imaging abdomen trauma introduction part 1 dr ahmed esawy
TRANSCRIPT


An Article By
Dr. Ahmed Esawy
MBBS M.Sc MD


Trauma to the abdomen
accounts for approximately 10% of the
traumatic deaths. Prompt recognition and
management of bleeding from intra-
abdominal organs is essential to
minimize morbidity and mortality from
trauma itself as well as minimizing the
need of surgical interference with
probable its complications.
Classification of Abdominal Trauma:
A. Blunt Abdominal Trauma (BAT):
- Compression or concussive forces (direct blows)
- Deceleration forces
• B. Penetrating Abdominal Trauma (PAT):
- High-velocity injuries (gunshots)
- Low-velocity penetrating injury (stab wounds)

Imaging Techniques:
1- Initial imaging:-
- FAST
- Plain X-ray
2- CT
3-conventional Angiography
4- MRI
5- Isotope Scan

The primary role of CT is to assess
the severity of abdominal injuries
in order to help the trauma
surgeon to decide if emergent
surgery is necessary.
Therefore, if surgery is mandatory
due to the severity of the
abdominal trauma, then CT is
generally avoided.

IN INTERPRETING CT FOR
PATIENTS WITH
ABDOMINAL TRAUMA, WE
HAVE TO SCREEN FOR

1) Pneumothorax and pneumoperitoneum using
lung windows for lower thorax and upper abdominal sections
and soft tissue windows for lower abdominal and pelvic
sections;
(2) left paracolic gutter
and spleen for blood
or laceration

(3) right paracolic
gutter and liver, for
blood or laceration

(4) upper abdominal
survey evaluating
duodenum and pancreas

(5) Retroperitoneal survey of
kidneys, adrenals, IVC and
aorta for evidence of
bleeding, laceration,
hematoma, urinoma

(6) GI tract and
mesentery for
extravasation or
hematoma
(7) muscle survey including
psoas,
iliopsoas,
rectus abdominus
and buttocks for hematoma

(8) bone survey including
ribs,transverse processes, sacrum, and
SI joints
and hips
for fracture
(9) lowest section search for groin
hematoma

BAT
FAST
Positive FAST Negative FAST
Stable Patient Unstable Patient Stable Patient Unstable Patient
CT Laparotomy Repeat FAST after 6 hrs Identify other cause
APPROACH FOR ABDOMINAL
TRAUMA

Abdominal Trauma Protocol
• Blunt injury -deceleration, crush, weapon
(e.g. bat)
– venous phase ~70 secs
– Delayed scan if injury present; ~3-5 mins
• Penetrating injury: knives, gun
– Same as blunt
– Additional scan after rectal contrast material

• The findings to look for in abdominal trauma are the following:
– Hemoperitoneum
– Pneumoperitoneum
– Contrast blush consistent with active extravasation
– Subcapsular hematomas
– Laceration
– Contusions
– Devascularization of organs or parts of organs


Active bleeding
The CT appearance of
intraperitoneal blood
depends on the age
and physical state of
the clot.

IMMEDIATELY AFTER
HEMORRHAGE,
INTRAPERITONEAL BLOOD
HAS THE SAME
ATTENUATION AS
CIRCULATING BLOOD OF
20-30 HU

Active bleeding
However, attenuation values less than 20 HU are
a frequent finding in the acute setting. The
proposed reason for this is that blood, being
a strong peritoneal irritant, causes a local
inflammatory response with transudation of
fluid across the peritoneum. Transudate fluid
mixes with and dilutes the blood before
coagulation begins, decreasing the attenuation.

Active bleeding
Within hours, a clot forms and attenuation increases as hemoglobin concentrates, and values in the range of 50-75 HU are seen. Densely clotted blood may have attenuation values upwards of 100 HU.
Clot lysis begins within 48-72 hours, and attenuation decreases to fluid values.
After a few weeks, most hematomas have attenuation values approaching those of water,
namely, 0-20 HU.

Active bleeding
In reality, hemoperitoneum can have a complex
appearance as a result of recurrent
hemorrhage and irregular resorption. Blood
may exist in many different stages at the time
of imaging if hemorrhage has been intermittent.
Fresh blood
confined to a localized space or that has been
relatively undisturbed may separate,with
plasma layered on top of precipitated red blood
cells causing the hematocrit effect.

Quantification of hemoperitoneum
Huang and associates scoring systems
• Total Score ranging from 0 to 8
• One point was assigned to each anatomic
site in which free fluid was detected during
the FAST scan
• Fluid of more than 2 mm in depth in the
hepatorenal or the splenorenal space was
given 2 points instead of 1
• Floating loops of bowel were given 1 point
• Scores > 3 required exploratory laparotomy

Approximately
• FAST can detect between 100-250ml
0.5 cm in Morison's Pouch = 500ml
1 cm in Morison's Pouch = 1000ml
CT can detect volumes of free fluid as
low as 100ml

Volume
• Detection of fluid in each paracolic
gutter indicates that at least 200 ml of
blood must be present in each gutter.
• CT visualization of blood in the
abdomen and pelvis corresponds with
the amounts of more than 500 ml.

Hemoperitoneum Hyperdense intraperitoneal fluid collection
0–20HU
Preexisting ascites
Bile
Urine
Digestive fluid
Diluted (acute blood) or old blood
30–45HU Free Unclotted intraperitoneal blood
45–70HU Clotted blood/sentinel clot sign hematoma
>100 HU Extravasation of contrast medium
(vascular or urinary)
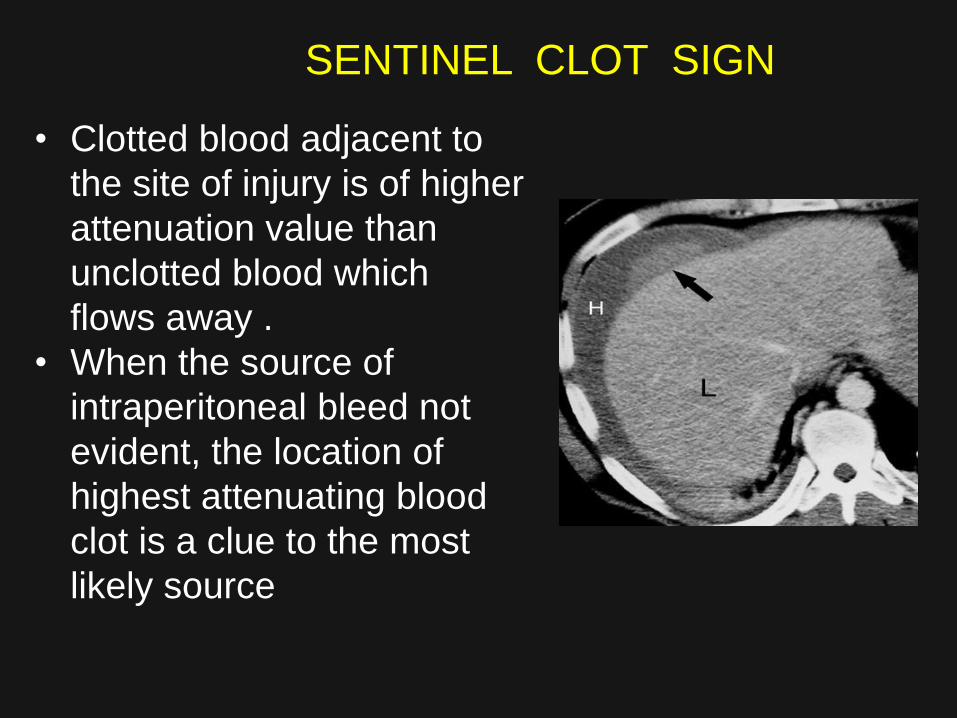
SENTINEL CLOT SIGN
• Clotted blood adjacent to
the site of injury is of higher
attenuation value than
unclotted blood which
flows away .
• When the source of
intraperitoneal bleed not
evident, the location of
highest attenuating blood
clot is a clue to the most
likely source

Ascites – Radiographic findings
• Obliteration of inferior edge of liver
• Widening of distance b/n flank stripe &asding colon
• AF b/n liver & lateral abd wall may result in visualization of a lucent band –Hellmer’s sign
• Dog ear sign or ‘Mickey mouse ears’ sign(100-
150ml)- fluid density lateral to rectal gas shadows.
• Separation and floating of bowel loops
• Bulging properitoneal flank stripe
• Poor definition of major abd. organs and psoas
• Overall abdominal haziness

Retroperitoneal Hemorrhage
• Retroperitoneal hemorrhage may
arise from injuries to major vascular
structures, hollow viscera, solid
organs, or musculoskeletal
structures or a combination
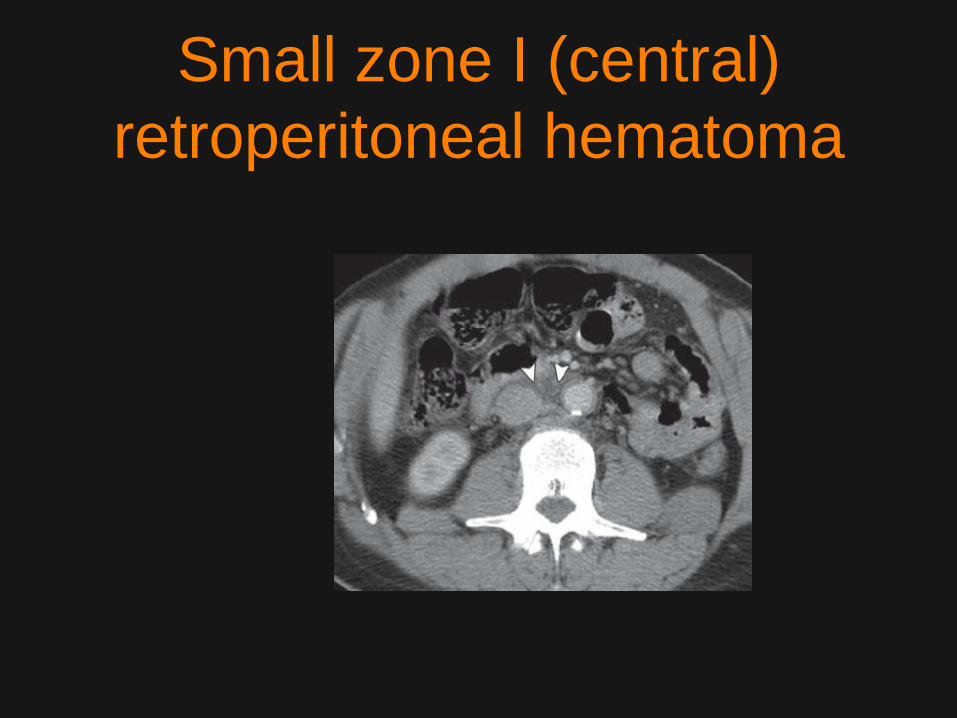
Small zone I (central)
retroperitoneal hematoma

Large zone I (central)
retroperitoneal hematoma with
active extravasation

Large zone II (lateral)
retroperitoneal hematoma

The CT appearance of intraperitoneal blood depends on the age and physical state of
the clot.
Active bleeding

IMMEDIATELY AFTER HEMORRHAGE,
INTRAPERITONEAL BLOOD HAS THE SAME
ATTENUATION AS CIRCULATING BLOOD OF
20-30 HU

However, attenuation values less than 20 HU
are a frequent finding in the acute setting. The
proposed reason for this is that blood, being
a strong peritoneal irritant, causes a local
inflammatory response with transudation of
fluid across the peritoneum. Transudate fluid
mixes with and dilutes the blood before
coagulation begins, decreasing the
attenuation.
Active bleeding

Within hours, a clot forms and attenuation increases as hemoglobin concentrates, and values in the range of 50-75 HU are seen. Densely clotted blood may have attenuation values upwards of 100 HU.
Clot lysis begins within 48-72 hours, and attenuation decreases to fluid values.
After a few weeks, most hematomas have attenuation values approaching those of water,
namely, 0-20 HU.
Active bleeding
In reality, hemoperitoneum can have a complex appearance as a result of recurrent hemorrhage and irregular resorption. Blood may exist in many different stages at the time of imaging if hemorrhage has been intermittent. Fresh blood
confined to a localized space or that has been relatively undisturbed may separate,with plasma layered on top of precipitated red blood cells causing the hematocrit effect.
Active bleeding

CT findings of shock
• Collapse of inferior vena cava
• Small aorta
• Persistent nephrogram without excretion
• Hypodense spleen, without enhancement and
normal vascular pedicle
• Increased enhancement of the small bowel wall
• Increased enhancement of the adrenal glands
• Sometimes findings of right cardiac insufficiency
with reflux into the hepatic veins

PNEUMOPERITONEUM
• FREE AIR SENSITIVITY OF IMAGING
STUDIES – COMPUTED TOMOGRAPHY- 99%
– AP UPRIGHT CHEST RADIOGRAPH - 76%
– LEFT DECUBITUS ABDOMEN RADIOGRAPH 80 -90%
– SUPINE ABDOMEN RADIOGRAPH - 56%

Signs of a pneumoperitoneum on the supine
radiograph
Right upper quadrant gas
Perihepatic
Subhepatic
Morrison’s pouch
Fissure for the ligamentum teres
Rigler’s (double wall) sign
Ligament visualization
Falciform (ligamentum teres)
Umbilical (inverted V sign) medial and lateral
Urachus
Triangular air
The cupola sign
Football or air dome
Scrotal air (in children)

SOLID ORGAN INJURY

Solid organ injury includes:
- liver, spleen and kidneys.
- Injury of the urinary bladder.
- Bowel and mesenteric injury.
- Pancreatic injury.
-Injury to the abdominal aorta.
- Diaphragmatic rupture.
- Pelvic trauma.

On CT, it is usually seen in a lenticular configuration. Sub-capsular hematomas cause direct compression and deformity of the shape of the underlying solid organs. On non-enhanced CT scans, the solid organs appear hypo-attenuating compared with a sub-capsular hematoma. On enhanced CT scans, a sub-capsular hematoma appears as a low-attenuating lenticular collection between the capsule and the enhancing parenchyma of the injured organ. Unless bleeding recurs, attenuation of the sub-capsular hematoma decreases with time. Sub-capsular hematomas resolve within 6-8 weeks
Subcapsular hematoma

On enhanced CT, laceration appears as a non-enhancing linear or branching structure, usually at periphery. Acute lacerations have a sharp or jagged margin, but with time, lacerations may enlarge, and the margins may develop rolled edges. Multiple parallel lacerations occur as result of compressive forces (bear claw lacerations).
Lacerations:

contusions are perceived as ill-defined
or sometimes sharply marginated
areas of reduced enhancement and
excretion

On enhanced CT, acute hematomas appear as irregular high-attenuation areas,which represent clotted blood, surrounded by low-attenuating unclotted blood. Over time, the attenuation of the hematoma is reduced, and the hematoma eventually forms a well-defined serous fluid collection that may expand slightly. A focal intraparenchymal hyper attenuating area with attenuation of 80-350 HU may represent an
active hemorrhage or pseudo-aneurysm. .
Intra-parenchymal hematomas