dr ahmed esawy 5 bowel imaging acute bowel ischemia abi
TRANSCRIPT


An Article By
Dr. Ahmed Abdullah
Esawy

Acute Mesenteric
Ischemia
ABI ACUTE BOWEL ISCHEMIA
Mesenteric ischemia is a medical condition in which inflammation and injury of the small intestine

occlusive Causes
Arterial occlusion
venous occlusion
Thromboembolism
Vasculitis

Bowel Obstruction
Decreased cardiac output (from
any cause, ncluding primary cardiac disease,
infarction, arrhythmia, and hypovolemia)
Neoplasms
Abdominal Inflammatory Conditions
Trauma
Blood disease
Drugs (Chemotherapy)
Radiation
Corrosive

Unfortunately, common CT findings in bowel ischemia are not specific
specific findings are rather uncommon.
Therefore, it often is a combination of nonspecific clinical, laboratory, and radiologic findings—especially detailed knowledge about the pathogenesis of acute bowel ischemia in different conditions—that helps most in correct interpretation of CT findings.

Role of
Plain x- ray
In ABI/AMI

PLAIN ABDOMINAL FILMS
Normal
Air distribution (intramural gas
Extraluminal air)
focally thickened bowel
adynamic ileus
small bowel obstruction
abscess

Air in L. bowel
NO
Distended loops
Localized ileus
few
Generalized ileus
multiple
Air in S. bowel
LBO SBO
Decompressed LBO
Air in the rectum
Yes


SUPINE VIEW UPRIGHT VIEW
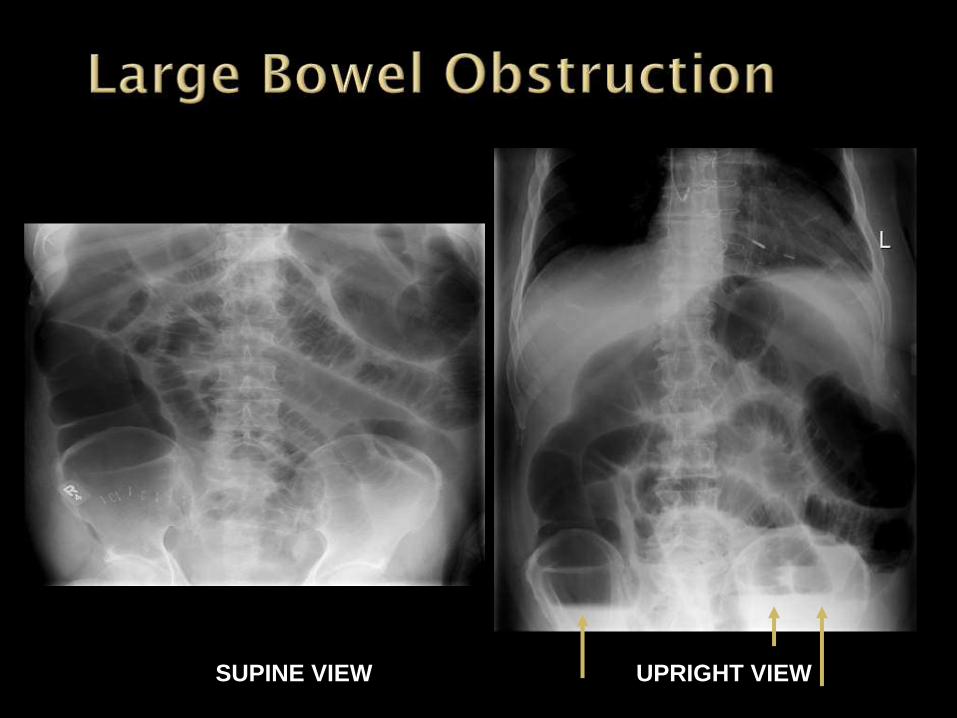
SUPINE VIEW UPRIGHT VIEW

LBO decompressed into SB

Extra-luminal air

a.Crescent sign :air beneath the diaphragm
b.Falciform ligament sign: air delineating the falciform ligament
c. Football sign: A large air collection beneath that does not conform to any bowel loop
d.Rigler's sign: If both the serosal and the related mucosal walls of the bowel are delineated it means free air is at that serosal surface

Falciform
Ligament
Sign
Football sign
Free intra-peritoneal air
Air on both sides of bowel wall –
Rigler’s Sign


1. Differentiation between mechanical
obstruction and paralytic ileus.
2- . Differentiation between small and
large bowel obstruction
3-Diagnosis of perforated viscus

ROLE OF
BARIUM ENEMA
In ABI/AMI


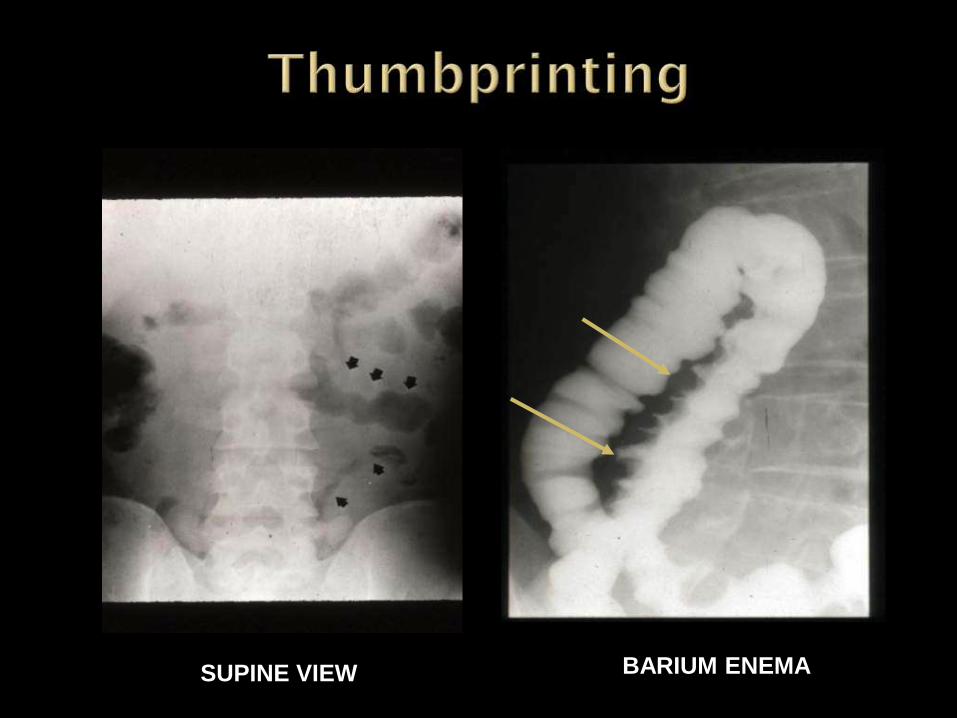
SUPINE VIEW BARIUM ENEMA

C T Computerized tomography
In ABI/AMI

low attenuation (thrombosis) in the SMV,
thickening of the small bowel wall
presence of peritoneal fluid

thrombosis of mesenteric arteries or veins circumferential or nodular thickening dilatation of the bowel lumen pneumatosis intestinalis poor enhancement of the bowel wall along its
mesenteric border, which is evidence of ischemia;
ascites, which is commonly present . mesenteric fat stranding, mesenteric fluid, and/or ascites adynamic ileus pleural effusion mesenteric/portal venous gas peritonitis

-intussception
-small bowel obstruction causes
-hernia

The most common manifestation of accompanying bowel ischemia is bowel wall thickening

more specific signs of ischemic bowel disease
bowel dilatation
intestinal pneumatosis

mesenteric or portal venous gas
Free intraperitoneal air

a filling defect within the proximal SMA (arrow) as well as a wedge-shaped infarct in the right kidney, compatible with prior embolic disease.

thickening of small bowel loops (short arrow) and mesenteric edema (long arrow) from venous occlusion.

White attenuation
thickened bowel wall that is equal to or
greater than that of venous
opacification in the same scan
The white pattern

The lower attenuation layer of the water halo sign is believed to represent edema
Water halo sign
water halo sign

equivalent of pneumatosis
Black attenuation
Black attenuation

SMV thrombus with infarction.
extraluminal free air •pneumatosis of the cecum (short arrow), with linear gas extending into the mesenteric veins (long arrow).
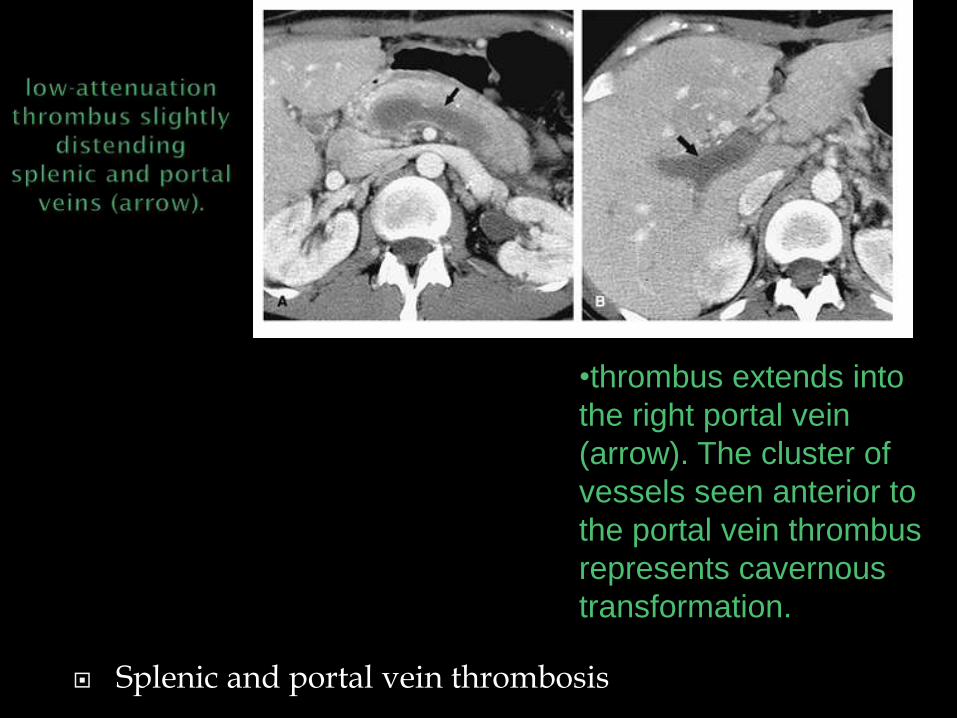
Splenic and portal vein thrombosis
•thrombus extends into
the right portal vein
(arrow). The cluster of
vessels seen anterior to
the portal vein thrombus
represents cavernous
transformation.

Chronic portal vein occlusion with cavernous transformation.
a tangle of collateral veins in seen
in the porta hepatis (arrow).


Small and large bowel ischemia on CT. Note the dilated and thick-walled loops of small bowel (S) and large bowel (L) with associated low-density submucosal edema, creating the "target sign." A large amount of pelvic free fluid (F) is also present.

several infarcted small-bowel loops (arrows), which manifest with dilatation and air-fluid levels
large cholesterol embolus (arrows) in the superior mesenteric artery, confirmed at surgery, which caused acute mesenteric infarction.

Stent can be seen in an infrarenal aortic aneurysm (arrows). The stent caused occlusion of the inferior mesenteric artery and subsequent ischemia of the sigmoid colon.
No c
Note moderate wall thickening of sigmoid colon (arrows), which has undergone transmural infarction.

pneumatosis (arrowheads) along the left-sided colon, due to transmural colonic infarction.
No c
•The patient had low cardiac output, but the wrong position of the intraaortic balloon (arrow), occluded the IMA

mesenteric venous infarction with massive small-bowel wall thickening (arrows)total absence of bowel wall enhancement, pronounced edema of mesenteric fat (arrowheads), ascites
c
patient with polycythemia vera who developed multiple thromboses of distal and intramural mesenteric veins.

pronounced homogeneous cecal wall thickening (arrows), representing transmural necrosis with superinfection in a patient with isolated cecal infarction.
No c

widely dilated colon with mildly thickened colonic wall, mesenteric gas, and mixed bubblelike (arrowheads) and bandlike (arrows) pneumatosis.
c occlusive transmural colonic infarction

massive circumferential and bandlike pneumatosis (arrows) of multiple necrotic loops and pronounced edema of mesenteric fat.
No c embolic transmural
small-bowel infarction

mesenteric venous gas with an air-contrast material level in the superior mesenteric vein (arrow). The infarcted small bowel shows minimal pneumatosis (arrowhead) but no wall thickening.
c embolic transmural small-bowel infarction

pronounced intrahepatic portal venous gas (branching hypoattenuating areas) extending into the periphery of both liver lobes.
c acute transmural mesenteric infarction

herniation of stool-filled, thin-walled colon (arrow) through a narrow abdominal wall defect. The patient was asymptomatic but presented with acute abdomen 1 month later.
c
Incarcerated
hernia
•multiple ventral hernias (arrowheads). The sac of the hernia shown in a now contains extraluminal fluid and fluid-filled, mildly thickened colon and causes colonic obstruction. Incarceration with colonic obstruction was confirmed at surgery.
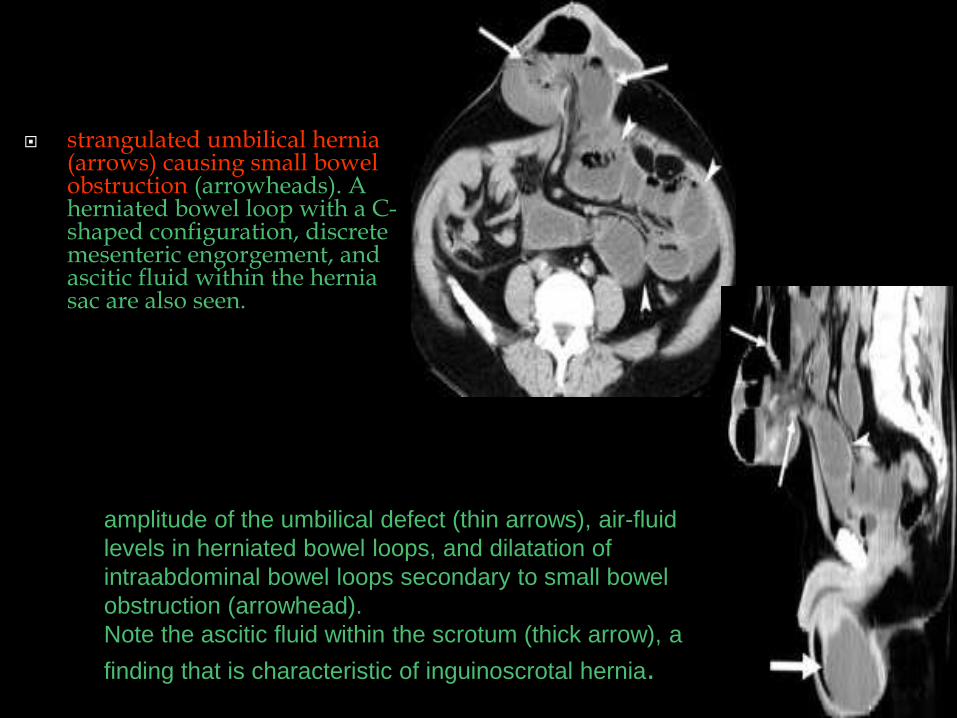
strangulated umbilical hernia (arrows) causing small bowel obstruction (arrowheads). A herniated bowel loop with a C-shaped configuration, discrete mesenteric engorgement, and ascitic fluid within the hernia sac are also seen.
amplitude of the umbilical defect (thin arrows), air-fluid
levels in herniated bowel loops, and dilatation of
intraabdominal bowel loops secondary to small bowel
obstruction (arrowhead).
Note the ascitic fluid within the scrotum (thick arrow), a
finding that is characteristic of inguinoscrotal hernia.

Spiral CT and rapid bolus injection of CM
Multidetector row CT provides more detailed information. 3D volume rendering and MIP imaging.

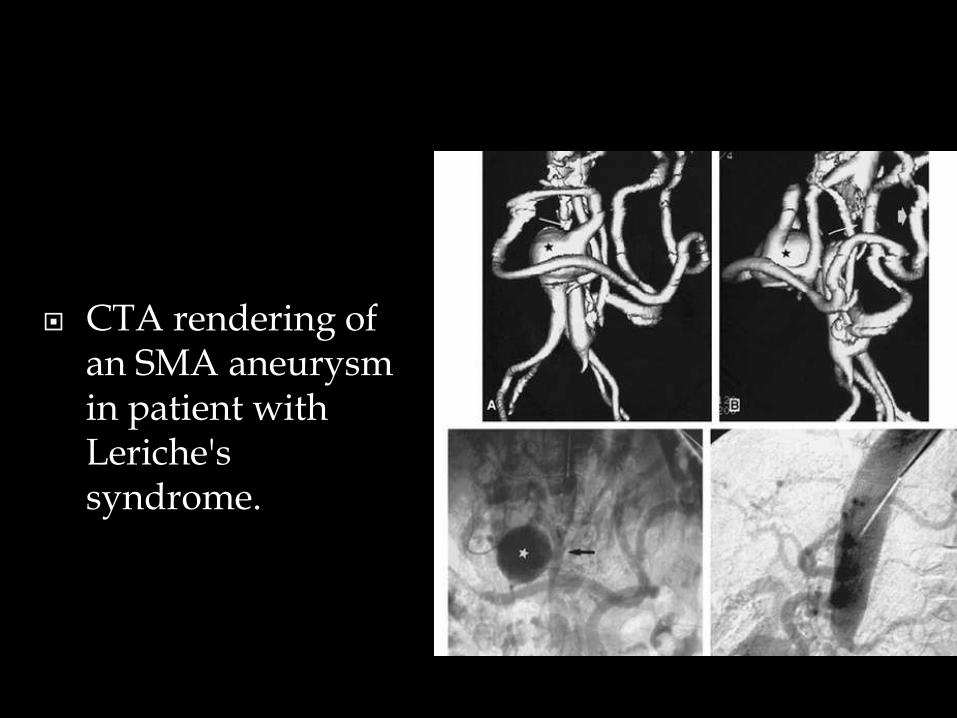
CTA rendering of an SMA aneurysm in patient with Leriche's syndrome.

Celiac artery aneurysms. Reformatted MRA images demonstrate aneurysms of the proximal celiac artery in three different patients (white arrows in A–C).

SMA dissection. Localized dissection of the SMA on CPR and VR images. A: Coronal CPR of SMA demonstrating intimal flap from dissection (short arrow) and aneurysmal dilatation of false lumen (long arrow). B: Lateral CPR revealing entry point into false lumen (arrow). VR image (C) demonstrates dilated false lumen (arrow).

Portomesenteric venous thrombosis
Portomesenteric venous thrombosis
enlarged portal vein
enlarged splenic vein
SMV
portovenous confluence (black
arrow)
with evidence of small-vessel
collateralization (white arrow).

Portomesenteric venous thrombosis
absence of flow in the splenic vein (black arrow) and
within the portovenous confluence (white arrow).
filling defects in the portal vein (arrow) with
cavernous transformation at the porta hepatis
thrombus in the SMV (white arrow). Prominence
of the pancreatic head (black arrows) and several
peripancreatic lymph nodes (arrowheads)
haziness of the
adjacent fat (arrow).


Portomesenteric venous thrombosis
obliteration of the SMV
(arrowhead) and proximal
portal vein near the
confluence. Diffuse tumor
infiltration along the aorta is
also present.

Bowel dilatation in a 54-year-old woman with mesenteric venous thrombosis. CT image shows multiple loops of distended, fluid-filled small intestine (B) secondary to SMV thrombosis (arrowhead). There is no pneumatosis or free intraperitoneal air. Trace ascites is also present (arrow).

Intestinal pneumatosis air along the course of the SMV (arrowhead), and pneumatosis is
present (arrow) within the wall of the distal ileum, ascending colon, and transverse colon. Extensive portal venous gas was also noted. At laparotomy, no large vascular (arterial or venous) clot was identified; therefore, thromboembolic disease at a microvascular level was suspected to be the likely cause.


MRI

pancreatic cancer encasing SMA
demonstrates both soft tissue encasement of the SMA (arrow) and the bland thrombus (arrowhead) within the SMV.

Time of Flight MRA
PC MRA
2D ECG gated cine PC MRA
Systolic-gated 3D PC MRA
3D Gd-enhanced MRA

Portomesenteric venous thrombosis
nonocclusive
thrombus at the
splenoportal venous
confluence (arrow).
nonocclusive thrombus
in the SMV (arrow).
the SMV thrombus (arrow).

Portomesenteric venous thrombosis
large heterogeneous mass (M) in
the lower pole of the right kidney,
consistent with renal cell carcinoma.
A filling defect is seen in the SMV
(arrow
long thrombus in the SMV
(arrows) that extends into the
portal vein
proximal extent of
the clot in the portal
vein (arrows).
thrombus that involves
the inferior vena cava
(arrow

long thrombus in the
SMV (arrows) that
extends into the
portal vein (PV).
superior extent of the
filling defect (solid arrow)
in the portal vein (PV).
The filling defect in the
SMV is not visualized due
to absence of flow, but the
inferior mesenteric vein is
seen (open arrows). The
hepatic vein (HV) and
splenic vein (SV) are well
visualized
The thrombus in
the proximal
portal vein (PV) is
seen (arrow).

ANGIOGRAPHY

Angiogram of the celiac trunk, showing absence of the common hepatic artery. The gastroduodenal artery arises directly from the bifurcation of the celiac trunk. The proper hepatic artery divides into the right and left hepatic arteries