antenatal sonographic findings in trisomy...
TRANSCRIPT
Junne Kamihara, HMS IIIGillian Lieberman, MD
Prenatal Sonographic Findings in Trisomy 21
Junne Kamihara, HMS Year IIIGillian Lieberman, MD
March 2007

Estroff, JA Semin Roentgenol. 2004, 39:2 2
Junne Kamihara, HMS IIIGillian Lieberman, MD
Prenatal imaging: Menu of tests Ultrasound
Advantages• Non-invasive• Not harmful to fetus,
even in first trimester• Cost-effective• Main modality for
screening
Disadvantages• Operator-dependent• Unable to detect many
anomalies in fetus
Estroff, JA Semin Roentgenol. 2004, 39:2 3
Junne Kamihara, HMS IIIGillian Lieberman, MD
Prenatal imaging: Menu of tests MRI and Maternal Radiography
MRI• Better characterization of
anatomic details (e.g. brain)
• Better tissue contrast• Large field of view• Safety for fetus still not
well characterized (avoid first trimester)
Maternal Radiography• Used historically for
limited survey of structural anomalies
• Currently investigated for use in additional studies (e.g. to evaluate fetal bone)
Shinmoto H, et. al. Radiographics 2000, 20
4
Junne Kamihara, HMS IIIGillian Lieberman, MD
Prenatal Ultrasound
• Full fetal survey: ~18 weeks gestation (structural anomalies can be detected)
• Early ultrasound: 10-14 weeks gestation– Nuchal translucency measurements

Emery’s Elements of Medical Genetics , 1995 5
Junne Kamihara, HMS IIIGillian Lieberman, MD
Down Syndrome
• Common: overall incidence about 1 in 700
• Trisomy 21 (47XX or 47XY)• Most Trisomy 21 caused by
non-disjunction event in maternal meiosis
• Strong association with advancing maternal age
Karyotype with 3 copies of Chromosome 21
http://www.biotechnologyonline.gov.au
6
Junne Kamihara, HMS IIIGillian Lieberman, MD
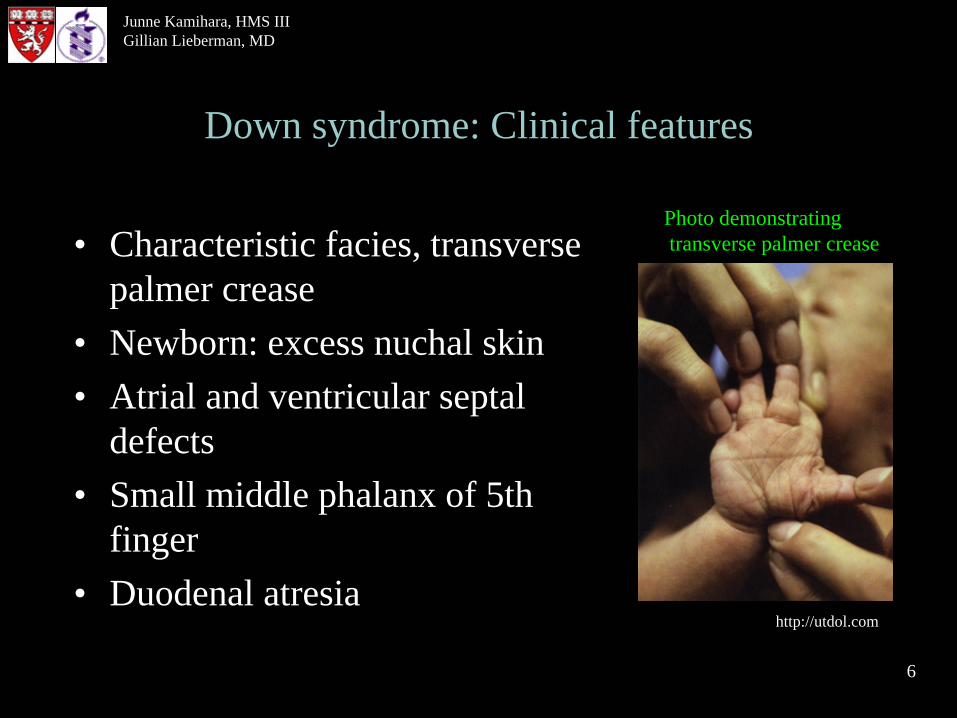
Down syndrome: Clinical features
• Characteristic facies, transverse palmer crease
• Newborn: excess nuchal skin• Atrial and ventricular septal
defects• Small middle phalanx of 5th
finger• Duodenal atresia
Photo demonstratingtransverse palmer crease
http://utdol.com
Adapted from Table 1: Estroff, JA Semin Roentgenol. 2004, 39:2
7
Junne Kamihara, HMS IIIGillian Lieberman, MD
Ultrasound detection of Down syndrome
Structural anomaliesNB: found in less than 20%
fetuses with Trisomy 21• Cardiac defects: e.g. VSD,
ASD• Duodenal atresia• Ventriculomegaly
Sonographic markers• Shortened proximal long
bones (humerus/femur)• Echogenic intracardiac
focus• Echogenic bowel• Absent nasal bone• Nuchal thickening• Pyelectasis (renal pelvis
dilation)

8
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient 1: JM 11 wks 2 days
• 36 yo G1P0 female who presents for her initial visit to the OB
• 11 weeks and 2 days pregnant and otherwise healthy
• No known history of inherited genetic or chromosomal disorders
• Expresses a desire to have first trimester screening.

9
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient JM: Early OB ultrasound 12 wks 4 days
• Transabdominal ultrasound• Crown rump length corresponding to
appropriate gestational age
• Significant abnormal finding: Thickened nuchal translucency (NT)

PACS, BIDMC 10
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient JM fetus: Sagittal Ultrasound Demonstrating Thickened NT of 4.2 mm
http://www.mums.me.uk
Thickened NT
*Landmark:*: Skin
11
Junne Kamihara, HMS IIIGillian Lieberman, MD
The following images show another example of thickened nuchal translucency in a 12-week fetus with Trisomy 21 (right), as well as an example of the corresponding subcutaneous fluid collection
which can be seen behind the neck (left)

http://www.centrus.com.br 12
Junne Kamihara, HMS IIIGillian Lieberman, MD
Companion Images of Nuchal Translucency: image of embryo & 12-week sagittal ultrasound
Thickened Nuchal Translucency

13
Junne Kamihara, HMS IIIGillian Lieberman, MD
Nuchal translucency• Normal subcutaneous fluid-filled space found between
the back of the fetal neck/upper trunk and overlying skin
• Measurements must be made between 10 wks 3 days and 13 wks 6 days
• With maternal age and biochemical markers, can detect Trisomy 21 to 90% with false positive rate of ~1%
• Possible pathophysiology of enlarged NT: abnormalities in extracellular matrix, delayed development of lymphatics, cardiac abnormalities.
Malone FD and D’Alton ME, Obstets and Gynecol 2003, 102:5Estroff JA, Semin Roentgenol. 2004, 39:2

Estroff, JA Semin Roentgenol. 2004, 39:2 14
Junne Kamihara, HMS IIIGillian Lieberman, MD
Differential diagnosis for increased NT
• Trisomy 21• Trisomy 13, trisomy 18• Turner Syndrome (XO)• Triploidy• Structural heart disease• Other anomalies
15
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient JM: Plan for further studies to confirm risk of Down syndrome in fetus
• First-trimester screen positive for Down syndrome, risk of 1 in 5
• Too late for CVS diagnosis- Amniocentesis planned
• Full fetal ultrasound scheduled

16
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient JM: Full fetal Ultrasound demonstrated 3 additional findings in fetus
15 wks 2 days
• Short femur• Echogenic focus in heart • Ventricular septal defect

PACS, BIDMC 17
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Pt JM fetus: Femur length measurement- Anatomic orientation
1
23
Femurs
Landmarks:1 & 2: Inner thighs 3: Posterior
18
Junne Kamihara, HMS IIIGillian Lieberman, MD
Two fetal length measurements were made for our Patient JM fetus as shown in the following
two slides

PACS, BIDMC 19
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Pt JM fetus: Femur length measurement 1- Short for gestational age
Femur length

PACS, BIDMC 20
Junne Kamihara, HMS IIIGillian Lieberman, MD
Femur length
Our Pt JM fetus: Femur length measurement 2- Short for gestational age

21
Junne Kamihara, HMS IIIGillian Lieberman, MD
The second finding in our Patient JM fetus was an Echogenic Intracardic focus (EIF). In Trisomy 21, this is thought to be due to
calcification of the papillary muscle

PACS, BIDMC 22
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Pt JM fetus: 4 chamber view of heart demonstrating echogenic intracardiac focus
Echogenic focus
Landmarks:1: Spine2: Ribs3: Left Atrium4: Left Ventricle
3
21
4

23
Junne Kamihara, HMS IIIGillian Lieberman, MD
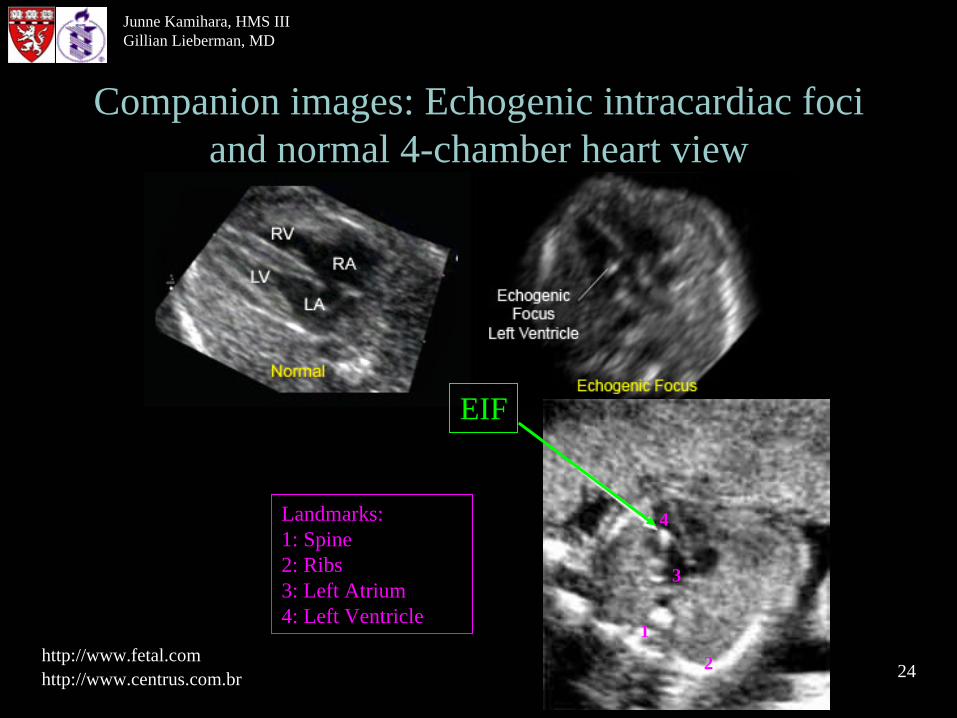
The following companion images show two other examples of echogenic intracardiac foci and a
normal 4-chamber heart for comparison
24
Junne Kamihara, HMS IIIGillian Lieberman, MD
Companion images: Echogenic intracardiac foci and normal 4-chamber heart view
http://www.centrus.com.brhttp://www.fetal.com
EIF
Landmarks:1: Spine2: Ribs3: Left Atrium4: Left Ventricle
1
2
3
4

25
Junne Kamihara, HMS IIIGillian Lieberman, MD
The third finding in our Patient JM fetus was a suspected endocardial cushion defect. No
normal 4-chamber views of the hearts could be obtained

PACS, BIDMC 26
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Pt JM fetus: 4-chamber views of the heart demonstrate a probable endocardial cushion defect
Ventricular septal defect

27
Junne Kamihara, HMS IIIGillian Lieberman, MD
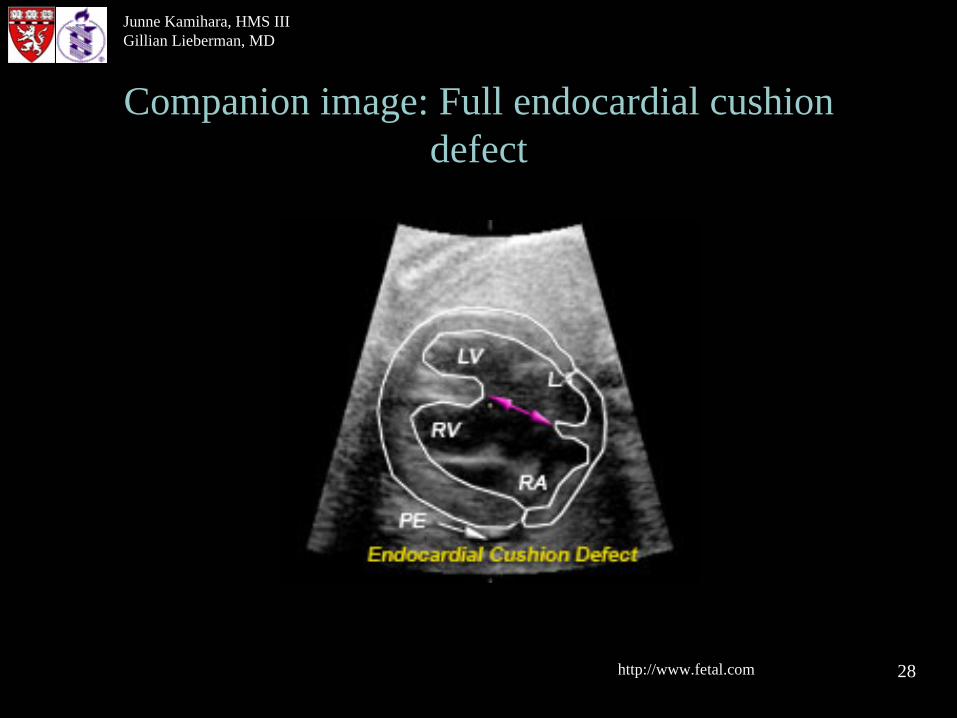
The following companion image shows an example outlining a full endocardial cushion
defect
http://www.fetal.com 28
Junne Kamihara, HMS IIIGillian Lieberman, MD
Companion image: Full endocardial cushion defect
29
Junne Kamihara, HMS IIIGillian Lieberman, MD
Differential diagnosis for each finding
Short Femur: Nonlethal osteogenesis imperfecta, Diabetic embryopathy, trisomy 21, fetal hypoplasia- unusual facies syndrome, ethnic variation
Echogenic intracardiac focus: Fetal cardiac tumors, endocardial fibroelastosis, trisomy 21, trisomy 13
Ventricular septal defect: Trisomy 21, trisomy 13, trisomy 18, prematurity, other chromosomal abnormalities and syndromes
http://www.acsu.buffalo.eduReeder and Felson’s Gamuts in Radiology, 3rd ed.

30
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient JM: Summary of findings
• Amniocentesis performed and confirmed Trisomy 21 in fetus
• Pt. elected to have pregnancy termination
• U/S 12 wks 4 d: Thickened NT in fetus• U/S 15 wks 3 d: Short femur, echogenic
intracardiac focus, probable endocardial cushion defect in fetus
31
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient 2: LG 16 weeks 6 days
• 40 yo who is 16 weeks 6 days pregnant and otherwise healthy
• Presents for full fetal ultrasound and amniocentesis
32
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Patient LG: Full fetal ultrasound demonstrated 2 significant findings in fetus
16 wks 6 days
• Echogenic bowel• Short femur

33
Junne Kamihara, HMS IIIGillian Lieberman, MD
The following image demonstrates the echogenic bowel seen in our Pt LG fetus. Note the echogenicity of bowel compared to bone

PACS, BIDMC 34
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Pt LG fetus: Sagittal ultrasound demonstrating Echogenic bowel
Spine
Echogenic bowel

35
Junne Kamihara, HMS IIIGillian Lieberman, MD
The second finding for our Pt LG fetus was a short femur, shown on the next slide

PACS, BIDMC 36
Junne Kamihara, HMS IIIGillian Lieberman, MD
Our Pt LG fetus: Short femur
Short femur

37
Junne Kamihara, HMS IIIGillian Lieberman, MD
Differential Diagnosis for each finding
Echogenic Bowel: Normal variant, Trisomy 21, Meconium ileus (cystic fibrosis), CMV infection
Short Femur: Nonlethal osteogenesis imperfecta, Diabetic embryopathy, Trisomy 21, fetal hypoplasia-unusual facies syndrome, ethnic variation
Sickler GK et. al. J Ultrasound Med 1998, 17Reeder and Felson’s Gamuts in Radiology, 3rd ed.

38
Junne Kamihara, HMS IIIGillian Lieberman, MD
• U/S 16 wks 6 d: Short femur, echogenic bowel in fetus
• Amniocentesis performed and confirmed Trisomy 21 in fetus
Our Patient LG: summary
• Pt. elected to have pregnancy termination at 19 wks
Sickler GK et. al. J Ultrasound med 1998 39
Junne Kamihara, HMS IIIGillian Lieberman, MD
Pathology report from our Pt LG fetus included findings of GI tract with calcifications and small
ventricular septal defect. Note that one hypothesis for echogenic bowel in Trisomy 21 includes calcified meconium due to
hypomotility of bowel leading to increased water absorption, thickening, and subsequent calcification. Also note that ventricular septal defect was not seen
in ultrasound performed earlier.

40
Junne Kamihara, HMS IIIGillian Lieberman, MD
• Sonographic markers, e.g. shortened femur, echogenic intracardiac focus, and echogenic bowel can be normal variants but also seen frequently in Trisomy 21 fetuses.
• Thickened nuchal translucency, (10-14 wks), when combined with maternal age and biochemical markers, can detect Trisomy 21 to 90%.
Main Summary
• Structural anomalies, e.g. endocardial cushion defects, found in less than 20% of fetuses with Trisomy 21, may be seen in the full fetal scan.

41
Junne Kamihara, HMS IIIGillian Lieberman, MD
References• Estroff JA. Prenatal Diagnosis and Imaging of Genetic Syndromes, Seminars in Roentgenology
2004; 39: 323-335.• Malone FD, D’Alton MR. First-Trimester Sonographic Screening for own Syndrome, Obstet
Gynecol. 2003; 102: 1066-1079.• Mueller RF, Young ID. Emery’s Elements of Medical Genetics 1995 Pearson Professional Ltd. New
York.• Nyberg DA, Souter VL. Sonographic Markers of Fetal Trisomies: Second Trimester, J Ultrasound in
Medicine 2001; 20:655-674.• Oh KY, Frias AE, Byrne JLB, Kennedy AM. Isolated short femur-what does this mean? 16th World
Congress on Ultrasound in Obstetrics and Gynecology, poster abstract P02.12. Ultrasound in Obstetrics and Gynecology 2006; 28: 525.
• Reeder MM, Bradley WG. Reeder and Felson’s Gamuts in Radiology: Comprehensive Lists of Roenten Differential Diagnosis, 3rd ed. 1993 Springer-Verlag Telos, New York.
• Sadler TW. Langman’s Medical Embryology, 7th ed. 1995 Williams and Wilkins, Baltimore.• Shinmoto HS, Kashima K, et. al. MR Imaging of Non-CNS Fetal Abnormalities: A Pictorial Essay,
Radiographics 2000; 20:1227-1243.• Sickler GK, Vang R, Maklad N. Echogenic Fetal Bowel and Calcified Meconium in a Fetus with
Trisomy 21, J Ultrasound Med 1998; 17: 591-593.• http://www.acsu.buffalo.edu/~brodger/foci.doc• http://www.biotechnologyonline.gov.au/popups/img_trisomy21.cfm• http://www.centrus.com.br/DiplomaFMF/SeriesFMF/11-14weeks/chapter-01/chapter-01-final.htm• http://familymed.uthscsa.edu/residency/maternityguide/ultrasound.htm• http://www.mums.me.uk/nuchal.htm• http://utdol.com/utd/content/topic.do?topicKey=dis_chld/13798

42
Junne Kamihara, HMS IIIGillian Lieberman, MD
Acknowledgements
• Shambhavi Venkataraman, MD• David Graham, MD• Maryellen Sun, MD• Gillian Lieberman, MD• Larry Barbaras• Pamela Lepkowski