icjr cleveland clinic: how i do the direct anterior approach with a table stefan kreuzer, md...
TRANSCRIPT

ICJR Cleveland Clinic:
How I do the Direct Anterior Approach with
a table
Stefan Kreuzer, MDHouston, TexasMemorial Bone and Joint Clinic

Disclosure and Disclaimers:• Consultant to Stryker
• Consultant to Makosurgical
• Consultant to Corin
• Principal of IOT
• Some of the x-rays may contain off label use of implants

Total hip replacement has been Total hip replacement has been
one of the most successful one of the most successful
operations of the 20operations of the 20thth century century
Where Have We Been?Where Have We Been?


Posterior: Posterior: Woolson et alWoolson et al Methods:
– consecutive THA– 3 surgeons– Posterior approach
Results: – Increased wound complication– Acetabular malposition – Poor fit and fill in MIS group
Conclusion: Their study did not support the benefit of MIS posterior approach.
Woolson et al, JBJS Woolson et al, JBJS 20042004

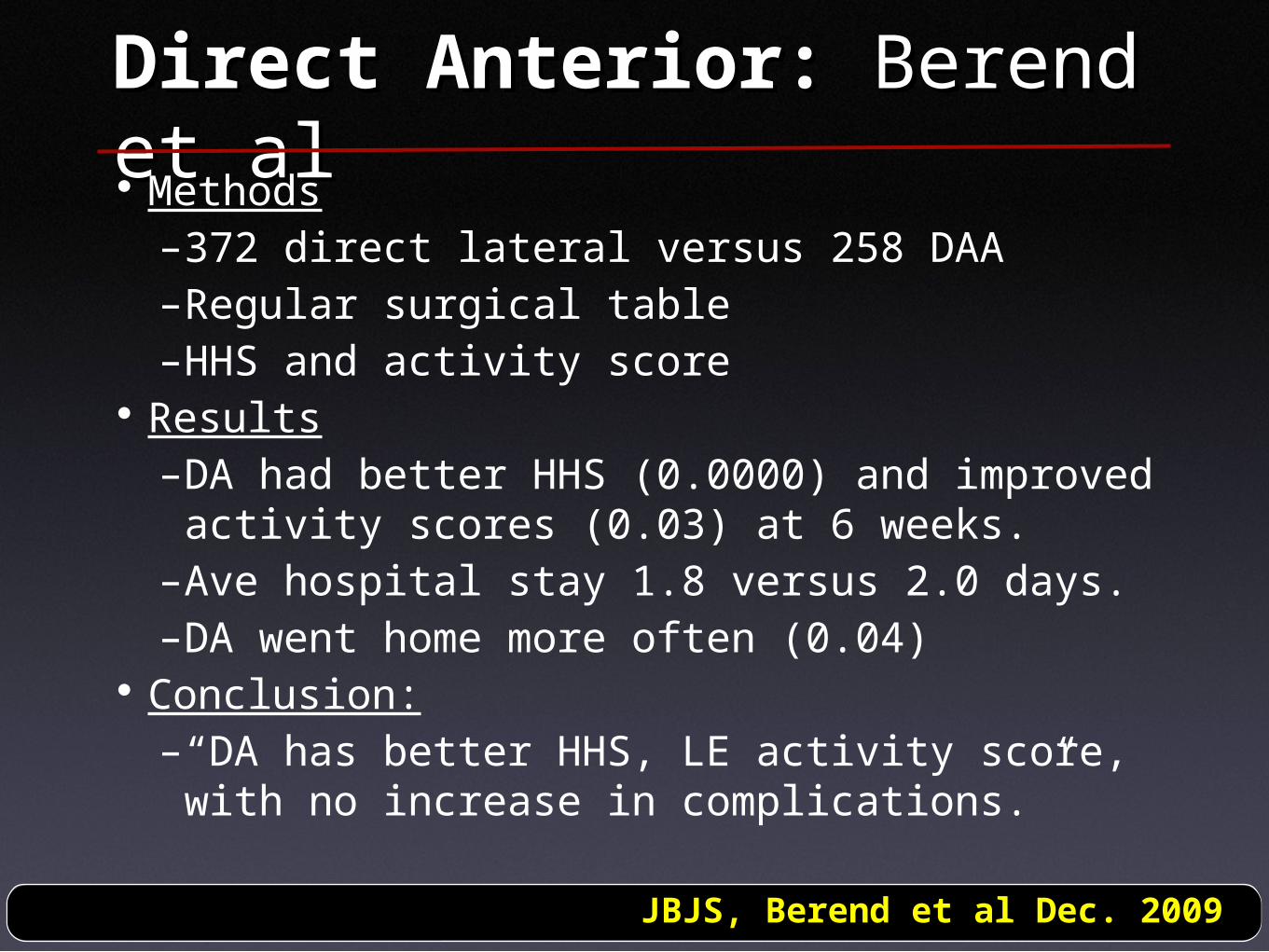
Direct Anterior: Direct Anterior: Berend Berend et alet al Methods
–372 direct lateral versus 258 DAA–Regular surgical table–HHS and activity score
Results–DA had better HHS (0.0000) and improved activity scores (0.03) at 6 weeks.
–Ave hospital stay 1.8 versus 2.0 days.–DA went home more often (0.04)
Conclusion:–“DA has better HHS, LE activity score, with no increase in complications.”
JBJS, Berend et al Dec. 2009

AAHKS meeting 2010, AAHKS meeting 2010, DallasDallas
With show of hand, how With show of hand, how many surgeon are doing many surgeon are doing the direct anterior the direct anterior approach:approach:2008:2008: 5%5%2009:2009: 9%9%2010:2010: 16%16%

1) Implant position: Harvard Study
At Massachusetts General Hospital, only 36.9% of cups were in the desired zone of placement.
Malchau, et al" 39th Annual Course, MGH/BWH, Advances in Arthroplasty, October 2009. Harvard Medical School, Boston

Can we improve implant position??

The patient of today

2) Bone Conservation?
Living longerMore activeHaving surgery earlierMore obese

Can we be more bone preserving??

Anterior Approach for Anterior Approach for THR:THR:Technique of Robert Technique of Robert JudetJudetHueter Approach (short Smith-
Pete)Performed on Orthopaedic Table
or leg holding deviceRecently popularized by Dr. Matta


Anterior Approach (one Anterior Approach (one incision)incision)
Incision (6-10 cm)- Smith-Petersen approach
Interval- Tensor fascia lata and
sartorius/rectus femoris
Releases - None really
C-arm is not requiredSpecial table attachment

Anterior Approach (one Anterior Approach (one incision)incision)
Incision (6-10 cm)- Smith-Petersen approach
Interval- Tensor fascia lata and
sartorius/rectus femoris
Releases - None really
C-arm is not requiredSpecial table attachment

Anterior Approach (one Anterior Approach (one incision)incision)
Incision (6-10 cm)- Smith-Petersen approach
Interval- Tensor fascia lata and
sartorius/rectus femoris
Releases - None really
C-arm is not requiredSpecial table attachment

Anterior Approach (one Anterior Approach (one incision)incision)
Incision (6-10 cm)- Smith-Petersen approach
Interval- Tensor fascia lata and
sartorius/rectus femoris
Releases - None really
C-arm is not requiredSpecial table attachment


$187'000

$38'000


1) Can we Improve implant 1) Can we Improve implant position?position?

Questions: Does computer navigation in conjunction with the direct anterior approach....
improve cup position ?improve leg length determination ?add surgical time ?

MethodMethod
Retrospective review of 300 patientsRetrospective review of 300 patients
Most recent 150 conventional compared to first Most recent 150 conventional compared to first 150 navigated THA comparing:150 navigated THA comparing:
Leg Length Discrepancy (LLD)Leg Length Discrepancy (LLD)
Cup AngleCup Angle
Total Surgical Time (Incision to final reduction)Total Surgical Time (Incision to final reduction)

Surgical TimeSurgical Time
AuthorAuthor Conv.Conv. Nav.Nav. P-valueP-value
NajarianNajarian 105105 124124 1919 0.0060.006
KalteisKalteis 7575 8383 88 0.0020.002
KreuzerKreuzer 6161 5656 -5-5 <0.0001<0.0001

Surgical TimeSurgical Time
AuthorAuthor Conv.Conv. Nav.Nav. P-valueP-value
NajarianNajarian 105105 124124 1919 0.0060.006
KalteisKalteis 7575 8383 88 0.0020.002
KreuzerKreuzer 6161 5656 -5-5 <0.0001<0.0001
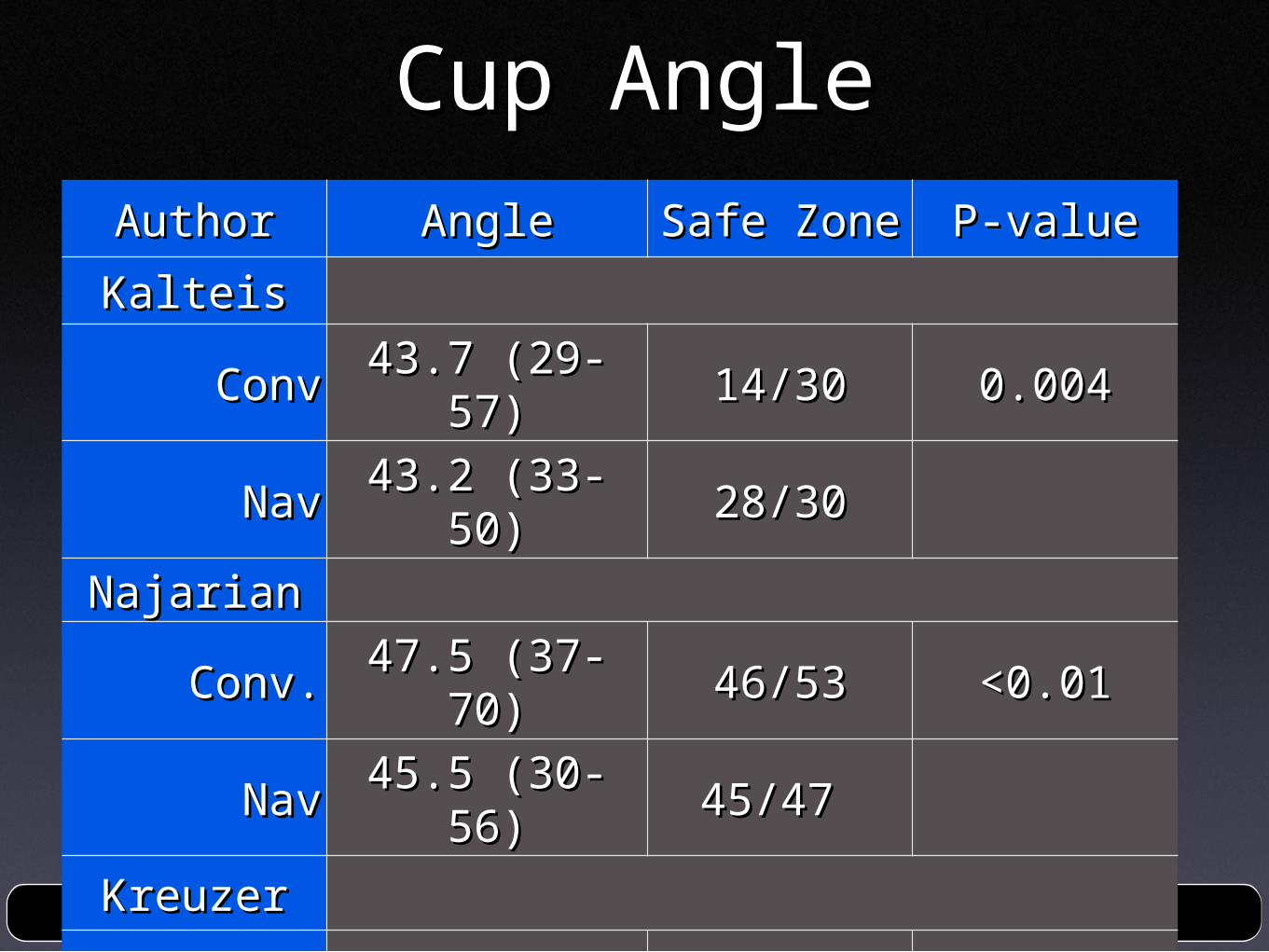
Cup AngleCup AngleAuthorAuthor AngleAngle Safe ZoneSafe Zone P-valueP-value
KalteisKalteis
ConvConv 43.7 (29-57)43.7 (29-57) 14/3014/30 0.0040.004
NavNav 43.2 (33-50)43.2 (33-50) 28/3028/30
NajarianNajarian
Conv.Conv. 47.5 (37-70)47.5 (37-70) 46/5346/53 <0.01<0.01
NavNav 45.5 (30-56)45.5 (30-56) 45/47 45/47
KreuzerKreuzer
ConvConv 36 (19-52)36 (19-52) 131/150131/150 <0.0001<0.0001
NavNav 41 (32-54)41 (32-54) 145/150145/150

Cup AngleCup AngleAuthorAuthor AngleAngle Safe ZoneSafe Zone P-valueP-value
KalteisKalteis
ConvConv 43.7 (29-57)43.7 (29-57) 14/3014/30
NavNav 43.2 (33-50)43.2 (33-50) 28/3028/30 46%46%
NajarianNajarian
Conv.Conv. 47.5 (37-70)47.5 (37-70) 46/5346/53
NavNav 45.5 (30-56)45.5 (30-56) 45/47 45/47 87%87%
KreuzerKreuzer
ConvConv 36 (19-52)36 (19-52) 131/150131/150
NavNav 41 (32-54)41 (32-54) 145/150145/150 87%87%

Cup AngleCup AngleAuthorAuthor AngleAngle Safe ZoneSafe Zone P-valueP-value
KalteisKalteis
ConvConv 43.7 (29-57)43.7 (29-57) 14/3014/30 0.0040.004
NavNav 43.2 (33-50)43.2 (33-50) 28/3028/30 93%93%
NajarianNajarian
Conv.Conv. 47.5 (37-70)47.5 (37-70) 46/5346/53 <0.01<0.01
NavNav 45.5 (30-56)45.5 (30-56) 45/47 45/47 96%96%
KreuzerKreuzer
ConvConv 36 (19-52)36 (19-52) 131/150131/150 <0.0001<0.0001
NavNav 41 (32-54)41 (32-54) 145/150145/150 97%97%

ConclusionConclusionNavigation is easily incorporated when using Navigation is easily incorporated when using the DAAthe DAA
Surgical time decreasedSurgical time decreased
Cup angle is comparable to conventional and Cup angle is comparable to conventional and more precisemore precise
LLD is better than conventional and more LLD is better than conventional and more preciseprecise
More work needed but preliminary results More work needed but preliminary results promisingpromising

2) Can We Be Bone 2) Can We Be Bone Conserving?Conserving?

What do we mean with Bone Conserving?
Less bone resectionMore anatomic reconstruction of the hip joint
More Physiologic loading of the proximal femur

Physiologic Loading of Proximal Femur
Long stems transfer less load to the bone, resulting in stress shielding
A neck preserving stem transfers more load to the proximal femur due to its reduced overall stem length and proximal geometry.
It minimize periprosthetic bone loss by optimizing prox. femoral loading and resecting less bone
There was no significant difference (p < 0.05) between strain energy density of implanted MiniHip vs. intact femur , i.e. MiniHip loads physiologically

Physiologic Loading of Proximal Femur
Where Are We Going next?Where Are We Going next?

Thank you.

Thank you