3/6/2015 - c.ymcdn.comc.ymcdn.com/sites/ · pdf file3/6/2015 1 exploring the tall tales of...
TRANSCRIPT

3/6/2015
1
Exploring the Tall Tales of Nutrition in the ICULori A. Duesing, MSN, RN, CPNP-AC, APNP
Financial Disclosures
▪ None related to this topic
Objectives
▪ Explain the relationship between nutrition and improved outcomes in the critically ill patient
▪ Understand terminology of relevant gastroenterology disease processes
▪ Recognize situations in which nutrition should be utilized in the critically ill patient▪ Recognize situations in which nutrition should be utilized in the critically ill patient
#1 Myth: Starvation or Under-nutrition is Ok!
▪ Nutrition is essential for survival.
▪ Supports anabolism
▪ Ameliorates uncontrolled catabolism
▪ Maintains a competent immune systemMaintains a competent immune system
▪ Bottom line … nutrition if given at the right time by the right route, will improve patient outcomes
Calorie Intake to meet the needs of ICU patients remains unclearMeta analysis including 4 studies showed:• No significant difference in mortality between under- and full fed group• Subgroup analysis showed underfed group significantly lower mortality when fed >33.3% of
standard requirement in comparison to the full-fed group• No difference in mortality between underfed group fed <33.3% of standard caloric
requirements• LOS and LOICUS did not differ
Indirect calorimetry and predictive equations:• 2349 publications retried, with 18 studies included• Predictive equations underestimated and overestimated energy expenditure in
13-90% and 0-88%, respectively• 43% below and 66% above indirect calorimetry values observed

3/6/2015
2
The latin phrase primum non nocere, translated to “first, do no harm” serves as a reminder to clinicians that good intentions may have harmful consequences. • Use of inaccurate predictive estimates for support of the critically ill• patient combined with aggressive therapy to achieve target nutrition intakes without
consideration of potential consequences of this therapy may have harmful consequences
• Each patient needs to be evaluated closely for signs and symptoms of overfeeding and feeding intolerance
Consensus
▪ Generalized belief that optimal calorie and protein intake are associated with improved patient outcomes
▪ Severity of illness is a variable = less sick patients tolerate EN
▪ Despite these limitations the Society of Critical Care Medicine American Society▪ Despite these limitations, the Society of Critical Care Medicine, American Society of Parenteral and Enteral Nutrition guidelines, and Canadian and European guidelines all recommend
▪ EN be initiated within 48 hours in the critically ill patient who is unable to maintain volitional intake.
▪ There is no known illness or disease that benefits from starvation
“Bowel rest”
▪ Popular in the 1970s for Crohn’s, colitis, acute and chronic pancreatitis, diverticulitis and a number of other GI disorders
▪ Why?
▪ Enteral nutrition (EN) enhances inflammation( )
▪ Removal the stimulus of luminal antigens and bowel function
▪ Contrary:
▪ Starvation does not inhibit bowel function
▪ Starvation decreases splanchnic blood flow resulting in profound structural and functional changes to the GI tract
The splanchnic circulation. Gelman S, Mushlin PS: Catecholamine induced changes in the splanchnic circulation affecting systemic hemodynamics. Anesthesiology 100:434–439, 2004.)
Characteristics of Splanchnic blood flow
▪ Regulates circulating blood volume and systemic blood pressure
▪ In acute hypovolemia, such as hemorrhage, splanchnic circulation is reduced to supply blood and oxygen to vital or essential organs = brain and heart.
▪ A key source of inflammatory mediators▪ A key source of inflammatory mediators
Regulators
Intrinsic
▪ Local metabolic & myogenic control
▪ Blood flow: Vasodilators/vasoconstrictors
Extrinsic
▪ Sympathetic innervations
▪ Increases vascular resistance to decrease blood flow
▪ Local reflexes
▪ Locally produced vasoactive substances
▪ Circulatory vasoactive substances
▪ Systemic hemodynamic changes

3/6/2015
3
#2 Myth: Parenteral Nutrition is Safe!
▪ If the gut works, use it!
▪ Parenteral nutrition (PN) prevents progressive malnutrition in patients unable to feed enterally
▪ Widely accepted to use the GI tract as a preferred route in delivering nutritional▪ Widely accepted to use the GI tract as a preferred route in delivering nutritional support.
▪ Strongly recommended in critically ill and postoperative patients
▪ Although widely accepted, parenteral nutrition is still used in patients who can be fed enterally
Adverse effects of Parenteral Nutrition▪ Double hit if you are not feeding the gut and using PN
▪ Metabolic, immunologic, endocrine and infective complications associated with high glucose concentration and fat globules via the systemic venous system.
▪ PN bypasses the GI tract and liver
▪ EN stimulates enterohormones which are crucial in regulating gut function and metabolic pathways
▪ EN supplies the portal system supplying the liver with a rich source of nutrients and hormones
▪ Increased risk for GI mucosal atrophy, bacterial overgrowth and translocation, increased intestinal permeability
▪ PN is associated with impaired leukocyte chemotaxis, impaired phagocytosis, impaired bacterial and fungal killing and an attenuated inflammatory response
4696 abstracts with 406 articles included:• PNAC directly correlated with length of PN use• No decrease in the past 4 decades• Multidisciplinary teams to treat PNAC/IFALD show improved outcomes• Discussion regarding Omegavan and SMOF to improve outlines
26 Randomized trials of 2211 patients:• PN + oral and IV dextrose = no difference in mortality• PN alone = risk of mortality doubled
#3 Myth: EN is Contraindicated with Vasopressors!
▪ Hemodynamically unstable and/or require vasopressors = common in the ICU
▪ Vasopressors improve hemodynamics as they shunt blood from the gut to the central circulation
▪ Feeding during these times?▪ Feeding during these times?
▪ No, if limited oxygen delivery to the gut, why would you increase oxygen demand by feeding?
▪ Will cause bowel ischemia NCP• In animal models, mesenteric and renal blood flows improved with low dose
enteral nutrition while receiving low dose vasopressin• As vasopressin therapy increased, the benefit of enteral nutrition on mesenteric
perfusion was not maintained• To promote splanchnic perfusion with use of enteral nutrition, the authors
advocate for enteral nutrition ~6 hours post fluid resuscitation

3/6/2015
4
In endotoxic and septic shock models, enteral feeding improved• hepatic artery and portal vein blood flow• superior mesenteric artery blood flow• intestinal mucosal microcirculatory flow• hepatic microcirculatory flow• hepatic and intestinal tissue oxygenation, and • hepatic energy stores
Prospective study = 886 ICU mechanically ventilated pts• Optimal nutritional therapy associated with a decrease in 28-day
mortality by 50%• Only reaching energy targets is not associated with a reduction in
mortality.
• Multicenter retrospective study showed lower hospital mortality in patients enterally fed within 48 hours
• EN benefits greater in the sickest receiving multiple vasopressors• Early enteral nutrition vs. late enteral group: 22.5% vs 28.3%; P = 03; and 34.0% vs
44.0%; P < .001, respectively• Early feeding = within 48 hours of the start of mechanical ventilation• Late feeding = Later than 48 hours• Protein/energy needs not reviewed
#4 Myth: Early EN is not Important in Patients Receiving Mechanical Ventilation!
▪ The commencement of enteral nutrition is typically delayed in mechanical ventilated patients
▪ Likely cause? Not a current priority and may be pushed to the back burner
▪ Older guidelines support mechanically ventilated patients go 1 weeks without▪ Older guidelines support mechanically ventilated patients go 1 weeks without nutrition.
▪ Mechanical ventilation is a predictor for failure to provide enteral nutrition
• Early EN within 2 days of admission associated with a significant reduction of ICU and hospital morality
• The implementation of an evidenced-based nutritional management protocol significantly shortened the duration of mechanical ventilation
• EN was associated with reduced risk of death

3/6/2015
5
#5 Myth: EN is Contraindicated with High Gastric Residual Volume!
▪ Many monitor gastric residual volume (GRV)
▪ Enteral nutrition is stopped with elevated GRVs
▪ High GRVs do not necessarily predict aspiration
▪ Low GRVs do not necessarily predict aspiration will not occur
▪ Interrupting EN with GRV 100-200mls not shown to decrease prevalence of aspiration
Speculation for GRVs
May have arisen from beliefs:
▪ #1 the stomach is a container of finite size
▪ #2 when input exceeds output over time, the stomach will “overflow”
▪ #3 overflow into … the esophagus which equals aspiration
▪ If we have knowledge of gastric contents at any given time through GRV we will predict risk of overflow and ultimately prevent aspiration
Implications to the theory of High GRVs
▪ GRVs accurately reflect the total volume in the stomach
▪ Formula retained in the stomach will alert the clinician to delayed gastric emptying equaling impending intolerance
▪ Stop the feeding to prevent vomiting or aspiration from occurring▪ Stop the feeding to prevent vomiting or aspiration from occurring
Implications of low GRVs
▪ Presumed to indicate low intra-gastric volume
▪ The formula is being emptied appropriately
▪ Risk for aspiration with a low GRV expected to be minimal, so the patient is tolerating enteral feedingstolerating enteral feedings
Flaws to rationale
▪ Total salivary and gastric secretion = output up to 1500mls salivary and 3000mls gastric secretions
▪ Aspiration of oropharyngeal secretions
▪ Some degree of aspiration may occur normally in normal healthy individuals
▪ Patient populations vary with regard to risk for aspiration pneumonia, specifically risk for aspiration of gastric contents.
▪ Must consider the specific patient:
▪ Communicative patients with functional GI tract = no benefit
▪ Uncommunicative patients with potential for impaired GI tracts = might benefit
▪ Patients with inability to handle oral secretions = no benefit
Do residual volumes impede nutritional support?
▪ GRVs may lead to clogging of feeding tubes = acid mixed with intact proteins in the tube clotting the formula
▪ Low GRVs may give clinicians false sense of security
▪ Institutional threshold values of GRVs guide the clinician to withhold nutrition▪ Institutional threshold values of GRVs guide the clinician to withhold nutrition

3/6/2015
6
• Randomized ICU ventilated patients
• #1 GRV >200ml
• #2 GRV >400mls• Aspiration prevalence was similar between groups
Tests to evaluate for aspiration
▪ Videofluorographic swallow study = “gold standard” modified barium swallow test looking at 3 phases of swallowing (oral, pharyngeal and esophageal phases)
▪ Fiberoptic Endoscopic Evaluation of Swallowing (FEES)
▪ Scintigraphy▪ Scintigraphy
McClave, et al recommends:
• High-risk patient populations should be identified by their disease process, not solely by GRV
• Trauma, head injury, sedated, altered mental status
• Pertinent physical findings suggesting ileus
• Abdominal distention, nausea, vomiting, or overt aspiration or regurgitationg p g g
• Clinicians should not depend on GRVs to distinguish high risk from low risk
• Obvious trend of increasing GRVs should prompt a clinical pathway or algorithm
• Rather than automatic cessation of enteral feeding, consider:
• Prokinetic agent, depending on age
• Reducing sedation
• Sepsis
• Elevate head of bed
#6 Myth: Post-pyloric Feeding Reduces the Risk of Aspiration!
▪ Many clinicians believe critically ill patients should receive post-pyloric feedings.
▪ Undoubtedly, some ICU patients would not tolerate early gastric feeding due to delayed gastric emptying
▪ Underlying co-morbidities
▪ Medications
▪ Electrolyte disturbances, hyperglycemia
▪ Surgery
▪ Shock
▪ No consensus for routine use of post-pyloric feeding and associated decrease aspiration risk
Meta-analysis. • Unable to demonstrate a clinical benefit from post-pyloric versus gastric tube feeding in a
mixed group of critically ill patients, including medical, neurosurgical, and trauma ICU patients.
• The incidences of pneumonia, ICU LOS, and mortality were similar between groups.
3/6/2015
7
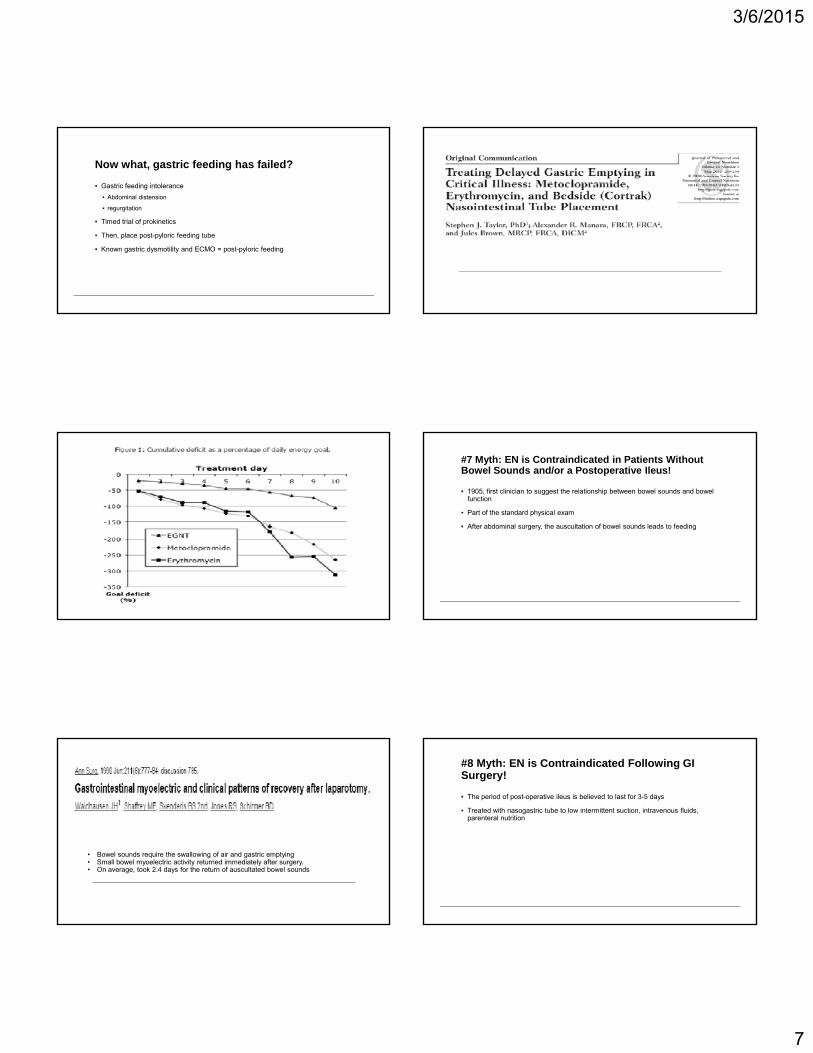
Now what, gastric feeding has failed?
▪ Gastric feeding intolerance
▪ Abdominal distension
▪ regurgitation
Timed trial of prokinetics▪ Timed trial of prokinetics
▪ Then, place post-pyloric feeding tube
▪ Known gastric dysmotility and ECMO = post-pyloric feeding
#7 Myth: EN is Contraindicated in Patients Without Bowel Sounds and/or a Postoperative Ileus!
▪ 1905, first clinician to suggest the relationship between bowel sounds and bowel function
▪ Part of the standard physical exam
▪ After abdominal surgery the auscultation of bowel sounds leads to feeding▪ After abdominal surgery, the auscultation of bowel sounds leads to feeding
• Bowel sounds require the swallowing of air and gastric emptying• Small bowel myoelectric activity returned immediately after surgery.• On average, took 2.4 days for the return of auscultated bowel sounds
#8 Myth: EN is Contraindicated Following GI Surgery!
▪ The period of post-operative ileus is believed to last for 3-5 days
▪ Treated with nasogastric tube to low intermittent suction, intravenous fluids, parenteral nutrition

3/6/2015
8
• Systematic review and meta-analysis of randomised controlled trials comparing any type of enteral feeding started within 24 hours after surgery with nil by mouth management in elective gastrointestinal surgery
• 837 patients, 11 studies• No clear advantage to keeping patients nil by mouth after elective gastrointestinal
resection
Enteral feeding post surgery
▪ Aggressive enteral nutrition does not come without risk
▪ Gastrointestinal intolerance:
▪ Abdominal distention
H t i▪ Hypotension
▪ Shock
▪ Small bowel ischemia or necrosis
▪ High mortality rate
• Before and after episodes of hypotension, the benefits of enteral nutrition warrant a fairly aggressive approach
• The risk:benefit ratio rises steeply during the period of hypotension• Feeds may be continued during this period, as long as there is close clinical monitoring
and a high index of suspicion is maintained for any signs of GI intolerance and the possibility of early mucosal ischemic injury
#9 Myth: EN is Contraindicated in Patients with an Open Abdomen!
▪ NPO or PN
▪ Assumption that enteral nutrition be held due to bowel wall edema and bowel dysfunction
Retrospective review = 78 patients
Early enteral nutrition in the open abdomen was associated with (1)earlier primary abdominal closure(2)lower fistula rate(3)lower hospital charges by $50,000
Retrospective study of 37 pts with ACS:
Enteral feeding was never started in 12 patients; 4 died within 48 hours of admission 7 required vasoactive agents until their death and 1 developed anadmission, 7 required vasoactive agents until their death, and 1 developed an enterocutaneous fistula requiring parenteral nutrition. Enteral feeding was initiated in the remaining 25 patients: 13 had feeds started within 24 hours of abdominal closure; 5 were fed with open abdomens; and 7 had a delay because of vasopressors (n = 2), multiple trips to the operating room (n = 2), paralytics (n = 2), and increased intra-abdominal pressures (n = 1). Once advanced, enteral feeding was tolerated in 23 (92%) of the 25 patients with attainment of goal feeds in a mean of 3.1 +/- 1 days.
3/6/2015
9
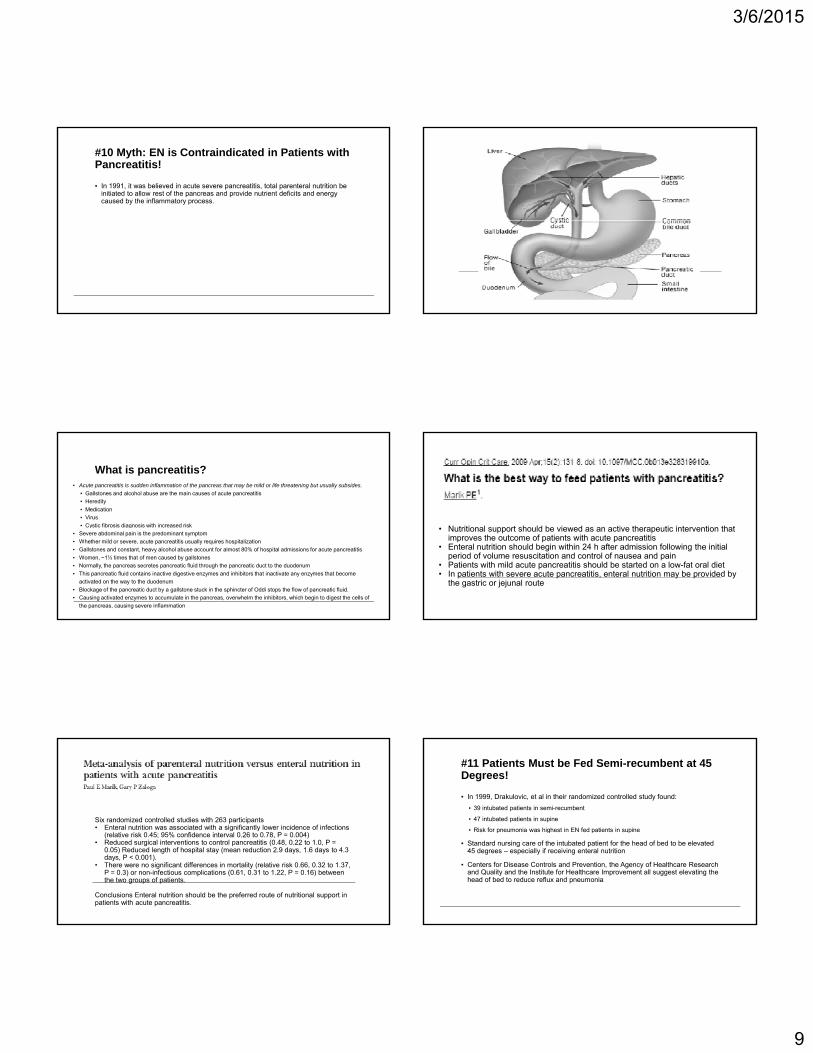
#10 Myth: EN is Contraindicated in Patients with Pancreatitis!
▪ In 1991, it was believed in acute severe pancreatitis, total parenteral nutrition be initiated to allow rest of the pancreas and provide nutrient deficits and energy caused by the inflammatory process.
What is pancreatitis?▪ Acute pancreatitis is sudden inflammation of the pancreas that may be mild or life threatening but usually subsides.
▪ Gallstones and alcohol abuse are the main causes of acute pancreatitis
▪ Heredity
▪ Medication
▪ Virus
▪ Cystic fibrosis diagnosis with increased risk▪ Cystic fibrosis diagnosis with increased risk
▪ Severe abdominal pain is the predominant symptom
▪ Whether mild or severe, acute pancreatitis usually requires hospitalization
▪ Gallstones and constant, heavy alcohol abuse account for almost 80% of hospital admissions for acute pancreatitis
▪ Women, ~1½ times that of men caused by gallstones
▪ Normally, the pancreas secretes pancreatic fluid through the pancreatic duct to the duodenum
▪ This pancreatic fluid contains inactive digestive enzymes and inhibitors that inactivate any enzymes that become
activated on the way to the duodenum
▪ Blockage of the pancreatic duct by a gallstone stuck in the sphincter of Oddi stops the flow of pancreatic fluid.
▪ Causing activated enzymes to accumulate in the pancreas, overwhelm the inhibitors, which begin to digest the cells of
the pancreas, causing severe inflammation
N t iti l t h ld b i d ti th ti i t ti th t• Nutritional support should be viewed as an active therapeutic intervention that improves the outcome of patients with acute pancreatitis
• Enteral nutrition should begin within 24 h after admission following the initial period of volume resuscitation and control of nausea and pain
• Patients with mild acute pancreatitis should be started on a low-fat oral diet • In patients with severe acute pancreatitis, enteral nutrition may be provided by
the gastric or jejunal route
Six randomized controlled studies with 263 participants• Enteral nutrition was associated with a significantly lower incidence of infections
(relative risk 0.45; 95% confidence interval 0.26 to 0.78, P = 0.004)• Reduced surgical interventions to control pancreatitis (0.48, 0.22 to 1.0, P =
0.05) Reduced length of hospital stay (mean reduction 2.9 days, 1.6 days to 4.3 days, P < 0.001).
• There were no significant differences in mortality (relative risk 0.66, 0.32 to 1.37, P = 0.3) or non-infectious complications (0.61, 0.31 to 1.22, P = 0.16) between the two groups of patients.
Conclusions Enteral nutrition should be the preferred route of nutritional support in patients with acute pancreatitis.
#11 Patients Must be Fed Semi-recumbent at 45 Degrees!
▪ In 1999, Drakulovic, et al in their randomized controlled study found:
▪ 39 intubated patients in semi-recumbent
▪ 47 intubated patients in supine
▪ Risk for pneumonia was highest in EN fed patients in supineRisk for pneumonia was highest in EN fed patients in supine
▪ Standard nursing care of the intubated patient for the head of bed to be elevated 45 degrees – especially if receiving enteral nutrition
▪ Centers for Disease Controls and Prevention, the Agency of Healthcare Research and Quality and the Institute for Healthcare Improvement all suggest elevating the head of bed to reduce reflux and pneumonia

3/6/2015
10
Semirecumbent versus supine or near supine
▪ Van Nieuwenhoven, et al (2006) randomized 112 intubated patients = 45 degrees was not achieved 85% of the time
▪ The non-supine patients were repositioned more frequently than supine
▪ No difference in ventilator associated pneumonia
▪ Grap, et al (2005) reported a mean backrest elevation of 21.7 degrees without association to pneumonia
▪ Rose et al (2010) of 2112 backrest elevation measurements in 371 patients in 32 ICUs▪ Rose, et al (2010) of 2112 backrest elevation measurements in 371 patients in 32 ICUs.
▪ 45 degrees = recorded in 5.3% of instances
▪ 30-45 degrees = recorded 22.3% of instances
▪ Nursing a patient semirecumbent at 45 degrees is not feasiable
▪ Attempts may not reduce ventilator associated pneumonia
▪ 45 degree positioning = patient slides down, sacral pressure, uncomfortable for patient
▪ Supine at 0 degrees probably increases the risk of pneumonia; however, no strong evidence that elevation of the head of the bed to 10-30 degrees will increase the risk for pneumonia
Conclusion
▪ Myths delay and limit optimal enteral nutrition
▪ Few exceptions prohibit enteral nutrition = GI bleed requiring endoscopy, surgical problem that must be repaired or planned extubation where oral feeding is likely to be resumed
▪ Early EN is feasible and improves outcomes of critically ill patients
▪ Patients who are about to die or are deceased
References▪ Artinian, V., Krayem, H., & DiGiovine, B. (2006). Effects of early enteral feeding on the outcome of critically ill mechanically ventilated medical patients. Chest, 129(4), 960-967.▪ Barr, J., Hecht, M., Flavin, K.E., Khorana, A., & Gould, M.K. (2004). Outcomes in critically ill patients before and after the implementation of an evidence-based nutritional management protocol. Chest,
125(4), 1446-1457.▪ Choi, E.Y., Park, D-A., Park, J. (2015). Calorie intake of enteral nutrition and clinical outcomes in acutely critically ill patients: a meta-analysis of randomized controlled trials. Journal of Parenteral and
Enteral Nutrition, ahead of print.▪ Collier, B., Guillamondegui, O., Cotton, B., Donahue, R., Conrad, A., Groh, K., Richman, J., Vogel, T., Miller, R. & Diaz, J. (2007). Feeding the open abdomen. JPEN, 31(5), 410-415.▪ Cothren, C.C., Moore, E.E., Ciesla, D.J., Johnson, J.L., Moore, J.B., Haenel, J.B., Burch, J.M. (2004). Postinjury abdominal compartment syndrome does not preclude early enteral feeding after definitive
closure. Am J. Surg, 188(6), 653-658.▪ Dickerson, R.N. (2011). Optimal caloric intake for critically ill patients: first do no harm. Nutrition in Clinical Practice, 26(1), 48-54.▪ Drakulovic, M.B., Torres, A., Bauer, T.T., Nicolas, J.M., Nogue, S., Ferrer, M. (1999). Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized
trial. The Lancet, 354, 1851-1858.▪ Grap, M.J., Monro, C.L., Hummel, R.S., et al (2005). Effect of backrest elevation on the development of ventilator-associated pneumonia. Am J Critical Care, 14, 396-402.▪ Heyland, D.K., MacDonald, S., Keefe, L. & Drover, J.W. (1998). Total parenteral nutrition in the critically ill patient: a meta-analysis. JAMA, 16(280), 2013-2019.▪ Khalid I Doshi P & DiGlovine B (2010) Early enteral nutrition and outcomes of critically ill patients treated with vasopressors and mechanical ventilation Nutrition in Critical Care 19(3) 261-268▪ Khalid, I., Doshi, P., & DiGlovine, B. (2010). Early enteral nutrition and outcomes of critically ill patients treated with vasopressors and mechanical ventilation. Nutrition in Critical Care, 19(3), 261-268.▪ Lauriti, G., Zani, A., Aufieri, R., Cananzi, M., Chiesa, P.L., Eaton, S., & Pierro, A. (2014). Incidence, prevention, and treatment of parenteral nutrition-associated cholestasis and intestinal failure-
associated liver disease in infants and children: a systematic review. JPEN, 38(1), 70-85.▪ Lewis, S.J., Egger, M., Sylvester, P.A., Thomas, S. (2001). Early enteral feeding versus “nil by mouth” after gastrointestinal surgery: systematic review and meta-analysis of controlled trials.▪ Marik, P.E. (2014). Enteral nutrition in the critically ill: myths and misconceptions. Critical Care Medicine 42 (4), 962-969.▪ Marik, P.E. (2009). What is the best way to feed patients with pancreatitis? Crit Care, 15(2), 131-138.▪ Marik, P.E., Zaloga, G.P. (2004). Meta-analysis of parenteral nutrition versus enteral nutrition in patients with acute pancreatitis. (2004), BMJ, 328, 1407. ▪ Marik, P.E. & Zaloga, G.P. (2003). Gastric versus post-pyloric feeding: a systematic review. Critical Care, 7(3), 46-51.▪ McClave, S.A. & Chang, W.K. (2003). Feeding the hypotensive patient: does enteral feeding precipitate or protect against ischemic bowel? Nutrition Clinical Practice, 18(4), 279-284.▪ McClave, S.A., Lukan, J.K., Stefater, J.A., Lowen, C.C., Looney, S.W., Matheson, P.J., Gleeson, & K., Spain, D.A. (2005). Poor validity of residual volumes as a marker for risk of aspiration in critically ill
patients. Critical Care Medicine, 33(2), 324-330.▪ McClave, S.A., & Snider, H.L. (2002). Clinical use of gastric residual volumes as a monitor for patients on enteral tube feeding. JPEN, 26(6), 43-48▪ Mushlin, G.S. (2004). Catecholamine induced changes in the splanchnic circulation affecting systemic hemodynamics. Anesthesiology 100, 434-439.▪ Parks, D.A., Jacobson, E.D. (1985). Physiology of the splanchnic circulation, JAMA, 145 (7), 1278-1281.▪ Rose, L., Baldwin, I., Crawford, T., et al. (2010). Semirecumbent positioning in ventilator-dependent patients: a multicenter, observational study. Am J Critical Care 19, 100-108.▪ Tatucu-Babet, O.A., BNutDiet, Ridley, E.J., Tierney, A.C. (2015). The prevalence of underprescription or overprescription of energy needs in critically ill mechanically ventilated adults as determined by
indirect calorimetry: a systematic literature review. Journal of Parenteral and Enteral Nutrition, ahead of print.▪ Taylor, S.J., Manara, A.R., & Brown, J. (2010). Treating delayed gastric emptying in critical illness: metoclopramide, erythromycin, and bedside (Cortrak) nasointestinal tube placement. JPEN, 34(3),
289-294.▪ Van Nieuwenhoven, C.A., Vandenbroucke-Grauls, C., van Tiel, F.H. (2012). Feasibility and effects of the semirecumbent position to prevent ventilator-associated pneumonia: a randomized study. Critical
Care Medicine, 34, 396-402.▪ Waldhausen, J.H.T., Shaffrey, M.E., Skenderis, S., Jones R.S., & Schrimer, B.D. (1990). Gastrointestinal myoelectric and clinical patterns of recovery after laparotomy. Annals of Surgery, 211(6), 777-
785.▪ Weijs, P.J.M., Stapel, S.N., deGroot, S.D.W., Driessen, R.H., deJong, E., Girbes, A.R.J., Strack van Schijndel, R.J.M., & Beishuizen, A. Optimal protein and energy nutrition decreases mortality in
mechanically ventilated, critically ill patients: a prospective observational cohort study. JPEN, 36(1) 60-68.▪ Yang,S., Wu, X., Yu, W., & Li, J. (2014). Early enteral nutrition in critically ill patients with hemodynamic instability: an evidence-based review and practical advice. Nutrition in Clinical Practice, 29(1), 90-
96.▪ Zaloga, G.P., Roberts, P.R., & Marik, P. (2003). Feeding the hemodynamically unstable patient: a critical evaluation of the evidence. Nutrition Clinical Practice, 18(4), 285-93.

3/6/2015
1
Failure to thrive
© Children’s Specialty Group. All rights reserved.
Lori A. Duesing, MSN, RN, CPNP-AC, APNPDivision of Pediatric Gastroenterology and Nutrition, Medical College of Wisconsin
Disclosures
I h l t fi i l
© Children’s Specialty Group. All rights reserved.
I have no relevant financial relationships to disclose
Objectives
• To define FTT and determine which children will benefit from nutritional intervention
• To describe the common interventions used in the management of FTT and feeding disorders
© Children’s Specialty Group. All rights reserved.
management of FTT and feeding disorders
• To describe FTT and feeding disorder scenarios where a primary care provider should seek help from specialists
Definitions
© Children’s Specialty Group. All rights reserved.
1. Weight < 75% of median weight for chronological age (Gomez criterion)
2. Weight < 80% of median weight for length (Waterlowcriterion)
3. Body mass index for chronological age < 5th centile
© Children’s Specialty Group. All rights reserved.
y g g4. Weight for chronological age < 5th centile5. Length for chronological age < 5th centile6. Weight deceleration crossing more than two major
centile lines from birth until weight within the given age group
7. Conditional weight gain = lowest 5%, adjusted for regression towards the mean from birth until weight within the given age group
Olsen EM, et al. Arch Dis Child. 2007. © Children’s Specialty Group. All rights reserved.

3/6/2015
2
• Is 3% of the population below the 3rd
percentile?– WHO growth charts for children under 24 months– Observations falling ≥ 3 SD and ≤ 3 SD of the
sample median were excluded
© Children’s Specialty Group. All rights reserved.
sample median were excluded
• Is weight alone enough?– Proportionately small children are often not
failing to thrive– Weight-for-length or BMI < 3rd percentile may be
a better marker of FTT
© Children’s Specialty Group. All rights reserved.
• What is stable growth during infancy?– 6-39% of full-term infants cross two weight
percentiles between birth and 2 years
© Children’s Specialty Group. All rights reserved.
• Growth curves are averages which are mathematically smoothed out
Mei Z, et al. Pediatrics. 2004 Mei Z, et al. Clin Pediatr. 2011
Which growth charts and for what ages?
© Children’s Specialty Group. All rights reserved.
• 0-2 years: use WHO growth standards
• 2 years +: use CDC growth charts
© Children’s Specialty Group. All rights reserved.
2 years +: use CDC growth charts
• Danish birth cohort– Significant undernutrition
• 3% under the age of 1– Poor concurrence among all seven criteria
© Children’s Specialty Group. All rights reserved.
– None of the FTT children met all the criteria– Most met only one criterion – Most single criteria
• Not accurate enough
Olsen et al. Arch Dis Child 2007

3/6/2015
3
© Children’s Specialty Group. All rights reserved.
• Genetic short stature– Short parents– Low percentiles but do not cross
percentiles
© Children’s Specialty Group. All rights reserved.
percentiles
• To the average of the parents’ heights– Add 2.5” if male– Subtract 2.5” if female
© Children’s Specialty Group. All rights reserved.
• This is the median height expected for that child – 8.5 cm on either side of the median will
give 2 SD on either side
• Ex-premature infant– Normal birth weight if corrected for
gestation– Low percentiles if uncorrected but may
© Children’s Specialty Group. All rights reserved.
Low percentiles if uncorrected, but may show catch-up growth
• Preemies under 32 weeks gestation– May never catch up if growth during first
months of life was poor
• Constitutional delay– Initial drop in percentiles, then follow their
own line– Family history +
© Children’s Specialty Group. All rights reserved.
Family history +– Bone age assessment
• Catch-down growth– Above-expected birth weight– Initial fall in percentiles, then follow
percentiles
© Children’s Specialty Group. All rights reserved.
percentiles– This is important in LGA babies
3/6/2015
4
© Children’s Specialty Group. All rights reserved.
• Weight-for-length < 2nd percentile (WHO growth chart) or BMI < 3rd percentile (CDC growth chart)
• Poor or no weight gain – Over a period of time that varies according to the age of
the child
© Children’s Specialty Group. All rights reserved.
• Significant downtrend in weight percentiles– 30% of full-term infants cross one percentile and 23% cross
two percentiles between birth and 2 years
• These should be done along with– Assessment of parental size / growth– Correction for prematurity (where applicable)
© Children’s Specialty Group. All rights reserved.
• Inadequate intake of calories• Loss of calories
– Vomiting– Maldigestion
M l b ti
© Children’s Specialty Group. All rights reserved.
– Malabsorption• Increased caloric need
– Cardiorespiratory disease– Liver disease– Renal disease– Chronic infections
• Inability to utilize calories consumed– Chromosomal disorders– Endocrine disorders
Metabolic disorders
© Children’s Specialty Group. All rights reserved.
– Metabolic disorders
• Failure of food intake underlies most cases of FTT– lack of available food– lack of knowledge about infant feeding
maternal depression
© Children’s Specialty Group. All rights reserved.
– maternal depression– specific dietary beliefs
• Parent-child interaction– parent not offering food– child refusing to take food
• Specific organic issues in the infant

3/6/2015
5
© Children’s Specialty Group. All rights reserved.
• Pregnancy and labor • Birth weight• Early neonatal history
© Children’s Specialty Group. All rights reserved.
• Early neonatal history• Feeding issues in the first year of life
• The most common definition of SGA is 2SD below the mean for gestational age (≤ 2SD)
• ~90% of SGA infants exhibit spontaneous catch-up growth
© Children’s Specialty Group. All rights reserved.
p g
• Appropriate weight gain (“Goldilocks” amounts) is associated with the best neurological outcomes– ↑↑ weight gain (> 5000 gm in the first 16 weeks of
life) is associated with ↓ cognition and ↑BMI at age 7 years
Karlberg et al. Pediatr Res 1995Pylipow et al. J Pediatr 2009
• If a child is ≤ 2SD below the mean for gestational age, then child is SGA
Female 2SD below mean Male
Gest age grams pounds‐ounces Gest age grams pounds‐ounces
23 427 15.1 oz 23 474 1 lb 0.7 oz
24 471 1 lb 0.6 oz 24 497 1 lb 1.5 oz
25 496 1lb 1.5 oz 25 545 1lb 3.2 oz
26 536 1 lb 2.9 oz 26 598 1 lb 5.1 oz
© Children’s Specialty Group. All rights reserved.
27 598 1 lb 5.1 oz 27 661 1 lb 8.3 oz
28 652 1 lb 7 oz 28 732 1 lb 9.8 oz
29 747 1 lb 10.3 oz 29 841 1 lb 13.6 oz
30 884 1 lb 15.2 oz 30 913 2 lb 0.2 oz
31 1006 2 lb 3.5 oz 31 1083 2 lb 6.2 oz
32 1130 2 lb 7.9 oz 32 1211 2 lb 10.7 oz
33 1304 2 lb 14 oz 33 1376 3 lb 0.5 oz
34 1480 3 lb 4.2 oz 34 1560 3 lb 7.0 oz
35 1540 3 lb 6.3 oz 35 1663 3 lb 10.6 oz
36 1647 3 lb 10.1 oz 36 1802 3 lb 15.6 oz
37 1844 4 lb 1 oz 37 2022 4 lb 7.31 oz
38 2160 4 lb 12.2 oz 38 2265 4 lb 15.9 oz
39 2364 5 lb 3.4 oz 39 2480 5 lb 7.4 oz
40 2531 5 lb 9.3 oz 40 2596 5 lb 11.6 oz
41 2592 5 lb 11.4 oz 41 2655 5 lb 13.7 oz
Adapted from Olsen et al. Pediatrics 2010.
• Immunizations• Development• Medical or surgical illnesses
© Children’s Specialty Group. All rights reserved.
• Frequent infections
• Plot previous points
© Children’s Specialty Group. All rights reserved.

3/6/2015
6
• Feeding behavior and environment• Allergies to foods• Assessment of intake
© Children’s Specialty Group. All rights reserved.
Assessment of intake– Qualitative vs quantitative– 24-hour food recall– 3-day diet record
• Who feeds the child?• Where and when does the child eat?• Are there distractions?
© Children’s Specialty Group. All rights reserved.
• Is there any force feeding?• Is there any grazing?
• Perception of growth failure as a problem
© Children’s Specialty Group. All rights reserved.
• Vital for accurate assessment of growth• Length
– Length board until age 2• Weight
© Children’s Specialty Group. All rights reserved.
• Weight– < 24 months
• Nude or in clean, dry diaper– 24+ months
• Light clothing
• Thorough physical exam
© Children’s Specialty Group. All rights reserved. © Children’s Specialty Group. All rights reserved.

3/6/2015
7
• Z-scores allow more precision in describing anthropometric status
© Children’s Specialty Group. All rights reserved.
z‐score = – 3.5
z‐score = – 2.1
• Causes – Genetics 50%– Constitutional/nutritional 35%– Chronic illness >10%
© Children’s Specialty Group. All rights reserved.
– Endocrine < 5%• Children with growth hormone
deficiency are not usually malnourished
• In malnutrition, serum IGF-1 will be low
• Low weight, low height → Malnutrition• Normal weight, low height → Endocrine• Normal weight, low height,
dysmorphism → Endocrine and
© Children’s Specialty Group. All rights reserved.
Genetics
• SGA patients without catch-up growth by the age of 3 years can be referred to an endocrinologist for possible growth hormone treatment
© Children’s Specialty Group. All rights reserved.
• Laboratory tests do not help in the evaluation of FTT– 1.4 – 3.2 % laboratory tests were helpful in
making a diagnosis
© Children’s Specialty Group. All rights reserved.
making a diagnosis– All positive results suspected clinically
Berwick et al. Arch Dis Child 1982Sills RH. Am J Dis Child 1978 Larson‐Nath C. 2015
• Do not perform lab tests unless– Child is not responding to standard interventions– Child has other symptoms or signs of disease
© Children’s Specialty Group. All rights reserved.
• Common labs– CBC, ESR– Metabolic panel, electrolytes– Anti-TTG IgA, serum IgA level– Fecal elastase– Urinalysis

3/6/2015
8
© Children’s Specialty Group. All rights reserved.
• Have parents describe typical day• Look for red flags
• Excessive juice intakeE i ilk i t k
© Children’s Specialty Group. All rights reserved.
• Excessive milk intake• ‘Grazing’
• 15 calories per ounce, no protein
• Has been shown to be
© Children’s Specialty Group. All rights reserved.
contributing factor to FTT
Smith MM, et al. Pediatrics. 1994
• Excessive milk consumption can cause iron deficiency anemia and constipation
• If milk intake excessive, cut back to promote increase in solid food intake
© Children’s Specialty Group. All rights reserved.
increase in solid food intake
• Whole milk - until age of 2
• Recommended milk intake– 2-3 years: 16-20 ounces– 4-12 years: 24-32 ounces
Children < 1 year• Adding powdered formula to expressed
breast milk• Increasing calories in formula
© Children’s Specialty Group. All rights reserved.
Children > 1 year• 30 calorie per ounce beverages
– Ready-to-feed: Pediasure, Nutren Jr– Mix powder with milk: Carnation Instant Breakfast
w/ whole milk– Milk with heavy cream : 7 oz of whole milk with 1
oz of heavy cream
• Use the family’s usual foods– Add fat to the child’s foods– Suggest fats that are appropriate to the
food being served
© Children’s Specialty Group. All rights reserved.
food being served
• Do not commence junk food

3/6/2015
9
• Meals/snacks – At table or in high chair
• Structured meals and snacks N th 20 30 i t t t/d i k
© Children’s Specialty Group. All rights reserved.
– No more than 20-30 minutes to eat/drink– Feed every 3 hours
• Only water between meals and snacks
• Ask parents to look for a complete Pediatric multivitamin (not a gummy!)
• Most complete multivitamins½ t bl t f 2 & 3 ld
© Children’s Specialty Group. All rights reserved.
– ½ tablet for 2 & 3-year-olds– Full tablet for 4+ years
© Children’s Specialty Group. All rights reserved.
• Establish Meal Time Routine– Meals and snacks offered every 3 hourly– Limit all feedings to maximum of 30 minutes
© Children’s Specialty Group. All rights reserved.
g– All meals and should be offered in a high
chair/at the table– Minimize distractions– Avoid force feeding– Eliminate grazing between meals and snacks– Water between meals and snacks
• Decrease or eliminate juice• High-calorie diet
– Use the family’s regular meals but add fats only to foods presented to the patient
© Children’s Specialty Group. All rights reserved.
only to foods presented to the patient
– Do not switch child over to junk food
– High-Calorie Beverages
• In moderate or severe failure to thrive• Unmotivated families
– risk of child worsening if something is not
© Children’s Specialty Group. All rights reserved.
done• Balance between high-calorie
beverage and solid food• Wean off high-calorie beverage at the
first possible opportunity
3/6/2015
10
• Investigate and appropriately treat causes of vomiting and diarrhea
© Children’s Specialty Group. All rights reserved.
• Investigate for malabsorption if child is consuming sufficient calories
• Referral to appropriate subspecialists
• Eliminate juice• Eliminate grazing
M i ll t t ll lid d
© Children’s Specialty Group. All rights reserved.
• Maximally concentrate all solids and liquids
• Consider tube-feeding early• Referral to appropriate subspecialists
Feeding Disorders
© Children’s Specialty Group. All rights reserved.
Feeding Disorders
Normal Feeding Milestones
• Rapid acquisition of feeding skills during 1st year of life– no plateau
• Consistent increase in variety and
© Children’s Specialty Group. All rights reserved.
Consistent increase in variety and volume consumed during 1st year of life
• Should transition through purees, finger foods and early table foods by 1st
birthday
Normal Feeding Milestones
• Demonstrate basic chewing skills by age1 – continued refinement throughout early
childhood
© Children’s Specialty Group. All rights reserved.
• Age and development should always guide feeding expectations
• Feeding a child should not be stressful
In any child with a feeding disorder
• Is it organic in origin? Is it a lack of skill?
• Is it a behavioral issue?
© Children’s Specialty Group. All rights reserved.
In general, the younger the child the less likely that it is a behavioral issue

3/6/2015
11
Any child with a feeding disorder
• Establish Meal Time Routine– Meals and snacks offered every 3 hourly– All meals and should be offered in a high
chair/at the table
© Children’s Specialty Group. All rights reserved.
chair/at the table– Minimize distractions– Avoid force feeding– Grazing in between meal and snack times
should be eliminated
Consider hunger manipulation
• This should only be done when it is fairly certain it is behavioral
• Should not be done in malnourished children
© Children’s Specialty Group. All rights reserved.
children• Should be done correctly up to ½ - 1
whole day • Should be abandoned if it does not
work
Candidates for the Feeding Team
• Have enough neurological abilities to PO feed
• Highly motivated families
© Children’s Specialty Group. All rights reserved.
g y
• Behavioral feeding problems
• Chronically G-tube-fed children who have the ability to eat by mouth
• Making a diagnosis of FTT requires a combination of objective and subjective information
• Once a diagnosis of FTT is made, further information is required to guide
© Children’s Specialty Group. All rights reserved.
information is required to guide management
• Most children with FTT do not require laboratory studies
• Most children with FTT and Feeding Disorders can be managed through a series of simple interventions

3/6/2015
1
The New Opportunities for Verification ofThe New Opportunities for Verification of Enteral Tube Location (NOVEL) Project Update
Lori A. Duesing, MSN, RN, CPNP-AC, APNPDivision of Pediatric Gastroenterology and Nutrition, Medical College of Wisconsin
Objectives:
▪ Discuss NG/OG/post-pyloric tube placement verification in pediatrics
▪ Discuss the NOVEL project mission
▪ Discuss research findings
▪ Discuss future direction
Background
▪ In 2012, a safety alert was distributed by the Child Health Patient Safety Organization recommending the immediate discontinuation of the auscultation method for NG tube placement verification
▪ 1.3-2.4% of NG tube in over 2,000 insertion were located outside of the t i t ti l t tgastrointestinal tract.
▪ 20% of those tubes led to pulmonary complications
▪ Abdominal film is current gold standard
Background continued
▪ In addition to this alert, the American Association of Critical Care Nurses (AACN) issued a practice alert3 and the American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) implemented practice recommendations4 to address the risks and potential complications associated with misplaced NG tubes.
▪ National Association Childrens Hospitals (N.A.C.H.), ECRI Institute. Blind Pediatric NG Tube Placements - Continue to Cause Harm. Child Health, Patient Safety Organization. Overland Park, KS: Child Health Patient Safety Organization, Inc.; 2012, August.
▪ Sorokin R, Gottlieb JE. Enhancing Patient Safety During Feeding-Tube Insertion: A Review of More than 2000 Insertions. JPEN J Parenter Enteral Nutr. 2006;30(5):440 - 445.
▪ American Association of Critical Care Nurses (AACN). AACN Practice Alert: Verification of Feeding Tube Placement (blindly inserted): American Association of Critical Care Nurses; 2010.
▪ Bankhead R, Boullata J, Brantley S, et al. A.S.P.E.N Enteral Nutrition Practice Recommendations. JPEN J Parenter Enteral Nutr. 2009;33(2):122 - 167.
Background continued
▪ Common in hospital and home settings
▪ Used for enteral nutrition, fluids and medication administration
▪ Broad discrepancies regarding verification of placement = lack of literature
▪ Pediatrics more complex than adults: size of patient in relationship to size of tube, goal to minimize exposure to radiation
▪ X-ray is the gold standard, followed by pH
▪ NG tube misplacement can cause serious neurological harm or death
▪ Nurses are primary health care providers who insert NG tubes in the hospital and home settings
A mother’s story: (get out the Kleenex)▪ M y n a m e i s D e a h n a V i s s c h e r a n d I l o s t m y s o n t o a n a v o i d a b l e m e d i c a l e r r o r. O n A p r i l 8 , 2 0 0 8
I g a v e b i r t h t o G r a n t L a r s V i s s c h e r. H e w a s b o r n w i t h a h e a r t d e f e c t t h a t r e q u i r e d s u r g e r y. H e f l e w t h r o u g h t h e r e c o v e r y o f h i s s u r g e r y w i t h a m a z i n g p r o g r e s s . A t 1 1 d a y s o l d , a n d w i t h i n a c o u p l e o f d a y s o f b e i n g r e l e a s e d f r o m t h e h o s p i t a l , h e d i e d b e c a u s e a n u r s e m a d e a m i s t a k e p l a c i n g h i s f e e d i n g t u b e . I n s t e a d o f g o i n g i n t o h i s s t o m a c h i t w e n t i n t o h i s l u n g s . A l l d a y w e w a t c h e d h i m s u f f e r a n d t h e n d i e t h a t n i g h t b e f o r e o u r e y e s . I t i s a g u t w r e n c h i n g p a i n t h a t I w i s h o n n o o n e .
▪ T h e d a y h i s f e e d i n g t u b e w a s m i s p l a c e d w a s a d a y I w i l l n e v e r f o r g e t . I t w a s a d a y t h a t q u e s t i o n s I a s k e d w o u l d f o r e s h a d o w t h e e v e n t s t h a t l e d t o h i s d e a t h . I n t h e m o r n i n g t h e n u r s e c a m e i n a n d w a s n o t c o m f o r t a b l e w i t h h i s c u r r e n t f e e d i n g t u b e p l a c e m e n t a n d w a n t e d t o p u t i n a n e w o n e . A s s h e w a s p l a c i n g h i s n e w f e e d i n g t u b e I a s k e d h e r h o w s h e w o u l d k n o w i t w a s i n t h e r i g h t p l a c e . T h e n u r s e t h e n s h o w e d m e t h a t s h e w o u l d p u t i n a b u r s t o f a i r i n t h e t u b e a n d l i s t e n t h r o u g h a s t e t h o s c o p e t o h e a r t h e b u b b l e i n h i s a b d o m e n I a s k e d t h e t h e t u b e a n d l i s t e n t h r o u g h a s t e t h o s c o p e t o h e a r t h e b u b b l e i n h i s a b d o m e n . I a s k e d t h e n u r s e h o w s h e c o u l d b e s u r e t h a t s o u n d w a s a c c u r a t e l y i n h i s a b d o m e n ? S h e t h e n s h o w e d m e h o w f l u i d w a s r e m o v e d f r o m t h e t u b e t o s h o w t h a t i t w a s i n h i s s t o m a c h . I t h e n a s k e d h e r h o w s h e k n e w t h a t w a s s t o m a c h f l u i d a n d n o t f l u i d f r o m e l s e w h e r e i n h i s b o d y ? S h e d i d n ’ t h a v e a n a n s w e r f o r t h a t . I n s t e a d s h e t o l d m e t h a t I w o u l d p r o b a b l y n e e d t o l e a r n h o w t o p l a c e h i s f e e d i n g t u b e i n h i m a s h e m a y g o h o m e w i t h i t a n d i f i t c a m e o u t a t h o m e I ’ d h a v e t o r e p l a c e i t . S h e t o l d m e t h a t i f t h a t w a s t h e c a s e t h e y w o u l d t e a c h m e h o w t o d o w h a t s h e d i d . I d i d n o t k n o w t h e n t h a t m y q u e s t i o n s w o u l d c o m e t o h a u n t m e , a s t h e v e r y t h i n g s t h a t I w a s s h o w n t o a b s o l v e m y f e a r s w e r e p r o v e n f a l s e . H e d i e d t h a t n i g h t b e c a u s e t h e p l a c e m e n t w a s n o t c o r r e c t d e s p i t e t h e t e s t s t h e n u r s e d i d t o v e r i f y p l a c e m e n t .
▪ G r a n t o n l y l i v e d 1 1 d a y s . I m o u r n m y l o s s d a i l y. M o s t l y, I m o u r n f o r t h e t i m e I d i d n o t g e t t o s p e n d w i t h h i m . S i n c e G r a n t ’ s d e a t h I h a v e b e c o m e d e t e r m i n e d t o f i n d a b e t t e r a n d s a f e r m e t h o d f o r f e e d i n g t u b e p l a c e m e n t s s o t h a t n o o t h e r p a r e n t o r p e r s o n w i l l h a v e t o e x p e r i e n c e t h e l o s s t h a t I h a v e . I k n o w t h e r e h a s t o b e a b e t t e r w a y a n d I k n o w w e w i l l f i n d i t .
* * P e r m i s s i o n f r o m D e a h n a t o s h a r e ( 9 / 1 1 / 1 4 )
3/6/2015
2
Ponder these questions
▪ How many of you have known of or been associated with an adverse outcome?
▪ Do you think NG tube misplacements is under-reported?
▪ What role does quality and safety have in relationship to placement?
▪ Should we be concerned just from this one story?
American Society for Parenteral and Enteral Nutrition (ASPEN)
▪ A literature review revealed very few pediatric studies to guide our practice
▪ ASPEN formed a task force to address this issue
▪ Invited participation from stakeholder organizations
N d th j t NOVEL (th N O t iti f V ifi ti f E t l T b▪ Named the project NOVEL (the New Opportunities for Verification of Enteral Tube Location)
Why ASPEN?
ASPEN Strategic Goals and the Novel Project
▪ Foster the discovery of new knowledge and its application to the field of nutritional science (NS) therapy
▪ Education healthcare professionals to provide optimal care
▪ Advocate on behalf of the field of NS to improve clinician experience and patient▪ Advocate on behalf of the field of NS to improve clinician experience and patient outcomes
▪ Position ASPEN a the leading organization in NS therapy
NOVEL Project
▪ Mission:
▪ Determine best practices in NG tube placement verification in pediatric patients
▪ Work with biomedical engineers and industry to develop non-radiologic methods to verify and re verify NG tube placementto verify and re-verify NG tube placement
▪ Disseminate knowledge to professionals to improve clinical practice
Study
▪ Email blasts were sent to members of ASPEN, AACN, SPN and Patient Safety Officers explaining the NOVEL project with directions for IRB and data collection
▪ 140+ individuals/hospitals requested the protocol and 8 withdrew▪ 140+ individuals/hospitals requested the protocol and 8 withdrew
▪ Final count = 63 participating institutions
▪ 2 conference calls were held in December 2013 to explain the data collection process to local investigators
▪ Hospitals sent in IRB approval letters and data collection forms
▪ Data were collected between January – April 2014

3/6/2015
3
Data Collection Tool
▪ Respondents were asked to fill out:
▪ Name of hospital (coded)
▪ Project coordinators credentials
▪ Census on the day of collectionCensus on the day of collection
▪ Number of critical care beds
▪ Number of NICU beds
▪ Verification method for checking placement
▪ Ranked in order 1, 2, 3
Example of toolPatient Number(1,2,3,4)
Patient Weight in kg Patient age (See below) Patient Location(PICU, NICU, med/surg floor)
Size of tube in Fr. Location of tube(NG,OG, postpyloric)
Participating Institutions▪ Children's of Mississippi, Jackson, MS▪ N.C. Children's Hospital at UNC Health Care, Chapel Hill, NC▪ Children’s Hospital & Medical Center, Omaha, NE▪ Virtua Health, Mount Holly, NJ▪ Children's Hospital at Montefiore, Bronx, NY▪ Cohen Children's Medical Center, New Hyde Park, NY▪ St Mary's Hospital for Children, Bayside, NY▪ Stony Brook University, Stony Brook, NY▪ MetroHealth Medical Center, Cleveland, OH▪ Akron Children's Hospital, Akron, OH▪ Akron Children's Hospital, Akron General Medical Center (NICU), Akron, OH▪ Akron Children's Hospital, Summa Akron City Hospital (NICU), Akron, OH▪ Akron Children’s Hospital, St. Elizabeth's Hospital (NICU), Youngstown, OH▪ Mahoning Valley Special Care Nursery at Beeghly in Boardman, Boardman, OH
▪ Banner Thunderbird Medical Center, Glendale, AZ▪ Banner Estrella Medical Center, Phoenix, AZ▪ Banner Del E Webb Medical Center, Sun City West, AZ▪ Children's Central, Madera, CA▪ Rady Children's Hospital, San Diego, CA▪ California Pacific Medical Center, San Francisco, CA▪ Lucile Packard Children's Hospital, Palo Alto, CA▪ Children's Hospital Oakland, Oakland, CA▪ Children's Hospital Colorado, Aurora, CO▪ Connecticut Children's Medical Center, Hartford, CT▪ Nemours/Alfred I. DuPont Hospital for Children, Wilmington, DE▪ UF Health Shands Children's Hospital, Gainesville, FL▪ Children's Healthcare of Atlanta at Scottish Rite, Atlanta, GA▪ Children's Healthcare of Atlanta at Egleston, Atlanta, GA
ChildS D M i IAg y y g y
▪ Dayton Children's, Dayton, OH▪ The Children's Hospital at OU Medical Center, Oklahoma City, OK▪ Children's Hospital of Pittsburgh, Pittsburgh, PA▪ The Children's Hospital of Philadelphia, Philadelphia, PA▪ Sanford USD Medical Center, Sioux Falls, SD▪ Monroe Carell Jr. Children's Hospital at Vanderbilt University Medical Center, Nashville, TN▪ East Tennessee Children's Hospital, Knoxville, TN▪ Cook Children's Medical Center, Fort Worth, TX▪ Dell Children's Medical Center, Austin, TX▪ Children’s Medical Center, Dallas, TX▪ Seattle Children's Hospital, Seattle, WA▪ University of Wisconsin Hospitals and Clinics, Madison, WI▪ Children's Hospital of Wisconsin, Milwaukee, WI▪ Brenner Children's Hospital, Winston-Salem, NC▪ Alaska Native Medical Center, Anchorage, AK▪ Phoenix Children's Hospital, Phoenix, AZ
▪ ChildServe, Des Moines, IA▪ Mercy Children's Hospital and Clinics, Des Moines, IA▪ Rehabilitation Institute of Chicago, Chicago, IL▪ University of Chicago Comer Children's Hospital, Chicago, IL▪ Rockford Memorial Hospital, Rockford, IL▪ Riley Hospital for Children at Indiana University Health, Indianapolis, IN▪ The Center for Women and Infants at University of Louisville Hospital, Louisville, KY▪ Our Lady of the Lake Children's Hospital, Baton Rouge, LA▪ Mount Washington Pediatric Hospital, Baltimore, MD▪ Mercy Medical Center, Baltimore, MD▪ Sparrow Hospital Children's Center, Lansing, MI▪ Children's Mercy Hospital, Kansas City, MO▪ Truman Medical Center, Kansas City, MO▪ Boone Hospital Center, Columbia, MO
▪ 63 Participating Sites
▪ Total census = 8333
▪ 39 pediatric facilities
▪ 8 adult with newborn
16 d lt ith di t i d b▪ 16 adults with pediatrics and newborn
▪ Percentage of patients with tube at time of collection = 23.94%
▪Total number of NICU beds = 2791
▪Total number of PICU beds = 1438
▪Location of patients with tubes
NICU 1219▪NICU = 1219
▪PICU = 359
▪Med/Surg beds = 421
▪Unknown = 5
▪Mean age = 14.33 months
▪Mean tube size = 6.5 French
▪Mean weight = 6.83kg

3/6/2015
4
▪ Prevalence of NG tubes, n=1995
▪NG = ~66% n=1316
▪OG = ~21% n=414
▪ Post pyloric = ~13% n=261
▪ 4 unknown
▪ Of the 63 sites:
▪ All listed a primary method of checking tube placement verification
▪ 55 sites listed a secondary method of checking
▪ 39 sites listed a tertiary method of checking
Verification of Placement
▪METHOD 1
▪Aspiration 21/63 = 33%
▪Auscultation 18/63 = 29%▪Auscultation 18/63 = 29%
▪Measurement 8/63 = 13%
▪pH 10/63 = 16%
▪X-ray 6/63 = 1%
Verification of Placement
▪METHOD 2
▪Aspiration 5/63 = .08%
▪Auscultation 20/63 = 0 32%▪Auscultation 20/63 = 0.32%
▪Measurement 4/63 = .06%
▪pH 5/63 = .08%
▪X-ray 19/63 = 30%
Verification of Placement
▪METHOD 3▪Aspiration 12/63 = 19%▪Auscultation 3/63 = 0.4%▪Measurement 9/63 = 14%▪pH 1/63 = 0.1%▪X-ray 13/63 = 21%▪ Some left blank, one indicated fluoroscopy
Verification by Type of Institution
▪ Pediatric Hospitals
▪ Method 1 – aspiration
▪ Method 2 – X-ray
▪ Method 3 – measurement
Adult hospitals with a NICU▪ Adult hospitals with a NICU
▪ Method 1 – auscultation
▪ Method 2 – auscultation
▪ Method 3 – auscultation
▪ Adult/Pediatric/Neonatal Hospital
▪ Method 1 – aspiration
▪ Method 2 – auscultation
▪ Method 3 – X-ray

3/6/2015
5
What does this mean?
▪ This data validates what is in the literature = limited
▪ Despite current recommendations, there is clearly inconsistencies across the country
▪ Research is needed▪ Research is needed
▪ Barriers to implementing current recommendations
▪ EBP studies for best practice
▪ Size/weight of patient affecting verification
▪ Negative effects of repeated X-ray exposure
Forward thinking for NOVEL
▪ Establish best practice
▪ Evidence based practice studies to evaluate the guidelines
▪ Potential for Enteral Access Safety Teams
▪ Dissemination of studies surrounding NG tube safety
From a nurse“…I placed the NG like I had done hundreds of times in the past, with no complications and checked placement with air bolus and started the feed. The patient ended up coding on the floor and being sent to our PICU where she was intubated and started on ECMO. The moment that the patient went into respiratory distress, my whole life changed. I had not missed a day of work in seven years and went to my nurse manager and told her I needed to leave and could no longer be a nurse, and that I would not be back to work…”from invited commentary in NCP June,2014

3/6/2015
1
Short bowel syndrome Short bowel syndrome ––A nutrition perspectiveA nutrition perspectivep pp p
Lori A. Duesing, MSN, RN, CPNPLori A. Duesing, MSN, RN, CPNP--AC, AC, APNPAPNP
Division of Gastroenterology and NutritionDivision of Gastroenterology and NutritionMedical College of WisconsinMedical College of Wisconsin
Milwaukee, WIMilwaukee, WI
ObjectivesObjectives
To review theTo review the definitiondefinition and and common etiologiescommon etiologiesof short bowel syndrome of short bowel syndrome
To discuss the To discuss the pathophysiologypathophysiology of short bowel of short bowel syndrome and thesyndrome and the physiology of adaptationphysiology of adaptationsyndrome and the syndrome and the physiology of adaptationphysiology of adaptation
To review the To review the clinical managementclinical management of short of short bowel syndromebowel syndrome
To discuss the To discuss the complicationscomplications of short bowel of short bowel syndromesyndrome
DefinitionDefinition
ShortShort--bowel syndrome (SBS) is bowel syndrome (SBS) is defined functionally and is defined functionally and is
considered to exist when the considered to exist when the patient has malabsorption in thepatient has malabsorption in thepatient has malabsorption in the patient has malabsorption in the
presence of a shortened small presence of a shortened small intestineintestine
Major features of SBSMajor features of SBS
dehydration secondary to diarrheadehydration secondary to diarrhea
malabsorption of macromalabsorption of macro and micronutrientsand micronutrients malabsorption of macromalabsorption of macro-- and micronutrientsand micronutrients
malnutritionmalnutrition
failure to thrivefailure to thrive
Neonates
Normal anatomy
Abnormal anatomy
NEC
Midgut volvulus
Multiple atresias
Gastroschisis
Etiology of SBSEtiology of SBS
Older children and
adults
Gastroschisis
Hirschsprung disease
Crohn’s diseaseMalrotation with volvulus TumorsRadiation enteritis

3/6/2015
2
Length needed for TPNLength needed for TPN--free survivalfree survival
In infants with ‘‘normal’’ birth weight at least 15 cm of jejunum or ileum and the ileocecal valve
or 40 cm of small bowel without the ileocecal valve
Gestational age is imperative when reporting residual g p p gbowel length 28-week-old neonate has approximately 200 cm of bowel,
and this increases to 300 cm at term
The anticipated increase in bowel length is greatest in premature infants - an important prognostic factor in SBS patients
Adapted Nonadapted p-value Small bowel length < 15 cm
7% 38% <0.05
Patients with IC valve
68% 23% <0.001
Colonic i
32% 77% <0.001 resection>50% of colonic length resected
29% 70% <0.05
Primary anastomosis
48% 15% <0.01
QuirosQuiros--Tejeira et al. J Peds 2005; 145: 157Tejeira et al. J Peds 2005; 145: 157--6363
The percent of daily energy intake through the The percent of daily energy intake through the enteral route at 12 weeksenteral route at 12 weeks Infants getting 75% of their calories enterally by 12 Infants getting 75% of their calories enterally by 12
weeks the likelihood of weaning off TPN is 90%weeks the likelihood of weaning off TPN is 90%weeks, the likelihood of weaning off TPN is 90% weeks, the likelihood of weaning off TPN is 90%
Those getting 50% enterally at 12 weeks, the Those getting 50% enterally at 12 weeks, the likelihood of weaning is 75%likelihood of weaning is 75%
those getting only 25% enterally, the likelihood of those getting only 25% enterally, the likelihood of weaning is only 50%weaning is only 50%
Sondheimer et al. J Pediatr 132:80-84, 1998
JejunoJejuno--ileal length in premiesileal length in premies
19 19 –– 27 weeks27 weeks 114.8 +/114.8 +/-- 21 cm21 cm
27 27 –– 35 weeks35 weeks 172.1 +/172.1 +/-- 29 cm29 cm
> 35 weeks> 35 weeks 248.0 +/248.0 +/-- 40 cm40 cm
Touloukian RJ, Smith GJ: Normal intestinal length in preterm infants. J Pediatr Surg 18:720-723, 1983
Physiology and Physiology and pathophysiologypathophysiologyp p y gyp p y gy

3/6/2015
3
JejunumJejunum
Long villiLong villi Large absorptive surfaceLarge absorptive surface
High concentration of High concentration of enzymes and carrier proteinsenzymes and carrier proteins Top site for nutrientTop site for nutrientTop site for nutrient Top site for nutrient
absorptionabsorption Large tight junctionsLarge tight junctions
Relatively porousRelatively porous Large influx of water and Large influx of water and
electrolytes into the electrolytes into the lumen from the lumen from the vasculaturevasculature
IleumIleum Short villiShort villi
Smaller absorptive surfaceSmaller absorptive surface AbsorptionAbsorption
Less important for Less important for nutrient absorptionnutrient absorption
Important for bile saltImportant for bile salt Important for bile salt Important for bile salt and vitamin Band vitamin B12absorptionabsorption
Small tight junctionsSmall tight junctions Conserves water and Conserves water and
electrolyteselectrolytes
Effect of resectionsEffect of resections
Normal physiology
Duodenum Jejunum Ileum
Concentrated Concentrated nutrients nutrients delivereddelivered
a large influx of a large influx of fluid and electrolytes fluid and electrolytes
into the lumen into the lumen
Absorption of Absorption of majority of fluid and majority of fluid and
electrolytes electrolytes
Effect of resectionsEffect of resections
Ileal resectionDuodenum Jejunum Ileum
Concentrated Concentrated nutrients nutrients delivereddelivered
a large influx of a large influx of fluid and electrolytes fluid and electrolytes
into the lumen into the lumen
Absorption of Absorption of majority of fluid and majority of fluid and
electrolytes electrolytes
Fluid and electrolyte disturbances
Effect of resectionsEffect of resections
Jejunal resectionDuodenum Jejunum Ileum
Concentrated Concentrated nutrients nutrients delivereddelivered
a large influx of a large influx of fluid and electrolytes fluid and electrolytes
into the lumen into the lumen
Absorption of Absorption of majority of fluid and majority of fluid and
electrolytes electrolytes
Less fluid and electrolyte disturbances
The ileocecal valveThe ileocecal valve
Serves as a barrier for reflux of colonic bacteria Serves as a barrier for reflux of colonic bacteria from the colon into the small intestinefrom the colon into the small intestineResection may result in bacterial overgrowth Resection may result in bacterial overgrowth
in the small intestinein the small intestine It also regulates the exit of fluid and nutrients It also regulates the exit of fluid and nutrients
from the small intestinefrom the small intestineRapid transit of nutrients into the colon may Rapid transit of nutrients into the colon may
worsen malabsorption and increase sensitivity worsen malabsorption and increase sensitivity to osmotic loadsto osmotic loads

3/6/2015
4
The colonThe colon
The adult colon receives and absorbs 1The adult colon receives and absorbs 1--2 liters 2 liters of fluid from the small bowelof fluid from the small bowel
ResectionResection Dehydration and electrolyte problemsDehydration and electrolyte problems Loss of energy via SCFALoss of energy via SCFA
Right colon absorbs the majority of water and Right colon absorbs the majority of water and electrolyteselectrolytes If the right colon is removed, gradual improvement If the right colon is removed, gradual improvement
in sodium and water absorption occurs in the left in sodium and water absorption occurs in the left coloncolon
AdaptationAdaptation
AdaptationAdaptation
Compensatory response that follows an abrupt decrease in mucosal surface area after an extensive small bowel resection
Incl des anatomic and f nctional changes that Includes anatomic and functional changes that increase the gut’s digestive and absorptive capacity
Begins within 48 hours of surgery but may require up to 5 years for completion
AdaptationAdaptationStructural alterationsStructural alterations
The remnant small bowel increases in length and caliber, with hyperplasia / hypertrophy of each intestinal layeres ye
The magnitude of the response is greater after resection of the proximal small bowel compared with a distal resection
AdaptationAdaptationStructural alterationsStructural alterations
The patient’s age at the time of resection affects the extent of bowel lengtheningthe extent of bowel lengthening Neonates are more likely than adults to achieve
independence from TPN after extensive resection
AdaptationAdaptationStructural alterationsStructural alterations
The adapting intestine develops an increased caliber and hypertrophy of the longitudinal and circular smooth muscle layers
The increased intestinal caliber increases the absorptive surface area
may result in ineffective peristalsis
This dysmotility leads to stasis, bacterial overgrowth, sepsis, and malabsorption

3/6/2015
5
AdaptationAdaptationStructural alterationsStructural alterations
Epithelial hyperplasia is the fundamental change Increases villus height
I d h Increases crypt depth
The number of villi is also increased
The sodium-glucose co-transporter increases its activity up to 2.5-fold
Di h id d di id l h
AdaptationAdaptationFunctional alterationsFunctional alterations
Disaccharidases and dipeptidases along the brush border of the adapting small bowel show increased activity when measured per villus
Intestinal epithelium performs an important barrier function to infection
Septic episodes in SBS may be secondary to a breach of this barrier with translocation of
AdaptationAdaptationIntestinal permeabilityIntestinal permeability
breach of this barrier with translocation of bacteria
Bacterial overgrowth secondary to gut dysmotility is common in patients with SBS and can lead to bacterial translocation
Mechanisms of adaptationMechanisms of adaptationIntestinal epithelium in resected bowel
E iProduction of
Exposure to pancreatic and biliary secretions
Exposure to nutrientsProduction of trophic factors
Disaccharides >> monosaccharidesHydrolyzed protein >> Intact proteinLong chain fats >> medium chain fats
Mechanisms of adaptationMechanisms of adaptationIntestinal epithelium in resected bowel
EProduction of trophic
Trophic hormonesTrophic hormones EnteroglucagonEnteroglucagon GastrinGastrin SecretinSecretin CholecystokininCholecystokinin Epidermal growth factorEpidermal growth factor InsulinInsulin--like growth factor Ilike growth factor I
P id YYP id YY Exposure
to nutrients
Production of trophic factors
Peptide YYPeptide YY GlucagonGlucagon--like peptide 2 (GLP like peptide 2 (GLP -- 2)2)
Trophic substancesTrophic substances ProstaglandinsProstaglandins PolyaminesPolyamines
NutrientsNutrients Long Long -- chain fatschain fats Omega Omega –– 3 fatty acids3 fatty acids Short Short -- chain fatty acidschain fatty acids FiberFiber ? Glutamine? Glutamine
‘Pharmacological’ manipulation‘Pharmacological’ manipulation
GlutamineGlutamine MCTMCT LCTLCT Soluble fiberSoluble fiber
-- UnclearUnclear-- Works with an intact colonWorks with an intact colon-- UnclearUnclear-- UnclearUnclear
Pancreatic enzymesPancreatic enzymes Bile acidsBile acids Growth hormoneGrowth hormone GLPGLP--22
-- Do not workDo not work-- UnclearUnclear
-- PromisingPromising-- PromisingPromising
3/6/2015
6
How to feed?How to feed?When to feed?When to feed?Wh t t f d?Wh t t f d?What to feed?What to feed?
MalabsorptionMalabsorption The major consequence of resection of the small intestine is The major consequence of resection of the small intestine is
malabsorptionmalabsorption Due to reduction of the absorptive surface area with loss of Due to reduction of the absorptive surface area with loss of
digestive enzymes and transport carrier proteinsdigestive enzymes and transport carrier proteins Carbohydrates Carbohydrates
PProduce tremendous osmotic diarrhea following resection roduce tremendous osmotic diarrhea following resection of the ileum as reabsorption of water is impairedof the ileum as reabsorption of water is impairedof the ileum as reabsorption of water is impairedof the ileum as reabsorption of water is impaired
ProteinsProteins Larger molecules which are ingested in smaller quantities, Larger molecules which are ingested in smaller quantities,
produce fewer symptoms when produce fewer symptoms when malabsorbedmalabsorbed FatsFats
Large molecules, whose malabsorption creates little additional fluid Large molecules, whose malabsorption creates little additional fluid loss from the small intestineloss from the small intestine
Fat Fat soluablesoluable vitamins vitamins may also be may also be malabsorbedmalabsorbed in large quantities in large quantities Following extensive Following extensive ilealileal resection, bile salt depletion may occurresection, bile salt depletion may occur
Motility changesMotility changes
Motility abnormalities following intestinal Motility abnormalities following intestinal resectionresection Intestinal transit time may increase as the intestine Intestinal transit time may increase as the intestine
adapts in an attempt to increase nutrient contactadapts in an attempt to increase nutrient contactadapts in an attempt to increase nutrient contact adapts in an attempt to increase nutrient contact time with the smalltime with the small--bowel mucosabowel mucosa
Mucosal surface area will likewise increase as the Mucosal surface area will likewise increase as the small intestine dilates small intestine dilates
Unfortunately, both of these changes result in Unfortunately, both of these changes result in increased bacterial content in the small bowelincreased bacterial content in the small bowel
Importance of enteral nutritionImportance of enteral nutrition
Atrophy has been observed in the small intestine deprived of nutrient contact either by bypassing the small intestine surgically or by using parenteral nutritionparenteral nutrition
Intravenous feeding following small-bowel resection results in slight mucosal atrophy, whereas enteral nutrition stimulates mucosal hyperplasia
Enteral nutritionEnteral nutrition
Enteral nutrition is also important for stimulating regeneration of the mucosa The combination of parenteral and enteral nutrition is
superior to parenteral nutrition in stimulating intestinal i i f i i h d di hregeneration in a group of patients with protracted diarrhea
of infancy
A more rapid resolution of malabsorption and diarrhea following enteral nutrition alone versus parenteral nutrition in the same disorder has also been observed
Enteral nutrition is also important in maintaining mucosal mass in SBS
Managing a patient with SBSManaging a patient with SBSInitial managementInitial management
The immediate postoperative period is characterized by a transient ileus, and all n trients m st be given parenterally to stabilizenutrients must be given parenterally to stabilize fluid and electrolyte imbalances

3/6/2015
7
Patients then develop large-volume fluid and electrolyte secretions once the ileus resolves, and gastric fluid and ostomy losses may be high Because these losses vary significantly with time, placing the
patient on a standard parenteral nutrition solution is optimal fl d l h b l d b d h
Managing a patient with SBSManaging a patient with SBSInitial managementInitial management
Excessive fluid losses can then be replaced based on the electrolyte content of these secretions as determined in the laboratory
These secretions can be replaced every few hours using a separate fluid and electrolyte solution
Losses tend to be high in sodium and solutions with at least 80 - 100 mEq/L of sodium are needed to maintain fluid and electrolyte homeostasis
The first stage of therapy is the time to replete any nutritional deficiency states that may have
Managing a patient with SBSManaging a patient with SBSInitial managementInitial management
any nutritional deficiency states that may have existed at the time of resection
When fluid and electrolyte losses have decreased, a continuous enteral infusion is initiated
Elemental diets are s ally sed
Managing a patient with SBSManaging a patient with SBSFurther managementFurther management
Elemental diets are usually used Some people use a lower concentration of formula
and advance the concentration prior to advancing the rate (this prevents overloading the patient)
Others start at optimal concentrations and advance the rate as tolerated
Continuous enteral infusion is gradually advanced based on the absence of the following: A marked increase in stool loss by more than 50%
Stool losses greater than 40 to 50 mL/kg/day or ostomy
Managing a patient with SBSManaging a patient with SBSFurther managementFurther management
output strongly positive for reducing substances
In patients with an intact colon, a decrease in stool pH below 5.5 is frequently indicative of carbohydrate malabsorption
Further advancement of enteral feedings is likely to result in a significant increase in osmotic diarrhea in such patients
The use of continuous enteral infusion is advantageous Feedings are frequently better tolerated Emesis is reduced Carrier proteins are continuously saturated and intestinal
function is optimized
Managing a patient with SBSManaging a patient with SBSFurther managementFurther management
function is optimized The increased enteral calories try to increase the functional
workload of the small intestine, resulting in additional stimulation of intestinal adaptation
Administration of extra calories through the enteral route reduces the need for parenteral nutrition and its complications
The appropriate solids to give initially to patients with short-bowel syndrome are a matter of controversy
Tradition has suggested high-carbohydrate diets
Managing a patient with SBSManaging a patient with SBSFurther managementFurther management
Tradition has suggested high carbohydrate diets
These are hyperosmolar and may increase fluid losses
Meat may be the best initial solid Feeding fats or proteins results in less fluid loss
Fat is also a good trophic agent to the small intestine

3/6/2015
8
Enteral formulasEnteral formulas Patients with SBS are given elemental diets
These are diets that contain amino acids rather than peptides However, most protein is absorbed in the form of di- and
tripeptides, so the concept of an elemental diet is extended in pediatrics to partially elemental formulas - extensive protein hydrolysateshydrolysates
Carbohydrates are usually present from one or more sources, including partially hydrolyzed starch and disaccharides such as sucrose
A mixture of medium- and long-chain fats is included Adult elemental formulas are usually inappropriate in pediatrics
deficient in vitamins, minerals, and essential fatty acids tend to be high in carbohydrate content
Alimentum and Pregestimil relatively high in fat content, reducing the osmotic load in the
small intestine Both contain substantial amounts of long-chain fats, important
for their trophic effect
Enteral formulasEnteral formulas
p In older infants and toddlers, fiber-supplemented complex formulas
may be instituted as they produce a firmer stool fiber, through its effect on SCFA production, may play a role in
adaptation Newer ‘amino-acid’ formulas do not confer any absorption
advantage
As parenteral nutrition is decreased and enteral nutrition is increased, intermittent parenteral nutrition can be used.
The patient is given the parenteral portion of his nutrition over an 8 to 16 hour period each day
Managing a patient with SBSManaging a patient with SBSLongLong--term managementterm management
nutrition over an 8- to 16-hour period each day In small infants, parenteral nutrition may be required
for the greater part of the 24-hour day, but soon the interval “off ” parenteral nutrition can gradually be increased as the patient’s tolerance of enteral calories increases
Caloric changes are gradually increased, based on the child’s growth needs, to ensure that the child parallels the 50th percentile for both height and weight
Excessive caloric administration is often a problem at
Managing a patient with SBSManaging a patient with SBSLongLong--term managementterm management
pthis stage of management as the child is incapable of regulating his/her own nutrient intake
Careful monitoring of the child’s growth to make certain that the patient’s weight gain is appropriate for length
Fluid losses are often substantial during early stages of short-bowel syndrome management The enteral diets may be diluted with oral electrolyte solution
and the rate of administration increased accordingly to l h l d i lif i ll
Managing a patient with SBSManaging a patient with SBSLongLong--term managementterm management
replace these losses and simplify patient management as well as improve absorption
In the absence of small bowel bacterial overgrowth, the antimotility agents, such as loperamide, may occasionally be useful in slowing intestinal transit and increasing fluid and nutrient retention
Early in the course of therapy, preparations for home parenteral nutrition should be made
Home parenteral nutrition d h f l
Managing a patient with SBSManaging a patient with SBSLongLong--term managementterm management
reduces the cost of long-term management
decreases family stresses and nosocomial infections
It has now become the standard of care in patients with short-bowel syndrome

3/6/2015
9
Colon presentColon present Colon absentColon absent
CarbohydrateCarbohydrate 5050--60% of calories60% of calories
Complex carbohydratesComplex carbohydrates
5050--60% of calories60% of calories
Complex carbohydratesComplex carbohydrates
FatFat 2020--30% of calories30% of calories
Adequate essential fatsAdequate essential fats
MCT / LCTMCT / LCT
3030--40% of calories40% of calories
Adequate essential fatsAdequate essential fats
LCTLCT
ProteinProtein 2020--30% of calories30% of calories
High biologic valueHigh biologic value
2020--30% of calories30% of calories
High biologic valueHigh biologic value
FiberFiber Net secretorsNet secretors
SolubleSoluble
Net secretorsNet secretors
SolubleSoluble
OxalateOxalate RestrictRestrict __
FluidsFluids ORS and /or hypotonicORS and /or hypotonic ORSORS
Chronic complicationsChronic complications
Chronic complicationsChronic complicationsBacterial overgrowthBacterial overgrowth
One of the least-recognized complications
Also one of the most treatable
Overgrowth is considered to occur when b i l i i h ll i ibacterial content increases in the small intestine above normal levels
Usually caused by facultative organisms and a variety of anaerobic bacteria
Treatment Broad-spectrum antibiotics Initially given intermittently, usually the first 5 days
of each month
Chronic complicationsChronic complicationsBacterial overgrowthBacterial overgrowth
Oral metronidazole, either alone or in combination with bactrim is frequently effective
Several other combinations are also helpful Refractory patients may require continuous
antibiotic therapy, with periodic rotation of antibiotics
Excessive fluid secretion frequently occurs in SBS Often due to excessive carbohydrate administration This complication occurs more frequently with bolus than
with continuous enteral feeding
Somatostatin analogs have been used usually with
Chronic complicationsChronic complicationsWatery diarrheaWatery diarrhea
Somatostatin analogs have been used - usually with transient results
Cholestyramine (bile acid binder) is sometimes helpful in short-bowel syndrome with watery diarrhea
Cholestyramine may worsen diarrhea in massive ileal resections
Once patients are free of parenteral nutrition, they are subject to nutritional deficiency states.
Usually, macronutrients can be absorbed in adequate quantities
Trace minerals and vitamins, are often less well
Chronic complicationsChronic complicationsNutritional deficienciesNutritional deficiencies
Trace minerals and vitamins, are often less well absorbed Malabsorption of fat-soluble vitamins, especially A, D, and E,
is common Iron and zinc deficiency is common Selenium absorption may also be impaired Low serum levels of calcium and magnesium are also
frequently observed

3/6/2015
10
Occasionally, the supplemental parenteral vitamins, minerals, micronutrients, and even fluid may be required even if the patient is able to absorb enough calories and protein to meet
Chronic complicationsChronic complicationsNutritional deficienciesNutritional deficiencies
to absorb enough calories and protein to meet growth needs.
Following ileal resection, patients should be monitored carefully for vitamin B12 deficiency
Parenteral nutrition liver diseaseParenteral nutrition liver disease The major cause of death in children with SBS Common in children receiving long-term parenteral
nutrition The incidence increases in inverse proportion to age;
therefore, it is more common in small infants Many mechanisms have been postulated Prevention (?)
aggressive use of enteral feedings – at least 20 - 30% of the total daily caloric intake through the enteral route
Prevention / treatment of bacterial overgrowth Reduction in catheter-related sepsis Omegaven
Surgical techniques in SBSSurgical techniques in SBS
Surgical techniques in SBSSurgical techniques in SBSTapering enteroplasty
Surgical techniques in SBSSurgical techniques in SBS
Intestinal plication
Surgical techniques in SBSSurgical techniques in SBS
Creation of intestinal valves

3/6/2015
11
Surgical techniques in SBSSurgical techniques in SBS
Bianchi procedure
Surgical techniques in SBSSurgical techniques in SBS
STEP procedure
Attempt to wean off PN
Unable to tolerate Participation in
Successful Unsuccessful or incomplete
Monitor for complications
Tolerating home PN
home PN
Appropriate nontransplant surgery
candidate
investigational studies
Successful Unsuccessful or incomplete