image-based coronary tracking and beat-to-beat motion compensation: feasibility for improving...
TRANSCRIPT

Image-Based Coronary Tracking and Beat-to-Beat MotionCompensation: Feasibility for Improving Coronary MRAngiography
Maneesh Dewan,1* Gregory D. Hager,1 and Christine H. Lorenz2,3
A method to reduce the effect of motion variability in MRI of thecoronary arteries is proposed. It involves acquiring real-timelow-resolution images in specific orthogonal orientations, ex-tracting coronary motion from these images, and then usingthis motion information to guide high-resolution MR image ac-quisition on a beat-to-beat basis. The present study establishesthe feasibility and efficacy of the proposed approach usinghuman motion data in an offline implementation, prior to futureonline implementation on an MRI scanner. To track the coro-nary arteries in low-resolution real-time MR images in an accu-rate manner, a tracking approach is presented and validated.The tracking algorithm was run on real-time images acquired at15–20 frames per second in four-chamber, short-axis, and coro-nal views in five volunteers. The systolic and diastolic periods inthe cardiac cycles, computed from the extracted motion infor-mation, had significant variability during the short time periodstypical of cardiac MRI. It is also demonstrated through simula-tion analysis using human tracked coronary motion data thataccounting for this cardiac variability by adaptively changingthe trigger delay for acquisition on a beat-to-beat basis im-proves overall motion compensation and hence MR image qual-ity evaluated in terms of SNR and CNR values. Magn ResonMed 60:604–615, 2008. © 2008 Wiley-Liss, Inc.
Key words: coronary magnetic resonance angiography; tem-plate tracking; motion compensation; image-based motiontracking; heart rate variability; adaptive trigger delay
The coronary arteries undergo a complex motion inducedby both respiratory and cardiac motion (1,2). Furthermore,there is significant variation between respiratory and car-diac motion cycles in a single subject as well as variationacross patients (3–5). This makes it difficult to gauge andpredict the motion of the coronary arteries and compen-sate for that motion during MRI. Therefore, a simple yeteffective way to image the coronary arteries is to acquireimaging data when the effect of cardiac and respiratorymotion is minimal. Current methods achieve this by gatingthe data acquisition for both types of motion. For respira-tory motion, the position of the diaphragm–lung interfacecan be tracked as a function of time using a one-dimen-
sional (1D) “navigator,” which is then used to gate the dataacquisition to the end-expiratory part of the breathingcycle (6,7). Some approaches further improve the respira-tory motion compensation by computing motion withinthe acceptance window through correlation between theacquired and the reference navigator echo. A correctionfactor is then used for slice correction (7,8). For cardiacmotion, it is generally well accepted that the effect ofcardiac motion can be ameliorated by restricting the dataacquisition to a very small time window in the mid-dias-tole (MD) part of the cardiac cycle, where heart motion isknown to be minimal.
Current coronary MRA methods (7,9–11) work reason-ably well in healthy volunteers, but few techniques havebeen shown to work well in larger patient populations(12). In general, these methods suffer from a lack of robust-ness and repeatability in patients as well as healthy vol-unteers. Although qualitatively the reasons for variabilityare not completely understood, we hypothesize that thelimitations of the current methods may be attributed to acombination of the following:
1. The assumption that the diaphragm motion and thecoronary motion are correlated is not perfect (3,13).Also, their relationship does not remain constantover a 10- to 15-min image acquisition period (9,10).
2. The motion of the right and left coronary arteries isdissimilar, with different timings of peak motion inthe cardiac cycle along with different absolute valuesof total displacement, velocity, and acceleration (4,5).
3. During multiple heartbeats, the motion of the coro-nary arteries can vary from beat to beat in a mannerthat cannot be predicted a priori (3,14). This is furthercomplicated in patients, especially those with car-diac arrhythmias.
4. Finally, there is variability of motion across subjectsand patients (3–5).
Proposed Subject-Specific Online Approach
In this study, we hypothesize that one way to reduce theeffect of motion variability and reduce the aforementionedlimitations of the current methods would be to directlymeasure the motion of a particular coronary artery in realtime and to correct for its overall motion during dataacquisition for each heartbeat. This is the basic concept ofthe proposed approach, shown in Fig. 1. As discussed inRef. 5, if it is assumed that the primary direction of motionof the left circumflex artery (LCX) and the right coronaryartery (RCA) are in the base–apex direction in a four-chamber view, and the primary direction of motion of theleft anterior descending (LAD) coronary artery is in ap-
1Department of Computer Science, Johns Hopkins University, Baltimore,Maryland, USA.2Imaging and Visualization, Siemens Corporate Research, Baltimore, Mary-land, USA.3Department of Radiology and Radiological Science, Johns Hopkins Univer-sity, Baltimore, Maryland, USA.Grant sponsor: National Science Foundation; Grant number: EEC-9731478;Grant sponsor: Siemens Corporate Research.*Correspondence to: Maneesh Dewan, Department of Computer Science,Johns Hopkins University, NEB 224, 3400 N. Charles Street, Baltimore, MD21218. E-mail: [email protected] 1 November 2006; revised 1 March 2008; accepted 21 March 2008.DOI 10.1002/mrm.21663Published online in Wiley InterScience (www.interscience.wiley.com).
Magnetic Resonance in Medicine 60:604–615 (2008)
© 2008 Wiley-Liss, Inc. 604

proximately the head–foot direction in a short-axis view, ageneric coordinate system to the heart can be assigned asshown in Fig. 2. Thus, if the motion of the LCX, RCA, andLAD coronary arteries can be measured in these two or-thogonal views, the main component of motion of thecoronary arteries in three dimensions can be derived andused to gate the data acquisition on a beat-to-beat basis. Wediscuss the proposed approach in more detail in the Ma-terials and Methods section.
The proposed subject-specific, online, beat-to-beat mo-tion compensation approach is different from the variousapproaches presented in recent years to account for respi-ratory and cardiac motion variability in coronary imaging.In the next two subsections, we briefly review these ap-proaches.
Respiratory Motion Variability
Various methods have been tried over the last few years toaddress the first limitation mentioned above, with modest
success. It has been shown that using additional navigatorson the heart in the anterior–posterior and the right–leftdirection along with the diaphragmatic navigator (superi-or–inferior direction) leads to an improvement in imagequality (15). The drawbacks of these approaches are thatthey still assume a correlation between heart motion andcoronary motion, and there can be hysteretic effects duringthe respiratory cycle, thereby incorporating more errors(16). Nguyen et al. (17) proposed the use of cardiac fatNAV, which monitors the epicardial fat surrounding thecoronary arteries, to estimate the bulk coronary respiratorymotion. The cardiac fat NAV approach showed improve-ment over the conventional diaphragmatic navigator ap-proach, but was limited by the contamination of the fatNAV by the chest wall signal and the use of only the S/Idisplacement component of the fat NAV.
The problem of drift in the relationship between thediaphragm and coronary motion has been addressed rea-sonably well by means of the diminishing variance algo-
FIG. 1. a: Basic sequence-timing diagram of the proposed approach using image-based navigators. b: Process flow in the proposedapproach.
Image-Based Tracking and Motion Compensation 605

rithm (DVA) (9) and phase ordering with automatic win-dow selection (PAWS) (10) approaches, along with reduc-tions in the scanning time, especially in patients. Recently,a subject-specific method (11) was proposed that builds alow-resolution motion model correlated with multiplenavigators and uses the inverse model online during scan-ning to correct for respiratory motion effects. Althoughthis approach is subject-specific, it does not address vari-ability in cardiac motion and long-term respiratory motionduring an acquisition. The limited success of the respira-tory motion compensation methods proposed so far can beattributed to recent studies (3,18,19) that demonstrated theneed for an online subject-specific complex model to com-pletely characterize the motion of the coronary arteriesdue to respiration.
Cardiac Motion Variability
It has been well established that there is significant heartrate variability (HRV) during both long-term and short-term (duration of 5–15 min) electrocardiographic record-ings in both healthy subjects and patient populations (20).Also, physiological interactions between respiration andcirculation affect the HRV and introduce a high-frequencycomponent of fluctuation in the RR interval variability(21). Unlike respiration variability, the issue of HRV forcoronary MRA has not been widely explored, and only afew methods have been proposed in recent years. Ustun etal. (22) proposed the selection of a subject-specific mini-mal motion window during prescan. The approach im-proves image quality but has the disadvantage that it doesnot account for HRV during the acquisition. Recent workon trigger delay adaptation through neural networks andadaptive averaging (23) has been proposed to account forHR changes during the coronary MRA scan. However, this
method includes the use of the ECG signal instead ofactual coronary motion data, uses the lung–diaphragminterface navigator for respiratory compensation, and doesnot account for beat-to-beat variability in cardiac motion.Recent advances in accelerated parallel imaging (24,25)have revived breath-hold coronary MRA, thereby eliminat-ing the need for complicated methods to compensate forrespiratory motion. However, since these approaches spanover multiple cardiac beats (usually around 30 beats), theyare still affected by beat-to-beat cardiac variability.
In this work, we investigate the extent of the coronaryartery motion variability, with focus on the proximal RCA,LCX, and LAD coronary arteries, and how a subject-spe-cific online proposed approach can be used to compensatefor it. In particular:
1. We hypothesize that real-time imaging can be used totrack these coronary arteries with sufficient accuracyto compensate for beat-to-beat variability in coronarymotion for reducing motion artifact in high-resolu-tion coronary MRA. To accomplish this goal, wepresent the development and validation of a motion-tracking algorithm.
2. We hypothesize that the extent of cardiac motionvariability during high-resolution coronary imagingis significant enough to affect image quality whenfixed acquisition periods are used.
3. We also hypothesize that beat-to-beat compensationusing the proposed approach can improve the imagequality and robustness of high-resolution coronaryMRA.
It is beyond the scope of this work to present a completeonline implementation of the proposed approach withcombined real-time and high-resolution imaging. Instead,our goal is to present initial evidence that this approachwould make an impact on image quality as a basis forfurther development of an online integrated solution.
MATERIALS AND METHODS
In this section we first outline the proposed approach inmore detail. The parameters of the data acquired to test thehypotheses are presented next. Then the details of thetracking algorithm and its validation are discussed. This isfollowed by a study to show the extent of HRV duringcardiac scans. Finally, we present a simulation using ex-tracted human coronary motion that shows the improve-ment in MR image quality when the cardiac variability iscompensated for.
Proposed Approach
The process flow and sequence diagram in Fig. 1 summa-rizes the proposed integrated online approach. The motionof the coronary arteries is tracked using real-time imagingin the two orthogonal slice orientations, as mentionedearlier. The tracked motion data are used to update theslice position/orientation through slice-following, i.e., up-dating the slice geometry at the next time point with thetracked motion data from the previous time point. Thetrigger delay and the acquisition window duration for eachheartbeat are predicted using the tracked coronary motion
FIG. 2. Subject-specific heart coordinate system. The x�, y�, and z�axes of the heart coordinate system are shown in four-chamber andshort-axis views separately in (a) 2D and (b) 3D.
606 Dewan et al.

data during the current and previous cardiac cycles. Thesystem then switches to high-resolution imaging and ac-quires data in the current cardiac cycle. After acquiring thehigh-resolution data, the system switches back to real-timeimaging and the procedure discussed above is repeated forall cardiac cycles. Using the tracked motion data followingthe high-resolution acquisition, one can detect whethersignificant motion occurred during the data acquisitionand whether particular high-resolution data can be reac-quired. We refer to this approach as “image-based naviga-tors.” To make the approach feasible in real time, weassume that the out-of-plane motion between frameswould be relatively small with slice following, and that thedurations of minimal motion of different segments of thecoronary artery are similar. Although presently we areproposing a translation motion model for tracking andslice updating, it is important to point out that the ap-proach is general and more complex motion models, in-cluding rotations, can be easily incorporated into theframework.
In the current study we explore the impact of this ap-proach on image quality in an offline implementation us-ing human motion data, but without the online feedbackloop shown in Fig. 2.
Data Acquisition
To investigate the feasibility of the proposed image-basednavigators, we acquired low-spatial-resolution real-time(LSRRT) images in five healthy volunteers with the sub-jects breathing freely. All subjects gave informed consentto a protocol approved by the local institutional reviewboard. The data consist of real-time steady-state with freeprecession (SSFP) images in short-axis, four-chamber, andcoronal views taken from the five volunteers (four malesand one female, age range � 22–41 years) with the follow-ing parameters: TR/TE/FL � 2.18–2.28 ms/1.09–1.14 ms/49–56°, generalized autocalibrating partially parallel ac-quisitions (GRAPPA) acceleration � 2, in-plane recon-structed resolution � 2.76–2.89 mm, slice thickness �6–8 mm, acquisition matrix size � 50 � 128 to 68 � 128pixels, interpolated matrix size � 88 � 128 to 112 � 128pixels, FOV � 243 � 354 to 324 � 370 mm, at 15–20frames/s for a total of approximately 750 frames duringfree breathing on a 1.5T scanner (Espree, Siemens). Tovalidate the tracking, we also acquired both low-resolu-tion real-time (parameters the same as mentioned abovefor free-breathing data) and high-resolution cine (HRC)images in all three views with the subjects holding theirbreath at end-expiration. The parameters for high-reso-lution cine images were as follows: TR/TE/FL � 1.9 –2.08/1.45–1.54/69 – 80, GRAPPA acceleration � 2, in-plane reconstructed resolution � 1.6 –1.92 mm, slicethickness � 6 mm, acquisition matrix size � 120 � 192to 156 � 192 pixels, FOV � 212.5 � 340 to 300.5 �370 mm, and temporal resolution � 21–33 ms.
The four-chamber and short-axis views were selected asthe orthogonal slice orientations to be used in the pro-posed approach as the coronary motion in these views ispredominantly in-plane (5). The coronal view was ac-quired to compare the actual respiratory motion of thecoronary artery with the lung–diaphragm interface mo-
tion. For more details and results corresponding to thiscomparison, we refer the reader to Ref. 3. The temporalresolution of the real-time data acquisition was selected bypreliminary frequency analysis of the coronary motion inthe high-resolution cine images; the sampling time con-taining the dominant frequency components of the truecoronary motion governed the temporal resolution, whichwas found to be 15–20 Hz.
Tracking Algorithm
One of the challenges for tracking in low-resolution real-time images is that the coronary arteries themselves are notvisible in all frames of the cardiac cycle. In preliminarystudies comparing the motion of the atrioventriculargrooves and the coronary arteries in high-resolution cineimages, we found a high correlation between the two mo-tion profiles. Thus, we rely on tracking the region contain-ing the atrioventricular groove and the fat surrounding thecoronaries as a surrogate for tracking coronary motion.Also, the magnitude of motion expected between frames issmall compared to the size of the tracked region. In thisscenario, region-based tracking methods (26,27) are usu-ally preferred over feature-based methods (28,29) becausethey provide highly accurate (typically to small fractionsof a pixel) motion estimates without depending on specificfeature extraction or enhancement methods. In region-based tracking approaches, one usually minimizes an ob-jective function that matches the appearance of an area ofan image with a stored reference window referred to as a“template.” During the cardiac cycle, the appearance of thetarget region undergoes significant change. As a result, asingle template is insufficient to track through an entirecardiac cycle. Therefore, our tracking framework makesuse of multiple templates selected at time points where thetarget undergoes large changes. There are several ways tomake use of multiple templates in tracking. For example,one simple way is to run the conventional template track-ing (26,27) with each template and then select the bestsolution that most effectively minimizes the objectivefunction. We found that this approach usually fails inmid-systole and early diastole when both appearancechanges and motion are large between frames. Anotherapproach is to compute a small number of orthogonal basisimages from the chosen templates, and to express theappearance variation of the target using linear combina-tions of this basis (30). We use a slightly different approachbut with a similar principle. The basic idea is that theappearance of the target is a rigid-body transformation ofan affine combination of the templates. The optimizationsimultaneously computes both the location and affine mix-ture in each image. Further details of the tracking algo-rithm can be found in Ref. 31.
Tracking of the coronary artery was performed indepen-dently in all three views. In the low-resolution images, a2D translation model was sufficient for modeling the trans-formation. It is important to note that the tracking frame-work is generic and can incorporate more complex mod-els, such as an affine model, without a significant increasein computational cost (26,27). The user identified the cor-onary artery location in real-time images in a single car-diac cycle with the help of high-resolution cine images
Image-Based Tracking and Motion Compensation 607

taken at the same location. Usually a set of two to threedistinctive templates was chosen at end-systolic (ES), MD,and end-diastolic (ED) time points in the cardiac cycle.The tracked motion data were filtered with Savitzky-Golayand Gaussian filters to remove noise. To bring the trackeddata from all volunteers into a consistent coordinate sys-tem, the motion data in the four-chamber and short-axisviews were transformed into the heart coordinate system(see Fig. 2) that was computed using the four-chamber andshort-axis slice orientations. Since the images in the twoorthogonal views were acquired separately, the tracking ofthe coronary artery was performed independently in theseviews. Also, since the slice locations were not updated, thecoronary artery was moving in and out of the plane, andtherefore we were not always tracking the same point onthe coronary artery. Thus, we had to make an assumptionthat the corresponding segment of the coronary artery wasundergoing a similar motion pattern. This is a reasonableassumption, as it is well known that out-of-plane coronarymotion in four-chamber and short-axis views is small (5).However, we note that in the planned online version withslice interleaving (acquiring both orthogonal views inter-leaved) and slice-following, both of these constraints/as-sumptions are relaxed.
In the free-breathing, low-resolution, real-time images,the LCX and RCA were tracked in the four-chamber viewand the LAD was tracked in the short-axis and coronalviews. In one of the volunteers, the foldover artifact fromthe chest wall affected the region around the RCA duringend-systole, thereby preventing the tracking algorithmfrom working. Therefore, we present the results of trackingthe RCA in the four-chamber view from only four of thefive volunteers. For validation of the tracking algorithm(presented in the next section), we focus on the LCA.
Tracking Validation
Since it is almost impossible to obtain the ground truthmotion of the coronary arteries on a beat-to-beat basis,owing to their complex motion, we validated the trackingusing two different approaches. First, we looked at thevariability in the tracked coronary motion in the real-timeimages taken during breath-hold. Since the effects of bothrespiration and cardiac variability are small during a shortduration (six to eight cardiac beats) in breath-hold images,we hypothesized that the variability in coronary motionover the normalized cardiac cycle duration would be smallas well. Thus, we tracked the coronary locations in thereal-time breath-hold images in all three views and thensegmented the systolic and diastolic periods of each car-diac cycle. The first- and second-order derivatives of thetracked displacement data were used to detect ES and EDtime points in each cardiac cycle. The zero crossing of thesecond derivative and the extremum in the first derivativewere used to compute the ES and ED points, and alsomanually checked. The noise in the computation of deriv-atives was reduced using Gaussian filtering (37). An aver-age systolic and diastolic length was computed over six toeight consecutive cardiac beats. The motion data for eachcardiac beat were interpolated to the average lengths, anda mean motion was computed by averaging the interpo-lated motion data from each cardiac beat. Finally, a root
mean squared (RMS) error between the interpolated mo-tion and the mean motion data was computed over theentire normalized cardiac cycle duration. Note that themotion data obtained by tracking were not filtered.
Second, we compared the coronary motion in “high-resolution cine” and “low-resolution real-time” imagestaken during breath-hold in all three views. The coronarylocations in the “high-resolution cine” images were man-ually selected. The systolic time point in the high-resolu-tion motion data was computed using the first- and sec-ond-order derivatives as mentioned above. The high-reso-lution motion data were interpolated to the mean length ofthe segmented breath-hold low-resolution motion data us-ing bilinear interpolation, with the systolic and diastolicsegments interpolated separately to the corresponding av-erage lengths. The error between the interpolated high-resolution motion data and the mean segmented breath-hold low-resolution motion data was then computed. Themean and standard deviation (SD) of the error during theMD to ED period, where the image acquisition is usuallydone, was also computed.
HRV
Since most HRV studies have focused on long-term vari-ability (24 h, for example), there are few quantitative dataindicating the magnitude of variability in the short timespans used for cardiac MRI (20). We analyzed HRV usingthe tracked motion data for the purpose of determining itsimpact on MRI quality (see Results). The systolic anddiastolic time periods were calculated, and the variability(mean and SD) for both time periods was assessed for allfive volunteers.
MR Simulation
To determine the effect of cardiac motion variability onimage quality prior to implementing the method online ona scanner, we used motion data derived from human sub-jects combined with simulation of the MR acquisition.This approach allowed us to combine realistic motion dataand variability into MR simulation data, and to explore anumber of algorithms for selecting the appropriate acqui-sition window and location to reduce motion artifacts.This approach is more efficient and less costly for refiningthe adaptive algorithms than implementing variants on-line in the scanner environment and acquiring live data.We used a synthetic image with a simple structure thatcontained two representative coronary arteries: one ori-ented through the image plane and the other in-plane(each 4 mm in diameter). The coronary arteries are embed-ded in simulated myocardium, which is surrounded bysimulated fat, as shown in Fig. 3. The flowchart in Fig. 3describes the MR simulation analysis. A 2D segmentedgradient-echo imaging sequence was simulated (MATLAB;Mathworks Inc., Natick, MA, USA) with the followingparameters: in-plane resolution � 1 mm, TE/TR/FL �8/15/20, T1 fat � 260 ms, blood � 100 ms (simulatingin-flow), myocardium 870 ms. For each of the five subjects,the coronary (RCA, LAD, or LCX) motion data obtainedfrom the tracking algorithm in each of the coronal, short-axis, and four-chamber views (see Results section) were
608 Dewan et al.

fed to the simulation. The coronary phantom underwentthe extracted coronary motion while the segmented k-space acquisition was performed. Respiratory motion wasfirst removed from the coronary trajectories by filtering outthe low-frequency respiratory component of the motion toreduce the analysis to cardiac motion only. We hypothe-sized that in the presence of cardiac variability (with therespiration removed), the proposed adaptive trigger delayacquisition window selection for each heartbeat wouldprovide better cardiac motion compensation than the stan-dard approach of fixed trigger delay for all heartbeats.Since the number of heartbeats used in the simulation issmall, there is a chance that a single beat with large motionthat falls in the center of k-space will have a large impacton the motion artifacts on the reconstructed image. Thuswe ran the simulation on 10 sets of heartbeats for each caseto remove bias. It is important to note that although wehave not implemented retrospective rejection of beats withlarge motion, this can be easily incorporated into the pro-posed method.
The ideal fixed trigger delay was determined by locatingthe minimal velocity time period of the coronary arteryduring MD in high-resolution cine images acquired at thesame location. The RCA, LCX, or LAD location in high-resolution cine images was manually selected throughoutthe cardiac cycle and then filtered using Savitzky-Golayfilters. A moving-window average approach with a 150-msduration window was run on the coronary velocity (com-puted by means of the finite difference method) and thetime point corresponding to the minimum was selected asthe fixed trigger delay for all acquisition window widths. Itis important to note that previous methods (22,32) chooseeither bulk cardiac or myocardium motion to determinethe optimal fixed trigger delay, in contrast to the actualcoronary motion as used in the present study. The adap-tive trigger delay was determined by the time point ofminimum velocity in the second half of each heartbeat ona beat-to-beat basis. The velocity was calculated using thefirst-order derivatives computed as mentioned in theTracking Validation section. Although one can argue that a
moving-window average approach similar to the one se-lected for estimating the fixed trigger delay would be abetter approach, we chose this simple approach due to itspracticality and ease of implementation for the plannedonline approach using prediction algorithms (38). Acqui-sition window widths of 65 ms, 100 ms, 150 ms, and200 ms were tested for each subject in each of the coronal,short-axis and four-chamber views. The number of lines ink-space per heartbeat was 3 ms, 5 ms, 7.6 ms, and 10.75 msfor acquisition window widths of 65 ms, 100 ms, 150 ms,and 200 ms, respectively.
The CNR of the coronary compared to background“myocardium,” and SNR of the coronary were computedin each case. The CNR and SNR were computed as follows:
SNR � Iavg_cor/�air CNR � �Iavg_cor � Iavg_myo�/�air,
where Iavg_cor and Iavg_myo are the average intensities in thecoronary artery region and the myocardium region sur-rounding the coronary artery, and �air is the SD of inten-sities in the air region. As the motion applied to the syn-thetic image is in two dimensions, the curved coronaryartery (see Fig. 3) is used to discern the effect of in-planemotion, and the circular coronary artery (see Fig. 3) de-picts the effect of through-plane motion. In the presentanalysis, the SNR and CNR values of only the curvedin-plane coronary artery in the synthetic image are pre-sented. We also computed the percent gain or loss inSNR (SNRg-l) of the adaptive delay method over the fixeddelay method as �SNRadaptive � SNRfixed�/min�SNRadaptive,SNRfixed�. For each view in all the subjects, an averageSNRg-l is computed over all the 10 simulation runs. Usingthe average SNRg-l we obtained the best- and worst-caseresults for each acquisition window across all the volun-teers.
Also, a three-way analysis of variance (ANOVA, withfull interaction) was performed on both SNR and CNRvalues to determine the significance of the adaptive triggerdelay approach over the fixed trigger delay method, using
FIG. 3. Flowchart describing the MR simulation analysis.
Image-Based Tracking and Motion Compensation 609

the acquisition window length, volunteer, and trigger de-lay method as the factors. The ANOVA was followed by apairwise comparison with acquisition window length andtrigger delay methods used as factors to test whether themeans for the two trigger delay methods were statisticallydifferent.
RESULTS
Tracking and Validation
The transformed coordinate system and tracked coronarymotion (for the RCA, LCX, and LAD) throughout the data-set (�750 frames) in the four-chamber and short-axisviews from one volunteer (out of five) are shown in Fig. 4.The RMS error values depicting the variability of trackedleft coronary motion in real-time breath-hold images for allfive volunteers in the four-chamber view ranged from 0.32to 0.83 mm in the x� direction and 0.68 to 1.34 mm in they� direction. The range of the RMS error in the short-axisview was 0.43–0.73 mm in the x� direction and 0.47–0.77 mm in the z� direction, whereas in the coronal view it
ranged from 0.5 to 0.81 mm in the x direction and 0.69 to1.17 mm in the y direction.
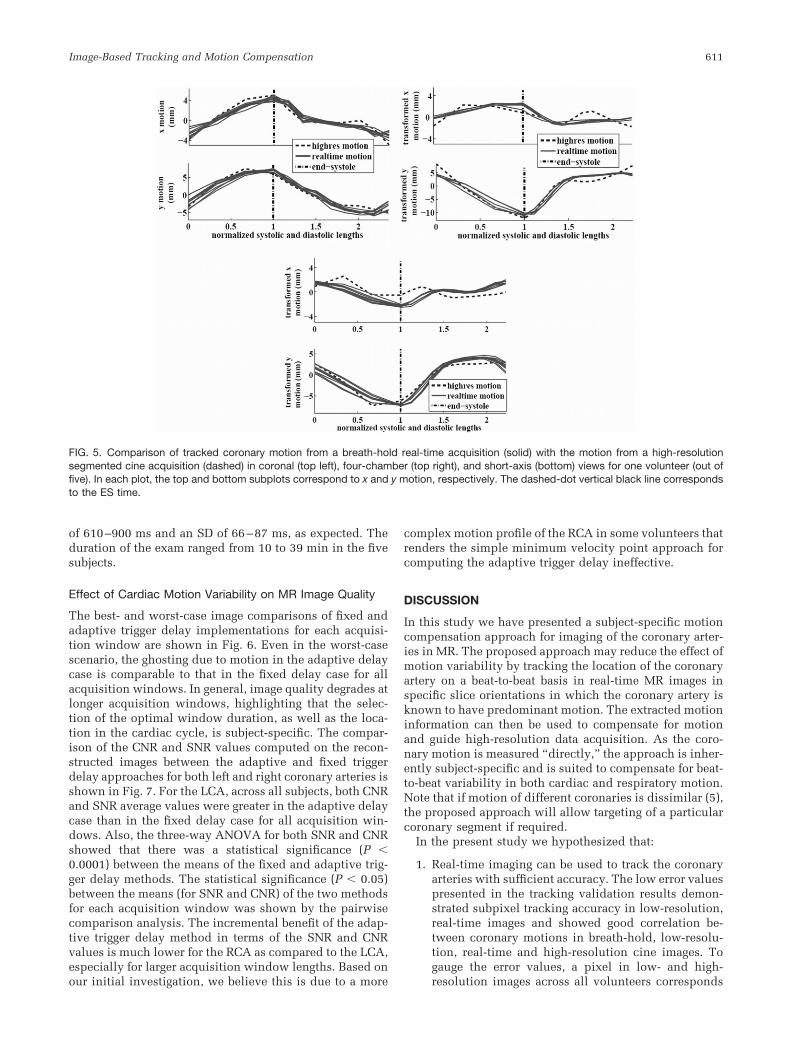
The comparison of the left coronary motion in high-resolution cine and low-resolution real-time imagestaken during breath-hold for one volunteer (out of the five)is shown in Fig. 5. In general, for all of the volunteers, thetotal error between high-resolution and average low-reso-lution tracked motion during the MD to ED period wherethe image acquisition was done was small. The meanvalues of the total error across five volunteers ranged from0.81 to 2.9 mm, 0.71 to 1.66 mm, and 1.0 to 1.94 mm in thefour-chamber, short-axis, and coronal views, respectively.The range of the SD of the total error across all volunteerswas 0.47–0.93 mm, 0.38–0.69 mm, and 0.45–0.84 mm infour-chamber, short-axis, and coronal views, respectively.
HRV
The mean systolic period over all volunteers was 380–400 ms with an SD of 48–62 ms. The diastolic period, onthe other hand, had a much larger variability, with a mean
FIG. 4. Tracked coronary motion in low-resolution real-time images. The (a) top and (b) bottom rows correspond to four-chamber andshort-axis views, respectively. The left column shows the transformed heart coordinate system (in gray), while the right column shows thetransformed tracked coronary motion of the LCX and RCA in four-chamber views and the LAD in short-axis views. The transformed trackedcoronary motion plot shows the x�, y�, and z� motions.
610 Dewan et al.
of 610–900 ms and an SD of 66–87 ms, as expected. Theduration of the exam ranged from 10 to 39 min in the fivesubjects.
Effect of Cardiac Motion Variability on MR Image Quality
The best- and worst-case image comparisons of fixed andadaptive trigger delay implementations for each acquisi-tion window are shown in Fig. 6. Even in the worst-casescenario, the ghosting due to motion in the adaptive delaycase is comparable to that in the fixed delay case for allacquisition windows. In general, image quality degrades atlonger acquisition windows, highlighting that the selec-tion of the optimal window duration, as well as the loca-tion in the cardiac cycle, is subject-specific. The compar-ison of the CNR and SNR values computed on the recon-structed images between the adaptive and fixed triggerdelay approaches for both left and right coronary arteries isshown in Fig. 7. For the LCA, across all subjects, both CNRand SNR average values were greater in the adaptive delaycase than in the fixed delay case for all acquisition win-dows. Also, the three-way ANOVA for both SNR and CNRshowed that there was a statistical significance (P �0.0001) between the means of the fixed and adaptive trig-ger delay methods. The statistical significance (P � 0.05)between the means (for SNR and CNR) of the two methodsfor each acquisition window was shown by the pairwisecomparison analysis. The incremental benefit of the adap-tive trigger delay method in terms of the SNR and CNRvalues is much lower for the RCA as compared to the LCA,especially for larger acquisition window lengths. Based onour initial investigation, we believe this is due to a more
complex motion profile of the RCA in some volunteers thatrenders the simple minimum velocity point approach forcomputing the adaptive trigger delay ineffective.
DISCUSSION
In this study we have presented a subject-specific motioncompensation approach for imaging of the coronary arter-ies in MR. The proposed approach may reduce the effect ofmotion variability by tracking the location of the coronaryartery on a beat-to-beat basis in real-time MR images inspecific slice orientations in which the coronary artery isknown to have predominant motion. The extracted motioninformation can then be used to compensate for motionand guide high-resolution data acquisition. As the coro-nary motion is measured “directly,” the approach is inher-ently subject-specific and is suited to compensate for beat-to-beat variability in both cardiac and respiratory motion.Note that if motion of different coronaries is dissimilar (5),the proposed approach will allow targeting of a particularcoronary segment if required.
In the present study we hypothesized that:
1. Real-time imaging can be used to track the coronaryarteries with sufficient accuracy. The low error valuespresented in the tracking validation results demon-strated subpixel tracking accuracy in low-resolution,real-time images and showed good correlation be-tween coronary motions in breath-hold, low-resolu-tion, real-time and high-resolution cine images. Togauge the error values, a pixel in low- and high-resolution images across all volunteers corresponds
FIG. 5. Comparison of tracked coronary motion from a breath-hold real-time acquisition (solid) with the motion from a high-resolutionsegmented cine acquisition (dashed) in coronal (top left), four-chamber (top right), and short-axis (bottom) views for one volunteer (out offive). In each plot, the top and bottom subplots correspond to x and y motion, respectively. The dashed-dot vertical black line correspondsto the ES time.
Image-Based Tracking and Motion Compensation 611

to 2.76–2.89 mm and 1.6–1.92 mm, respectively.Other factors of variability, such as the effect of res-piration and the repeatability of the cardiac positionover heartbeats, are still present. Keeping in mind thevariability in coronary motion, manual coronary se-lection, and tracking, the error values are small andwithin acceptable limits. The interpolation of motiondata is another source of error. The tracking resultswere also assessed visually and found to be in goodagreement, with the exception of occasional mis-aligned frames in early diastole, which is character-ized by rapid motion. Also, the tracking algorithmwas able to handle long-term variations in appear-ance due to respiration. Although in the presentedwork the tracking was done offline in MATLAB(Mathworks Inc.), we have implemented the trackingalgorithm in C, and the tracking computation timeper image frame is now less than half a millisecondon a standard laptop.
2. The variability in heart rate and cardiac motion sig-nificantly affect the image quality when fixed acqui-sition periods are used. We have shown that there isa significant amount of variation in the heart rate
during the time spans used for cardiac MRI. Thevariability in the diastolic period is much larger thanduring the systolic period, which is in agreementwith prior work in HRV (33,34). As shown in Fig. 6,motion artifacts are more pronounced when a fixedtrigger delay is used, resulting in low SNR and CNRvalues (Fig. 7). Thus, we conclude that the imagequality of the current MR methods for coronary im-aging that use fixed trigger delays for cardiac motiongating is limited in part due to the motion artifactsintroduced by the variability in cardiac cycles.
3. Beat-to-beat motion compensation can improve im-age quality. We demonstrate that compensating forthe cardiac motion variability by adaptively choosingthe trigger delay on a beat-to-beat basis reduces themotion artifacts and hence improves the image qual-ity (Fig. 6). This was done by simulating imaging of arepresentative synthetic coronary artery that under-goes the motion extracted from tracking the actualcoronary artery in real-time MR images. For the LCA,the SNR and CNR for all of the volunteers increasedfor different acquisition windows if the trigger delaywas chosen adaptively as compared to the fixed case
FIG. 6. Comparison of adaptive and fixed trigger delays for image acquisition as a function of the acquisition window (in milliseconds) forthe simulation analysis. The left and right columns show the best and worst results in terms of percent gain or loss in SNR of the adaptivedelay method over the fixed delay method for a particular acquisition window from the set of 10 runs for all volunteers in all views (see MRSimulation section). The five most representative images out of the 10 are shown. The top and bottom rows in each subfigure correspondto the adaptive and fixed trigger delay case, respectively. Note that the phase-encoding and frequency-encoding directions are along thecolumn and row of the image, respectively. Note that even in the worst-case comparison, the adaptive delay method quality is comparableto the fixed delay method, while in the best-case comparison, the adaptive delay method shows significantly better image quality ascompared to the fixed delay.
612 Dewan et al.
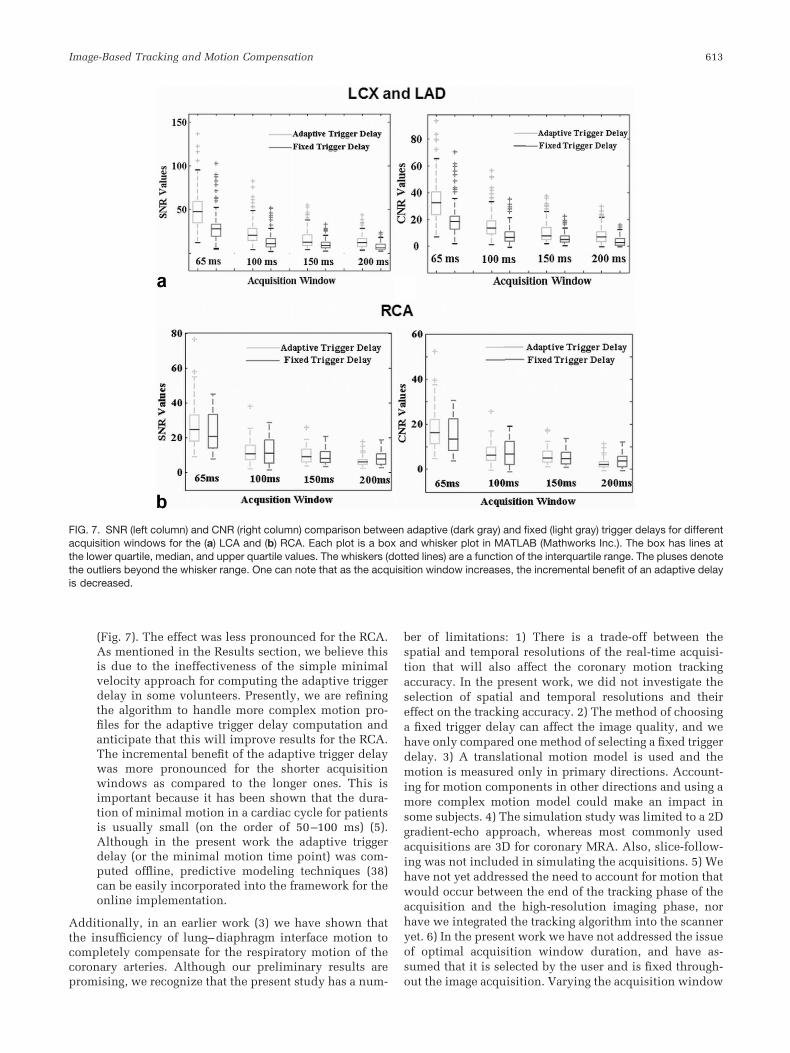
(Fig. 7). The effect was less pronounced for the RCA.As mentioned in the Results section, we believe thisis due to the ineffectiveness of the simple minimalvelocity approach for computing the adaptive triggerdelay in some volunteers. Presently, we are refiningthe algorithm to handle more complex motion pro-files for the adaptive trigger delay computation andanticipate that this will improve results for the RCA.The incremental benefit of the adaptive trigger delaywas more pronounced for the shorter acquisitionwindows as compared to the longer ones. This isimportant because it has been shown that the dura-tion of minimal motion in a cardiac cycle for patientsis usually small (on the order of 50–100 ms) (5).Although in the present work the adaptive triggerdelay (or the minimal motion time point) was com-puted offline, predictive modeling techniques (38)can be easily incorporated into the framework for theonline implementation.
Additionally, in an earlier work (3) we have shown thatthe insufficiency of lung–diaphragm interface motion tocompletely compensate for the respiratory motion of thecoronary arteries. Although our preliminary results arepromising, we recognize that the present study has a num-
ber of limitations: 1) There is a trade-off between thespatial and temporal resolutions of the real-time acquisi-tion that will also affect the coronary motion trackingaccuracy. In the present work, we did not investigate theselection of spatial and temporal resolutions and theireffect on the tracking accuracy. 2) The method of choosinga fixed trigger delay can affect the image quality, and wehave only compared one method of selecting a fixed triggerdelay. 3) A translational motion model is used and themotion is measured only in primary directions. Account-ing for motion components in other directions and using amore complex motion model could make an impact insome subjects. 4) The simulation study was limited to a 2Dgradient-echo approach, whereas most commonly usedacquisitions are 3D for coronary MRA. Also, slice-follow-ing was not included in simulating the acquisitions. 5) Wehave not yet addressed the need to account for motion thatwould occur between the end of the tracking phase of theacquisition and the high-resolution imaging phase, norhave we integrated the tracking algorithm into the scanneryet. 6) In the present work we have not addressed the issueof optimal acquisition window duration, and have as-sumed that it is selected by the user and is fixed through-out the image acquisition. Varying the acquisition window
FIG. 7. SNR (left column) and CNR (right column) comparison between adaptive (dark gray) and fixed (light gray) trigger delays for differentacquisition windows for the (a) LCA and (b) RCA. Each plot is a box and whisker plot in MATLAB (Mathworks Inc.). The box has lines atthe lower quartile, median, and upper quartile values. The whiskers (dotted lines) are a function of the interquartile range. The pluses denotethe outliers beyond the whisker range. One can note that as the acquisition window increases, the incremental benefit of an adaptive delayis decreased.
Image-Based Tracking and Motion Compensation 613

duration on a beat-to-beat basis may provide additionalbenefit.
Future Work
Online Implementation Issues
As the results from our present study are promising, weplan to integrate the real-time coronary tracking into theMR scanner and further evaluate the proposed approach.This will involve sequence modification that will allowswitching between a real-time tracking mode and a high-resolution data acquisition mode. The real-time capabili-ties of the Siemens Avanto/Espree scanners allow real-time decisions regarding the keeping/discarding of dataand shifting of slice position, based on the implementationof traditional navigators. Including the application ofpreparation pulses (fat saturation, T2 prep, approach tosteady state), the transition time is estimated to be approx-imately 50–70 ms. The temporal resolution for a low-resolution image acquisition is 50–70 ms (15–20 framesper second), and since the approach requires the acquisi-tion of two orthogonal views, the total acquisition time forlow-resolution real-time images is 100–140 ms. The com-putation time for the tracking algorithm is on the order of1 ms and prediction algorithms should be on the order of10 ms (38), which is relatively small compared to theimage acquisition time and should not be a limiting factorin the online implementation. Since the motion informa-tion can be extracted after the image acquisition, it will benecessary to be able to accurately predict the adaptivetrigger delay at least 200 ms before the high-resolution dataacquisition. Thus, we are investigating the development ofonline algorithms based on Ref. 38 for predicting the adap-tive trigger delay using tracked coronary motion history, aswell as a retrospective (next heartbeat) review of motionand discarding of beats with motion that is dissimilar tothat of an average cardiac cycle. We would also like tobriefly mention the issue of saturation bands that will becreated by real-time data acquisition and might affect thehigh-resolution data acquisition. The signal saturationbands would be restricted to the intersection planes of theorthogonal views and result in a signal dropoff of approx-imately 30%, so we believe their effect on the trackingalgorithm would be minor.
In parallel, we plan to extend the simulation study to 3Dwith different k-space sampling schemes and image con-trasts (SSFP, for example). We are currently working onautomating the following steps in the overall tracking al-gorithm: 1) selecting templates in an optimal manner toreplace the current manual template selection algorithm,and 2) incorporating the Kalman filter (36) estimation tech-nique to perform the filtering online, which is currentlydone offline.
Finally, the generic nature of the proposed approachallows the use of motion extracted from other sources togate the data acquisition on a beat-to-beat basis. For exam-ple, bulk cardiac motion from self-gating (39) can also beused to correct for beat-to-beat motion variability. In thefuture, we plan to compare the proposed approach usingdifferent motion extraction methods.
CONCLUSIONS
We have presented a multiple template-based tracking al-gorithm that tracks coronary motion reliably and accu-rately in low-resolution real-time MR images in differentviews. Using the tracked coronary motion, it was shownthat there is significant variability in coronary motion.Through simulations, we have also demonstrated that ac-counting for that variability with adaptive window selec-tion improves MR image quality. Therefore, we believe theproposed subject-specific “image-based navigators” ap-proach is feasible and will potentially provide an advan-tage over existing methods for coronary MRI by reducingthe assumptions regarding motion of the coronary arteries.Also, the generic nature of the approach makes it easilyextendable to imaging other cardiac structures undergoingcomplex motion, such as valve imaging.
ACKNOWLEDGMENTS
We thank Siemens Corporate Research and the Engineer-ing Research Center for Computer-Integrated Surgical Sys-tems and Technology for their support in this research.
REFERENCES
1. Shechter G, Devernay F, Coste-Maniere E, Quyyumi A, McVeigh ER.Three-dimensional motion tracking of coronary arteries in biplanecineangiograms. IEEE Trans Med Imaging 2003;22:493–503.
2. Wang Y, Riederer SJ, Ehman RL. Respiratory motion of the heart:kinematics and implications for the spatial resolution in coronaryimaging. Magn Reson Med 1995;33:713–719.
3. Dewan M, Hager GD, Lorenz CH. Image-based tracking and predictionof coronary motion for coronary MR angiography (abstract). J Cardio-vasc Magn Reson 2006;8:215–216.
4. Wang Y, Vidan E, Bergman GW. Cardiac motion of coronary arteries:variability in the rest period and implications for coronary MR angiog-raphy. Radiology 1999;213:751–758.
5. Hofman MBM, Wickline SA, Lorenz CH. Quantification of in-planemotion of the coronary arteries during the cardiac cycle: implicationsfor acquisition window duration for MR flow quantification. J MagnReson Imaging 1998;8:568–576.
6. Wang Y, Rossman PJ, Grimm RC, Riederer SJ, Ehman RL. Navigator-echo-based real-time respiratory gating and triggering for reduction ofrespiration effects in three-dimensional coronary MR angiography. Ra-diology 1996;198:55–60.
7. Stuber M, Botnar RM, Spuentrup E, Kissinger KV, Manning WJ. Three-dimensional high resolution fast spin echo coronary magnetic reso-nance angiography. Magn Reson Med 2001;45:206–211.
8. Oshinski JN, Hofland L, Dixon WT, Pettigrew RI. Magnetic resonancecoronary angiography using navigator echo gated real-time slice follow-ing. Int J Card Imaging 1998;14:191–199.
9. Sachs T, Meyer C, Irarrazabal P, Hu B, Nishimura D, Macovski A. Thediminishing variance algorithm for real-time reduction of motion arti-facts in MRI. Magn Reson Med 1995;34:412–422.
10. Jhooti P, Gatehouse PD, Keegan J, Bunce NH, Taylor AM, Firmin DN.Phase ordering with automatic window selection (PAWS): a novelmotion-resistant technique for 3D coronary imaging. Magn Reson Med2000;43:470–480.
11. Manke D, Nehrke K, Bornert P. Novel prospective respiratory motioncorrection approach for free-breathing coronary MR angiography usinga patient-adapted affine motion model. Magn Reson Med 2003;50:122–131.
12. Kim WY, Danias PG, Stuber M, Flamm SD, Plein S, Nagel E, LangerakSE, Weber OM, Pedersen EM, Schmidt M, Botnar RM, Manning WJ.Coronary magnetic resonance angiography for the detection of coronarystenoses. N Engl J Med 2001;345:1863–1869.
13. Danias PG, Stuber M, Botnar RM, Kissinger KV, Edelman RR, WanningWJ. Relationship between motion of coronary arteries and diaphragmduring free-breathing: lessons from real-time MR imaging. AJR Am JRoentgenol 1999;172:1061–1065.
614 Dewan et al.

14. Dewan M, Hager GD, Shea SM, Lorenz CH. Compensating for beat-to-beat variation in coronary motion improves image quality in coronaryMR. In: Proceedings of the 14th Annual Meeting of ISMRM, Seattle,WA, USA, 2006 (Abstract 2159).
15. Sachs TS, Craig MH, Pauly JM, Hu BS, Nishimura DG, Macovski A. Thereal-time interactive 3-D-DVA for robust coronary MRA. IEEE TransMed Imaging 2000;19:73–79.
16. Nehrke K, Bornert P. Study of the respiratory motion of the heart usingmultiple navigator pulses. In: Proceedings of the 8th Annual Meeting ofISMRM, Denver, CO, USA, 2000 (Abstract 404).
17. Nguyen TD, Nuval A, Mulukutla S, Wang Y. Direct monitoring ofcoronary artery motion with cardiac fat navigator echoes. Magn ResonMed 2003;50:235–241.
18. Shechter G, Ozturk C, Resar JR, McVeigh ER. Respiratory motion of theheart: translation, rigid body, affine, or more? J Cardiovasc Magn Reson2004;6:435–436.
19. Manke D, Nehrke K, Bornert P, Rosch P, Dossel O. Respiratory motionin coronary magnetic resonance angiography: a comparison of differentmotion models. J Magn Reson Imaging 2002;15:661–671.
20. Heart rate variability. Standards of measurement, physiological inter-pretation, and clinical use. Task Force of the European Society ofCardiology and the North American Society of Pacing and Electrophys-iology. Eur Heart J 1996;17:354–381.
21. Yasuma F, Hayano J. Respiratory sinus arrhythmia: why does theheartbeat synchronize with respiratory rhythm? Chest 2004;125:683–690.
22. Ustun AO, Abd-Elmoniem KZ, Stehning C, Stuber M. Automated iden-tification of minimal myocardial motion period during a cardiac cyclefor coronary MRI. J Cardiovasc Magn Reson 2005;7:194–95.
23. Buehrer M, Kozerke S, Boesiger P. Trigger delay adaptation duringcoronary MRA by prediction of heart rate variations. In: Proceedings ofthe 13th Annual Meeting of ISMRM, Miami Beach, FL, USA, 2005(Abstract 2240).
24. Park J, Larson AC, Zhang Q, Simonetti O, Li D. 4D radial coronaryartery imaging within a single breath-hold: cine angiography withphase-sensitive fat suppression (CAPS). Magn Reson Med 2005;54:833–840.
25. Niendorf T, Hardy CJ, Cline H, Giaquinto RO, Grant AK, Rofsky NM,Sodickson DK. Highly accelerated single breath-hold coronary MRA
with whole heart coverage using a cardiac optimized 32-element coilarray. In: Proceedings of the 13th Annual Meeting of ISMRM, MiamiBeach, FL, USA, 2005 (Abstract 702).
26. Hager GD, Belhumeur PN. Efficient region tracking with parametricmodels of illumination and geometry. IEEE Trans Patt Anal Mach Intel1998;20:1025–1039.
27. Baker S, Mathews I. Lucas-Kanade 20 years on: a unifying framework.Int J Comput Vis 2004;56:221–255.
28. Blake A, Isard M. Active contours. Berlin: Springer-Verlag; 1998.29. Faugeras OD, Lustaman F, Toscani G. Motion and structure from point
and line matches. In: Proceedings of the International Conference onComputer Vision, London, UK, June 1987, pp. 25–33, IEEE ComputerSociety Press.
30. Black MJ, Jepson AD. Eigentracking: robust matching and tracking ofarticulated objects using a view-based representation. Int J Comput Vis1998;26:63–84.
31. Dewan M, Hager GD, Lorenz CH. Robust image-based motion trackingfor coronary MR angiography. In: Proceedings of the 1st InternationalWorkshop on Computer Vision for Intravascular and Intracardiac Im-aging, MICCAI, 2006.
32. Bi X, Chung Y, Zuehlsdorff S, Li D. Optimal selection of the subject-specific data acquisition window for coronary MRA. In: Proceedings ofthe 14th Annual Meeting of ISMRM, Seattle, WA, 2006 (Abstract 2163).
33. Lewis RP, Rittogers SE, Froester WF, Boudoulas H. A critical review ofthe systolic time intervals. Circulation 1977;56:146–158.
34. Boudoulas H, Rittogers SE, Lewis RP, Leier CV, Weissler AM. Changesin diastolic time with various pharmacologic agents: implications formyocardial perfusion. Circulation 1979;60:164–169.
35. Huber ME. Coronary artery magnetic resonance angiography. Ph.D.dissertation, Swiss Federal Institute of Technology, Zurich, 2003.
36. Sorenson HW. Kalman filtering: theory and application. New York:IEEE Press; 1985.
37. Gonzalez RC, Woods RE. Digital image processing. Saddle River, NJ:Prentice Hall; 2002.
38. Ginhoux R, Gangloff J, de Mathelin M, Soler L, Sanchez MMA, Mares-caux J. Active filtering of physiological motion in robotized surgeryusing predictive control. IEEE Trans Robot Automat 2005;21:67–79.
39. Larson AC, White RD, Laub G, McVeigh ER, Li D, Simonetti OP.Self-gated cardiac cine MRI. Magn Reson Med 2004;51:93–102.
Image-Based Tracking and Motion Compensation 615