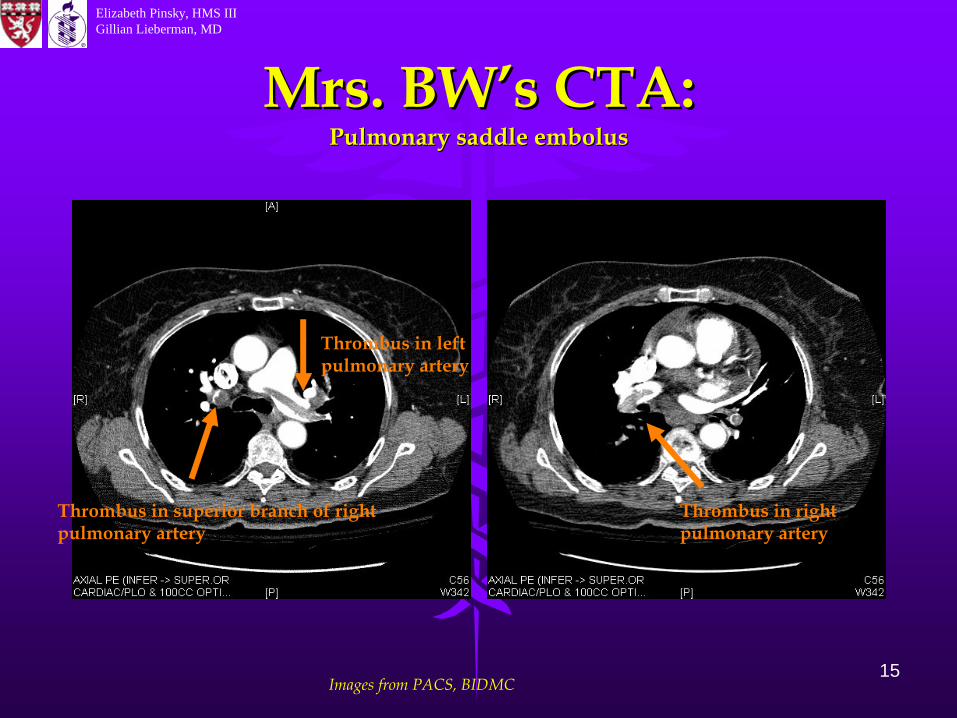
Mrs. BW’s CTA:Mrs. BW’s CTA: Pulmonary saddle embolusPulmonary saddle embolus
Images from PACS, BIDMC
Thrombus in left pulmonary artery
Thrombus in superior branch of right pulmonary artery
Thrombus in right pulmonary artery

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
16
Summary of CTA v. VQSummary of CTA v. VQCTA AdvantagesCTA Advantages––
Convenient, fast, and Convenient, fast, and specific.specific.
––
Sensitivity of newer CT Sensitivity of newer CT scanners is likely scanners is likely underestimated by much underestimated by much of the current data.of the current data.
––
Appropriate for patients Appropriate for patients with preexisting lung with preexisting lung disease, in whom V/Q is disease, in whom V/Q is particularly lowparticularly low--yield.yield.
V/Q AdvantagesV/Q Advantages––
Normal scan is very Normal scan is very sensitive; high sensitive; high probability scan is very probability scan is very specific.specific.
––
Lower dose radiation.Lower dose radiation.––
Unlike CTA, can Unlike CTA, can visualize physiologic visualize physiologic impact of disease. impact of disease.
––
Can be used in patients Can be used in patients who are not candidates who are not candidates for IV contrast.for IV contrast.
So, how should we approach patients like Mrs. BW?
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
17
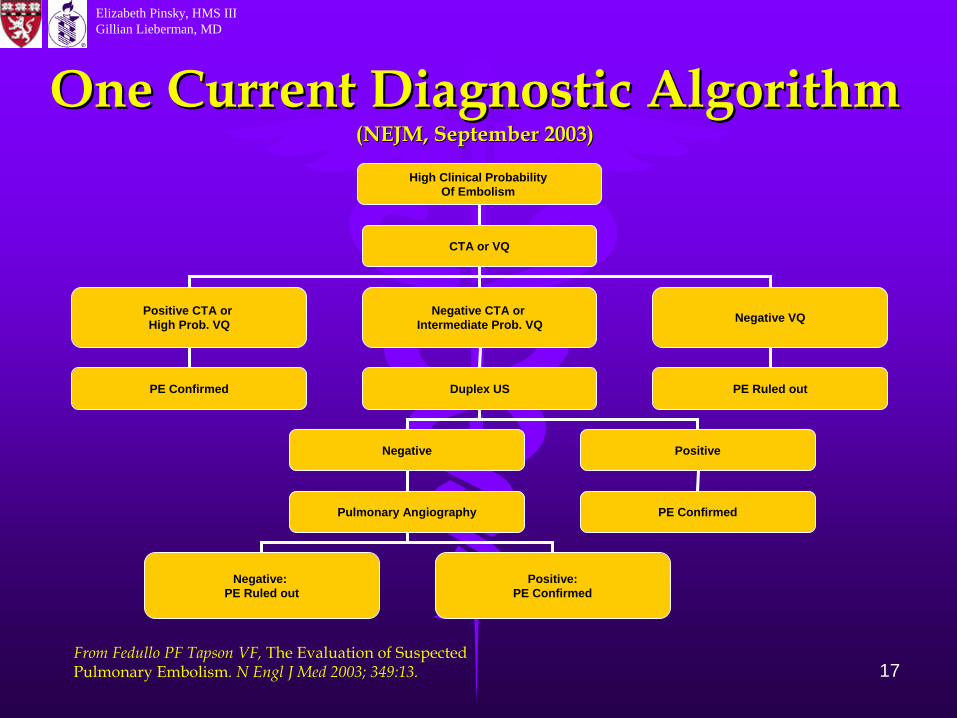
High Clinical Probability Of Embolism
CTA or VQ
Positive CTA or High Prob. VQ
Negative CTA or Intermediate Prob. VQ Negative VQ
PE Confirmed PE Ruled outDuplex US
Negative Positive
PE ConfirmedPulmonary Angiography
Negative: PE Ruled out
Positive:PE Confirmed
One Current Diagnostic Algorithm One Current Diagnostic Algorithm (NEJM, September 2003)(NEJM, September 2003)
From Fedullo
PF Tapson
VF, The Evaluation of Suspected Pulmonary Embolism. N Engl
J Med 2003; 349:13.
Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
18
The Future of Suspected The Future of Suspected PE EvaluationPE Evaluation
MRI angiography has shown potential in evaluation of MRI angiography has shown potential in evaluation of PE, with sensitivity of 75PE, with sensitivity of 75--100% and specificity of 95100% and specificity of 95--100% in one recent study100% in one recent study(6)(6)
MRI is more expensive, less convenient, and more time MRI is more expensive, less convenient, and more time consuming than CTA and has yet to be widely used. consuming than CTA and has yet to be widely used. PIOPED II: currently recruiting, will assess CTA for PIOPED II: currently recruiting, will assess CTA for evaluation of pulmonary embolismevaluation of pulmonary embolism(5).(5).
As CT technology improves, the sensitivity and As CT technology improves, the sensitivity and specificity of CTA for PE will also likely improve; specificity of CTA for PE will also likely improve; PIOPED II may not accurately represent this. PIOPED II may not accurately represent this. The convenience, speed and availability of CTA are The convenience, speed and availability of CTA are likely to only solidify its position as a mainstay of likely to only solidify its position as a mainstay of evaluation for suspected PE, but V/Q scanning still has evaluation for suspected PE, but V/Q scanning still has a role and is an important weapon in our diagnostic a role and is an important weapon in our diagnostic arsenal.arsenal.

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
19
ReferencesReferences1. Dalen JE. 1. Dalen JE. Pulmonary Embolism: What Have We Learned Since Virchow? Pulmonary Embolism: What Have We Learned Since Virchow? Chest Chest 2002; 122:4.2002; 122:4.2. 2. FedulloFedullo PF, PF, TapsonTapson VF. VF. The Evaluation of Suspected Pulmonary Embolism. The Evaluation of Suspected Pulmonary Embolism. The The New England Journal of Medicine 2003; 349: 1247New England Journal of Medicine 2003; 349: 1247--1256.1256.3. 3. GargGarg, K. , K. CT of CT of PulmonsryPulmonsry ThromboembolicThromboembolic Disease. Disease. Radiologic Clinics of North Radiologic Clinics of North America 2002; 40:1.America 2002; 40:1.4. 4. GoldhaberGoldhaber, SZ. , SZ. Pulmonary Embolism. Pulmonary Embolism. The New England Journal of Medicine The New England Journal of Medicine 2003; 339: 932003; 339: 93--104.104.5. Gottschalk A, Stein PD, Goodman LR, 5. Gottschalk A, Stein PD, Goodman LR, SostmanSostman HD. HD. Overview of Prospective Overview of Prospective Investigation of Investigation of PulmonsryPulmonsry Embolism Diagnosis II. Embolism Diagnosis II. Seminars in Nuclear Medicine Seminars in Nuclear Medicine 2002; 32:3.2002; 32:3.6. Meany JFM, 6. Meany JFM, WegWeg JG, JG, ChenevertChenevert TL, StaffordTL, Stafford--Johnson D, Hamilton BH, Prince Johnson D, Hamilton BH, Prince MR. MR. Diagnosis of Pulmonary Embolism with Magnetic Resonance AngiograDiagnosis of Pulmonary Embolism with Magnetic Resonance Angiography. phy. The The New England Journal of Medicine 2003; 336: 1422New England Journal of Medicine 2003; 336: 1422--1427.1427.7. PIOPED Investigators. 7. PIOPED Investigators. Value of the Ventilation/Perfusion Scan in Acute Pulmonary Embolism. Results of the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED). JAMA 1990; 263: 2753-2759.8. 8. WorsleyWorsley DF, DF, AbassAbass A. A. Radionuclide Imaging of Acute Pulmonary Embolism. Radionuclide Imaging of Acute Pulmonary Embolism. Radiologic Clinics of North America 2001; 39:5.Radiologic Clinics of North America 2001; 39:5.

Elizabeth Pinsky, HMS IIIGillian Lieberman, MD
20
AcknowledgementsAcknowledgements Many thanks to:Many thanks to:
Drs. James Busch, Kevin Drs. James Busch, Kevin DonohoeDonohoe, and , and Steven Weinberger for their help in Steven Weinberger for their help in obtaining images for this presentation.obtaining images for this presentation.Dr. Gillian LiebermanDr. Gillian LiebermanPamela Pamela LepkowskiLepkowskiLarry BarbarasLarry Barbaras